Back to Journals » Advances in Medical Education and Practice » Volume 16
Perceptions of Medical Students’ Unprofessional Behaviors Among Faculty Members and Medical Students: A Cross-Sectional Study at a Japanese Medical School
Authors Yamashita S ![]() , Sakamoto M, Yaita S, Inoue K, Mizoguchi Y, Hoshino Y, Yamaguchi M, Ide N, Katsuki NE, Tago M
, Sakamoto M, Yaita S, Inoue K, Mizoguchi Y, Hoshino Y, Yamaguchi M, Ide N, Katsuki NE, Tago M ![]() , Miyata Y, Oda Y
, Miyata Y, Oda Y
Received 11 June 2025
Accepted for publication 9 September 2025
Published 2 October 2025 Volume 2025:16 Pages 1815—1823
DOI https://doi.org/10.2147/AMEP.S546418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Md Anwarul Azim Majumder
Shun Yamashita,1,2 Maiko Sakamoto,1 Shizuka Yaita,1,2 Kaori Inoue,1 Yukari Mizoguchi,1 Yuki Hoshino,1 Manami Yamaguchi,3 Noriko Ide,4 Naoko E Katsuki,2 Masaki Tago,2 Yasushi Miyata,5 Yasutomo Oda1
1Education and Research Center for Community Medicine, Faculty of Medicine, Saga University, Saga, Japan; 2Department of General Medicine, Saga University Hospital, Saga, Japan; 3Graduate School of Medical Science, Saga University, Saga, Japan; 4Department of General Medicine, NHO Ureshino Medical Center, Saga, Japan; 5Department of Primary Care and Community Health, Aichi Medical University School of Medicine, Aichi, Japan
Correspondence: Shun Yamashita, Education and Research Center for Community Medicine, Faculty of Medicine, Saga University, 5-1-1 Nabeshima, Saga, 849-8501, Japan, Tel +81952343238, Fax +81952342029, Email [email protected]
Introduction: Understanding the perceptions of medical students and faculty members regarding unprofessional behavior is crucial to appropriately guide medical students’ behavior. This study aimed to clarify the differences in perceptions of unprofessional behavior in clinical settings among Japanese medical students and faculty members.
Methods: This single-center, cross-sectional survey was conducted at the Faculty of Medicine, Saga University. Participants were faculty members who participated in a faculty development program on medical students’ unprofessional behaviors in December 2024 and fourth-year medical students who attended a similar lecture in January 2025. The survey items were determined through identifying common unprofessional behaviors based on previous reports and following a discussion with faculty members responsible for pre-graduate education. Participants were divided into faculty and student groups, and differences in perceptions were analyzed using logistic regression analysis.
Results: Participants comprised 40 (response rate 22%) faculty and 65 (64%) students. The faculty group showed significantly lower perceptions of being unprofessional in the following behaviors than the student group: violation of privacy or confidentiality obligations (odds ratio 0.089, 95% confidence interval 0.010– 0.766); false statements or misrepresentation (0.180, 0.034– 0.940); inappropriate use of social networking services (0.150, 0.029– 0.762); fabrication or falsification of data (0.228, 0.005– 0.941); bullying, discrimination, and sexual harassment (0.047, 0.006– 0.383). Multivariate logistic regression analysis identified “bullying, discrimination, and sexual harassment (0.058, 0.007– 0.487)” as the only factor on which their perceptions differed significantly.
Conclusion: Both faculty members and medical students perceived the unprofessional behaviors of medical students similarly, except in the cases of bullying, discrimination, and sexual harassment. However, since faculty members considered five behaviors to be less unprofessional, their perceptions regarding unprofessional behaviors need to be realigned so that they can better guide medical students toward becoming better professionals in the future, thereby improving patient outcomes.
Keywords: unprofessional behavior, medical students, faculty members, difference of perception
Introduction
Physicians are expected to have a certain degree of professionalism. This includes accountability, altruism, excellence, and humanism (compassion, empathy, or integrity) based on excellent clinical skills, communication skills, and sound ethics.1 Patients expect physicians to be professional,2 and creating trusting relationships between patients and physicians can contribute to improving patient outcomes and increasing patient satisfaction.3,4 Medical students should be educated on what constitutes unprofessional behavior during their graduation itself, as it can be a risk factor for disciplinary measures after graduation.5 Unprofessional behavior is generally categorized into four behaviors: lack of engagement, dishonesty, disrespect, and poor self-awareness.6 In Pakistan, 65% of medical students reported that their peers had involved in such behaviors,7 indicating the need to instill professionalism in students.8 However, evaluating medical students’ and physicians’ professionalism is rather complicated as it encompasses multiple aspects such as individual, interpersonal, social, organizational, and cultural values.6,9,10
Medical educators do not always instruct or report on observed unprofessional behaviors.11 Although they observe such behaviors in 20% of the medical students, these are reported in only 3–5% of the cases.12 This may happen due to various reasons, including the fear that reported students may give faculty members a low evaluation, lack of clarity regarding what constitutes unprofessional behavior, concerns that decisions regarding unprofessional behaviors may be subjective, or the time constraint of educating students.13 Therefore, education on professionalism and standardization methods to improve unprofessional behaviors remains insufficient worldwide.4,14,15 However, failing to address unprofessional behaviors may undermine patient safety.
To appropriately educate and report medical students’ unprofessional behavior, it is important to assess and realign their perceptions regarding such behaviors. In particular, the concerns of educators’ subjective evaluations and fears of negative evaluations by students may be resolved by understanding what behaviors medical students and faculty members perceive as unprofessional and the differences in their perceptions.16 However, to the best of our knowledge, there are only two existing quantitative studies on such differences, which are cross-sectional studies performed in England and Saudi Arabia.14,17 In these studies, faculty members judged medical students’ misconduct more severely than the medical students. In the England study, the public gave the harshest evaluations.17 In England, the Good Medical Practice framework established by the General Medical Council, which serves as a global standard for medical professionalism, is likely embedded in the professional consciousness of healthcare providers.18 In Saudi Arabia, professionalism is evaluated based on medical standards, as well as religious and cultural concepts.19 These may have influenced the difference in perceptions observed in England and Saudi Arabia. Although these studies have clarified differences in perceptions regarding academic integrity, unethical conduct, and clinical behaviors, they have not addressed perceptions related to interpersonal issues or personal characteristics. In England, clinical behaviors related to patient interactions and unethical actions are emphasized.18 In contrast, in Japan, actions that cause discomfort to others or disrupt one-on-one relationships, as well as clinical behaviors, are emphasized.18 Given these differences, the findings from England and Saudi Arabia may not necessarily be applicable to the Japanese context.
Hence, this study was conducted based on the hypothesis that perceptions of unprofessional behaviors in clinical settings differ between Japanese medical students and faculty members. Investigating these differences may allow for improvements in faculty training and curriculum design, potentially contributing to patient safety in the future.
Materials and Methods
Study Design and Setting
This single-center cross-sectional study was conducted at the Faculty of Medicine, Saga University, Japan. Saga Prefecture is a regional city in northern Kyushu, southern Japan, with a population of 830,000 people. Saga University is the only medical school in the Saga Prefecture. Medical education in Japan spans six years, and after graduating from high school, students enroll in medical schools to become doctors. Medical students with qualifications as student doctors can start clinical practice. These qualifications can be obtained by passing a public test (computer-based testing and an objective structured clinical examination) in the fourth year.5 After 1.5 years of clinical practice and passing the national medical examination, they can work as medical residents in Japan. At the time of this study, there were 186 faculty members and 101 fourth-year medical students at this medical school. All fourth-year students were scheduled to take public tests within one month. Though they had several lectures on professionalism, none were specifically conducted on medical students’ unprofessional behavior.
Participants
Participants included faculty members of the Faculty of Medicine, Saga University, who had participated in the faculty development (FD) on “Responding to unprofessional behaviors of medical students” in December 2024, and fourth-year medical students of the same institution who participated in the lecture on “unprofessional behaviors of medical students” in January 2025. One month prior to the FD program, the theme and outline were sent to all faculty members via e-mail, encouraging them to attend the program. The lecture was also announced to all medical students, encouraging them to attend. Medical students and faculty members who did not consent to participate in this study were excluded from the analysis.
Sample Size
In a previous report, which investigated the differences in perceptions of student misconduct between medical students and faculty members, the recognition scores for “attending ward teaching whilst drunk (alcohol misuse and lack of insight)” were 3.1 and 3.9, respectively (6-point scale).17 Based on the results of the previous study, an alpha error of 0.05, and a beta error of 0.20, we calculated a sample size of 26 participants in each group for this study.
Data Collection
To collect data, this study employed a Google Forms questionnaire, the items for which were determined by the faculty members of the Education and Research Center for Community Medicine, who are the core members of medical education. The types of unprofessional behaviors of medical students and the categorization proposed in a previous study were used for the final determination.6 This questionnaire was used on a pilot basis. The uniform resource locator of the questionnaire was sent to the faculty members and fourth-year medical students (using a QR code) prior to the commencement of the respective FD program and lecture. All responses were obtained before the sessions began.
Variables
Respondents’ identification numbers or names, gender, and age or year of graduation were obtained. In addition, the respondents were asked to choose all applicable medical students’ unprofessional behaviors from the following list that they believed should be taught and reported: lack of active participation or minimal effort during clinical training; disruptive behavior during clinical training; unexcused absence or tardiness; acting without obtaining the necessary consent; avoiding communication with others; being uncooperative; improper dressing and personal hygiene; failure to comply with rules and regulations; false statements or misrepresentation; fabrication or falsification of data; inappropriate use of social networking services (SNS); bullying, discrimination, and sexual harassment; violation of privacy or confidentiality obligations; rejection of feedback or refusal to accept feedback content; resistance to change; failure to reflect on oneself and blaming others or external factors; and complaining about early start times or late end times of clinical training. Details of the questionnaire are provided in Supplementary Materials 1 and 2.
Statistical Analysis
Categorical variables are expressed as percentages and were compared using the χ2 test. Continuous variables are expressed as medians, and interquartile ranges were compared using the Mann–Whitney U-test. Missing data were excluded from the analysis, and statistical significance was set at p < 0.05. Univariate logistic regression analysis was used to assess the odds ratios (OR) and 95% confidence intervals (CI) for the perceptions of unprofessional behaviors among medical students and faculty members. To complement the OR, Cohen’s h was calculated to quantify the magnitude of differences in proportions between the two groups. Multivariate logistic regression with stepwise reduction was used to identify variables that differentiated the two groups, and the OR and 95% CI were assessed. Considering multicollinearity, among the variables that showed statistical significance in the univariate analysis, one variable from each pair with a Spearman correlation coefficient of 0.7 or higher was selected, and the other was excluded. The internal consistency of the questionnaire was assessed using Cronbach’s α coefficient. SPSS (version 29; IBM Corp., Armonk, NY, USA) was used for statistical analyses.
Ethical Considerations
This study was approved by the Ethics Committee of the Faculty of Medicine at Saga University (approval number R6-58), and the content is disclosed on the website of the Faculty of Medicine, Saga University. Participant consent was obtained using the opt-out method, and participants’ anonymity was ensured. The study was performed in accordance with the 1975 Declaration of Helsinki and approved by the Medical Ethics Committee of the Faculty of Medicine.
Results
Participant Characteristics
A total of 42 faculty members attended the FD, of which 40 agreed to participate in this study (response rate 21.5%) and were included in analyses (faculty group). The median number of years since their graduation was 22. A total of 65 fourth-year medical students attended the lecture on unprofessional behaviors without agreements to participate in this study (response rate 64.4%). The median age of medical students was 22 (22–23) years (student group). Among the participants, 20 of the 40 (50%) faculty members were men, and 27 of the 65 (42%) medical students were men (p=0.556).
Medical Students’ and Faculty Members’ Perceptions of Unprofessional Behavior
The Cronbach’s α coefficient for the items assessing perceptions of unprofessional behaviors was 0.877 overall, with 0.871 for the faculty group and 0.883 for the student group. Table 1 shows the comparison of perceptions of unprofessional behaviors between faculty members and medical students. More than 80% of the participants in both groups recognized the following behaviors as unprofessional behaviors, the highest being “disruptive behavior during clinical training” followed by “violation of privacy or confidentiality obligations”, “false statements or misrepresentation”, “inappropriate use of SNS”, “fabrication or falsification of data”, “acting without obtaining the necessary consent”, and “unexcused absence or tardiness” (Figure 1). Behaviors that were recognized by less than 50% of the students and faculty members were “lack of active participation or making minimal effort during clinical training”, “failure to reflect on oneself and blaming others or external factors”, “avoiding communication with others”, “complaining about early start times or late end times of clinical training”, and “resistance to the change”. Among all unprofessional behaviors, the faculty group was significantly less likely than medical students to recognize the following behaviors as unprofessional: “violation of privacy or confidentiality obligations (85% vs 98%, p=0.007)”, “false statements or misrepresentation (85% vs 97%, p=0.025)”, “inappropriate use of SNS (83% vs 98%, p=0.010)”, “fabrication or falsification of data (83% vs 95%, p=0.029)”, and “bullying, discrimination, and sexual harassment (75% vs 98%, p<0.001)”. The ORs (95% CI) for these unprofessional behaviors in the univariate logistic regression analysis were 0.089 (0.010–0.766), 0.180 (0.034–0.940), 0.150 (0.029–0.762), 0.228 (0.005–0.941), 0.047 (0.006–0.383), respectively.
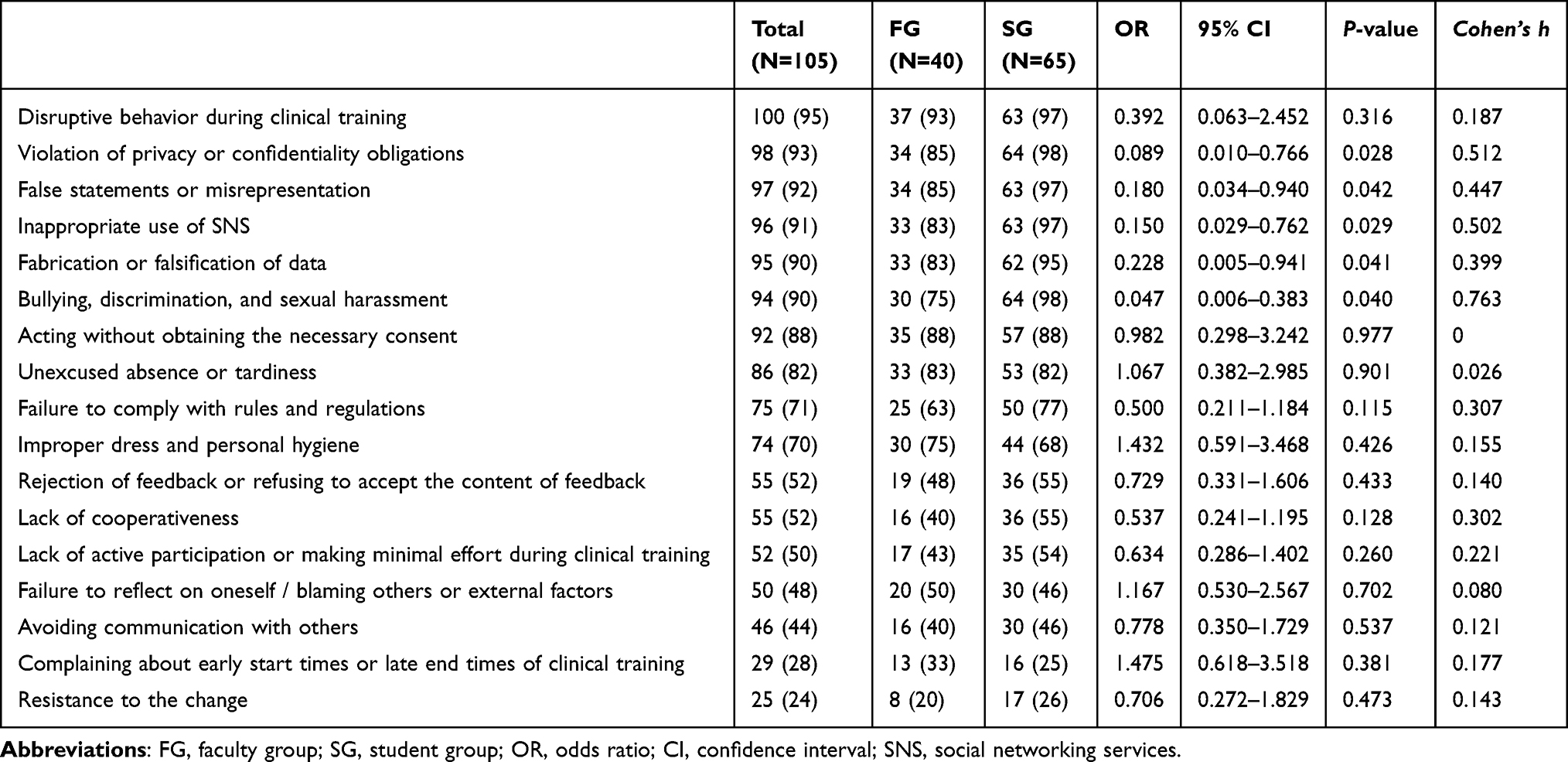 |
Table 1 Comparison of Faculty and Student Perceptions of Medical Students’ Unprofessional Behaviors |
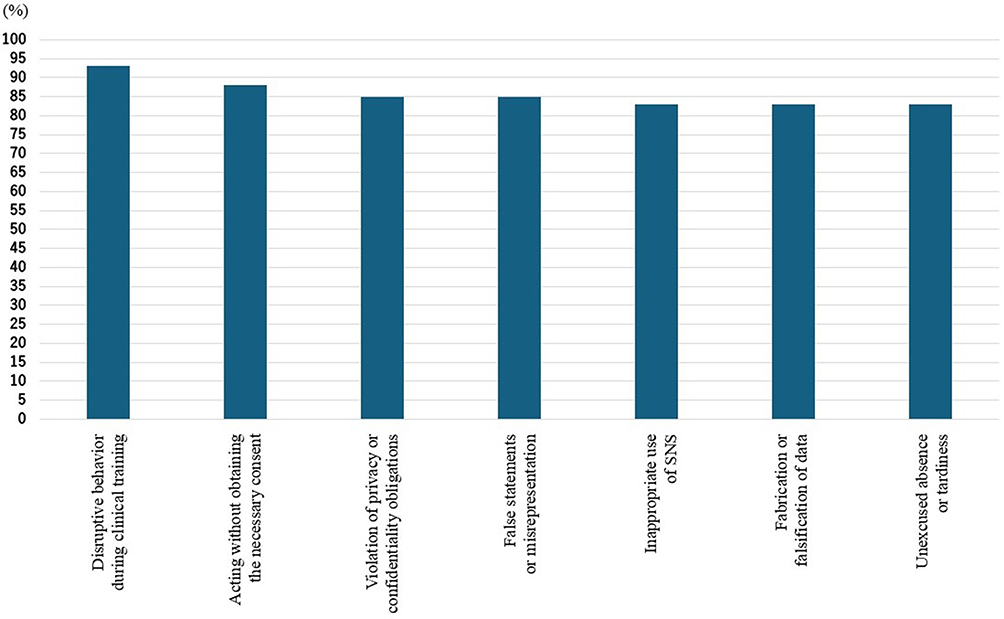 |
Figure 1 The seven unprofessional behaviors with the highest agreement between faculty members and medical students. More than 80% of the participants in both faculty members and medical students recognized the following behaviors as unprofessional behaviors, the highest being “disruptive behavior during clinical training” followed by “violation of privacy or confidentiality obligations”, “false statements or misrepresentation”, “inappropriate use of SNS”, “fabrication or falsification of data”, “acting without obtaining the necessary consent”, and “unexcused absence or tardiness”. |
Unprofessional Behavior Perceptions That Differed Between Medical Students and Faculty Members
The results of the multivariate logistic regression analysis are shown in Table 2. Stepwise reduction identified “bullying, discrimination, and sexual harassment” (OR 0.058, 95% CI 0.007–0.487) as the only significant factor that differed in terms of perceptions between medical students and faculty members.
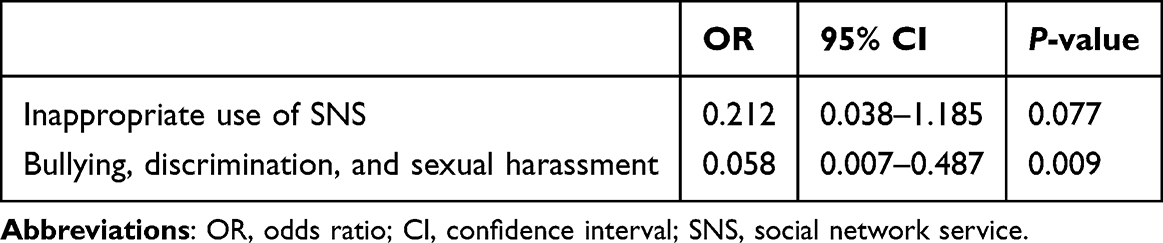 |
Table 2 The Findings of Multivariable Logistic Regression Analysis with Stepwise Reduction on the Perceptions of Unprofessional Behaviors in Medical Students and Faculty Members |
Discussion
In the present study, 80% or more of both the medical students and faculty members of the studied university recognized the following behaviors as unprofessional behaviors: “disruptive behavior during clinical training”; “violation of privacy or confidentiality obligations”; “false statements or misrepresentation”; “inappropriate use of SNS”; “fabrication or falsification of data”; “acting without obtaining the necessary consent”; and “unexcused absence or tardiness”. Among these, disruptive behavior, false statements or misrepresentations, inappropriate use of SNS, and unexcused absence or tardiness were consistent with a previous study conducted in Saudi Arabia.14 Violations of privacy and confidentiality, as well as acting without necessary consent, suggest a diminished sense of responsibility as a physician, and medical students who engage in such behaviors are likely to be subject to disciplinary action after graduation.5,20 Therefore, students should be educated about such behaviors before graduation, which highlights the need for developing a curriculum that facilitates effective professionalism education. However, only 43% of the faculty members and 54% of the medical students in our study perceived a lack of active participation or minimal effort during clinical training as unprofessional. Previous reports in Saudi Arabia showed that 100% of faculty members and 85% of medical students recognized reduced initiative, such as dereliction of the allocated duty in group work, as unprofessional.14 Given that medical students who exhibit such a lack of positivity and motivation are more likely to be subject to disciplinary action after graduation,5,20 it is important to recognize this behavior as unprofessional among both educators and medical students.
In previous studies, faculty members were more severe in their ratings of almost all unprofessional behaviors than medical students.14,17 However, in the present study, faculty members rated the following unprofessional behaviors significantly lower than the medical students: “violation of privacy or confidentiality obligations”, “false statements or misrepresentation”, “inappropriate use of SNS”, “fabrication or falsification of data”, and “bullying, discrimination, and sexual harassment”. Among them, it is possible that false statements or misrepresentation and fabrication, or falsification of data are more frequently encountered by faculty members. It has been reported that faculty members tend to analyze professionalism in multiple aspects.17 As they may consider the reasons for and motivations behind some of these behaviors, these may be more permissible,21 and may lead them to make ambiguous and inconsistent decisions. It is also believed that physicians may ignore misconduct by medical students as they consider that they have little or no clinical responsibility.17 This may have affected the results of this study. Moreover, 5–15% of the medical residents tend to indulge in plagiarism, misconduct during exams, and fraudulent description of publications, and 40–50% tend to report inaccurate results of patient tests and false work hours.22 Faculty members’ memories of their own experiences as residents may have also influenced the results.
In the present study, faculty members were less likely to recognize “bullying, discrimination, and sexual harassment” as an unprofessional behavior than medical students, which was the only significant factor that differed significantly between the groups in the multivariate analysis. Unprofessional and destructive behaviors are often seen in physicians, and 95% of them routinely face insults, angry voices, rude attitudes, or abuse from other physicians.23 In addition, female physicians are more likely to be seen as contributing less to their work, experience economic inequality and lose opportunities for career advancement,24,25 and may consider bullying, discrimination, and sexual harassment common; therefore, they may no longer recognize it as unprofessional behavior. In fact, the proportion of female physicians at Japanese medical schools decreases in accordance with the increase in academic ranks.26 Moreover, female leaders are highly underrepresented and report feeling undervalued in their positions as leaders.27 However, if faculty members do not address these unprofessional behaviors, medical students would begin to feel that these are acceptable.12 Therefore, despite commonly encountering these behaviors, faculty members should not overlook such dishonest, inappropriate, and unacceptable behaviors. Institutionalizing professionalism training, regularly conducting FD workshops, and offering lectures on gender inequality are important strategies to help faculty members recognize such behaviors as unprofessional and provide appropriate guidance to medical students.
Study Limitations
This study had some limitations that must be considered. First, this study may have had a selection bias because it was a single-center cross-sectional study. Therefore, the generalizability of the results is limited. Second, the results may not reflect the perceptions of the entire institution because only the data obtained from faculty members and medical students who participated in the FD and lecture, respectively, were analyzed. Especially, the response rate of faculty members was low, and it is possible that those who participated ware more interested in unprofessional behaviors. Therefore, the perception of faculty members toward unprofessional behaviors may be more lenient than the results of this study. Third, obtained data may be influenced by social desirability bias and response bias. As a result, medical students’ recognition of unprofessional behaviors may be overestimated. Fourth, this study did not investigate the grade of perceptions for each unprofessional behavior, willingness to report it, confidence in handling it, and the barriers and facilitators to reporting. Therefore, even though faculty members are less likely to perceive the behaviors as unprofessional, they may choose to take harsher measures when sanctions are applied. Additionally, even when these behaviors were observed, whether they were actually reported remains unclear. Fifth, this study investigated the recognition of unprofessional behaviors to be taught and reported. Therefore, whether faculty members and medical students believe such behaviors should be addressed through guidance or reporting remains unclear. Finally, different results may be observed if globalization increases the number of faculty members or medical students from abroad, as cultural aspects can influence the perceptions of unprofessional behaviors.
Conclusions
The perceptions of unprofessional behaviors among faculty members and medical students were generally in agreement. However, faculty members were significantly less likely than medical students to consider some behaviors, particularly bullying, discrimination, and sexual harassment, as unprofessional. Hence, faculty members’ perceptions of these behaviors could be improved through the institutionalization of faculty development programs on professionalism, thereby facilitating the effective education of medical students in professional ethics and contributing to the advancement of patient outcomes. To ensure the generalizability pf these findings, multi-center and multi-cultural studies are required to capture the influence of cultural aspects on perceptions of unprofessional behaviors.
Abbreviations
FD, faculty development; SNS, social networking service; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author on reasonable request.
Consent for Publication
All authors gave the final approval for the version to be published, consented to the journal being submitted, and agreed to take responsibility and be accountable for the contents of the article.
Acknowledgments
We would like to thank Editage (https://www.editage.jp/) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Ministry of Education, Culture, Sports, Science and Technology under the project “Formation of Medical Human Resource Development Centers for the Post-COVID-19 Era (Japanese project name)”. No grant number was assigned. The funding source had no role in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mueller PS. Teaching and assessing professionalism in medical learners and practicing physicians. Rambam Maimonides Med J. 2015;6(2):e0011. doi:10.5041/RMMJ.10195
2. Bendapudi NM, Berry LL, Frey KA, Parish JT, Rayburn WL. Patients’ perspectives on ideal physician behaviors. Mayo Clin Proc. 2006;81(3):338–344. doi:10.4065/81.3.338
3. Brennan MD, Monson V. Professionalism: good for patients and health care organizations. Mayo Clin Proc. 2014;89(5):644–652. doi:10.1016/j.mayocp.2014.01.011
4. Tay KT, Ng S, Hee JM, et al. Assessing professionalism in medicine - a scoping review of assessment tools from 1990 to 2018. J Med Educ Curric Dev. 2020;7:2382120520955159. doi:10.1177/2382120520955159
5. Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school. N Engl J Med. 2005;353(25):2673–2682. doi:10.1056/NEJMsa052596
6. Mak-van der Vossen M, van Mook W, van der Burgt S, et al. Descriptors for unprofessional behaviours of medical students: a systematic review and categorisation. BMC Med Educ. 2017;17(1):164. doi:10.1186/s12909-017-0997-x
7. Dar UF, Khan YS. Self-reported academic misconduct among medical students: perception and prevalence. Sci World J. 2021;2021:5580797. doi:10.1155/2021/5580797
8. Ministry of Education, Culture, Sports, Science and Technology. Model core curriculum for medical education in Japan 2022 [Web site]. Available from https://www.mext.go.jp/content/20250411-mxt_igaku-000028108_00003-2.pdf.
9. Goldie J. Assessment of professionalism: a consolidation of current thinking. Med Teach. 2013;35(2):e952–e956. doi:10.3109/0142159X.2012.714888
10. Al-Rumayyan A, Van Mook WNKA, Magzoub ME, et al. Medical professionalism frameworks across non-western cultures: a narrative overview. Med Teach. 2017;39(sup1):S8–S14. doi:10.1080/0142159X.2016.1254740
11. Byszewski A, Gill JS, Lochnan H. Socialization to professionalism in medical schools: a Canadian experience. BMC Med Educ. 2015;15:204. doi:10.1186/s12909-015-0486-z
12. Mak-van der Vossen M, Teherani A, van Mook W, Croiset G, Kusurkar RA. How to identify, address and report students’ unprofessional behaviour in medical school. Med Teach. 2020;42(4):372–379. doi:10.1080/0142159X.2019.1692130
13. Ziring D, Frankel RM, Danoff D, Isaacson JH, Lochnan H. Silent witnesses: faculty reluctance to report medical students’ professionalism lapses. Acad Med. 2018;93(11):1700–1706. doi:10.1097/ACM.0000000000002188
14. Sattar K, Roff S, Meo SA. Your professionalism is not my professionalism: congruence and variance in the views of medical students and faculty about professionalism. BMC Med Educ. 2016;16(1):285. doi:10.1186/s12909-016-0807-x
15. Maristany D, Hauer KE, Leep Hunderfund AN, et al. The problem and power of professionalism: a critical analysis of medical students’ and residents’ perspectives and experiences of professionalism. Acad Med. 2023;98(11S):S32–S41. doi:10.1097/ACM.0000000000005367
16. Yepes-Rios M, Dudek N, Duboyce R, Curtis J, Allard RJ, Varpio L. The failure to fail underperforming trainees in health professions education: a BEME systematic review: BEME Guide No. 42. Med Teach. 2016;38(11):1092–1099. doi:10.1080/0142159X.2016.1215414
17. Brockbank S, David TJ, Patel L. Unprofessional behaviour in medical students: a questionnaire-based pilot study comparing perceptions of the public with medical students and doctors. Med Teach. 2011;33(9):e501–e508. doi:10.3109/0142159X.2011.599450
18. Stanyon M, Shikama Y, Horsburgh J, et al. Exploring conceptions of medical unprofessionalism in Japan and the UK: a Q-methodology study. Fukushima J Med Sci. 2025;71(2):105–118. doi:10.5387/fms.24-00055
19. Tayeb HO, Tekian A, Baig M, Koenig HG, Lingard L. The role of religious culture in medical professionalism in a muslim arab society. Perspect Med Educ. 2023;12(1):56–67. doi:10.5334/pme.920
20. Teherani A, Hodgson CS, Banach M, Papadakis MA. Domains of unprofessional behavior during medical school associated with future disciplinary action by a state medical board. Acad Med. 2005;80(10 Suppl):S17–S20. doi:10.1097/00001888-200510001-00008
21. Ginsburg S, Regehr G, Mylopoulos M. From behaviours to attributions: further concerns regarding the evaluation of professionalism. Med Educ. 2009;43(5):414–425. doi:10.1111/j.1365-2923.2009.03335.x
22. Fargen KM, Drolet BC, Philibert I. Unprofessional behaviors among tomorrow’s physicians: review of the literature with a focus on risk factors, temporal trends, and future directions. Acad Med. 2016;91(6):858–864. doi:10.1097/ACM.0000000000001133
23. Weber DO. Poll results: doctors’ disruptive behavior disturbs physician leaders. Phys Exec. 2004;30(5):6–14.
24. Kumakawa T, Yamashita S, Aoki N, Harada A, Kondo T. Career building for Japanese female hospitalists compared to hospitalists overseas. JHGM. 2022;4(6):279–283.
25. Halley MC, Rustagi AS, Torres JS, et al. Physician mothers’ experience of workplace discrimination: a qualitative analysis. BMJ. 2018;363:k4926. doi:10.1136/bmj.k4926
26. Nagano N, Watari T, Tamaki Y, Onigata K. Japan’s academic barriers to gender equality as seen in a comparison of public and private medical schools: a cross-sectional study. Womens Health Rep. 2022;3:115–123.
27. Cha H, Uchida Y, Choi E. Gender differences in perceived legitimacy and status perception in leadership role. Front Psychol. 2023;14:1088190. doi:10.3389/fpsyg.2023.1088190
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.