Back to Journals » Journal of Pain Research » Volume 18
Pericapsular Nerve Group Block for Hip Fracture Pain Management: A Narrative Review of Emergency Applications
Authors Li YB ![]() , Zuo M
, Zuo M ![]() , Zhu JP
, Zhu JP ![]() , Ma RL, Liao XZ
, Ma RL, Liao XZ ![]()
Received 22 March 2025
Accepted for publication 8 September 2025
Published 15 September 2025 Volume 2025:18 Pages 4801—4807
DOI https://doi.org/10.2147/JPR.S528497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Ya-bei Li,1,2,* Man Zuo,3,* Jing-ping Zhu,2 Ri-liang Ma,4 Xiao-zu Liao1,5
1Anesthesiology Major, Guangdong Medical College, Guangzhou, Guangdon, People’s Republic of China; 2Anesthesiology Department, Heyuan People’s Hospital, Heyuan, Guangdong, People’s Republic of China; 3Emergency Department, Anesthesiology Department, Heyuan People’s Hospital, Heyuan, Guangdong, People’s Republic of China; 4Anesthesiology Department, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, People’s Republic of China; 5Anesthesiology Department, Zhongshan People’s Hospital, Zhongshan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-zu Liao, Department of Anesthesiology, Guangdong Medical University, No. 1 Xincheng Avenue, Songshan Lake High-Tech Industrial Development Zone, Dongguan City, Guangdong Province, 523808, People’s Republic of China, Tel +8613450921219, Email [email protected]
Abstract: The pericapsular nerve group (PENG) block is a regional anaesthesia technique for acute pain management that is becoming frequently employed for emergency lower limb fractures, particularly hip injuries. While current evidence has been predominantly derived from postoperative randomized trials and case series, the results of recent clinical reports support the preprocedural utility of the PENG block in emergency settings for rapid analgesia 40– 60% pain score reduction and preservation of motor function. This review synthesizes mechanistic insights and clinical outcomes from the literature, comparing the targeted sensory blockade of the hip capsule with the PENG block with that of systemic opioids (which risks inducing respiratory depression) and fascia iliaca block (which can induce motor impairment). Key advantages of PENG blockade include significant opioid-sparing effects (50– 70% reduction morphine use) and almost no motor complications. Standardized ultrasound-guided protocols can address challenges related to anatomical variability. Preliminary evidence from case reports suggests that the efficacy of the PENG block to pelvic and femoral shaft fractures, although multicentre trials are needed to establish optimal doses and long-term functional outcomes. This evidence indicates that PENG blockade could serve as a promising emergency intervention, but further protocol refinement is warranted.
Keywords: regional anaesthesia techniques, hip fracture management, opioid-sparing analgesia, trauma care, pain control strategies
Corrigendum for this paper has been published.
Introduction
Effective pain control in emergency hip fracture remains a critical challenge, as it requires balancing analgesia against opioid-related complications (respiratory depression, dependency) and delayed mobilization.1–3 While systemic opioids are mainstays in pain control regional techniques such as fascia iliaca compartment blocks (FICBs), particularly the suprainguinal approach for hip fracture, can improve pain control but cause motor weakness in 30–70% of cases, limiting the effects of rehabilitation.4–6
The pericapsular nerve group (PENG) block, introduced by Girón-Arango et al,7 overcomes these limitations through the ultrasound-guided targeting of the sensory nerves innervating the anterior hip capsule (femoral and accessory obturator nerves). Importantly, it does not substantially impair motor function enabling immediate weight-bearing rehabilitation in fragile patients.8 Pooled data from 3 randomized controlled trials involving hip fracture patients demonstrated the superiority of the PENG block over suprainguinal FICB: achieving (1) 40–60% greater pain reduction at 15 min (NRS)and (2) 50–70% lower opioid consumption.9–11 Despite these advantages, the adoption of the PENG block in emergency departments faces challenges including a steep operator learning curves (due to anatomical complexity)12 and protocol heterogeneity.13,14
This review evaluates the role of the PENG block in emergency hip fracture through three objectives:
- To synthesize mechanistic and clinical evidence (focusing on Level I–III studies);
- To analyse implementation barriers using implementation science frameworks;
- To propose standardized ultrasound-guided workflows for trauma teams.
By addressing these objectives, we aim to establish the PENG block as an opioid-sparing cornerstone procedure for hip fractures, with exploratory applications in the management of pelvic trauma.
Anatomy, Mechanism, and Procedure of the PENG Block
Neuroanatomical Basis
The hip joint capsule receives sensory innervation from three primary nerves: the femoral (anterior), obturator (medial), and accessory obturator nerves.15,16 While the sciatic nerve predominantly has motor functions, it also contributes minor sensory fibres to the posterior capsule15–17. The PENG block selectively targets these sensory pathways, sparing motor fibres, a critical distinction from traditional nerve blocks that impair mobility.18,19
Anatomy and Mechanism
The PENG block delivers local anaesthesia near the sensory nerve entry points surrounding the hip capsule under ultrasound guidance (Figures 1 and 2). This approach achieves dual objectives: (1) blockade of nociceptive signalling via sodium channel inhibition; and (2) preservation of motor function by avoiding efferent pathways.20,21 By selectively inhibiting nociceptive pathways, the PENG block preserves motor function, enabling early mobilization which is important for reducing postoperative complications such as deep vein thrombosis.18,22 Ultrasound visualization improves safety by reducing local anaesthetic systemic toxicity (LAST) risk through the real-time vascular identification of key vessels.23
 |
Figure 1 Ultrasound-guided PENG block: Anatomical landmarks. (A) Cross-section at the iliopubic eminence (IPE) showing the muscular/vascular compartments. (B) Transverse view showing the anterior inferior iliac spine (AIIS) with the psoas tendon (PT) and needle trajectory (arrow). (C) Oblique view showing the spread of the anaesthetic (*) between the PT and IPE. Abbreviations: ASIS, anterior superior iliac spine; AIIS, anterior inferior iliac spine; IPE, iliopubic eminence; PT, psoas tendon; IPM, iliopsoas muscle; FA, femoral artery; FV, femoral vein. |
 |
Figure 2 Two ultrasound approaches. Scanning Technique 1 (Curvilinear Probe): (A) Initial placement at the AIIS. (B) Probe rotation (30–45°) to align with the superior pubic ramus (SPR). Scanning Technique 2 (Curvilinear Probe): (C) Transverse placement over the Hip capsule. (D) Cephalad movement to visualize the IPE/AIIS. Abbreviations: AIIS, anterior inferior iliac spine; IPE, iliopubic eminence; SPR, superior pubic ramus. |
Procedural Workflo
The standardized ultrasound-guided protocol involves three key steps:
Landmark Identification
The anterior inferior iliac spine (AIIS) and iliopubic eminence (IPE) are chosen as the primary reference points.
Probe Positioning
A curvilinear probe (5–10 MHz) is aligned to visualize the iliopsoas compartment, including the psoas tendon (PT) and femoral artery (FA).24
Needle Trajectory
The needle is advanced in-plane to administer the anaesthetic between the PT and IPE, ensuring diffusion around the pericapsular nerves (Figure 3).25
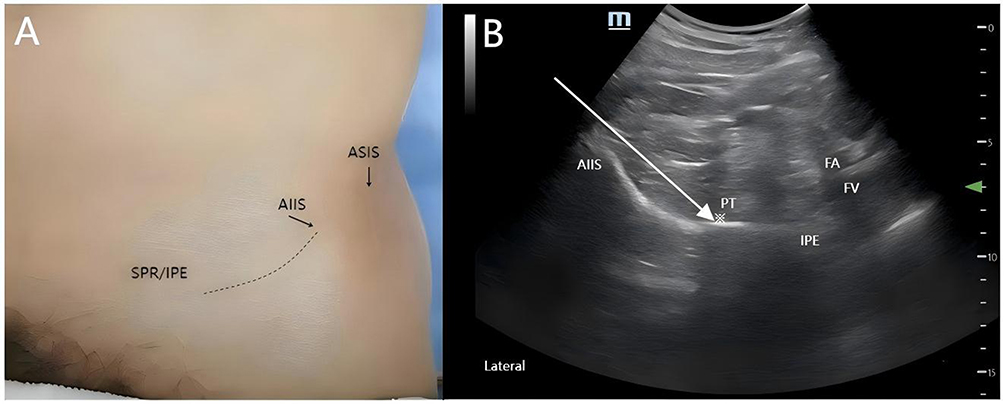 |
Figure 3 PENG blockade in trauma care. (A) Surface landmarks: ASIS, AIIS, IPE, and SPR. (B) Needle trajectory (white arrow) with spread of the anaesthetic (*) near the PT/FA/SPR. Abbreviations: AIIS, anterior inferior iliac spine; ASIS, anterior superior iliac spine; FA, femoral artery; IPE, iliopubic eminence; PT, psoas tendon; SPR, superior pubic ramus. |
Application Scenarios in Trauma Emergency Care
Hip Fractures
In elderly patients, hip fractures often require rapid analgesia to mitigate the risk of delirium associated with the administration of systemic opioids. The PENG block outperforms the suprainguinal fascia iliaca blocks (US-guided) in reducing pain (change in visual analogue scale score (ΔVAS) = 2.26 vs 3.04) and can reduces respiratory complications by 68% in elderly patients with hip fractures patients.26,27
Pelvic Fractures
For pubic ramus fractures, combining the PENG block with femoral lateral cutaneous nerve blockade achieves a 72% reduction in opioid use while preserving quadriceps muscle strength.28 Ultrasound guidance ensures precise anaesthetic delivery to the pelvic ring, addressing both osseous and soft tissue pain sources.29
Polytrauma
In polytrauma patients, the PENG block can be integrated into multimodal analgesia protocols, reducing the length of ICU stays by 1.8 days compared with opioid-centric approaches.9 Its compatibility with other regional techniques (eg, thoracic epidurals) improves systemic analgesia without increasing respiratory risks.30,31
Technical Considerations and Comparative Advantages
Technical Considerations
Accurate needle placement for the PENG block requires ultrasound guidance, typically with a curvilinear probe (5–10 MHz), to visualize the iliopsoas compartment, femoral artery, and psoas tendon. Anatomical variability among patients requires careful adjustment of the needle trajectory. The needle should be inserted in-plane to ensure accurate diffusion of the local anesthetic around the pericapsular nerves, while avoiding motor pathways. A volume of 15–20 mL of 0.375% ropivacaine is commonly used, but care must be taken to avoid over-dosing and systemic toxicity. While ultrasound guidance reduces complication risks, including vascular injury and local anaesthetic systemic toxicity (LAST), practitioners should remain vigilant for complications. The PENG block technique has a steep learning curve, with proficiency requiring approximately 25 cases. Proper patient positioning, such as supine positioning with slight external hip rotation, is crucial for optimal visualization. Experience plays a key role in ensuring high success rates and minimizing complications.
Comparative Advantages
95% success rate, outperforming ultrasound-guided FICB (85%).
Limitations
Learning curve (>25 cases) for novice sonographers.12
Low efficacy in subtrochanteric fractures.11,32
Comparison with Traditional Blocks
Femoral Nerve Block (FNB)
FNB causes quadriceps weakness in 70% of cases, delaying mobilization.4,33–35
Fascia Lliaca Block (FIB)
The FIB results in relatively imprecise sensory coverage, with 30% of cases requiring supplemental opioids.36–38
In contrast, the PENG block achieves complete sensory blockade in 85% of patients with hip fractures without motor deficits.39,40
Future Directions
Protocol Standardization
A consensus on anaesthetic volumes (eg, 15–20 mL ropivacaine 0.375%) should be established for diverse populations.
Technological Integration
AI-assisted ultrasound systems could be developed to shorten training periods.
Outcome Studies
Additional investigations should be conducted in multicentre cohorts to evaluate functional recovery and opioid dependence rates.
Conclusion
The ultrasound-guided PENG block redefines trauma analgesia from the following perspectives:
① Precision: The PENG block reduces opioid reliance by 68–85% in patients with hip fractures while sparing motor function.
② Safety: Complications are minimized (vascular injury <1%; LAST risk reduction 82%) through real-time visualization.
③ Versatility: The technique is effective for patients with hip/pelvic fractures with subtrochanteric limitations.
Despite resource constraints, the integration of the PENG block promises global outcome improvements. Multiple trials (eg, the PENGLISH trial) could aid in solidifying protocols.
Abbreviations
PENG, Pericapsular Nerve Group; FICB, Fascia Iliaca Compartment Block; FNB, Femoral Nerve Block; AIIS, Anterior Inferior Iliac Spine; IPE, Iliopubic Eminence; PT, Psoas Tendon; FA, Femoral Artery; LAST, Local Anaesthetic Systemic Toxicity; NRS, Numerical Rating Scale; US, Ultrasound; VAS, Visual Analogue Scale; ICU, Intensive Care Unit.
Data Sharing Statement
This manuscript is a review article and does not involve original data collection. Therefore, no datasets are available for sharing. All information and data cited in this review are publicly available in the referenced articles.
Ethics Approval and Informed Consent
This paper is a review article and does not involve original research with human participants or animals. Therefore, ethical approval and informed consent are not applicable. The review is based on existing published literature.
Consent for Publication
The authors declare that consent for publication has been obtained for any personal information, images, or data included in this paper, where applicable. No personal identifiers or sensitive information have been used without explicit consent.
Acknowledgments
I would like to sincerely thank my colleagues in the Department of Anaesthesiology at Heyuan People’s Hospital for their unwavering support and invaluable contributions during the preparation of this article. I am also deeply grateful to my family, who have always provided me with encouragement and understanding. Their support has been the source of strength throughout my entire research process.
Funding
This review was funded by the Guangdong Provincial Medical Science and Technology Research Fund (2024HY-A3005) and the High-level Hospital Construction Research Project of Heyuan People’s Hospital (YNKT202208).
Disclosure
The authors declare that they have no competing interests.
References
1. Cogan CJ, Kandemir U. Role of peripheral nerve block in pain control for the management of acute traumatic orthopaedic injuries in the emergency department: diagnosis-based treatment guidelines. Injury. 2020;51(7):1422–1425. doi:10.1016/j.injury.2020.04.016
2. Johnson M, Strait L, Ata A, et al. Do lidocaine patches reduce opioid use in acute rib fractures? Am Surg. 2020;86(9):1153–1158. doi:10.1177/0003134820945224
3. Lin X, Liu CW, Goh QY, et al. Pericapsular nerve group (PENG) block for early pain management of elderly patients with Hip fracture: a single-center double-blind randomized controlled trial. Reg Anesth Pain Med. 2023;48(11):535–539. doi:10.1136/rapm-2022-104117
4. Jin Z, Sugiyama D, Higo F, et al. Efficacy of pericapsular nerve group (PENG) block in preoperative rehabilitation (Prehabilitation) for patients with femoral neck fractures: study protocol for a randomized, placebo-controlled, double-blinded trial. BMC Anesthesiol. 2024;24(1):436. doi:10.1186/s12871-024-02620-8
5. Lin DY, Morrison C, Brown B, et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in Hip fracture surgery: a single-center double-blinded randomized comparative trial. Reg Anesth Pain Med. 2021;46(5):398–403. doi:10.1136/rapm-2020-102315
6. Morrison C, Brown B, Lin DY, Jaarsma R, Kroon H. Analgesia and anesthesia using the pericapsular nerve group block in Hip surgery and hip fracture: a scoping review. Reg Anesth Pain Med. 2021;46(2):169–175. doi:10.1136/rapm-2020-101826
7. Girón-Arango L, Peng PWH, Chin KJ, Brull R, Perlas A. Pericapsular nerve group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018;43(8):859–863. doi:10.1097/AAP.0000000000000847
8. Pagano T, Scarpato F, Chicone G, et al. Analgesic evaluation of ultrasound-guided pericapsular nerve group (PENG) block for emergency hip surgery in fragile patients: a case series. Arthroplasty. 2019;1(1):18. doi:10.1186/s42836-019-0018-0
9. Marrone F, Graziano G, Paventi S, Tomei M, Gucciardino P, Bosco M, Analgesic efficacy of Pericapsular Nerve Group (PENG) block compared with Fascia Iliaca Block (FIB) in the elderly patient with fracture of the proximal femur in the emergency room. A randomised controlled trial. Rev Esp Anestesiol Reanim. 2023;70(9):501–508. doi:10.1016/j.redar.2022.10.002
10. Rocha-Romero A, Arias-Mejia K, Salas-Ruiz A, Peng PWH. Pericapsular nerve group (PENG) block for Hip fracture in the emergency department: a case series. Anaesth Rep. 2021;9(1):97–100. doi:10.1002/anr3.12118
11. Vergari A, Console E, Nestorini R, et al. PENG block associated with dexmedetomidine sedation for intramedullary femoral fixation in high-risk elderly patients: a case series and review of the literature. Eur Rev Med Pharmacol Sci. 2023;27(20):10061–10068. doi:10.26355/eurrev_202310_34186
12. Xiao B, Chen Y, Lin S, et al. Evaluating the learning curve of total ultrasound guided percutaneous nephrolithotomy in complex renal stones using “30-degree triangulation” technique. World J Urol. 2025;43(1):312. doi:10.1007/s00345-025-05674-6
13. Le D, Sacchi MD, Lou E, Le LH. Robust guided wave inversion for estimating bone thickness and elasticity. J Acoust Soc Am. 2024;156(6):3973–3983. doi:10.1121/10.0034604
14. Parag AK, Raducanu BC, Erden OK, et al. Dynamic sub-array selection-based energy-efficient localization and tracking method to power implanted medical devices in scattering heterogenous media employing ultrasound. IEEE Trans Biomed Circuits Syst. 2025;19(3):657–668. doi:10.1109/TBCAS.2024.3487782
15. Del Buono R, Padua E, Pascarella G, et al. Pericapsular nerve group block: an overview. Minerva Anestesiol. 2021;87(4):458–466. doi:10.23736/S0375-9393.20.14798-9
16. Zheng L, Jo Y, Hwang J, et al. Comparison of the analgesic efficacy of periarticular infiltration and pericapsular nerve group block for total hip arthroplasty: a randomized, non-inferiority study. Ann Palliat Med. 2022;11(4):1222–1230. doi:10.21037/apm-21-2785
17. Nagpal AS, Brennick C, Occhialini AP, et al. Innervation of the posterior hip capsule: a cadaveric study. Pain Med. 2021;22(5):1072–1079. doi:10.1093/pm/pnab057
18. Aliste J, Layera S, Bravo D, et al. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Reg Anesth Pain Med. 2021;46(10):874–878. doi:10.1136/rapm-2021-102997
19. Yoo SH, Lee MJ, Beak MH, Kim WJ. Efficacy of supplemental ultrasound-guided pericapsular nerve group (PENG) block combined with lateral femoral cutaneous nerve block in patients receiving local infiltration analgesia after hip fracture surgery: a prospective randomized controlled trial. Medicina (Kaunas). 2024;60(2). doi:10.3390/medicina60020315
20. Ahiskalioglu A, Aydin ME, Ahiskalioglu EO, Tuncer K, Celik M. Pericapsular nerve group (PENG) block for surgical anesthesia of medial thigh. J Clin Anesth. 2020;59:42–43. doi:10.1016/j.jclinane.2019.06.021
21. Girón-Arango L, Peng P. Pericapsular nerve group (PENG) block: what have we learned in the last 5 years? Reg Anesth Pain Med. 2025;50(5):402–409. doi:10.1136/rapm-2024-105427
22. Domagalska M, Ciftci B, Reysner T, Kolasiński J, Wieczorowska-Tobis K, Kowalski G. Pain management and functional recovery after pericapsular nerve group (PENG) block for total hip arthroplasty: a prospective, randomized, double-blinded clinical trial. J Clin Med. 2023;12(15):1.
23. Kong M, Tang Y, Tong F, et al. The analgesic efficacy of pericapsular nerve group block in patients with intertrochanteric femur fracture: a randomized controlled trial. PLoS One. 2022;17(10):e0275793. doi:10.1371/journal.pone.0275793
24. Wang QR, Ma T, Hu J, Yang J, Kang PD. Comparison between ultrasound-guided pericapsular nerve group block and anterio quadratus lumborum block for total Hip arthroplasty: a double-blind, randomized controlled trial. Eur Rev Med Pharmacol Sci. 2023;27(16):7523–7532. doi:10.26355/eurrev_202308_33404
25. Nuthep L, Klanarong S, Tangwiwat S. The Analgesic effect of adding ultrasound-guided pericapsular nerve group block to suprainguinal fascia iliaca compartment block for Hip fracture surgery: a prospective randomized controlled trial. Medicine. 2023;102(44):e35649. doi:10.1097/MD.0000000000035649
26. Bravo D, Aliste J, Layera S, et al. Randomized clinical trial comparing pericapsular nerve group (PENG) block and periarticular local anesthetic infiltration for total hip arthroplasty. Reg Anesth Pain Med. 2023;48(10):520–521. doi:10.1136/rapm-2023-104487
27. Hu J, Wang Q, Hu J, Kang P, Yang J. Efficacy of ultrasound-guided pericapsular nerve group (PENG) block combined with local infiltration analgesia on postoperative pain after total hip arthroplasty: a prospective, double-blind, randomized controlled trial. J Arthroplasty. 2023;38(6):1096–1103. doi:10.1016/j.arth.2022.12.023
28. Simić A, Nesek Adam V, Rošić D, et al. PERIPHERAL NERVE BLOCKS FOR HIP FRACTURES IN EMERGENCY MEDICINE. Acta Clin Croat. 2022;61(Suppl 1):78–83. doi:10.20471/acc.2022.61.s1.13
29. Liu S, Ren X, Li X, et al. Application of hip pericapsular nerve block combined with spinal anesthesia in the treatment of elderly patients with femoral intertrochanteric fracture. J Musculoskelet Neuronal Interact. 2024;24(2):178–184.
30. Cripps E, Fahey A, Snelling PJ. Point-of-care ultrasound-guided pericapsular nerve group block for superior pubic ramus fracture in the emergency department: a case report. Australas J Ultrasound Med. 2022;25(3):154–156. doi:10.1002/ajum.12308
31. Moorthy A, Choi S, Safa B, McHardy PG, Niazi AU. Novel use of continuous pericapsular nerve group (PENG) block technique for traumatic superior and inferior pubic rami fractures: a case report. Reg Anesth Pain Med. 2023;48(5):230–233. doi:10.1136/rapm-2022-104151
32. Zhang L, He M, Jia W, et al. Analysis of high-risk factors for preoperative DVT in elderly patients with simple hip fractures and construction of a nomogram prediction model. BMC Musculoskelet Disord. 2022;23(1):441. doi:10.1186/s12891-022-05377-8
33. Guay J, Kopp S. Peripheral nerve blocks for hip fractures in adults. Cochrane Database Syst Rev. 2020;11(11):Cd001159.
34. Martínez Martín A, Pérez Herrero M, Sánchez Quirós B, López Herrero R, Ruiz Bueno P, Cocho Crespo S. Benefits of analgesic blocks, PENG block (Pericapsular Nerve Group), in fast recovery after Hip surgery. Rev Esp Cir Ortop Traumatol. 2023;67(1):27–34. doi:10.1016/j.recot.2022.03.007
35. Noaman SS, Abdallah ES, Elsawy SMA, Abd El-Radi M, Kamel MM. The efficacy of pericapsular nerve group block versus facia iliaca block on immediate postoperative pain and opioid consumption after hip arthroscopy randomized trial. Pain Physician. 2023;26(4):357–367. doi:10.36076/ppj.2023.26.357
36. Huang KT, Tsai HI, Kao SC. Supra-inguinal fascia iliaca block versus peri-capsular nerve group (PNEG) block for pain management in patients with Hip fracture: a double-blind randomised comparative trial. Injury. 2024;55(12):111936. doi:10.1016/j.injury.2024.111936
37. Saini T, Aggarwal M, Singh U, Singh MR. Pericapsular nerve group (PENG) block versus supra-inguinal fascia iliaca (SIFI) block for functional outcome in patients undergoing Hip surgeries - A randomised controlled study. Indian J Anaesth. 2024;68(12):1043–1048. doi:10.4103/ija.ija_838_24
38. Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Nerve Block vs, Vetrone F, Saglietti F, Galimberti A, et al. Fascia Iliaca compartment block in hip replacement surgery. J Clin Med. 2025;14(3):984. doi:10.3390/jcm14030984.
39. Senthil KS, Kumar P, Ramakrishnan L. Comparison of pericapsular nerve group block versus fascia iliaca compartment block as postoperative pain management in hip fracture surgeries. Anesth Essays Res. 2021;15(4):352–356. doi:10.4103/aer.aer_119_21
40. Vichainarong C, Kampitak W, Ngarmukos S, Tanavalee A, Tanavalee C, Jinaworn P. Comparison of analgesic efficacy between ultrasound-guided supra-inguinal fascia iliaca block and pericapsular nerve group block following total hip arthroplasty: a randomized controlled trial. Hip Pelvis. 2024;36(4):290–301. doi:10.5371/hp.2024.36.4.290
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.