")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Perinevoid Alopecia: Report of Two Cases and Literature Review
Authors Zhang Y, Zhang J, Zhou C
Received 26 January 2023
Accepted for publication 20 March 2023
Published 11 April 2023 Volume 2023:16 Pages 1003—1008
DOI https://doi.org/10.2147/CCID.S400247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Yujing Zhang, Jianzhong Zhang, Cheng Zhou
Department of Dermatology, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Cheng Zhou, Department of Dermatology, Peking University People’s Hospital, No. 11 Xizhimen South Street, Xicheng District, Beijing, People’s Republic of China, Tel +86-10-88325472, Fax +86 10-68318386, Email [email protected]
Abstract: Perinevoid alopecia (PA) is a rare variant of alopecia areata (AA) associated with a central pigmented nevus. In this study, we reported two cases of PA and reviewed 14 cases from 11 studies in the literature. In one of our cases, PA was combined with a halo nevus and white terminal hairs were spared in the hair loss patch, which was rarely reported in the literature. It is implicated that antigens from melanocytes might be involved in the development of AA in PA.
Keywords: alopecia areata, hair loss, nevus, halo nevus
Introduction
Perinevoid alopecia (PA), first described by Yesudian and Thambiah in 1976, is a variant of alopecia areata (AA) associated with a central pigmented nevus.1,2 We found 14 cases from 11 studies in the literature from 1976 to 2022. PA is an extremely rare disorder with a clinically distinctive feature of alopecic patch with a central pigmented nevus and a histologically specific finding of inflammatory cell infiltration in nevus cell nests and perifollicular areas.4 With dermoscopy, the manifestations of both central nevi and AA were revealed. Although the pathogenesis is still unclear, it is thought that PA is secondary to an inflammatory response against nevus cells or melanocytic structures.1 We reported the clinical findings of two patients with PA.
Case Reports
Case 1
A 46-year-old Chinese male complained of a patchy hair loss with a central blue nevus on his left temporal (Figure 1A). The nevus had been presented more than ten years, while the patch of hair loss was noticed one month prior to the clinic visit. Upon dermatological examination, an area of nonscarring alopecia, approximately 2.0×2.0 cm, without signs of inflammation, surrounding a 4-mm diameter nevus, was observed in the left temporal region. Dermoscopy examination revealed a well-circumscribed lesion with homogenous blue-grayish globular pattern, broken hairs, black dots, yellow dots and short vellus hairs (Figure 1B). The diagnosis of PA was made based on the clinical findings, and two sessions of intralesional steroid injections with a month interval resulted in a complete recovery of hair growth.
 |
Figure 1 Case 1: (A) Macroscopic image showing an area of nonscarring alopecia, approximately 2.0×2.0 cm, without signs of inflammation, surrounding a 4-mm diameter well-circumscribed nevus, was observed in the left temporal region. (B) Dermoscopic image showed a well-circumscribed lesion with homogenous blue-grayish globular pattern, broken hairs, black dots, yellow dots and short vellus hairs. Case 2: (C) Macroscopic image revealed a patchy hair loss with a central nevus and surrounding hypopigmentation in the left temporal region. (D) With dermoscopy, we noticed a globular, dark brown pigmented tumor with peripheral areas of light-brown pigment, short vellus hairs and broken hairs. (E) Wood’s light examination of the area of alopecia was positive with fluorescence enhancement. |
Case 2
A 28-year-old Chinese male patient began to experience a patchy hair loss with a central nevus and surrounding hypopigmentation in the left temporal region two months ago, which increased in size progressively (Figure 1C). The central pigmented nevus had been presented more than ten years, while the asymptomatic patch of hair loss was noticed two months prior to the clinic visit. Dermatological examination revealed a 2-mm diameter dark brown pigmented papule, surrounded by a 0.7-cm diameter area of non-scarring alopecia, and white terminal hairs in the area of previous hair loss were unaffected. With dermoscopy, we noticed a globular, dark brown pigmented tumor with peripheral areas of light-brown pigment, short vellus hairs and broken hairs (Figure 1D). Wood’s light examination of the area of alopecia was positive with fluorescence enhancement (Figure 1E). Halo nevi (HN) consists of central pigmented nevi surrounded by a sharp zone of hypopigmentation, so the diagnosis of PA and HN was made. He was treated with topical minoxidil (5% solution) while complete hair regrowth was observed after a few months.
Discussion
We preferred to define PA as alopecia areata around a pigmented nevus and summarized some clinical findings.3 Various pigmented nevi in 14 cases from 11 studies were found (Table 1), including intradermal nevi (n=5), compound nevi (n=2), blue nevi (n=3), etc.1–11 A blue nevus and a melanocytic nevus were observed in our cases. It seems PA may affect more males than females. In all the 16 reported cases, 13 were males and 3 were females. The age of these patients was from 19 to 46 years old, and the average age was 31.06 years old. The hair loss patches were most frequently located on the vertex (n=7) and occipital (n=5), followed by the beard area (n=1), the back of the scalp (n=1), chin (n=1) and neck area (n=1).
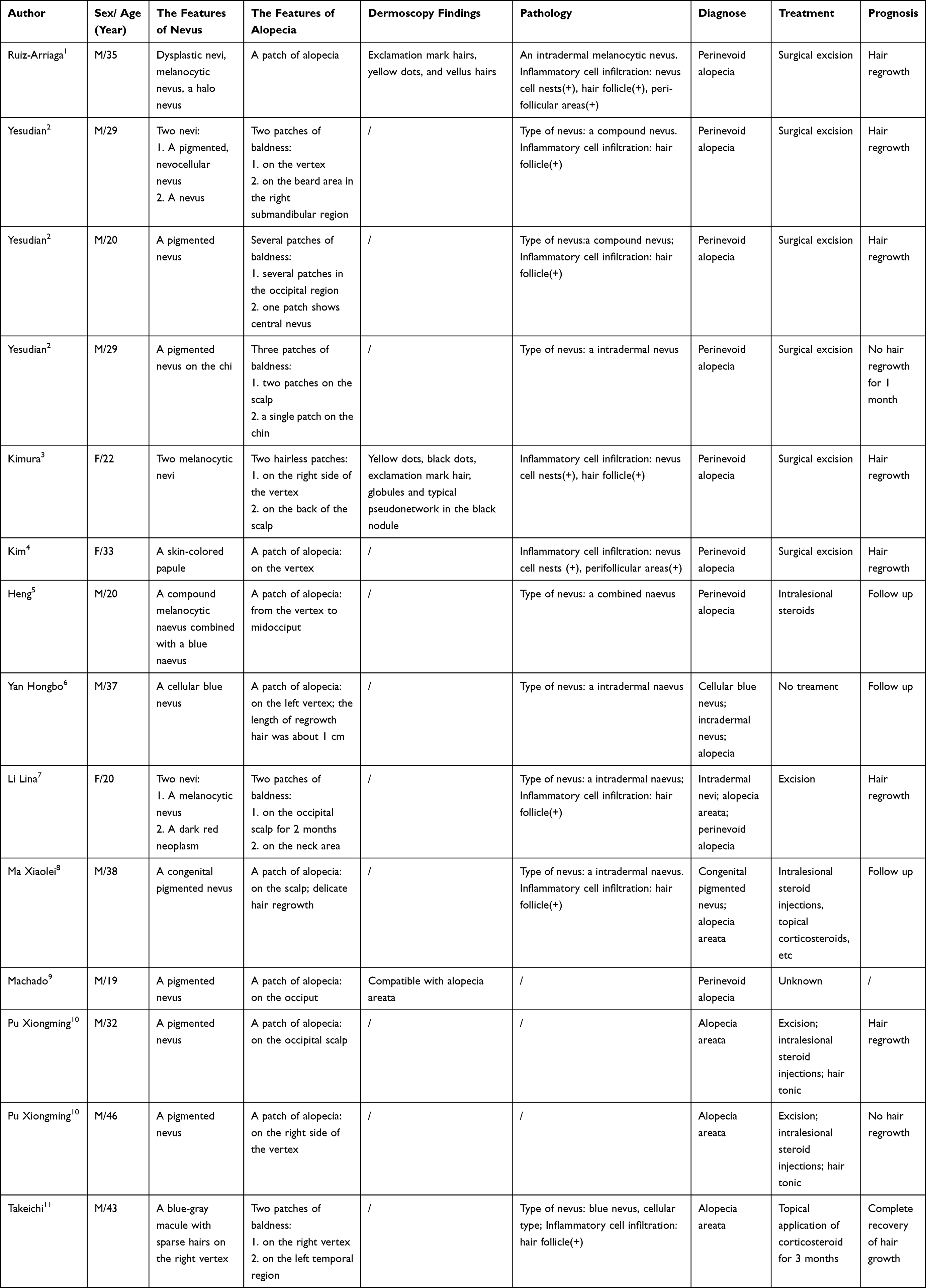 |
Table 1 14 Cases of Perinevoid Alopecia Reported in the Literature |
Dermoscopy examination revealed manifestations of both central nevi and AA. Dermoscopy is the noninvasive diagnostic equipment used increasingly in dermatological practice. In all 5 cases with dermoscopy alterations (including our two cases), yellow dots (n=3), vellus hairs (n=3), black dots (n=2), exclamation mark hairs (n=2), and broken hairs (n=2) were identified, which were consistent with active alopecia areata. A well-circumscribed lesion with homogenous blue-grayish globular pattern and a globular, dark brown pigmented tumor with peripheral areas of light-brown pigment were observed in our cases. Of note, one of our patients had a typical patch of AA with a central halo nevus and remaining white terminal hairs in the area of hair loss, which had not been reported previously.
Histopathologically, inflammatory cell infiltration was most frequently located in perifollicular areas. Skin biopsy in 11 cases showed inflammatory cell infiltration in the hair follicle (HF) (n=7), nevus cell nests (n=3), and perifollicular areas (n=2). Nevus cell nests were present in the upper dermis almost in all cases.
The pathogenesis of PA is unclear, and it might be secondary to an inflammatory response against nevus cells or melanocytic structures.1 HF-derived autoantigens (eg, keratinocyte and melanocyte antigen) have long been suspected as the potential specific autoantigen for AA.12 PA, defined as AA around a pigmented nevus, is a special variant of AA and may be valuable for the better understanding of the pathogenesis of AA. In one of our cases, we found a patch of alopecia with a central halo nevus and white terminal hairs spared in the hair loss patch. A halo phenomenon around a nevus has been suggested to be due to immunologic responses against melanocytes.13 White terminal hairs lack melanocytes so they are not attacked by CD8+ T cells. What’s more, in this case, Wood’s light examination of the area of alopecia was positive with fluorescence enhancement, representing the loss of melanin, which indicated PA might be secondary to an inflammatory response against melanocytes. Unfortunately, no case about PA observed under Wood’s lamp was found and objective biopsy was refused in this case. Moreover, hair regrowth was observed after surgical removal of the whole lesion of the nevus in 7 cases. Therefore, we postulated that the immune cells around the naevi led to an attack on the peripheral HF similar to the autoimmune destruction of melanocytes in a halo naevus. Some antigens of nevus cells were assumed to be similar to the antigens of anagen hair bulbs, such as antigens of melanocytes or melanin granules. Antigens from melanocytes might be involved in the development of AA in PA.
Diagnosis and treatment of PA were summarized. The diagnoses of this disease in 14 cases were PA (n=8), AA (n=5), nevi (n=3), and alopecia (n=1). PA might be misdiagnosed as AA, nevi or alopecia because of unawareness of this rare condition, and the central pigmented nevus was frequently overlooked. Therefore, it is worth reporting this case series to raise the awareness of this rare condition. In most cases, surgical removal of the whole lesion of the nevus (n=9) might lead to hair regrowth (n=7). However, there were two cases that showed no significant hair regrowth after excision of the central nevus. Intralesional steroids may also be effective, as in one of our cases.
A pigmented nevus may lead to inflammatory cell infiltration and immune response, causing peripheral vitiligo or AA. Why it causes these differences remains to be elucidated. Further researches are required to clarify the mechanisms of PA. This special variant of AA may be valuable for the better understanding of pathogenesis and further treatment development of AA.
Abbreviations
PA, perinevoid alopecia; AA, alopecia areata; HN, halo nevus; HF, hair follicle.
Consent Statement
Written informed consent was provided to the patient to have the case details and associated images published. Institutional approval was not required to publish the case details.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82073459).
Disclosure
The authors declare no conflict of interest.
References
1. Ruiz-Arriaga LF, López-García L, Vega-Memije ME. Perinevoid alopecia: a case report. Skin Appendage Disord. 2019;5(2):94–96. doi:10.1159/000490469
2. Yesudian P, Thambiah AS. Perinevoid alopecia - an unusual variety of alopecia areata. Arch Dermatol. 1976;112(10):1432–1434. doi:10.1001/archderm.112.10.1432
3. Kimura H, Nagase K, Narisawa Y. Perinevoid alopecia: a case report and literature review. Br J Dermatol. 2018;179(4):969–970. doi:10.1111/bjd.16709
4. Kim SM, Sohng C, Kim JY et al. A Case of perinevoid alopecia on the scalp.Ann Dermatol. 2019;31(2):244–246. doi:10.5021/ad.2019.31.2.244s
5. Heng YK, Ng SK, Tan KB et al . Congenital combined melanocytic nevus of the scalp with associated alopecia areata. Am J Dermatopathol. 2013;35(4):486–488. doi:10.1097/DAD.0b013e318261ea3a
6. Yan H, Zhang J, Yu J et al. A giant compound naevus associated with alopecia: a case report. J Clin Dermatol. 2014;43(05):312–313.
7. Li L, Li Z, Wang Y et al . Alopecia areata around a nevus: a case report. Chin J Dermatol. 2009;42(11):800.
8. Ma X, Cai L, Zhang J. A congenital pigmented nevus associated with alopecia areata: a case report. Chin J Dermatol. 2011;40(03):158.
9. Machado JLR, Cortez de Almeida RF, Frattini SC, et al. Perinevoid alopecia: an unusual presentation of alopecia areata. Dermatol Pract Conce. 2022;12(3):e2022112. doi:10.5826/dpc.1203a112
10. Pu X, Shi D et al. Alopecia areata around the pigmented nevus: two cases. Chin J Dermatovenereol. 1999;3:46.
11. Takeichi S, Kubo Y, Murao K et al . Coexistence of giant blue nevus of the scalp with hair loss and alopecia areata. J Dermatol. 2011;38(4):377–381. doi:10.1111/j.1346-8138.2010.01020.x
12. Zhou C, Li X, Wang C et al. Alopecia areata: an update on etiopathogenesis, diagnosis, and management. Clin Rev Allergy Immunol. 2021;61(3):403–423. doi:10.1007/s12016-021-08883-0
13. Strazzulla LC, Wang EHC, Avila L et al . Alopecia areata: Disease characteristics, clinical evaluation, and new perspectives on pathogenesis. J Am Acad Dermatol. 2018;78(1):1–12. doi:10.1016/j.jaad.2017.04.1141
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.