Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Perifollicular Lymphocytic Inflammation and Fibrosis in Dissecting Cellulitis: Evidence of a Consistent Histopathologic Pattern
Authors Umar S ![]() , Ogah O, Yang J, Tan BH
, Ogah O, Yang J, Tan BH ![]() , Aiead N, Shitabata PK
, Aiead N, Shitabata PK ![]()
Received 15 April 2026
Accepted for publication 8 July 2026
Published 17 July 2026 Volume 2026:19 614816
DOI https://doi.org/10.2147/CCID.S614816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Sanusi Umar,1– 3 Ochanya Ogah,4 Jason Yang,2 Belinda H Tan,5 Nancy Aiead,3 Paul K Shitabata1,2,6
1Department of Medicine, University of California at Los Angeles, Los Angeles, CA, USA; 2Division of Dermatology, Department of Medicine, Harbor-UCLA Medical Center, Torrance, CA, USA; 3Dr. U Hair and Skin Clinic, Manhattan Beach, CA, USA; 4Division of Pediatric Dermatology, Department of Dermatology, Stanford University School of Medicine, Stanford, CA, USA; 5People Science Inc., Los Angeles, CA, USA; 6Dermatopathology Institute, Torrance, CA, USA
Correspondence: Sanusi Umar, Dr. U Hair and Skin Clinic, 2121 N. Sepulveda Avenue, Suite 200, Manhattan Beach, CA, 90266, USA, Tel +1-310-318-1500, Fax +1-310-318-1590, Email [email protected]
Purpose: Dissecting cellulitis of the scalp (DCS) is a chronic, relapsing, suppurative primary cicatricial alopecia. Perifollicular infundibulo-isthmic lymphocytic inflammation and fibrosis (PIILIF) occurs in clinically normal-appearing scalp (cNAS) in other primary cicatricial alopecias but has not been systematically evaluated in DCS.
Patients and Methods: In this retrospective exploratory study, we reviewed consecutive patients with clinicopathologically concordant DCS evaluated at a single Los Angeles dermatology clinic from December 2022 to November 2024. Patients underwent trichoscopy-guided 6-mm punch biopsy of cNAS and a second biopsy of an active lesion or inactive nodule. Specimens were processed with vertical and transverse sections and independently reviewed by two blinded board-certified dermatopathologists. CD4, CD8, CD117, and, when needed, α-smooth muscle actin immunostaining supported characterization. Exact tests with false-discovery-rate adjustment were exploratory.
Results: Twelve men were included (mean age, 30 years; range, 21– 46 years). PIILIF was identified in all cNAS biopsies (12/12; 100%; exact 95% CI, 73.5– 100%) and all inactive nodules (3/3). Active lesions (9/9) showed suppurative inflammation and remodeling superimposed on PIILIF (infundibulo-isthmic fibrosis, 9/9; lymphocytes, 8/9), with increased neutrophilic infiltrates (9/9 vs 0/9 in matched cNAS; adjusted P< 0.001), granulation tissue (5/9 vs 0/9; adjusted P=0.035), and complete sebaceous gland loss (6/9 vs 0/9; adjusted P=0.012). Infiltrates were CD4-predominant with prominent CD117-positive mast cells. PIILIF was observed in a sideburn biopsy in one patient, and 3 patients (25%) had concurrent histologic acne keloidalis nuchae.
Conclusion: In this small cohort, PIILIF was consistently observed in cNAS and inactive nodules from patients with DCS, while active lesions showed additional suppurative destruction. These findings support the hypothesis that PIILIF may represent a subclinical histopathologic component of DCS. Prospective controlled studies are needed to determine specificity, temporal sequence, and prognostic significance.
Keywords: dissecting cellulitis, cicatricial alopecia, primary cicatricial alopecia, scarring alopecia, perifollicular inflammation, trichoscopy
Introduction
Dissecting cellulitis of the scalp (DCS), also termed perifolliculitis capitis abscedens et suffodiens, is an uncommon, chronic, relapsing suppurative primary cicatricial alopecia (PCA) that results in sinus tracts and scarring alopecia.1–4 Although traditionally categorized among neutrophilic PCAs, many patients experience recurrent flares despite antibiotics, oral retinoids, intralesional corticosteroids, and biologics, suggesting that the histopathologic drivers of relapse and extension remain incompletely addressed.2,3
Published DCS studies have emphasized follicular occlusion, follicular rupture, abscess formation, sinus tracts, granulation tissue, and scarring.2–4 These features define active destructive disease, but they do not fully explain why flares recur, why disease extends into adjacent scalp, or why clinically quiet nodules may later reactivate.
Across multiple PCAs, increasing evidence indicates that a low-grade lymphocytic perifollicular process can be present beyond the clinically obvious disease margin. Perifollicular infundibulo-isthmic lymphocytic inflammation and fibrosis (PIILIF) has been reported in clinically normal-appearing scalp (cNAS) in acne keloidalis nuchae (AKN), central centrifugal cicatricial alopecia (CCCA), lichen planopilaris (LPP), frontal fibrosing alopecia (FFA), and folliculitis decalvans (FD), among others.5–11 These studies support a field-effect hypothesis in which upper-follicle immune inflammation and early fibrosis may be present beyond clinically inflamed or scarred skin.
The present study differs from our prior PIILIF work by focusing specifically on DCS and by examining paired cNAS and lesional biopsies across active and clinically inactive DCS states. Whether a similar subclinical PIILIF pattern is present in DCS, and whether it differs across cNAS, clinically inactive nodules, and active lesions, has not been systematically evaluated.
If present, PIILIF in cNAS could help explain (1) extension of disease beyond clinically inflamed nodules, (2) relapse after apparent clinical quiescence, and (3) overlap with other folliculocentric scarring disorders.5,12 In this clinicopathologic study, we evaluated paired biopsies from cNAS and lesional scalp across clinical stages of DCS and characterized associated immune and adnexal features. We hypothesized that PIILIF is present in cNAS of patients with DCS and may represent a subclinical histopathologic substrate associated with DCS.
Patients and Methods
Study Design and Ethics
This retrospective clinicopathologic study included consecutive patients evaluated for DCS in a single dermatology clinic (Los Angeles, California) from December 2022 through November 2024. The Western Institutional Review Board (WIRB) Copernicus Group (WCG IRB Work Order #1-1775045-1) granted exemption from full review because the analysis used deidentified data from routine clinical care with no intent to re-identify or contact participants. All patients provided written informed consent, including permission to use and publish anonymized clinical photographs. The study followed the Declaration of Helsinki (1964) and its later amendments.
Analyses were performed retrospectively on deidentified clinical and histopathology data from routine care. Trichoscopy and biopsies were performed contemporaneously during clinical evaluation; no procedures were performed prospectively for research, and endpoints and follow-up intervals were not prespecified.
No formal sample-size calculation was performed. The sample comprised all consecutive eligible patients who underwent the protocolized biopsy approach during the study interval; analyses were exploratory.
Study Population
Patients were eligible if they had a clinical diagnosis of DCS (Figure 1A and B) supported by characteristic clinicopathologic findings (eg, suppurative folliculitis with follicular rupture, abscess formation and/or granulation tissue, and scarring) and underwent protocolized biopsies of both cNAS and lesional scalp Patients were excluded if biopsy specimens were inadequate for assessment of the upper follicle and surrounding dermis.
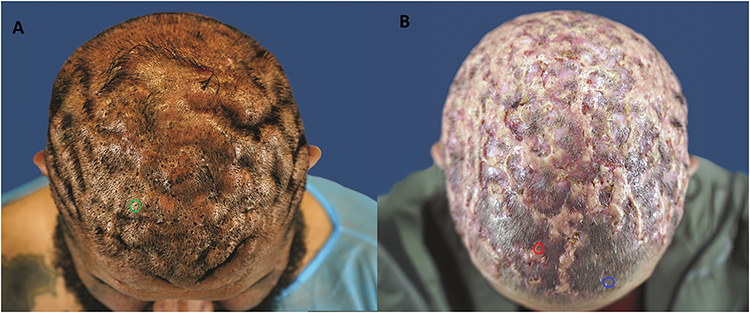 |
Figure 1 Clinical overview photographs showing representative active and clinically inactive DCS lesions and the typical cNAS trichoscopy/biopsy target zone. (A) Top-down view of a patient with DCS showing multifocal indurated nodules and scalp folds of cutis verticis gyrata. The green circle identifies a representative clinically inactive DCS lesion, defined as an uninflamed indurated residual nodule. (B) Top-down view of a second patient with advanced DCS showing confluent inflammatory plaques, crusting, and scarring alopecia. The red circle identifies a representative active DCS lesion, defined clinically by visible inflammation. The blue circle identifies a representative cNAS trichoscopy/biopsy target zone in uninvolved-appearing scalp, approximately 2–3 cm from the nearest clinically evident lesion. Abbreviations: cNAS, clinically normal-appearing scalp; DCS, dissecting cellulitis of the scalp; CVG, cutis verticis gyrata. |
Biopsies were performed during routine clinical evaluation. Prior treatment exposure before biopsy was extracted from the medical record and was heterogeneous; treatment timing was not standardized because the study was retrospective.
Clinical Definitions
cNAS was defined as scalp skin without visible nodules, pustules, sinus tracts, or alopecia on inspection and palpation at the time of biopsy. Lesions were classified as active when associated with erythema, tenderness, drainage, or fluctuance, and as clinically inactive when presenting as residual indurated nodules without signs of active inflammation. Representative spatial relationships among active lesions, clinically inactive lesions, and the cNAS target zone are illustrated in Figure 1, while the trichoscopic appearance used for cNAS biopsy targeting is shown in Figure 2.
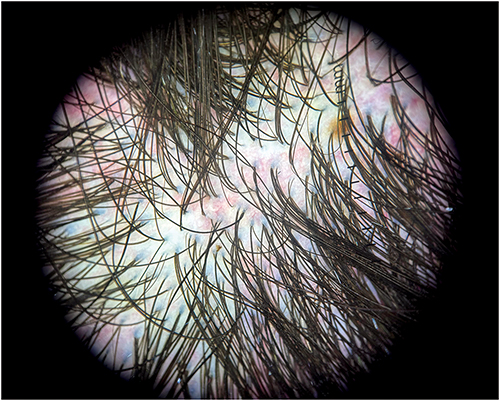 |
Figure 2 Representative trichoscopic appearance of cNAS used for biopsy targeting in a patient with DCS. Trichoscopy of cNAS demonstrated subtle perifollicular abnormalities, including mild perifollicular erythema/hyperpigmentation and/or scale, which were used to guide biopsy site selection. Abbreviations: cNAS, clinically normal-appearing scalp; DCS, dissecting cellulitis of the scalp. |
Biopsy Protocol and Processing
All patients underwent a 6-mm punch biopsy from cNAS, typically in the parietal scalp, approximately 2–3 cm from clinically evident lesions. A second 6-mm punch biopsy targeted either an active DCS lesion (when present) or a clinically inactive nodule (when active lesions were absent). The paired cNAS and lesional biopsies were obtained from the same scalp during the same clinical evaluation. Specimens were processed with both vertical and transverse sections to optimize visualization of perifollicular inflammation and fibrosis.13,14
Histopathologic Assessment
Two board-certified dermatopathologists independently reviewed all slides while blinded to clinical information, sampling site, clinical activity status, and treatment history. Discrepancies were resolved by consensus, and the consensus diagnosis was used for analysis.
PIILIF was defined as a perifollicular lymphocytic infiltrate centered on the infundibulum and/or isthmus with associated perifollicular lamellar fibroplasia or early concentric fibrosis, in the absence of an alternative diagnostic pattern such as interface dermatitis involving the interfollicular epidermis. Fibrosis was recorded as present or absent rather than graded semiquantitatively because no validated DCS-specific grading scale for subtle upper-follicle fibrosis was used in this retrospective study. For active lesions, additional features assessed included neutrophilic infiltrates, granulation tissue, follicular rupture, sinus tract formation, and sebaceous gland status. When perifollicular fibrosis was equivocal on hematoxylin and eosin, α-smooth muscle actin (α-SMA) was used to highlight early myofibroblast-rich stromal remodeling.15
Immunohistochemistry
CD4 and CD8 immunostaining was used to characterize T-cell subsets and report relative predominance (CD4>CD8 vs CD8≥CD4). CD117 immunostaining was used to support mast cell identification. Immunohistochemistry was performed on all specimens with sufficient remaining tissue (see Results). Cases without sufficient residual tissue were excluded from immunohistochemistry-only analyses, and denominators are reported for each immunohistochemistry comparison.
Statistical Analysis
For the subset of patients with paired active lesion and cNAS biopsies, categorical histopathologic variables were compared using exact tests. False-discovery rate was controlled using the Benjamini-Hochberg procedure. Exact binomial 95% confidence intervals were calculated for the primary prevalence estimate. Clinically inactive nodules were summarized descriptively because only 3 patients had inactive nodules; formal hypothesis testing in that subgroup would be unstable and potentially misleading. Analyses were performed using R (R Foundation for Statistical Computing). All analyses were exploratory, and nonsignificant comparisons should not be interpreted as equivalence.
Results
Patient Characteristics
Baseline demographic and clinical characteristics are summarized in Table 1. Briefly, the cohort included 12 men (mean age, 30 years; range, 21–46 years). Most patients underwent lesional biopsy during clinically active DCS (9/12), while 3/12 had no active lesions at the time of biopsy but reported prior recurrent episodes of painful, draining nodules with progressive hair loss. Comorbid acne vulgaris was common and hidradenitis suppurativa occurred in a minority (Table 1). Notably, 3/12 (25%) had previously been treated for presumed seborrheic dermatitis, yet none of the study biopsies showed histopathologic features of seborrheic dermatitis. Treatment exposure before biopsy was heterogeneous and is detailed in Table 1, with corticosteroids and oral retinoids most frequently reported and antibiotics or tumor necrosis factor inhibition less common. Because exposures were heterogeneous and the cohort was small, no treatment-specific histopathologic inference was made.
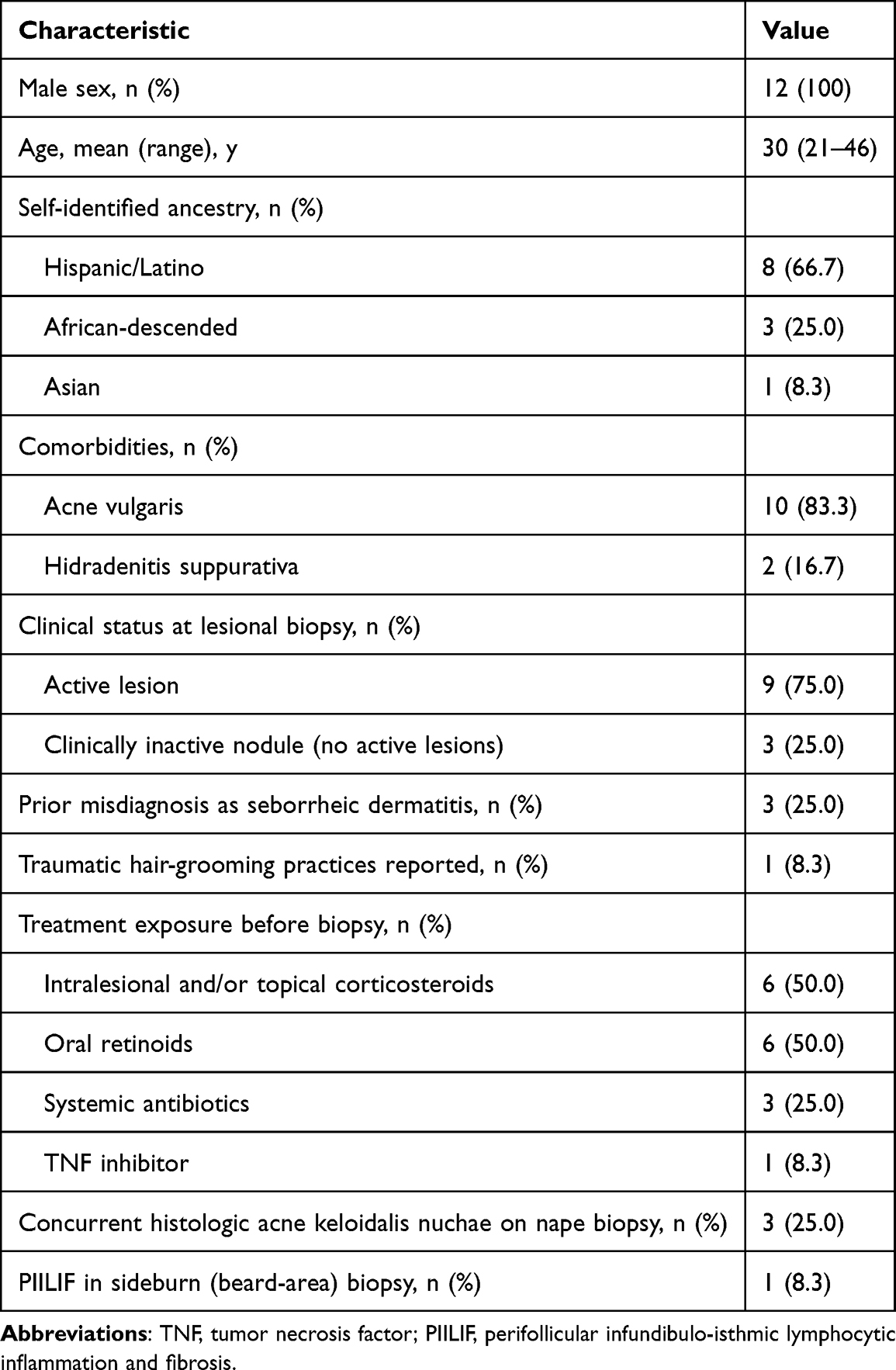 |
Table 1 Patient Characteristics (N=12) |
Histopathology of cNAS and Clinically Inactive Nodules
PIILIF was identified in all cNAS biopsies (12/12; 100%; exact 95% CI, 73.5–100%) and all clinically inactive nodules (3/3). Representative transverse sections from a cNAS biopsy demonstrating PIILIF are shown in Figure 3. In clinically inactive nodules, PIILIF mirrored cNAS, including preservation of sebaceous glands and absence of the destructive suppurative features seen in active disease. Because only 3 patients had clinically inactive nodules, these specimens were summarized descriptively rather than included in formal hypothesis testing.
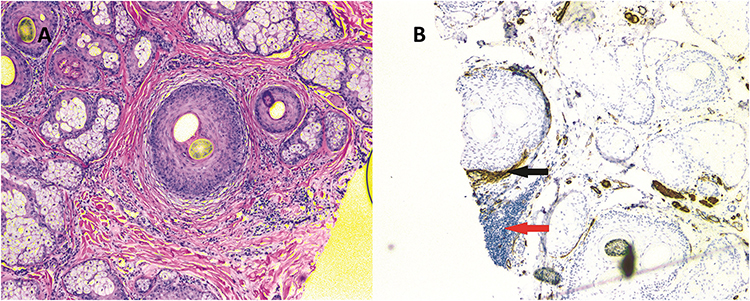 |
Figure 3 Representative cNAS histology from a patient with DCS. Hematoxylin and eosin (A) and/or α-SMA-stained (B) vertical and transverse sections demonstrate perifollicular lymphocytic inflammation centered on the infundibulo-isthmic region with associated perifollicular fibrosis. Magnification x4. Abbreviations: cNAS, clinically normal-appearing scalp; DCS, dissecting cellulitis of the scalp; α-SMA, alpha-smooth muscle actin. |
Histopathology of Active Lesions
Among 9 active DCS lesions, prominent neutrophilic inflammation and tissue remodeling were superimposed on a PIILIF background (Figure 4 and Table 2). Compared with matched cNAS biopsies from the same patients (n=9 pairs), active lesions demonstrated increased neutrophilic infiltrates (9/9 vs 0/9; adjusted P<0.001), granulation tissue (5/9 vs 0/9; adjusted P=0.035), and complete sebaceous gland loss (6/9 vs 0/9; adjusted P=0.012). In contrast, most upper-follicle PIILIF features were shared between active lesions and cNAS (infundibulo-isthmic fibrosis, 9/9 vs 9/9; infundibulo-isthmic lymphocytes, 8/9 vs 9/9).
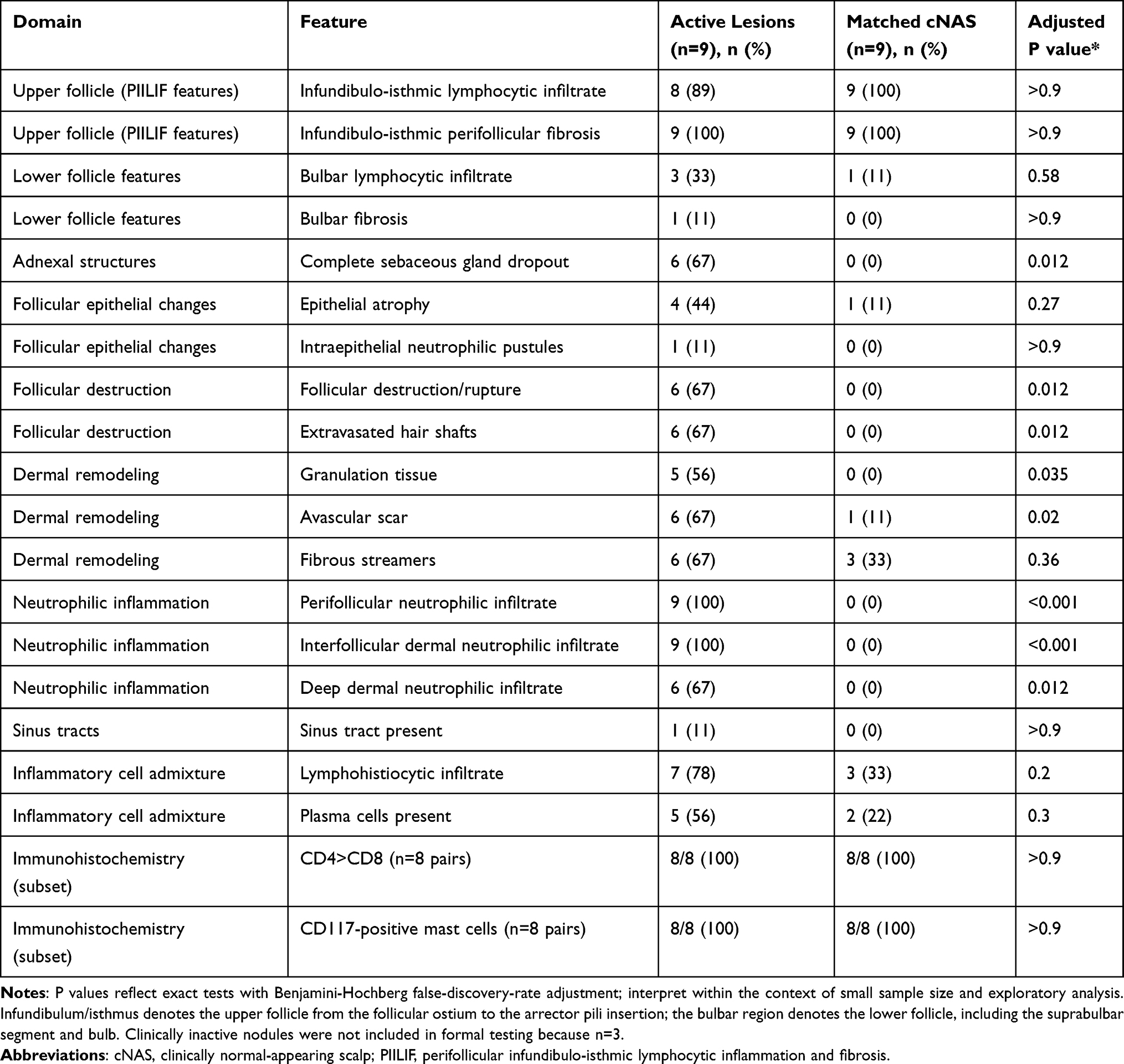 |
Table 2 Histopathologic Features in Active DCS Lesions vs Matched Clinically Normal-Appearing Scalp (cNAS) (n=9 Pairs) |
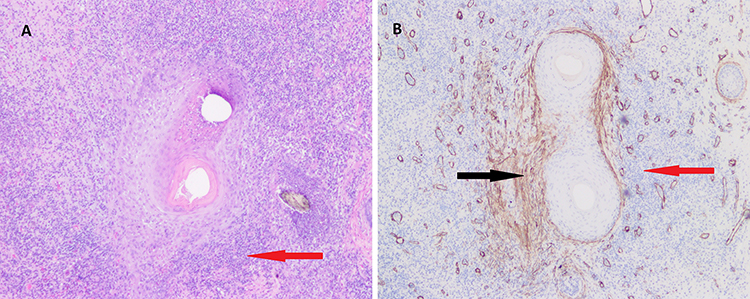 |
Figure 4 Hematoxylin and eosin stain (A) and α-SMA stain (B) of a transverse section from an active DCS lesion from the patient in Figure 3 showing mixed perifollicular inflammation with neutrophilic predominance and associated infundibulo-isthmic lymphocytes (red arrow) with perifollicular fibrosis (black arrow). Magnification x4. Abbreviations: α-SMA, alpha-smooth muscle actin; DCS, dissecting cellulitis of the scalp. |
Immunophenotype
Immunohistochemistry was evaluable in 8 active lesion/cNAS pairs. Across disease stages, infiltrates were consistently CD4-predominant (CD4>CD8) and CD117-positive mast cells were prominent (Figure 5, Table 2 and Supplementary Table S1).
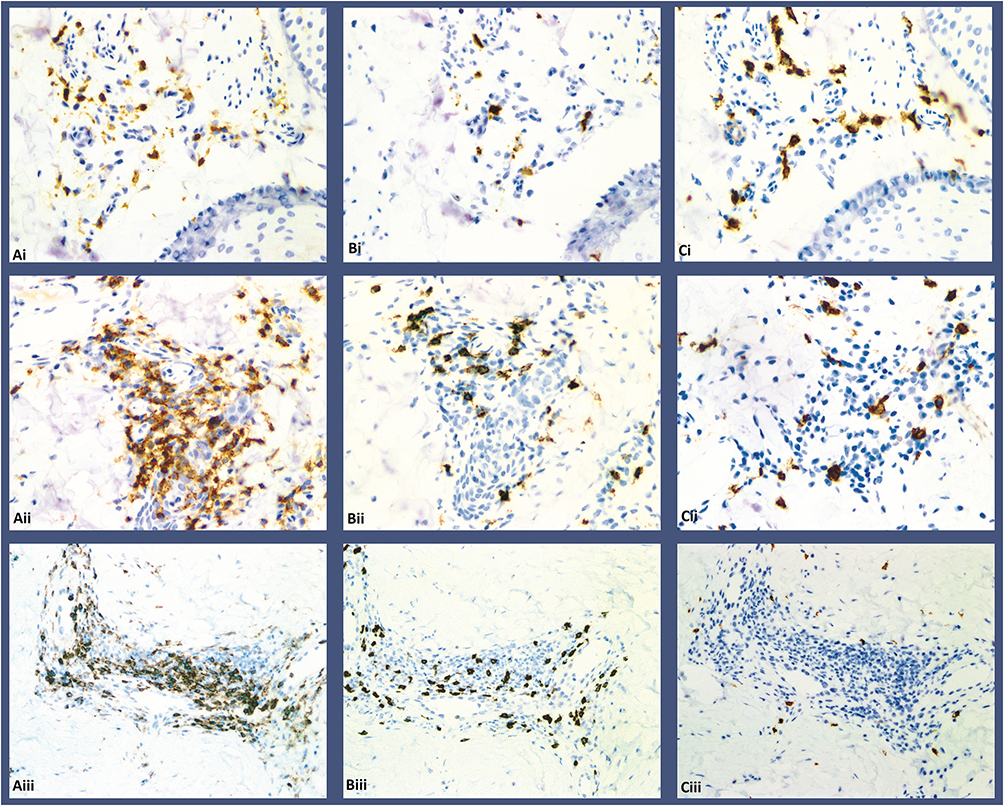 |
Figure 5 Immunohistochemistry from a single patient with DCS and AKN demonstrating CD4 (A column), CD8 (B column), and CD117 (C column) staining in cNAS PIILIF (Ai-Ci), active DCS lesion (Aii-Cii), and AKN lesion (Aiii-Ciii). Abbreviations: AKN, acne keloidalis nuchae; cNAS, clinically normal-appearing scalp; DCS, dissecting cellulitis of the scalp; PIILIF, perifollicular infundibulo-isthmic lymphocytic inflammation and fibrosis. |
Extension Beyond the Scalp and Overlapping Folliculocentric Disease
PIILIF was identified in a sideburn (beard-area) biopsy in one patient. In addition, 3 patients (25.0%) had nape biopsies diagnostic of acne keloidalis nuchae (AKN), suggesting overlapping pathology within the same individuals (Figure 5).
Discussion
In this small retrospective, exploratory clinicopathologic study, PIILIF was observed in all cNAS biopsies and clinically inactive nodules from patients with DCS, while active lesions showed destructive suppurative inflammation and adnexal loss superimposed on this upper-follicle lymphocytic-fibrotic pattern. These observations support a field-effect hypothesis in DCS that parallels reports in other PCAs, in which upper-follicle immune inflammation and early scarring may extend beyond the clinically obvious disease margin.5–11 Because this cohort was small and lacked healthy controls, these findings should not be interpreted as evidence that PIILIF is universal or specific to all DCS cases.
Prior DCS histopathology has emphasized destructive suppurative folliculitis, follicular rupture, abscess formation, sinus tracts, granulation tissue, and scarring.2–4 Our paired-biopsy approach complements that literature by showing that active DCS features may coexist with, or be superimposed on, an upper-follicle lymphocytic-fibrotic pattern detectable outside clinically active lesions.
A key conceptual implication is that DCS may not be confined to clinically inflamed nodules but may instead include a wider low-grade inflammatory field that can coexist with episodic neutrophil-dominant flares. This interpretation is associative rather than causal. The cross-sectional design cannot determine whether PIILIF precedes, follows, or persists after active DCS lesions. Notably, prior studies in LPP, FFA, AKN, FD and CCCA found that histopathologic activity in clinically unaffected scalp may occur without clear correlation to symptoms or visible inflammation.5–11
Why can PIILIF exist in cNAS without overt alopecia? We interpret PIILIF as a low-grade or smoldering folliculocentric process centered on the infundibulum and isthmus. At this stage, follicular cycling may remain largely preserved and clinical hair density may appear normal, particularly when inflammation is patchy or below a destructive threshold. A transition to clinically evident scarring likely requires additional events such as follicular rupture, intense neutrophilic recruitment, and sustained dermal remodeling, which were prominent in active lesions in our cohort.
Clinically inactive nodules in our cohort retained PIILIF with preserved sebaceous glands and without the destructive suppurative features of active lesions. This finding can be interpreted in more than one way. Clinically inactive nodules may represent partially treated or spontaneously improved lesions, an earlier-stage component of a clinically larger lesion, or a sampling point that missed a destructive focus. Although our cross-sectional design cannot determine temporal directionality, the separation of sebaceous gland preservation in cNAS and clinically inactive nodules from dropout in active lesions raises the hypothesis that sebaceous gland loss may mark a transition point toward less reversible disease, akin to observations in LPP studies.16
Diagnostic implications include the risk of misattribution of subtle perifollicular erythema and scale in cNAS to seborrheic dermatitis. In this cohort, several patients had previously been managed as seborrheic dermatitis; however, none of the study biopsies showed histopathologic features supportive of seborrheic dermatitis. Nevertheless, because many patients use antifungal shampoos or topical corticosteroids prior to referral, we cannot exclude partial treatment effects that might attenuate seborrheic dermatitis features. Alternative explanations, including nonspecific perifollicular inflammation or treatment-related modification of disease expression, cannot be excluded. These observations support a low threshold for biopsy when perifollicular changes are persistent or when symptoms and clinical course are discordant with a diagnosis of seborrheic dermatitis.
Accurate recognition of PIILIF requires adequate follicular sampling and review of both vertical and transverse sections. Vertical sections best assess infundibulo-isthmic lymphocytic inflammation, whereas transverse sections improve detection of concentric perifollicular fibrosis and adnexal dropout.13,14 Because the change may be confined to a narrow perifollicular rim, detection is plane dependent and false negatives occur when only one plane is examined or the transverse level misses the peripilar collar. When fibrosis is subtle on hematoxylin and eosin, α-SMA can highlight early perifollicular myofibroblast activity consistent with incipient fibrosis and epithelial-mesenchymal transition.15 However, α-SMA cannot eliminate under-calling because fibrosis may still be missed if sections pass above or below the affected zone. Accordingly, an infundibulo-isthmic perifollicular lymphocytic infiltrate should raise suspicion for early fibrosis even when fibrosis is not demonstrable on available H&E or α-SMA sections.
We also observed overlapping pathology with AKN in 25% of patients. AKN is itself a PCA with upper-follicle lymphocytic inflammation and early fibrosis described in clinically non-alopecic scalp.5,11 The co-occurrence of DCS and AKN in the same individuals (Figure 5) supports the possibility of shared folliculocentric immune pathways and warrants consideration of broader pan-follicular susceptibility in some patients.
Hypothesis-generating framework. Addressing PIILIF may help mitigate progression in DCS, but this study did not directly test therapeutic or molecular mechanisms. DCS predominantly affects men, most commonly in early adulthood, and an androgenic contribution has been proposed based on epidemiologic patterns and clinical observations of disease onset or exacerbation in the setting of exogenous androgen exposure.5,17,18 One working hypothesis is that a chronic upper-follicle lymphocytic-fibrotic pattern can coexist with episodic neutrophilic activation in DCS. This is biologically plausible because dihydrotestosterone can upregulate IL-6 in follicular dermal papilla cells, IL-6 participates in inflammatory amplification and fibrotic wound-healing programs, CXCL8/IL-8 recruits neutrophils, mast cells can contribute to fibrotic remodeling, and Cutibacterium acnes may amplify TLR/NF-κB signaling.19–23 These pathways were not measured in this study and should be viewed as a framework for future mechanistic work, not as conclusions from the present data. Consistent with the possibility that PIILIF can be hormonally and immunologically modulated, PIILIF has been described as an inflammatory endotype in androgenetic alopecia, including beard and eyebrow sites, with improved outcomes reported when treatment addressed both dihydrotestosterone signaling and inflammation.24
This study has limitations. The sample size was small and derived from a single specialty clinic, introducing potential referral and spectrum bias. The study was retrospective and cross-sectional; therefore, it cannot establish whether PIILIF temporally precedes the onset of clinically apparent DCS lesions or predicts relapse. Treatment exposures before biopsy were heterogeneous and may have modified histopathologic features. The study was underpowered for treatment-stratified or subgroup analyses, including clinically inactive nodules. Histopathologic variables were recorded categorically, so quantitative inflammatory burden and fibrosis severity could not be assessed. Interobserver agreement statistics were not prespecified; instead, final interpretation was based on independent blinded review followed by consensus.
We did not include healthy control scalp biopsies; therefore, specificity for DCS cannot be established. Prior studies in other PCA contexts have reported absent or substantially lower similar changes in control scalp, but prospective controlled DCS studies are needed. These limitations should temper prevalence estimates, particularly the 100% cNAS finding in this small cohort.
Future work should include prospective, longitudinal studies with standardized clinical scoring and paired serial biopsies to determine whether PIILIF in cNAS predicts lesion development, extension, or relapse. Larger controlled studies should include healthy controls or disease controls, prespecified quantitative histopathologic scoring, interobserver reliability analysis, and spatial immune phenotyping. Mechanistic studies integrating microbiome profiling, cytokine signatures, and spatial immune phenotyping across cNAS, inactive nodules, and active lesions could clarify the pathways that govern transition from PIILIF to suppurative destruction. Interventional trials are required to determine whether targeting the PIILIF stage, in addition to suppressing neutrophilic flares, prevents irreversible follicular loss.
Conclusion
PIILIF was consistently observed in this cohort of patients with DCS and may represent a subclinical histopathologic component of disease. Active lesions showed additional neutrophilic inflammation, granulation tissue, and sebaceous gland dropout superimposed on this pattern. Recognizing PIILIF in DCS may refine diagnostic evaluation, but the present findings demonstrate association rather than temporal sequence. Prospective controlled studies are needed to determine whether PIILIF predicts disease progression, extension, relapse, or treatment response.
Abbreviations
AKN, acne keloidalis nuchae; α-SMA, alpha-smooth muscle actin; cNAS, clinically normal-appearing scalp; CCCA, central centrifugal cicatricial alopecia; CD, cluster of differentiation; CI, confidence interval; CVG, cutis verticis gyrata; DCS, dissecting cellulitis of the scalp; DHT, dihydrotestosterone; FD, folliculitis decalvans; FDR, false-discovery rate; FFA, frontal fibrosing alopecia; H&E, hematoxylin and eosin; IHC, immunohistochemistry; IL, interleukin; IRB, institutional review board; LPP, lichen planopilaris; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; PCA, primary cicatricial alopecia; PIILIF, perifollicular infundibulo-isthmic lymphocytic inflammation and fibrosis; TGF-β, transforming growth factor beta; TNF, tumor necrosis factor; WIRB, Western Institutional Review Board.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request, subject to institutional requirements and privacy considerations.
Ethics Approval and Informed Consent
This study was granted exemption from full review by the Western Institutional Review Board (WIRB) Copernicus Group (WCG IRB Work Order #1-1775045-1), as it involved retrospective analysis of deidentified data from routine clinical procedures, with no plans for re-identification or patient contact. All patients provided written informed consent, including consent for the use and publication of anonymized clinical photographs. The study was conducted in accordance with the Declaration of Helsinki (1964) and its later amendments.
Acknowledgments
We thank Ms Hadeel Sherif for the statistical analysis. We are particularly grateful to our patients for participating in the study and our clinical and laboratory staff involved in specimen processing and patient care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding or sponsorship was received for this study.
Disclosure
Dr. Umar owns shares and patent applications in FineTouch Laboratories Inc., shares, patents, and patent applications in Dr. U Devices Inc. and reports no other potential conflicts of interest for this work. Ms Aiead, Drs. Ogah, Yang, Tan, and Shitabata declare no conflicts of interest in this work. The disclosed commercial and patent-related interests did not influence dermatopathologic review, which was performed independently and blinded to clinical information, or the statistical interpretation of the data.
References
1. Olsen EA, Bergfeld WF, Cotsarelis G, et al. Summary of North American Hair Research Society (NAHRS)-sponsored workshop on cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48(1):103–11. doi:10.1067/mjd.2003.68
2. Masson R, Hawkins S, Shapiro J, et al. Treatments for dissecting cellulitis of the scalp: a systematic review and treatment algorithm. Dermatol Ther. 2023;13(11):2487–2526. doi:10.1007/s13555-023-01018-7
3. Guo W, Willis A, Mueller A, et al. Analyzing the efficacy of isotretinoin in treating dissecting cellulitis: a literature review and meta-analysis. Drugs R D. 2021;21(1):29–37. doi:10.1007/s40268-020-00335-y
4. Ehsani AH, Yolme H, Akhavan Sabagh M, et al. Demographic and histopathological evaluation in 71 patients diagnosed with dissecting cellulitis of the scalp. Dermatol Ther. 2023;2023:2959140. doi:10.1155/2023/2959140
5. Umar S, Ton D, Carter MJ, Shitabata PK. Unveiling a shared precursor condition for acne keloidalis nuchae and primary cicatricial alopecias. Clin Cosmet Invest Dermatol. 2023;16:2315–2327. doi:10.2147/CCID.S422310
6. Felix K, De Souza B, Portilla N, et al. Dermatoscopic evaluation of central centrifugal cicatricial alopecia beyond the vertex scalp. JAMA Dermatol. 2020;156(8):916–918. doi:10.1001/jamadermatol.2020.1287
7. Doche I, Romiti R, Hordinsky MK, Valente NS. “Normal-appearing” scalp areas are also affected in lichen planopilaris and frontal fibrosing alopecia: an observational histopathologic study of 40 patients. Exp Dermatol. 2020;29(3):278–281. doi:10.1111/exd.13834
8. Pindado-Ortega C, Perna C, Saceda-Corralo D, et al. Frontal fibrosing alopecia: histopathological, immunohistochemical and hormonal study of clinically unaffected scalp areas. J Eur Acad Dermatol Venereol. 2020;34(2):e84–e85. doi:10.1111/jdv.15977
9. Porriño-Bustamante ML, Pinedo-Moraleda F, Fernández-Flores A, et al. Frontal fibrosing alopecia: a histopathological comparison of the frontal hairline with normal-appearing scalp. J Clin Med. 2022;11(14):4121. doi:10.3390/jcm11144121
10. Doche I, Hordinsky MK, Valente NS, Sotto MN. Evidence for lymphocytic inflammation in non-lesional scalp of folliculitis decalvans: an observational study of 25 patients. J Eur Acad Dermatol Venereol. 2022;36(2):e109–e111. doi:10.1111/jdv.17649
11. Sperling LC, Homoky C, Pratt L, Sau P. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136(4):479–484. doi:10.1001/archderm.136.4.479
12. Turegano MM, Sperling LC. Lichenoid folliculitis: a unifying concept. J Cutan Pathol. 2017;44(7):647–654. doi:10.1111/cup.12938
13. Ozcan D, Özen Ö, Seçkin D, et al. Vertical vs. transverse sections of scalp biopsy specimens: a pilot study on the comparison of the diagnostic value of two techniques in alopecia. Clin Exp Dermatol. 2011;36(8):843–849. doi:10.1111/j.1365-2230.2011.04154.x
14. Gurusamy U, Venkataswamy C, Sivaraman A. Evaluation of alopecia: a new processing technique combining vertical and transverse sections from a single scalp biopsy specimen. International Journal of Trichology. 2018;10(1):11–16. doi:10.4103/ijt.ijt_66_17
15. Ding H, Chen J, Qin J, Chen R, Yi Z. TGF-β-induced α-SMA expression is mediated by C/EBPβ acetylation in human alveolar epithelial cells. Mol Med. 2021;27(1):22. doi:10.1186/s10020-021-00283-6
16. Kamyab Hesari K, Ghanadan A, Azhari V, et al. Lichen planopilaris: histopathological survey of 70 vertical sections of scalp biopsies. Iran J Dermatol. 2022;25(1):24–28. doi:10.22034/ijd.2021.267246.1304
17. Cuellar TA, Roh DS, Sampson CE. Dissecting cellulitis of the scalp: a review and case studies of surgical reconstruction. Plast Reconstr Surg Glob Open. 2020;8(8):e3015. doi:10.1097/GOX.0000000000003015
18. Rodrigues Machado JL, Domingos Almeida M, Cortez de Almeida RF, Fernandes Melo D. Dissecting cellulitis associated with hormone therapy in a transgender man. Actas Dermosifiliogr. 2026;117(4):104555. doi:10.1016/j.ad.2025.104555
19. Kwack MH, Ahn JS, Kim MK, Kim JC, Sung YK. Dihydrotestosterone-inducible IL-6 inhibits elongation of human hair shafts by suppressing matrix cell proliferation and promotes regression of hair follicles in mice. J Invest Dermatol. 2012;132(1):43–49. doi:10.1038/jid.2011.274
20. Johnson BZ, Stevenson AW, Prêle CM, Fear MW, Wood FM. The role of IL-6 in skin fibrosis and cutaneous wound healing. Biomedicines. 2020;8(5):101. doi:10.3390/biomedicines8050101
21. Cambier S, Gouwy M, Proost P. The chemokines CXCL8 and CXCL12: molecular and functional properties, role in disease and efforts towards pharmacological intervention. Cell Mol Immunol. 2023;20(3):217–251. doi:10.1038/s41423-023-00974-6
22. Conti P, Caraffa A, Mastrangelo F, et al. Critical role of inflammatory mast cell in fibrosis: potential therapeutic effect of IL-37. Cell Prolif. 2018;51(5):e12475. doi:10.1111/cpr.12475
23. Noh HH, Shin SH, Roh YJ, Moon NJ, Seo SJ, Park KY. Particulate matter increases Cutibacterium acnes-induced inflammation in human epidermal keratinocytes via the TLR4/NF-κB pathway. PLoS One. 2022;17(8):e0268595. doi:10.1371/journal.pone.0268595
24. Umar S, Tan BH, Shitabata PK. Perifollicular inflammation and fibrosis in androgenetic alopecia: implications for diagnosis and treatment - A comparative histopathologic and clinical study with normal-appearing scalp. Clin Cosmet Invest Dermatol. 2026;19:548520. doi:10.2147/CCID.S548520
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perifollicular Inflammation and Fibrosis in Androgenetic Alopecia: Implications for Diagnosis and Treatment - A Comparative Histopathologic and Clinical Study with Normal-Appearing Scalp

Umar S, Tan BH, Shitabata PK
Clinical, Cosmetic and Investigational Dermatology 2026, 19:548520
Published Date: 12 January 2026