Back to Journals » Journal of Pain Research » Volume 14
Percutaneous Vertebroplasty for C1 Osteolytic Lesions via Lateral Approach Under Fluoroscopic Guidance
Authors Yang Y, Tian Q ![]() , Wang D, Yi F, Song H, Li W, Wu C
, Wang D, Yi F, Song H, Li W, Wu C
Received 30 April 2021
Accepted for publication 30 June 2021
Published 13 July 2021 Volume 2021:14 Pages 2121—2128
DOI https://doi.org/10.2147/JPR.S318236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Yue Yang, Qinghua Tian, Dan Wang, Fei Yi, Hongmei Song, Wenbin Li, Chungen Wu
Department of Diagnostic and Interventional Radiology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai, People’s Republic of China
Correspondence: Chungen Wu; Wenbin Li
Department of Diagnostic and Interventional Radiology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, 600 Yi Shan Road, Shanghai, People’s Republic of China
Tel/Fax +86 18930177559
; +86 18930177524
Email [email protected]; [email protected]
Objective: To report our experience of treating painful C1 osteolytic lesions with cement augmentation via a lateral approach under fluoroscopic guidance.
Materials and Methods: Nine consecutive patients (eight men and one woman; mean age: 56.7± 13.2 years) with osteolytic lesions of the atlas who underwent cementoplasty via a lateral approach were enrolled in this study. The technical success rate, operation time, and complications were recorded. Visual analogue scale (VAS) and Neck disability index (NDI) were used to evaluate the pain relief and neck function status pre-procedure (baseline) and post-procedure (at 3 days; after 1, 3, 6, 12, 18, and 24 months; and at the last follow-up).
Results: The procedure was technically successful without any complications in all patients. The mean procedure time was 44.3± 7.8 min. There were three cases of bone cement leakage, but no clinical symptoms. The mean VAS score decreased from 6.7± 1.0 before the procedure to 3.7 three days after the procedure. The mean NDI score decreased from 67.3± 11.2 before the procedure to 39.3± 13.7 three days after the procedure. The VAS and NDI scores decreased at each follow-up time point, and the difference was statistically significant compared with the scores before the procedure (P< 0.01).
Conclusion: Fluoroscopy-guided lateral approach is a feasible, safe, and effective method for treatment of osteolytic lesions of the atlas and can relieve pain and stabilize the bone.
Keywords: atlas, C1, lateral, vertebroplasty, fluoroscopy
Introduction
In the past few decades, percutaneous vertebroplasty (PVP) has been shown to be effective in relieving pain and stabilizing the spine in the treatment of spinal tumors. Given the significant advantages of this procedure, it has also been used in the treatment of cervical osteolytic lesions. However, in the cervical spine, C1 (also known as the atlas) has the most special anatomic shape and position. The atlas is circular with no vertebral body and has two bilateral lateral masses. The atlas is at the craniocervical junction and is surrounded by important blood vessels and nerves. The vertebral artery and suboccipital nerve run cranially in the posterior superior horn of the atlas. The bilateral lateral mass of the atlas support the skull by forming a joint with the occipital bone.1 Therefore, osteolytic lesions in the C1 region have unstable characteristics and need to be treated in a timely manner.2,3 For cancer patients with limited life expectancy, PVP is the most suitable choice to relieve pain, maintain head activity, and obtain spinal stability.4
As per current literature, PVP of the C1 has been rarely reported. The puncture approaches mainly include transoral, lateral, posterolateral, and anterior retropharyngeal approaches.5–14 Among them, only transoral PVP has been proven to be a relatively safe procedure, but it is not suitable for all patients.
To our knowledge, only 29 atlas vertebrae have been reported across all existing publications, and 22 of them were treated using PVP by transoral approach.5,6,8,9,14 Other puncture routes are rarely mentioned, and most of them are in the form of case reports.7,10–13 They used different puncture methods, and all studies used auxiliary means such as preventive vertebral artery occlusion and CT-guided puncture positioning.
The lack of relevant reports reflect the rare incidence rate of C1 lesions and the challenge of navigating around important structures in close proximity to the atlas. Therefore, there is an urgent need for more experienced clinical practice regarding C1 bone cement augmentation. The purpose of this study was to report our experience in the treatment of painful C1 osteolytic lesions with cement augmentation via a lateral approach under fluoroscopic guidance.
Materials and Methods
Study Design and Patients
This study was a single-center, retrospective study. This study was approved by the institutional review board of our Hospital and all patient provided written informed consent. All procedures were in accordance with the ethical standards of the agency and/or the National Research Council, as well as the 1964 Helsinki Declaration and subsequent amendments or similar ethical standards. From January 2011 to December 2020, nine consecutive patients (eight men and one woman; mean age: 56.7±13.2 years) with osteolytic lesions of the atlas who underwent cementoplasty were enrolled in this study. All patients were referred to our department because of severe pain that could not be relieved by conventional treatment such as opioids, radiotherapy, and chemotherapy. None of the patients had any neurological deficit, and had a life expectancy of more than 3 months.
The treatment plan of each patient was decided by a multidisciplinary team composed of interventional physicians, neurosurgeons, and orthopedic specialists after excluding the contraindications of interventional procedures, including uncorrectable coagulation disorders (International normalized ratio: >1.5, platelet count: <90,000/ mm3) and persistent systemic infection.
Data of patients, including age and primary tumor were prospectively entered into the database. Meanwhile, we provide a questionnaire for patients awaiting treatment to reflect the severity and duration of the pain and dysfunction. Before treatment, computed tomography (CT) or both CT and magnetic resonance imaging (MRI) were performed to confirm the shape and characteristics of osteolytic lesions and to ascertain whether there were pathological fractures and bone wall damage.
Procedure
Under the guidance of biplane fluoroscopy (axiom Zee biplane), all procedures were performed with the patient in a left or right lateral position. The whole process of PVP was monitored by electrocardiography, pulse oxygen saturation, and non-invasive blood pressure readings. All interventional procedures were performed using a lateral approach. Briefly, the patient’s jaw was raised to fully expose the neck. According to the preoperative non-enhanced CT and enhanced MRI, the puncture path was determined, and the needle entry point and needle entry angle and depth were designed, and appropriate marks were made on the body surface. The C1 lateral mass was projected under the guidance of anteroposterior and lateral fluoroscopy, and the lines were drawn on the body surface respectively. The intersection of the two lines was used as the superficial landmark.
After disinfection of the puncture site, the puncture approach was anesthetized layer-by-layer with 2% lidocaine (Astra). In order to prevent anesthetics from being injected into the blood vessels, the combination of injection and withdrawal was used. A 17G coaxial biopsy needle (C1816A, Bard Peripheral Vascular Inc.) was used for puncture. The coaxial biopsy needle included a conventional puncture needle and an additional blunt tip stylet. Under the guidance of biplane fluoroscopy, the needle was inserted from the anterior edge of the mastoid process and the posterior edge of the mandible, and slowly pushed forward along the posterior edge of carotid sheath and the anterior edge of the transverse foramen of the atlas (Figure 1). During this time, the patient’s reaction was closely monitored. During the puncture process, before entering the bone, the additional blunt tip stylet was used in the soft tissue to move forward along the space between the carotid sheath and the vertebral artery, to avoid damaging the blood vessels and achieve safe insertion. When the puncture needle reached the atlas, the angle was adjusted to make the puncture needle enter the lesion along the front edge of the transverse foramen of the atlas to avoid damaging the vertical upward vertebral artery in the transverse foramen. This is the first key point. After aligning with the lesion area of the atlas, the lesion was slowly punctured and the needle moved into the predetermined position; the trocar was then pulled out to establish the working path.
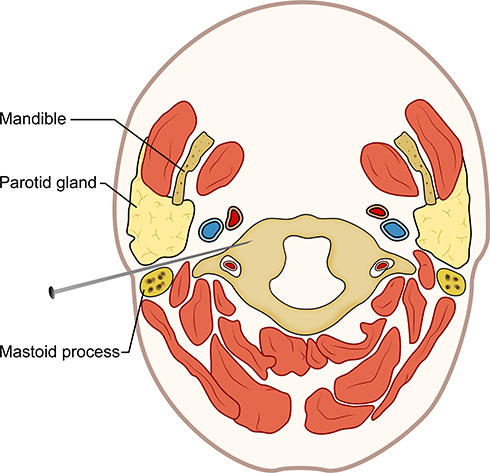 |
Figure 1 Anatomical diagram of the PVP puncture path using a lateral approach via the space between the carotid sheath and vertebral artery. |
Before injection of bone cement, angiography with contrast medium was performed to observe the details of the peripheral vessels. Bone cement (polymethylmethacrylate [PMMA]) (PALACOS®V) was then prepared and loaded into the dispenser. PMMA was injected in very small increments (about 0.1–0.3-mL increments). The diffusion of PMMA was closely monitored under anteroposterior and lateral fluoroscopy. When the bone wall of the transverse foramen is damaged, it is necessary to strictly control the amount of injection to avoid diffusion of the cement to the transverse foramen area. This is the second key point. Under biplane fluoroscopy, the injection was stopped when the PMMA reached the edge of the atlas or when it encountered a similar resistance feeling during injection. The procedure was then terminated (Figures 2 and 3)
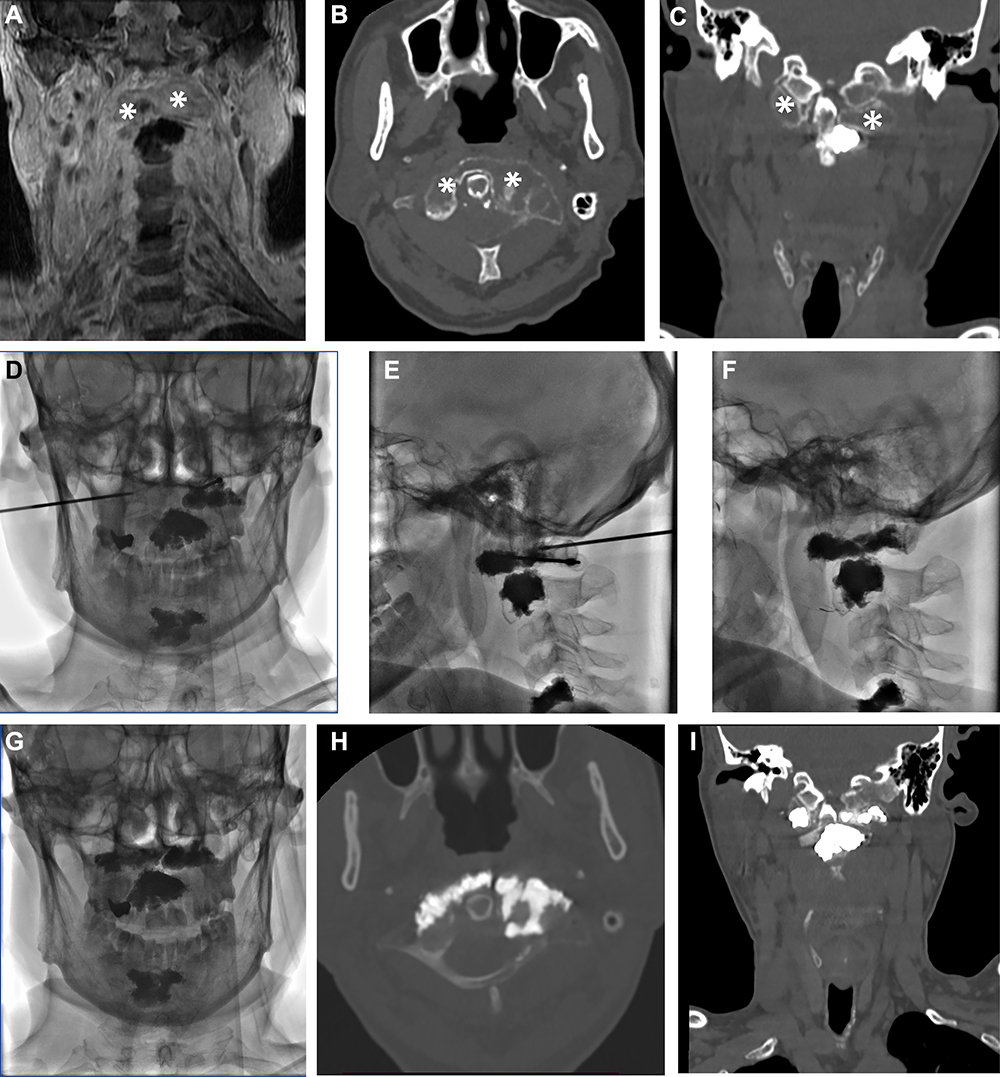 |
Figure 2 A 65-year-old man with atlas metastasis due to prostate cancer. (A) coronal T1W non-suppressed fat MR enhancement sequence showed obvious bone destruction and soft tissue mass in the lesion, and the mass showed abnormal enhancement (asterisk). (B and C) axial and reconstructed coronal images showed osteolytic lesions (asterisks) in the bilateral lateral mass of the atlas, with enlargement of the left lateral mass. (D and E) showed that the puncture was successful through the lateral approach guided by biplane fluorescence, and the puncture needle accurately entered the target site. (F and G) showed that the bone cement of the bilateral side mass was well dispersed. (H and I) axial and reconstructed coronal images of non-enhanced CT immediately after operation showed no leakage of bone cement. |
 |
Figure 3 A 55-year-old woman presented with bone destruction in the left lateral mass of the atlas due to lymphoma. (A and B) Axial and reconstructed coronal images showed osteolytic lesions (asterisks) in the left lateral mass of the atlas, bone destruction in the anterior part of the left lateral mass, and around the transverse foramen, and the lesion is adjacent to the vertebral artery with unclear boundary (arrow). (C) Axial T1W fat suppression MR enhancement sequence showed bone destruction and soft tissue mass in the left lateral mass (asterisks). The mass showed abnormal enhancement, and the mass surrounded the left vertebral artery (white arrow). (D, E and F) showed that the lateral puncture under the guidance of biplane fluorescence was successful, and the puncture needle accurately entered the target area, and the bone cement was well dispersed. (G) Axial CT image immediately after operation showed no cement leakage around the vertebral artery (white arrow). (H) Coronal reconstructed CT image immediately after operation showed a little bone cement leaked into the soft tissue below the left mass of atlas (white arrow). |
Data Collection
This study was a single center, prospective, observational experiment performed using the same group of patients before and after the comparison to evaluate the treatment effect.
The technical success of the procedure was defined as successful puncture into the proper part of the atlas through the lateral approach with no obvious complications occurring during the injection of bone cement. The volume of bone cement injected into the atlas and the procedure duration were recorded. During the procedure, related complications such as infection, pulmonary embolism, and systemic manifestations were recorded.15 Two specialists (each with more than 10 years’ clinical experience) performed the clinical examinations on all patients.
The clinical outcome was evaluated by the visual analogue scale (VAS) and Neck Disability Index (NDI). The VAS score was used to reflect the severity of subjective pain. VAS scores ranged from 1 to 10, wherein a score of 0 indicated no pain and a score of 10 indicated the most severe pain. NDI was used to evaluate the severity of dysfunction caused by neck symptoms.16 An NDI questionnaire comprises 10 questions, and each item has six possible answers. The score ranges from 1 to 100. The higher the score, the higher the degree of neck dysfunction.
Both VAS and NDI scores of patients were recorded pre-operation (baseline) and at 3 days, 1 month, 3 months, 6 months, 12 months, and 18 months post-operation, until the final follow-up.
Statistical Analysis
All statistical tests were conducted using SPSS 25.0 (IBM Corporation) software. The data were expressed as mean±standard deviations. The paired t-test was used to compare the differences of mean VAS scores and NDI between each follow-up point and preoperative scores. P<0.05 was considered to indicate statistical significance.
Results
Patient Demographics
The demographic and clinical characteristics of the patients are shown in Table 1.
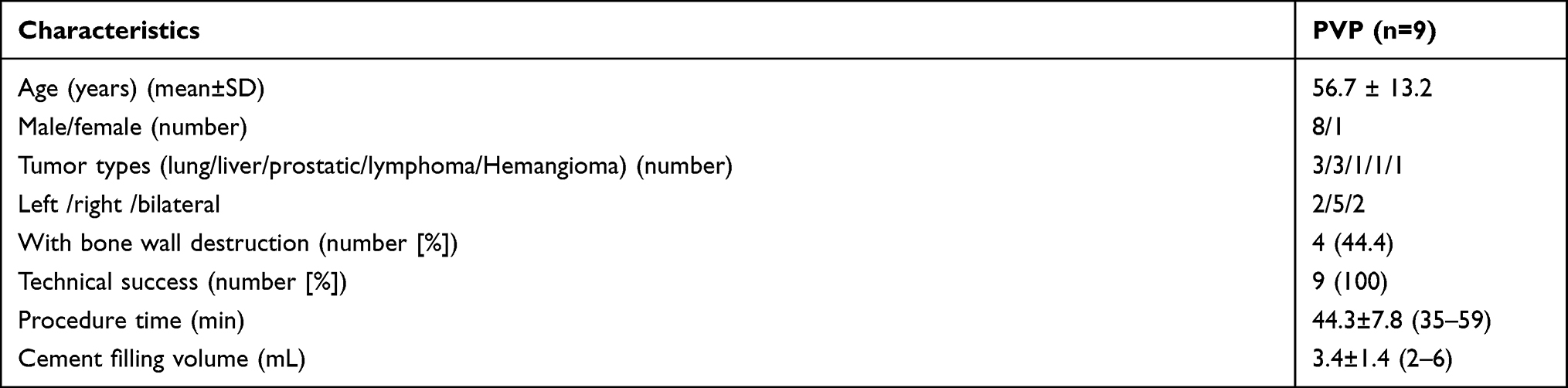 |
Table 1 Baseline Characteristics and Clinical Outcomes of the Patients |
Of the nine patients, seven had metastatic tumors of the atlas. The primary tumors were from the lung (n=3), liver (n=3), and prostate (n=1). The remaining two cases were a hemangioma and a primary lymphoma of the spine. The lesions were located in the lateral mass of the atlas–seven were unilateral and two were bilateral. Out of nine cases of osteolytic lesions, four had bone wall destruction. The interval between non-enhanced CT evaluation and the procedure ranged from 1 to 8 days (mean: 3.9±2.4 days).
Procedure Safety
The procedure was technically successful in all patients. All patients tolerated the procedure under local anesthesia. There were no documented neurological and/or important vascular damage or other complications such as infection, pulmonary embolism, and systemic manifestations.
The procedure time ranged from 35 min to 59 min (mean: 44.3±7.8 min). The volume of bone cement injected into each atlas ranged from 2.0 to 6.0 mL (mean: 3.4±1.4 mL). Two patients had lesions on the bilateral lateral mass of the atlas, and the amount of bone cement injected was the sum of the two sides. Of the nine cases, three (33.3%) had cement leakage. In all three cases, the cement leaked to the soft tissue around the C1-C2 joint. No patients presented with clinical symptoms due to bone cement leakage.
Clinical Evaluation
The VAS score was 6.7±1.0 before the procedure, 3.7±0.7 three days after the procedure, and 2.8 ± 0.8 one month after the procedure. The NDI score decreased from 67.3±11.2 before the procedure to 39.3±13.7 three days post-procedure. Meanwhile, the mean VAS and NDI scores at each post-procedural time point decreased, and the difference was statistically significant compared with the scores before the procedure (P<0.01) (Table 2, Figure 4).
 |
Table 2 Clinical Outcomes as Assessed by VAS Scores and NDI During Follow Up |
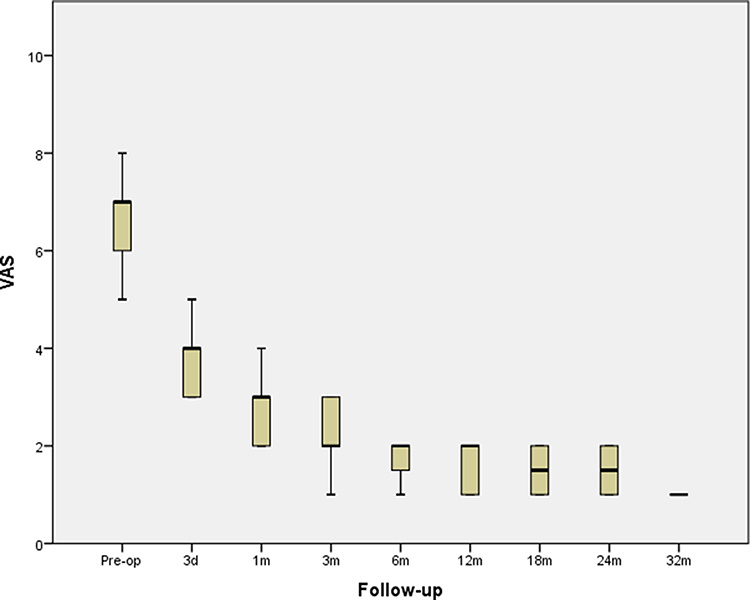 |
Figure 4 The process of pain relief (assessed by VAS) before and after the procedure and during follow-up. Abbreviation: VAS, Visual Analog Scale. |
The follow-up time ranged from 3 to 32 months, and the mean follow-up time was 14.4±9.7 months. Up to the final follow-up, four patients died of the primary tumor.
Discussion
Although metastases are the most common osteolytic lesions in C1, C1 metastases are still rare compared to other spinal metastases, accounting for <1% of all spinal metastases.17 Although the quality of life and survival time of patients with metastatic spinal tumors have been significantly improved, palliative treatment is still the main goal of treatment. PVP has an irreplaceable value in pain relief and vertebral reinforcement in patients with C1 osteolytic lesions.4 Owing to the complex anatomical structure of C1 and its close proximity to the surrounding important structures, C1 cementoplasty is very challenging. Excluding PVP via the transoral approach, the evidence of other puncture approaches is very limited. Our report shows that nine consecutive patients underwent successful puncture via the lateral approach under fluoroscopic guidance. The procedure was successfully completed under local anesthesia without complications in all patients. Three of the nine patients had asymptomatic bone cement leakage. The effect of relieving pain, maintaining head activity, restoring stability, and preventing fracture is noteworthy. Through this series of cases, we can provide a safe and effective treatment for patients with C1 metastasis and hemangioma. The treatment experience of patients with C1 symptomatic osteolytic lesions has been increased.
The puncture route of the lateral approach is to enter the needle between the internal carotid artery, vein, and vertebral artery. There are very few reports in the past, and all of them used CT-guided puncture positioning.7,12 To our knowledge, this is the first fluoroscopically guided C1 cementoplasty via the lateral approach and the largest sample size study except for a report on C1 cementoplasty via the transoral approach.6 In the past, it was considered that the lateral approach was very dangerous, as the space between the carotid sheath and vertebral artery was very narrow, and the needle entry direction was perpendicular to the vertebral artery. However, our experience is that the lateral approach is relatively safe and has unique advantages, especially when the main body of the lesion is located in the lateral mass. Because the needle is inserted along the front edge of the transverse process hole of the atlas, it bypasses the vertical vertebral artery in the transverse process hole, and also directly bypasses the horizontal V3 segment of the vertebral artery. When the puncture needle bypasses this critical area, it can fine tune the angle in all directions to accurately enter the lesion, because it is relatively safe for the V3 segment of the vertebral artery and the accompanying suboccipital nerve.
The innovation of our technology was the use of additional blunt tip stylet in the puncture needle complex, thus reducing the puncture risk associated with neurovascular structures. It improves the safety of puncture under fluoroscopy. Moreover, when the main body of the lesion was located in the lateral mass, the volume of the lesion area increased because of the existence of tumor tissue, which can increase the space for safe insertion. In addition, the needle direction was along the long axis of the lesion, which seems to be the best treatment choice for such patients.
In addition to the methods we reported, the puncture paths of C1 cementoplasty mainly include the transoral approach, posterolateral approach, anterolateral approach, and retropharyngeal approach. Theoretically, each puncture route has its advantages and disadvantages. However, owing to the low incidence rate of C1 and the challenge of treatment, some methods still lack clinical practice.
Transoral Approach
C1 vertebroplasty via the transoral approach is the most commonly reported method in literature.5,6,8,18 It is the most direct route from C1, and the direction of needle entry is safe for the vertebral artery, unless there are some patients with congenital variation of blood vessels.19 However, the needle path has a medial to lateral direction, which is often not along the long axis of the lesion. Moreover, under fluoroscopic guidance, the skull will obviously block the field of vision. At the same time, some patients such as those after parotid gland cancer surgery cannot achieve the action required by the oral spreader. In addition, it does increase the risk of infection.
Posterolateral Approach
The puncture path of the posterolateral approach is that the needle passes through the posterior cervical space and advances forward and from the outside to the inside. The advantage is to avoid injury to the anterolateral carotid artery, away from the vertebral artery in the transverse foramen, and relatively safely to the spinal cord. The difficulty lies in the potential harm to the horizontal segment of the vertebral artery, because it is horizontal and slightly oblique along the vertebral artery sulcus, and accompanied by suboccipital nerve. The special transverse and oblique upward direction of the vertebral artery makes it very difficult to avoid this segment of the vertebral artery when inserting the needle. It has been reported that prophylactic occlusion of the vertebral artery was used to avoid cement entering the vertebral artery.20 However, this is not feasible if there are lesions in both lateral masses of the atlas.
Anterolateral Approach
We believe that this method is not convenient, and the path of the needle is very long, and it needs to extend the cervical spine properly. However, for obese patients and patients with severe pain, it is difficult to maintain excessive stretching. Therefore, it is not suitable for each patient and it depends on the specific anatomical structure.
Our case series has some limitations. First, our case series is from a single center. Because of the low incidence rate of osteolytic lesions in C1, the sample size is small; our findings should be verified in studies with a larger sample size. Second, the study lacked a control group. Third, the procedure described in this study was completed by experienced interventional doctors. For those who are not familiar with this technology, this procedure could be somewhat challenging to perform. Our results need further validation. However, we believe our report has still provided a method and experience for the program to achieve a wider range of applications.
Conclusion
It is feasible, safe, and effective to treat osteolytic lesions of the lateral mass of the atlas using the lateral approach under fluoroscopic-guidance, which can relieve pain and stabilize bone.
Ethics Statement
This study was approved by the institutional review board of Shanghai Sixth People’s Hospital and all patient provided written informed consent.
Acknowledgments
This study was supported by the Natural Fund from Shanghai Science and Technology Commission (grant number 19411971800).
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Robles LA, Mundis GM, Cuevas-Solórzano A. Atlanto-Occipital rotatory dislocation: a Case Report and Systematic Review. World Neurosurg. 2018;110:106–114. doi:10.1016/j.wneu.2017.11.005
2. Abdelgawaad AS, Ezzati A, Govindasamy R, Krajnovic B, Elnady B, Said GZ. Kyphoplasty for osteoporotic vertebral fractures with posterior wall injury. Spine J. 2018;18:1143–1148. doi:10.1016/j.spinee.2017.11.001
3. Ahmadi SA, Slotty PJ, Munoz-Bendix C, Steiger H-J, Cornelius JF. Early surgical occipitocervical stabilization for plasma cell neoplasms at the craniocervical junction: systematic review and proposal of a treatment algorithm. Spine J. 2016;16:91–104. doi:10.1016/j.spinee.2015.09.032
4. Lvov I, Grin A, Talypov A, et al. Potential intraoperative factors of screw-related complications following posterior transarticular C1–C2 fixation: a systematic review and meta-analysis. Eur Spine J. 2019;28:400–420. doi:10.1007/s00586-018-5830-7
5. Kavakebi P, Girod PP, Hartmann S, Tschugg A, Thomé C. Transoral vertebroplasty of the lateral mass of C1 using image guidance. Acta Neurochir. 2017;159:1159–1162. doi:10.1007/s00701-017-3158-4
6. Clarençon F, Shotar E, Cormier E, et al. Transoral vertebroplasty for the C1 lateral mass. J Neurointerv Surg. 2020;12:879–885. doi:10.1136/neurintsurg-2020-015853
7. Huegli RW, Schaeren S, Jacob AL, Martin JB, Wetzel SG. Percutaneous cervical vertebroplasty in a multifunctional image-guided therapy suite: hybrid lateral approach to C1 and C4 under CT and fluoroscopic guidance. Cardiovasc Intervent Radiol. 2005;28:649–652. doi:10.1007/s00270-004-0159-5
8. Clarençon F, Cormier E, Pascal-Moussellard H, et al. Transoral approach for percutaneous vertebroplasty in the treatment of osteolytic tumor lesions of the lateral mass of the atlas: feasibility and initial experience in 2 patients. Spine. 2013;38(3):E193–E197. doi:10.1097/BRS.0b013e31827d41c7
9. Cianfoni A, Distefano D, Chin SH, Varma AK, Rumboldt Z, Bonaldi G. Percutaneous cement augmentation of a lytic lesion of C1 via posterolateral approach under CT guidance. Spine J. 2012;12:500–506. doi:10.1016/j.spinee.2012.05.012
10. Wetzel SG, Martin J-B, Somon T, Wilhelm K, Rufenacht DA. Painful osteolytic metastasis of the atlas: treatment with percutaneous vertebroplasty. Spine. 2002;27(22):E493–E495. doi:10.1097/00007632-200211150-00022
11. Yang JS, Chu L, Xiao FT, et al. Anterior retropharyngeal approach to C1 for percutaneous vertebroplasty under C-arm fluoroscopy. Spine J. 2015;15:539–545. doi:10.1016/j.spinee.2014.12.014
12. Guo WH, Meng MB, You X, et al. CT-guided percutaneous vertebroplasty of the upper cervical spine via a translateral approach. Pain Physician. 2012;15:E733–741.
13. Anselmetti GC, Manca A, Chiara G, Regge D. Painful osteolytic metastasis involving the anterior and posterior arches of C1: percutaneous vertebroplasty with local anesthesia. J Vasc Interv Radiol. 2009;20:1645–1647. doi:10.1016/j.jvir.2009.08.008
14. Bundy JJ, Griauzde J, Srinivasa RN, Chaudhary N, Chick JFB, Gemmete JJ. Transoral radiofrequency ablation and cementoplasty for lateral mass of the C1 vertebral body. J Vasc Interv Radiol. 2018;29:1246–1247. doi:10.1016/j.jvir.2018.05.001
15. Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of interventional radiology clinical practice guidelines. J Vasc Interv Radiol. 2003;14:S199–202. doi:10.1097/01.RVI.0000094584.83406.3e
16. Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14:409–415.
17. Bilsky MH, Shannon FJ, Sheppard S, Prabhu V, Boland PJ. Diagnosis and management of a metastatic tumor in the atlantoaxial spine. Spine. 2002;27:1062–1069. doi:10.1097/00007632-200205150-00011
18. Masala S, Anselmetti GC, Muto M, Mammucari M, Volpi T, Simonetti G. Percutaneous vertebroplasty relieves pain in metastatic cervical fractures. Clin Orthop Relat Res. 2011;469:715–722. doi:10.1007/s11999-010-1550-y
19. Ballivet de Regloix S, Maurin O. Retropharyngeal course of the internal carotid artery. J R Army Med Corps. 2017;163:426. doi:10.1136/jramc-2017-000852
20. Jan-Helge K, Marie Therese K, Evangelos K, Stefanie MB, Ulrich H, Christian S. Minimally invasive resection and vertebroplasty for an osteolytic C-1 metastasis of malignant meningioma: case report. J Neurosurg Spine. 2015;23:602–606.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.