Back to Journals » Infection and Drug Resistance » Volume 19
Performance Characteristics of Real-Time Quantitative PCR and Cycle Threshold (Ct) Values for the Diagnosis of Pneumocystis jirovecii pneumonia in Hospitalized Patients
Authors Cao G, Wang D, Shi X, Ru J, Chen Y, Lu Z
Received 21 November 2025
Accepted for publication 28 January 2026
Published 7 February 2026 Volume 2026:19 577623
DOI https://doi.org/10.2147/IDR.S577623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Guomei Cao, Dan Wang, Xiaodi Shi, Jincheng Ru, Yafang Chen, Zhiyong Lu
Department of Clinical Laboratory, Shaoxing University Affiliated Central Hospital, Shaoxing, Zhejiang, People’s Republic of China
Correspondence: Zhiyong Lu, Department of Clinical Laboratory, Shaoxing University Affiliated Central Hospital, No. 1 Huayu Road, Shaoxing, Zhejiang, 312000, People’s Republic of China, Email [email protected] Guomei Cao, Department of Clinical Laboratory, Shaoxing University Affiliated Central Hospital, No. 1 Huayu Road, Shaoxing, Zhejiang, 312000, People’s Republic of China, Email [email protected]
Purpose: Pneumocystis jirovecii pneumonia (PCP) is a critical opportunistic infection that predominantly affects immunocompromised patients, particularly those with underlying diseases, and leads to significant morbidity and mortality. This study aimed to enhance the diagnostic accuracy and treatment strategies for PCP by investigating the clinical and laboratory characteristics of patients with suspected PCP and focusing on the diagnostic performance of qPCR and Cycle Threshold (Ct) values.
Patients and Methods: We retrospectively analyzed the clinical and laboratory data of 249 patients at the Central Hospital of Shaoxing University between 2024 and 2025. Clinical characteristics, qPCR test performance, and Ct values were compared between these PCP diagnostic groups, revealing that 8 were classified as definite cases, 32 as probable, and 88 as non-PCP.
Results: The definite group exhibited significantly lower lymphocyte percentages and counts than the probable and non-PCP groups (P =0.003 and P =0.009, respectively). Additionally, beta-d-glucan (BDG) levels were elevated in the definite group (p< 0.001), indicating their potential as reliable biomarkers for PCP diagnosis. The qPCR assay demonstrated high sensitivity (95%) and specificity (99%) in detecting PCP between the PCP and non-PCP groups, with an optimal cut-off Ct value of 35.305 (area under the curve (AUC)=0.98). Correlations among Ct values, lymphocyte percentages, and lactate dehydrogenase (LDH) levels were observed, underscoring the prognostic implications of these laboratory parameters.
Conclusion: Our findings support the integration of qPCR Ct values and BDG in clinical settings to refine the diagnostic criteria and enhance patient management strategies for PCP, paving the way for further research on additional biomarkers and their roles in prognostic assessments.
Keywords: qPCR, cycle threshold Ct values, Pneumocystis jirovecii pneumonia, clinical indicators
Introduction
PCP is a critical opportunistic infection that primarily affects immunocompromised individuals, particularly those with underlying disease. The burden of PCP on healthcare systems is significant, as it is associated with high morbidity and mortality rates, which translate into increased hospitalization costs and prolonged treatment durations.1 Despite advancements in antiretroviral therapy, PCP remains the leading cause of opportunistic infections in patients with HIV, underscoring the need for effective diagnostic and therapeutic strategies to manage this condition.2
Current diagnostic approaches, including microscopy and serum beta-D-glucan (BDG) testing, present challenges such as false negatives and delays in definitive diagnosis.3,4 Although qPCR has demonstrated improved sensitivity and specificity in detecting Pneumocystis jirovecii, further exploration is required to optimize these methods and enhance their diagnostic performance.5 Additionally, the distinction between PCP and other respiratory infections is often challenging, necessitating a refined understanding of clinical and laboratory characteristics to improve diagnostic accuracy.6
Polymerase chain reaction (PCR) is a highly sensitive and specific technique for detecting Pneumocystis jirovecii DNA in respiratory samples, offering an advantage in diagnosis.3–5 However, not all patients with a positive qPCR test for Pneumocystis jirovecii necessarily have PCP. Asymptomatic colonization of Pneumocystis jirovecii, detected by qPCR in uninfected individuals is relatively common.7 Therefore, positive qPCR results in such patients should be interpreted with caution as they do not definitively indicate PCP. Several studies using quantitative PCR have proposed threshold values for the molecular diagnosis of Pneumocystis jirovecii infection.8–10 Despite this potential, the precise clinical utility of qPCR, particularly the use of Ct values in diagnosing PCP, along with its standardization, requires further investigation.
By evaluating the diagnostic accuracy of qPCR, this study aimed to establish cut-off values that differentiate between various clinical categories of PCP. Ultimately, the objectives are to enhance clinical decision making and improve patient outcomes through more accurate diagnostic strategies.
In summary, addressing the challenges associated with PCP diagnosis and treatment is vital for improving the care of immunocompromised patients. The integration of novel diagnostic technologies and biomarkers, along with a thorough evaluation of existing clinical data, offers the potential to advance our understanding of PCP and optimize management strategies for affected individuals.2,6
Materials and Methods
Study Design and Subjects
We conducted a retrospective study by analyzing clinical and laboratory data from electronic medical records, including diagnostic test results for PCP, to evaluate patients with suspected PCP. This study enrolled 249 patients hospitalized in our institution between January 15, 2024, and September 15, 2025, with a diagnosis of respiratory tract infection. All patients underwent respiratory specimen testing including cytological staining and qPCR for Pneumocystis jirovecii. Comprehensive clinical diagnosis of PCP or non-PCP was based on the revised EORTC/MSGERC 2020 criteria for invasive fungal disease11 incorporating clinical symptoms, laboratory findings, microbiological tests, chest imaging features, and treatment response. To minimize bias, the final diagnosis was determined by two senior pulmonologists after discussion with the medical team. The study was reviewed and approved by the Medical Ethics Committee of the Shaoxing University Affiliated Central Hospital (202529001). And all patients signed the informed consent for participation. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Definitions
PCP diagnosis was categorized as “Definite”, “Probable”, or “Non-PCP” by two independent infectious disease specialists based on the following criteria:
Definite: Suggestive clinical manifestations and/or radiographic features + positive microscopic examination for PCP.
Probable: Suggestive clinical and radiographic features with negative microscopic examination for PCP + response to anti-PCP therapy and no alternative diagnosis (without reference to qPCR results).
Non-PCP: Failure to meet the criteria for either Definite or Probable PCP.
This classification aligns with international guidelines, which universally require identification of the organism using specific staining methods for “ definite diagnosis of PCP. The definition of “Probable PCP” was based on guidelines of the European AIDS Society guidelines.11
Laboratory Methods
Microscopic Examination for Pneumocystis Jirovecii
Bronchoalveolar lavage (BAL) samples from patients suspected of having PCP were stained for Pneumocystis jirovecii according to the standard protocol of our hospital. After centrifugation, the specimens were smeared onto slides, stained using the Grocott’s methenamine silver (GMS) stain method, and examined microscopically by senior laboratory technologists.
qPCR Assay
A commercial quantitative PCR assay kit (Beijing ZC Bio-Tech Co., Ltd., China) was used for the detection of Pneumocystis jirovecii. The assay employs specific primers and a TaqMan probe targeting the conserved region of the mitochondrial large subunit ribosomal RNA (mtLSU rRNA) gene.
Specimen Pre-Treatment
Sputum or bronchoalveolar lavage fluid (BALF) samples were aliquoted into 50 mL screw‑capped tubes. Depending on viscosity, 3–10 mL of 4% NaOH digestion solution was added. Tubes were vortexed for 1 min and incubated at room temperature in a biological safety cabinet for 15–20 min to ensure complete liquefaction.
DNA Extraction
Nucleic acids were extracted from 200 µL of each processed sample using the Magnetic Bead Nucleic Acid Extraction Kit (DAAN GENE Co., Ltd., China) according to the manufacturer’s protocol. Extractions were performed on an automated extraction system (DAAN GENE Co., Ltd., China). A recombinant plasmid containing the target mtLSU rRNA fragment was used as the positive control, and nuclease‑free water served as the negative control.
qPCR Amplification
Each 50 µL reaction contained 10 µL of extracted DNA and 40 µL of PCR master mix (35 µL amplification mix + 5 µL primer‑probe mix). Reactions were run in duplicate on an ABI 7500 Real‑Time PCR System (Applied Biosystems, USA) under the following cycling conditions:
Step 1: 50 °C for 2 min, then 95 °C for 5 min (1 cycle).
Step 2: 95 °C for 15s, 60 °C for 45s (signal acquisition), 40 cycles.
Interpretation
According to the reagent instructions, the Ct value<36 was considered positive, provided that the positive control showed a Ct within the expected range and the negative control yielded no amplification signal.
Sequencing Verification
To validate the specificity of the qPCR assay, randomly selected positive qPCR products were sent to a third-party testing laboratory (Sangon Biotech Shanghai Co., Ltd.) for confirmation via sequencing.
Clinical and Laboratory Data
Demographic characteristics, clinical manifestations, and laboratory findings were obtained from patients’ medical records (Table 1). Laboratory data included microscopic examination results for Pneumocystis jirovecii in bronchoalveolar lavage (BAL) samples, Pneumocystis jirovecii qPCR results, and the corresponding Ct values.
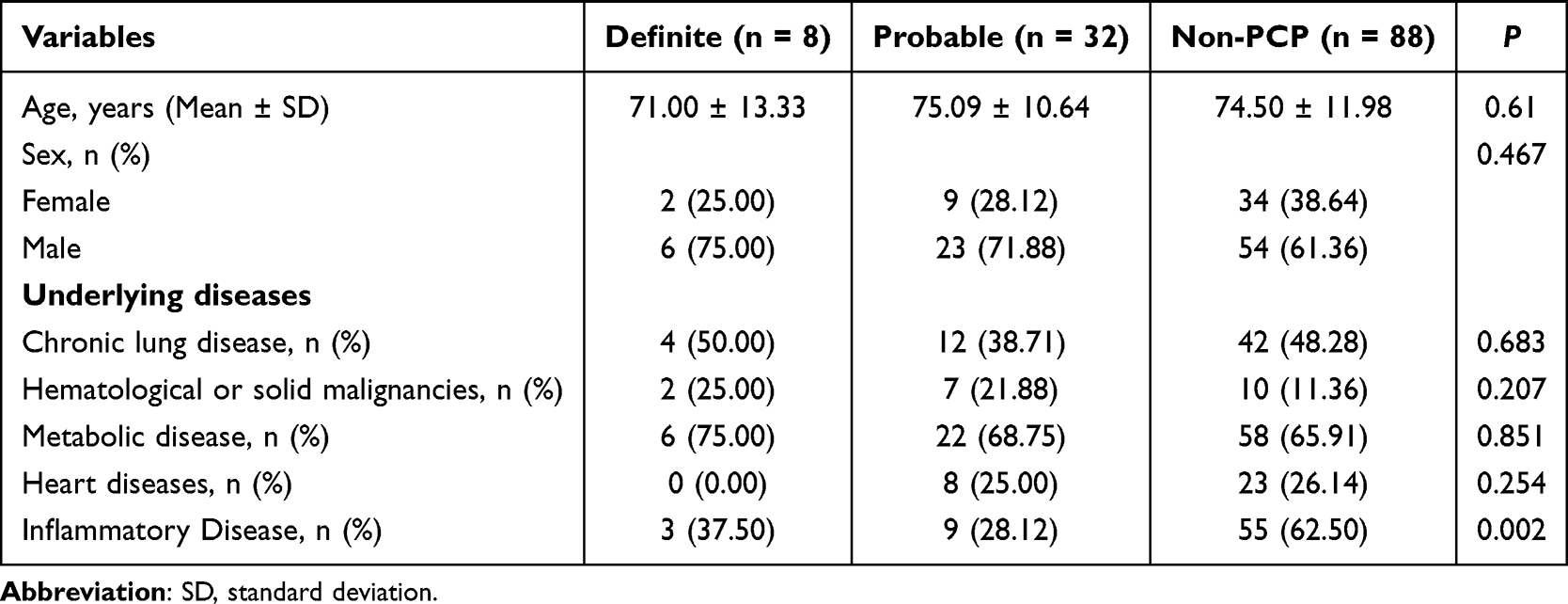 |
Table 1 Clinical Characteristics of Patients |
Statistical Analysis
Data processing and analysis were performed using R version 4.4.0, along with Zstats 1.0 (https://www.zstats.net).
Associations between categorical variables were analyzed using the chi-squared test and Fisher’s exact test, whereas associations involving continuous variables were assessed using the Kruskal–Wallis test, t-test, and Mann–Whitney test. To determine the optimal Ct value for distinguishing between different diagnostic groups, a receiver operating characteristic (ROC) curve analysis was performed. The relationship between the Ct values and laboratory parameters was evaluated using Pearson’s correlation analysis. All tests were two-sided, and statistical significance was set at p < 0.05.
Results
In total, 249 patients with a clinical suspicion of PCP were enrolled in our study. Of these, 128 patients were categorized based on final comprehensive clinical diagnoses into three groups: definite PCP (n = 8), probable PCP (n = 32), and non-PCP (n = 88) (Figure 1). A definite case was defined by the detection of Pneumocystis jirovecii under oil immersion microscopy (Figure 2A). Furthermore, for verification, Sanger sequencing was performed on randomly selected PCR-positive samples from both the definite and probable groups, and the results showed alignment consistency with the BLAST database (Figure 2B and C).
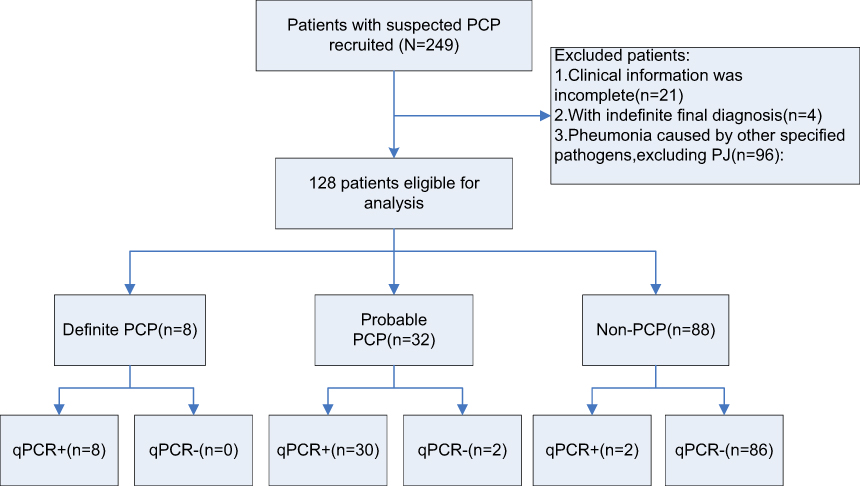 |
Figure 1 The flowchart of the study. |
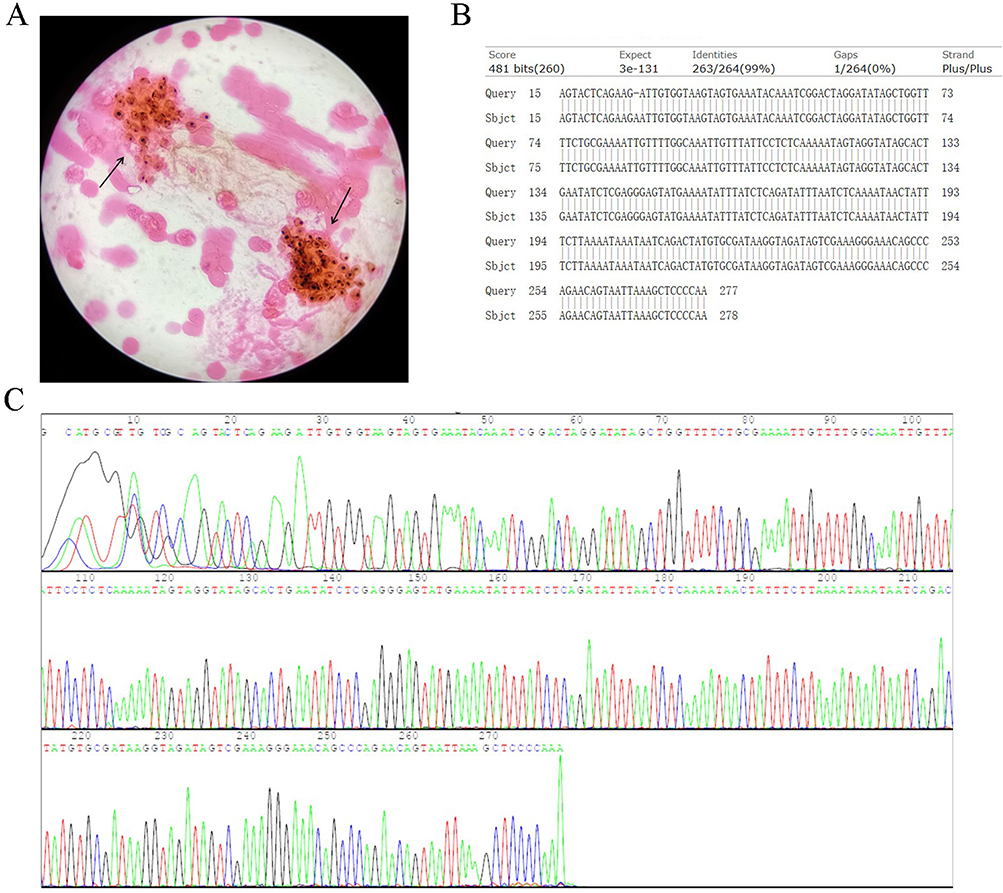 |
Figure 2 Laboratory Diagnostic Methods for Pneumocystis jirovecii. (A) Grocott’s methenamine silver stain of a bronchoalveolar lavage fluid sample, showing characteristic cysts of Pneumocystis jirovecii (arrow). Original magnification: ×1000. (B) BLAST alignment of the sequenced amplicon against the nucleotide database, confirming its identity as Pneumocystis jirovecii. (C) representative chromatogram of Sanger Sequencing. |
Among these 128 analyzed patients, 45 (35.16%) were female and 83 (64.84%) were male. Significant differences were observed among the groups for several clinical variables. The prevalence of underlying inflammatory diseases differed significantly (p=0.002), with 3 cases (37.5%) in the definite group, 9 (28.1%) in the probable group, and 55 (62.5%) in the non-PCP group. However, no significant differences were found in the prevalence of chronic lung disease (p=0.683), hematological or solid malignancies (p=0.207), metabolic disease (p=0.851), or heart disease (p=0.254) (Table 1).
Patients in the definite PCP group demonstrated characteristic alterations in key inflammatory and immunological parameters. Serum BDG levels were significantly elevated in the definite PCP group (133.67, 95% CI: 13.42 to 253.92), being substantially higher than those in the probable PCP group (39.21, 95% CI: 37.42 to 41.00) and the non-PCP group (38.78, 95% CI: 36.01 to 41.55) (p < 0.001) (Figure 3A). Concurrently, the definite PCP group showed a markedly lower lymphocyte percentage (5.25, 95% CI: 2.90 to 7.60) compared with the probable PCP group (13.53, 95% CI: 11.94 to 15.12) and the non-PCP group (18.69, 95% CI: 13.84 to 23.54) (p = 0.003) (Figure 3B). The absolute lymphocyte count was also significantly reduced in the definite PCP group (0.51, 95% CI: 0.30 to 0.72) relative to the probable PCP group (0.95, 95% CI: 0.85 to 1.05) and the non-PCP group (1.19, 95% CI: 0.93 to 1.45) (p = 0.009) (Figure 3C). In contrast, no statistically significant difference was observed in LDH levels among the three groups (p = 0.587) (Figure 3D). These quantitative differences further confirm that confirmed Pneumocystis jirovecii infection exhibits a distinct immunopathological profile characterized by concurrent immunosuppression and inflammatory activation.
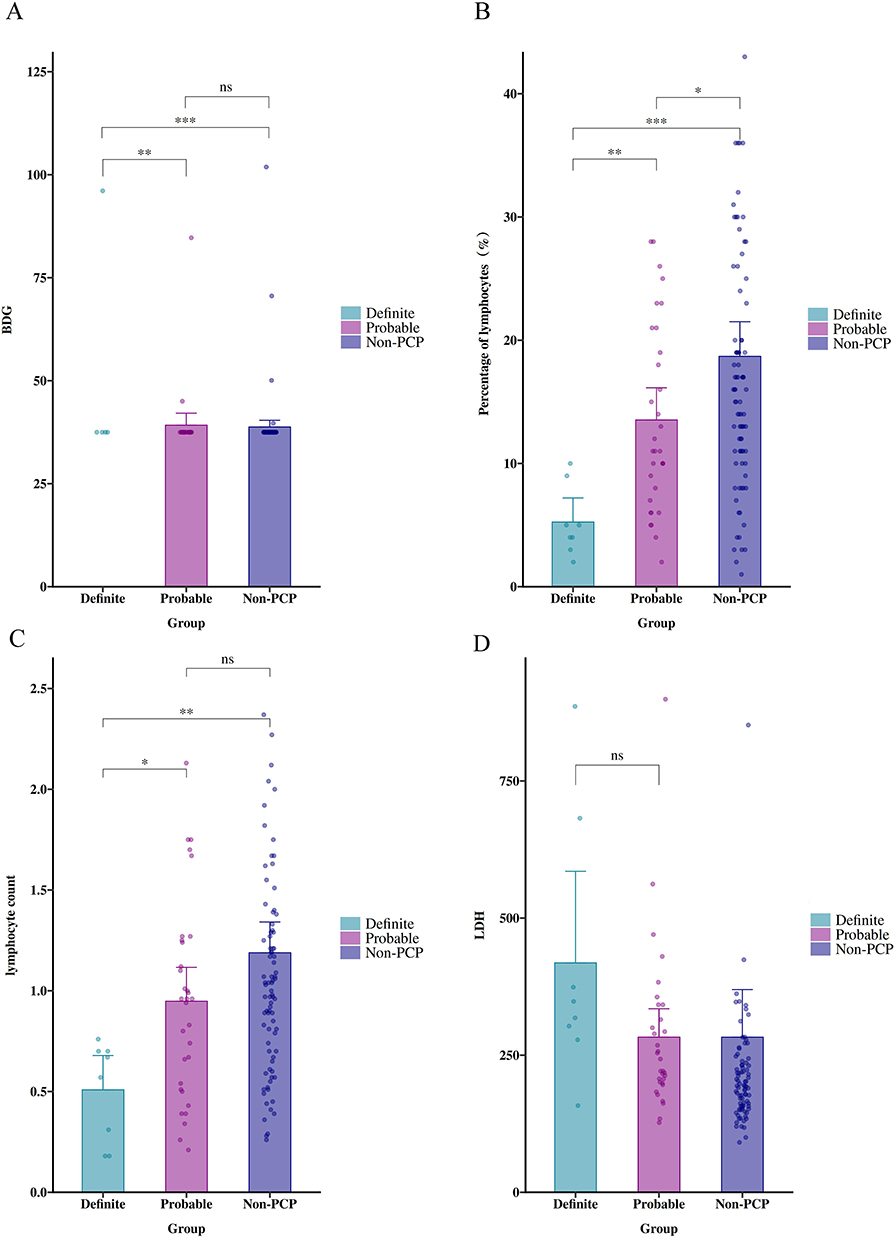 |
Figure 3 Comparison of key laboratory parameters among patients in the definite PCP, probable PCP, and non-PCP groups. (A–D) Comparisons of serum BDG levels, lymphocyte percentage, absolute lymphocyte count, and LDH levels among the three groups. Data are expressed as mean (95% CI). *p < 0.05, **p < 0.01, ***p < 0.001; ns, not significant. |
Forty patients in the study group had positive qPCR results, including eight “definite” cases, thirty “probable” cases, and two “non-PCP” cases. Of the 88 patients in the non-PCP group, only 2 had positive qPCR results for PCP (Table 2). Ct values were calculated for 38 of the 40 positive cases. Values ranged from 24.10 to 40, with a mean value of 36.52 ± 3.98. The mean Ct value was significantly lower in the definite group than in the probable group (28.24, 95% CI: 26.10 to 30.38 vs 32.56, 95% CI: 32.28 to 32.84; p < 0.001) (Table 2). Two patients in the non-PCP group had positive qPCR results with Ct were 35.60 and 35.80. Figure 4 shows the qPCR DNA loads of Definite PCP, Probable PCP, and non-PCP patients. These differences were statistically significant (p < 0.001).
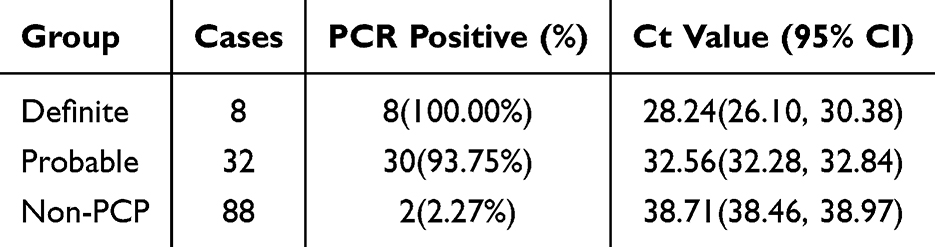 |
Table 2 PCR Positivity Rate and Ct Values by Study Group |
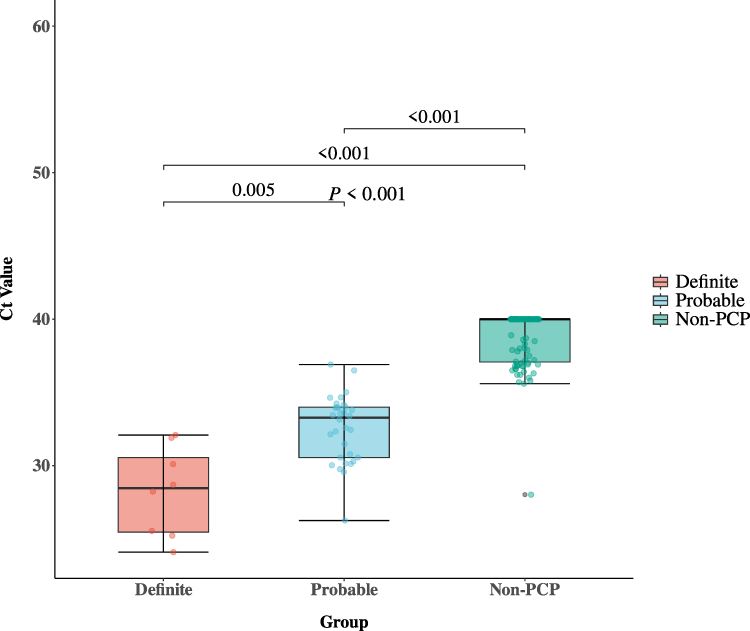 |
Figure 4 PCR quantification cycle Ct values in patients with definite, probable and non-PCP groups. |
We further evaluated the accuracy of qPCR in the diagnosis of PCP. First, using the clinical definition of PCP as the gold standard and categorizing both probable and definite PCP cases as “true positives” within the study group, the ROC curve (Figure 5A) showed an area under the curve (AUC) of 0.98, with a Ct value of 35.305 identified as the optimal threshold for distinguishing between PCP and non-PCP patients. At this cutoff, the PCR test demonstrated a sensitivity, specificity, PPV, and NPV of 95%, 99%, 97%, and 98%, respectively (Table 3). The ROC curve (Figure 5B) yielded an AUC of 0.89, indicating that a Ct value of 32.115 was the optimal threshold for discriminating between definite and probable PCP cases. Using this value as the cutoff, the test achieved a sensitivity of 100%, specificity of 66%, PPV of 42%, and NPV of 100% (Table 3).
 |
Table 3 Accuracy, Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Ct Cut-off Value for All the Tested Samples |
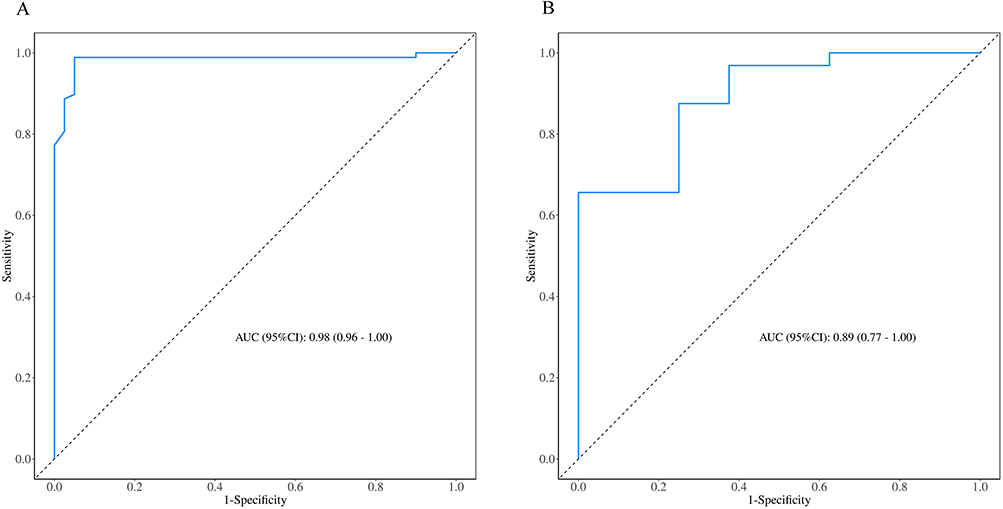 |
Figure 5 Receiver operating characteristic curves of Pneumocystis jirovecii Ct values. (A) Comparison between the PCP group and the non-PCP group. (B) Comparison between the definite PCP group and the probable PCP group. |
Next, we investigated the correlation between the qPCR Ct values and disease prognosis in patients infected with Pneumocystis jirovecii. We found no significant correlation between qPCR Ct values and serum BDG levels (Figure 6A and C). Further analysis showed a positive correlation between qPCR Ct values and the percentage of lymphocytes (r = 0.360, 95% CI: 0.055–0.604; p = 0.022), as well as a negative correlation between LDH (r = −0.314, 95% CI: −0.570 to −0.003; p = 0.048) and qPCR Ct values in PCP cases (Figure 6B and D).
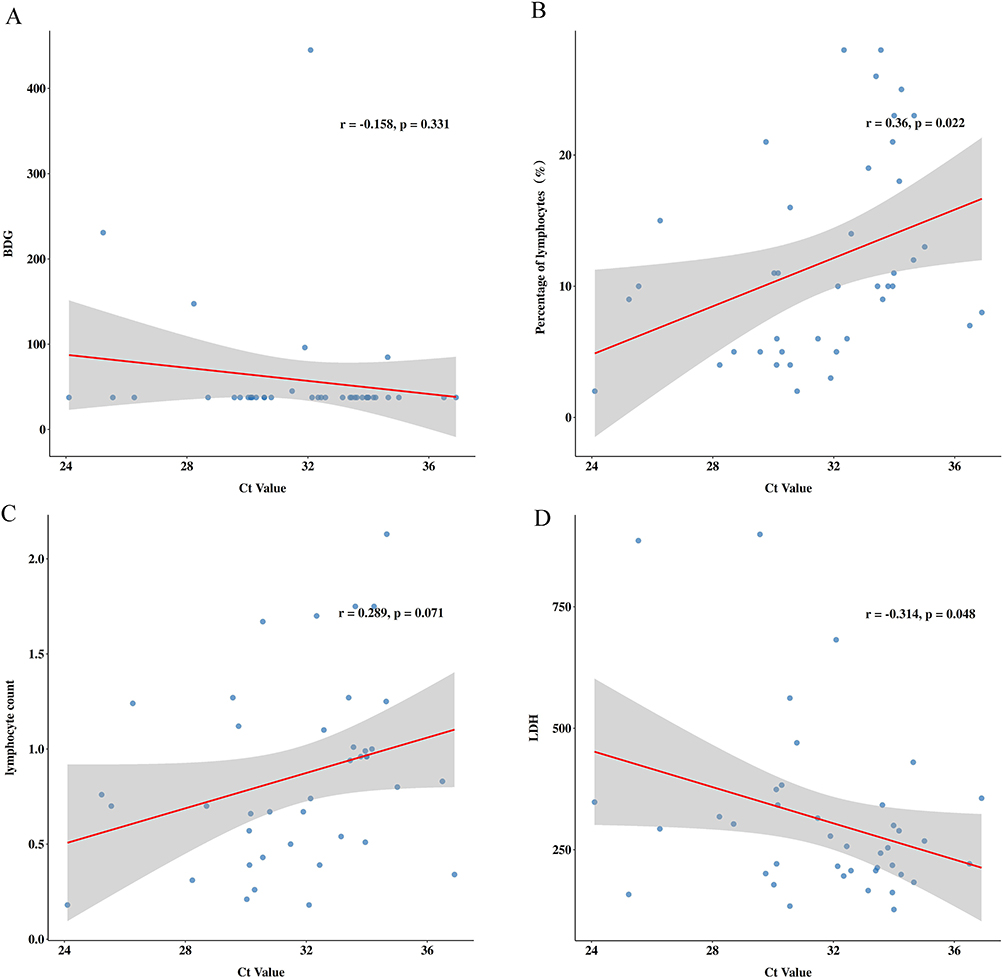 |
Figure 6 Correlation between qPCR Ct Values and clinical indicators. (A–D) illustrated the correlation between Ct values and several indicators, including serum BDG, percentage of lymphocytes, lymphocytes count and LDH. |
Discussion
PCP is an opportunistic infection predominantly affecting immunocompromised individuals. The incidence of PCP has been significantly reduced due to the advent of highly active antiretroviral therapy; however, recent studies indicate that pneumocystis infections have a higher incidence and mortality risk in patients with compromised immune function and underlying conditions, especially in those with solid tumors and hematologic diseases.1,12 Considering the importance of timely diagnosis and effective management strategies, PCP is associated with prolonged hospitalization and increased healthcare costs.1,2 Once classified as a protozoan, the pathogen is now recognized as a fungus, necessitating the reevaluation of diagnostic and therapeutic approaches tailored to this unique infectious agent.2
This study systematically analyzed the clinical and laboratory characteristics of patients suspected of PCP, with a primary focus on evaluating the diagnostic performance of qPCR. The results revealed significant differences in sensitivity and specificity compared to conventional methods, underscoring the challenges in distinguishing PCP from other respiratory infections. Through a retrospective analysis, we aimed to establish a cut-off value for the qPCR cycle threshold and investigate the associations between this threshold and various laboratory parameters. The Ct cut-off value, determined via ROC curve analysis, was primarily designed to optimize the specificity of this differential diagnosis, thereby transforming qPCR from a highly sensitive screening tool into a more diagnostically definitive method. Furthermore, a negative correlation was observed between Ct values and LDH levels, suggesting that a higher fungal burden may contribute to more pronounced pulmonary parenchymal inflammation and injury, which further highlights the prognostic significance of this association. Previous studies have found that lactate dehydrogenase levels can preliminarily predict the need for assisted ventilation in patients with chronic obstructive pulmonary disease complicated by invasive pulmonary aspergillosis.13 Additionally, other research has demonstrated a positive correlation between lactate dehydrogenase levels and the time from symptom onset to the initiation of oral compound sulfamethoxazole therapy in HIV-negative PCP patients.14 These insights have the potential to refine the diagnostic criteria and enhance clinical decision-making, thereby improving patient outcomes in the management of PCP.
This study presents several innovative aspects that fill significant gaps in the existing knowledge regarding PCP diagnosis and management. Notably, our research provides evidence of distinct immunological profiles among patients with definite PCP, characterized by lower lymphocyte percentages and counts, compared with the probable and non-PCP groups. This finding aligns with previous studies that highlighted the importance of the immune response in the pathogenesis of PCP.15 However, our study is among the first to quantitatively analyze these profiles in a large cohort of human subjects, thereby reinforcing the hypothesis that a compromised immune response is pivotal in the development of PCP.16 Furthermore, we identified beta-d-glucan (BDG) as a reliable biomarker for diagnosing PCP, showing a significant elevation in the definite PCP group. This contrasts with earlier studies that primarily focused on diagnostic accuracy without elucidating the immunological mechanisms at play, thereby providing new insights into potential diagnostic approaches.17,18 Our findings have profound implications for clinical practice. The study underscores the utility of qPCR and BDG levels in enhancing diagnostic accuracy, which is crucial for timely and effective treatment of PCP, particularly in immunocompromised patients. The identification of specific cut-off values for the qPCR Ct values and BDG levels has the potential to refine the diagnostic criteria, enabling clinicians to differentiate more effectively between PCP and other respiratory infections. This is particularly relevant given the high morbidity and mortality associated with PCP in this vulnerable population.
However, this study has several limitations. The retrospective design may introduce bias, and the single-center nature restricts the generalizability of the findings. The relatively small sample size of definite PCP cases makes the findings more susceptible to random variation, which may compromise the generalizability of Ct cut-off values and the statistical power of subgroup analyses. Previous methodological studies have indicated that small-sample diagnostic studies carry an inherent risk of overestimating diagnostic performance.19 Future research should validate these findings in larger, multicenter studies to confirm the utility of qPCR as diagnostic tools for PCP across diverse populations. Additionally, a longer follow-up period is needed to assess the long-term prognostic value of these biomarkers in the management of PCP.
Another significant limitation pertains to the suboptimal standardization of PCR-based assays. Although multiple gene targets exist for the detection of Pneumocystis jirovecii, there is currently no consensus on standardized testing protocols or preferred gene targets across different laboratories, which compromises the comparability of results.20 To address this issue, the present study utilized a commercially available and analytically validated reagent kit. Moreover, the high analytical sensitivity of qPCR increases the risk of false-positive results and potential overdiagnosis, especially in immunosuppressed individuals lacking characteristic clinical or radiological evidence, possibly leading to unnecessary therapeutic interventions.20 Consequently, positive qPCR findings require careful interpretation within the broader clinical context, incorporating the patient’s immune competence, symptomatic presentation, imaging features, and supplementary biomarker profiles. It should also be noted that the presence of PCR inhibitors in clinical specimens may contribute to false-negative outcomes.
In recent years, a variety of emerging technologies have been progressively applied to the differential diagnosis of Pneumocystis jirovecii, significantly improving the detection sensitivity, specificity, and efficiency. qPCR provides pathogen load information through Ct values, which aids in distinguishing colonization from infection.21 Its operational procedures are easily standardized, making it well-suited for widespread clinical use. However, this method cannot differentiate between viable and non-viable pathogens, and its quantitative thresholds require validation in multicenter studies. Droplet digital PCR maintains high accuracy and sensitivity, even in samples with low pathogen loads, making it particularly suitable for early screening in immunocompromised patients. Nevertheless, this technique is associated with high costs and limited throughput and has not yet been widely implemented in routine clinical practice.22 mNGS enables simultaneous detection of multiple pathogens and offers significant advantages for identifying mixed infections and rare strains. However, its application is constrained by complex data analysis, substantial background microbial interference, high expenses, and demanding requirements for bioinformatics expertise.23 The emerging technology, CRISPR-Cas-Based Detection Technology, demonstrates single-molecule-level sensitivity and high specificity, and can be integrated with portable devices for rapid point-of-care testing.24 Currently, it remains in the development and validation phases, with stability and standardization awaiting further improvement. Currently, diagnostic technologies for Pneumocystis jirovecii are rapidly transitioning from traditional microscopy and culture methods to molecular and nucleic acid amplifications.
Conclusion
In conclusion, this study enhances our understanding of PCP by identifying the critical clinical and laboratory characteristics that differentiate it from non-PCP cases. These findings underscore the potential of qPCR and serum β-D-glucan as valuable diagnostic tools, which may significantly improve clinical decision-making and patient management. By establishing correlations between immunological markers and disease outcomes, this study paves the way for future investigations aimed at refining the diagnostic criteria and treatment protocols, ultimately striving for better patient outcomes in this vulnerable population.
Acknowledgments
The authors wish to thank all volunteers for their participation in this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ishihara M, Tanzawa S, Honda T, et al. Clinical features of pneumocystis pneumonia in non-human immunodeficiency virus-infected patients: a systematic review and meta-analysis. J Clin Question. 2024;1(2):12–12. doi:10.69854/jcq.2024.0003
2. Noor A, Krilov LR. Pneumocystis Pneumonia. Pediatr Rev. 2023;44(12):720–722. doi:10.1542/pir.2022-005516
3. Hitzenbichler F, Fisser C, Schlitt A, Salzberger B. Infection image: cystic pneumocystis jirovecii pneumonia - forgotten? Infection. 2025;53(2):763–765. doi:10.1007/s15010-024-02403-w
4. Jaramillo Cartagena A, Asowata OE, Ng D, Babady NE. An overview of the laboratory diagnosis of Pneumocystis jirovecii pneumonia. J Clin Microbiol. 2025;63(3):e0036124. doi:10.1128/jcm.00361-24
5. Zhang L, Zheng C, Sun Y, et al. Diagnostic tests performance in detecting Pneumocystis jirovecii: a systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis. 2025;44(4):789–805. doi:10.1007/s10096-025-05051-6
6. Meyer AMJ, Sidler D, Hirzel C, et al. Distinct clinical and laboratory patterns of Pneumocystis jirovecii pneumonia in renal transplant recipients. J Fungi. 2021;7(12):1072. doi:10.3390/jof7121072
7. Rouhi F, Erami M, Rastgufar S, et al. Quantitative real time PCR for distinction between Pneumocystis jirovecii infection/colonization in hospitalized patients. Front Cell Infect Microbiol. 2024;14:1426200. doi:10.3389/fcimb.2024.1426200
8. Abramovich T, Korem M, Kuint R, Michael-Gayego A, Moran-Gilad J, Olshtain-Pops K. The role of polymerase chain reaction (PCR) and quantification cycle values in the diagnosis of Pneumocystis jirovecii Pneumonia. J Fungi. 2025;11(8):557. doi:10.3390/jof11080557
9. Permpalung N, Uhteg K, Rodrigues M, Memon W, Totten M, Zhang SX. Evaluation of a multiplex PCR assay using barcoded magnetic bead technology for detection of fungal pathogens in bronchoalveolar lavage fluid. Clin Microbiol Infect. 2025;31(9):1546–1552. doi:10.1016/j.cmi.2025.05.022
10. Trovato L, Calvo M, Palermo CI, Scalia G. The role of quantitative real-time PCR in the invasive pulmonary aspergillosis diagnosis: a retrospective study. Microorganisms. 2025;13(2):409. doi:10.3390/microorganisms13020409
11. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
12. Yang SL, Wen YH, Wu YS, et al. Diagnosis of Pneumocystis pneumonia by real-time PCR in patients with various underlying diseases. J Microbiol Immunol Infect. 2020;53(5):785–790. doi:10.1016/j.jmii.2019.08.012
13. Long Z, Li X, Li Z, et al. Improved diagnostic markers for invasive pulmonary aspergillosis in COPD patients. Front Cell Infect Microbiol. 2024;14:1294971. doi:10.3389/fcimb.2024.1294971
14. Wang W, Mo Q, Yu Q, Ding X. Clinical characteristics of Pneumocystis jirovecii pneumonia in 20 non-HIV-infected patients. J Thorac Dis. 2025;17(10):8904–8914. doi:10.21037/jtd-2025-499
15. Li J, Mu X, Li H, Liu X. Clinical course and prognostic factors of Pneumocystis pneumonia with respiratory failure in non-HIV patients. Front Cell Infect Microbiol. 2024;14:1380494. doi:10.3389/fcimb.2024.1380494
16. Messiaen PE, Cuyx S, Dejagere T, van der Hilst JC. The role of CD4 cell count as discriminatory measure to guide chemoprophylaxis against Pneumocystis jirovecii pneumonia in human immunodeficiency virus-negative immunocompromised patients: a systematic review. Transpl Infect Dis. 2017;19(2). doi:10.1111/tid.12651
17. Chen Q, Chen X, Mo P, et al. Diagnostic values of BALF metagenomic next-generation sequencing, BALF real-time PCR and serum BDG for Pneumocystis jirovecii pneumonia in HIV-infected patients. Front Microbiol. 2024;15:1421660. doi:10.3389/fmicb.2024.1421660
18. Huang Y, Yi J, Song JJ, et al. Negative serum (1,3) -β-D-glucan has a low power to exclude Pneumocystis jirovecii pneumonia (PJP) in HIV-uninfected patients with positive qPCR. Ann Clin Microbiol Antimicrob. 2023;22(1):102. doi:10.1186/s12941-023-00650-7
19. Bhandari PM, Levis B, Neupane D, et al. Data-driven methods distort optimal cutoffs and accuracy estimates of depression screening tools: a simulation study using individual participant data. J Clin Epidemiol. 2021;137:137–147. doi:10.1016/j.jclinepi.2021.03.031
20. Brown L, Alanio A, Cruciani M, et al. Strengths and limitations of molecular diagnostics for Pneumocystis jirovecii pneumonia. Expert Rev Mol Diagn. 2024;24(10):899–911. doi:10.1080/14737159.2024.2405920
21. Grønseth S, Rogne T, Hannula R, Åsvold BO, Afset JE, Damås JK. Semiquantitative real-time PCR to distinguish pneumocystis pneumonia from colonization in a heterogeneous population of HIV-negative immunocompromised patients. Microbiol Spectr. 2021;9(1):e0002621. doi:10.1128/Spectrum.00026-21
22. Bian W, Shang Y, Zhao L, et al. Clinical performance of BALF droplet digital PCR for differential diagnosis of Pneumocystis jirovecii pneumonia and Pneumocystis jirovecii colonization. Diagn Microbiol Infect Dis. 2024;108(3):116168. doi:10.1016/j.diagmicrobio.2023.116168
23. Ren G, Ma L, Yan C, et al. Application of targeted metagenomic next-generation sequencing in pneumonia patients. Microbiol Spectr. 2025;13(8):e0171324. doi:10.1128/spectrum.01713-24
24. Zhan Y, Gao X, Li S, et al. Development and evaluation of rapid and accurate CRISPR/Cas13-based RNA diagnostics for Pneumocystis jirovecii Pneumonia. Front Cell Infect Microbiol. 2022;12:904485. doi:10.3389/fcimb.2022.904485
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.