Back to Journals » Clinical Ophthalmology » Volume 20
Perceptual Learning Therapy Using RevitalVision in Patching-Failed Amblyopia: Visual Outcomes, Predictors of Response, and Durability
Authors Samant M, Mhatre R ![]() , Kaushal R, Haldipurkar S, Sengupta S
, Kaushal R, Haldipurkar S, Sengupta S
Received 19 January 2026
Accepted for publication 12 May 2026
Published 3 June 2026 Volume 2026:20 597384
DOI https://doi.org/10.2147/OPTH.S597384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Monica Samant,1 Rupam Mhatre,1 Rakesh Kaushal,2 Suhas Haldipurkar,1 Sabyasachi Sengupta1,3
1Laxmi Eye Hospital & Institute, Panvel, India; 2Laxmi College of Optometry, Panvel, India; 3Future Vision Eye Care, Mumbai, India
Correspondence: Sabyasachi Sengupta, Laxmi Eye Hospital & Institute, Mulla Hamid Road, Old Panvel, Panvel, Navi Mumbai, Maharashtra, 410206, India, Tel +91-9943909766, Email [email protected]
Purpose: To evaluate the effectiveness, predictors, and durability of perceptual learning therapy using ReVitalVision in older children with amblyopia who had failed prolonged patching therapy.
Methods: This prospective interventional study included children (≤ 18 years) and adults with amblyopia, with pediatric participants having failed ≥ 2 years of patching due to poor compliance or non-response. All participants completed a mandatory minimum of 40 ReVitalVision sessions; up to 80 sessions were optional. Vision (logMAR) and stereoacuity were assessed at baseline, after 40 and 80 sessions, and at 3, 6, and 12 months. Multivariable regression was performed to identify predictors of outcome.
Results: Seventy-three participants (mean age 14.6 ± 5.5 years; 67% male) were included: anisometropic (n=34), strabismic (n=20), isometropic (n=6), deprivational (n=4), and other causes (n=9). After 40 sessions, significant visual improvement was observed across subtypes, greatest in anisometropic amblyopia (0.50 to 0.32 logMAR), with 40% achieving 20/40 or better. Strabismic amblyopia showed slower recovery (0.54 to 0.38 logMAR) and greater variability, while deprivational amblyopia showed limited response. Stereoacuity improved significantly in anisometropic (175 to 67 arcsec) and strabismic amblyopia (214 to 48 arcsec). Baseline BCVA was the strongest predictor of outcome (β = 0.061 per line worsening; p < 0.001), independent of amblyopia subtype and age. Time taken to complete 40 sessions did not influence outcomes. Eighty sessions produced marginally better vision but significantly greater stereoacuity improvement (p = 0.002). A subtle trend toward regression was observed at 6– 12 months.
Conclusion: ReVitalVision therapy produces clinically meaningful visual and binocular improvements in patching-failed amblyopia. Baseline visual acuity strongly predicts response and durability, and extended therapy may benefit patients with denser amblyopia, supporting individualized treatment duration.
Keywords: amblyopia, perceptual learning, ReVitalVision, patching-resistant amblyopia, visual acuity, stereoacuity
Introduction
Amblyopia remains one of the most common cause of monocular visual impairment in children and young adults worldwide.1 Conventional treatments such as patching or pharmacologic penalization are most effective in early childhood, when visual neuroplasticity is at its peak. However, treatment outcomes are often limited by commonly reported factors such as poor compliance, psychosocial challenges, and diminishing efficacy beyond the age of 8–9 years.2,3 In particular, children who have undergone prolonged or repeated courses of patching therapy beyond the expected period of response, with minimal improvement represent a highly resistant group for whom few effective alternatives exist.
Several therapeutic modalities have been developed to address these limitations. Binocular therapies and dichoptic training aim to reduce suppression and improve stereopsis by engaging both eyes simultaneously, with promising results in older children and integration into modern platforms such as virtual reality.2,4,5 Perceptual learning therapies, such as ReVitalVision, work differently: they employ repetitive visual tasks to directly enhance cortical processing and contrast sensitivity, offering the potential to improve vision even after the conventional therapeutic window has closed.6–9
ReVitalVision therapy is an FDA-cleared computer-based program that employs Gabor patch–based visual stimuli to stimulate cortical processing, enhance contrast sensitivity, and improve visual acuity.3,10,11 Unlike patching, which forces reliance on the amblyopic eye by occluding the fellow eye, ReVital is designed to promote binocular interaction and retrain neural circuits, thereby addressing the central processing deficits characteristic of amblyopia.4,12
Clinical studies have demonstrated that ReVital therapy can produce meaningful improvements of 2–2.5 lines in visual acuity in adults (generally ≥18 years) and older children, with long-term retention of visual gains.5,13,14 Most of the published evidence, however, has focused on adults with amblyopia, whereas relatively few investigations have evaluated its efficacy in older children who have already failed prolonged patching therapy.3,15 This population is particularly important because they often face both limited residual neuroplasticity and reduced motivation after years of unsuccessful conventional therapy.16
The present study was therefore designed to assess the effectiveness of ReVital therapy in a cohort of older children with deep amblyopia who had previously failed at least two years of patching. By examining outcomes across different amblyopia subtypes, and by documenting both visual acuity and stereopsis over 12 months of follow-up, this study provides insight into the role of perceptual learning therapy in an especially resistant group of patients.
Methods
This prospective interventional study was approved by the Laxmi Eye Institute Institutional Ethics Committee (LEI/007/2025). Written informed consent was obtained from all adult participants. For participants ≤18 years of age, written informed consent was obtained from parents or legal guardians, and assent was obtained from the participants where age-appropriate. The study adhered to the tenets of the Declaration of Helsinki.
Participants
Eligible participants included children (≤18 years) and adults with amblyopia, defined as a ≥2-line interocular difference in best-corrected visual acuity (BCVA) despite appropriate refractive correction (or lower than 6/12 in both eyes) and removal of any coexisting ocular pathology (eg, strabismus surgery, correction of media opacity, or optimal spectacle prescription). For children, a further requirement was prior attempted patching therapy for a minimum of two years, with treatment failure defined as either poor compliance or lack of visual improvement. All participants were required to be willing to engage with ReVitalVision therapy for a minimum of 40 sessions.
Exclusion criteria included ocular pathology likely to confound visual acuity outcomes (such as corneal opacity, progressive retinal or optic nerve disease), neurological disorders affecting vision, prior refractive surgery, or inability to complete the training program as prescribed. Patients who failed to complete at least 40 sessions of therapy were also excluded from analysis.
Intervention
All participants were enrolled in the ReVitalVision perceptual learning therapy program, delivered on laptops with specifications recommended by the manufacturer. Each participant was instructed to complete a minimum of 40 sessions, performed as 5 sessions per week (approximately one session per weekday), for an expected duration of 8 weeks (55–60 days). An additional 40 sessions were offered if participants wished to continue beyond the initial treatment phase.
Each session could be monitored remotely by the treating physician to ensure adherence. Effective training requires sustained attention at the individual’s contrast threshold, as cortical activation is maximised when Gabor targets are presented at very low contrast with higher-contrast flankers outside the receptive field; accordingly, patients were encouraged to maintain focus at this threshold, and session monitoring allowed identification of instances where training fell outside the effective contrast range. On completion of 40 sessions, participants were recalled to the clinic for evaluation within 7 days. The actual time taken to complete the 40 sessions was documented for all participants.
Assessments
At baseline, all participants underwent comprehensive ophthalmic evaluation, including BCVA and stereopsis testing. BCVA was measured using standard logMAR visual acuity charts (ETDRS charts at 4 m), and stereopsis was assessed using the Randot Preschool Stereoacuity Test (Stereo Optical Co., Chicago, IL, USA) or equivalent validated test. Follow-up assessments were performed after 40 sessions, after 80 sessions (if undertaken), and subsequently at 3 months, 6 months, and 12 months from initiation of therapy.
Outcomes
The primary outcome measure was improvement in BCVA and stereopsis following completion of 40 sessions of ReVital therapy. Secondary outcomes included changes in BCVA and stereopsis at later follow-up intervals (3, 6, and 12 months).
Statistical Analysis
Descriptive statistics were calculated for visual acuity (VA) and stereoacuity at baseline, after 40 sessions, and at 12 months. Within-group changes in VA and stereoacuity over time were assessed using paired t-tests (for normally distributed data) or Wilcoxon signed-rank tests (for non-normally distributed data). Similarly, between-group comparisons of VA and stereoacuity (eg, anisometropic vs. strabismic amblyopia) were performed using independent samples t-tests or Mann–Whitney U-tests, as appropriate. Comparisons of proportions of children achieving specific VA thresholds (≤0.4 and ≤0.3 logMAR) between groups were conducted using chi-square tests or Fisher’s exact tests, depending on cell counts.
Multivariable linear regression was used to assess the association between change in VA and baseline VA, diagnosis group, and age. These variables were selected a priori based on clinical relevance rather than univariate screening. Regression coefficients, 95% confidence intervals, and p-values were reported. All data were captured in Microsoft Excel and statistical analyses were performed using R (version 4.3.3) with the Julius-AI interface. Statistical significance was set at p < 0.05.
Results
There were 73 participants; the mean age was 14±5.5 years, and 49 were boys (67%). The cohort was predominantly pediatric, with 60/73 participants (82%) aged ≤18 years (median 11.5 years, range 5–18 years) and 13/73 (18%) aged >18 years (median 23 years, range 19–33 years). Of these, 34 had anisometropic amblyopia (46%), 20 (27%) had strabismic, 6 (8%) had isometropic, 4 (5%) had deprivational amblyopia and 9 (12%) had amblyopia due to other causes, mainly comprising of retinal diseases such as treated retinal detachment, healed toxoplasmosis and prior dense laser for retinopathy of prematurity. Of the total cohort, 41 (56%) had 80 sessions of ReVital therapy.
Anisometropic Amblyopia
Children with anisometropic amblyopia (n=34) demonstrated the most consistent improvements in VA following perceptual learning therapy with ReVital (Table 1). The mean baseline VA was 20/60 Snellen’s equivalent, which improved steadily to 20/40 after 40 sessions and remained stable through 12 months of follow-up. By the end of 40 sessions, 68% of eyes had reached 20/50 or better, and more than a third (40%) achieved 20/40 or better (Figure 1). Stereoacuity also improved substantially (Table 2), from a baseline of 175 arcsec to 67 arcsec at 12 months (p<0.001).
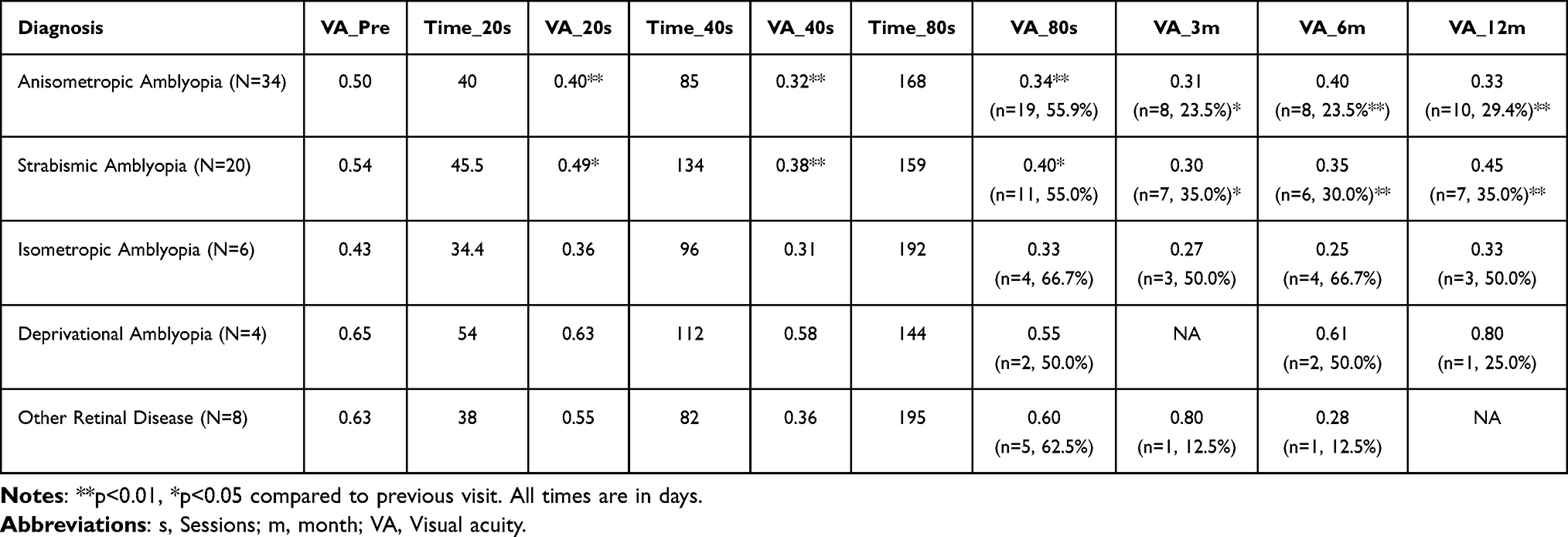 |
Table 1 Comparison of Best-Corrected Visual Acuity at Various Time Points Across Different Types of Amblyopia |
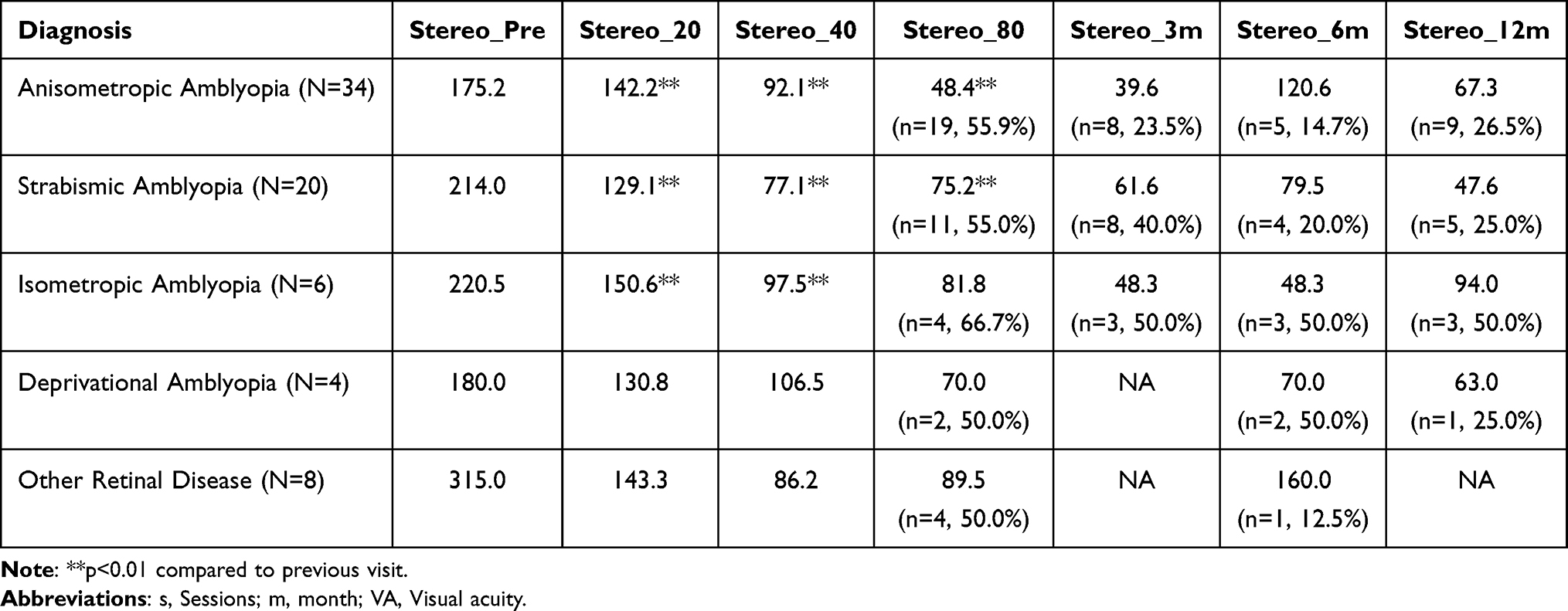 |
Table 2 Comparison of Stereo-Acuity at Various Time Points Across Different Types of Amblyopia |
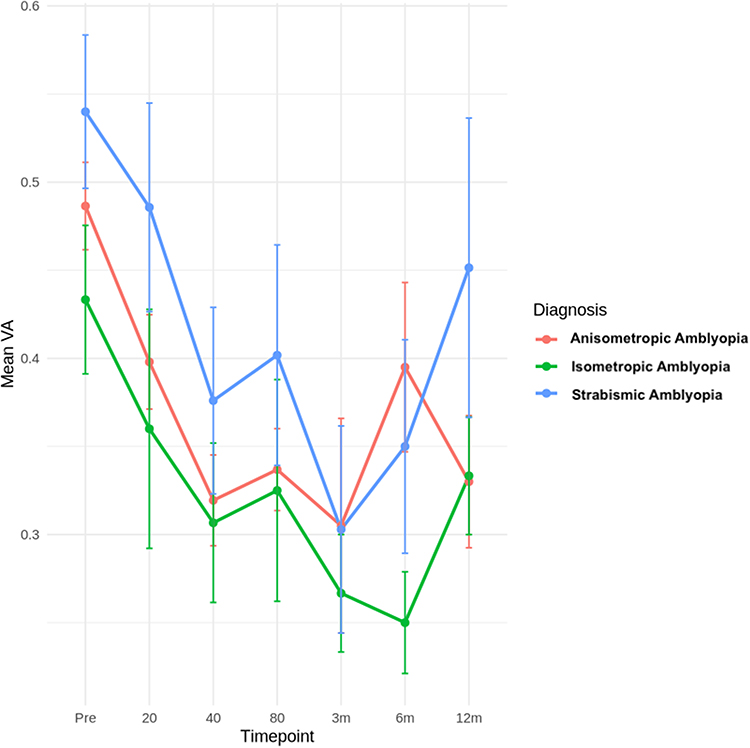 |
Figure 1 Visual acuity outcomes over time by amblyopia subtype. |
Strabismic Amblyopia
In the strabismic group (n=20), baseline VA was 20/70, improving to 20/50 at 40 sessions (Table 1). The improvement was maintained at 12 months, with 60% of children retaining VA better than 20/50, whereas 35% retained vision of better than 20/40. Stereoacuity gains were also evident, improving from 214 arcsec at baseline to 48 arcsec at 12 months (Table 2). Compared with anisometropic amblyopia, the strabismic subgroup showed a slower trajectory of recovery and more variability in long-term outcomes (Figure 1).
Isometropic Amblyopia
Children with isometropic amblyopia (n=6) had a baseline VA of 20/50, which improved to 20/40 by 40 sessions and further to 20/32 at 6 months and was maintained at 12 months (Table 1). Stereoacuity improved from 220 arcsec at baseline to 82 arcsec at 80 sessions, dipped modestly at 6 months, and partially recovered to 94 arcsec at 12 months (Table 2). While limited by the small sample size, these results suggest stable benefit overall, but with the same mid-term regression seen in other groups.
Deprivational Amblyopia
Children with deprivational amblyopia showed more limited improvement overall. Although some patients achieved modest VA and stereoacuity gains, the magnitude and consistency of response were less robust compared with the other subtypes (Table 1).
Predictors of Response
Multivariable regression (Table 3) analysis revealed that poorer baseline VA was the strongest predictor of greater improvement at 40 sessions (β = 0.06, p < 0.001). The type of amblyopia was not an independent predictor of outcome after adjusting for baseline VA. In a subgroup analysis comparing patients completing 40 versus 80 sessions, 80 sessions were associated with slightly better visual acuity (approximately half a line), although this difference was not statistically significant; however, stereoacuity improvement was significantly greater with 80 sessions (median [IQR]: 63 [40–100] at 40 sessions vs 45 [40–63] at 80 sessions; p = 0.002). While trends toward greater stereoacuity improvement with extended therapy were observed in anisometropic and strabismic amblyopia (Table 2), subgroup-level interpretations should be made cautiously, given the small sample sizes in other categories. Furthermore, analysis of treatment adherence showed that the time interval taken to complete 40 sessions did not significantly affect VA outcomes, as both above-median and below-median groups achieved comparable results (Figure 2).
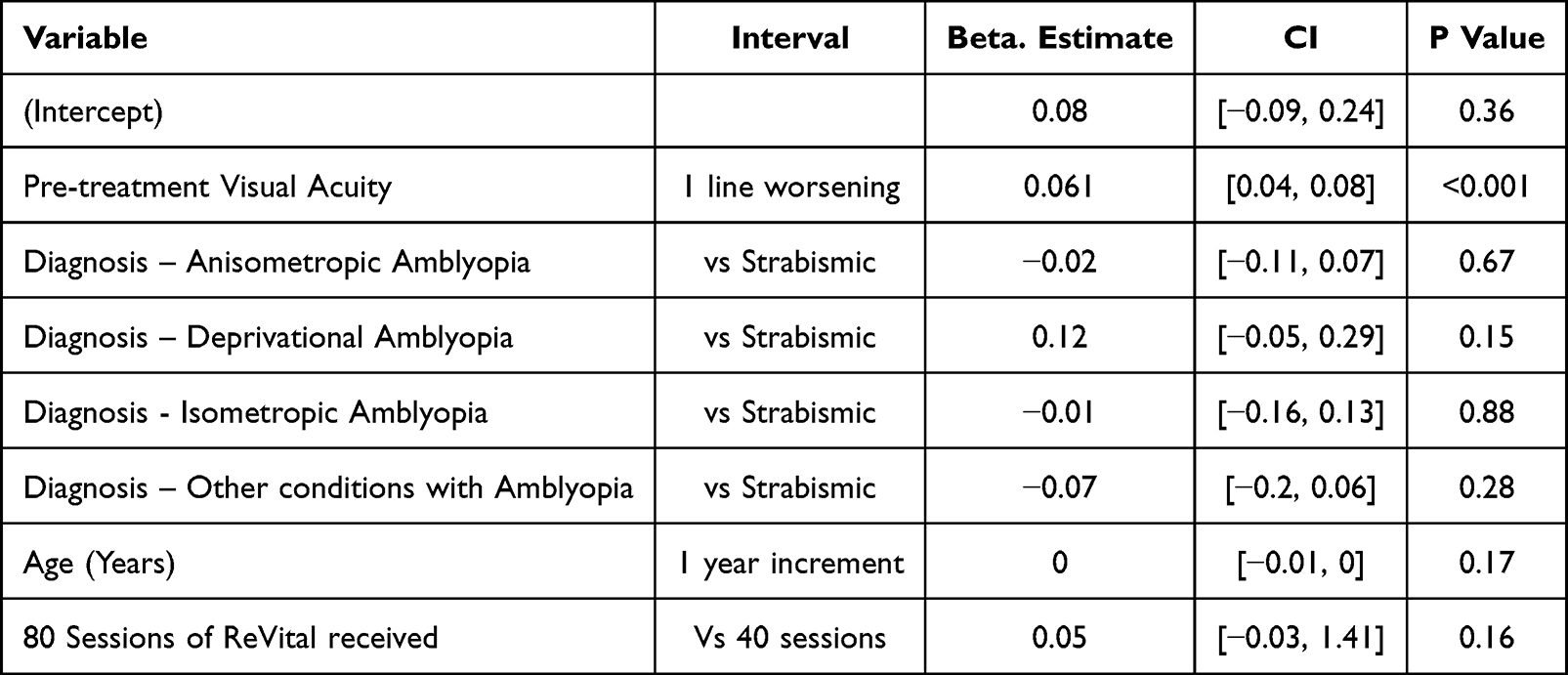 |
Table 3 Factors Predictive of Visual Improvement After ReVital Therapy |
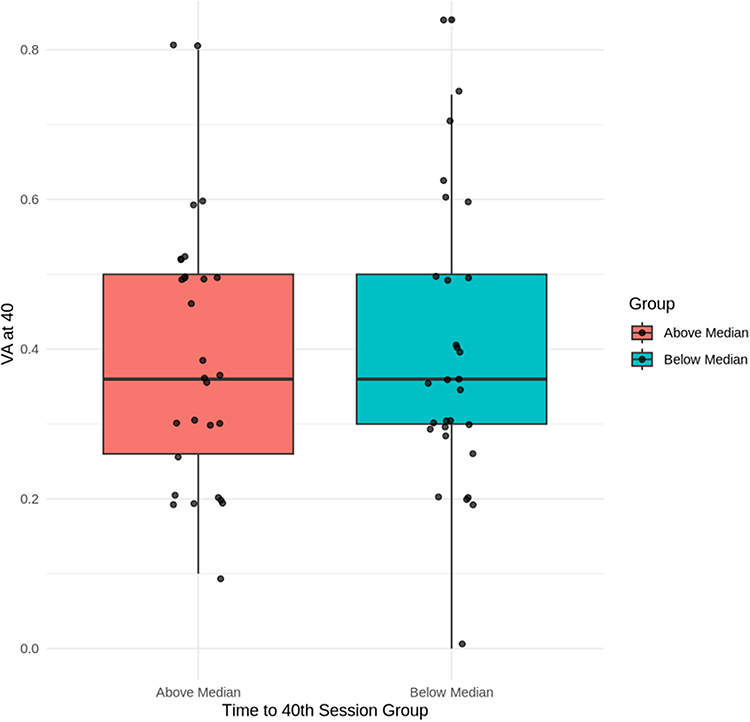 |
Figure 2 Visual acuity at 40 sessions by time to completion. |
Longitudinal Trends
Across the three main amblyopia subtypes (anisometropic, strabismic, and isometropic), a consistent trend of slight regression was observed around the 6-month mark, affecting both VA and stereoacuity (Figure 1).
Discussion
This study evaluated the effect of perceptual learning therapy with ReVital in a cohort of older children with amblyopia who had failed conventional patching, either due to poor compliance or genuine non-response despite two years of therapy. Despite this being a particularly resistant population, meaningful improvements were observed across several types of amblyopia. Both anisometropic and isometropic amblyopia responded well, with at least two lines of visual acuity gain after 40 sessions. Overall, we found that anisometropic amblyopia was particularly responsive to ReVital training, with durable visual gains. Strabismic amblyopia also improved, though the magnitude of gain was less pronounced. Encouragingly, nearly half of anisometropic eyes and more than one-third of strabismic eyes achieved 20/40 or better following therapy, despite poor baseline vision. Deprivational amblyopia showed the least benefit, consistent with its recognized refractoriness to treatment. Though limited by our relatively small sample size, we found that baseline vision was the strongest predictor of visual improvement with ReVital therapy, with poorer initial vision independently associated with poorer visual acuity after 40 sessions, regardless of amblyopia subtype or age.
Although the manufacturer prescribes 40 sessions over approximately 60–70 days, our cohort took considerably longer, with a median of 85 days in anisometropic and over 120 days in strabismic amblyopia. Importantly, this delay did not appear to affect outcomes, as children completing therapy within or beyond the prescribed timeframe achieved comparable visual gains. Finally, a subtle but consistent trend of “waning effect” was observed at 6–12 months across all major subgroups, reflected in marginal regressions in both visual acuity and stereoacuity. While these regressions were small and occurred in limited subsets, they highlight the potential need for sustained engagement or booster therapy to consolidate long-term outcomes in eyes with failed prolonged patching.
The outcomes observed in anisometropic amblyopia in our study are consistent with previously published data on perceptual learning–based amblyopia therapy, while extending these findings to a more refractory population. Magdalene et al,11 in a predominantly anisometropic cohort from an Indian setting with similar age and baseline visual acuity, reported a comparable magnitude of visual improvement at 12 months. However, their participants were recruited after achieving maximal benefit from optical correction and patching and were not explicitly described as patching failures, whereas our cohort consisted exclusively of children who had failed at least two years of patching. Additionally, their protocol involved 30–40 sessions, compared with a minimum of 40 sessions (and up to 80) in our study. In contrast to the sustained gains reported in this cohort of up to 5 years, we observed a subtle trend toward regression at 6–12 months in a subset of patients, possibly reflecting greater disease severity and smaller numbers at later follow-up. Importantly, despite the markedly refractory nature of amblyopia in our cohort, a substantial proportion of children achieved clinically meaningful visual improvement, underscoring the ability of ReVital therapy to induce benefit even in dense amblyopia.
Similarly, Yalcin et al10 reported larger visual gains in a hypermetropic anisometropic amblyopia; however, their cohort had better baseline vision, included treatment-naïve patients, and had shorter follow-up. Zhou et al also demonstrated that treatment-naïve amblyopic patients, without a history of patching, show significantly greater visual improvement with perceptual learning therapy, representing the opposite end of the disease spectrum compared with the highly refractory, patching-failed cohort studied in our setting17 Taken together, these findings suggest that while perceptual learning therapy yields robust benefits in anisometropic amblyopia, baseline visual acuity and prior treatment failure substantially influence the magnitude and durability of response, and that introducing such therapy earlier in the disease course may result in even greater and more sustained visual gains, particularly in anisometropic and isometropic amblyopia.
Most published ReVitalVision and perceptual learning studies have predominantly included patients with anisometropic or refractive amblyopia, with strabismic amblyopia typically constituting a small minority (often 4–5% of cohorts), yet generally reported to show comparable efficacy through enhancement of neural plasticity. In contrast, over one-quarter of our cohort (27%) comprised strabismic amblyopia, representing one of the largest such subgroups reported to date. In our study, although strabismic amblyopia demonstrated meaningful visual and stereoacuity improvement, the trajectory of recovery was slower and long-term outcomes were more variable compared with anisometropic amblyopia, with greater regression over follow-up and final visual acuity remaining more than one line lower on average. Whether this reflects the inherently poorer baseline visual acuity in this subgroup, which emerged as the strongest predictor of outcome in our multivariable analysis, irrespective of amblyopia etiology, or a differential biological response of strabismic amblyopia to perceptual learning remains uncertain. It is plausible that persistent binocular suppression and abnormal binocular interaction in strabismic amblyopia may limit the durability of cortical reorganization compared with purely refractive amblyopia, a hypothesis that warrants further targeted investigation.
The optimal duration of perceptual learning therapy remains an open question. In our cohort, patients completing 80 sessions achieved only marginally greater visual acuity gains compared with those completing 40 sessions, and this difference was not significant after adjusting for baseline vision. However, stereoacuity improvement was significantly greater in the extended-treatment group, suggesting that prolonged exposure may preferentially benefit binocular visual function. This observation aligns with emerging evidence from Zhou et al,17 who demonstrated continued functional gains with extended perceptual learning therapy beyond initial treatment cycles. Taken together with our finding of a subtle “waning effect” at 6–12 months, these results suggest that patients with denser amblyopia, characterized by poorer baseline vision, worse stereoacuity, and prolonged failure of patching, may require longer or staged ReVital therapy to consolidate and sustain gains. In addition to baseline visual acuity, variability in engagement with contrast-threshold–based training may also influence individual response, an aspect that warrants focused evaluation in future studies. Future studies incorporating larger cohorts and comprehensive covariate analysis may allow prediction of the optimal duration of therapy for individual patients, enabling a personalized approach that balances efficacy, durability, and cost.
This study has several limitations. The sample size was modest, particularly for isometropic and deprivational amblyopia, and the study lacked a randomized control group, limiting causal inference. Attrition at later follow-up points may have influenced the assessment of long-term durability and regression trends. However, key strengths include the real-world clinical design, inclusion of a uniquely refractory cohort with prolonged failed patching, stratified analysis by amblyopia etiology, and longitudinal assessment of both visual acuity and stereoacuity. Notably, this study represents one of the largest reported series of strabismic amblyopia treated with perceptual learning therapy.
In conclusion, ReVitalVision perceptual learning therapy resulted in clinically meaningful improvements in visual acuity and stereoacuity in older children with amblyopia who had failed prolonged patching therapy. Despite the highly refractory nature of this cohort, anisometropic and isometropic amblyopia demonstrated robust responses, while strabismic amblyopia showed slower and more variable recovery. Baseline visual acuity emerged as the strongest predictor of outcome, underscoring the importance of disease severity in determining both the magnitude and durability of response. Although extending therapy beyond 40 sessions conferred limited additional benefit in visual acuity, improvements in stereoacuity suggest a role for longer or staged treatment in selected patients. These findings support the use of perceptual learning therapy as a valuable adjunct in resistant amblyopia and highlight the need for future studies to individualize treatment duration based on baseline characteristics to optimize long-term outcomes.
Disclosure
Dr Sengupta reports receiving speaker honoraria from Novartis India, Roche India, Lupin, and Appasamy Associates. The remaining authors declare no conflicts of interest for this work.
References
1. Fu Z, Hong H, Su Z, Lou B, Pan CW, Liu H. Global prevalence of amblyopia and disease burden projections through 2040: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1164–9. doi:10.1136/bjophthalmol-2019-314759
2. Kelly KR, Jost RM, Dao L, Beauchamp CL, Leffler JN, Birch EE. Binocular iPad game vs patching for treatment of amblyopia in children. JAMA Ophthalmol. 2016;134(12):1402. doi:10.1001/jamaophthalmol.2016.4224
3. Zhou Y, He Y, Feng L, et al. Perceptual learning based on the lateral masking paradigm in anisometropic amblyopia with or without a patching history. Trans Vision Sci Technol. 2024;13(1):16. doi:10.1167/tvst.13.1.16
4. Chen C, Zhu Q, Duan YB, Yao J. Comparison between binocular therapy and patching for treatment of amblyopia: a meta-analysis of randomised controlled trials. BMJ Open Ophthalmol. 2021;6(1):e000625. doi:10.1136/bmjophth-2020-000625
5. Holmes JM, Manny RE, Lazar EL, et al. A randomized trial of binocular dig rush game treatment for amblyopia in children aged 7 to 12 years. Ophthalmology. 2019;126(3):456–466. doi:10.1016/j.ophtha.2018.10.032
6. Barollo M, Contemori G, Battaglini L, Pavan A, Casco C. Perceptual learning improves contrast sensitivity, visual acuity, and foveal crowding in amblyopia. Restorat Neurol Neurosci. 2017;35(5):483–496. doi:10.3233/RNN-170731
7. Lan FF, Zhao W, Gan L. Evaluation of visual plasticity in patients with refractive amblyopia treated using a visual perceptual learning system. Technol Health Care. 2024;32(1):327–333. doi:10.3233/THC-230183
8. Maniglia M, Pavan A, Sato G, et al. Perceptual learning leads to long lasting visual improvement in patients with central vision loss. Restorat Neurol Neurosci. 2016;34(5):697–720. doi:10.3233/RNN-150575
9. Ming X, Huang G, Chen X, Liao M, Liu L. A systematic review and meta-analysis of perceptual learning and video game training for adults with monocular amblyopia. Ophthalmol Ther. 2025;14(5):857–881. doi:10.1007/s40123-025-01128-9
10. Yalcin E, Balci O. Efficacy of perceptual vision therapy in enhancing visual acuity and contrast sensitivity function in adult hypermetropic anisometropic amblyopia. Clin Ophthalmol. 2014;8:49–53. doi:10.2147/OPTH.S48300
11. Magdalene D, Dutta P, Blah P, et al. Long-term efficacy of perceptual learning therapy in amblyopia: a 5-year follow-up study. Latin Am J Ophthalmol. 2025;8:8. doi:10.25259/LAJO_2_2025
12. Roda M, Pellegrini M, d GN, Vagge A, Fresina M, Schiavi C. Binocular treatment for amblyopia: a meta-analysis of randomized clinical trials. PLoS One. 2021;16(10):e0257999. doi:10.1371/journal.pone.0257999
13. Manh V, Holmes JM, Lazar EL, et al. A randomized trial of a binocular ipad game versus part-time patching in children aged 13 to 16 years with amblyopia. Am J Ophthalmol. 2018;186:104–115. doi:10.1016/j.ajo.2017.11.017
14. Pineles SL, Aakalu VK, Hutchinson AK, et al. Binocular treatment of amblyopia. Ophthalmology. 2020;127(2):261–272. doi:10.1016/j.ophtha.2019.08.024
15. Irfan S, Aadil N, Saqib M. Can amblyopia of any severity be treated successfully irrespective of a patient’s age? 2023.
16. Rajavi Z, Soltani A, Vakili A, et al. Virtual reality game playing in amblyopia therapy: a randomized clinical trial. J Pediatr Ophthalmol Strabismus. 2021;58(3):154–160. doi:10.3928/01913913-20210108-02
17. Zhou Y, Ye Q, Qiu X, et al. Extending treatment duration in perceptual learning for amblyopia. Ophthalmol Sci. 2025;6:101005. doi:10.1016/j.xops.2025.101005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.