Back to Journals » Open Access Emergency Medicine » Volume 15
Perioperative Adverse Outcome and Its Predictors After Emergency Laparotomy Among Sigmoid Volvulus Patients: Retrospective Follow-Up Study
Authors Deresse T ![]() , Tesfahun E
, Tesfahun E ![]() , Gebreegziabher ZA
, Gebreegziabher ZA ![]() , Bogale M, Alemayehu D
, Bogale M, Alemayehu D ![]() , Dessalegn M
, Dessalegn M ![]() , Kifleyohans T, Eskandar G
, Kifleyohans T, Eskandar G
Received 12 July 2023
Accepted for publication 11 October 2023
Published 19 October 2023 Volume 2023:15 Pages 383—392
DOI https://doi.org/10.2147/OAEM.S430193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Tilahun Deresse,1 Esubalew Tesfahun,2 Zenebe Abebe Gebreegziabher,2 Mandante Bogale,3 Dawit Alemayehu,3 Megbar Dessalegn,3 Tewodros Kifleyohans,1 George Eskandar4
1Department of Surgery, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Public Health, Debre Berhan University, Debre Berhan, Ethiopia; 3Department of Surgery, Debre Markos University, Debre Markos, Ethiopia; 4Department of Surgery, Glan Clwyd Hospital, Rhyl, UK
Correspondence: Tilahun Deresse, Department of Surgery, Debre Berhan University, Debre Berhan, Ethiopia, Email [email protected]
Background: Acute sigmoid volvulus is a surgical emergency with closed-loop obstruction of the colon that often requires emergency laparotomy, which is associated with a multitude of post-operative complications. Although sigmoid volvulus is the main cause of intestinal obstruction in Ethiopia, local studies of its management outcomes are limited.
Objective: To assess the magnitude and predictors of adverse perioperative outcomes of emergency laparotomy for acute sigmoid volvulus in the Debre Markos Comprehensive Specialized Hospital (DMCSH), Amhara region, Ethiopia in 2023.
Methods: This was a retrospective follow-up study. Descriptive statistics were used to measure perioperative outcomes and other study variables. Bivariable and multivariable logistic regression models were used to identify the predictors of adverse surgical outcomes. Associations were considered significant at p < 0.05 (95% confidence interval).
Results: In total, 170 study participants were enrolled, with a response rate of 91.4%. Forty-nine patients (28.8%) developed perioperative adverse outcomes. Pneumonia (29 patients, 28.1%), surgical site infection (19 patients, 18.4%), and wound dehiscence (10 patients, 9.7%) were the most common complications. Pre-operative shock [AOR: 3.87 (95% CI: (1.22, 12.28))], pus or fecal matter contamination of the peritoneum [AOR: 4.43 (95% CI: (1.35, 14.47)], and a higher American Society of Anesthesiologists (ASA) score [AOR: 2.37 (95% CI: (1.05, 5.34))] were identified as predictors of perioperative adverse events.
Conclusion: The perioperative adverse outcomes in this study were higher than those reported in Ethiopian national and global reports following emergency laparotomies. Hypotension at presentation, pus and/or fecal matter contamination of the peritoneum, and higher ASA scores are strong predictors of increased perioperative adverse outcomes. Therefore, healthcare providers and institutions involved in the delivery of emergency surgical care should emphasize the importance of early surgical intervention, adequate resuscitation, and patient monitoring to improve perioperative outcomes.
Keywords: sigmoid volvulus, perioperative outcome, emergency laparotomy, Ethiopia
Introduction
Acute sigmoid volvulus is a surgical emergency with closed-loop obstruction of the colon that often requires an emergency laparotomy, known to man since the time of immemorial.1 It is an abnormal twist of the sigmoid colon on its mesenteric axis more than 180 degrees. It initially results in obstruction of the intestinal lumen and, if not managed urgently, obstruction of the mesenteric vessels will end up causing bowel ischemia, which will require emergent laparotomy, which is not a benign procedure, it is associated with a multitude of post-operative complications, a fourfold risk of mortality when compared with elective procedures, and even the difference becomes dramatic when compared with viable bowel (50% versus 7.5% mortality).2
The prevalence of sigmoid volvulus as a cause of large bowel obstruction ranges from 1–7% in the United States3 and 80% in the Andes.4 The highest incidence in Africa has been reported in Ethiopia, which accounts for 56% of patients with intestinal obstruction.5
Management options for sigmoid volvulus include temporary measures like colonoscopic deflation, surgery with resection and primary anastomosis, surgery with derotation and later sigmoidectomy and anastomosis, and surgery with resection and end colostomy and later colostomy takedown.6,7
Emergency laparotomy (EL) is a collective term for procedures involving a variety of time-sensitive and urgent intra-abdominal surgical conditions that require surgical intervention shortly after symptom onset.8 As surgery is inherently invasive, emergency laparotomy may result in all forms of postoperative complications, including death.9,10 Perioperative adverse events included unfavorable intra-operative and post-operative complications.11 It is obvious that events occurring during the post-operative period may have a major impact on patient well-being. However, significant intra-operative events should also be recorded and reported, even if they do not lead to post-operative morbidity or affect the post-operative well-being of the patient.12
Perioperative adverse outcomes following emergency laparotomy for acute sigmoid volvulus are particularly high because it is a disease of the elderly with multiple comorbidities, which are known factors associated with an increased risk of adverse outcomes.7,13
The most common complications reported globally, following sigmoid volvulus surgery are surgical site infection, pneumonia (chest infection), wound dehiscence, anastomotic leak, and intra-abdominal abscess.7,14–16 Ethiopian studies have also revealed similar complications following sigmoid volvulus surgery.5,6,17 The factors associated with an increased risk of perioperative adverse outcomes can be pre-operative, intra-operative, or post-operative.18 Perioperative adverse outcomes appear to be neglected, but they can support the transition to high-quality health systems in low-income and middle-income countries. This can be achieved by analyzing perioperative adverse outcomes to understand the burden of the problem by monitoring and using it as an entry point to explore and diagnose system failures, practical priority setting, and quality improvement programs.19
Studies on perioperative adverse outcomes following emergency laparotomy (EL) for sigmoid volvulus in Ethiopia are limited despite the high prevalence of the disease as a cause of large bowel obstruction.6 Therefore this study aimed to assess the prevalence and predictors of adverse perioperative outcomes in patients operated for sigmoid volvulus in Ethiopia.
Methods and Materials
Study Setting, Design, and Period
This study was conducted at the Debre Markos Comprehensive Specialized Hospital (DMCSH) in Debre Markos City, Northwest Ethiopia. Debre Markos City is located approximately 295 km northwest of Addis Ababa. The hospital is a teaching hospital with 300 beds serving over five million people. This was a retrospective, follow-up study. The study was conducted from April 15, 2023, to May 30, 2023, on patients who underwent surgery between January 1, 2020, and December 31, 2022.
Study Subjects
All patients who underwent emergency laparotomy for acute sigmoid volvulus from January 2020 to December 2022 in the DMCSH, Amhara Region, Ethiopia. Pediatric patients aged less than 18 years were excluded from the study because they have significantly different physiologic states and quite different prevalence of the disease in this age group. Patients who were transferred from another hospital after laparotomy were excluded from the (because it is difficult to retrieve full pre-operative, intra-operative, and immediate post-operative status from a single-page referral paper) and patients with incomplete charts (without at least one progress note and discharge summary) were excluded from the study and analysis.
Operational Definition
Adverse Outcome
The condition of the patient after the procedure where he/she develops one or more of the following post-operative complications (Death, wound dehiscence, surgical site infection (all types), pneumonia, urinary tract infection, acute kidney injury).5–7,15,17,20
Data Collection Tool and Procedure
A data extraction checklist was prepared based on the literature reviewed5,7,14,17,21,22 and used to extract the necessary data from the charts of the study participants taken from the archive of the Debre Markos Comprehensive Specialized Hospital. The tool was evaluated by four general surgeons, and a pre-test was performed before it was used to collect real data. It contains the following four sections: sociodemographic, pre-operative clinical, intra-operative clinical, and post-operative follow-up data. Data were collected by four general practitioners. The chart numbers of patients who underwent surgery for acute sigmoid volvulus on an emergency basis were identified from the operating room registry book (log book). Charts were retrieved from the chart archive of the hospital, and data were collected from individual folders after confirming that they fulfilled the inclusion criteria.
Data Quality Assurance
The data extraction checklist was prepared based on the findings and tools used in the literature from peer-reviewed journals. In addition, it was evaluated by four general surgeons from Debre Berhan and Debre Markos universities to determine whether it included all relevant items and its general applicability for retrieving the intended data. The tool was pretested before actual data collection started on 12 subjects and at three sites (DMCSH, Woldia, and Debre Tabor hospitals) for general applicability, clarity, readability, and comprehensiveness. One day of training was provided to the data collectors by the principal investigator before starting data collection. During the data collection period, the investigator closely supervised and monitored the data.
Data Analysis
Data were exported from Kobo-tool, an online data collection tool, to Microsoft Office Excel and data cleaning and coding were performed using Excel. The data were exported to SPSS version 20 for recording and analysis. Outcomes were stated in binary form as developing or not developing adverse perioperative outcome. Descriptive statistics were presented as percentages, means, medians, interquartile ranges, standard deviations, and rates. The assumptions of the chi-square test were duly verified and deemed to have been met before its execution, while the model fitness test was examined before logistic regression analysis. Bivariable logistic regression analysis was used to assess the relationship between each predictor variable and the adverse perioperative outcomes. Variables with p < 0.20 in the bivariable logistic regression analysis, were entered for multivariable logistic regression analysis. Statistically significant associations between predictors and adverse perioperative outcomes were accepted at p-value < 0.05.
Results
Socio-Demographic Characteristics and Mode of Arrival
A total of 186 patients underwent emergency laparotomy for acute sigmoid volvulus, among whom 16 were excluded because of incomplete charts, resulting in a response rate of 91.4%. The average age of the respondents was 53.84 ± 13.52 SD years. Most of the respondents 136 (80%) were referred from other institutions and 152 (89.4%) (Table 1).
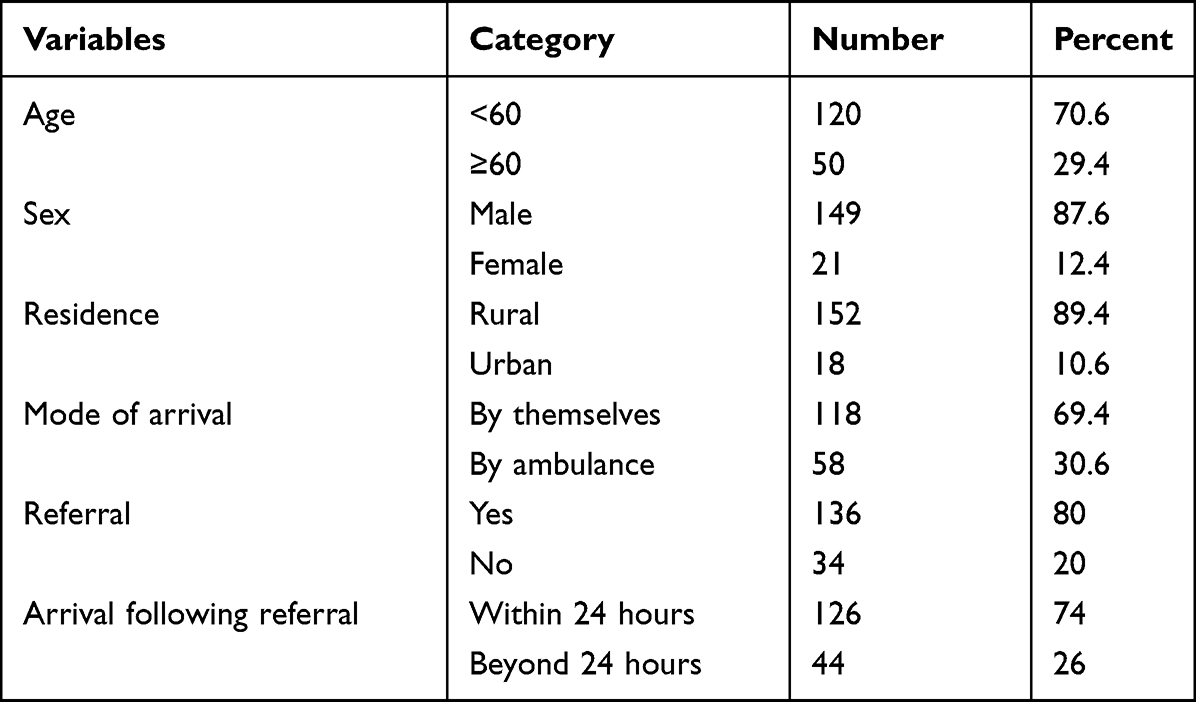 |
Table 1 Socio-Demographic Characteristics and Mode Arrival of Post-Emergency Laparotomy Sigmoid Volvulus Patients at Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia, from January 1, 2020, to December 31, 2022 |
Clinical Presentation and Characteristics of Study Participants
2The majority of the patients enrolled in this study presented with constipation 162 (95.3%) and gross abdominal distension 144 (84.7%). The duration of symptoms ranged from one to seven days, with a median duration of two days. Fifteen patients (8.8%) had comorbid diseases, such as hypertension, cardiac disease, chronic renal disease, HIV/AIDS, and chronic pulmonary disease; two patients had been treated for malignancies; and four patients had a previous history of abdominal surgery. Ninety (52.9%) patients in this study had plain abdominal radiographs and demonstrated the classical features of sigmoid volvulus (Table 2).
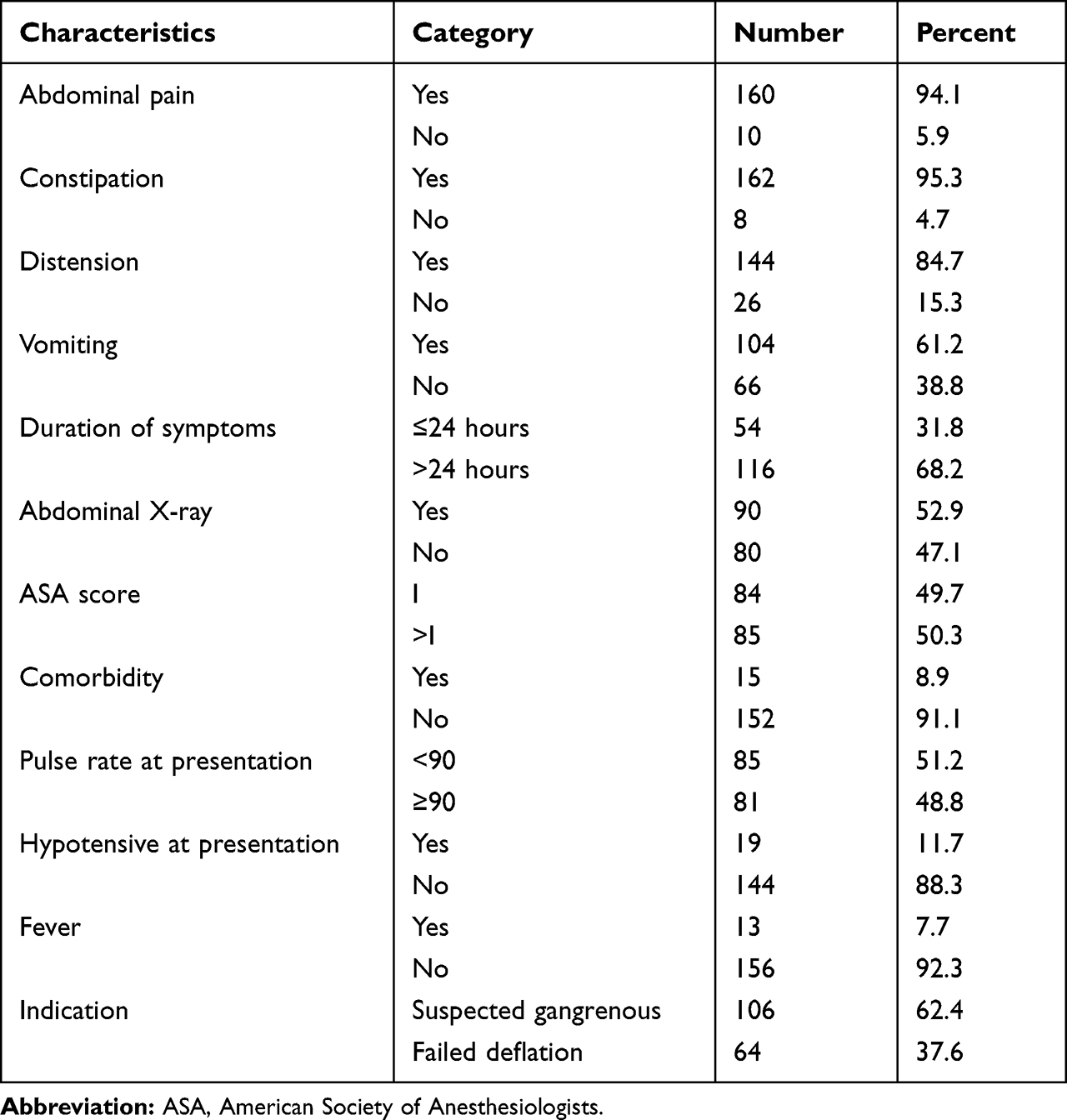 |
Table 2 Clinical Presentation and Characteristics of Patients Who Underwent Emergency Laparotomy for Sigmoid Volvulus at Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia, from January 1, 2020, to December 31, 2022 |
Treatment Modalities and Intra-Operative Findings
All 170 patients underwent an emergency laparotomy, with either resection and end-to-end anastomosis (REEA), or colostomy. Before entering the operating theatre, 151 (88.8%) patients required fluid resuscitation and three (1.8%) required pre-operative vasopressor use. Pre-operative transfusion was performed in 10 (5.9%) patients. Resection and end-to-end anastomosis (REEA) was the most common 104 (61.2%) procedure performed (Table 3). The World Health Organization (WHO) Surgical Safety Checklist format was found in 97% of the charts. Two patients experienced massive intra-operative bleeding (greater than 500 mL), but no serious intra-operative incidents occurred. Two other patients were also taking vasopressors to maintain their blood pressure.
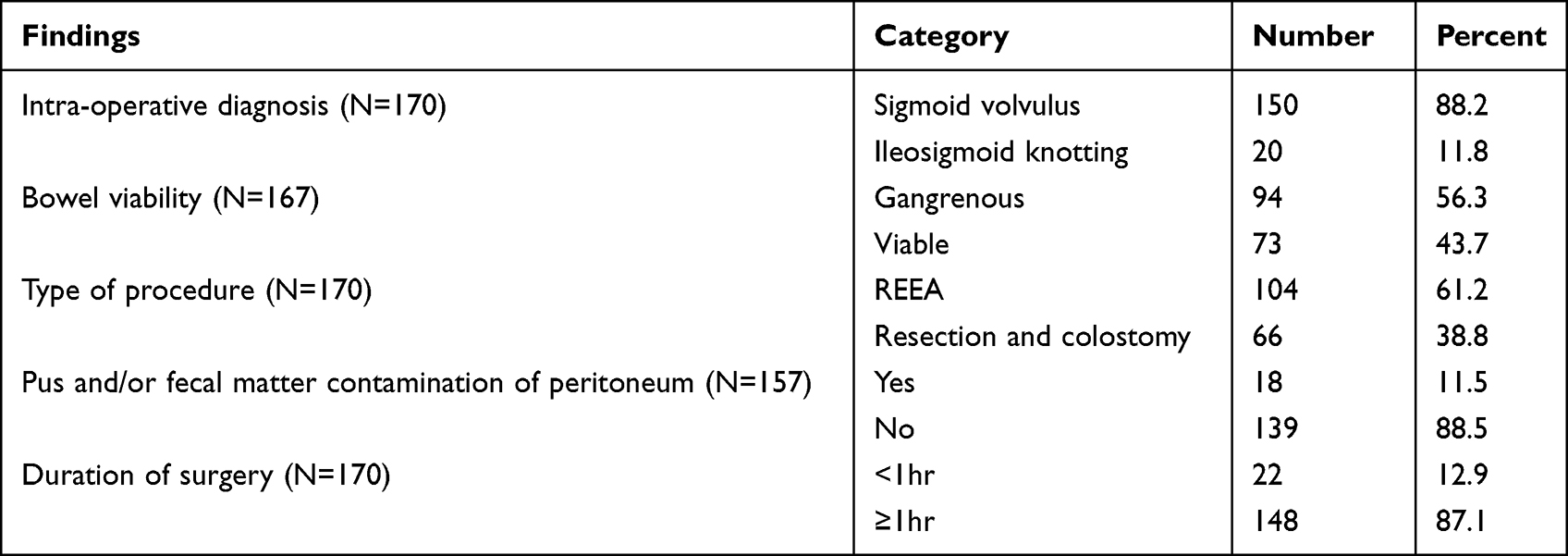 |
Table 3 Treatment Modalities and Intra-Operative Findings of Patients Who Underwent Emergency Laparotomy for Sigmoid Volvulus at Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia, from January 1, 2020, to December 31, 2022 |
Overall Perioperative Adverse Outcome
A total of 103 post-operative complications, including death, were recorded in 49 (28.8%) patients. Post-operative chest infection (pneumonia) (n = 29, 17.5%) was the most common (Table 4).
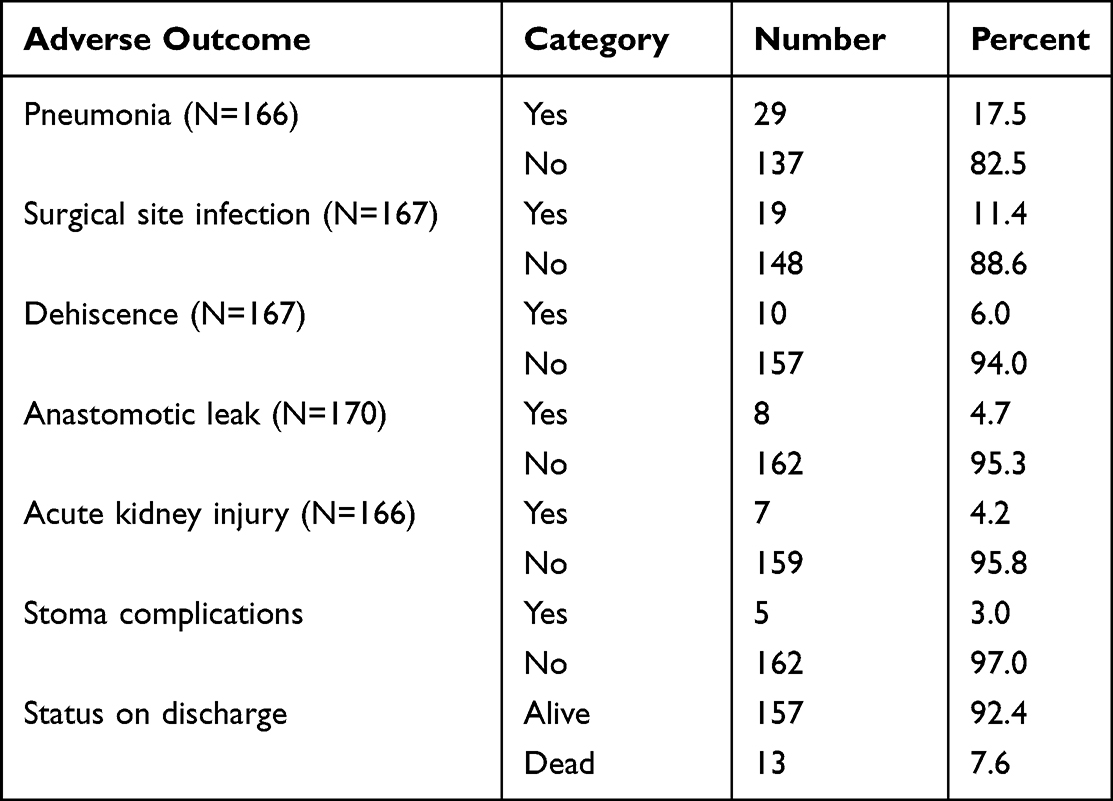 |
Table 4 Perioperative Adverse Outcomes Among Post-Emergency Laparotomy Sigmoid Volvulus Patients at Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia, from January 1, 2020, to December 31, 2022 |
Predictors of Perioperative Adverse Outcome
All variables with a p-value less than 0.20 were candidates for multivariable logistic regression analysis. In the multivariable logistic regression, hypotension at presentation [AOR: 3.87 (95% CI: (1.22, 12.28))], pus or fecal matter contamination of the peritoneum [AOR: 4.43 (95% CI: (1.35, 14.47)], and advanced ASA score [AOR: 2.37 (95% CI: (1.05, 5.34)] were found to be significant predictors of perioperative adverse outcomes (Table 5).
 |
Table 5 Bivariable and Multivariable Logistic Regression Analyses of Post-Emergency Laparotomy Sigmoid Volvulus Patients at Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia, from January 1, 2020, to December 31, 2022 |
Discussion
This study aimed to determine the perioperative adverse outcome status and its predictors after emergency laparotomy in patients with sigmoid volvulus within 30 days of follow-up.
In this study, the overall rate of adverse outcomes was 28.8% (CI: 21.5, 35.9). This finding is higher than that reported in a study from West Ethiopian District Hospital (22.1%),6 which might be explained by disease severity. The findings of this study are also higher than those of other studies conducted in Mali (11%), Turkey (15%), Pakistan (19%), Tanzania (20.5%), Korea (27%), and Cote d’Ivoire (27.2%).7,15,23–26 This difference might be explained by the relatively delayed presentation of the patients. These discrepancies may be further related to the relatively better quality of surgical care delivery and systems of care found in the study areas which we are comparing with. Moreover, it was higher than that of a multinational prospective study conducted by the World Health Organization (WHO) between October 2007 and September 2008, which reported an adverse outcome rate of 7%.27 The difference in the rate of adverse outcomes may be explained by the inclusion of elective cases in the reporting of overall adverse outcomes, which may have moderated the overall rate of adverse outcomes. However, this finding revealed a lower overall adverse outcome rate when compared with findings from studies conducted in Ethiopia (48.4%), the United States (64%), France (35%), and Turkey (37.2%).16,17,21,28 These differences might be explained by the relatively older age of participants with multiple comorbidities in the aforementioned studies. Perioperative adverse outcomes are key quality indicators associated with high-level process indicators in healthcare settings.29 Similarly, factors related to perioperative adverse outcomes may go beyond individual patient-related parameters. This may be associated with hospital-related adverse events.30,31
This study revealed that patients who were hypotensive at presentation were 3.87 times more likely to develop perioperative adverse outcomes. These results are consistent with those of previous studies conducted in Ethiopia, Tanzania, and the U.S.7,10,32,33 Optimization of blood pressure during the perioperative period has been shown to enhance surgical outcomes. According to a systematic review, hypotension increases the likelihood of adverse post-operative outcomes. The presence of hemodynamic instability pre-operatively raises the likelihood of complications including postoperative mortality.34 The major difference between patients who underwent emergency laparotomy and those who underwent elective intra-abdominal procedures was that the former group presented with physiological disarray.35 The attainment of hemodynamic stability via timely evaluation and resuscitation with goal-oriented fluid therapy is a fundamental facet of emergency laparotomy quality improvement bundles.36 These findings have significant implications for ascertaining the sufficiency of pre-operative resuscitation in accordance with pre-operative care guidelines and for making informed evidence-based decisions regarding the imperative of surgical intervention among patients exhibiting pre-operative hemodynamic instability.
Intra-operative finding of gross peritoneal contamination by pus and/or fecal matter was found to be a significant predictor of perioperative adverse outcomes [AOR: 4.43 (95% CI: (1.35, 14.47)]. This was consistent with studies conducted in Gondar (Ethiopia), Metu (Ethiopia), and Mekelle (Ethiopia), which found an increased likelihood of adverse perioperative outcomes following emergency laparotomy if peritoneal contamination with pus and fecal matter was present.5,6,37 Furthermore, studies conducted in Tanzania, Nigeria, Cote d’ Ivore and France have confirmed that patients with peritoneal complications are more likely to develop perioperative adverse outcomes.7,21,38,39 Peritoneal contamination of pus and/or fecal matter in the sigmoid volvulus is a sign of an advanced stage due to delayed presentation or neglect to be managed urgently after arrival. The obstructed bowel develops ischemia and perforation due to abnormal and prolonged distension of the twisted loop40 and This may be because patients coming from rural areas, who account for the majority of cases in this study (89.4%), may have to travel long distances and may prefer traditional remedies before coming to the hospital, which may delay their presentation. Other reasons related to this delay may be related to long referral chains,41 individual health-seeking behavior for social or economic reasons,42,43 or poor overall access to surgical services, which takes more than 28.4 Hours to access a specialized hospital in Ethiopia.44 In this study, 80% of patients were referred or transferred from other health institutions, and only 52 (30.6%) were transported by ambulance. Therefore, the problem related to delayed presentation needs further characterization to improve early admission, understand the causes of delay, and improvement in the referral chain, or surgical care delivery within a reasonable distance.
This study found that patients with a higher ASA status (ASA II–IV) were 2.37 times more likely to develop perioperative adverse outcomes [AOR: 2.37 (95% CI: (1.05, 5.34))]. This finding was consistent with those of a multicenter study conducted in southern Ethiopia,32 Cologne (Germany),45 and Wales (United Kingdom),46 which demonstrated that the risk of developing post-operative complications was highly influenced by a higher ASA category. This may be attributed to the patients’ poor physical condition and debilitating comorbidities during the pre-operative period.
The mean length of hospital stay in this study was 8.32 + 6.40 days; which is consistent with a similar study from Pakistan with a mean hospital stay of 7.6 days.15 However, in contrast to reports from West Ethiopia and Tanzania, the mean hospital stay was 13.5 days6 and 14 days,7 respectively. Development of complications and type of procedure (Resection + colostomy) were identified as factors associated with prolonged hospital stay, which is in contrast to a study from India that reported prolonged hospital stay in the resection and primary anastomosis groups.47
Limitations of the Study
As this was a retrospective study, all the limitations associated with the study design must be considered. This study evaluated only 30 days of the perioperative period, whereas surgical complications, including death, can happen over months. Since this was a single-center study, the external validity may be limited.
Conclusion & Recommendation
The magnitude of perioperative adverse outcomes in this study was higher than those in several national and global perioperative adverse outcome reports following emergency surgery for acute sigmoid volvulus. Hemodynamic instability, pus and/or fecal peritonitis, and advanced ASA score were strong predictors of adverse perioperative outcomes. Therefore, healthcare providers and institutions involved in the delivery of emergency surgical care should emphasize the importance of early surgical intervention, adequate resuscitation, and patient monitoring to improve perioperative outcomes. In addition, researchers should investigate the problem with a larger sample, multicenter study, and better design to overcome the limitations mentioned in this study.
Abbreviations
AOR, Adjusted Odds Ratio; ASA, American Society of Anesthesiologists; AWHSC, Asrat Waldeyes Health Science Campus; CI, Confidence Interval; CT, Computed Tomography; DBU, Debre Berhan University; DMCSH, Debre Markos Comprehensive Specialized Hospital; EL, Emergency laparotomy; EOPD, emergency outpatient department; ETB, Ethiopian Birr; HIMS, Health Information Management System; ICU, Intensive Care Unit; LMICs, Low- and Middle-Income Countries; mmHg, Millimeter Mercury; PACU, Post Anesthesia Care Unit; USA, United States of America; WHO, World Health Organization.
Data Sharing Statement
The raw data can be accessed in response to reasonable requests from the corresponding author of this paper.
Ethical Approval and Consent to Participate
Ethical clearance was obtained, and the need for written informed consent was waived by the ethical review board of Debre Berhan University, Asrat Waldeyes Health Science Campus (IRB-158). Subsequently, permission was obtained from the Debre Markos Comprehensive Specialized Referral Hospital Quality Assurance Office, relevant departments, and unit heads of the hospital. No personal identifiers were included in the patients’ medical records during data extraction; therefore, it did not inflict any harm to the patients. All information used from the charts was kept confidential, and all methods were performed in accordance with the relevant guidelines and complies with the Declaration of Helsinki.
Acknowledgments
We extend our sincere gratitude to the research team members, who contributed to the completion of this study. Finally, we would like to express our heartfelt gratitude to all participants, data collectors, and supervisors for their time and effort.
Funding
There are no specific grants for this research from funding agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Brothwell D. The evidence for neoplasms. Dis Antiquity. 1967;1967:320–345.
2. Wertkin MG, Aufses AH. Management of volvulus of the colon. Dis Colon Rectum. 1978;21(1):40–45. doi:10.1007/BF02586545
3. Swenson BR, Kwaan MR, Burkart NE, et al. Colonic volvulus: presentation and management in metropolitan Minnesota, United States. Dis Colon Rectum. 2012;55(4):444–449. doi:10.1097/DCR.0b013e3182404b3d
4. Asbun H, Castellanos H, Balderrama B, et al. Sigmoid volvulus in the high altitude of the Andes. Dis Colon Rectum. 1992;35(4):350–353. doi:10.1007/BF02048112
5. Ali M. Treatment of sigmoid volvulus: experience in Gondar, north-west Ethiopia. Ethiop Med J. 1998;36(1):47–52.
6. Mulugeta GA, Awlachew S. Retrospective study on pattern and outcome of management of sigmoid volvulus at district hospital in Ethiopia. BMC Surg. 2019;19(1):1–5. doi:10.1186/s12893-019-0561-1
7. Chalya PL, Mabula JB. Sigmoid volvulus and ileo-sigmoid knotting: a five-year experience at a tertiary care hospital in Tanzania. World J Emerg Surg. 2015;10(1):1–8. doi:10.1186/s13017-015-0001-1
8. Ahmed A, Azim A. Emergency Laparotomies: causes, pathophysiology, and outcomes. Indian J Crit Care Med. 2020;24(Suppl 4):S183–s9.
9. Shimada H, Fukagawa T, Haga Y, Oba K. Does postoperative morbidity worsen the oncological outcome after radical surgery for gastrointestinal cancers? A systematic review of the literature. Ann Gastroenterol Surg. 2017;1(1):11–23. doi:10.1002/ags3.12002
10. Martin ND, Patel SP, Chreiman K, et al. Emergency laparotomy in the critically ill: futility at the bedside. Crit Care Res Pract. 2018;2018:1–6. doi:10.1155/2018/6398917
11. Li Q, Zhang X, Xu M, Wu J. A retrospective analysis of 62,571 cases of perioperative adverse events in thoracic surgery at a tertiary care teaching hospital in a developing country. J Cardiothorac Surg. 2019;14(1):98. doi:10.1186/s13019-019-0921-z
12. Kazaryan AM, Røsok BI, Edwin B. Morbidity assessment in surgery: refinement proposal based on a concept of perioperative adverse events. ISRN Surg. 2013;2013:625093. doi:10.1155/2013/625093
13. Atamanalp SS, Disci E, Atamanalp RS. Sigmoid volvulus: comorbidity with sigmoid gangrene. Pak J Med Sci. 2019;35(1):288. doi:10.12669/pjms.35.1.295
14. Kapan M, Onder A, Arikanoglu Z, et al. Sigmoid volvulus treated by resection and primary anastomosis: urgent and elective conditions as risk factors for postoperative morbidity and mortality. Eur J Trauma Emerg Surg. 2012;38:463–466. doi:10.1007/s00068-012-0191-0
15. Naseer A, Ahmad S, Naeem M. One stage emergency resection and primary anastomosis for sigmoid volvulus. J Coll Physicians Surg Pak. 2010;20(5):307–309.
16. Smothers L, Hynan L, Fleming J, Turnage R, Simmang C, Anthony T. Emergency surgery for colon carcinoma. Dis Colon Rectum. 2003;46(1):24–30. doi:10.1007/s10350-004-6492-6
17. Engida A, Ayelign T, Mahteme B, Aida T, Abreham B. Types and Indications of Colostomy and Determinants of Outcomes of Patients After Surgery. Ethiop J Health Sci. 2016;26(2):117–120. doi:10.4314/ejhs.v26i2.5
18. Temesgen N, Fenta E, Eshetie C, Gelaw M. Early intraoperative hypotension and its associated factors among surgical patients undergoing surgery under general anesthesia: an observational study. Ann Med Surg. 2021;71:102835. doi:10.1016/j.amsu.2021.102835
19. Speizer IS, Story WT, Singh K. Factors associated with institutional delivery in Ghana: the role of decision-making autonomy and community norms. BMC Pregnancy Childbirth. 2014;14(1):1–13. doi:10.1186/s12884-014-0398-7
20. Tekalign T, Balta H, Kelbiso L. Magnitude of post-operative mortality and associated factors among patients who underwent surgery in Wolaita Sodo teaching and referral hospital, SNNPR region, Ethiopia. Afr Health Sci. 2021;21(4):1842–1848. doi:10.4314/ahs.v21i4.42
21. Alves A, Panis Y, Mathieu P, et al. Postoperative mortality and morbidity in French patients undergoing colorectal surgery: results of a prospective multicenter study. Arch Surg. 2005;140(3):278–283. doi:10.1001/archsurg.140.3.278
22. Bagarani M, Conde AS, Longo R, Italiano A, Terenzi A, Venuto G. Sigmoid volvulus in West Africa: a prospective study on surgical treatments. Dis Colon Rectum. 1993;36(2):186–190. doi:10.1007/BF02051177
23. Bengaly B, Kanté A, Ouattara D, et al. Volvulus acute of the colonist sigmoid to mopti: diagnostic and therapeutic aspects. Surg Sci. 2018;9(11):446–453. doi:10.4236/ss.2018.911050
24. Sozen S, Das K, Erdem H, Menekse E, Cetinkunar S, Karateke F. Resection and primary anastomosis with modified blow-hole colostomy or Hartmann’s procedure. Which method should be performed for gangrenous sigmoid volvulus. Chirurgia. 2012;107:751–755.
25. Lee K, H-K O, Cho JR, et al. Surgical management of sigmoid volvulus: a multicenter observational study. Ann Coloproctol. 2020;36(6):403. doi:10.3393/ac.2020.03.23
26. Mirande RL. Restoration of Digestive Continuity after Digestive Ostoma: Indications and Management. Doctor of Medicine Thesis (Madagascar: University of Antananarivo); 2017.
27. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491–499. doi:10.1056/NEJMsa0810119
28. Ören D, Atamanalp SS, Aydinli B, et al. An algorithm for the management of sigmoid colon volvulus and the safety of primary resection: experience with 827 cases. Dis Colon Rectum. 2007;50:489–497. doi:10.1007/s10350-006-0821-x
29. Ngantcha M, Le-Pogam M-A, Calmus S, et al. Hospital quality measures: are process indicators associated with hospital standardized mortality ratios in French acute care hospitals? BMC Health Serv Res. 2017;17(1):1–9. doi:10.1186/s12913-017-2534-3
30. Chung W, Sohn M. The impact of nurse staffing on in-hospital mortality of stroke patients in Korea. J Cardiovasc Nurs. 2018;33(1):47–54. doi:10.1097/JCN.0000000000000415
31. Aranaz Andrés JM, Limón Ramírez R, Aibar Remón C, et al. Comparison of two methods to estimate adverse events in the IBEAS Study (Ibero-American study of adverse events): cross-sectional versus retrospective cohort design. BMJ Open. 2017;7(10):e016546. doi:10.1136/bmjopen-2017-016546
32. Hailu S, Ayinie A, Amsalu H, et al. Perioperative mortality and its predictors among patients undergoing emergency laparotomy at selected southern Ethiopian governmental hospitals, 2022: a multicenter prospective cohort study. Ann Med Surg. 2023;85(4):746. doi:10.1097/MS9.0000000000000437
33. Easterday A, Aurit S, Driessen R, Person A, Krishnamurty DM. Perioperative outcomes and predictors of mortality after surgery for sigmoid volvulus. J Surg Res. 2020;245:119–126. doi:10.1016/j.jss.2019.07.038
34. Lizano-Díez I, Poteet S, Burniol-Garcia A, Cerezales M. The burden of perioperative hypertension/hypotension: a systematic review. PLoS One. 2022;17(2):e0263737. doi:10.1371/journal.pone.0263737
35. Shafi S, Aboutanos MB, Agarwal JS, et al. Emergency general surgery: definition and estimated burden of disease. J Trauma Acute Care Surg. 2013;74(4):1092–1097. doi:10.1097/TA.0b013e31827e1bc7
36. Peden CJ, Aggarwal G, Aitken RJ, et al. Guidelines for perioperative care for emergency laparotomy enhanced recovery after surgery (ERAS) Society recommendations: part 1—preoperative: diagnosis, rapid assessment and optimization. World J Surg. 2021;45(5):1272–1290. doi:10.1007/s00268-021-05994-9
37. Hagos M. ACUTE ABDOMEN IN ADULTS: a TWO YEAR EXPERIENCE IN MEKELLE, ETHIOPIA. Ethiop Med J. 2015;53(1):19–24.
38. Sule A, Ajibade A. Adult large bowel obstruction: a review of clinical experience. Ann Afr Med. 2011;10(1). doi:10.4103/1596-3519.76586
39. Kassi A, Lebeau R, Yenon K, Katche E, Diané B, Kouassi J. Morbidity and mortality of Hartmann’s procedure for sigmoid volvulus at the university hospital of Cocody, Abidjan. West Afr J Med. 2011;30(3):169–172.
40. Cirocchi R, Farinella E, La Mura F, et al. The sigmoid volvulus: surgical timing and mortality for different clinical types. World J Emerg Surg. 2010;5:1–5. doi:10.1186/1749-7922-5-1
41. Royal C, McKerrow N. A retrospective review of the transfer of critically ill children to tertiary care in KwaZulu-Natal Province, South Africa. S Afr J Child Health. 2015;9(4):112–118. doi:10.7196/SAJCH.2015.v9i4.913
42. O’Toole SJ, Karamanoukian HL, Allen JE, et al. Insurance-related differences in the presentation of pediatric appendicitis. J Pediatr Surg. 1996;31(8):1032–1034. doi:10.1016/S0022-3468(96)90079-2
43. Smink DS, Fishman SJ, Kleinman K, Finkelstein JA. Effects of race, insurance status, and hospital volume on perforated appendicitis in children. Pediatrics. 2005;115(4):920–925. doi:10.1542/peds.2004-1363
44. Meshesha BR, Sibhatu MK, Beshir HM, et al. Access to surgical care in Ethiopia: a cross-sectional retrospective data review. BMC Health Serv Res. 2022;22(1):973. doi:10.1186/s12913-022-08357-9
45. Wolters U, Wolf T, Stützer H, Schröder T. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996;77(2):217–222. doi:10.1093/bja/77.2.217
46. Farrow S, Fowkes FR, Lunn J, Robertson I, Samuel P. Epidemiology in anaesthesia II: factors affecting mortality in hospital. Br J Anaesth. 1982;54(8):811–817. doi:10.1093/bja/54.8.811
47. Pattanayak S, Saha D, Bara BK, Nayak SK. Comparison of primary resection and anastomosis with Hartmann’s procedure in management of acute sigmoid volvulus. Hell J Surg. 2016;88:263–267. doi:10.1007/s13126-016-0329-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.