Back to Journals » International Medical Case Reports Journal » Volume 18
Percutaneous Vertebroplasty Using GeneX® in Osteoporotic Vertebral Compression Fractures: A Case Report
Received 18 December 2024
Accepted for publication 31 July 2025
Published 14 August 2025 Volume 2025:18 Pages 1041—1046
DOI https://doi.org/10.2147/IMCRJ.S505160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Taibang Chen, Lei Cui, Di Du
Department of Orthopaedic Surgery of 920th Hospital of Joint Logistics Support Force, Kunming, People’s Republic of China
Correspondence: Taibang Chen, Email [email protected]
Background: GeneX® allows adsorption and aggregation of molecules and proteins to promote bone formation. According to reports in the literature, it is used in bone defect reconstruction and percutaneous vertebroplasty to promote bone formation.
Case Report: We designed a prospective cohort study to evaluate the outcomes following of percutaneous vertebroplasty using GeneX in patients with osteoporotic vertebral compression fractures. Vertebroplasty was performed at seven vertebrae in the first seven patients. Overall, there were four leaks in four (57%) of the seven patients. Asymptomatic leak of the GeneX material into the intradiscal and paravertebral structures at the treated vertebral level was observed in three patients (43%). However, the material leaked into the intradural and epidural space in the seventh patient (14%), causing severe neurological deficits. Primary diagnosis was bone cement implantation syndrome. The patient’s neurological status improved gradually during the month after surgery. She was able to resume her activities of daily living and had regained her urinary function by 3 months after surgery.
Conclusion: Owing to its physicochemical characteristics, even with sophisticated surgical techniques, GeneX cannot be recommended for use in percutaneous vertebroplasty for OVCF. The long-term safety and efficacy of GeneX need to be further validated through Phase II clinical trials. Lumbar cistern drainage can significantly improve neurological deficits in patients caused by GeneX implantation syndrome.
Keywords: vertebroplasty, osteoporosis, bone cements, fractures, bone
Introduction
Percutaneous vertebroplasty with polymethylmethacrylate (PMMA) is widely used to treat osteoporotic vertebral compression fracture (OVCF) and can relieve the associated low back pain rapidly.1 However, PMMA bone cement presents notable limitations, including its non-biodegradable nature and elevated biomechanical stress, which may contribute to vertebral re-collapse and subsequent instability.2 This instability not only exacerbates spinal degenerative processes and micromotion but may also trigger the formation of a reactive biological membrane around extravasated cement- a mechanism analogous to the fibrous encapsulation observed around PMMA spacers in Masquelet’s induced membrane technique.3 Therefore, there has been a need for a better vertebral filling material. GeneX (Biocomposites Ltd, Keele, UK) is an injectable composite of calcium sulfate and tricalcium beta-phosphate (β-TCP) with a weight ratio of 1:1. According to the manufacturer, it has the ability to adsorb and aggregate specific molecules and proteins, promote bone formation, and set with a high degree of compressive strength in situ at body temperature within 15 minutes, after which it is gradually absorbed. According to the literature, GeneX can be used as an alternative to PMMA in percutaneous vertebroplasty and has good clinical outcomes.4 We designed a prospective cohort study to assess the clinical efficacy of percutaneous vertebroplasty using GeneX in patients with OVCF. Leak of the artificial bone material was detected in four (57.1%) of the first seven patients enrolled in the study. The leaks were intradiscal and paravertebral in three patients and intradural and subdural in one, resulting in severe neurological deficits. This is the first report of serious complications after percutaneous vertebroplasty using GeneX and includes a literature review.
Case Presentation
The patient was a 70-year-old woman who was admitted to hospital with low back pain after a fall while traveling 5 days earlier. On admission, a magnetic resonance imaging examination revealed an OVCF at T12. The patient had a 5-year history of hypertension and was on antihypertensive medication but did not take it regularly. She had been diagnosed to have type 2 diabetes mellitus 10 years earlier and self-administered insulin but did not monitor her blood glucose levels.
Percutaneous vertebroplasty with GeneX was performed for the OCVF at T12. The patient did not complain of discomfort during the procedure and returned to the ward uneventfully. Two hours later, she started to complain of pruritus and weakness in both lower limbs. Physical examination showed her muscle strength in the right lower limb to be grade 2 in iliopsoas and grade 4 in quadriceps femoris, tibialis anterior, extensor hallucis, extensor toe, and gastrocnemius. The muscle strength was grade 4 in the left lower limb. Hormone pulse therapy and analgesics did not improve her symptoms. By 3 hours postoperatively, the patient was in a comatose state with a blood pressure of 88/56 mmHg and oxygen saturation of 98% but was responsive to deep stimulation. Her condition then deteriorated suddenly, with a further decrease in blood pressure to 78/51 mmHg. Intravenous dopamine was administered to maintain her blood pressure. A few moist rales were heard in both lungs, and there was a large amount of frothy white sputum in her throat. Direct and indirect pupillary light reflexes were slow. The patient was transferred to the intensive care unit, where she was intubated and treated by cooling measures and sedation for febrile convulsions.
Magnetic resonance imaging of the brain revealed cerebral artery stenosis but no evidence of early cerebral infarction or intracerebral hemorrhage. A computed tomography scan of the spine showed a high-density mass in the ventral epidural and intradural space at the T9 to L2 vertebral levels, especially on the left side (Figure 1). On postoperative day (POD) 1, the patient was still in a coma with a low-grade fever. At this time, her blood pressure was stable without medication. However, she had not resumed spontaneous breathing. On POD 2, she developed somnolence but could open her eyes on verbal command. Her temperature was 39.4°C at this time. Muscle strength was grade 2 in the upper extremities and grade 1 in the lower extremities. The patient resumed spontaneous breathing (12 breaths per minute) on POD 3. Lumbar cistern drainage revealed reddish-tinged cerebrospinal fluid, which was analyzed for cytology (Table 1). On POD 5, the patient was successfully weaned from the ventilator and her tracheal cannula was removed. At this time, her muscle strength was grade 3 in both upper extremities, grade 2 in the right lower extremity, and grade 3 in the left lower extremity. The patient was transferred to the rehabilitation department where she was treated with acupuncture and underwent rehabilitative training. She was able to walk without assistance 1 month later but had lower urinary tract symptoms related to a long-term indwelling catheter. The patient resumed her normal activities of daily living at 3 months after surgery.
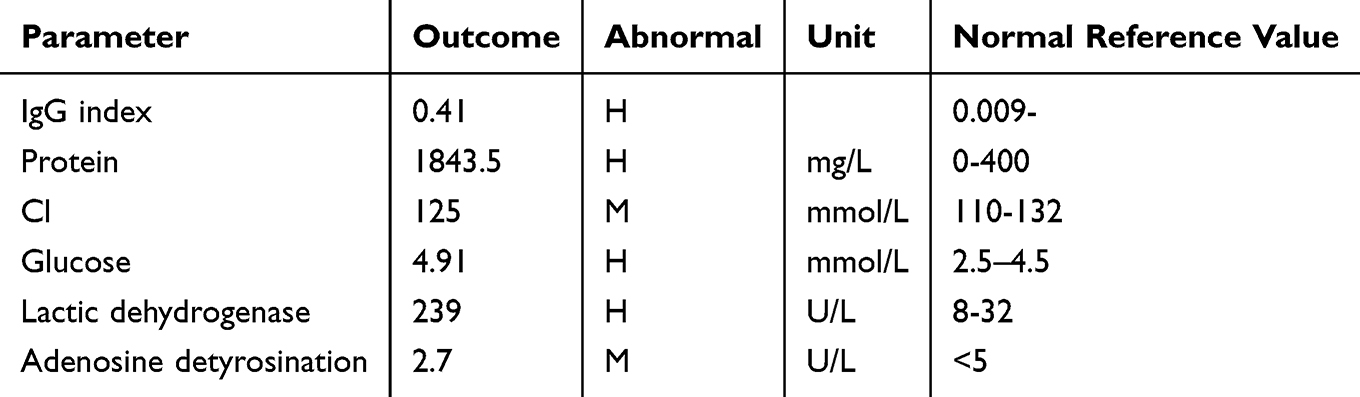 |
Table 1 Findings on Analysis of Cerebrospinal Fluid |
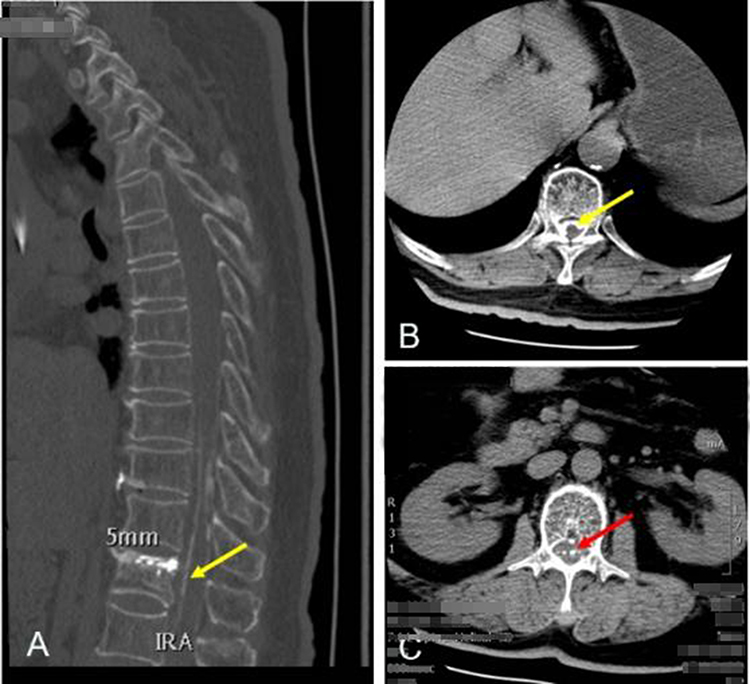 |
Figure 1 Postoperative computed tomography scans. The yellow arrow in (A and B) indicates epidural leak. The red arrow in (C) indicates intradural leak. |
Discussion
Percutaneous vertebroplasty was first performed in France in 1984, first described by Galibert et al in 1987,5 and introduced in the US in 1993.6 It can rapidly restore vertebral height, correct kyphosis, stabilize the spine, and relieve pain, and has been used widely in clinical practice.7,8 PMMA is commonly used as a filler in percutaneous vertebroplasty and has achieved good clinical results, especially in terms of pain relief, but has been criticized for its poor biocompatibility and unsatisfactory long-term clinical efficacy. GeneX has been reported to be effective when used in vertebroplasty for OVCF9 and to maintain vertebral height in the short term, promote rapid improvement of vertebral strength and stiffness, and to have a low complication rate. We initiated a prospective cohort study to evaluate the short-term and long-term outcomes of vertebroplasty with GeneX. Leak of this material was detected in four (57%) of the first seven patients enrolled and was symptomatic in one case (14.2%). The mean visual analog scale (VAS) pain score decreased significantly from 5.0 ± 2.0 preoperatively to 3.4 ± 2.7 at 24 h after surgery (P<0.05). The Cobb angle was corrected by an average of 6.50 ± 4.0°. Review of radiographs obtained at 3 months postoperatively showed no significant loss of vertebral height (P>0.05). The VAS pain score was better in the PMMA group than in the GeneX group at 1 month postoperatively (P<0.05). There was no significant between-group difference in recovery of vertebral height at the 6-month postoperative follow-up visit (P>0.05).
The available literature suggests that β-TCP and calcium sulfate are safe and efficacious artificial bone filling materials.10 However, serious complications occurred when GeneX is used as a bone graft in spinal decompression and fusion surgery.11 Three patients in that study developed sterile pus in soft tissues adjacent to the site where GeneX was injected, followed by breakdown of the skin in two cases and pharyngeal perforation in one. In a study in mice, injection of GeneX produced moderate or severe skin damage and inflammation in the dermis, whereas controls that received DBX (demineralized bone matrix) or saline injection showed no or only mild skin damage.
Friesenbichler et al reported the type and frequency of complications observed in patients treated for bone tumors by curettage and filling of the defect using GeneX.12 Five (16%) of their 31 patients developed complications after surgery. In three of these five patients, sterile inflammation developed adjacent to the site where GeneX was injected, with delayed wound healing in two cases and local pain in one. In the third patient, GeneX produced moderate to severe skin damage in the area of the scar, which needed revision surgery. In the other two patients, inflammatory cysts measuring up to 15 cm developed in the soft tissue and gradually reduced in size over time. The authors concluded that GeneX causes soft tissue inflammation and pain and that this type of bone substitute should not be used in the treatment of bone defects.13
Park et al described complications related to GeneX in some cases after skull reconstruction,14 including early resorption of GeneX before bone regeneration, formation of serous cysts, and local inflammation. Use of GeneX at anatomic sites adjacent to the nervous system, such as the skull, might cause neurological deficits as a consequence of subcutaneous inflammation and cysts. They concluded that there is a need for more extensive research regarding the safety and potential complications of GeneX.
In a letter to the editor,15 Laycock and Cooper, both of whom are employees in the product development section of Biocomposites Ltd., offered an alternative view to that expressed by Friesenbichler et al.12 They commented that the data published by Redenbacher indicated a 16% complication rate, which is less than the 33% quoted above when using allografts and autografts.14 The worst case involved severe damage to the skin, histology examination of which showed chronic lymphocytic inflammation with plasma cells.12 They also mentioned the concomitant use of allograft material in that case and considered that attribution of all the adverse events that occurred to GeneX was questionable. Friesenbichler et al believed that the instructions for GeneX advise not to overfill or pressurize the treatment site and recommend avoiding the addition of other substances to the product.12 However, The usage guidelines for GeneX warn against overfilling or pressurizing the treatment site and suggest not mixing the product with other substances.14 Therefore, Laycock and Cooper considered it arbitrary to conclude that according to the data published by Redenbacher, GeneX is not recommended for treating bone defects and that the results did not support their conclusions.14 In the same letter, they also responded to comments on a paper by Saadoun et al.11 GeneX is approved as a Class II medical device by the US Food and Drug Administration (FDA), is CE marked in compliance with the Medical Devices Directive 93/42/EEC and meets all safety and biocompatibility standards. Since its introduction in 2004, over 20,000 packs of GeneX have been utilized globally, according to our internal records (procedure QAP0018), the complaint rate has been 0.24%.14
The reported rate of PMMA leak after percutaneous vertebroplasty ranges from 38% to 87.9%.15 Leak of bone cement into the intradural, epidural, paravertebral, and venous areas may result in serious complications, including increased pain, radiculopathy, spinal cord compression, and pulmonary embolism.16 Until now, there have been no reports of serious complications involving leak of GeneX artificial bone after percutaneous vertebroplasty. Unlike PMMA, GeneX must be in a paste state in order for the β-TCP/calcium sulfate to be pushed through the channel into the vertebral body. Without sufficient viscosity, β-TCP/calcium sulfate can easily flow into the paravertebral, intradiscal, epidural, foraminal, and venous areas along the needle track. A major problem with GeneX is that the flow of β-TCP/calcium sulfate cannot be observed by intraoperative fluoroscopy (Figure 2). Two punctures were performed during the operation. Possible reasons for this rare complication were perforation of the medial wall and penetration of the dura during needle insertion through the pedicle at the time of the first puncture. The second puncture entered the vertebral body through the pedicle, and the position was confirmed to be good under C-arm fluoroscopy. When the β-TCP/calcium sulfate was injected into the vertebral body through the second channel, some of it leaked into the epidural space via the first channel (Figure 3). The patient did not report any discomfort at that time. However, based on the clinical symptoms and imaging findings, we concluded that a small amount of β-TCP/calcium sulfate slowly infiltrated into the subarachnoid space through the needle hole injury in the dural area and caused central nervous system depression, manifesting as a decrease in blood pressure, acute flaccid paralysis, depression of the respiratory center, and a comatose state. The β-TCP/calcium sulfate was in a paste state and was eventually cleared from the central nervous system by lumbar cistern drainage and circulation of cerebrospinal fluid, leading to resolution of the patient’s symptoms within a short time. All of the patient’s symptoms eventually disappeared when the β-TCP/calcium sulfate was completely metabolized.
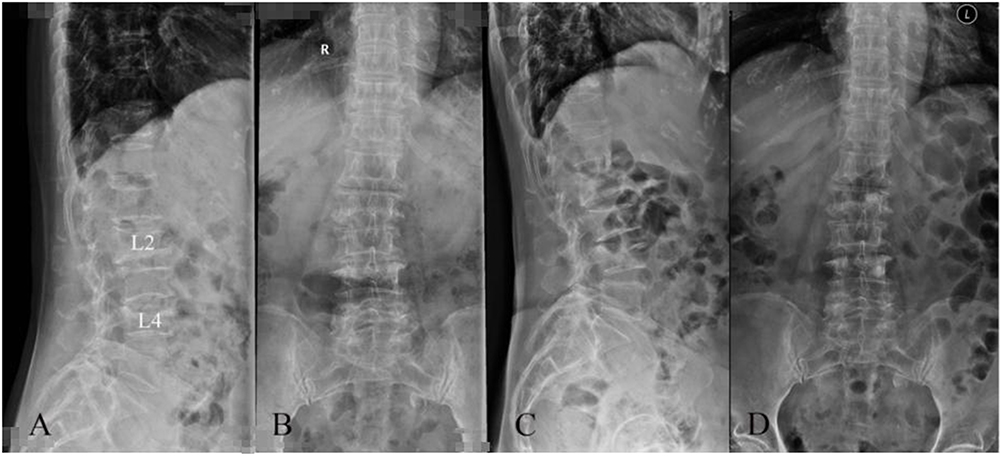 |
Figure 2 (A and B) Preoperative X-ray of OVCF at L2 and L4. (C and D) Postoperative X-ray of vertebroplasty using GeneX. |
 |
Figure 3 Intraoperative scan showing the needle track. (A) Red line indicated first puncture channel. (B) Yellow line indicated second puncture channel. |
The FDA and Medicines and Healthcare products Regulatory Agency classify bone graft substitutes as medical devices. Unlike drugs, medical devices do not require clinical safety testing before use. In view of our experience with GeneX and review of the literature, we urge caution when using GeneX as a bone graft substitute. We recommend that bone graft substitutes undergo rigorous clinical safety testing before approval for use in patients. Reclassifying bone graft substitutes as drugs is one way to ensure clinical safety. The FDA6 definition of a medical device states that “A product is usually a drug if its primary intended use is achieved by chemical action or metabolism by the body”. Artificial bone graft substitutes are more like drugs than devices because they are composed of chemicals that work by stimulating bone-forming cells to produce new bone. Therefore, GeneX cannot be recommended for use in percutaneous vertebroplasty for OVCF.
Conclusion
Owing to its physicochemical characteristics, even with sophisticated surgical techniques, GeneX cannot be recommended for use in percutaneous vertebroplasty for OVCF. The long-term safety and efficacy of GeneX need to be further validated through phase ii clinical trials. Lumbar cistern drainage can significantly improve neurological deficits in patients caused by GeneX implantation syndrome.
Informed Consent
This case series was approved by the Research Ethical Committee of 920th Hospital of Joint Logistics Support Force. Informed consents to publish have been obtained from both patients and also from the patient’s legal guardian for the case.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lamanna A, Maingard J, Kok HK, et al. Vertebroplasty for acute painful osteoporotic vertebral compression fractures: an update. J Med Imaging Radiat Oncol. 2019;63:779–785. doi:10.1111/1754-9485.12900
2. Yu W, Xu W, Jiang X, et al. Risk factors for recollapse of the augmented vertebrae after percutaneous vertebral augmentation: a systematic review and meta-analysis. World Neurosurg. 2018;111:119–129. doi:10.1016/j.wneu.2017.12.019
3. Ma CH, Chiu YC, Tsai KL, et al. Masquelet technique with external locking plate for recalcitrant distal tibial nonunion. Injury. 2017;48:2847–2852. doi:10.1016/j.injury.2017.10.037
4. Zhan BL, Ye Z. Significance of percutaneous vertebroplasty with Genex in the treatment of thoracolumbar burst fractures. Zhongguo Gu Shang. 2011;24:223–226.
5. Galibert P, Deramond H, Rosat P, Le Gars D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33:166–168.
6. Jensen M. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997;12(10):1897–1904.
7. Hadjipavlou AG, Tzermiadianos MN, Katonis PG, Szpalski M. Percutaneous vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and osteolytic tumours. J Bone Joint Surg Br. 2005;87:1595–1604. doi:10.1302/0301-620X.87B12.16074
8. Pateder DB, Khanna AJ, Lieberman IH. Vertebroplasty and kyphoplasty for the management of osteoporotic vertebral compression fractures. Orthop Clin North Am. 2007;38:409–418. doi:10.1016/j.ocl.2007.03.010
9. Zhang S, Jiang J, Zhu Q, Huang Z. Biomechanical study of vertebroplasty with geneX((R)) cement augmentation in a calf osteoporotic vertebral compression fracture model. Nan Fang Yi Ke Da Xue Xue Bao. 2012;32:843–846.
10. Van Hoff C, Samora JB, Griesser MJ, Crist MK, Scharschmidt TJ, Mayerson JL. Effectiveness of ultraporous beta-tricalcium phosphate (vitoss) as bone graft substitute for cavitary defects in benign and low-grade malignant bone tumors. Am J Orthop. 2012;41:20–23.
11. Saadoun S, Macdonald C, Bell BA, Papadopoulos MC. Dangers of bone graft substitutes: lessons from using GeneX. J Neurol Neurosurg Psychiatry. 2011;82:232–237. doi:10.1136/jnnp.2010.232371
12. Friesenbichler J, Maurer-Ertl W, Sadoghi P, Pirker-Fruehauf U, Bodo K, Leithner A. Adverse reactions of artificial bone graft substitutes: lessons learned from using tricalcium phosphate geneX(R). Clin Orthop Relat Res. 2014;472:976–982. doi:10.1007/s11999-013-3305-z
13. Park JH, Suh SJ, Lee YS, Lee JH, Ryu KY, Kang DG. Lytic complications after skull reconstruction using GeneX(R). Korean J Neurotrauma. 2015;11:135–138. doi:10.13004/kjnt.2015.11.2.135
14. Friesenbichler J, Maurer-Ertl W, Sadoghi P, Pirker-Fruehauf U, Bodo K, Leithner A. Reply to the letter to the editor: adverse reactions of artificial bone graft substitutes: lessons learned from using tricalcium phosphate geneX (R). Clin Orthop Relat Res. 2014;472:767–768. doi:10.1007/s11999-013-3421-9
15. Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res. 2018;13:264–269. doi:10.1186/s13018-018-0952-5
16. Cosar M, Sasani M, Oktenoglu T, et al. The major complications of transpedicular vertebroplasty. J Neurosurg Spine. 2009;11:607–613. doi:10.3171/2009.4.SPINE08466
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges in Delivering Effective Care for Older Persons with Fragility Fractures
Hurtado Y, Hernández OA, Atencio De Leon DP, Duque G
Clinical Interventions in Aging 2024, 19:133-140
Published Date: 24 January 2024
Bone Cements Used in Vertebral Augmentation: A State-of-the-art Narrative Review
Williams TD, Adler T, Smokoff L, Kaur A, Rodriguez B, Prakash KJ, Redzematovic E, Baker TS, Rapoport BI, Yoon ES, Beall DP, Dordick JS, De Leacy RA
Journal of Pain Research 2024, 17:1029-1040
Published Date: 13 March 2024