Back to Journals » Journal of Asthma and Allergy » Volume 16
Perioperative Care of the Pediatric Patient and an Algorithm for the Treatment of Intraoperative Bronchospasm
Received 24 March 2023
Accepted for publication 17 June 2023
Published 23 June 2023 Volume 2023:16 Pages 649—660
DOI https://doi.org/10.2147/JAA.S414026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Birva Khara,1 Joseph D Tobias2,3
1Department of Anesthesiology, Shree Krishna Hospital, Pramukhswami Medical College and Bhaikaka University, Karamsad, Gujarat, India; 2Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 3The Ohio State University College of Medicine, Columbus, OH, USA
Correspondence: Joseph D Tobias, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH, 43205, USA, Tel +1 614 722-4200, Fax +1 614 722-4203, Email [email protected]
Abstract: Asthma remains a common comorbid condition in patients presenting for anesthetic care. As a chronic inflammatory disease of the airway, asthma is known to increase the risk of intraoperative bronchospasm. As the incidence and severity of asthma and other chronic respiratory conditions that alter airway reactivity is increasing, a greater number of patients at risk for perioperative bronchospasm are presenting for anesthetic care. As bronchospasm remains one of the more common intraoperative adverse events, recognizing and mitigating preoperative risk factors and having a pre-determined treatment algorithm for acute events are essential to ensuring effective resolution of this intraoperative emergency. The following article reviews the perioperative care of pediatric patients with asthma, discusses modifiable risk factors for intraoperative bronchospasm, and outlines the differential diagnosis of intraoperative wheezing. Additionally, a treatment algorithm for intraoperative bronchospasm is suggested.
Keywords: asthma, bronchospasm, pediatric anesthesia, wheezing, wheezing-associated respiratory illness
Introduction
Asthma is a chronic inflammatory disease of the airway, characterized by recurrent episodes of wheezing. Histologic examination reveals the accumulation of inflammatory mediators (eosinophils and leukotrienes) that result in inflammation and provoke exaggerated smooth-muscle reactivity and constriction.1 Common clinical manifestations include intermittent episodes of reversible airway obstruction that may be manifested as coughing, shortness of breath, wheezing, and chest tightness. Treatment algorithms can be separated into immediate acting agents to treat acute bronchospasm or medications and interventions to achieve long-term control of airway reactivity. Common pharmacologic approaches include bronchodilating medications, anti-cholinergic agents, and anti-inflammatory medications (corticosteroids and leukotriene modifiers).1 The following manuscript reviews the changing demographic pattern of asthma, current clinical diagnostic criteria, and the pathophysiologic processes responsible for airway reactivity. Perioperative interventions are reviewed, being divided into specifics of the preoperative anesthetic evaluation with a focus on identifying patients at high risk for airway reactivity and suggestions for intraoperative care to lessen the incidence of bronchospasm. Additionally, intraoperative interventions including the pharmacologic treatment of bronchospasm are provided as suggestions to guide clinical care. The manuscript is meant as a brief review and to provide suggestions for the perioperative care of patients with asthma and airway reactivity. It is not intended as a clinical guideline for all patients.
Demographic and Diagnostic Information
Throughout the world, it is currently estimated that there are more than 300 million people affected by asthma. The prevalence across all ages in the United States is estimated at 6.7%.2 It remains the most common chronic comorbid condition disease in children in the United States with an estimated incidence of 8.4%3,4 of the United States and asthma exacerbations are a leading cause of pediatric hospitalization.3,4 Over the past 4–5 decades, its impact in the pediatric population has increased. The prevalence of asthma has increased most significantly in the younger age group (patients 0–4 years of age) with the mean age at diagnosis decreasing from 4.7 years (children born in 1993) to 2.6 years (children born in 2000).4–6 While part of the increased incidence has been attributed to improved diagnostic techniques and heightened clinical awareness, various patient-related and environmental factors may be increasing the true incidence of the disease, including the incidence of obesity and its association with asthma.
Although the hallmark clinical sign of asthma is wheezing, various comorbid conditions other than asthma may be associated with wheezing in children including allergies, gastroesophageal reflux disease (GERD), infections (wheezing-associated respiratory illness or WARI), and obstructive sleep apnea.7,8 Childhood wheezing illnesses have two most common phenotypes including atopic asthma classically associated with inflammatory markers (eosinophils and mast cells) in the airway and episodic viral wheezing. At times, it remains challenging to determine whether the specific etiology of recurrent wheezing is either asthma or episodic wheezing accompanying acute viral upper respiratory tract infections, otherwise known as wheezing associated with respiratory illness (WARI).
WARI, without wheezing episodes during the interval between acute respiratory viral illnesses, is most commonly diagnosed in preschool-aged children. The incidence and severity of such episodes tends to decrease with age. Asthmatic wheezing usually occurs in school-aged children, is triggered by multiple factors like infection, cigarette smoke, allergens or exercise. It tends to persist even during the in-between interval episodes of exacerbations. Although both groups may be at risk for perioperative concerns, clinical differentiation may be helpful when deciding upon the need for chronic treatment regimens. Specific factors that may help differentiate the two conditions have been proposed by the Global Initiative for Asthma (GINA) guidelines. A diagnosis of asthma is generally supported by a cough that occurs without an associated viral respiratory infection; is triggered by exercise or emotional changes (laughing or crying); or occurs when the child is asleep (nocturnal cough).9
The presence of atopic dermatitis, allergic rhinitis, parental asthma, and wheezing apart from colds are used as major and minor criteria in the Asthma Predictive Index (API).10–12 To aid in the differential diagnosis of wheezing and the diagnosis of asthma, clinical guidelines recommend pulmonary function testing. Reversible airway obstruction is the hallmark of asthma. The spirometry is the main test to detect airway obstruction in children more than 5 years of age.12 Among asthmatic children, a FEV1 <60% is a risk factor for exacerbations and the severity of the decrease is associated with increasing asthma severity.13 The assessment of bronchodilator reversibility with spirometry not only helps in the clinical diagnosis of asthma, but also in monitoring treatment efficacy. The American Thoracic Society recommendations define a significant bronchodilator response (BDR) as an increase in FEV1 ≥12% and/or 200 mL.14 If bronchodilator reversibility is absent on forced spirometry, specific challenges or provocative tests such as exercise or aerosolized histamine in specialized lung function testing laboratories can be performed to assess bronchial hyper-responsiveness. Although bronchial provocation tests are not routinely performed in asthmatic children, the exercise test may be an important tool in assessing bronchial hyper reactivity indirectly.15 Peak expiratory flow monitoring can be used in children over 5 years of age to guide variability in airway obstruction. However, due to variations in peak expiratory flow values, the “personal best” is generally used in children to monitor therapy and guide changes in progression of asthma. Allergy testing and measuring serum IgE levels may help when features are atypical and simple treatments to relieve wheeze, breathlessness and cough are not working.
With the recognized increased incidence of asthma and its prevalence in a younger aged population, a greater number of children with asthma and chronic comorbid conditions that impact airway reactivity can be expected to present for perioperative care.1 Regardless of the surgical procedure, intraoperative bronchospasm remains one of the more commonly encountered, acute life-threatening adverse events. In addition to preoperative preparation and optimizing of patients, having a specific treatment algorithm in place may facilitate safe care. In the remainder of this review, the pathophysiology of airway reactivity and wheezing is presented and the preoperative preparation of the patient with airway reactivity is discussed. Additionally, the differential diagnosis of intraoperative wheezing is reviewed, risk factors for intraoperative bronchospasm discussed, and a treatment algorithm presented.
Pathophysiology of Wheezing
The key pathological features of asthma at the cellular and tissue level are bronchoconstriction, airway edema and inflammation, airway hyperreactivity, and airway remodeling with smooth muscle hypertrophy. Various triggers including allergens, viruses, cold, exercise, and various genetic factors such as HLA gene mutation or defects in bronchial airway epithelium function can result in activation of the antigen presenting dendritic cells. This leads to sensitization of T helper (TH)-memory cells with Th-1 mediated release of IFN-gamma, lymphotoxins, IL-2 and Th-2 mediated interleukin (IL-4, IL-5, IL-13) release. The Th-1 response leads to cell mediated immunity and neutrophilic inflammation. The Th-2 cascade amplifies IgE-mediated activation of mast cells, basophils and eosinophils. This shift of the Th-2 cytokine profile results in the eosinophilic inflammation characteristic of asthma.16 Eosinophils contain inflammatory enzymes, generate leukotrienes, and express a wide variety of pro-inflammatory cytokines. Th-2 cytokines cause widespread release of inflammatory mediators like histamine, prostaglandins, leukotrienes and enzymes. These factors increase the vascular permeability of the airway mucosa, lead to goblet cell hyperplasia, increase mucus secretion, and augment bronchial smooth muscle contraction resulting in airway inflammation and narrowing of the airways. Airway narrowing results in the classic wheezing noted in asthmatic patients as air passes through the narrowed small and medium airways, the pathognomonic feature of asthma. Acute and chronic inflammation increase bronchial reactivity and the susceptibility to bronchospasm.
Overall, the mechanisms influencing airway hyperresponsiveness include inflammation and dysfunctional neuroregulatory mechanisms. The inflammatory infiltrate in the airway epithelium and smooth muscle leads to airway remodeling with epithelial desquamation, subepithelial fibrosis, angiogenesis, mucus gland hyperplasia and hypersecretion, and smooth muscle hypertrophy. These pathologic changes result in the classic symptoms of asthma including recurrent wheezing, chest tightness, cough, and shortness of breath. These episodes are associated with spontaneous or therapeutic reversibility of airflow obstruction.
Preoperative Care
Intraoperative bronchospasm can be manifested by decreased airway exchange, wheezing, a prolonged expiratory phase or increased peak airway pressure during positive pressure ventilation. During spontaneous ventilation, increased work of breathing or air hunger may be noted. Profound reductions or absence of air flow may result in no air exchange and hence no audible wheezing. The clinical scenario in which bronchospasm occurs may vary significantly. Airway hyper-reactivity and bronchospasm are commonly seen in patients with pre-existing conditions including asthma, prematurity, acute respiratory infections (WARI), pulmonary edema, and acute lung injury. Alternatively, it may occur as an acute, isolated event related to sudden airway reactivity in a patient with no associated comorbid conditions.17,18 Bronchospasm may also be a component of other acute life-threatening conditions including aspiration or anaphylaxis. Airway sounds that mimic wheezing may occur with a mal-positioned endotracheal tube (mainstem intubation), mucus plugging, and obstruction of any component of the breathing circuit.
Care of the patient at risk for bronchospasm begins with a thorough preoperative examination with an evaluation of the previous history of airway reactivity including provocative factors. During this time, patient comorbid risk factors for perioperative bronchospasm are identified and treatment algorithms initiated to limit their impact on airway reactivity. Although proper preoperative preparation of patients may limit the need for cancellation of surgical procedures, acutely ill patients, such as those who present with worsening upper respiratory infections, fever, wheezing, stridor, rales, or purulent nasal discharge, may require cancellation or postponement of elective surgical procedures.2
Patients with a history of frequent prior asthma exacerbations, especially those requiring ICU admission, frequency of emergency visits, use of systemic corticosteroids, may be at higher risk for bronchospasm during intraoperative care and also post-operative major adverse outcomes.19 Specific anatomic abnormalities may increase the incidence of intraoperative airway and respiratory complications, including cleft lip or cleft palate.20 Patients may benefit from referral to a pediatric pulmonary specialist. Chronic medication regimens including the use of inhaled corticosteroids should be optimized. Additional interventions include avoiding second-hand tobacco smoke and ensuring that there are no acute infectious concerns. The preoperative administration of a short course of oral corticosteroids and an inhaled β-adrenergic agonist and anticholinergic agent on the day of surgery can decrease airway reactivity and lessen the incidence of perioperative bronchospasm (Box 1).21–25
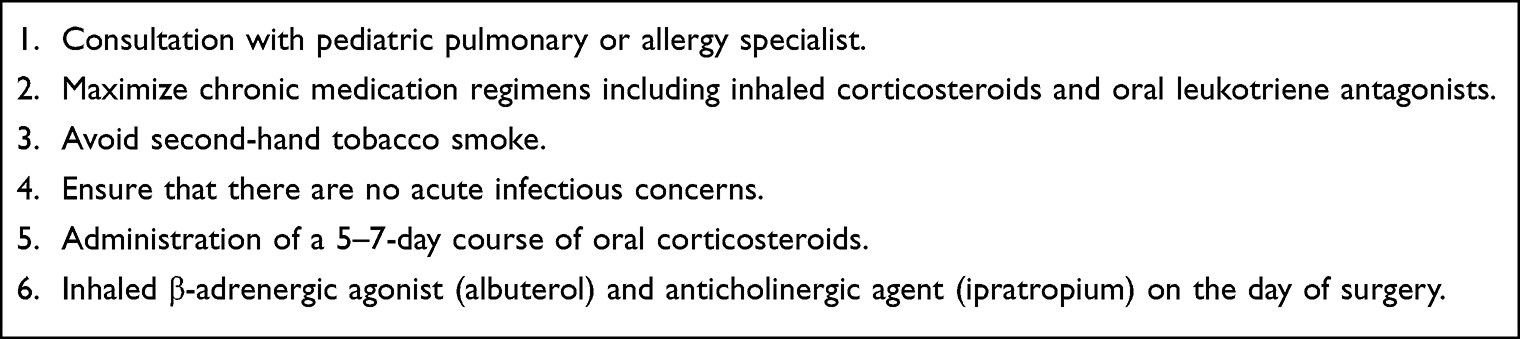 |
Box 1 Preoperative Interventions for the Patient with Asthma |
Tobacco smoke is a significant risk factor for perioperative bronchospasm as it increases respiratory complications and prolongs postoperative stays, even in patients without comorbid respiratory conditions such as asthma.22,25 Parental and patient smoking cessation at least two months prior to anesthesia has been advised. In the absence of exposure to second-hand smoke, postoperative respiratory complications were reported in 8 of 96 patients compared to 44 of 156 patients with second-hand smoke exposure.22 Laryngospasm after tracheal extubation was 10 times more likely in those exposed to second-hand some. These effects were noted were exposure to as few as 10 cigarettes/day. Children exposed to second-hand smoke also have a higher incidence of airway reactivity, acute and chronic respiratory disorders, and asthma exacerbations.26 These effects are magnified by active or recent upper respiratory tract infections. Other associated conditions known to increase the incidence of intraoperative bronchospasm include bronchitis, atopy, and viral upper respiratory tract infections.24,25
There also exists an association of obesity and asthma. It has also been observed that there is an increase in intraoperative bronchospasm in obese children even without a diagnosis of asthma. In a prospective study of 1465 pediatric patients, ranging in age from 2 to 16 years, there were increased rates of arterial oxygen desaturation, difficult mask ventilation, airway obstruction, and bronchospasm in obese children during perioperative care.16 Additionally, the relative risk (RR) of adverse respiratory events was higher among obese subjects than non-obese subjects. There was a significant association between obesity with both asthma and obstructive sleep apnea. The association with asthma was higher odds in the younger age group. Although the immunopathological mechanisms underlying obesity-associated asthma require further investigation, it is generally accepted that the imbalance in the quantity of adipose tissue favors a pro-inflammatory state both systemically and in the airways.
Upper respiratory infections increase airway reactivity for several weeks following an acute infection. Perioperative adverse respiratory events are 4–7 times more likely in children with active or recent URIs.27 Airway reactivity in response to provocative agents (cold air, histamine, or citric acid) is also increased in the setting of acute or recent URIs. Muscarinic receptors (M2) on vagal pre-synaptic nerve endings, which respond to acetylcholine release, are inhibited by viral neuraminidases. These pre-synaptic M2 receptors act as negative feedback receptors, decreasing ongoing acetylcholine release. The decreased affinity of the receptor for acetylcholine, blunts the negative feedback loop and results in increased acetylcholine release with facilitation of the cholinergic pathway and increased airway responsiveness. As universal cancellation of surgical procedures due to recent or ongoing URIs is not practical, decisions regarding the postponement of surgical procedures mandates considering the or balance of risk and benefit. The decision as to whether or not to proceed must consider the urgency of the procedure as well as the severity and course of the infection. For elective procedures, other considerations include the duration of the procedure, its complexity, and the requirements for airway management. For example, it may be reasonable to proceed with a brief otolaryngologic procedure that can be accomplished with a mask or an LMA, while more thought may be given to cancellation of surgery for congenital heart disease or upper abdominal procedures requiring endotracheal intubation. Children with severe symptoms including mucopurulent secretions, productive cough, fever >38°C, lethargy, or signs of pulmonary involvement should have elective surgical procedures postponed.
For procedures that are cancelled, the question arises as to the appropriate symptom-free period prior to elective surgery. This is especially true in younger children who may average 6–8 URIs a year. Hence, if one insists on a 6-week period following URIs prior to proceeding with elective surgery, scheduling may be impossible. As such, the recommendations for proceeding in the presence of milder URI symptoms have been modified. In general, procedures can generally proceed in afebrile and otherwise healthy appearing children without significant cough and no audible wheezing or rales in the setting of an uncomplicated URI with clear secretions.25,27 Furthermore, the time period after an acute infection does not generally need to be as long as 6 weeks.
In patients with asthma or in those with airway reactivity related to a recent URI, a preoperative course of oral corticosteroids is a useful adjunct to decrease perioperative complications. Although chronic corticosteroid therapy for patients with asthma has shifted to the preferential use of inhaled corticosteroids to limit the systemic effects, there are limited prospective clinical data comparing the efficacy of oral versus inhaled corticosteroids prior to a surgical procedure. However, as the preoperative regimen entails a 5–7-day course, the adverse effect profile is limited compared to chronic, long-term administration.28,29 In adult patients, various regimens have been shown to be effective, including both oral and intravenous administration.2,29,30 Intravenous administration can be considered the day of the surgery with one dose administered preoperatively and the other postoperatively. Recommendations for pediatric dosing include oral prednisone (1 mg/kg/day, maximum 60 mg) for 3–5 days prior to surgery, a two-day course of oral dexamethasone (0.6 mg/kg, maximum 16 mg once a day), or a single dose of oral methylprednisolone (1 mg/kg) 48 hours before surgery.24 Systemic corticosteroids decrease airway inflammation, blunt airway hyperreactivity, and enhance β2-adrenergic and M2 receptor function. Corticosteroids act increase adrenergic and cholinergic receptor number and function, acting synergistically with inhaled β2-adrenergic agonists and anticholinergic agents to treat and prevent bronchospasm.30,31
The preoperative administration of inhaled β2-adrenergic agonists (albuterol) 1–2 hours before surgery blunts airway reactivity, including the response to endotracheal intubation.2,17,18 These medications may be administered at home by the parent using the patient’s standard drug regimen with a metered dose inhaler (MDI) or administered after arrival to the hospital via a standard nebulizer. The addition of an inhaled anticholinergic to the β2-adrenergic agonists (albuterol) acts synergistically through an effect on airway muscarinic cholinergic receptors. Combined nebulized ipratropium bromide and albuterol results in greater bronchodilation than a β2-adrenergic agonist alone. The combination may be useful in treating bronchospasm or in treating those with a poor initial response to β2-adrenergic agonist alone. These two agents (ipratropium bromide and albuterol) are available combined in a commercially available solution (DuoNeb®) or can be administered from separate vials. Anti-cholinergic agents are recommended in patients with viral-induced airway reactivity as these effects are partially mediated through enhanced cholinergic transmission due to dysfunction of the pre-synaptic M2 receptor. In our practice, for patients who routinely use a β2-adrenergic agonist and/or anticholinergic agent, we ask parents to administer these the evening before and the day of surgery, frequently before travelling to the hospital for their surgical procedure. Alternatively, these can be administered preoperatively prior to transport to the operating room.
Intraoperative Care: Induction and Maintenance of Anesthesia
Choices regarding intraoperative care in patients with asthma or those at risk for perioperative respiratory adverse events (PRAEs) can be focused on the method of anesthetic induction (intravenous versus inhalational), choice of induction agent, choice of maintenance agent(s), and the airway device used (Box 2). In patients with two or more risk factors for PRAEs, intravenous induction with propofol may limit the incidence when compared to inhalational induction with sevoflurane in nitrous oxide.32 Propofol suppresses the laryngeal reflex and blunts the reflex bronchoconstriction that occurs following mechanical stimulation of the airway to a greater degree than the inhalational anesthetic agents. Propofol has been shown to be superior to thiopental, thiamylal or methohexital, in limiting airway reactivity and wheezing with intravenous induction.33 Respiratory resistance after endotracheal intubation was lower following the induction dose of intravenous propofol compared to thiopental or etomidate.34
 |
Box 2 Intraoperative Considerations for the Patient with Asthma |
Aside from the evidence-based medicine showing the efficacy of propofol, ketamine has remained the time-honored agent for the induction of anesthesia in patients with asthma. Following ketamine, bronchodilatation is achieved through the release of endogenous catecholamines. Ketamine has been shown to effectively prevent or treat bronchospasm.35,36 In animal models, propofol and ketamine also produce local bronchoprotective effects by diminishing vagally induced airway constriction.
The inhalational anesthetic agents act as bronchodilators of tracheal smooth muscle by a variety of mechanisms including direct and indirect actions. Volatile anesthetic agents relax airway smooth muscle through a reduction of intracellular free calcium with inhibition of protein kinase C, decreased calcium release from sarcoplasmic reticulum, and modulation of voltage-dependent calcium channels.37–39 Although these direct effects are equivalent regardless of the volatile anesthetic agent used, the direct irritant effects of desflurane may counteract its bronchodilatory properties, provoking airway and bronchial constriction.40,41 When considering the choice of agents for maintenance anesthesia, there is limited evidence-based medicine to definitively demonstrate improved outcomes when comparing the volatile agents with total intravenous anesthesia (TIVA) using propofol and an opioid such as remifentanil. However, some authorities have suggested advantages of TIVA with propofol over volatile agents including reduced airway reactivity, bronchodilatation, reduced laryngospasm and bronchospasm, improved ciliary function, improved pulmonary shunt fraction, preservation of hypoxic pulmonary vasoconstriction, and reduced coughing on emergence.42–46 These effects may translate into a decreased incidence of laryngospasm and bronchospasm during the postoperative period especially follow airway procedures.
The airway device and whether or not a neuromuscular blocking agent (NMBA) is used to facilitate endotracheal intubation may impact the incidence of bronchospasm. As clinically appropriate, an LMA or facemask is preferable over an ETT as a greater incidence of bronchospasm has been reported with the use of an ETT in patients with an ongoing or recent URI.47 Direct laryngoscopy stimulates oropharyngeal reflexes and may provoke bronchospasm directly or following placement of an ETT. During the intubation process, the administration of a NMBA may blunt these processes and decrease the incidence and severity of airway reflexes, wheezing, and bronchospasm during endotracheal intubation.48,49 In a study evaluating 566 adult patients undergoing emergent endotracheal intubation in the ICU, the administration of a NMBA was associated with a lower incidence of hypoxemia and procedure-related complications with significantly improved conditions for endotracheal intubation.50
Once the decision is made to use a NMBA, the choice of NMBA may also affect airway reactivity and the potential for bronchospasm. In general, given its effects on airway responsiveness and bronchospasm, NMBAs associated with histamine release (atracurium, mivacurium, and d-tubocurarine) should be avoided.51 Cholinergic fibers innervate the smooth musculature of the trachea and bronchi, modulating airway tone through the release of acetylcholine. Acetylcholine regulates airway tone through pre-synaptic (M2) and post-synaptic (M3) receptors. M2 receptors of the muscarinic system act as negative feedback receptors, decreasing further release of acetylcholine. M3 receptors on the smooth muscle cause bronchoconstriction. Although NMBAs specifically block nicotinic receptors (cholinergic) on skeletal muscle, they may have secondary effects on muscarinic (cholinergic) receptors as well. These include partial blockade (anti-cholinergic effects) of M2 receptors thereby augmenting the release of acetylcholine.
These effects, as well as facilitating of the action of acetylcholine on M3 receptors, have been identified as the mechanisms responsible for bronchospasm with the non-depolarizing NMBA, rapacuronium.52,53 Although rapacuronium was subsequently withdrawn from clinical care due to its potential to provoke bronchospasm, other NMBAs may modulate cholinergic transmission.54 Rocuronium has both M2 and M3 muscarinic receptor blocking effects in clinically used concentrations. As its effects at the M2 receptor exceed those at the M3 receptor, it may inhibit the negative feedback loop and potentiate cholinergic transmission. These effects may cause bronchoconstriction in clinical scenarios where there is enhanced vagal stimulation, such as tracheal intubation. Furthermore, just like rapacuronium, rocuronium has positive allosteric effects at the M3 muscarinic receptor, which may further enhance any bronchoconstriction. However, there is limited evidence-based medicine to suggest that rocuronium is contraindicated in patients with a history of asthma or airway reactivity.
Another issue to consider revolving around the use of neuromuscular blockade during intraoperative care is which reversal agent is optimal. Although the muscarinic effects can be partially blocked by the administration of an anticholinergic agent, neostigmine potentiates cholinergic transmission, increases airway reactivity, and increases respiratory and upper airway secretions.55 Given its different mechanism of agent and lack of cholinergic effects, reversal with sugammadex may be preferable in patients with airway reactivity.56 However, its use may be associated with a higher incidence of allergic reactions (see below).
Another issue that must be considered when bronchospasm occurs intraoperatively is the identification of a possible anaphylactic or anaphylactoid reaction. In such instances, bronchospasm may be one component of the systemic clinical manifestations of allergy. Neuromuscular blocking agents (NMBAs), latex containing products, radiologic contrast agents, and antibiotics have been identified as the agents most commonly responsible for perioperative hypersensitivity reactions.57 Rocuronium administration is associated with more frequent allergic reactions compared to other NMBAs, while the incidence of hypersensitivity to latex is decreasing as a result of its elimination from the perioperative environment and identification of at-risk patients.57–59 During allergic reactions, bronchospasm is generally one component of the clinical manifestations which may also include an erythematous rash frequently with urticaria and cardiovascular manifestations ranging from hypotension to cardiovascular collapse.60 Separation of these two clinical scenarios (primary bronchospasm from an allergic reaction) is necessary as treatment of the latter requires the immediate administration of epinephrine to increase the probability of an optimal outcome. Delayed diagnosis and the late administration of epinephrine may lead to a prolonged or biphasic clinical course, or even fatal outcome.60–62
Other pharmacologic agents may provide protection against reflex bronchoconstriction following endotracheal intubation including an anticholinergic agent or lidocaine. Although the use of inhaled anticholinergic agents (ipratropium) is not generally effective in providing acute and immediate relief of bronchospasm, there may be some benefit from the administration of an anticholinergic agent prior to endotracheal intubation. Given its lack of central nervous system effects, glycopyrrolate is frequently chosen over atropine. When administered prior to endotracheal intubation, it may provide protection against cholinergic-mediated bronchoconstriction.63 However, conflicting data were reported by Tait et al in a prospective trial of 130 children with upper respiratory tract infections presenting for elective surgery.63 Following randomization to glycopyrrolate (0.01 mg/kg) or placebo, there was no difference in the incidence of perioperative respiratory adverse events between the two groups. However, compared with the placebo group, children in the glycopyrrolate group had significantly shorter discharge times and less postoperative nausea and vomiting. The administration of aerosolized or intravenous lidocaine may also minimize reflex bronchoconstriction through neural blockade of vagal reflex pathways or direct effects on airway smooth musculature.64,65 Finally, a single intraoperative dose of the corticosteroid, dexamethasone, may provide protection against postoperative bronchospasm through its anti-inflammatory effects, especially in patients who have not received preoperative oral corticosteroids.66
Treatment of Intraoperative Bronchospasm
Of primary importance during intraoperative care of patients with asthma is to have a specific algorithm for recognizing and treating acute bronchospasm (Box 3). Treatment is directed at maintaining adequate oxygenation and ventilation while providing effective pharmacologic management to treat and reverse bronchospasm. Initial management includes the administration of 100%, manual ventilation, and cessation of any interventions including surgical stimulation that may be precipitating bronchospasm. This is followed by auscultation to ensure bilateral breath sounds are present with proper positioning of the ETT, ensuring appropriate positioning of the endotracheal tube, to identify ETT obstruction, secretions or pneumothorax. One should also rule out that the respiratory concern is not related to a mechanical problem such as ETT obstruction or kinking, mainstem intubation or ventilatory malfunction.67 As indicated, a suction catheter should be passed through the ETT and a chest radiograph obtained.
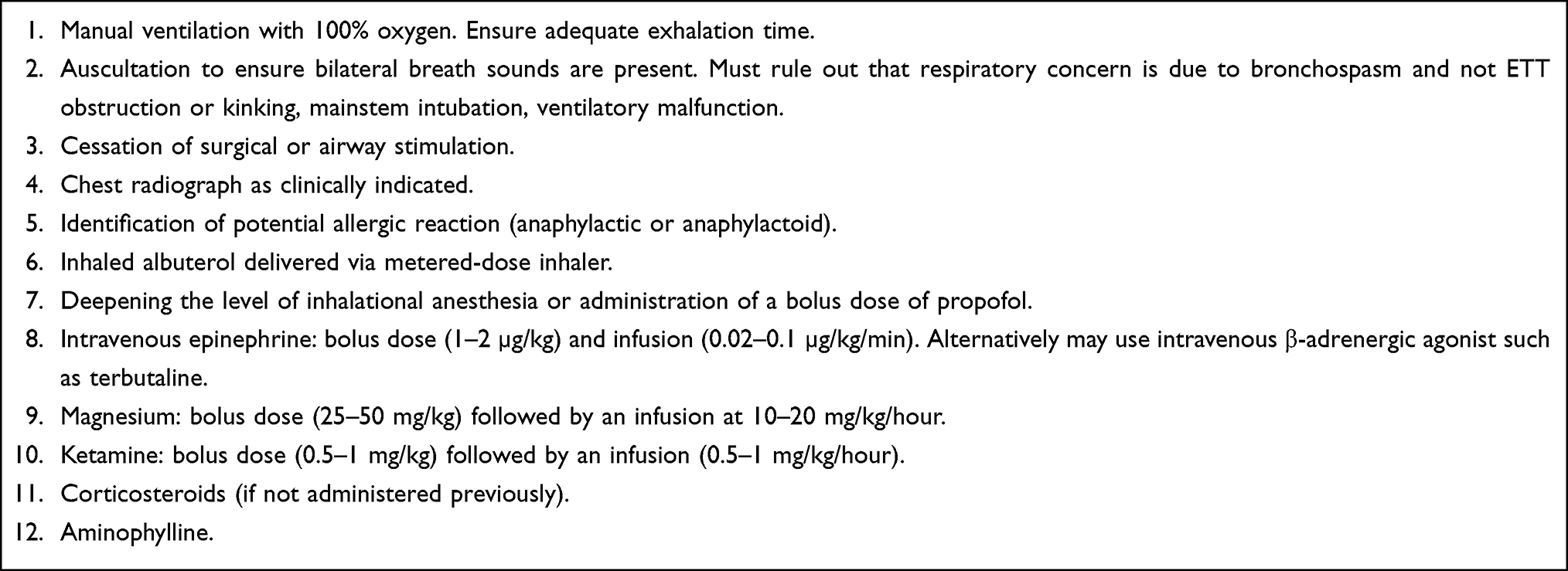 |
Box 3 Acute Intraoperative Treatment of Bronchospasm |
When bronchospasm is confirmed, the depth of anesthesia should be deepened with an intravenous anesthetic agent (propofol) or the administration of increased concentration of the volatile anesthetic agent, sevoflurane. Close monitoring of hemodynamic function is mandatory as the depth of anesthesia is increased and ventilator support augmented as hypotension may ensue due to increases in airway pressure. Attention is directed at ensuring adequate oxygenation and ventilation with the administration of 100% and manual ventilation. Ventilation should be directed at minimizing peak inflating pressure and allowing ample time for exhalation to prevent the development of auto-PEEP.68 This can be facilitated by using higher inspiratory flow rates and lower tidal volumes. Monitoring the end-tidal carbon dioxide (ETCO2) capnograph is helpful to evaluate response to therapy as the capnograph can be used as an index of expiratory airway flow. However, as bronchospasm worsens, the ETCO2 to PaCO2 gradient widens, making ETCO2 an unreliable indicator of PaCO2. As time permits, placement of an arterial cannula should be considered to allow for monitoring of arterial blood gases.
Pharmacologic therapy starts with the administration of a β-adrenergic agonist (albuterol) via a metered dose inhaler (MDI) with a spacer attached to the connection between the anesthesia circuit and the 15 mm adaptor of the ETT. Alternatively, the MDI device can be placed into a 60 mL syringe and the puffs administered into the port used for attachment of the ETCO2 monitoring tubing in the elbow of the anesthesia circuit. Due to deposition of the medication in the ETT, 8–10 puffs are recommended. Adverse effects of albuterol are generally rare in pediatric-aged patients and may include tachycardia, hypotension, or arrhythmias. Hypokalemia may occur due to intracellular shift related to β-adrenergic effects. Repeat dosing in 10 minutes should be considered for persistent bronchospasm, provided heart rate is within acceptable ranges.
If bronchospasm is severe, limiting gas exchange, and preventing the effective delivery of aerosolized albuterol, intravenous epinephrine (1–2 µg/kg) should be administered early in the course. Persistent bronchospasm may require further pharmacologic therapy including the administration of a bolus and a continuous intravenous infusion of magnesium, ketamine, or even epinephrine.69–71 Magnesium has seen significant clinical use in the treatment of status asthmaticus in the ICU setting. It results in bronchial smooth relaxation independently of the β2-receptor, by decreasing the pre-synaptic transmembrane movement of calcium and inhibiting acetylcholine release. Magnesium dosing includes a bolus dose (25–50 mg/kg) over 10–15 minutes followed by an infusion at 10–20 mg/kg/hour if a therapeutic response is noted with the bolus dose. Adverse effects include hypotension from vasodilatation of the vascular smooth musculature. Additionally, magnesium can result in skeletal muscle weakness and potentiation of neuromuscular blockade from the effects of magnesium at the neuromuscular junction. Hypotension can frequently be prevented by the slow administration of the bolus dose or the administration of an isotonic fluid bolus. When a continuous infusion of magnesium is required, serum levels should be monitored every 4–6 hours and the infusion adjusted accordingly. An additional therapeutic intervention for the treatment of bronchospasm is the administration of a ketamine bolus (1 mg/kg) followed by a continuous infusion. Ketamine stimulates the release of endogenous catecholamines and decreases vagally induced airway constriction, thereby preventing bronchospasm.
Aminophylline and theophylline have been used for decades in the treatment of acute exacerbations of asthma.72–74 Although still occasionally used to treat refractory status asthmaticus in the PICU setting, aminophylline has been moved to an alternative option in treatment algorithms following continuous inhaled β-adrenergic agonists and anticholinergic agents, corticosteroids, magnesium, and ketamine. Its use in the perioperative setting especially intraoperatively will generally be limited.
Emergence from Anesthesia and Postoperative Care
As the patient emerges from anesthesia, bronchospasm may recur or worsen. There remains limited evidence-based medicine to demonstrate whether the patient’s trachea is best extubated awake or deep (while still anaesthetized). Although deep tracheal extubation has been practiced and advocated for decades in various clinical scenarios,75 even following uneventful deep tracheal extubation, bronchospasm and adverse respiratory events can occur as the patient emerges. The keys to minimizing postoperative pulmonary complications are continuous patient monitoring so as to determine early clinical signs of bronchospasm or deterioration in respiratory status, prevention of emergence delirium and agitation, adequate pain control, and ongoing bronchodilator therapies. This process may be facilitated by the administration of dexmedetomidine (0.3–0.5 µg/kg) prior to the emergence process.76,77 In addition to its efficacy in preventing agitation and allowing for a smooth emergence from anesthesia, it may have other physiologic and therapeutic effects in preventing or reversing bronchospasm.78 Should bronchospasm and increased work of breathing during emergence fail to respond to effective bronchodilator therapy, non-invasive ventilation using BiPAP should be considered (Box 4).79,80
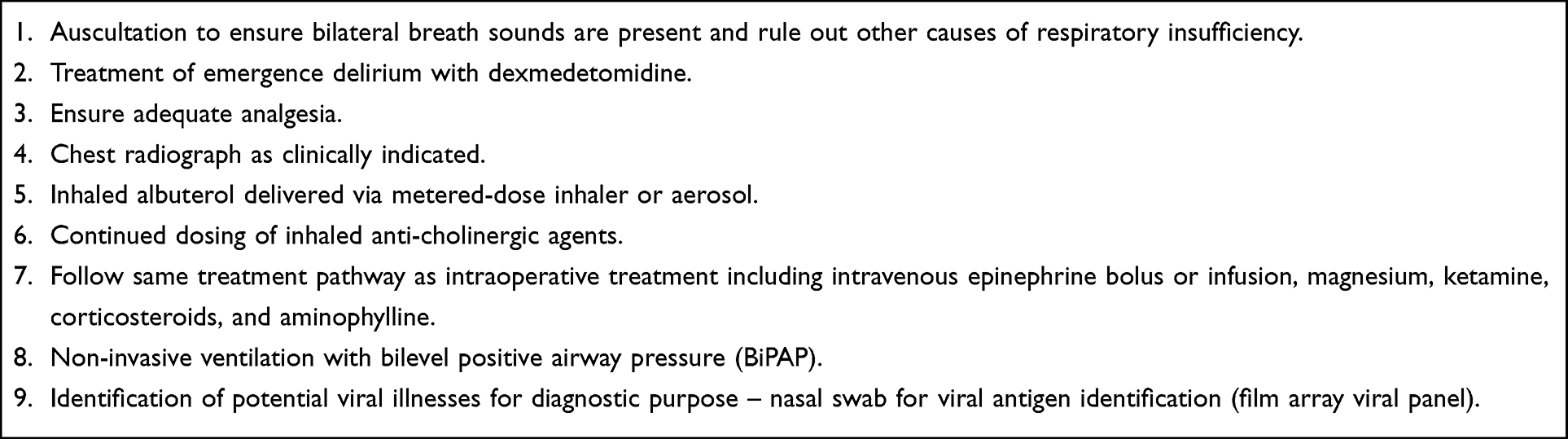 |
Box 4 Postoperative Treatment of Bronchospasm |
Summary
As the incidence and perhaps severity of asthma is increasing worldwide, there are an increased number of children presenting to the operating room with a history of airway hyperreactivity and asthma. Overall, with improvements in treatment modalities in the outpatient and inpatient setting, rates of morbidity and mortality continue to decrease. The chances of an adverse perioperative respiratory event can be decreased by an organized preoperative approach and appropriate therapeutic interventions to maximize bronchodilator and anti-inflammatory therapies. This manuscript, its tables, and references have been provided as an algorithm to be considered when caring for patients with asthma and reactive airway disease who present for perioperative care. The provided outline and tables are meant only to suggest options for clinical care and are not meant to be specific clinical guidelines. All clinical care should be individualized with each patient evaluated and considered on a case by case basis. Furthermore, availability of interventions and medications may vary from country to country and center to center further impacting the clinical care decision process.
Preoperative interventions should focus on maximizing treatment regimens, including inhaled therapies (corticosteroids, anticholinergic agents, and β-adrenergic agonists), an evaluation for potential acute upper respiratory infections, avoidance of second-hand tobacco smoke, and the administration of a short course of oral corticosteroids. When intraoperative bronchospasm occurs, a structured algorithm for investigation and treatment is recommended. These therapies may need to be continued or accelerated during emergence from anesthesia and throughout the perioperative course.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fanta CH. Asthma. N Engl J Med. 2009;360:1002–1014. doi:10.1056/NEJMra0804579
2. Woods BD, Sladen RN. Perioperative considerations for the patient with asthma and bronchospasm. Br J Anaesth. 2009;103(Suppl 1):i57–65. doi:10.1093/bja/aep271
3. Hoch HE, Houin PR, Stillwell PC. Asthma in children: a brief review for primary care providers. Pediatr Ann. 2019;48:e103–9. doi:10.3928/19382359-20190219-01
4. Akinbami LJ, Schoendorf KC. Trends in childhood asthma: prevalence, health care utilization, and mortality. Pediatrics. 2002;110:315–322. doi:10.1542/peds.110.2.315
5. Akinbami LJ, Simon AE, Rossen LM. Changing trends in asthma prevalence among children. Pediatrics. 2016;137:1–7. doi:10.1542/peds.2015-2354
6. Radhakrishnan DK, Dell SD, Guttmann A, et al. Trends in the age of diagnosis of childhood asthma. J Allergy Clin Immunol. 2014;134:1057–1062. doi:10.1016/j.jaci.2014.05.012
7. Martinati LC, Boner AL. Clinical diagnosis of wheezing in early childhood. Allergy. 1995;50:701–710. doi:10.1111/j.1398-9995.1995.tb01210.x
8. Balbani AP, Weber SA, Montovani JC. Update in obstructive sleep apnea syndrome in children. Rev Bras Otorrinolaringol. 2005;71:74–80. doi:10.1590/S0034-72992005000100013
9. Levy ML, Fletcher M, Price DB, et al. International Primary Care Respiratory Group (IPCRG) Guidelines: diagnosis of respiratory diseases in primary care. Prim Care Respir J. 2006;15:20–34. doi:10.1016/j.pcrj.2005.10.004
10. Castro-Rodríguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162(4 Pt 1):1403–1406. doi:10.1164/ajrccm.162.4.9912111
11. Castro-Rodriguez JA. The asthma predictive index: early diagnosis of asthma. Curr Opin Allergy Clin Immunol. 2011;11:157–161. doi:10.1097/ACI.0b013e3283464c4a
12. Gallucci M, Carbonara P, Pacilli AMG, Di Palmo E, Ricci G, Nava S. Use of symptoms scores, spirometry, and other pulmonary function testing for asthma monitoring. Front Pediatr. 2019;7:54. doi:10.3389/fped.2019.00054
13. Moeller A, Carlsen KH, Sly PD, et al. ERS task force monitoring asthma in children. Monitoring asthma in childhood: lung function, bronchial responsiveness and inflammation. Eur Respir Rev. 2015;24:204–215. doi:10.1183/16000617.00003914
14. Reddel HK, Taylor DR, Bateman ED, et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180:59–99. doi:10.1164/rccm.200801-060ST
15. Riiser A, Hovland V, Carlsen KH, Mowinckel P, Lødrup Carlsen KC. Does bronchial hyperresponsiveness in childhood predict active asthma in adolescence? Am J Respir Crit Care Med. 2011;186:493–500. doi:10.1164/rccm.201112-2235OC
16. Cohn L, Elias JA, Chupp GL. Asthma: mechanisms of disease persistence and progression. Annu. Rev Immunol. 2004;22:789–815. doi:10.1146/annurev.immunol.22.012703.104716
17. Westhorpe RN, Ludbrook GL, Helps SC. Crisis management during anaesthesia: bronchospasm. Qual Saf Health Care. 2005;14:e7. doi:10.1136/qshc.2002.004457
18. Dewachter P, Mouton-Faivre C, Emala CW, Beloucif S, Riou B. Case scenario: bronchospasm during anesthetic induction. Anesthesiology. 2011;114:1200–1210. doi:10.1097/ALN.0b013e3182172cd3
19. Lin CS, Chang CC, Yeh CC, Chung CL, Chen TL, Liao CC. Postoperative adverse outcomes in patients with asthma: a nationwide population-based cohort study. Medicine. 2016;95:e2548. doi:10.1097/MD.0000000000002548
20. Desalu I, Adeyemo W, Akintimoye M, Adepoju A. Airway and respiratory complications in children undergoing cleft lip and palate repair. Ghana Med J. 2010;44:16–20. doi:10.4314/gmj.v44i1.68851
21. Dones F, Foresta G, Russotto V. Update on perioperative management of the child with asthma. Pediatr Rep. 2012;4:e19. doi:10.4081/pr.2012.e19
22. Simsek E, Karaman Y, Gonullu M, Tekgul Z, Cakmak M. The effect of passive exposure to tobacco smoke on perioperative respiratory complications and the duration of recovery. Rev Bras Anestesiol. 2016;66:492–498. doi:10.1016/j.bjan.2015.03.003
23. Tait AR, Malviya S, Voepel-Lewis T, Munro HM, Seiwert M, Pandit UA. Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology. 2001;95:299–306. doi:10.1097/00000542-200108000-00008
24. Lauer R, Vadi M, Mason L. Anaesthetic management of the child with co-existing pulmonary disease. Br J Anaesth. 2012;109(Suppl 1):i47–i59. doi:10.1093/bja/aes392
25. Tait AR, Malviya S. Anesthesia for the child with an upper respiratory tract infection: still a dilemma? Anesth Analg. 2005;100:59–65. doi:10.1213/01.ANE.0000139653.53618.91
26. El-Metainy S, Ghoneim T, Aridae E, Abdel Wahab M. Incidence of perioperative adverse events in obese children undergoing elective general surgery. Br J Anaesth. 2011;106:359–363. doi:10.1093/bja/aeq368
27. Cohen MM, Cameron CB. Should you cancel the operation when a child has an upper respiratory tract infection? Anesth Analg. 1991;72:282–288. doi:10.1213/00000539-199103000-00002
28. Azhar N. Pre-operative optimisation of lung function. Indian J Anaesth. 2015;59:550–556. doi:10.4103/0019-5049.165858
29. Matsuse H, Shimoda T, Machida I, et al. Perioperative corticosteroids for intermittent and mild persistent asthma. Allergol Int. 2002;51:185–190. doi:10.1046/j.1440-1592.2002.00263.x
30. Silvanus MT, Groeben H, Peters J. Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology. 2004;100:1052–1057. doi:10.1097/00000542-200405000-00004
31. Groeben H. Strategies in the patient with compromised respiratory function. Best Pract Res Clin Anaesthesiol. 2004;18:579–594. doi:10.1016/j.bpa.2004.05.013
32. Ramgolam A, Hall GL, Zhang G, Hegarty M, von Ungern-Sternberg BS. Inhalational versus intravenous induction of anesthesia in children with a high risk of perioperative respiratory adverse events: a randomized controlled trial. Anesthesiology. 2018;128:1065–1074. doi:10.1097/ALN.0000000000002152
33. Pizov R, Brown RH, Weiss YS, et al. Wheezing during induction of general anesthesia in patients with and without asthma. A randomized, blinded trial. Anesthesiology. 1995;82:1111–1116. doi:10.1097/00000542-199505000-00004
34. Eames WO, Rooke GA, Wu RS, Bishop MJ. Comparison of the effects of etomidate, propofol, and thiopental on respiratory resistance after tracheal intubation. Anesthesiology. 1996;84:1307–1311. doi:10.1097/00000542-199606000-00005
35. Brown RH, Wagner EM. Mechanisms of bronchoprotection by anesthetic induction agents: propofol versus ketamine. Anesthesiology. 1999;90:822–828. doi:10.1097/00000542-199903000-00025
36. Baraka A, Harrison T, Kachachi T. Catecholamine levels after ketamine anesthesia in man. Anesth Analg. 1973;52:198–200. doi:10.1213/00000539-197303000-00012
37. Yamakage M, Namiki A. Cellular mechanisms of airway smooth muscle relaxant effects of anesthetic agents. J Anesth. 2003;17:251–258. doi:10.1007/s00540-003-0194-4
38. Stucke AG, Stuth EA, Tonkovic-Capin V, et al. Effects of sevoflurane on excitatory neurotransmission to medullary expiratory neurons and on phrenic nerve activity in a decerebrate dog model. Anesthesiology. 2001;95:485–491. doi:10.1097/00000542-200108000-00034
39. Rooke GA, Choi JH, Bishop MJ. The effect of isoflurane, halothane, sevoflurane, and thiopental/nitrous oxide on respiratory system resistance after tracheal intubation. Anesthesiology. 1997;86:1294–1319. doi:10.1097/00000542-199706000-00010
40. Goff MJ, Arain SR, Ficke DJ, Uhrich TD, Ebert TJ. Absence of bronchodilation during desflurane anesthesia: a comparison to sevoflurane and thiopental. Anesthesiology. 2000;93:404–408. doi:10.1097/00000542-200008000-00018
41. Klock PA Jr, Czeslick EG, Klafta JM, Ovassapian A, Moss J. The effect of sevoflurane and desflurane on upper airway reactivity. Anesthesiology. 2001;94:963–967. doi:10.1097/00000542-200106000-00008
42. Lauder GR. Total intravenous anesthesia will supercede inhalational anesthesia in pediatric anesthetic practice. Paediatr Anaesth. 2015;25:52–64. doi:10.1111/pan.12553
43. Royse CF, Liew DFL, Wright CE, et al. Persistent depression of contractility and vasodilation with propofol but not with sevoflurane or desflurane in rabbits. Anesthesiology. 2008;108:87–93. doi:10.1097/01.anes.0000296077.32685.26
44. Hohlrieder M, Tiefenthaler W, Klaus H, et al. Effect of total intravenous anaesthesia and balanced anaesthesia on the frequency of coughing during emergence from the anaesthesia. Br J Anaesth. 2007;99:587–591. doi:10.1093/bja/aem203
45. Oberer C, von Ungern-Sternberg BS, Frei FJ, et al. Respiratory reflex responses of the larynx differ between sevoflurane and propofol in pediatric patients. Anesthesiology. 2005;103:1142–1148. doi:10.1097/00000542-200512000-00007
46. Von Ungern-Sternberg BS, Boda K, Chambers NA, et al. Risk assessment for respiratory complications in paediatric anaesthesia: a prospective cohort study. Lancet. 2010;376:773–783. doi:10.1016/S0140-6736(10)61193-2
47. Tait AR, Pandit UA, Voepel-Lewis T, Munro HM, Malviya S. Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal intubation. Anesth Analg. 1998;86:706–711. doi:10.1213/00000539-199804000-00006
48. Lundstrøm LH, Duez CHV, Nørskov AK, et al. Effects of avoidance or use of neuromuscular blocking agents on outcomes in tracheal intubation: a Cochrane systematic review. Br J Anaesth. 2018;120:1381–1393. doi:10.1016/j.bja.2017.11.106
49. Brenner B, Corbridge T, Kazzi A. Intubation and mechanical ventilation of the asthmatic patient in respiratory failure. J Allergy Clin Immunol. 2009;124(2 Suppl):S19–S28. doi:10.1016/j.jaci.2009.05.008
50. Wilcox SR, Bittner EA, Elmer J, et al. Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012;40:1808–1813. doi:10.1097/CCM.0b013e31824e0e67
51. Basta SJ. Modulation of histamine release by neuromuscular-blocking drugs. Curr Opin Anesth. 1992;5:572–576. doi:10.1097/00001503-199208000-00021
52. Rajchert DM, Pasquariello CA, Watcha MF, Schreiner MS. Rapacuronium and the risk of bronchospasm in pediatric patients. Anesth Analg. 2002;94:488–493. doi:10.1097/00000539-200203000-00003
53. Jooste E, Klafter F, Hirshman CA, Emala CW. A mechanism for rapacuronium-induced bronchospasm: M2 muscarinic receptor antagonism. Anesthesiology. 2003;98:906–911. doi:10.1097/00000542-200304000-00017
54. Yang CI, Fine GF, Jooste EH, Mutich R, Walczak SA, Motoyama EK. The effect of cisatracurium and rocuronium on lung function in anesthetized children. Anesth Analg. 2013;117(6):1393–1400. doi:10.1213/ANE.0b013e3182a6d191
55. Hazizaj A, Hatija A. Bronchospasm caused by neostigmine. Eur J Anaesthesiol. 2006;23:85–86. doi:10.1017/S0265021505241820
56. Tobias JD. Current evidence for the use of sugammadex in children. Paediatr Anaesth. 2017;27:118–125. doi:10.1111/pan.13050
57. Hepner DL, Castells MC. Anaphylaxis during the perioperative period. Anesth Analg. 2003;97:1381–1395. doi:10.1213/01.ANE.0000082993.84883.7D
58. Laxenaire M, Mertes P. Anaphylaxis during anaesthesia. Results of a two-year survey in France. Br J Anaesth. 2001;87:549–558. doi:10.1093/bja/87.4.549
59. Wakimoto M, Miller R, Kim SS, et al. Perioperative anaphylaxis in children: a report from the wake-up safe collaborative. Paediatr Anaesth. 2021;31(2):205–212. doi:10.1111/pan.14063
60. Harper NJN, Cook TM, Garcez T, et al. Anaesthesia, surgery, and life-threatening allergic reactions: management and outcomes in the 6th National Audit Project (NAP6). Br J Anaesth. 2018;121:172–188. doi:10.1016/j.bja.2018.04.015
61. Harboe T, Guttormsen A, Irgens A, Dybendal T, Florvaag E. Anaphylaxis during anesthesia in Norway. Anesthesiology. 2005;102:897–903. doi:10.1097/00000542-200505000-00006
62. Gurrieri C, Weingarten TN, Martin DP, et al. Allergic reactions during anesthesia at a large United States referral center. Anesth Analg. 2011;113:1202–1212. doi:10.1213/ANE.0b013e31822d45ac
63. Tait AR, Burke C, Voepel-Lewis T, Chiravuri D, Wagner D, Malviya S. Glycopyrrolate does not reduce the incidence of perioperative adverse events in children with upper respiratory tract infections. Anesth Analg. 2007;104(2):265–270. doi:10.1213/01.ane.0000243333.96141.40
64. Groeben H, Peters J. Lidocaine exerts its effect on induced bronchospasm by mitigating reflexes, rather than by attenuation of smooth muscle contraction. Acta Anaesthesiol Scand. 2007;51:359–364. doi:10.1111/j.1399-6576.2006.01205.x
65. Chang HY, Togias A, Brown RH. The effects of systemic lidocaine on airway tone and pulmonary function in asthmatic subjects. Anesth Analg. 2007;104:1109–1115. doi:10.1213/01.ane.0000260638.57139.87
66. Patra P, Nayak D. Dexamethasone as prophylaxis! Is it effective in reducing postoperative extubation blues in paediatric age group? A retrospective review of 331 patients. Indian J Anaesth. 2018;2018:52305–52310.
67. D’Mello A, Grischkan J, Tobias JD. Intraoperative endotracheal tube kinking: clinical findings and early diagnosis. Pediatr Anesth Crit Care J. 2022;10:17–21.
68. Kao CC, Jain S, Guntupalli KK, Bandi V. Mechanical ventilation for asthma: a 10-year experience. J Asthma. 2008;45:552–556. doi:10.1080/02770900801999090
69. Alter HJ, Koepsell TD, Hilty WM. Intravenous magnesium as an adjuvant in acute bronchospasm: a meta-analysis. Ann Emerg Med. 2000;36:191–197. doi:10.1067/mem.2000.109170
70. Hemmingsen C, Nielsen PK, Odorico J. Ketamine in the treatment of bronchospasm during mechanical ventilation. Am J Emerg Med. 1994;12(4):417–420. doi:10.1016/0735-6757(94)90051-5
71. Marshall PS, Possick J, Chupp GL. Intensive care unit management of status asthmaticus. Clin Pulm Med. 2009;16:293–301. doi:10.1097/CPM.0b013e3181bdff38
72. Dalabih A, Harris ZL, Bondi SA, Arnold DH. Contemporary aminophylline use for status asthmaticus in pediatric ICUs. Chest. 2012;141:1122–1123. doi:10.1378/chest.11-2873
73. Dalabih AR, Bondi SA, Harris ZL, Saville BR, Wang W, Arnold DH. Aminophylline infusion for status asthmaticus in the pediatric critical care unit setting is independently associated with increased length of stay and time for symptom improvement. Pulm Pharmacol Ther. 2014;27:57–61. doi:10.1016/j.pupt.2013.03.001
74. Mitra A, Bassler D, Goodman K, Lasserson TJ, Ducharme FM. Intravenous aminophylline for acute severe asthma in children over two years receiving inhaled bronchodilators. Cochrane Database Syst Rev. 2005;2005:CD001276. doi:10.1002/14651858.CD001276.pub2
75. Veyckemans F. Tracheal extubation in children: planning, technique, and complications. Paediatr Anaesth. 2020;30:331–338. doi:10.1111/pan.13774
76. Shi M, Miao S, Gu T, Wang D, Zhang H, Liu J. Dexmedetomidine for the prevention of emergence delirium and postoperative behavioral changes in pediatric patients with sevoflurane anesthesia: a double-blind, randomized trial. Drug Des Devel Ther. 2019;13:897–905. doi:10.2147/DDDT.S196075
77. Shukry M, Clyde MC, Kalarickal PL, Ramadhyani U. Does dexmedetomidine prevent emergence delirium in children after sevoflurane-based general anesthesia? Paediatr Anaesth. 2005;15:1098–1104. doi:10.1111/j.1460-9592.2005.01660.x
78. Mikami M, Zhan Y, Kim B, et al. Dexmedetomidine’s inhibitory effects on acetylcholine release from cholinergic nerves in Guinea pig trachea: a mechanism that accounts for its clinical benefit during airway irritation. BMC Anesthesiol. 2017;17:52. doi:10.1186/s12871-017-0345-z
79. Beers SL, Abramo TJ, Bracken A, Wiebe RA. Bilevel positive airway pressure in the treatment of status asthmaticus in pediatrics. Am J Emerg Med. 2007;25:6–9. doi:10.1016/j.ajem.2006.07.001
80. Silva Pde S, Barreto SS. Non-invasive ventilation in status asthmaticus in children: levels of evidence. Rev Bras Ter Intensiva. 2015;27:390–396.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anaphylaxis in Chinese Children: Different Clinical Profile Between Children with and without a History of Asthma/Recurrent Wheezing
Jiang N, Xu W, Huang H, Hou X, Xiang L
Journal of Asthma and Allergy 2022, 15:1093-1104
Published Date: 18 August 2022
The Effects of a Healthy Diet on Asthma and Wheezing in Children and Adolescents: A Systematic Review and Meta-Analysis
Zhang J, He M, Yu Q, Xiao F, Zhang Y, Liang C
Journal of Asthma and Allergy 2023, 16:1007-1024
Published Date: 25 September 2023