Back to Journals » Cancer Management and Research » Volume 11
Performance characteristics of prostate-specific antigen density and biopsy primary Gleason score to predict biochemical failure in patients with intermediate prostate cancer who underwent radical prostatectomy
Authors Peng C, Zhang J, Hou JQ
Received 10 October 2018
Accepted for publication 27 December 2018
Published 1 February 2019 Volume 2019:11 Pages 1133—1139
DOI https://doi.org/10.2147/CMAR.S190443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Chao Peng, Jun Zhang, Jianquan Hou
Department of Urology, First Affiliated Hospital of Soochow University, Suzhou 215006, China
Background: Prognosis for intermediate-risk prostate cancer (PCa) remains variable; therefore, we aimed to investigate high-risk factors for biochemical recurrence (BCR), and intermediate-risk PCa using radical prostatectomy to identify patients having equivalent BCR-free survival rates when compared to high-risk PCa.
Patients and methods: A total of 441 medical records were analyzed, including those of 169 intermediate-risk and 272 high-risk PCa patients. Risk factors for time to BCR were tested and analyzed using Kaplan–Meier survival analysis, log-rank tests, and Cox proportion hazards models.
Results: In the intermediate-risk group, prostate-specific antigen density (PSAD) and primary Gleason pattern were significant preoperative risk factors for BCR. Moreover, BCR-free survival of patients in the intermediate-risk group with a higher PSAD (>0.5 ng/mL/cm3) was comparable with that of patients in the high-risk group (P=0.735). When combining primary Gleason pattern 4 and 3 with PSAD cut-offs 0.3–0.7 ng/mL/cm3, we found that BCR-free survival of patients in the intermediate-risk group with a primary Gleason pattern 4 and PSAD >0.3 ng/mL/cm3 was comparable with that of patients in the high-risk group (P=0.463).
Conclusion: PSAD and primary Gleason pattern are potential risk factors associated with biochemical failure in intermediate-risk PCa patients after radical prostatectomy. Regarding significant differences in prognosis according to PSAD as well as primary Gleason pattern on biopsy, a subset of the intermediate-risk patients could be identified with outcomes that were equivalent to that of high-risk patients.
Keywords: biochemical recurrence, Gleason grade, intermediate risk, prostate cancer, PSA density
Introduction
Prostate cancer (PCa) is the most common solid malignancy in many western countries.1 Although the incidence and mortality rate of PCa is lower in Asian countries, in recent years, the incidence has risen.2 PCa shows a heterogeneous characterization, ranging from insignificant and organ confined to aggressive. The D’Amico PCa risk classification system has been widely applied for the selection of appropriate treatment and prediction of prognosis for PCa.3 Moreover, significant heterogeneity remained in every given risk group, and the established risk stratification system inefficiently preoperatively identified patients with advanced pathologic features, leading to biochemical and systemic recurrence.4 Published reports suggested that biochemical recurrence (BCR) rates after definitive primary treatment for intermediate-risk PCa are variable, with 5-year BCR rates ranging from 2% to 70%.5 In addition, in several studies, it has been suggested that a wider range of intermediate-risk PCa patients is suitable for active surveillance (AS).6–8 However, a significant proportion of patients with intermediate-risk PCa have poor prognosis and are not suitable for AS. Thus, a more precise stratification of intermediate-risk PCa is warranted to identify the unrecognized high-risk disease, in order to treat these patients more accurately and aggressively.
The purpose of the present study was to investigate the effects of various clinical and pathological factors on BCR in intermediate-risk PCa and to identify patients with a similar prognosis in the high-risk group according to BCR after radical prostatectomy (RP).
Patients and methods
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Committee Board of the First Affiliated Hospital of Soochow University, Suzhou, China. The representative population of the single-center study included the residents of eastern China. Written informed consent was waived as there were no conflicts of interest or damage to patients, and patient data confidentiality was guaranteed according to the requirement of the institutional review board.
After obtaining approval from our institutional review board, the databases of 634 men who underwent RP for PCa were reviewed in the archives of the First Affiliated Hospital of Soochow University between August 2012 and April 2017. After excluding patients who received neoadjuvant androgen deprivation or radiation therapy prior to prostatectomy or if adjuvant treatment was received immediately after surgery, a total of 441 patients were enrolled in the present study. Classifying the patients into modified National Comprehensive Cancer Network risk groups,9 169 (38.3%) were at intermediate-risk PCa (clinical stage T2b–T2c, biopsy Gleason score 7, or prostate-specific antigen [PSA] 10–20 ng/mL) and 272 (61.7%) were at high-risk PCa (clinical stage T3a, biopsy Gleason score 8–10, or PSA >20 ng/mL). All patients had biopsy GS7 with both a primary and secondary grade recorded, and all sections were pathologically reviewed before patients underwent RP. RP was carried out using a laparoscopic approach. All biopsy and RP specimens were pathologically analyzed by at least two genitourinary pathologists. Postoperative BCR was defined as two consecutive increases in PSA level ≥0.2 ng/mL after RP. Prostate-specific antigen density (PSAD) was defined as the ratio of preoperative serum PSA level (ng/mL) to transrectal ultrasound-estimated prostate volume (cm3). As recommended by the physicians, all patients had their scrum PSA levels assessed monthly in the first year after surgery and at least every 4 months in the following 4 years. Because follow-up treatment was received in other hospitals, the scrum PSA data of a small number of patients were obtained through telephone follow-up. Patients who followed up for <1 year and patients who did not have their PSA level tested for >6 months after surgery were excluded from the study.
Quantitative data were compared using a Mann–Whiney U test and qualitative data using a Fisher’s exact test. Postoperative BCR-free survival rates were calculated using the Kaplan–Meier survival method for which a log-rank test was used to compare BCR-free survival rates among groups or subgroups. Cox proportional hazards regression analysis was used for univariate and multivariate analyses in which these factors were examined in relation to BCR, including: patient age, biopsy primary Gleason pattern, preoperative PSA level, prostate volume, PSAD, percent of positive biopsies, number of intermediate risk factors, extracapsular tumor extension, positive surgical margins, and seminal vesicle invasion. Baseline variables that were considered clinically relevant or that showed a univariate relationship with outcome were entered into multivariate Cox proportional hazards regression model. Given the number of events available, we carefully selected the variables to ensure that the final model was concise. SPSS version 19.0 software (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Two-tailed P-values <0.05 were considered statistically significant.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Committee Board of the First Affiliated Hospital of Soochow University, Suzhou, China. Written informed consent was waived as there were no conflicts of interest or damage to patients, and patient data confidentiality was guaranteed according to the requirement of the institutional review board.
Results
In the preoperative characteristics indicated in Table 1, significant differences were observed in PSA, PSAD, the percentage of positive biopsies at median value, the composition of primary Gleason patterns, and the clinical T stage between the intermediate-risk and high-risk groups. Pathological characteristics are presented in Table 2. Significant differences were observed in surgical margin, seminal vesicle, and prostate capsule status. Of the 169 intermediate-risk PCa patients, 101 had a primary Gleason pattern 4, 84 had cT2b–T2c, and 82 had PSA >10 ng/mL. At the median follow-up of 31 months, 36 patients in the intermediate-risk group showed BCR after RP. The 3-year BCR-free survival rate was 75.1%. Table 3 shows the results of univariate and multivariate analyses of the intermediate-risk PCa patients. Among the preoperative variables, PSAD and primary Gleason pattern were significant prognostic factors for BCR univariate analyses (P=0.008 and P=0.026, respectively). In addition, patient age, preoperative PSA level, prostate volume, percentage of positive biopsies, and number of intermediate risk factors were not significant risk factors for BCR. All postoperative pathological variables, including extracapsular tumor extension, positive surgical margins, and seminal vesicle invasion, were significant prognostic factors in univariate analysis of patients with intermediate-risk PCa who were treated using RP. In a multivariable Cox proportional hazards model including all preoperative and postoperative variables, PSAD and a primary Gleason pattern were found to be independent factors associated with BCR among the intermediate-risk group.
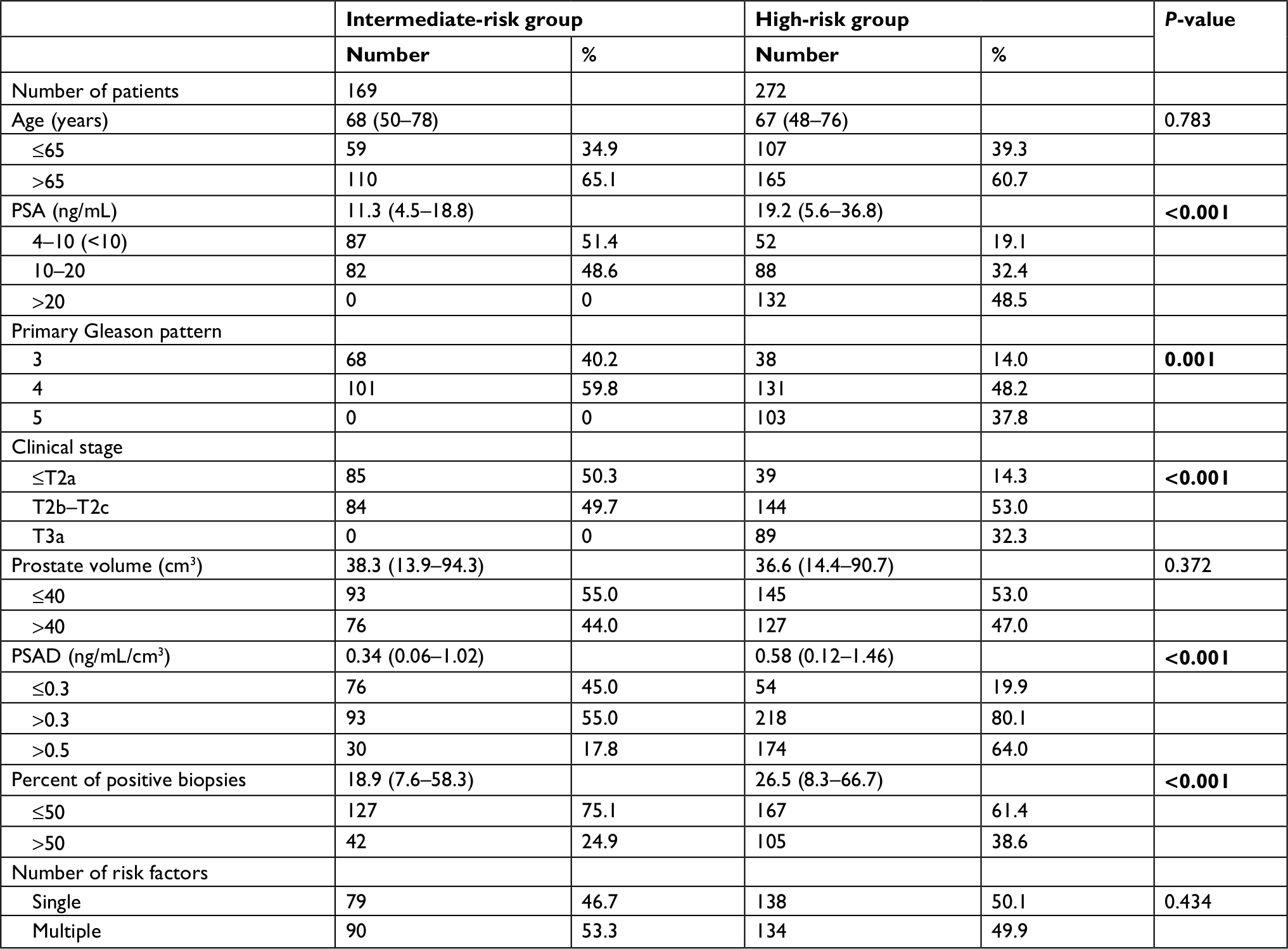 | Table 1 Preoperative clinical characteristics for the intermediate- and high-risk PCa patients Note: Bold text indicates statistical significance. Abbreviations: PSA, prostate-specific antigen; PSAD, PSA density. |
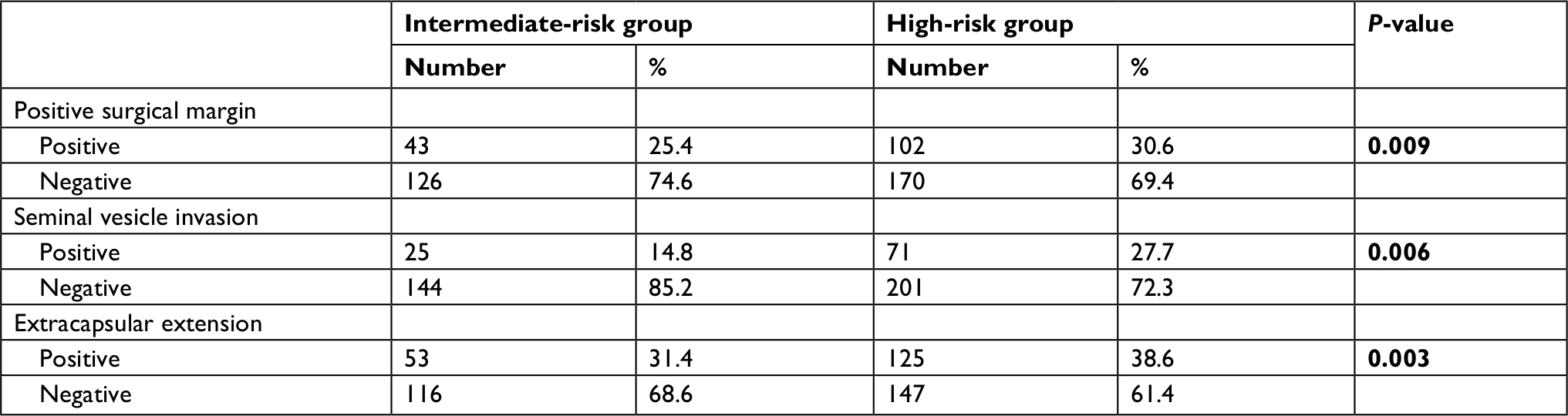 | Table 2 Pathological features for the intermediate- and high-risk groups Note: Bold text indicates statistical significance. |
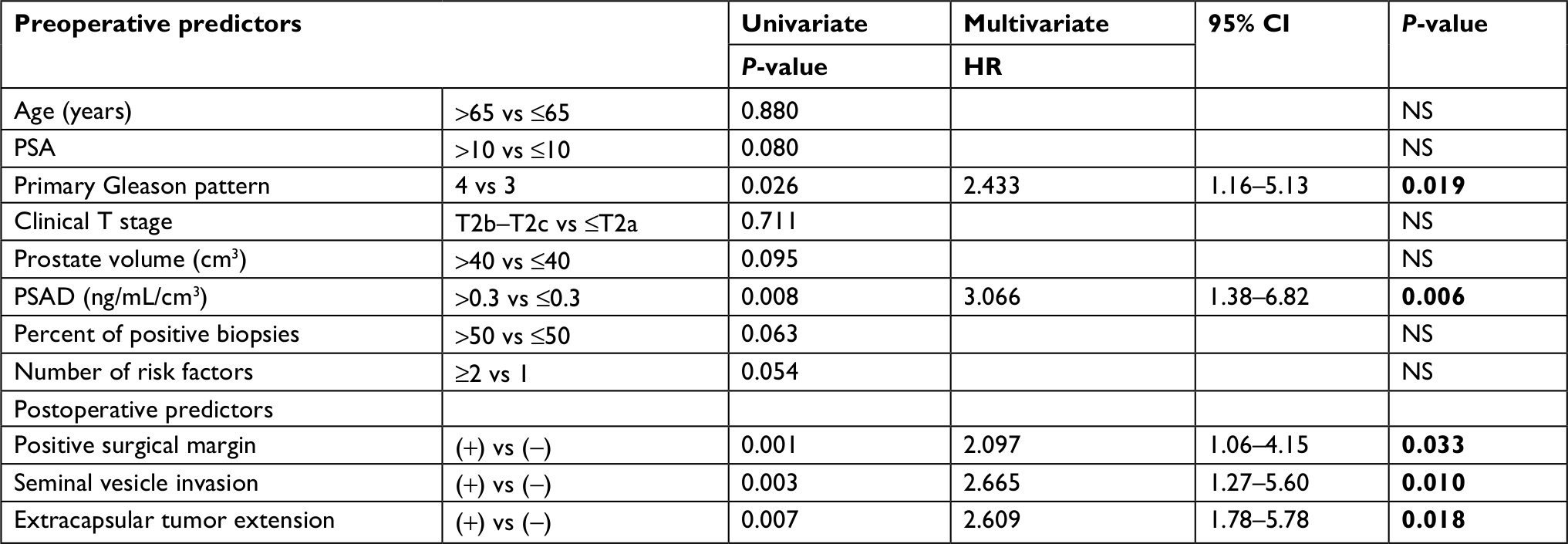 | Table 3 Univariate and multivariable analyses for BCR prediction in intermediate-risk prostate cancer patients Abbreviations: BCR, biochemical recurrence; NS, nonsignificant; PSA, prostate-specific antigen; PSAD, PSA density. Note: Bold text indicates statistical significance. |
A total of 36 (21.3%) patients in the intermediate-risk group and 85 (31.2%) patients in the high-risk group experienced BCR within 5 years. The overall BCR-free survival of the two groups is shown in Figure 1. The overall postoperative BCR-free survival rate was significantly higher in the intermediate-risk group when compared with the high-risk group (68.5% vs 56.1%; log-rank P=0.008). Patients in the intermediate-risk group with PSAD >0.3 ng/mL/cm3 had a significantly higher BCR rate compared to those with PSAD ≤0.3 ng/mL/cm3 (P=0.008). Based on the preoperative risk factors associated with BCR in the present study, we attempted to identify the patients in the intermediate-risk group with similar BCR-free survival rate as in the high-risk group using several cut-off points of PSAD. When in the current study, the difference in the BCR rate between individuals with a PSAD 0.3–0.7 ng/mL/cm3 was analyzed in units of 0.1 ng/mL/cm3, that BCR-free survival in the intermediate-risk group with a PSAD >0.5 ng/mL/cm3 was comparable with that in the high-risk group (P=0.735; Figure 2). Moreover, pairwise comparisons among the three groups revealed that subgroups 2 and 3 showed similar recurrence curves. Also, patients in the intermediate-risk group with a PSAD >0.5 ng/mL/cm3 had a significantly higher BCR rate when compared to those with a PSA density ≤0.5 ng/mL/cm3 (P=0.003; Figure 2). Furthermore, when combining the primary Gleason pattern with PSAD, we demonstrated that patients with a primary Gleason pattern 4 and PSAD >0.3 ng/mL/cm3 had a BCR-free survival that was comparable with that of high-risk group patients (P=0.463; Figure 3). Similarly, patients in the intermediate-risk group with a primary Gleason pattern 4 and PSAD >0.3 ng/mL/cm3 had a significantly higher BCR rate when compared to that in those with a primary Gleason pattern 3 and PSAD ≤0.3 ng/mL/cm3 (P=0.004; Figure 3).
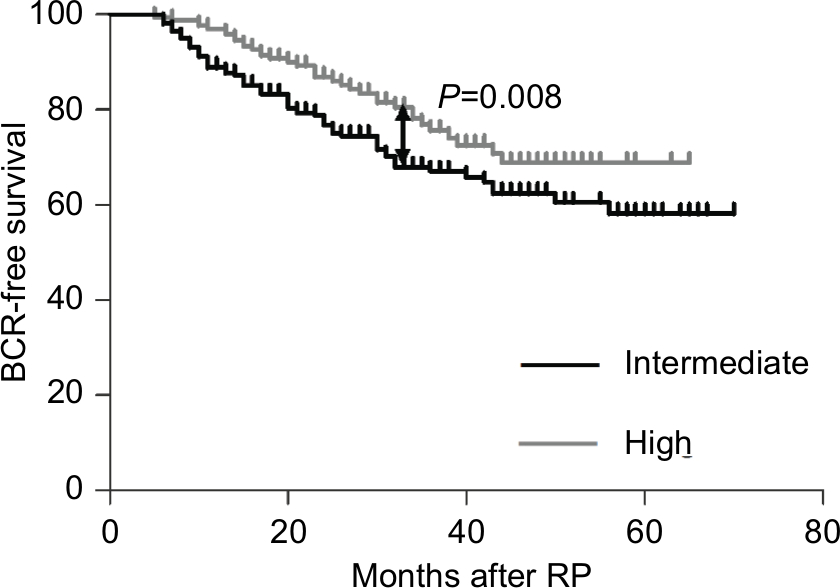 | Figure 1 Kaplan–Meier: a comparison of intermediate-risk patients with high-risk patients undergoing RP, showing significant differences in BCR-free survival rates. Abbreviations: BCR, biochemical recurrence; RP, radical prostatectomy. |
 | Figure 2 Kaplan–Meier: BCR-free survival by the risk group of PSAD. Notes: Pairwise P-values are as follows: high-risk vs intermediate-risk groups with PSAD >0.5, P=0.735; intermediate-risk group with PSAD >0.5 vs PSAD ≤0.5, P=0.003. Abbreviations: BCR, biochemical recurrence; PSAD, prostate-specific antigen density. |
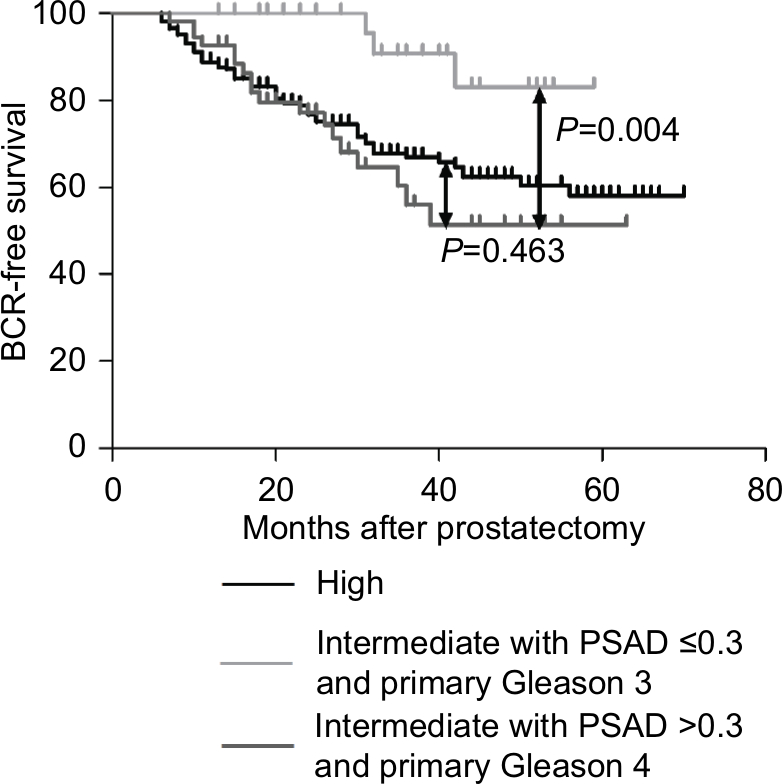 | Figure 3 Kaplan–Meier: BCR-free survival by the risk group of PSAD and primary Gleason pattern. Notes: Pairwise P-values are as follows: high-risk vs intermediate-risk groups with PSAD >0.3 and primary Gleason 4, P=0.463; intermediate-risk group with PSAD >0.3 and primary Gleason 4 vs PSAD ≤0.3 and primary Gleason 3, P=0.004. Abbreviations: BCR, biochemical recurrence; PSAD, prostate-specific antigen density. |
Discussion
Due to the high heterogeneity in the prognosis for patients with PCa, improvement of the individual risk prediction remains to be discussed and may be relevant to improve patient management. In general, patients with low-risk disease are diagnosed early and may be cured with local treatment. High-risk PCa patients often need to accept further treatment in the form of androgen therapy, chemotherapy, or other systemic treatments to achieve a better outcome. In the present study, we aimed to explore whether preoperative factors can be used to predict the prognosis of patients with intermediate-risk PCa, so as to identify the part with similar adverse outcomes in the high-risk group. We found that those patients had significantly different postoperative outcomes based on both PSAD and the biopsy primary Gleason pattern.
In many studies, the heterogeneity of intermediate-risk PCa with regard to its prognosis has been reported. Indeed, Reese et al demonstrated that BCR-free survival rates were superior in men with an advanced clinical stage when compared to those in men with an advanced Gleason score or higher PSA level.4 When analyzing the outcomes of intermediate-risk PCa patients treated with external-beam radiation therapy, Zumsteg et al10 compared patients who were classified as having an unfavorable disease (a primary Gleason pattern of 4, percent of positive biopsy scores ≥50%, and the presence of multiple intermediate-risk factors) with other favorable patients with intermediate-risk PCa. They showed that unfavorable patients had an inferior PSA recurrence-free survival, distant metastasis, and PCa-specific morality. Jung et al11 applied a similar classification system to patients with intermediate-risk PCa who received RP, and observed that unfavorable patients had significantly higher rates of adverse pathological features and inferior postoperative biochemical outcomes. In addition, Jung et al showed that the 5-year BCR-free survival of unfavorable patients was significantly higher when compared to that in the high-risk group after RP. In the present study, we found that when using the preoperative PSAD calculated from transrectal ultrasound measurement and the updated Gleason grading system, PSAD and the primary Gleason pattern were independent predictors that were associated with BCR after prostatectomy, whereas clinical T stage, percentage of positive biopsy scores, and the number of intermediate-risk factors were not independent predictors.
Since the introduction of the Gleason scoring system in the 1960s, it has been shown to be one of the most significant prognosis factors in PCa and has greatly promoted people’s understanding of its pathological features. In 2014, the International Society of Urological Pathology (ISUP) Consensus further revised the Gleason grading system of PCa, which not only defined the morphological criteria of Gleason PCa in more detail and clearly but also proposed a new set of prognostic differentiation-based grouping of PCa grading.12 The differences between Gleason 3+4 and 4+3 tumors may well have become more evident. In part, these changes may contribute to the recent increase in the diagnosis of Gleason score 7 as opposed to Gleason score 6 and the heterogeneity in men in the intermediate-risk group. In many studies, it was demonstrated that Gleason score 4+3=7 had a worse prognosis than 3+4=7 in RP specimens.13,14 When analyzing these differences in biopsy specimens, we subcategorized Gleason score 7 into 4+3 and 3+4 as recommended in the ISUP Consensus 2005, and found there was still prognostic significance relative to the risk of BCR after RP in the two groups, which corresponded to most previous studies.11,15,16
The major classification systems use a cut-off PSA level of 10–20 ng/mL to define intermediate-risk PCa, and PSA is recognized as an independent predictor of outcome in PCa patients. However, because benign epithelium of PCa also secretes PSA, the value of total serum PSA will, to some extent, be affected by the volume of prostate glands. PSAD, originally introduced by Benson et al17 in an effort to improve the specificity of PSA testing for PCa screening, was thought to reduce the error caused by prostate volume. In some studies, the role of PSAD in predicting adverse pathology or BCR of PCa was explored.18–21 In other studies, PSAD was compared with PSA to see if this would be a better predictor after primary treatment.22–25 In most studies, it was agreed that PSAD can serve as an independent prognosis predictor of PCa, but whether it can take the place of PSA to predict adverse pathological findings and BCA is still controversial. In our study, multivariate analysis showed that in the intermediate-risk group, the preoperative PSAD was a strong predictor of BCR-free survival after RP, whereas PSA was not. The preoperative PSAD cut-off points of <0.3 and >0.3 ng/mL/cm3 were in line with those published in previous studies showing that PSAD >0.3 ng/mL/cm3 increased the likelihood of BCR after RP.23–26 Furthermore, a cut-off of 0.5 ng/mL/cm3 achieved the most significant results, and patients in the intermediate-risk group with PSAD >0.5 ng/mL/cm3 had a risk that was equivalent to that of patients in the high-risk group. Moreover, when combining these cut-off points with biopsy primary Gleason patterns 3 and 4, we found that patients with PSAD >0.3 ng/mL/cm3 and primary Gleason pattern 4 had a similar BCR-free survival when compared with patients in the high-risk group. Freedland et al22 used the PASD and Gleason score to create an improved version of risk stratification for BCR after RP, and they showed that patients with a PSAD >0.7 ng/mL/cm3 in both the intermediate-risk and low-risk groups experienced a risk that was equivalent to that of patients in the high-risk group. However, the Gleason grading in that study was not based on the 2005 ISUP; therefore, the impact of the primary Gleason score on BCR may change. Additionally, the PASD used in their study was calculated by dividing serum PSA by the pathological weight of the prostatectomy specimen.
Existing risk assessment stratification may be lacking in patient treatment strategies and individual management. However, incorporation of PSAD and the primary Gleason pattern may help provide additional prognostic information, thereby leading to better and more accurate treatment strategies. Data analysis results from the Mayo Clinic and Johns Hopkins University showed that the BCR rates and prognostic outcomes were significantly different in intermediate-risk patients when a Gleason score of 7 was stratified according to the primary Gleason pattern.27,28 PSAD has been adopted as a useful tool for selecting candidates for AS in low-risk PCa. Kang et al29 proposed to apply PSAD to the selection of intermediate-risk PCa patients suitable for AS. In the current study, we further demonstrated that incorporation of the PSAD and the primary Gleason pattern can be used to identify patients who need a more invasive treatment.
Our study has some limitations. It is a retrospective study based on a relatively small patient population, the number of the patients enrolled in the current study was limited, and the median follow-up of the cohort was relatively short. Since the morality rate during our follow-up was extremely low, we could not analyze long-term postoperative follow-up data, such as PCa-specific or metastasis-free survival. Another limitation of the current study was that most patients in our study did not have a standard pelvic lymph node dissection; therefore, we could not incorporate lymph node metastasis into the multivariate analysis.
In conclusion, preoperative PSAD and the primary Gleason pattern were important preoperative factors to predict biochemical failure and should be incorporated into risk assessment for intermediate-risk PCa patients after RP. They were able to help us identify patients in the intermediate-risk with outcomes that were equivalent to those of high-risk patients. Since the BCR-free survival rates of intermediate-risk group patients with a PSAD >0.3 ng/mL/cm3, a primary Gleason pattern 4, or PSAD >0.5 ng/mL/cm3 were comparable to those of high-risk group patients, it may be reasonable to propose that these patients need to receive invasive and comprehensive treatments similar to those for high-risk PCa. The findings of the current study should be validated using a larger data set.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. | ||
Baade PD, Youlden DR, Krnjacki LJ. International epidemiology of prostate cancer: geographical distribution and secular trends. Mol Nutr Food Res. 2009;53(2):171–184. | ||
D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280(11):969–974. | ||
Reese AC, Pierorazio PM, Han M, Partin AW. Contemporary evaluation of the National Comprehensive Cancer Network prostate cancer risk classification system. Urology. 2012;80(5):1075–1079. | ||
Grossfeld GD, Latini DM, Lubeck DP, et al. Predicting disease recurrence in intermediate and high-risk patients undergoing radical prostatectomy using percent positive biopsies: results from CaPSURE. Urology. 2002;59(4):560–565. | ||
Abern MR, Aronson WJ, Terris MK, et al. Delayed radical prostatectomy for intermediate-risk prostate cancer is associated with biochemical recurrence: possible implications for active surveillance from the search database. Prostate. 2013;73(4):409–417. | ||
Loeb S, Berglund A, Stattin P. Population based study of use and determinants of active surveillance and watchful waiting for low and intermediate risk prostate cancer. J Urol. 2013;190(5):1742–1749. | ||
Cooperberg MR, Cowan JE, Hilton JF, et al. Outcomes of active surveillance for men with intermediate-risk prostate cancer. J Clin Oncol. 2011;29(2):228–234. | ||
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology Prostate Cancer. NCCN; 2017 [version 2; February 21, 2017]. Available from: https://www.nccn.org/professionals/physician_gls/PDF/prostate.pdf. Accessed June 4, 2017. | ||
Zumsteg ZS, Spratt DE, Pei I, et al. A new risk classification system for therapeutic decision making with intermediate-risk prostate cancer patients undergoing dose-escalated external-beam radiation therapy. Eur Urol. 2013;64(6):895–902. | ||
Jung JW, Lee JK, Hong SK, Byun SS, Lee SE. Stratification of patients with intermediate-risk prostate cancer. BJU Int. 2015;115(6):907–912. | ||
Epstein JI, Amin MB, Reuter VE, Humphrey PA. Contemporary Gleason grading of prostatic carcinoma: an update with discussion on practical issues to implement the 2014 International Society of Urological Pathology (ISUP) Consensus conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol. 2017;41(4):e1–e7. | ||
Alenda O, Ploussard G, Mouracade P, et al. Impact of the primary Gleason pattern on biochemical recurrence-free survival after radical prostatectomy: a single-center cohort of 1,248 patients with Gleason 7 tumors. World J Urol. 2011;29(5):671–676. | ||
Herman CM, Kattan MW, Ohori M, Scardino PT, Wheeler TM. Primary Gleason pattern as a predictor of disease progression in Gleason score 7 prostate cancer: a multivariate analysis of 823 men treated with radical prostatectomy. Am J Surg Pathol. 2001;25(5):657–660. | ||
Amin A, Partin A, Epstein JI. Gleason score 7 prostate cancer on needle biopsy: relation of primary pattern 3 or 4 to pathological stage and progression after radical prostatectomy. J Urol. 2011;186(4):1286–1290. | ||
Burdick MJ, Reddy CA, Ulchaker J, et al. Comparison of biochemical relapse-free survival between primary Gleason score 3 and primary Gleason score 4 for biopsy Gleason score 7 prostate cancer. Int J Radiat Oncol Biol Phys. 2009;73(5):1439–1445. | ||
Benson MC, Whang IS, Pantuck A, et al. Prostate specific antigen density: a means of distinguishing benign prostatic hypertrophy and prostate cancer. J Urol. 1992;147(3 Pt 2):815–816. | ||
Busch J, Hamborg K, Meyer HA, et al. Value of prostate specific antigen density and percent free prostate specific antigen for prostate cancer prognosis. J Urol. 2012;188(6):2165–2170. | ||
Kundu SD, Roehl KA, Yu X, Antenor JA, Suarez BK, Catalona WJ. Prostate specific antigen density correlates with features of prostate cancer aggressiveness. J Urol. 2007;177(2):505–509. | ||
Magheli A, Hinz S, Hege C, et al. Prostate specific antigen density to predict prostate cancer upgrading in a contemporary radical prostatectomy series: a single center experience. J Urol. 2010;183(1):126–132. | ||
Radwan MH, Yan Y, Luly JR, et al. Prostate-specific antigen density predicts adverse pathology and increased risk of biochemical failure. Urology. 2007;69(6):1121–1127. | ||
Brassell SA, Kao TC, Sun L, Moul JW. Prostate-specific antigen versus prostate-specific antigen density as predictor of tumor volume, margin status, pathologic stage, and biochemical recurrence of prostate cancer. Urology. 2005;66(6):1229–1233. | ||
Freedland SJ, Wieder JA, Jack GS, Dorey F, Dekernion JB, Aronson WJ. Improved risk stratification for biochemical recurrence after radical prostatectomy using a novel risk group system based on prostate specific antigen density and biopsy Gleason score. J Urol. 2002;168(1):110–115. | ||
Freedland SJ, Kane CJ, Presti JC, et al. Comparison of preoperative prostate specific antigen density and prostate specific antigen for predicting recurrence after radical prostatectomy: results from the search data base. J Urol. 2003;169(3):969–973. | ||
Horninger W, Rogatsch H, Reissigl A, et al. Correlation between preoperative predictors and pathologic features in radical prostatectomy specimens in PSA-based screening. Prostate. 1999;40(1):56–61. | ||
Narita S, Mitsuzuka K, Tsuchiya N, et al. Reassessment of the risk factors for biochemical recurrence in D’Amico intermediate-risk prostate cancer treated using radical prostatectomy. Int J Urol. 2015;22(11):1029–1035. | ||
Lau WK, Blute ML, Bostwick DG, Weaver AL, Sebo TJ, Zincke H. Prognostic factors for survival of patients with pathological Gleason score 7 prostate cancer: differences in outcome between primary Gleason grades 3 and 4. J Urol. 2001;166(5):1692–1697. | ||
Chan TY, Partin AW, Walsh PC, Epstein JI. Prognostic significance of Gleason score 3+4 versus Gleason score 4+3 tumor at radical prostatectomy. Urology. 2000;56(5):823–827. | ||
Kang HW, Jung HD, Lee JY, et al. Prostate-specific antigen density predicts favorable pathology and biochemical recurrence in patients with intermediate-risk prostate cancer. Asian J Androl. 2016;18(3):480–484. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.