Back to Journals » Journal of Pain Research » Volume 13
Perioperative Analgesic Modalities for Breast Cancer Surgeries: A Prospective Randomized Controlled Trial
Authors Elsabeeny WY ![]() , Shehab NN
, Shehab NN ![]() , Wadod MA
, Wadod MA ![]() , Elkady MA
, Elkady MA
Received 3 August 2020
Accepted for publication 22 October 2020
Published 12 November 2020 Volume 2020:13 Pages 2885—2894
DOI https://doi.org/10.2147/JPR.S274808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Walaa Y Elsabeeny, Nahla N Shehab, Mohamed A Wadod, Mostafa A Elkady
Department of Anesthesia and Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt
Correspondence: Walaa Y Elsabeeny
Department of Anesthesia and Pain Management, National Cancer Institute, Kasr Al Eini Street, Fom El Khalig, Cairo 11796, Egypt
Tel +20 1007798466
Email [email protected]
Purpose: Various analgesic modalities are adopted for perioperative analgesia in breast cancer surgeries. This study aimed to compare the efficacy of intravenous morphine versus serratus anterior plane block (SAPB) and erector spinae plane block (ESPB) in breast cancer surgeries.
Patients and Methods: Seventy-five breast cancer patients undergoing modified radical mastectomy from January 2020 to June 2020 were randomly allocated into 3 groups; the morphine group received morphine 0.1 mg/kg, the SAPB group received ultrasound-guided SAPB with 25 mL bupivacaine 0.25% and the ESPB group received ultrasound-guided ESPB with 25 mL bupivacaine 0.25%. A visual analogue scale (VAS) 0– 10 was used to evaluate pain postoperatively, where 0 denotes no pain and 10 worst pain. If any patient in the 3 studied groups reported breakthrough pain with VAS ≥ 4 then a bolus of 3 mg morphine was given.
Results: There was no difference in VAS scores between the 3 groups postoperatively. Morphine consumption was higher in the morphine group (9.19 ± 2.32 mg) than the SAPB group (4.00 ± 1.55 mg) and the ESPB group (4.20 ± 1.64 mg), respectively. First time to receive postoperative morphine was significantly longer for the ESPB and SAPB groups than the morphine group (20.40 ± 4.98 hours), (19.00 ± 5.9 hours), (5.00 ± 4.62 hours), respectively. Intraoperative hemodynamics and fentanyl consumption showed no difference between groups, whereas postoperative mean arterial blood pressure values at 2 and 4 hours were higher in the morphine group. Ramsay sedation score and postoperative nausea and vomiting values in the post anesthesia care unit were higher for the morphine group compared to the SAPB and ESPB groups. No complications related to the blocks were reported.
Conclusion: SAPB and ESPB can be used as an effective and safe alternative to opioids with fewer side effects in breast cancer patients undergoing modified radical mastectomy.
Trial Registration: This trial was prospectively registered at Clinical Trials.gov on 22 January 2020 with registration number NCT04248608 (https://register.clinicaltrials.gov/prs/app/action/SelectProtocol?sid=S0009JS5&selectaction=Edit&uid=U0004LIG&ts=7&cx=− 81xkwa).
Keywords: modified radical mastectomy, morphine, serratus plane block, erector spinae block
Background
Breast cancer is one of the most common types of cancer affecting women.1 The rate of detection increased after the introduction of mammography as a screening tool.2 Surgical resection is one of the main treatment approaches for the management of solid tumors,3 which involves tumor resection and in some cases lymph node resection from the axilla which can result in acute postoperative pain leading to chronic pain in around 50% of patients.4 Various analgesic modalities are used for proper perioperative pain control. Morphine has always been considered the gold standard analgesic; however, opioids have multiple side effects.5 Several ultrasound-guided loco-regional analgesic modalities have been introduced for perioperative pain management of breast surgeries.6 These include pectoral nerve I and pectoral nerve II blocks,7 paravertebral block (PVB)8 serratus plane block (SPB)9 and erector spinae plane block (ESPB).6 SPB was introduced as a safe alternative to PVB to provide analgesia of the anterolateral chest wall, through blocking the thoracic intercostal nerves' lateral cutaneous branches (T2–T12).9 Recently, ESPB has been introduced as another loco-regional analgesic technique that can be used for perioperative analgesia in surgeries involving the anterior, lateral and posterior chest wall. It has a promising role in perioperative analgesia of breast cancer surgeries,10 as it achieves analgesia through blocking thoracic spinal nerves' dorsal and ventral rami.11
This study was designed to evaluate different analgesic modalities for breast cancer surgery regarding safety and efficacy, comparing intravenous morphine to serratus anterior plane block (SAPB) and erector spinae plane block (ESPB).
Patients and Methods
Following approval of the institutional review board of the National Cancer Institute, Cairo University IRB (201,920,002.2P), this parallel double-blinded (patient and postoperative outcome assessor) randomized controlled study was done in the period from January 2020 to June 2020. A written informed consent was taken from all patients enrolled in the study. The study was prospectively registered at clinicaltrials.gov (NCT 04248608). This study was obliged to the standards of the Declaration of Helsinki. Data generated and analyzed are available upon reasonable request by contacting the corresponding author.
Adult female patients aged from 18 to 65 years with an American Society of Anesthesiologists (ASA) I, II with breast cancer scheduled for modified radical mastectomy (MRM) were included consecutively. Exclusion criteria included patient refusal, local infection at site of injection, coagulation defects, thrombocytopenia, allergy to any of the used drugs, impaired hepatic or renal function and patients with any chronic pain syndrome receiving chronic pain medications. Patients meeting the eligibility criteria were recruited from the preoperative anesthesia assessment clinic by the anesthesia resident. A computer system-generated randomization was used and patients were randomly allocated by the anesthesia resident using the closed-envelope technique into one of three study groups to receive either intravenous (IV) morphine sulfate 0.1 mg/kg, SAPB or ESPB. All patients were made familiar with the Visual Analogue scale (VAS) used, with 0 meaning no pain and 10 being the worst experienced pain.
Upon arrival to the holding area patients were pre-medicated with midazolam (2 mg IV) and metoclopramide 0.1 mg/kg after fixation of a 20 G cannula. Before induction of anesthesia, pulse oximetry, electrocardiogram (ECG), and non-invasive automated blood pressure monitors were connected to the patient. Induction of anesthesia was done by propofol 2 mg/kg, fentanyl 2 µg/kg and rocuronium 0.6 mg/kg followed by endotracheal intubation and controlled mechanical ventilation with 50% FiO2, then anesthesia was maintained by sevoflurane and rocuronium. All patients received 500 mL lactated Ringer’s solution infusion.
Morphine group (control group): Patients received intravenous morphine sulphate 0.1 mg/kg.
SAPB group (experimental group 1): After induction of anesthesia and before surgical incision patients were positioned in the lateral position with the operating side up and the ipsilateral arm abducted 90°. After sterilization and draping, the fifth rib in the mid-axillary line was identified using the SonoSite M-Turbo ultrasound machine (FUGIFILM Sonosite, Inc., Bothel, WA 98021, USA) and ultrasound linear probe (6–13 MHz) then the probe was directed in a horizontal manner. The serratus anterior, latissimus dorsi, and the intercostal muscles were identified in the fourth and fifth intercostal levels, an 18-gauge Tuohy needle was advanced using an in-plane technique with 45° angle in the craniocaudal direction towards the fifth rib underneath the serratus anterior muscle. Confirmation of correct needle position was done by injecting 1–2 mL of normal saline. After negative aspiration of blood, a bolus dose of 25 mL bupivacaine 0.25% was administered into the fascial plane under the serratus muscle with continuous ultrasound guidance where linear separation of the plane was visualized (Figure 1).
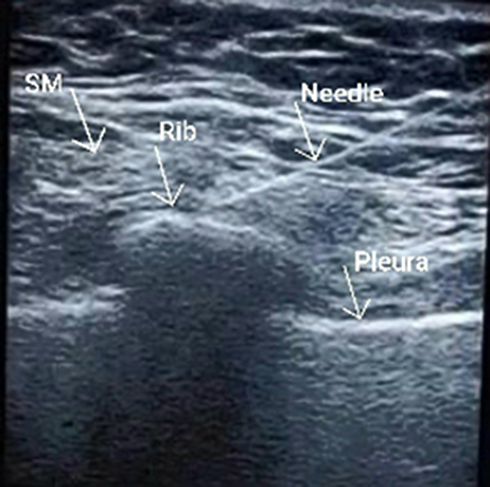 |
Figure 1 Serratus anterior plane. |
ESPB group (experimental group 2): The block was performed after induction of anesthesia. Patients were positioned in the lateral position and slightly leaning forward with the side of the operation facing up. After sterilization and draping, the fifth vertebral spinous process was identified using the SonoSite M-Turbo ultrasound machine with ultrasound curved probe (2–5 MHz) placed in a longitudinal parasagittal manner 3 cm lateral to the T5 spinous process to identify trapezius, rhomboid major, and erector spinae muscles superficial to the hyperechoic transverse process shadow. Then an 18-gauge epidural needle was introduced in a craniocaudal direction until it contacted the transverse process and the needle tip visualized in the plane deep to the erector spinae muscle. The needle tip position was confirmed by visualizing linear spread of 1–2 mL normal saline between the erector spinae muscle and the transverse process. After negative aspiration, an initial bolus dose of 25 mL of 0.25% bupivacaine was injected (Figure 2).
 |
Figure 2 Erector spinae plane. |
Starting from induction of anesthesia, heart rate (HR), arterial oxygen saturation (SpO2) and mean arterial blood pressure (MAP) were continuously monitored and recorded every 15 minutes. In order to ensure adequate analgesia throughout the operation, all patients were closely observed and upon appearance of signs of inadequate analgesia in the form of an increase in HR or MAP 20% above the baseline, fentanyl rescue doses of 0.5 µg/kg were supplemented and recorded. At the end of surgery, patients were transferred to the post anesthesia care unit (PACU) and then to the ward. VAS scores, HR and MAP were assessed and recorded at 0, 2, 4, 6, 12, 24 hours postoperatively. All patients received standard postoperative pain control with IV paracetamol, 1 g every 8 hours. If any patient reported pain at any time other than the scheduled time for VAS assessment, VAS score was assessed, patients with a score <4 were then given a nonsteroidal anti-inflammatory drug (NSAID) in the form of 30 mg IV ketorolac, whereas patients with a score of ≥4 were given IV morphine 3 mg incremental doses with a maximum dose of 0.1 mg/kg (Figure 3). The first time to receive postoperative morphine analgesic and total dose of morphine in the first 24 hours was recorded for each group. Our primary outcome measures were postoperative VAS score, total postoperative morphine consumption and first time to receive morphine; secondary outcome measures included intraoperative and postoperative hemodynamics.
 |
Figure 3 Postoperative analgesic protocol. IV, intravenous; VAS, visual analogue score. |
Statistical Methods and Sample Size Calculation
Sample size was calculated based on the previous paper by Gaballah and colleagues.12 The difference in VAS score between at least two groups was 0.4 ± 0.46. Using power 80% and 5% significance level, 22 patients were required in each group. This number was increased to 25 per group to adjust for nonparametric usage. PS: Power and Sample Size Calculation Software Version 3.1.2 (Vanderbilt University, Nashville, Tennessee, USA) was used to calculate sample size. Data were encrypted and entered using Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA). Interpretation of data was done using IBM SPSS advanced statistics (Statistical Package for Social Sciences), version 24 (SPSS Inc., Chicago, IL). Numerical data were described in the form of mean and standard deviation or median and range. Data were explored for normality using Kolmogorov–Smirnov and Shapiro–Wilk tests. Comparisons between three groups for normally distributed numeric variables were done using the ANOVA (analysis of variance), while comparisons between the three groups for nonnormally distributed numeric variables were done by Kruskal–Wallis test. Categorical data were described in the form of numbers and percentages and comparisons were done by chi square test or fisher exact test as appropriate. All tests used were two-tailed. A p-value less than or equal to 0.05 was considered statistically significant.
Results
One hundred and five female patients were consecutively enrolled in the study from January 2020 to June 2020. Eleven patients refused to participate in the study, 14 patients did not meet the inclusion criteria and data from five patients were missing (Figure 4).
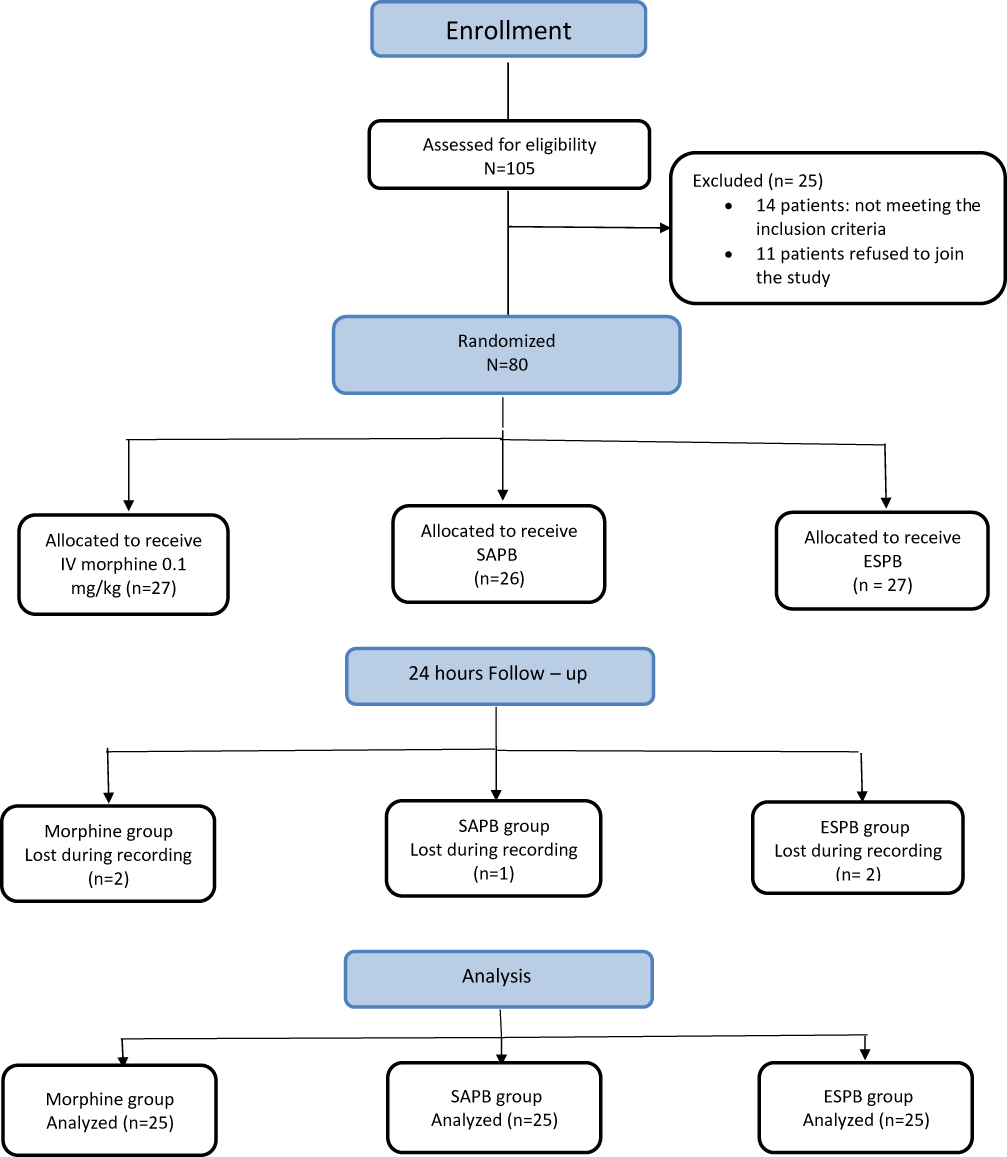 |
Figure 4 Consort flow diagram. IV, intravenous; SAPB, serratus anterior plane block; ESPB, erector spinae plane block. |
The three groups were comparable in their demographic data and clinical characteristics (Table 1). All patients underwent unilateral MRM with no immediate reconstruction. Duration of surgery was longer for the SAPB and ESPB groups compared to the morphine group, p value = 0.005 (Table 1). The difference in duration of surgery was secondary to the block procedure time, which was found to be significantly higher in the ESPB group than in the SAPB group, p value < 0.001 (Table 1).
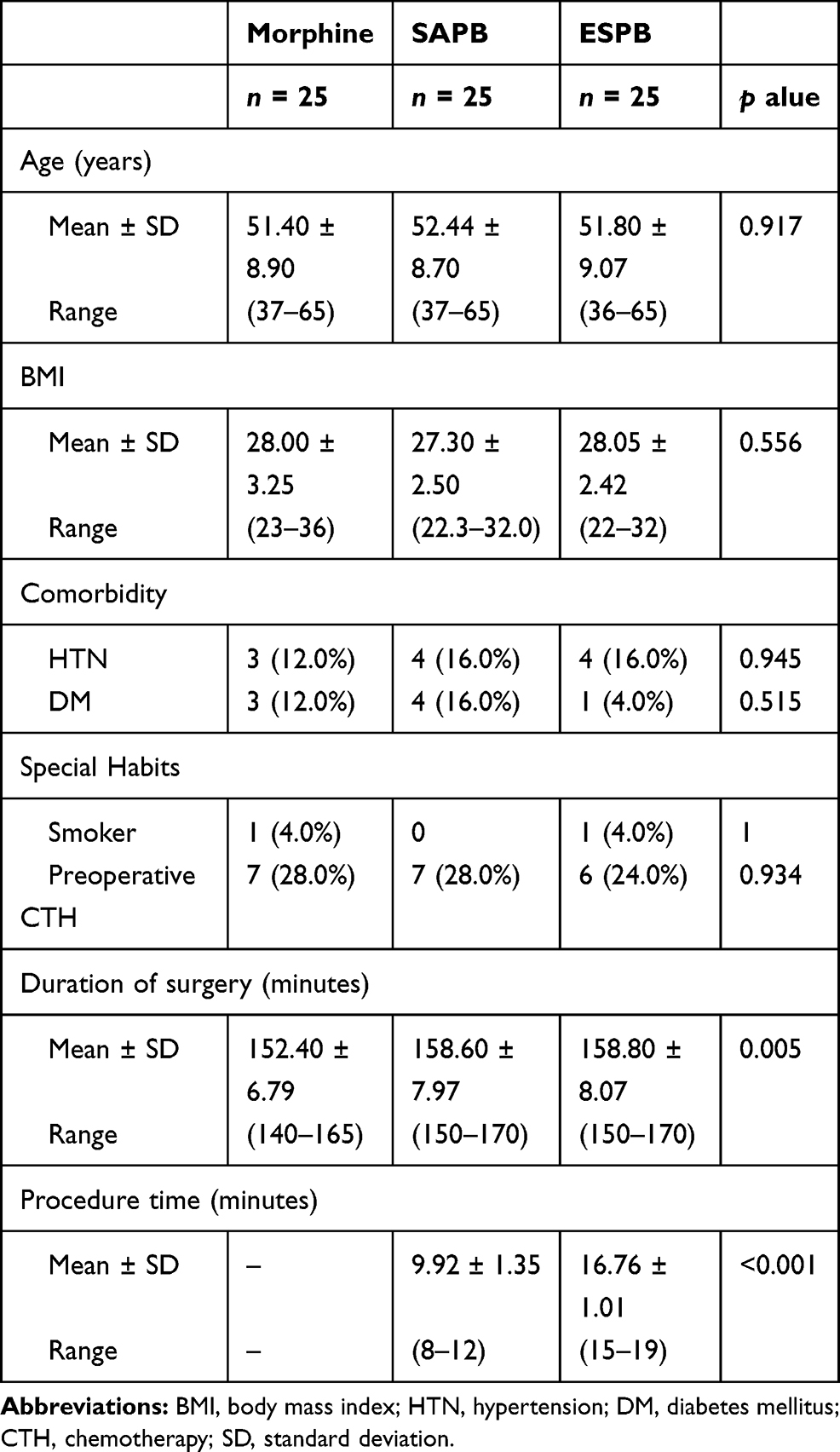 |
Table 1 Demographic Data, Clinical Characteristics, Duration of Surgery and Procedure Duration |
The three groups were comparable for their preoperative and intraoperative data with no statistically significant difference in HR values or MAP values, p value > 0.05 (Figures 5 and 6). There was no statistically significant difference in intraoperative fentanyl consumption, p value 0.436 (Table 2).
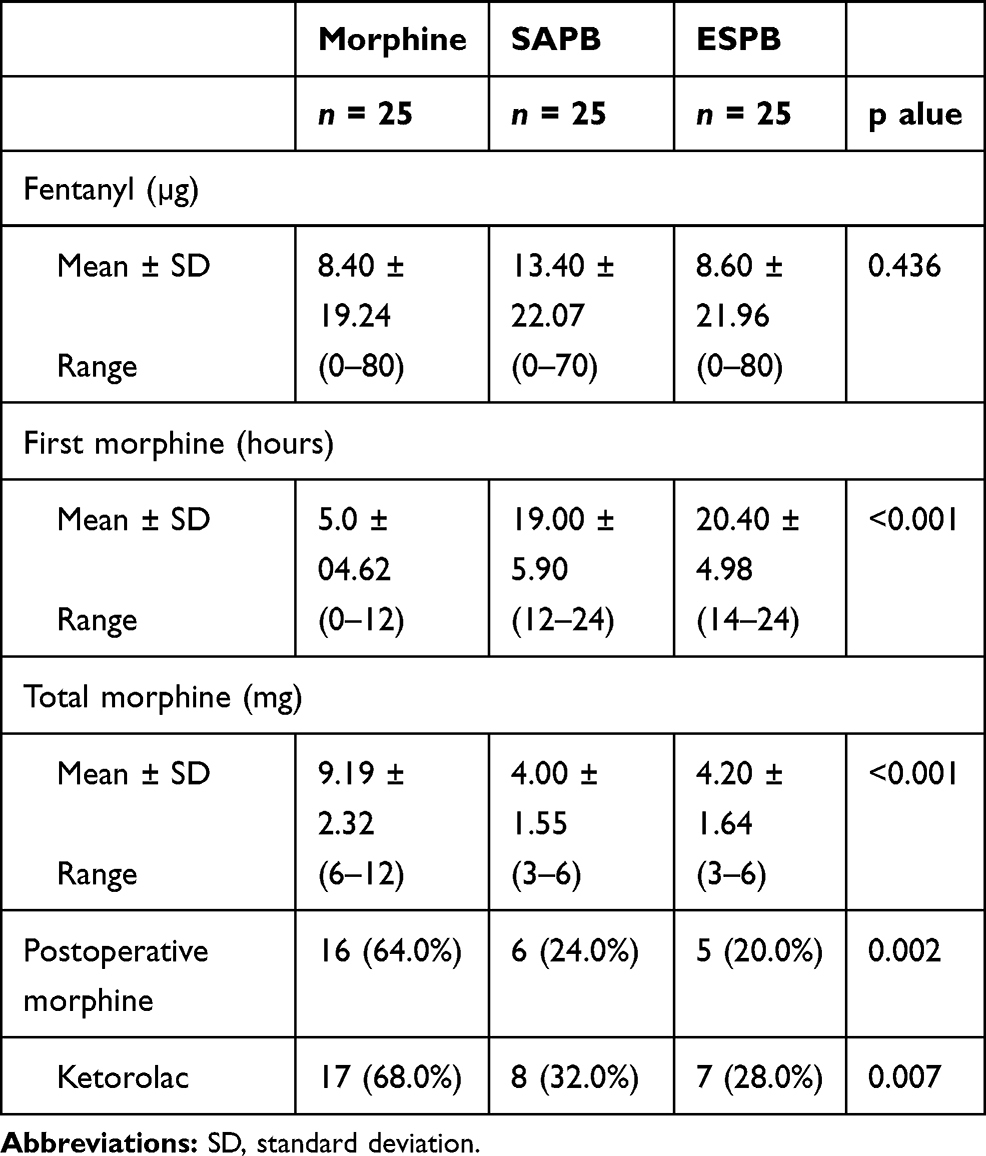 |
Table 2 Intraoperative Fentanyl Consumption, First Time to Receive Postoperative Morphine and Total Postoperative Morphine Consumption, Patients Who Received Morphine or Ketorolac in the First 24 Hours Postoperatively |
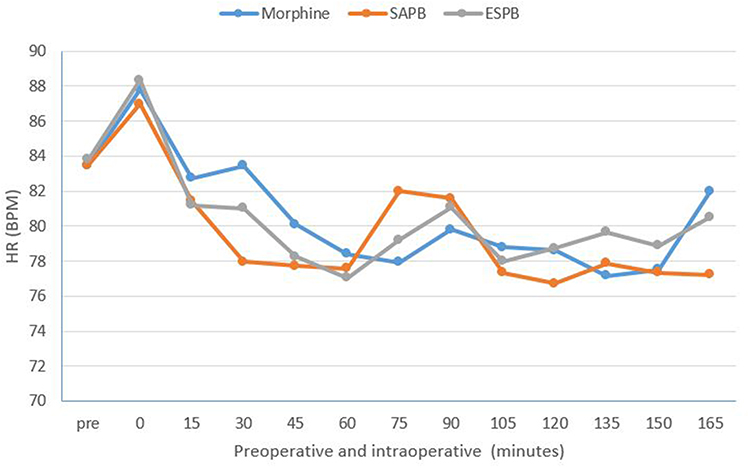 |
Figure 5 Preoperative and intraoperative heart rate. HR, heart rate; BPM, beats per minute. |
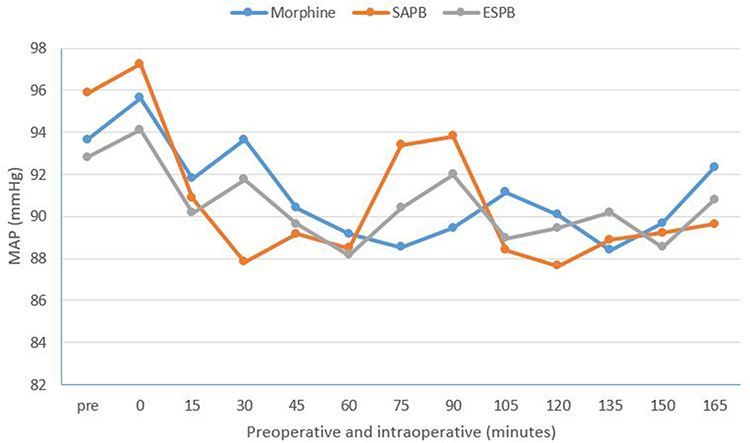 |
Figure 6 Preoperative and intraoperative mean arterial blood pressure (MAP). |
In the postoperative period the groups showed no statistically significant difference in their HR values and MAP values except MAP values at 2 and 4 hours, where the morphine group showed higher values compared to the SAPB and ESPB groups (p value 0.002 and 0.005), respectively (Figures 7 and 8).
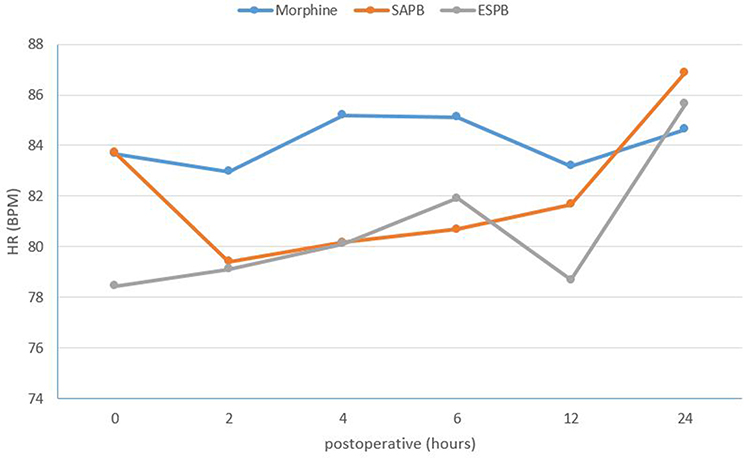 |
Figure 7 Postoperative heart rate. HR, heart rate; BPM, beats per minute; SAPB, serratus anterior plane block; ESPB, erector spinae plane block. |
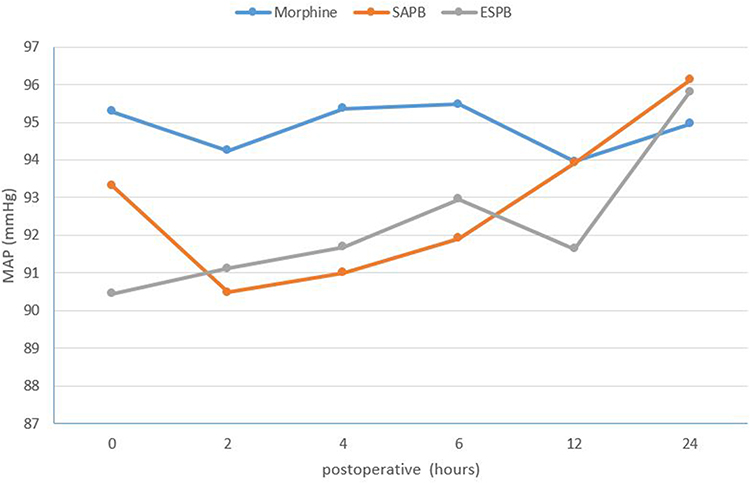 |
Figure 8 Postoperative mean arterial blood pressure (MAP). SAPB, serratus anterior plane block; ESPB, erector spinae plane block. |
There was no difference between the three groups in their VAS scores over the first 24 hours postoperatively (Figure 9). On the other hand, there was a significantly higher number of patients in the morphine group (64%) who required morphine analgesia compared to 24% in the SAPB group and 20% in the ESPB group (Table 2). The morphine group showed statistically significant higher values for total morphine consumption (9.19 ± 2.32 mg) as compared to the SAPB group (4.00 ± 1.55 mg) and the ESPB group (4.20 ± 1.64 mg), respectively, with p value < 0.001 (Table 2). First time to receive postoperative morphine was significantly longer for the ESPB and SAPB groups than the morphine group: 20.40 ± 4.98 hours, 19.00 ± 5.9 hours and 5.00 ± 4.62 hours, respectively, with p value < 0.001 (Table 2).
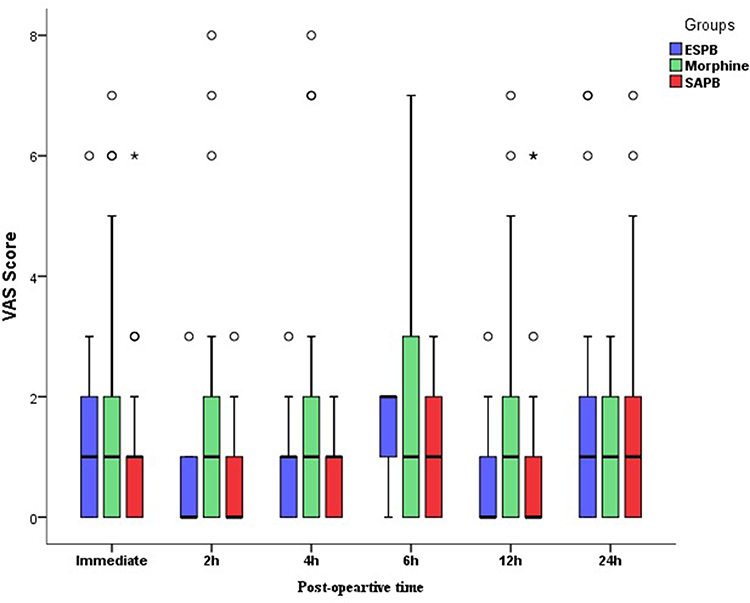 |
Figure 9 Postoperative visual analogue scores (VAS). SAPB, serratus anterior plane block; ESPB, erector spinae plane block. |
Sixty-eight percent of patients in the morphine group required rescue ketorolac analgesia versus 32% in the SAPB group and 28% in the ESPB group, p value 0.007 (Table 2).
Ramsay Sedation Score (RSS) at 0 and 2 hours and postoperative nausea and vomiting (PONV) values were higher in the PACU for the morphine group compared to the SAPB and ESPB groups, p values 0.006, < 0.001 and 0.014, respectively (Table 3). There were no reported cases of pneumothorax, injection site bruises or hematoma in both SAPB and ESPB groups.
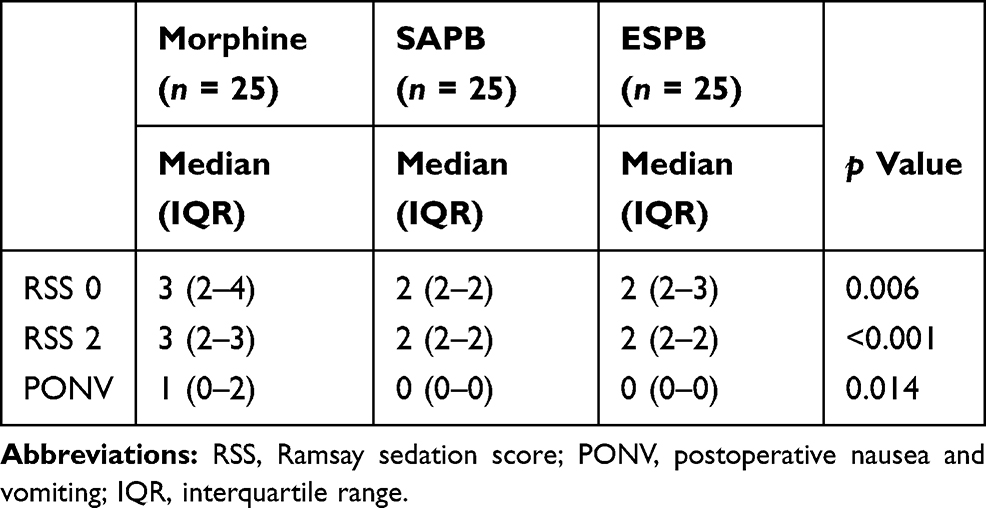 |
Table 3 Ramsay Sedation Scores at 0 and 2 Hours and PONV Score for the Three Studied Groups |
Discussion
The aim of this study was to evaluate the efficacy of ultrasound-guided SAPB and ESPB versus IV morphine analgesia in perioperative pain control of breast cancer patients undergoing modified radical mastectomy. Optimal pain control following breast surgery is essential, not only to eliminate acute pain but also to prevent post-mastectomy chronic pain syndrome.13 Advances in ultrasound-guided blocks along with the introduction of new regional analgesic techniques increased the safety and efficacy of analgesic modalities used in perioperative analgesia for thoracic wall surgeries.14,15 We reported that both SAPB and ESPB can be used as an efficient alternative to IV opioid analgesia with better analgesic profile, less postoperative opioid consumption, prolonged time to receive first dose analgesia and fewer side effects. On the other hand, we documented a longer procedural time for ESBP than for SAPB; we believe that this was secondary to the deeper targeted plane of ESPB. However, both blocks can be considered simple and can be performed safely under ultrasound guidance.
SAPB is a simple block to perform that provides adequate analgesia to the anterolateral chest wall. The plane is superficial, easily identified and relatively safe as injection is not in close proximity to vascular structures.9 Our results demonstrating the efficacy of SAPB are in agreement with Mazzinari and colleagues, who reported a superior analgesic profile of SAPB with lower opioid consumption and longer time to receive first dose analgesia over conventional analgesia in breast cancer patients undergoing mastectomies.16 In a case series of 11 patients undergoing mastectomies with axillary lymph node dissection and breast reconstruction with flap, Khemaka and colleagues reported that SAPB is an effective analgesic technique that improves perioperative pain and reduces postoperative opioid consumption.15 Similarly, Rahimzadeh and colleagues studied the effect of SAPB on postoperative mastectomy pain, where they found that the first time to receive rescue analgesia was longer in SAPB with lower opioid consumption and reduced pain scores when compared to conventional analgesic technique.17
The effect of ESPB is obtained through blocking the sensory supply to both the anterolateral and posterior chest wall. It provides both visceral and somatic analgesia through the spread of local anesthetic to the paravertebral space.18 Our results came in accordance with several studies investigating the role of ESPB in different types of breast surgeries. They documented its perioperative analgesic efficacy and its role in reducing postoperative morphine consumption.19–21 Moreover, a systematic review was done by Elhawary and colleagues to investigate the role of ESPB in breast surgeries. They concluded that it is a simple technique which can be easily performed under ultrasound guidance, with a valuable role in controlling postoperative pain and reducing opioid consumption.10 Recently, Wang and colleagues compared SAPB and ESPB to general anesthesia in patients undergoing radical mastectomy. Both SAPB and ESPB groups showed lower intraoperative propofol and remifentanil consumption along with lower postoperative VAS scores and sufentanil requirements when compared to the general anesthesia group.22 Altlparmak and colleagues studied the efficacy of different concentrations of bupivacaine in ESPB for patients undergoing modified radical mastectomy. They reported that ESPB using both bupivacaine 0.25% and 0.375% were effective in providing postoperative analgesia with reduced tramadol consumption in the higher concentration group.23
The use of ketorolac when the VAS score was <4 contributed to the reduction of opioids used in the postoperative period. Ketorolac is an injectable NSAID with analgesic properties, where NSAIDs were found to be useful in reducing opioid requirement thus reducing opioid side effects.24 However, ketorolac should be avoided in some conditions, such as in patients with ongoing or significant bleeding, coagulation disorders, platelet dysfunction, renal or hepatic impairment and in some asthmatic patients.25,26
Regarding RSS and PONV in the PACU, we reported higher values for the morphine group compared to the SAPB and ESPB groups, which may be explained as side effects of morphine administration.
Conclusion
Erector spinae plane block and serratus anterior plane bock can be used as a safe, effective perioperative analgesic modality with opioid-sparing effect. Both can be used as an effective alternative to morphine for perioperative pain control for breast cancer surgeries.
Abbreviations
ASA, American Society of Anesthesiology; ECG, electrocardiogram; ESP, erector spinae plane; ESPB, erector spinae plane block; HR, heart rate; IV, intravenous; MAP, mean arterial blood pressure; MRM, modified radical mastectomy; NSAID, nonsteroidal anti-inflammatory drug; PACU, post anesthesia care unit; PONV, postoperative nausea and vomiting; PVB, paravertebral block; RSS, Ramsay Sedation Score; SAPB, serratus anterior plane block; SPB, serratus plane block; VAS, visual analogue score.
Disclosure
The authors report no conflicts of interest in this work.
References
1. DeSantis CE, Bray F, Ferlay J, Lortet-Tieulent J, Anderson BO, Jemal A. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2015;24(10):1495–1506. doi:10.1158/1055-9965.EPI-15-0535
2. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(8):1194–1220. doi:10.1093/annonc/mdz173
3. Cho JS, Lee MH, Kim S
4. Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 2011;12(7):725–746. doi:10.1016/j.jpain.2010.12.005
5. Abraham AA. Gold standards and anaesthesia. Indian J Anaesth. 2013;57(2):207–209. doi:10.4103/0019-5049.111876
6. Singh S, Kumar G, Akhileshwar A. Ultrasound-guided erector spinae plane block for postoperative analgesia in modified radical mastectomy: a randomised control study. Indian J Anaesth. 2019;63(3):200–204. doi:10.4103/ija.IJA-758-18
7. Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of pecs II (modified pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59(9):470–475. doi:10.1016/j.redar.2012.07.003
8. Kairaluoma PM, Bachmann MS, Korpinen AK, Rosenberg PH, Pere PJ. Single-injection paravertebral block before general anesthesia enhances analgesia after breast cancer surgery with and without associated lymph node biopsy. Anesth Analg. 2004;99(6):1837–1843. doi:10.1213/01.ANE.0000136775.15566.87
9. Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107–1113. doi:10.1111/anae.12344
10. Elhawary H, Abdelhamid K, Meng F, Janis JE. Erector spinae plane block decreases pain and opioid consumption in breast surgery: systematic review. Plast Reconstr Surg Glob Open. 2019;7(11):1–8. doi:10.1097/GOX.0000000000002525
11. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
12. Gaballah KM, Soltan WA, Bahgat NM. Ultrasound-guided serratus plane block versus erector spinae block for postoperative analgesia after video-assisted thoracoscopy: a pilot randomized controlled trial. J Cardiothorac Vasc Anesth. 2019;33(7):1946–1953. doi:10.1053/j.jvca.2019.02.028
13. Woodworth GE, Ivie RMJ, Nelson SM, Walker CM, Maniker RB. Perioperative breast analgesia: a qualitative review of anatomy and regional techniques. Reg Anesth Pain Med. 2017;42(5):609–631. doi:10.1097/AAP.0000000000000641
14. Wild K, Chin KJ. Regional techniques for thoracic wall surgery. Curr Anesthesiol Rep. 2017;7(2):212–219. doi:10.1007/s40140-017-0212-y
15. Khemka R, Chakraborty A. Ultrasound-guided modified serratus anterior plane block for perioperative analgesia in breast oncoplastic surgery: a case series. Indian J Anaesth. 2019;63(3):231. doi:10.4103/ija.IJA_752_18
16. Mazzinari G, Rovira L, Casasempere A, et al. Interfascial block at the serratus muscle plane versus conventional analgesia in breast surgery: a randomized controlled trial. Reg Anesth Pain Med. 2019;44(1):52–58. doi:10.1136/rapm-2018-000004
17. Rahimzadeh P, Imani F, Faiz SHR, Boroujeni BV. Impact of the ultrasound-guided serratus anterior plane block on post-mastectomy pain: a randomised clinical study. Turk Anesteziyoloji Ve Reanimasyon Dern Derg. 2018;46(5):388–392. doi:10.5152/TJAR.2018.86719
18. Kot P, Rodriguez P, Granell M, et al. The erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72(3):209–220. doi:10.4097/kja.d.19.00012
19. Gürkan Y, Aksu C, Kuş A, Yörükoğlu UH, Kılıç CT. Ultrasound guided erector spinae plane block reduces postoperative opioid consumption following breast surgery: a randomized controlled study. J Clin Anesth. 2018;50(April):65–68. doi:10.1016/j.jclinane.2018.06.033
20. Selvi O, Tulgar S. Use of the ultrasound-guided erector spinae plane block in segmental mastectomy. Turk J Anaesthesiol Reanim. 2019;47(2):158–160. doi:10.5152/TJAR.2019.50024
21. Seelam S, Nair A, Christopher A, Upputuri O, Naik V, Rayani B. Efficacy of single-shot ultrasound-guided erector spinae plane block for postoperative analgesia after mastectomy: a randomized controlled study. Saudi J Anaesth. 2020;14(1):22. doi:10.4103/sja.SJA_260_19
22. Wang HJ, Liu Y, Ge WW, et al. Comparison of ultrasound-guided serratus anterior plane block and erector spinae plane block perioperatively in radical mastectomy. Zhonghua Yi Xue Za Zhi. 2019;99(23):1809–1813. doi:10.3760/cma.j.issn.0376-2491.2019.23.012
23. Altlparmak B, Korkmaz Toker M, Uysal AI, Gümüş Demirbilek S. Comparison of the efficacy of erector spinae plane block performed with different concentrations of bupivacaine on postoperative analgesia after mastectomy surgery: randomized, prospective, double blinded trial. BMC Anesthesiol. 2019;19(1):1–9. doi:10.1186/s12871-019-0700-3
24. Garimella V, Cellini C. Postoperative pain control. Clin Colon Rectal Surg. 2013;26(3):191–196. doi:10.1055/s-0033-1351138
25. Tobias JD. Weak analgesics and nonsteroidal anti-inflammatory agents in the management of children with acute pain. Pediatr Clin North Am. 2000;47(3):527–543. doi:10.1016/S0031-3955(05)70224-8
26. Kokki H. Nonsteroidal anti-inflammatory drugs for postoperative pain. Paediatr Drugs. 2003;5(2):103–123. doi:10.2165/00128072-200305020-00004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.