Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Perianal Pseudoverrucous Papules and Nodules in an Elderly Patient
Authors Kim EH, Park JS ![]() , Lee JS, Lee JY
, Lee JS, Lee JY
Received 20 July 2023
Accepted for publication 5 October 2023
Published 13 October 2023 Volume 2023:16 Pages 2863—2867
DOI https://doi.org/10.2147/CCID.S428120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Jeffrey Weinberg
En Hyung Kim,1,2 Jun Su Park,1,2 Ji Su Lee,2 Ji Yeoun Lee1,2
1Department of Dermatology, College of Medicine, Chungbuk National University, Cheongju, Chungbuk, South Korea; 2Department of Dermatology, Chungbuk National University Hospital, Cheongju, Chungbuk, South Korea
Correspondence: Ji Yeoun Lee, Department of Dermatology, College of medicine, Chungbuk National University, Chungdae-ro 1, Seowon-Gu, Cheongju, Chungbuk, 28644, South Korea, Tel +82-43-269-6385, Fax +82-43-266-1698, Email [email protected]
Abstract: Pseudoverrucous papules and nodules is a reaction to irritation usually associated with urostomies. We report a case of perianal pseudoverrucous papules and nodules in an elderly patient who developed a characteristic diaper dermatitis after infrequent diaper change. The perianal papulonodular lesions improved after saline wet dressing and topical steroid application. These perianal pseudoverrucous papules and nodules indicate a unique type of irritant diaper dermatitis, which can be distinguished from Jacquet erosive diaper dermatitis and granuloma gluteale adultorum. Identifying this condition is important because pseudoverrucous papules and nodules can resemble more serious dermatoses, leading to unnecessary investigations being carried out.
Keywords: diaper dermatitis, irritant dermatitis, Jacquet erosive diaper dermatitis, granuloma gluteale adultorum
Introduction
Diaper dermatitis encompasses a range of acute, inflammatory reactions that occur as a result of irritant contact dermatitis caused by exposure to feces, urine or both. In uncomplicated cases, the affected areas exhibit diffuse erythema, with occasional presence of micropapules and scaling. Several uncommon clinical patterns, regarded as complications of diaper dermatitis, have also been described: granuloma gluteale infantum/adultorum, Jacquet erosive diaper dermatitis, and perianal pseudoverrucous papules and nodules (PPPN).1
PPPN is an uncommon manifestation of irritant contact dermatitis that was first reported around urostomy sites.2 PPPN consisted of flat-topped, erythematous-brown papules and nodules that develop in the diaper and perianal areas in patients of any age whose skin is chronically exposed to moisture, including the elderly and children with prolonged urinary or fecal incontinence.3 These lesions are relatively rare and occasionally misdiagnosed, which may even result in their surgical removal. Only a limited number of case reports exist documenting the occurrence of PPPN on the perianal skin or in the elderly.1,4,5
Case
An 84-year-old woman visited the dermatologic department with a 3-month history of multiple verrucous papules and nodules on the perianal area, which were causing discomfort and pain. She had a previous medical history of hypertension and spinal stenosis. The patient was bedridden due to her medical condition. Despite frequent defecation and urination, her caregiver had changed her diapers only twice a day, using wet wipes and povidone. A month ago, the patient was prescribed topical antibiotics at a local clinic with limited improvement and was referred to our clinic under the impression of viral infection. The patient’s laboratory test results were nonspecific, and polymerase chain reaction did not detect human papillomavirus. Treponema pallidum hemagglutination (TPHA) tests were negative/non-reactive. No bacterial or fungal growth was observed on culture. On physical examination, multiple, 3–12 mm sized flat-topped moist verrucous papules and nodules with some lesions coalescing to form plaques were noticed at the perianal area (Figure 1). Punch biopsy specimen revealed prominent hyperkeratosis, parakeratosis, irregular epidermal hyperplasia (Figure 2A) and mild lymphocytic infiltration in the dermis (Figure 2B). Periodic Acid-Schiff with diastase (PAS-D) staining did not reveal any pathogenic organism. The lesions were diagnosed as perianal pseudoverrucous papules and nodules based on the clinical and histopathologic features. The patient was treated with daily saline wet dressings and 0.25% prednicarbate lotion. The diapers were changed on more regular and frequent intervals. After 6 weeks of treatment, the lesions improved significantly (Figure 3).
 |
Figure 1 Multiple eroded hyperpigmented flat-topped papules and nodules with few verrucous papules and nodules on the perianal area. |
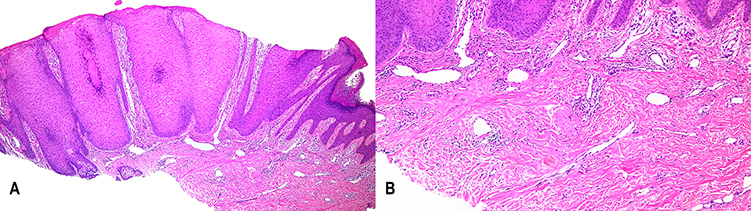 |
Figure 2 Histopathologic findings. (A) Prominent hyperkeratosis, parakeratosis and irregular hyperplasia in the epidermis (Hematoxylin and eosin; x 40). (B) Mild lymphocytic infiltration in the dermis (Hematoxylin and eosin; x 100). |
 |
Figure 3 The lesions improved after 6 weeks of treatment. |
Discussion
Goldberg et al introduced the term PPPN for the first time in 1992.3 PPPN predominately affects children in the diaper area and around surgical ostomies, related to gastrointestinal or urologic diseases.3 PPPN presents as multiple, wart-like erythematous-brown papules and nodules in perianal, genital, suprapubic, buttocks, and peristomal areas.6 Histopathological examination of these lesions reveals psoriasiform epidermal hyperplasia with acanthosis, broad hyperparakeratosis, papillary edema, prominent dermal blood vessels, and mild-to-moderate dermal perivascular infiltrate. It is controversial whether PPPN constitutes a distinct form of primary irritant diaper dermatitis1 or that granuloma gluteale infantum/adultorum, Jacquet’s erosive dermatitis, and PPPN are all part of the same entity coined under the term “erosive papulonodular dermatosis”.6 Granuloma gluteale adultorum is usually manifested as reddish-purple, firm, oval, or elongated plaques and nodules in the pubic area, buttocks, scrotum, and medial aspects of the thighs.6 This is a different feature from the observed papules and small nodules located in the perianal area of our patient. Moreover, PPPN tends to exhibit a higher number of verrucous lesions compared to granuloma gluteale adultorum.7 Compared to PPPN, the histology of granuloma gluteale adultorum is relatively nonspecific. The histopathological features show epidermal hyperplasia and a dense dermal inflammatory cell infiltration, with proliferation of blood vessels and a variable degree of dilation. The term “granuloma” can be misleading because histologically, granulomatous inflammation is not observed in cases of granuloma gluteale adultorum.6,7 In Jacquet’s erosive diaper dermatitis, well-demarcated, 2 to 5 mm punched-out ulcers or erosions with elevated borders typically occur on the peri-vulvar or penis area.1,8,9 Biopsy findings usually show a nonspecific inflammatory pattern.6,7,9 Thus, the term PPPN is preferred in our case because it is more clinically descriptive (Table 1).
 |
Table 1 Characteristic Features in Various Types of Irritant Diaper Dermatitis |
PPPN is an uncommon type of irritant contact dermatitis and sometimes can be misdiagnosed. Due to clinical similarities, several dermatoses, infections and neoplasms may be considered in the differential diagnosis including condyloma lata, condyloma acuminata, bacterial infections, candidiasis, scabietic nodules, anogenital warts, Langerhans cell histiocytosis and cutaneous Crohn’s disease.3,5,10 The sexual history, rapid plasma reagin (RPR), venereal disease research laboratory (VDRL), bacterial culture, fungus culture and skin biopsy may be helpful in differentiating from other diseases. In histology, condyloma lata caused by Treponema pallidum reveals spirochetes in silver stain.
The mechanism of development of PPPN is not clear. However, the most important factor is presumed to be the humid environment resulting from repeated or continuous contact with urine or loose feces. This state can exacerbate maceration and increase the vulnerability to the damaging effects of fecal irritants such as pancreatic proteases and lipases.1,10 The urinary ammonia produced by intestinal bacteria ureases in feces makes an alkaline environment, and in this high pH environment, these enzymes become more active and have a stronger damaging effect.11 Other suggested contributing pathogenetic factors include occlusion by nylon or cloth diapers, contact with detergents, starch containing powders, halogenated steroids, plastic pants, Candida infection, and urinary infection.5,6,11 The treatment should primarily focus on removing the precipitating factors and restoring the skin barrier function to reduce irritation and prevent secondary infection. Thus, timely changing of diapers is important. Superabsorbent disposable diapers are recommended over cloth diapers as cloth diapers wet more easily and may contain remnant detergents, a potential pathogenic factor.12 There have been reports that shave excision, and repeated cryotherapy sessions are effective in PPPN treatment.5,13 However, these destructive or surgical methods only provided temporary relief. Additional treatment options are applying topical steroid and topical zinc oxide as a protective barrier.4 In a recent study, applying potato protease inhibitors was tested as a novel treatment for preventing perianal dermatitis caused by protease.14
Recognition and correct diagnosis of PPPN is important as topical steroids and starch containing powders, two most commonly used treatments for diaper rash, may aggravate PPPN. As the elderly population increases and the number of patients with colostomies and urostomies rises, PPPN in the elderly is expected to increase in the future. In order to minimize unnecessary investigations and treatments, clinicians should be aware of various manifestations of peristomal and diaper area dermatitis.
Ethics Statement
The publications of images were included in the patient’s consent for publication of the case. Institutional approval has been obtained to publish the case details.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of the case details and images.
Author Contributions
All authors contributed to the diagnosis and conception of the case report. The first draft of the manuscript was written by En Hyung Kim and Jun Su Park. All authors substantially revised or critically reviewed the article. All authors agreed on the journal to which the article is submitted. All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors agree to take responsibility and be accountable for the contents of the article.
Disclosure
En Hyung Kim, Jun Su Park, Ji Su Lee, Ji Yeoun Lee declare that they have no conflicts of interest in this work.
References
1. Rodríguez Cano L, García-Patos Briones V, Pedragosa Jové R, Castells Rodellas A. Perianal pseudoverrucous papules and nodules after surgery for Hirschsprung disease. J Pediatr. 1994;125(6):914–916. doi:10.1016/S0022-3476(05)82008-6
2. Borglund E, Nordström G, Nyman CR. Classification of peristomal skin changes in patients with urostomy. J Am Acad Dermatol. 1988;19(4):623–628. doi:10.1016/S0190-9622(88)70215-7
3. Goldberg NS, Esterly NB, Rothman KF, et al. Perianal pseudoverrucous papules and nodules in children. Arch Dermatol. 1992;128(2):240–242. doi:10.1001/archderm.1992.01680120112014
4. Lee YY, Ko JH, Shih YC. Multiple erythematous erosive papules and nodules on the perianal area of an 84-year-old bedridden woman. Dermatologica Sinica. 2012;30(3):115–116. doi:10.1016/j.dsi.2011.10.005
5. Mansur AT, Ramadan S, Oguz N. Pseudoverrucous papules and nodules in an elderly woman with encopresis: effects of cryotherapy. Hong Kong J Dermatol Venereol. 2020;28:121–124.
6. Robson KJ, Maughan JA, Purcell SD, Petersen MJ, Haefner HK, Lowe L. Erosive papulonodular dermatosis associated with topical benzocaine: a report of two cases and evidence that granuloma gluteale, pseudoverrucous papules, and Jacquet’s erosive dermatitis are a disease spectrum. J Am Acad Dermatol. 2006;55(5):74–80. doi:10.1016/j.jaad.2005.12.025
7. Aşkin Ü, Ada S, Bilezikçi B, Arda S. Erosive papulonodular dermatosis in an adolescent with encopresis. Br J Dermatol. 2008;158(2):413–415. doi:10.1111/j.1365-2133.2007.08291.x
8. Rodriguez-Poblador J, González-Castro U, Herranz-Martínez S, Luelmo-Aguilar J. Jacquet erosive diaper dermatitis after surgery for Hirschsprung disease. Pediatr Dermatol. 1998;15(1):46–47. doi:10.1046/j.1525-1470.1998.1998015046.x
9. Hara M, Watanabe M, Tagami H. Jacquet erosive diaper dermatitis in a young girl with urinary incontinence. Pediatr Dermatol. 1991;8(2):160–161. doi:10.1111/j.1525-1470.1991.tb00309.x
10. Amiry SA, Pride HB, Tyler WB. Perianal pseudoverrucous papules and nodules mimicking condylomata acuminata and child sexual abuse. Cutis. 2001;67(4):335–338.
11. Isogai R, Yamada H. Factors involved in the development of diaper-area granuloma of the aged. J Dermatol. 2013;40(12):1038–1041. doi:10.1111/1346-8138.12337
12. Erasala GN, Romain C, Merlay I. Diaper area and disposable diapers. Curr Probl Dermatol. 2011;40:83–89.
13. Singh MK, Wendelschafer-Crabb G, Davis MD. Incapacitating pseudoverrucous papules and nodules: cure by shave excision. Cutis. 2013;92:7–9.
14. Ruseler-van Embden JG, van Lieshout LM, Smits SA, van Kessel I, Laman JD. Potato tuber proteins efficiently inhibit human faecal proteolytic activity: implications for treatment of peri-anal dermatitis. Eur J Clin Invest. 2004;34(4):303–311. doi:10.1111/j.1365-2362.2004.01330.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.