Back to Journals » Cancer Management and Research » Volume 13
Performance of Plasma HSP90α, Serum EBV VCA IgA Antibody and Plasma EBV DNA for the Diagnosis and Prognosis Prediction of Nasopharyngeal Carcinoma
Authors Ye Q, Guo J ![]() , Chen Y, Cui Z, Chen Y
, Chen Y, Cui Z, Chen Y
Received 17 May 2021
Accepted for publication 29 June 2021
Published 20 July 2021 Volume 2021:13 Pages 5793—5802
DOI https://doi.org/10.2147/CMAR.S320541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Qian Ye, Junying Guo, Yansong Chen, Zhaolei Cui, Yan Chen
Department of Laboratory Medicine, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, Fuzhou City, Fujian Province, 350014, People’s Republic of China
Correspondence: Zhaolei Cui; Yan Chen
Department of Laboratory Medicine, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, No. 420 Fuma Road, Jin’an District, Fuzhou City, Fujian Province, 350014, People’s Republic of China
Email [email protected]; [email protected]
Objective: The aim of this study was to evaluate the effectiveness of Epstein–Barr virus (EBV) VCA-IgA antibody, EBV DNA and HSP90α alone or in combinations for the diagnosis and prognostic prediction of nasopharyngeal carcinoma (NPC).
Methods: A total of 113 treatment-naïve patients with NPC and 40 healthy controls were enrolled. Plasma HSP90α and serum EBV VCA IgA antibody were detected using ELISA, and plasma EBV DNA was quantified using qPCR assay. The effectiveness of plasma HSP90α level, serum EBV VCA IgA antibody and plasma EBV DNA was examined in the diagnosis and prognosis prediction of NPC.
Results: Higher plasma HSP90α, serum EBV VCA IgA antibody and plasma viral load of EBV DNA were detected in NPC patients than in healthy controls (P < 0.001). The plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were significantly greater in NPC patients with stages III and IV than in those with stages I and II (P < 0.001), and significantly lower plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were found in the good prognosis group than in the poor prognosis group post-treatment (P < 0.05). The area under representative operating curves (AUCs) of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA alone and in combination were 0.884, 0.841, 0.934 and 0.954 for the diagnosis of NPC, respectively. Univariate and multivariate Cox proportional hazards regression analyses identified HSP90α as an independent prognostic factor for NPC.
Conclusion: The combination of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA shows high diagnostic performance for NPC, and plasma HSP90α may be a potential marker for diagnosis and prognosis prediction of NPC.
Keywords: nasopharyngeal carcinoma, EBV VCA-IgA antibody, EBV DNA, HSP90α, diagnostic performance, prognosis prediction
Introduction
Nasopharyngeal carcinoma (NPC), the most common head and neck cancer, is characterized by a distinct geographic distribution.1 Although relatively rare worldwide,2 this malignancy is highly prevalent in eastern and southeastern Asia, notably in southern China.3 Epstein–Barr virus (EBV) infection and genetic susceptibility foci have been identified to be responsible for the development of NPC; however, the exact pathogenesis remains to be unraveled.4–6 Currently, radiotherapy and chemotherapy are standard treatments for NPC.7–10 The prognosis of NPC is determined by the disease stage.11 Patients with early-stage NPC have a 5-year survival rate of approximately 90%, while those at an advanced stage have a 5-year survival rate of less than 50%.1 Early and precise detection is therefore of great importance to improve the prognosis of NPC.12
Currently, the diagnosis of NPC primarily depends on biopsy and imaging tools1; however, early diagnosis is very difficult because of the specific anatomic location of the nasopharynx.13 Most individuals are diagnosed at late stages of NPC with distal metastases since there are no specific symptoms or signs at an early stage, which greatly affects the clinical outcomes.11 Screening of biomarkers is therefore of great clinical significance for the diagnosis and prognostic prediction of NPC.14
Previous studies have shown the diagnostic and prognostic values of Epstein–Barr virus capsid antigen (VCA)-IgA antibody and EBV DNA in NPC.15–20 Recently, heat shock protein 90α (HSP90α) was identified as a novel diagnostic marker for NPC21; however, there is little knowledge on its performance for the clinical diagnosis of NPC. This study was therefore designed with aims to evaluate the effectiveness of EBV VCA-IgA antibody, EBV DNA and HSP90α alone or in combinations for the diagnosis and prognostic prediction of NPC.
Methods
Ethical Statement
This study was approved by the Ethics Review Committee of Fujian Medical University Cancer Hospital. All procedures were performed in accordance with the 2018 Declaration of Helsinki,22 as well as international and national laws and guidelines. Written informed consent was obtained from all participants included in this study, following a detailed description of the major purpose of the study.
Subjects
A total of 113 treatment-naïve patients with pathologically diagnosed NPC in Fujian Medical University Cancer Hospital during the period from September 2016 through March 2017 were recruited, while 40 healthy subjects without any tumor-related disorders in the hospital during the same period were sampled as controls. The inclusion criteria included 1) definitive diagnosis of NPC for the first time without prior chemotherapy or other antitumor treatments; 2) complete imaging and clinical data; 3) willingness to sign the informed consent; and 4) no abnormality identified in healthy controls. Those meeting any of the following criteria were excluded from the study: 1) patients undergoing radiotherapy or chemotherapy; 2) patients with severe hepatic or renal insufficiency, pulmonary disorders, severe cardiovascular disorders, diabetes, or other tumors; 3) patients with acute infections or hematologic diseases; or 4) pregnant or lactating women. Patients’ demographic and clinical characteristics were collected, including age, gender, the World Health Organization (WHO) pathological classification,23 and American Joint Committee on Cancer (AJCC) clinical stage and TNM stage,24 and treatment, as well as follow-up and prognosis data.
Detection of Plasma HSP90α and EBV DNA and Serum EBV VCA-IgA Antibody
Approximately 3 mL of venous blood samples were collected from all patients and centrifuged at 3,000 r/min for 10 min, and plasma and serum samples were collected. Plasma HSP90α level was detected using an enzyme-linked immunosorbent assay (ELISA) with the human HSP90α ELISA kit (Yantai Protgen Biotechnology Development Co. Ltd.; Yantai, China), and serum EBV VCA IgA antibody was detected using the EBV VCA IgA Antibody ELISA Test Kit (EUROIMMUN Medizinische Labordiagnostika AG; Luebeck, Germany). In addition, plasma EBV DNA was quantified using the quantitative real-time PCR (qPCR) assay with the EBV viral nucleic acid amplification kit (Da An Gene Co., Ltd. of Sun Yat-sen University; Guangzhou, China) on the Applied Biosystems™ 7500 Real-Time PCR Systems (Thermo Fisher Scientific, Waltham, MA, USA). All detection procedures were done in strict accordance with the manufacturers’ instructions.
Follow-Up and Survival Estimates
Post-treatment follow-up was done using outpatient visits or telephone calls once every 3 months within 2 years post-treatment, and once every half a year 2 years post-treatment until death. Overall survival (OS) was defined as the duration from the start of the treatment to death of any causes or the final follow-up date.
Statistics
All statistical analyses were performed using the statistical software SPSS version 23.0 (SPSS, Inc.; Chicago, IL, USA), and all figures were plotted using the software GraphPad Prism version 8.0 (GraphPad Software; San Diego, CA, USA). Normally distributed data were presented with mean ± standard deviation (SD), and differences of means of measurement data were tested for statistical significance with Student’s t-test, while comparisons of proportions were conducted with chi-square test or Fisher’s exact test. Non-normally distributed data were expressed as median (P25, P75), and comparisons of medians were done with Mann–Whitney U-test. The representative operating characteristic curve (ROC) was plotted and the area under ROC (AUC), confidential interval (CI), sensitivity and specificity of diagnostic assays were estimated with the greatest Youden index as the cut-off. The associations of HSP90α level with the EBV VCA IgA antibody titer and the viral load of EBV DNA were examined in NPC patients with Pearson correlation analysis. Survival was estimated using the Kaplan–Meier curve, and comparison of survival was tested for statistical significance using the Log rank test. The prognostic factors for NPC were identified using univariate and multivariate Cox proportional hazards regression analyses. A P value of < 0.05 was considered statistically significant.
Results
Patient Characteristics
Among the 113 subjects, there were 72 men and 41 women and the mean age was 48.24 ± 11.02 years (range, 19 to 78 years). There were 92.92% of the study subjects with non-keratinizing undifferentiated carcinoma according to the WHO pathological classification, and 60.18% with stage III and 29.2% with stage IV according to the AJCC staging system (Table 1). Of the 40 healthy controls, there were 25 men and 15 women and the mean age was 45.94 ± 10.32 years (range, 25 to 64 years). The mean age and gender distribution were comparable between the NPC patients and healthy controls (P > 0.05). In addition, significantly higher plasma HSP90α levels (t = 15.317), serum EBV VCA IgA antibody titers (Z = 11.459) and plasma viral load of EBV DNA (t = 24.261) were detected in NPC patients than in healthy controls (P < 0.001) (Figure 1), and Pearson correlation analysis revealed that the plasma HSP90α level positively correlated with the plasma viral load of EBV DNA (r = 0.873, P < 0.05) and serum EBV VCA IgA antibody titer (r = 0.768, P < 0.05) in patients with NPC (Figure 2).
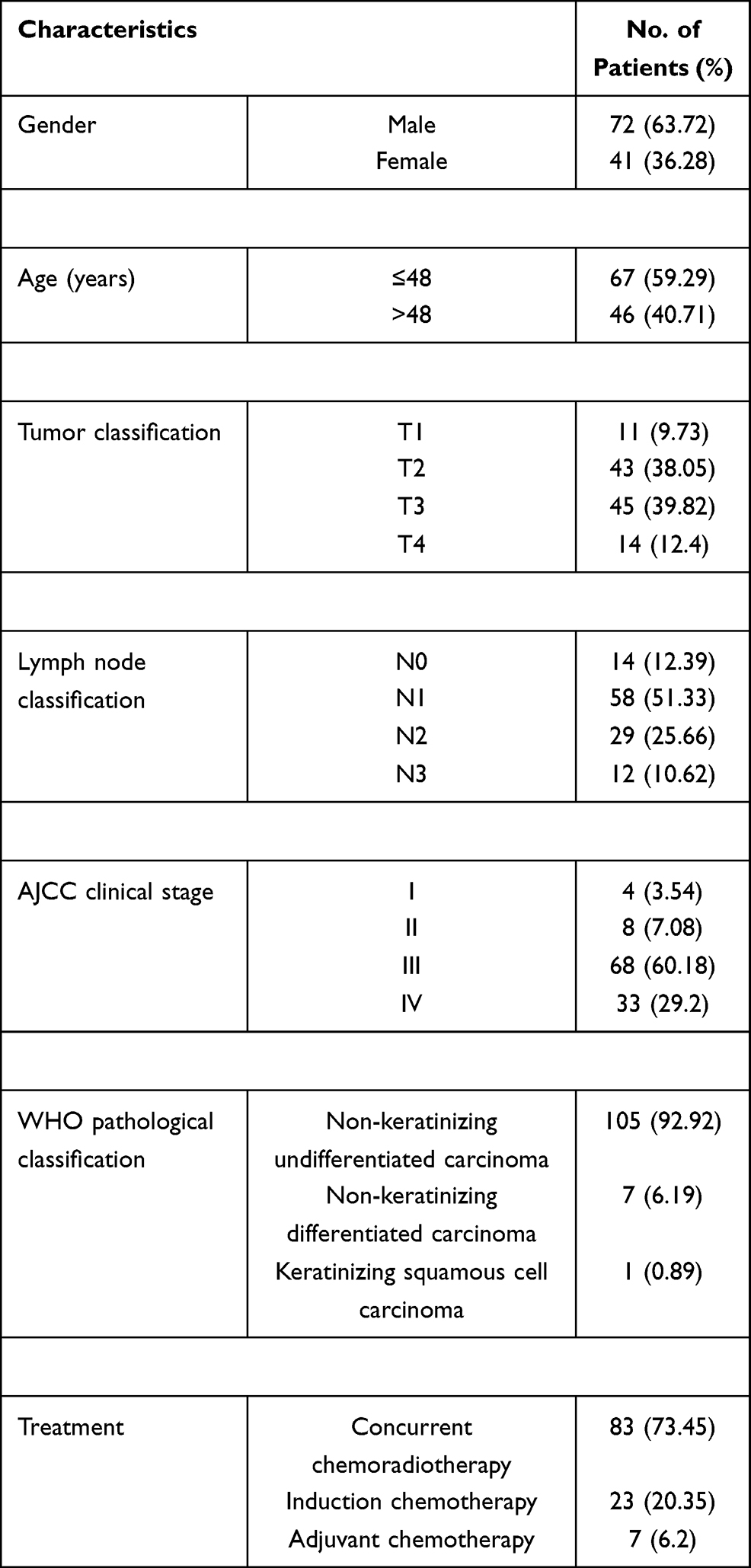 |
Table 1 Demographic and Clinical Characteristics of the 113 Patients with Nasopharyngeal Carcinoma |
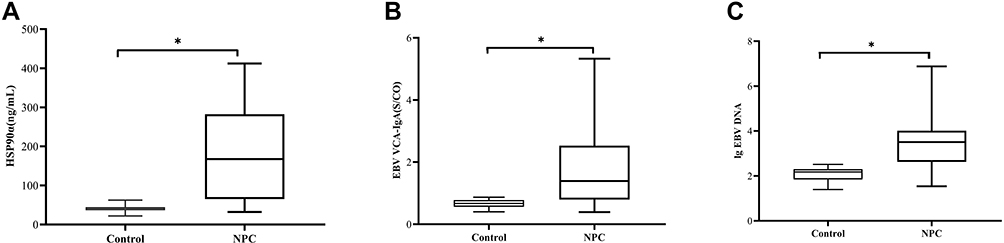 |
Figure 1 Comparison of plasma HSP90α level, serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA between nasopharyngeal carcinoma patients and healthy controls. (A) plasma HSP90α level; (B) serum EBV VCA IgA antibody titer; (C) plasma viral load of EBV DNA. *P < 0.001 vs healthy controls. Abbreviation: NPC, nasopharyngeal carcinoma. |
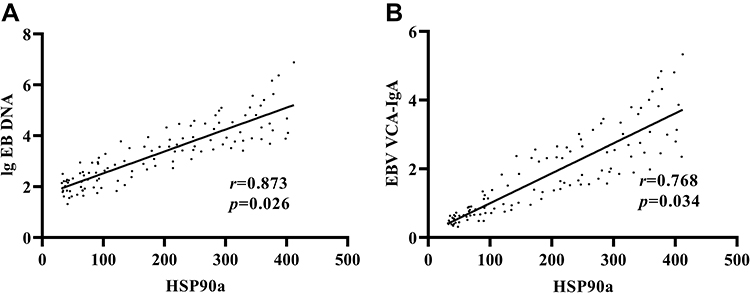 |
Figure 2 Pearson correlation analysis reveals the associations of plasma HSP90α level with serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA in nasopharyngeal carcinoma patients. (A) correlation between plasma HSP90α level and plasma viral load of EBV DNA in nasopharyngeal carcinoma patients; (B) correlation between plasma HSP90α level and serum EBV VCA IgA antibody titer in nasopharyngeal carcinoma patients. |
Stage- and Prognosis-Specific HSP90α, EBV VCA IgA Antibody and EBV DNA Levels in NPC Patients
The plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were significantly greater in NPC patients with stages III or IV than in those with stages I and II, and the plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were significantly greater in NPC patients with stage IV than in those with stage III (P < 0.001) (Figure 3).
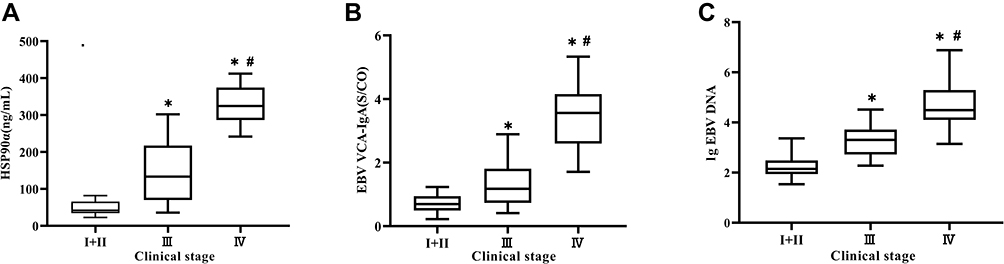 |
Figure 3 Clinical stage-specific plasma HSP90α level, serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA in nasopharyngeal carcinoma patients. (A) plasma HSP90α level; (B) serum EBV VCA IgA antibody titer; (C) plasma viral load of EBV DNA. *P < 0.001 vs stages I and II; #P < 0.05 vs stage III. |
The post-treatment follow-up was terminated until April 2020, and the median follow-up period was 31 months (range, 3 to 44 months). Of the 113 NPC patients, 91 cases with improvements following treatment were assigned to the good prognosis group, and 22 cases with discharge from hospital due to disease aggravation or death were assigned to the poor prognosis group. Lower plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were detected in the good prognosis group post-treatment relative to pretreatment (P < 0.05), and higher plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were seen in the poor prognosis group post-treatment relative to pretreatment (P < 0.05). In addition, significantly lower plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral load of EBV DNA were found in the good prognosis group than in the poor prognosis group post-treatment (P < 0.05) (Figure 4).
 |
Figure 4 Prognosis-specific plasma HSP90α level, serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA in nasopharyngeal carcinoma patients. (A) plasma HSP90α level; (B) serum EBV VCA IgA antibody titer; (C) plasma viral load of EBV DNA. *P < 0.05 vs the pretreatment group; #P < 0.001 vs the good prognosis group. |
Performance of HSP90α, EBV VCA IgA Antibody and EBV DNA for Detection of NPC
The AUC of plasma HSP90α was 0.884 (95% CI: 0.832 to 0.935; P = 0.032), and the HSP90α cut-off of 121.7 ng/mL corresponded to the maximum Youden index of 0.607, which yielded an 85.7% sensitivity and 75% specificity for the diagnosis of NPC. The AUC of serum EBV VCA IgA antibody was 0.841 (95% CI: 0.781 to 0.901; P = 0.058), and the EBV VCA IgA antibody cut-off of 1.84 S/CO corresponded to the maximum Youden index of 0.453, which yielded a 76.5% sensitivity and 68.8% specificity for the diagnosis of NPC. The AUC of plasma EBV DNA was 0.934 (95% CI: 0.897 to 0.97; P = 0.021) for the diagnosis of NPC, and the EBV DNA cut-off of 2.7×103 copies/mL corresponded to the maximum Youden index of 0.692, which yielded an 88.8% sensitivity and 83% specificity for NPC diagnosis. In addition, the AUC of combined plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA was 0.954 (95% CI: 0.907 to 0.982; P = 0.012), and the combined use of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA showed a 92.5% sensitivity and 86% specificity for the diagnosis of NPC (Table 2, Figure 5). Our data showed that plasma EBV DNA presented the highest diagnostic performance, followed by plasma HSP90α, and serum EBV VCA IgA antibody exhibited the lowest diagnostic performance for NPC, and the combination of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA presented a higher diagnostic efficiency for NPC than plasma HSP90α, serum EBV VCA IgA antibody or plasma EBV DNA alone.
 |
Table 2 Diagnostic Performance of Plasma HSP90α, Serum EBV VCA IgA Antibody and Plasma EBV DNA Alone or in Combination for Nasopharyngeal Carcinoma |
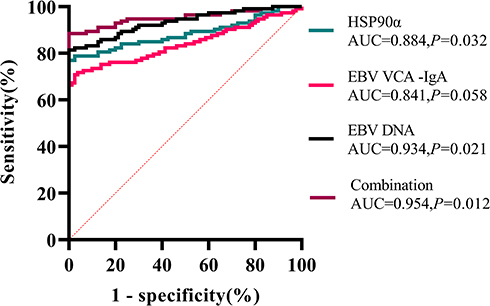 |
Figure 5 Performance of plasma HSP90α level, serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA for the diagnosis of nasopharyngeal carcinoma. Abbreviation: AUC, area under the representative operating curve. |
Prognostic Factors for NPC
During the follow-up period, there were two NPC patients lost to the follow-up, with a follow-up rate of 98.23%. If plasma HSP90α, serum EBV VCA IgA antibody titer and plasma EBV DNA levels were classified into low and expression at cut-off values of 121.7 ng/mL, 1.84 S/CO and 2.7×103 copies/mL, we found a significantly higher OS rate in patients with low HSP90α than in those with high HSP90α (22.8% vs 77.2%; log-rank χ2 = 9.715, P < 0.01), and a significantly lower OS rate in patients with low EBV DNA viral load than in those with high load (24.6% vs 75.4%; log-rank χ2 = 12.805, P < 0.01), while the OS rate was numerically lower in patients with low EBV VCA IgA antibody titer than in those with high titer (32.6% vs 67.4%; log-rank χ2 = 0.805, P > 0.05) (Figure 6).
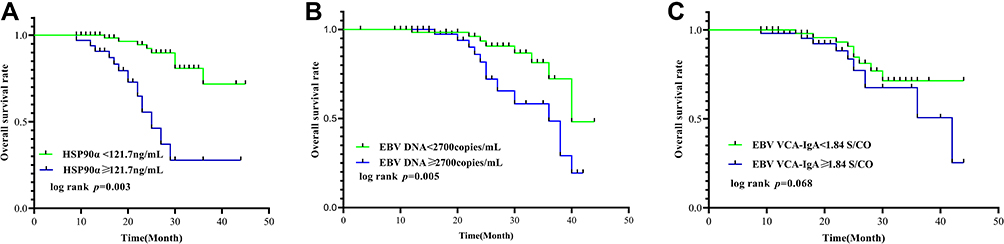 |
Figure 6 Comparison of overall survival among nasopharyngeal carcinoma patients in terms of plasma HSP90α level, serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA. (A) plasma HSP90α level; (B) serum EBV VCA IgA antibody titer; (C) plasma viral load of EBV DNA. |
Then, the Cox proportional hazards regression model was employed to identify the factors affecting OS in NPC patients. Univariate Cox proportional hazards regression analysis revealed that lymph node classification, AJCC clinical stage, number of metastatic sites, pretreatment plasma HSP90α and pretreatment EBV DNA viral load affected the OS in NPC patients (P < 0.05), and multivariate Cox proportional hazards regression analysis identified AJCC clinical stage, number of metastatic sites, pretreatment plasma HSP90α level and pretreatment EBV DNA viral load as independent prognostic factors in NPC patients (P < 0.05) (Table 3).
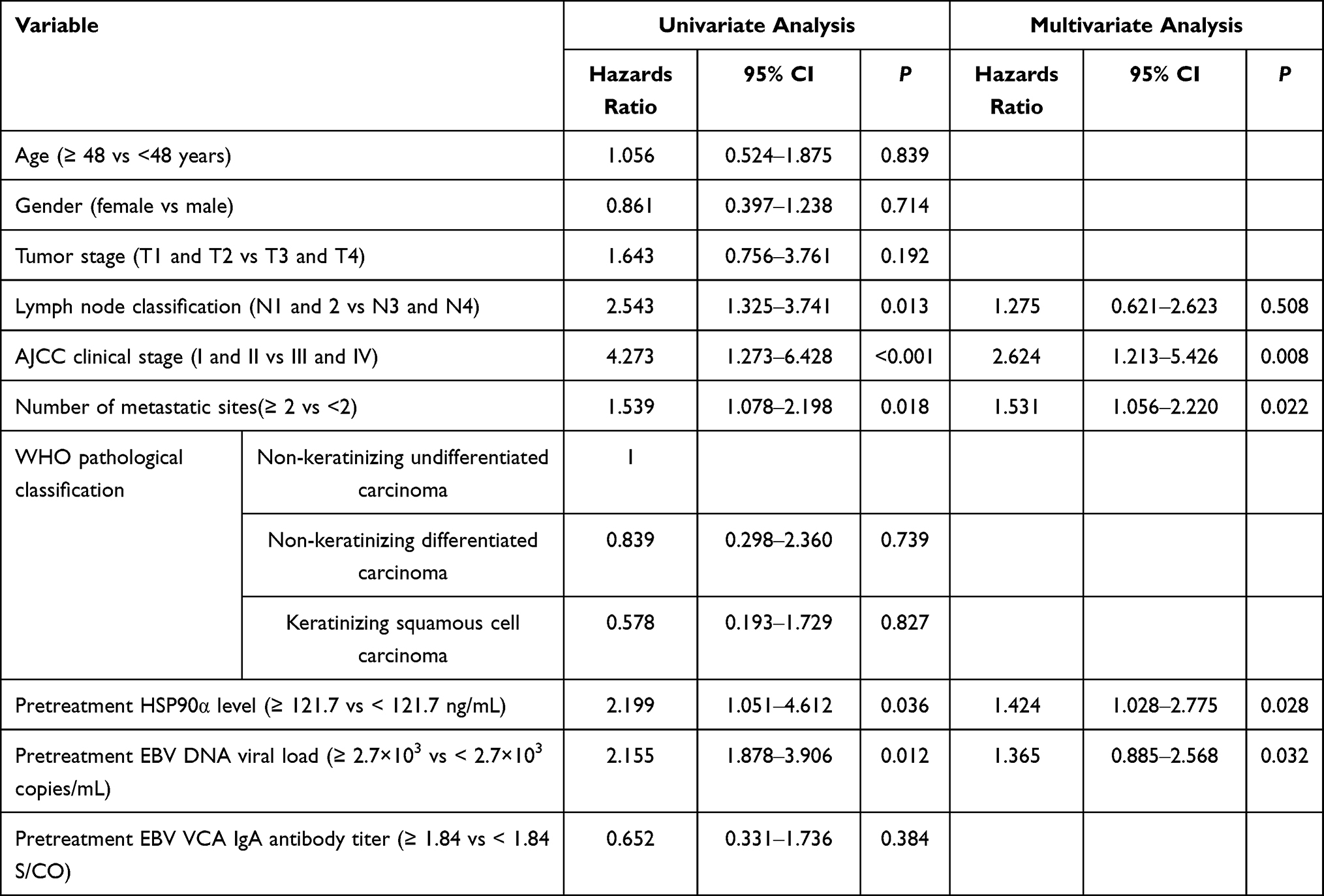 |
Table 3 Univariate and Multivariate Cox Proportional Hazards Regression Analyses of Prognostic Factors of Overall Survival in Nasopharyngeal Carcinoma Patients |
Discussion
NPC presents multiple and non-specific clinical manifestations, and the major clinical symptoms include neck lymph nodes enlargement, hemorrhinia of unknown causes and otological symptoms and signs.1 Since there are no specific early symptoms or signs of NPC, initial diagnosis is very difficult.1 Screening of blood-based tumor biomarkers facilitates the early identification and prevention of cancers.25–27 NPC is an EBV-associated malignancy.5 Currently, EBV VCA-IgA antibody and EBV DNA are the two most common biomarkers used for screening of NPC, and are commonly employed for prognostic prediction and monitoring of therapeutic efficacy; however, these two biomarkers show no apparent values in early diagnosis of NPC.16–18,28,29 In addition, a recent meta-analysis including 2,126 NPC patients and 15,644 controls showed that serum EBV Zta antibody exhibited a high diagnostic accuracy with a sensitivity of 0.85, a specificity of 0.9 and an AUC of 0.94 for NPC.30 Nevertheless, serum EBV Zta antibody is not popular for the identification of NPC in clinical practices.31
Heat shock protein (HSP), also termed stress protein, is a class of proteins that are highly expressed in cells in response to physicochemical stimuli.32 Based on the molecular weight, HSPs are classified into HSP110, HSP90, HSP70, HSP60 and small HSPs (sHSPs).33 HSP90 is only present in the extracellular region, and are classified into two subtypes, HSP90α and HSP90β.34 Under normal physiological conditions, HSP90α is not secreted out of cells; however, it may be secreted into the extracellular region by tumor cells to function.35 In 2009, HSP90α was firstly detected to be highly expressed in the blood of liver cancer patients, and the plasma HSP90α concentration correlated positively with the malignant degree of liver cancer, indicating that HSP90α may serve as a tumor biomarker for early screening of liver cancer.36 In this study, we found significantly greater plasma HSP90α levels, serum EBV VCA IgA antibody titers and plasma viral loads of EBV DNA in patients with NPC than in healthy controls (P < 0.05), suggesting that overexpression of HSP90α, EBV VCA IgA antibody and EBV DNA may be involved in the development of NPC. In highly prevalent areas for NPC, EBV-encoded small RNA (EBER) gene was detected positive in more than 90% of NPC specimens, and plasma EBV DNA was detectable in patients with initial diagnosis of NPC, accompanied by elevated EBV VCA IgA antibody levels.37 As a serum tumor biomarker,38 HSP90 is highly expressed in gastric cancer, liver cancer and colorectal cancer, and plays a vital role in promoting tumor invasion, metastasis, progression and angiogenesis and inhibiting the apoptosis of tumor cells.39–41 The mechanisms underlying elevated HSP90α levels remain unknown in patients with NPC until now. It is considered that tumor cells may overexpress epidermal growth factor receptor (EGFR) and signal transduction proteins PI3K and AKT, and HSP90 binds to and stabilize these proteins to protect tumor cells from apoptosis.42 HSP90 was found to participate in tumor cell growth and angiogenesis via the HIF-1α/VEGF/VEGFR-2 signaling,43 and activate oncogenic ERK1/2 in NPC cells and phosphorylate ERK1/2 and AKT to promote cell proliferation.44 In addition, overexpression of HSP90 and HIF-1α has been reported to serve as novel independent biomarkers for poor prognosis in patients with NPC.45 These data demonstrate that HSP90α participates in tumor development and progression and may be used as a diagnostic marker for NPC.
In this study, NPC patients with AJCC clinical stages I and II were pooled because of the small sample size of patients with stage I. We found that the plasma HSP90α levels, EBV VCA IgA antibody titers and the viral load of EBV DNA increased with the stage of NPC (P < 0.05), and high plasma HSP90α levels were found to correlate with advanced stage and high viral load of EBV DNA in NPC patients, indicating that elevated HSP90α and EBV DNA viral load are associated with NPC progression. Previous studies have shown no correlation between the viral load of EBV DNA and levels of serum antibodies against EBV in NPC patients.46,47 In the present study, we detected a correlation between the plasma viral load of EBV DNA and serum IgA antibody against EBV VCA, indicating that the viral load of EBV DNA appears a tendency towards a rise with an increase in the serum EBV VCA IgA antibody titer. Our findings demonstrate a high concordance among HSP90α, EBV VCA IgA antibody and EBV DNA for the diagnosis of NPC, indicating high serum EBV VCA IgA antibody titers and plasma HSP90α levels in NPC patients with high viral loads of EBV DNA.
In this study, a lower OS rate and shorter median survival period were observed in NPC patients with high HSP90α and EBV DNA viral load than in those with low levels, and univariate and multivariate Cox proportional hazards regression analyses showed pretreatment HSP90α and EBV DNA viral load were independent prognostic factors in NPC patients, demonstrating that HSP90α and EBV DNA may be a promising potential for prediction of prognosis. Pearson correlation analysis revealed that plasma HSP90α level correlated positively with the serum EBV VCA IgA antibody titer and plasma viral load of EBV DNA, and a stronger correlation was seen between EBV DNA viral load and plasma HSP90α level that between plasma HSP90α level and serum EBV VCA IgA antibody titer in patients with NPC. It was reported that HSP90α level correlated with the stage, disease progression and timing of surgical treatment in liver cancer patients.48 Our data showed a remarkable decline in HSP90α level among NPC patients with a good prognosis, and the plasma HSP90α level increased with the disease severity, suggesting that elevated HSP90α level may predict the migration or aggravation of NPC. In addition, our findings confirm that HSP90α has a potential as a biomarker for NPC, and high HSP90α level may trigger tumor development and progression. In vivo and in vitro assays have shown that HSP90 contributes to the development of primary breast cancer,49 and HSP90 was found to be predictive of breast cancer and HSP90 expression correlates positively with the progression of breast cancer.50 There is also evidence showing that HSP90 overexpression correlates positively with the metastasis and poor prognosis of gastrointestinal and lung cancers.51,52 In both cell assays and tumor growth xenograft models, AT13387, a novel HSP90 inhibitor, was found to suppress tumor development and progression, which may serve a new agent against NPC.53 Taken these finding together, it is considered that HSP90α may serve as diagnostic and prognostic biomarkers for NPC.
In the current study, plasma EBV DNA showed the highest performance for the diagnosis of NPC, followed by plasma HSP90α, while serum EBV VCA IgA antibody exhibited the lowest diagnostic performance. Our data demonstrate that both EBV DNA and plasma HSP90α exhibit higher performance for the diagnosis of NPC than serum EBV VCA IgA antibody, which was in agreement with previous studies reporting a higher diagnostic efficacy of EBV DNA than serum EBV VCA IgA antibody for NPC.54 In addition, serum EBV Zta antibody was also found to present a high diagnostic accuracy for NPC30; however, there have been no comparisons of the performance between plasma HSP90α and serum EBV Zta antibody for the diagnosis of NPC until now. Previous studies have shown that the combination of multiple biomarkers may increase the detection of cancers.16,55 Similarly, our data show that the combination of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA increased the diagnostic efficacy of NPC than plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA alone.
Our study has some limitations. First, the sample size is relatively small, which may cause some bias. Second, only plasma HSP90α was detected. Further studies recruiting more samples to detect the relative HSP90α expression in NPC specimens are required to unravel the correlation between HSP90α expression and the prognosis in NPC patients.
In summary, the results of the present study demonstrate elevated HSP90α in NPC patients, and high HSP90α level correlates with the severity and poor prognosis in patients with NPC, and univariate and multivariate Cox proportional hazards regression analyses identify HSP90α as an independent prognostic factor for NPC. It is considered that plasma HSP90α may be a potential marker for diagnosis and prognosis prediction of NPC. In addition, the combination of plasma HSP90α, serum EBV VCA IgA antibody and plasma EBV DNA shows high diagnostic performance for NPC. Our findings provide novel insights into the diagnosis of NPC.
Acknowledgments
The authors would like to thank all participants and the reviewers. This study was supported by the Joint Funds for the Innovation of Science and Technology, Fujian province (Grant number: 2017Y9072), and Science and Technology Program of Fujian Province, China (Grant number: 2018Y2003).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chen YP, Chan ATC, Le QT, et al. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/S0140-6736(19)30956-0
2. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Petersson F. Nasopharyngeal carcinoma: a review. Semin Diagn Pathol. 2015;32(1):54–73.
4. Lee HM, Okuda KS, González FE, Patel V. Current perspectives on nasopharyngeal carcinoma. Adv Exp Med Biol. 2019;1164:11–34.
5. Tsao SW, Tsang CM, Lo KW. Epstein-Barr virus infection and nasopharyngeal carcinoma. Philos Trans R Soc B Biol Sci. 2017;72(1732):20160270. doi:10.1098/rstb.2016.0270
6. Bei JX, Li Y, Jia WH, et al. A genome-wide association study of nasopharyngeal carcinoma identifies three new susceptibility loci. Nat Genet. 2010;42(7):599–603. doi:10.1038/ng.601
7. Lam WKJ, Chan JYK. Recent advances in the management of nasopharyngeal carcinoma. F1000Res. 2018;7:F1000 Faculty Rev-1829. doi:10.12688/f1000research.15066.1
8. Lee AW, Ma BB, Ng WT, et al. Management of nasopharyngeal carcinoma: current practice and future perspective. J Clin Oncol. 2015;33(29):3356–3364. doi:10.1200/JCO.2015.60.9347
9. Sun XS, Li XY, Chen QY, et al. Future of radiotherapy in nasopharyngeal carcinoma. Br J Radiol. 2019;92(1102):20190209. doi:10.1259/bjr.20190209
10. Guan S, Wei J, Huang L, et al. Chemotherapy and chemo-resistance in nasopharyngeal carcinoma. Eur J Med Chem. 2020;207:112758. doi:10.1016/j.ejmech.2020.112758
11. Farias TP, Dias FL, Lima RA, et al. Prognostic factors and outcome for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg. 2003;129(7):794–799. doi:10.1001/archotol.129.7.794
12. Paul P, Deka H, Malakar AK, et al. Nasopharyngeal carcinoma: understanding its molecular biology at a fine scale. Eur J Cancer Prev. 2018;27(1):33–41. doi:10.1097/CEJ.0000000000000314
13. Ens EAR, Irekeola AA, Yean Yean C. Diagnostic and prognostic indications of nasopharyngeal carcinoma. Diagnostics. 2020;10(9):611. doi:10.3390/diagnostics10090611
14. Liu Z, Yu KJ, Coghill AE, et al. Multilaboratory assessment of Epstein-Barr virus serologic assays: the case for standardization. J Clin Microbiol. 2019;57(11):e01107–e01119. doi:10.1128/JCM.01107-19
15. Chen Y, Zhao W, Lin L, et al. Nasopharyngeal Epstein-Barr virus load: an efficient supplementary method for population-based nasopharyngeal carcinoma screening. PLoS One. 2015;10(7):e0132669. doi:10.1371/journal.pone.0132669
16. Guo J, Cui Z, Zheng Y, et al. Comparison of Epstein-Barr virus serological tools for the screening and risk assessment of nasopharyngeal carcinoma: a large population-based study. Pathol Oncol Res. 2020;26(4):2185–2190. doi:10.1007/s12253-020-00808-0
17. Li S, Deng Y, Li X, et al. Diagnostic value of Epstein-Barr virus capsid antigen-IgA in nasopharyngeal carcinoma: a meta-analysis. Chin Med J. 2010;123(9):1201–1205.
18. Chen Y, Xin X, Cui Z, et al. Diagnostic value of serum Epstein-Barr virus capsid antigen-IgA for nasopharyngeal carcinoma: a meta-analysis based on 21 studies. Clin Lab. 2016;62(6):1155–1166. doi:10.7754/Clin.Lab.2015.151122
19. Tan LP, Tan GW, Sivanesan VM, et al. Systematic comparison of plasma EBV DNA, anti-EBV antibodies and miRNA levels for early detection and prognosis of nasopharyngeal carcinoma. Int J Cancer. 2020;146(8):2336–2347. doi:10.1002/ijc.32656
20. Chan KCA, Woo JKS, King A, et al. Analysis of plasma Epstein-Barr virus DNA to screen for nasopharyngeal cancer. N Engl J Med. 2017;377(6):513–522. doi:10.1056/NEJMoa1701717
21. Mao M, Wang X, Sheng H, et al. Heat shock protein 90α provides an effective and novel diagnosis strategy for nasopharyngeal carcinoma. Adv Ther. 2021;38(1):413–422. doi:10.1007/s12325-020-01518-4
22. Puri KS, Suresh KR, Gogtay NJ, et al. Declaration of Helsinki, 2008: implications for stakeholders in research. J Postgrad Med. 2009;55(2):131–134. doi:10.4103/0022-3859.52846
23. Wei KR, Xu Y, Liu J, et al. Histopathological classification of nasopharyngeal carcinoma. Asian Pac J Cancer Prev. 2011;12(5):1141–1147.
24. Guo R, Mao YP, Tang LL, et al. The evolution of nasopharyngeal carcinoma staging. Br J Radiol. 2019;92(1102):20190244. doi:10.1259/bjr.20190244
25. Kang H, Kiess A, Chung CH. Emerging biomarkers in head and neck cancer in the era of genomics. Nat Rev Clin Oncol. 2015;12(1):11–26. doi:10.1038/nrclinonc.2014.192
26. Zhang SQ, Pan SM, Liang SX, et al. Research status and prospects of biomarkers for nasopharyngeal carcinoma in the era of high‑throughput omics. Int J Oncol. 2021;8(4):9. doi:10.3892/ijo.2021.5188
27. Ma BBY, Chen YP, Hui EP, et al. Recent advances in the development of biomarkers and chemoradiotherapeutic approaches for nasopharyngeal carcinoma. Am Soc Clin Oncol Educ Book. 2020;40:1–11. doi:10.1200/EDBK_280747
28. Gao R, Wang L, Liu Q, et al. Evaluation of seven recombinant VCA-IgA ELISA kits for the diagnosis of nasopharyngeal carcinoma in China: a case-control trial. BMJ Open. 2017;7(6):e013211. doi:10.1136/bmjopen-2016-013211
29. Fung SY, Lam JW, Chan KC. Clinical utility of circulating Epstein-Barr virus DNA analysis for the management of nasopharyngeal carcinoma. Chin Clin Oncol. 2016;5(2):18. doi:10.21037/cco.2016.03.07
30. Zhang G, Li Z, Zhou Q. Utility of serum EB virus Zta antibody in the diagnostic of nasopharyngeal carcinoma: evidences from 2,126 cases and 15,644 controls. Front Oncol. 2019;9:1391. doi:10.3389/fonc.2019.01391
31. Feng Y, Xia W, He G, et al. Accuracy evaluation and comparison of 14 diagnostic markers for nasopharyngeal carcinoma: a meta-analysis. Front Oncol. 2020;10:1779. doi:10.3389/fonc.2020.01779
32. Martine P, Rébé C. Heat shock proteins and iInflammasomes. Int J Mol Sci. 2019;20(18):4508. doi:10.3390/ijms20184508
33. Li Z, Srivastava P. Heat-shock proteins. Curr Protoc Immunol. 2004. doi:10.1002/0471142735.ima01ts58
34. Zuehlke AD, Moses MA, Neckers L. Heat shock protein 90: its inhibition and function. Philos Trans R Soc B Biol Sci. 2018;373(1738):20160527. doi:10.1098/rstb.2016.0527
35. Hoter A, El-Sabban ME, Naim HY. The HSP90 family: structure, regulation, function, and implications in health and disease. Int J Mol Sci. 2018;19(9):2560. doi:10.3390/ijms19092560
36. Wang X, Song X, Zhuo W, et al. The regulatory mechanism of Hsp90alpha secretion and its function in tumor malignancy. Proc Natl Acad Sci U S A. 2009;106(50):21288–21293. doi:10.1073/pnas.0908151106
37. Zeng Z, Fan S, Zhang X, et al. Epstein-Barr virus-encoded small RNA 1 (EBER-1) could predict good prognosis in nasopharyngeal carcinoma. Clin Transl Oncol. 2016;18(2):206–211. doi:10.1007/s12094-015-1354-3
38. Trepel J, Mollapour M, Giaccone G, et al. Targeting the dynamic HSP90 complex in cancer. Nat Rev Cancer. 2010;10(8):537–549. doi:10.1038/nrc2887
39. Lee HW, Kim KM. Clinical significance of heat shock protein 90α expression as a biomarker of prognosis in patients with gastric cancer. Niger J Clin Pract. 2019;22(12):1698–1705. doi:10.4103/njcp.njcp_68_19
40. Nouri-Vaskeh M, Alizadeh L, Hajiasgharzadeh K, et al. The role of HSP90 molecular chaperones in hepatocellular carcinoma. J Cell Physiol. 2020;235(12):9110–9120. doi:10.1002/jcp.29776
41. Kasanga M, Liu L, Xue L, et al. Plasma heat shock protein 90-alpha have an advantage in diagnosis of colorectal cancer at early stage. Biomark Med. 2018;12(8):881–890. doi:10.2217/bmm-2018-0155
42. Ye M, Huang W, Wu WW, et al. FM807, a curcumin analogue, shows potent antitumor effects in nasopharyngeal carcinoma cells by heat shock protein 90 inhibition. Oncotarget. 2017;8(9):15364–15376. doi:10.18632/oncotarget.14970
43. Zhang PC, Liu X, Li MM, et al. AT-533, a novel Hsp90 inhibitor, inhibits breast cancer growth and HIF-1α/VEGF/VEGFR-2-mediated angiogenesis in vitro and in vivo. Biochem Pharmacol. 2020;172:113771. doi:10.1016/j.bcp.2019.113771
44. Liu F, Wang L, Yi S, et al. Clinical and biological significances of heat shock protein 90 (Hsp90) in human nasopharyngeal carcinoma cells and anti-cancer effects of Hsp90 inhibitor. Biomed Pharmacother. 2019;120:109533. doi:10.1016/j.biopha.2019.109533
45. Feng J, Xie G, Zhan Y, et al. Elevated HSP90 associates with expression of HIF-1α and p-AKT and is predictive of poor prognosis in nasopharyngeal carcinoma. Histopathology. 2019;75(2):202–212. doi:10.1111/his.13862
46. Song C, Yang S. A meta-analysis on the EBV DNA and VCA-IgA in diagnosis of nasopharyngeal carcinoma. Pak J Med Sci. 2013;29(3):885–890. doi:10.12669/pjms.293.2907
47. Liu W, Chen G, Gong X, et al. The diagnostic value of EBV-DNA and EBV-related antibodies detection for nasopharyngeal carcinoma: a meta-analysis. Cancer Cell Int. 2021;1(1):164. doi:10.1186/s12935-021-01862-7
48. Fu Y, Xu X, Huang D, et al. Plasma heat shock protein 90alpha as a biomarker for the diagnosis of liver cancer: an official, large-scale, and multicenter clinical trial. EBioMedicine. 2017;24:56–63. doi:10.1016/j.ebiom.2017.09.007
49. Stivarou T, Stellas D, Vartzi G, et al. Targeting highly expressed extracellular HSP90 in breast cancer stem cells inhibits tumor growth in vitro and in vivo. Cancer Biol Ther. 2016;17(8):799–812. doi:10.1080/15384047.2016.1195041
50. Klimczak M, Biecek P, Zylicz A, et al. Heat shock proteins create a signature to predict the clinical outcome in breast cancer. Sci Rep. 2019;9(1):7507. doi:10.1038/s41598-019-43556-1
51. Zhang Y, Ni L, Li Q, et al. Diagnostic, clinicopathologic, therapeutic and prognostic value of plasma heat shock protein 90 levels in patients with advanced gastrointestinal carcinoma. J Cancer. 2020;11(20):5890–5899. doi:10.7150/jca.46343
52. Mittal S, Rajala MS. Heat shock proteins as biomarkers of lung cancer. Cancer Biol Ther. 2020;21(6):477–485. doi:10.1080/15384047.2020.1736482
53. Chan KC, Ting CM, Chan PS, et al. A novel Hsp90 inhibitor AT13387 induces senescence in EBV-positive nasopharyngeal carcinoma cells and suppresses tumor formation. Mol Cancer. 2013;12(1):128. doi:10.1186/1476-4598-12-128
54. Kondo S, Horikawa T, Takeshita H, et al. Diagnostic value of serum EBV-DNA quantification and antibody to viral capsid antigen in nasopharyngeal carcinoma patients. Cancer Sci. 2004;95(6):508–513. doi:10.1111/j.1349-7006.2004.tb03241.x
55. Luo YL, Chen H, Peng SG, et al. Assessment of detection assays of Epstein-Barr viral Rta-IgG, VCA-IgA, EA-IgA and Epstein-Barr viral DNA at different clinical stages in the diagnosis of nasopharyngeal carcinoma. Zhonghua Yi Xue Za Zhi. 2013;93(44):3516–3519.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.