Back to Journals » Advances in Medical Education and Practice » Volume 13
Perceptions of the CanMEDS Competencies of Faculty and Students in Different Curriculum Systems of a Medical School in China
Authors Li P, Jiang F, Yin L, Chen YQ, Shao L, Li Y, Gao YJ, Lu MH
Received 19 March 2022
Accepted for publication 6 September 2022
Published 15 September 2022 Volume 2022:13 Pages 1061—1070
DOI https://doi.org/10.2147/AMEP.S367129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Pingping Li,1 Fan Jiang,2 Lei Yin,3 Yi Qi Chen,4 Li Shao,5 Yi Li,6 Yi Jin Gao,7 Mei Hua Lu1
1Department of Medical Teaching, Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Developmental and Behavior Pediatrics, Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Department of Nephrology, Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 4School of Pediatrics, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 5Office of Educational Administration, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 6School of Clinical Medicine, Renji Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 7Department of Hematology/Oncology, Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Correspondence: Mei Hua Lu; Yi Jin Gao, Shanghai Children’s Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China, Tel +86 021 38626190, Email [email protected]; [email protected]
Introduction: The Ottawa-Shanghai Joint School of Medicine (OSJSM) has adopted the uOttawa’s undergraduate medical education (UGME) program vertically integrated (VI) curriculum.However, limited information is available regarding whether the VI and non-VI curricula foster different perspectives on necessary competencies.
Methods: This study included 167 undergraduate medical students and 142 faculty members from different curricula at the Shanghai Jiao Tong University School of Medicine. Participants completed a questionnaire, rating the importance of competencies relating to the seven CanMEDS roles.
Results: The cognitive level regarding the competencies required to be a successful clinician was significantly higher among participants from VI versus non-VI curricula. All participants gave the highest ratings to the Medical Expert and Professional roles, and rated the Health Advocate role as least important. Competency ratings did not significantly differ between students from VI versus non-VI curricula. Ratings between VI and non-VI faculty showed only one significant difference, namely the competence of“Constantly update clinical knowledge and professional skills” was ranked significantly higher by faculty of non-VI curricula. In the top rated 10 competencies, the Communicator role was considered more important by participants from VI versus non-VI curricula.
Conclusion: The cognitive level regarding the competencies was related to the curriculum system. The Communicator role seemed to be paid more attention in VI curricula, however, other competencies was not demonstrated to be related to the curriculum system.
Keywords: competency, vertically integrated curriculum, medical education
Background
In China, the majority of medical schools follow a discipline-based curricular model, in which theory, clerkship, and internship are completed in three isolated phases, and competencies are largely neglected.1 As medical education has developed, most Chinese medical schools have attempted to revise the undergraduate medical curricula, with the majority of schools attempting to apply an organ system-based curriculum model. In terms of integration methods, most colleges focus on horizontal integration, and the scope of integration is largely basic medicine.2 Very few schools have adopted vertically integrated (VI) curricula. A fully vertically integrated undergraduate medical curriculum includes four elements:3 provision of early clinical experience, integration of biomedical sciences and clinical cases, progressive longitudinal increase of clinical responsibility, and extended clerkships in the final year of medical school.4,5
In October 2014, the Ottawa-Shanghai Joint School of Medicine (OSJSM) was launched by the Shanghai Jiao Tong University School of Medicine (SJTUSM) and the University of Ottawa (uOttawa).6 OSJSM has adopted uOttawa’s fully vertically integrated undergraduate medical education (UGME) program curriculum, which is based on the seven CanMEDS roles:7 Medical Expert, Professional, Communicator, Collaborator, Leader, Health Advocate, and Scholar. This program has been implemented for 5 years, but no study has examined the perspective of students and faculty regarding competencies.
Different undergraduate educational strategies may affect the degree of adaptation during medical students’ transition from medical school to clinical practice and postgraduate training.8 Previous studies show that compared with graduates who have followed non-VI curricula, graduates of VI curricula seem to feel better prepared for work and postgraduate training.9,10 However, limited information is available regarding how different curriculum systems may influence the perspectives of competence among undergraduate medical students and faculty.
The CanMEDS is used as an educational framework at the undergraduate level throughout medical schools in Canada, and has also been adapted for international use.11 It describes seven roles, each of which is represented by two to five key competencies that describe the related abilities, skills, and attitudes.12 Within this framework, medical students are expected to develop competencies related to the following CanMEDS roles: Medical Expert, Professional, Communicator, Collaborator, Leader, Health Advocate, and Scholar.13 Research regarding the competencies of clinicians in China is still in its infancy,14 and it mainly focuses on the postgraduate stage. China has not yet developed a model or evaluation system for medical students’ competence.15
The present study was performed at Shanghai Jiao Tong University School of Medicine (SJTUSM) in China. Participants were recruited from two different clinical medical schools of SJTUSM: the OSJSM and School of Pediatrics. As described above, the OSJSM uses a vertically integrated curriculum. On the other hand, the School of Pediatrics applies a discipline-based curricular model that is not vertically integrated. Undergraduate medical education spans five years, with the first and second years considered preclerkship, and the third, fourth and fifth years called clerkship.
In the present study, we aimed to investigate the perceptions of the competencies of faculty and students in different curriculum systems. The findings are intended to provide curricular planners with some insight regarding whether different curricula learning situations can affect the perspectives on competency of the students and faculties.
Methods
Participants
This study was conducted at Shanghai Jiao Tong University School of Medicine of 411 undergraduate medical students from years one to five, and 300 faculty members, were asked to complete an anonymous online questionnaire. Informed consent was obtained from all individual participants included in the study. The survey was available online for four weeks in December 2018. After two weeks, the students and faculty were sent a reminder via WeChat by staff members from OSJSM and the School of Pediatrics.
Questionnaire
The questionnaire comprised a list of the CanMEDS competency framework,16 including 7 dimensions of Medical Expert, Professional, Communicator, Collaborator, Leader, Health Advocate, and Scholar. The items of questionnaire were selected with 73 indicators from a previous study.17 A Delphi method was used to selecte the items, with 2 iterations in order to reach consensus.The questionnaire’s reliability was assessed using Cronbach’s alpha by SPSS 22.0. A pre-test survey was performed in participants (N = 3), 1 medical student and 2 faculty, who were asked to consider every item in the questionnaire. After finishing the questionnaire, participants were asked to consider every item in terms of (1) difficult to answer, (2) unclear, (3) use of difficult words, or (4) upsetting. Participants were also asked to provide comments or suggest alternative words or terms to researcher. Participants were also asked to provide comments or suggest alternative words or terms to researcher.
For each item, respondents were asked to rate the importance of competence using a 5-point Likert-type scale, where 1 = very unimportant and 5 = very important.18 Respondents were also asked to indicate their gender and class, and faculty were asked to indicate their teaching years.
Statistical Analysis
To optimize the response rate, we provided the same number of items for each of the seven roles.11 As the role of Health Advocate includes four items, we chose the top four items for each of the other roles. The questionnaire’s reliability was assessed using Cronbach’s alpha. To calculate the overall ratings of importance within each role, we averaged the ratings of the four items. Scores were analyzed using SPSS 22.0. Mean and standard deviation (SD) was calculated for each individual item. Statistical differences between groups were analyzed using the Chi-square test and Kruskal Wallis test, with P < 0.05 considered statistically significant.
Results
A total of 167 medical students and 142 faculty members completed the survey. Table 1 shows the characteristics of the participating medical students and faculty. The participating undergraduate medical students included 87 from VI curricula and 80 from non-VI curricula. Among participating faculty, 70 were from VI curricula and 72 from non-VI curricula. Between the two different curriculum groups, we found no differences in students’ gender (H = 0.147, P = 0.883) or grade (H = 0.054, P = 0.816), or in faculty’s teaching year (H = 0.361, P = 0.835) (Table 1). Based on the scoring of importance for the items on the questionnaire, Cronbach’s alpha was 0.992.
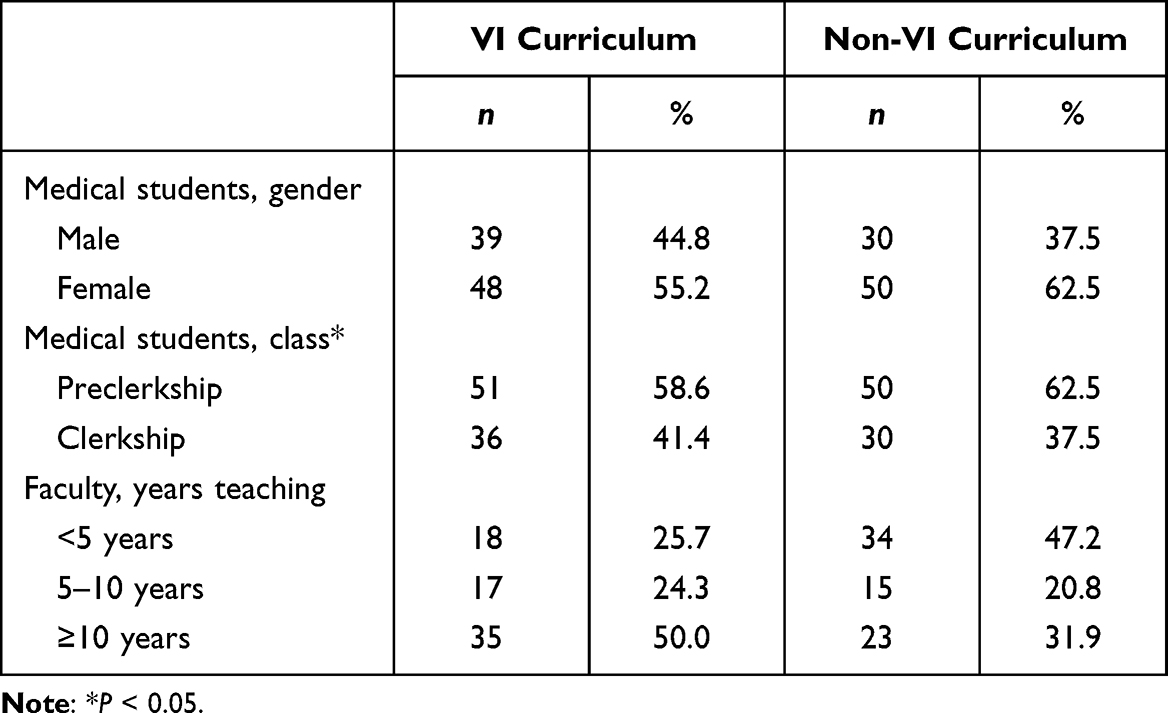 |
Table 1 Characteristics of the Participating Medical Students and Faculty |
Compared to students, faculty had a higher cognitive level regarding competencies. This cognitive level significantly differed between faculty from VI curricula versus non-VI curricula (χ2 = 4.060, P = 0.044), and was significantly higher in students of the VI curriculum versus the non-VI curriculum (χ2 = 25.424, P = 0.000) (Figure 1). We also found differences in overall means between the competences related to the CanMEDS roles. The role of Medical Expert was rated significantly higher than any other CanMEDS role, and the role of Health Advocate was rated lowest (one-sample t-test, P < 0.001) (Figure 2).
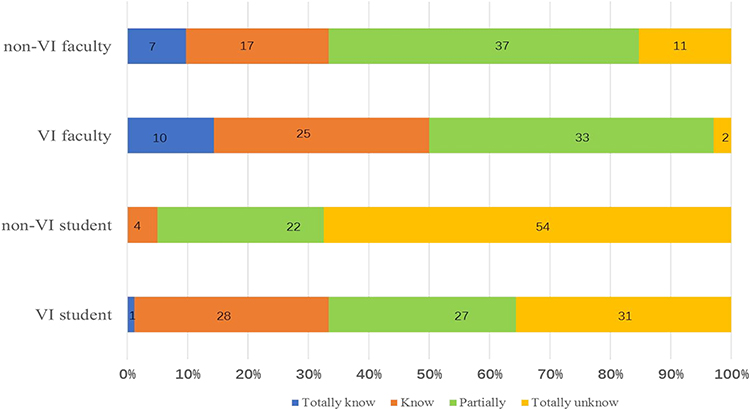 |
Figure 1 Differences among students and faculty from vertically integrated (VI) and non-VI curricula in terms of cognitive level, eg, knowledge about the competencies required to become a good doctor. |
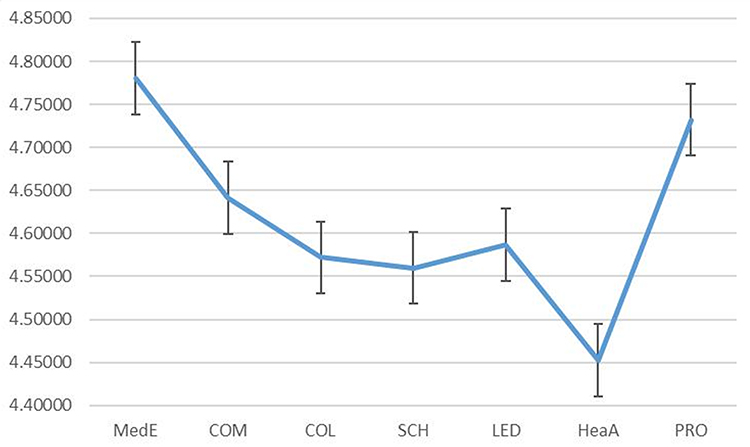 |
Figure 2 Mean ratings of competencies related to the CanMEDS roles by all participants. Error bars represent 95% confidence intervals. Abbreviations: MedE, Medical Expert; COM, Communicator; COL, Collaborator; SCH, Scholar; LED, Leader; HeaA, Health Advocate; PRO, Professionalism. |
In Table 2, the top 10 ranked competencies are marked in bold, and significant differences in rank positions are noted, indicating the higher rank.19 Nine of the top 10 competencies were the same between students of VI and non-VI curricula, with both groups indicating that the most importance competency was “Identify and be able to carry out on-site rescue for emergency, serious, and dangerous patients” within the role of Medical Expert. Regarding the seven roles of the CanMEDS, none of the top rated 10 competencies were under the roles of Collaborator, Scholar, or Health Advocate. In terms of ratings, compared to students from non-VI curricula, the students of VI curricula placed more importance on the role of Communicator. However, no significant differences were found in the ratings of competencies between participating students from VI versus non-VI curricula (Table 2).
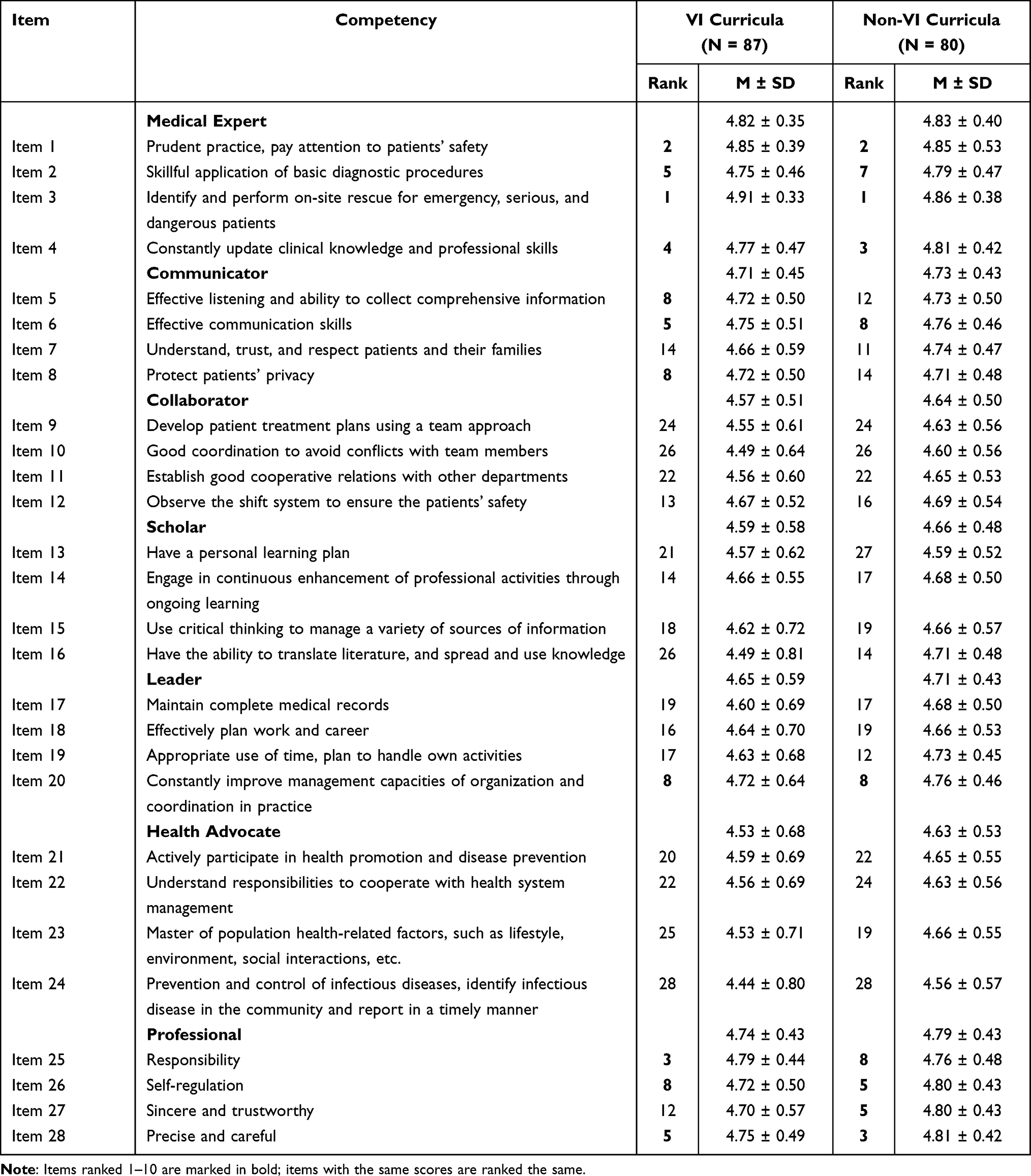 |
Table 2 Competency Fields and Ranking Order of the Key Competencies by All Participating Medical Students |
Among the top rated 10 competencies, nine were the same between faculty of VI and non-VI curricula. All faculty rated the most important competence as one from the role of Medical Expert. Compared to the 10 items top rated by faculty from non-VI curricula, the faculty of VI curricula placed more importance on the role of Communicator. We found one significant difference in the competency ranking by the faculty of VI versus non-VI curricula: “Constantly update clinical knowledge and professional skills” was ranked significantly higher by faculty of non-VI curricula (Table 3).
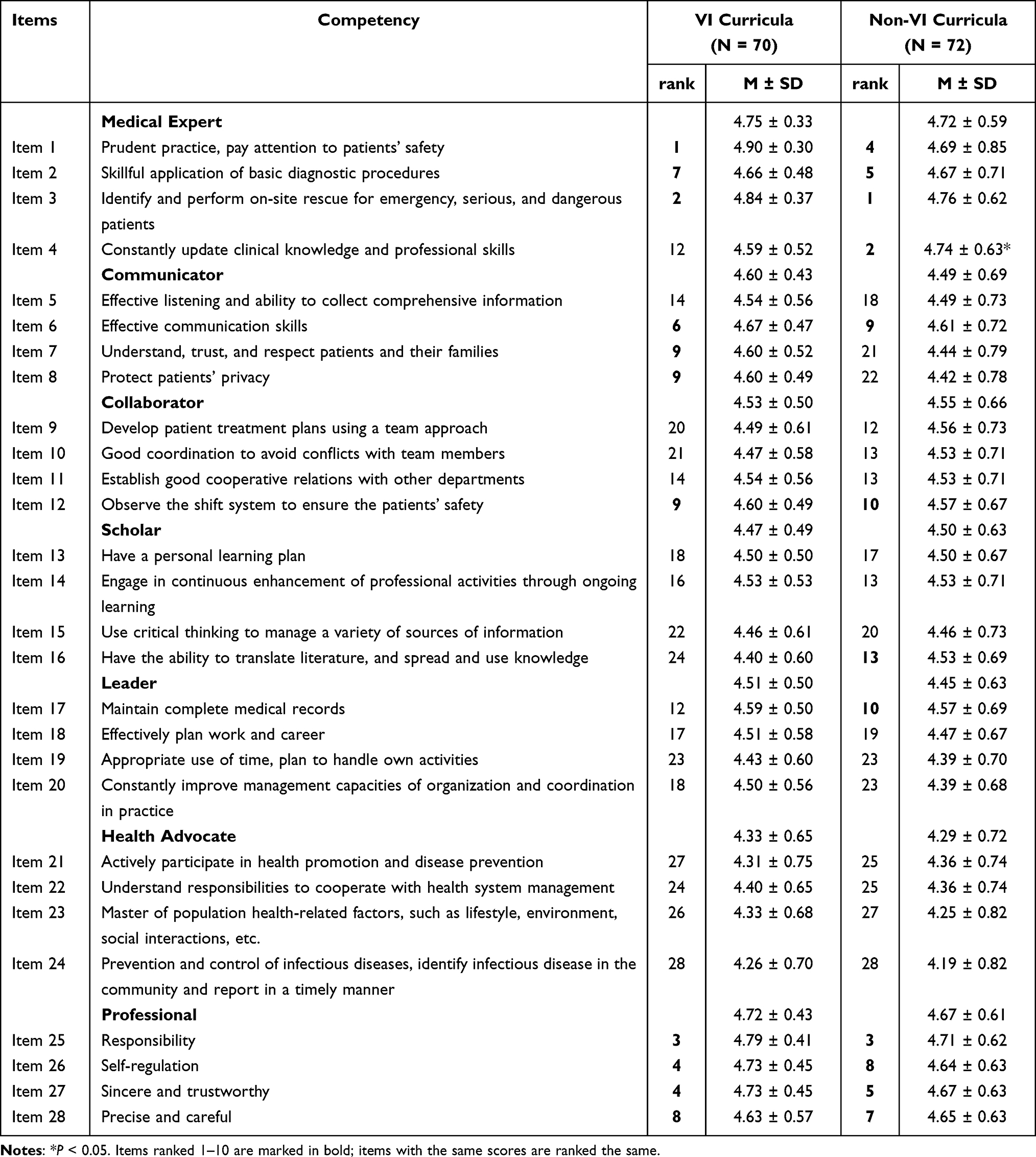 |
Table 3 Competency Fields and Ranking Order of the Key Competencies by All Participating Faculties |
Among all 28 key competencies, the difference of mean rating between the faculty versus and students was greater among non-VI curricula participants than among VI curricula participants (Figures 3 and 4). The students and faculty of non-VI curricula gave statistically different mean ratings for the roles of Medical Expert (P = 0.043), Communicator (P = 0.005), Leader (P = 0.003), and Health Advocate (P = 0.001). Students and faculty from VI curricula gave significantly different ratings for competencies related to the CanMEDS roles of Communicator (P = 0.042), Leader (P = 0.022), and Health Advocate (P = 0.021).
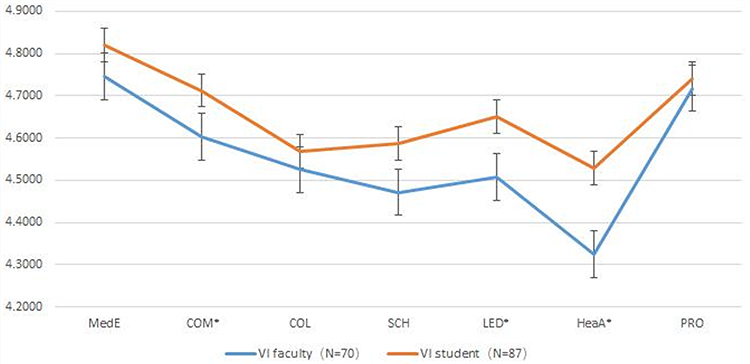 |
Figure 3 Appraisal of aspects of competence related to the CanMEDS roles by faculty and students from VI curricula. Error bars represent 95% confidence intervals. *P < 0.05. Abbreviations: MedE, Medical Expert; COM, Communicator; COL, Collaborator; SCH, Scholar; LED, Leader; HeaA, Health Advocate; PRO, Professionalism. |
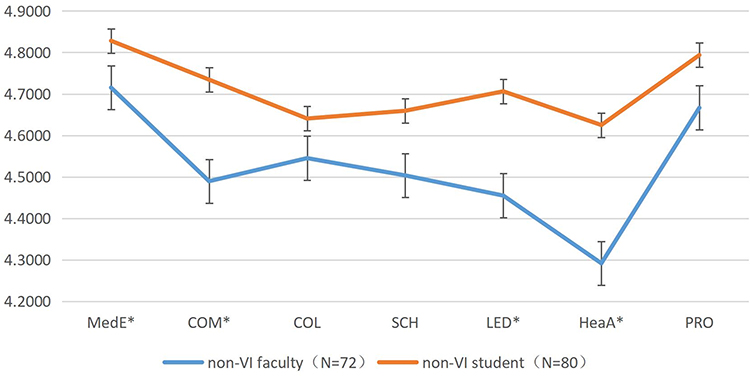 |
Figure 4 Appraisal of aspects of competence related to the CanMEDS roles by faculty and students from non-VI curricula. Error bars represent 95% confidence intervals. *P < 0.05. Abbreviations: MedE, Medical Expert; COM, Communicator; COL, Collaborator; SCH, Scholar; LED, Leader; HeaA, Health Advocate; PRO, Professionalism. |
Discussion
The term “competence” was proposed to describe medical skills by David McClelland of Harvard University in 1973.20 At present, many countries have published the competencies required to be a successful clinician, such as the six critical components of the Accreditation Council for Graduate Medical Education (ACGME),21 the good medical practice of the General Medical Council (GMC),22,23 and CanMEDS. These publications have been very influential on medical education development, both nationally and internationally. Undergraduate medical education is an important stage, during which medical students establish a solid foundation of medical knowledge. Knowing the competencies that future physicians need will help undergraduate medical students identify the abilities they need to master, and make their goals more directional. All faculty of OSJSM were sent to Ottawa Medical College to receive training in teaching, and the medical education in OSJSM was more focused on the cultivation of medical students’ vision and mission.24 This may lead to a higher recognition rate of competencies among students and faculty of VI curricula.
Respondents to our survey did not place equal value on the seven roles of CanMEDS, with all participants giving the highest rating to the role of Medical Expert. This finding differed from a previous study at the University Medical Centre Utrecht in the Netherlands, in which senior medical students appraised CanMEDS competencies and most highly scored the roles of Professionalism and Communication.18 In a study of Danish doctors, Charlotte Ringsted et al11 reported that the role of Communicator was most highly rated. Thus, it was interesting that all faculty and students with different curriculum systems in China attached great importance to clinical competence. This finding may be related to the current model and evaluation system of medical education in China. The Chinese medical education system has undergone reform in recent years.25 Medical education models in China had always followed “discipline-based” education, which has obvious weaknesses in terms of cultivating medical students’ abilities regarding clinical thinking and solving practical problems.26 At present, the evaluation system of medical education in China is mainly focused on medical knowledge and skills. However, a comprehensive and coherent evaluation system has not yet been developed.27 Our present data support the idea that medical education must involve more than medical knowledge and skills.
We also found that faculty and students considered the role of professionalism to be very important. The Charter of Medical Professionalism in the New Millennium (Charter) was published in 2002 by American and European medical associations.28 The Chinese Medical Doctors Association (CMDA) adopted the Physician Charter in 2005, and drafted the Chinese Medical Doctor Declaration (Declaration) six years later.29 Similar findings were reported in a study of Chinese medical students’ attitude to the Physician Charter, showing that Chinese medical students endorsed the Physician Charter and its core values of medical professionalism.30 However, professionalism is not something to be temporarily learned; it is both a commitment and a skill/competency that must be practiced over a lifetime.31 Thus, it may be important to include aspects of professionalism in medical education in a longitudinal manner.
All students and faculty rated the role of Health Advocate as least important. Similar findings have been reported in European studies.18,32 The involvement of undergraduate students in health advocacy throughout medical school can inspire a long-term commitment to addressing health disparities and bridging the gap between the social determinants of health and clinical medicine.33 However, there is no consensus regarding the best methods for teaching this critical medical competency.34 A study by Verma et al35 revealed that faculty knew little about how to teach and evaluate the health advocate role played by residents. Thus, the means of teaching and evaluating a subject may be related to the faculty’s view of the competency’s importance. It remains a challenge to effectively integrate health advocacy-related competencies into medical education.36
With regards to the top rated 10 items, the role of communicator was regarded as more important by faculty and students from VI curricula than non-VI curricula. To adapt the integrative medical curricula, new methods of teaching were used to improve medical students’ competencies, such as project-based learning (PBL), case-based learning (CBL), seminars, etc.37 Previous research has suggested that a teaching strategy that integrates problem-based learning and simulation may be superior to traditional lectures in terms of encouraging communication skills.38,39 Thus, it is possible that the teaching methods of the VI curricula explain why the communicator role was considered more important by the students and faculty from the VI curricula than the non-VI curricula.
Limitations
One important weakness of this study is that it was based in one medical school with two different curricula. The response rate was somewhat low, likely due to the time-consuming task of reading and properly ranking the competency definitions. Additionally, among the respondents to the questionnaire, the internship period of medical students accounted for 3/5. Especially with non VI curricula, the competencies are mostly integrated in the clerkship period, thus this potentially influence the outcome of the intended study. A strength of our study is the recruitment of medical students especially in the clerkship period from different medical schools to evaluate the competencies. Comparison of the perspectives on the competencies between students and faculty from different curricula offers insights that will be useful for further reformation of undergraduate medical curricula.
Conclusions
CanMEDS identified the essential skills that physicians should acquire.The medical students who accept different curricular model have different perceptions of CanMEDS competencies, which may indicate that the curriculum training system pays different attention to the cultivation of students’ competence. Chinese medical students and faculty rated the roles of Medical Expert and Professional as being most important. All participants scored the role of Health Advocate to be least important, which must be addressed in the future. Compared with non-VI participants, VI faculty and students rated communication ability as more important. So, two different curricular model seems to affect medical students’ perspective of communication competence.In china, with the increasing tensiving relationship between doctors and patients. A good communication between doctors and patients seem to be more important.Medical students are future physicians. Strengthening the training of communication ability of medical students is the need of establishing a good doctor-patient relationship, and also the need of training high-quality medical talents. The present results provide some insights that may be useful for curricula planners throughout the reform of the undergraduate medical curricula in China.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request. All methods were carried out in accordance with relevant guidelines and regulations.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the institutional research ethics committee of Shanghai Children’s Medical Center Affiliated to Shanghai Jiao Tong University School of Medicine. The work was carried out in accordance with the Declaration of Helsinki. Participants took the survey anonymously, so their personal information was protected. A consent declaration was presented before the survey, and informed consent was obtained from all subjects. Once starting the survey, participants can withdraw consent by closing the app or website, and no data will be collected.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financed by Shanghai Education Commission Program on Teaching Reform Key Projects in Undergraduate in Shanghai Universities. Shanghai Jiao Tong University School of Medicine Program on Pediatric Education Reform (No.EKJX2020012DGD), Key Teaching Reform Projects for Undergraduates in Shanghai Universities (Shanghai Education Commission Gao (2017)71) Shanghai Jiao Tong University School of Medicine 2018 Pediatrics. Professional “5+3” Intergrated Training Course Construction Project(EKJX2018011SYL).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lei H, Li MC, Cai Q, et al. Curriculum reform at Chinese medical schools: what have we learned? Med Teach. 2014;36(12):1043–1050. doi:10.3109/0142159X.2014.918253
2. Wang J, Sowden S, Dunn WR, et al. Analysis of development and main topics of medical curriculum integration. Med Soc. 2015;28(4):93–95.
3. Wijnen-Meijer M, ten Cate O, Van der Schaaf M, Harendza S. Graduates from vertically integrated curricula. Clin Teach. 2013;10(3):155–159. doi:10.1111/tct.12022
4. Harden RM, Sowden S, Dunn WR. Educational strategies in curriculum development: the SPICES model. Med Educ. 1984;18(4):284–297. doi:10.1111/j.1365-2923.1984.tb01024.x
5. Ten Cate O. Medical education in The Netherlands. Med Teach. 2007;29(8):752–757. doi:10.1080/01421590701724741
6. Ottawa-Shanghai Joint School of Medicine [EB/OL]. Available from: https://www.shsmu.edu.cn/osjsm/About_Us/History.htm.2015.
7. Hall P, Byszewski A, Sutherland S, Stodel EJ. Developing a sustainable electronic portfolio (ePortfolio) program that fosters reflective practice and incorporates CanMEDS competencies into the undergraduate medical curriculum. Acad Med. 2012;87(6):744–751. doi:10.1097/ACM.0b013e318253dacd
8. Vidic B, Weilauf HM. Horizontal and vertical integration of academic disciplines in the medical school curriculum. Clin Anat. 2002;15:233–235. doi:10.1002/ca.10019
9. Wijnen-Meijer M, Ten Cate OTJ, Rademakers JJDJM, Van Der Schaaf M, Borleffs JCC. Borleffs. The influence of a vertically integrated curriculum on the transition to postgraduate training. Med Teach. 2009;31(11):e528–e532. doi:10.3109/01421590902842417
10. Wijnen-Meijer M, Cate OT, Van der Schaaf M, Borleffs JC. Vertical integration in medical school: effect on the transition to postgraduate training. Med Educ. 2010;44(3):272–279. doi:10.1111/j.1365-2923.2009.03571.x
11. Ringsted C, Hansen TL, Davis D, Scherpbier A. Are some of the challenging aspects of the CanMEDS roles valid outside Canada? Med Educ. 2006;40(8):807–815. doi:10.1111/j.1365-2929.2006.02525.x
12. Homberg A, Hundertmark J, Krause J, Brunnée M, Neumann B, Loukanova S. Promoting medical competencies through a didactic tutor qualification programme-A qualitative study based on the CanMEDS Physician Competency Framework. BMC Med Educ. 2019;19:187. doi:10.1186/s12909-019-1636-5
13. Hefler J, Ramnanan CJ. Can CanMEDS competencies be developed in medical school anatomy laboratories?A literature review. Int J Med Educ. 2017;8:231–238. doi:10.5116/ijme.5929.4381
14. Zhuang L. Research on Construction and Evaluation of Competency Model for Clinical Physician [D]. Liaoning: China Medical University; 2017.
15. Xie XH, Shen KL, Wang AH. Thoughts on the cultivation of competence of medical students. Continuing Med Educ. 2015;29(6):58–59.
16. Frank JR, Snell L, Sherbino J, eds. The Draft CanMeds 2015 Physician Competency Framework, Series IV. Ottawa, ON: Royal College of Physicians and Surgeons of Canada; 2015.
17. Cen H. The Research About Clinician’s Competence in Several Teaching Hospitals of a Medical University[D]. Chongqing: Chongqing Medical University; 2014:1–62.
18. Rademakers JJDJM, de Rooy N, ten Cate OTJ. Senior medical students’ appraisal of canMEDs competencies. Med Educ. 2007;41(10):990–994.
19. Fürstenberg S, Harendza S. Differences between medical student and faculty perceptions of the competencies needed for the first year of residency. BMC Med Educ. 2017;17(1):198. doi:10.1186/s12909-017-1036-7
20. McClelland DC. Testing for competence rather than for “intelligence”. Am Psychol. 1973;28(1):1–14. doi:10.1037/h0034092
21. Swing SR. The ACGME outcome project: retrospective and prospective. Med Teach. 2007;29(7):648–654. doi:10.1080/01421590701392903
22. Palmer KT, Harling CC, Harrison J, Macdonald EB, Snashall DC. Good medical practice: guidance for occupational physicians. Occup Med. 2002;52(6):341–352. doi:10.1093/occmed/52.6.341
23. Irvine D. Doctors in the UK: their new professionalism and its regulatory framework. Lancet. 2001;358(9295):1807–1810. doi:10.1016/S0140-6736(01)06800-3
24. Gao YJ, Lu MH, Yin L, Wang Y, Wang W, Jing ZY. Comparison of curriculum of pediatrics education for medical students between Canada and China. J Shanghai Jiao Tong Univ Med Sci. 2015;35(9):1414–1417.
25. Huang L, Cai Q, Cheng L, et al. Analysis of curricular reform practices at Chinese medical schools. Teach Learn Med. 2014;26(4):412–419. doi:10.1080/10401334.2014.910463
26. Zhu HY, Xie XY, Zeng ZR. Practice and Reflection on the reform of medical curriculum integration under the new situation. Chin J Med Edu. 2018;38(2):183–186.
27. Zhang FF, Huang LY. Research progress of clinical teaching evaluation methods. Nursing Rehabilitation. 2014;13(2):119–121.
28. ABIM Foundation. American Board of Internal Medicine; ACP-ASIM Foundation. American College of Physicians-American Society of Internal Medicine; European Federation of Internal Medicine. Medical professionalism in the new millennium: a physician charter. Ann Intern Med. 2002;136(3):243–246. doi:10.7326/0003-4819-136-3-200202050-00012
29. Wang X, Shih J, Kuo FJ, Ho MJ. A scoping review of medical professionalism research published in the Chinese language. BMC Med Educ. 2016;16(1):300. doi:10.1186/s12909-016-0818-7
30. Ding N, Yan D, Li H, Ma Y, Wen D. Chinese medical students’ agreement with and fulfillment of the Physician Charter. BMC Med Educ. 2018;18(1):212. doi:10.1186/s12909-018-1324-x
31. Chestnut DH. On the Road to Professionalism. Anesthesiology. 2017;126(5):780–786. doi:10.1097/ALN.0000000000001545
32. Stutsky BJ, Singer M, Renaud R. Determining the weighting and relative importance of CanMEDS roles and competencies. BMC Res Notes. 2012;5:354. doi:10.1186/1756-0500-5-354
33. Suzanne Boroumand MJ, Stein MJ, Shen JW, Hirsh M, Dharamsi S, Dharamsi S. Addressing the health advocate role in medical education. BMC Med Educ. 2020;20(1):28. doi:10.1186/s12909-020-1938-7
34. Smith MJ. Please don’t make us write an essay! Reflective writing as a tool for teaching health advocacy to medical students. Paediatr Child Health. 2018;23(7):429–430. doi:10.1093/pch/pxy055
35. Verma S, Flynn L, Seguin R. Faculty’s and residents’ perceptions of teaching and evaluating the role of health advocate: a study at one Canadian university. Acad Med. 2005;80(1):103–108. doi:10.1097/00001888-200501000-00024
36. Dharamsi S, Ho A, Spadafora SM, Woollard R. The physician as health advocate: translating the quest for social responsibility into medical education and practice. Acad Med. 2011;86(9):1108–1113. doi:10.1097/ACM.0b013e318226b43b
37. Li X. The Study of Integration Course by Organ Disease. Continuing Med Educ. 2019;33(12):27–29.
38. Li Y, Wang X, Zhu XR, Zhu YX, Sun J. Effectiveness of problem-based learning on the professional communication competencies of nursing students and nurses: a systematic review. Nurse Educ Pract. 2019;37:45–55. doi:10.1016/j.nepr.2019.04.015
39. Nandi PL, Chan JN, Chan CP, Chan P, Chan LP. Undergraduate medical education: comparison of problem-based learning and conventional teaching. Hong Kong Med J. 2000;6(3):301–306.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.