Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Perceptions of Community Pharmacists Towards Patient Counseling and Continuing Pharmacy Education Programs in Sudan
Authors Hamadouk RM ![]() , Yousef BA
, Yousef BA ![]() , Albashair ED
, Albashair ED ![]() , Mohammed FM
, Mohammed FM ![]() , Arbab AH
, Arbab AH ![]()
Received 28 January 2023
Accepted for publication 31 March 2023
Published 4 April 2023 Volume 2023:12 Pages 77—85
DOI https://doi.org/10.2147/IPRP.S406219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Riham M Hamadouk,1 Bashir A Yousef,2 Esra D Albashair,1 Fatimah M Mohammed,1 Ahmed H Arbab3
1Department of Clinical Pharmacy, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan; 2Department of Pharmacology, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan; 3Department of Pharmacognosy, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan
Correspondence: Ahmed H Arbab, Department of Pharmacognosy, Faculty of Pharmacy, University of Khartoum, Al-Qasr Ave, Khartoum, 11111, Sudan, Tel +249 991893200, Fax +249 183780696, Email [email protected]
Background: Community pharmacists are uniquely positioned at the heart of communities, and their patient counseling role is the cornerstone for achieving the required therapeutic goals. Therefore, the main objective of this study is to explore the perceptions of community pharmacists regarding patient counseling, and their perception towards continuing pharmacy education programs.
Methods: A descriptive, cross-sectional design was performed among randomly selected 238 community pharmacies in Khartoum locality (Sudan) from September 2022 to December 2022. The data were collected using a self-administered questionnaire adopted from a previous study with few minor modifications, which was adding three sociodemographic questions. Descriptive statistics were carried out according to the study objective to analyze the pharmacists’ responses.
Results: The majority of the community pharmacists gave counseling and understood its importance to the patients, most of them (70.6%) took 1– 5 minutes during the dispensing process. The dose was the most provided information by community pharmacists (26.7%) followed by administration (23.7%) and duration (22.4%). Few (28.2%) of the patients ask the pharmacists about the cost of the medication. Lack of patients’ interest (55%) was the major barrier to effective counseling followed by lack of time (47.9%). Almost all (96.2%) pharmacists in this study were interested in continuing pharmacy education programs, and they preferred programs focusing on common diseases (36.6%), and common drugs (30.3%).
Conclusion: This study showed that the majority of community pharmacists in the Khartoum locality had positive perceptions toward patient counseling and they were interested in continuing pharmacy education programs.
Keywords: community pharmacist, continuing pharmacy education, patient counseling, Sudan
Introduction
Community pharmacists play an important role in the healthcare system, they are uniquely positioned at the heart of communities due to their free accessibility and smooth approaches to patients.1 Their conventional role has shifted from compounding and supplying medicinal products toward a patient‑centered role.2 The patient‑centered role of community pharmacist aims to improve the effectiveness of the therapy and minimize preventable drug-related problems which might cause morbidity and mortality.3 Community pharmacists’ role has evolved substantially in the last decades, it involves treating diseases, managing chronic diseases, providing advice to other healthcare givers, contributing in immunization programs, and enhancing healthy lifestyles.4 Despite that, patient counseling is considered one of the most important services provided by community pharmacists.5
Patient counseling is the provision of oral and/or written information about the patient’s medication including the route of administration and regimen, precautions, potential side effects, and storage conditions, along with counseling non-pharmacologic treatments like diet and lifestyle modification.6 According to the International Pharmaceutical Federation (FIP), patient counseling is considered a major priority, and pharmacists are accountable for offering the required information for the optimal use of medications.7 To provide effective counseling pharmacists should have good knowledge of pharmacotherapy and possess suitable communication skills. They should use open-ended questions and active listening to obtain information from patients, as well as know patients’ cultures, beliefs, attitudes, and practices, especially toward health and illness. Also, they should understand patients’ feelings regarding the health system, and educate them about their participation in decision-making and management of their health.8
The World Health Organization (WHO) called for greater participation and utilization of pharmacists’ broad academic backgrounds in the health care system. Accordingly, FIP recommends that the expansion of the pharmacist’s role must be reproduced in the student learning and continuing education of pharmacists.9 Counseling is a complex process, especially in a community setting, which may justify the poor quality of counseling practices in community pharmacies.10
Many studies have investigated the counseling practices of community pharmacists, either regarding specific illness,11,12 detection of drug interactions,13 or general counseling practice,14 and most of these studies revealed the suboptimal practice. Other previous studies have examined the impact of community pharmacist counseling on patient outcomes.15,16 Although in Sudan and other African countries, some studies have addressed the counseling practice of community pharmacists,17–19 however, further research is still needed to cover different aspects related to the profession of pharmacy. Furthermore, since pharmacists are one of the health professions that face the challenge of rising their competencies to meet the changeable requirements of society,3 and their effective patient counseling is the cornerstone for achieving the required therapeutic goals20. This study aims to explore the perceptions of community pharmacists regarding patient counseling, and their perceptions toward continuing pharmacy education programs.
Materials and Methods
Study Design
It was a descriptive cross-sectional design per the STROBE statement,20 using a self-administered questionnaire provided to the pharmacists working in the community pharmacies in Khartoum locality.
Sample Size and Sampling
The number of community pharmacies used in this study was derived from a list obtained from The Sudanese General Directorate of Pharmacy, which contains all registered community pharmacies in Khartoum locality. The minimum sample size(n) of this study was 238 pharmacies, it was determined using the equation:
n = N/1 + N(e)2, where N is the study population which was 587 pharmacies, and (e) an error margin of 0.05. The formula is based on a degree of variability of P = 0.5, and a 95% confidence interval. A simple random sampling technique was performed to select the sample in this study.
Data Collection
Data were collected between September 2022 and December 2022, using a questionnaire adopted from a previous study,21 with few minor modifications, the researchers revised the questionnaire to evaluate its content validity by showing it to three faculty members in the Faculty of Pharmacy, University of Khartoum. Accordingly, three additional questions were added to the original questionnaire which were the age, gender, and years of experience as community pharmacist. After that After that, a pre-test study was made in fifteen community pharmacists to ensure the clarity and appropriateness of the questions. The data from the pretest were not included in the final study. The questionnaire consists of 23 questions, it includes a multiple response question. It contains four parts, the first part consists of four questions regarding the sociodemographic characteristics. The second part includes seven questions pertained to the pharmacy setting’s such as the number of patients per day, the number of pharmacists in the pharmacy, and the source of information available in the pharmacy. The third parts contains nine questions regarding patient counseling and problems faced by the pharmacist during counseling and how to overcome them. The fourth part of the questionnaire consists of three questions about pharmacists’ perceptions regarding continuing education programs. A pharmacist in each selected pharmacy was asked to fill out the questionnaire, and the questionnaires were collected during the same visit. A total of 238 questionnaires were obtained at the end of the study period.
Data Management and Analysis
Pharmacists’ responses were analyzed using Statistical Package for Social Sciences software, version 26.0 (IBM SPSS Inc., Chicago, IL). Descriptive statistics were carried out according to the study objective, and the results were presented as tables containing frequencies and percentages.
Ethical Consideration
The study was conducted agreeing with the recommendations of the Declaration of Helsinki. The Ethical Committee of the Faculty of Pharmacy University of Khartoum (FPEC-03-2020) approved this study, Additional approval was obtained from the scientific research authority ministry of health and The Sudanese General Directorate of Pharmacy. Written informed consent was collected from the community pharmacists involved in this study, and the purpose of the study was explained to each participating pharmacist.
Results
Sociodemographic Characteristics of the Respondents
A total of 238 community pharmacists were included in the study (100% response rate). Females were representing the majority of the respondents 66% (n=157), while males represented 34% (n=81) of the respondents. The mean age of the community pharmacists was 28.68 ± 4.88, and the most common age category was from 26–30 years representing 46.2% (n=110) of the community pharmacist under study. The characteristics of the community pharmacists are in Table 1.
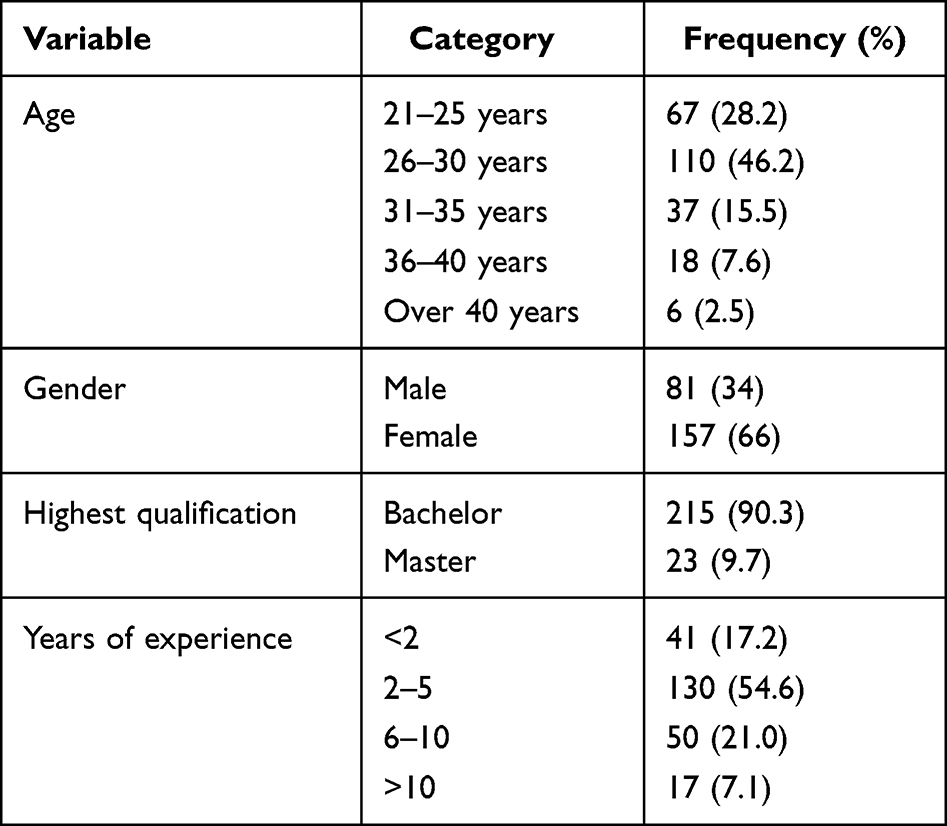 |
Table 1 Socio-Demographic Characteristics of the Community Pharmacists |
Number of Patients Visiting Community Pharmacies
In this study most of the community pharmacies 55.5% (n=132) were daily visited by more than 50 patients, followed by 20–25 patient visits in 22.7% (n=54) community pharmacies, and 35–50 patient visits in 18.5% (n=44) community pharmacies.
Dispensing Time in Community Pharmacies
More than two-thirds 70.6% (n=168) community pharmacists took 1–5 minutes during dispensing a prescription, followed by 5–10 minutes by 14.7% (n=35), and 13.4% (n=32) pharmacists took less than 1 minute, while pharmacists who took more than 10 minutes were 1.3% (n=3).
The Sources of Drug Information in the Community Pharmacies
The results showed that 23.5% of the community pharmacist do not have any sources of drug information in their pharmacies. The British National Formulary (BNF) was the commonest source of drug information available and used by community pharmacists (23.5%), followed by Sudan Medicine Handbook (SMH) (13.4%). While 12.8% of community pharmacists depended mainly on online resources (Table 2).
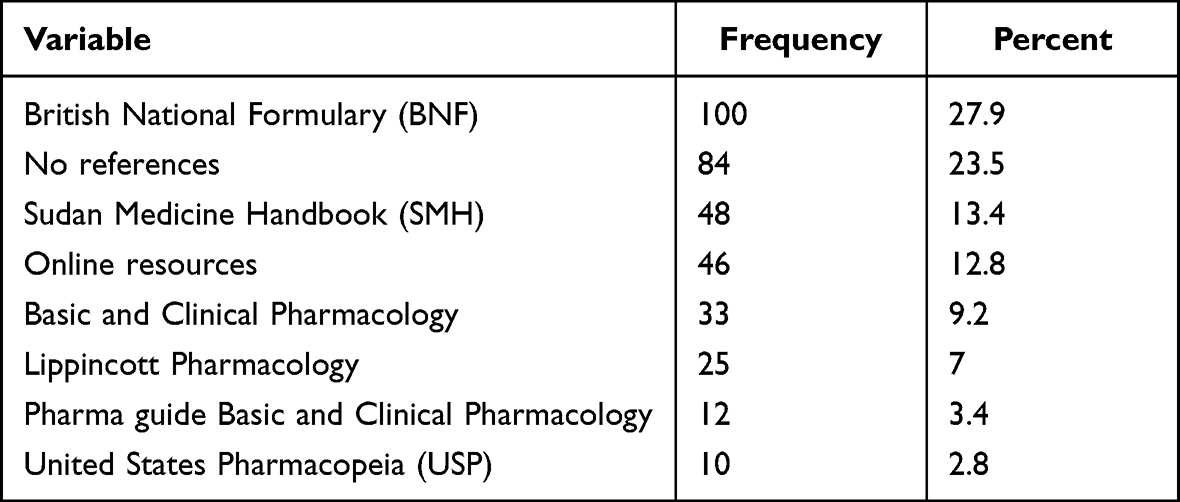 |
Table 2 The Sources of Drug Information Available and Used by the Community Pharmacist During Their Work in the Community Pharmacies |
The Reasons for Giving Medication Counseling
Almost all community pharmacists (99.6%) said they counseled their patients about their medications and 98.3% thought that counseling is vital to patients. Regarding this counseling, 33.7% of the community pharmacists believed that giving counseling improves the patient’s compliance, and 23.3% of them do counseling to have professional satisfaction, while 22.7% of pharmacists considered counseling is their duty (Table 3).
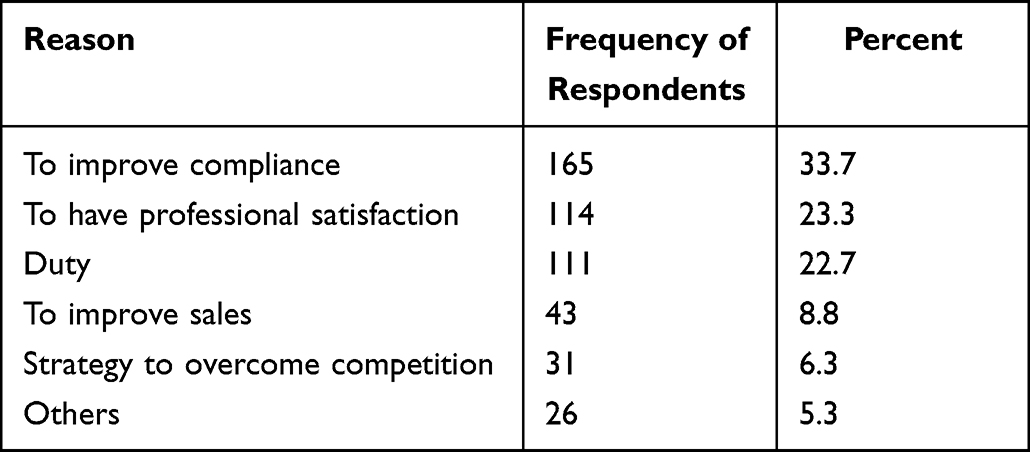 |
Table 3 Reasons for Giving Medication Counseling |
The dose of the medication was the most provided information by community pharmacists 26.7%, followed by 23.7% and 22.4% for administration and duration of the treatment respectively (Table 4).
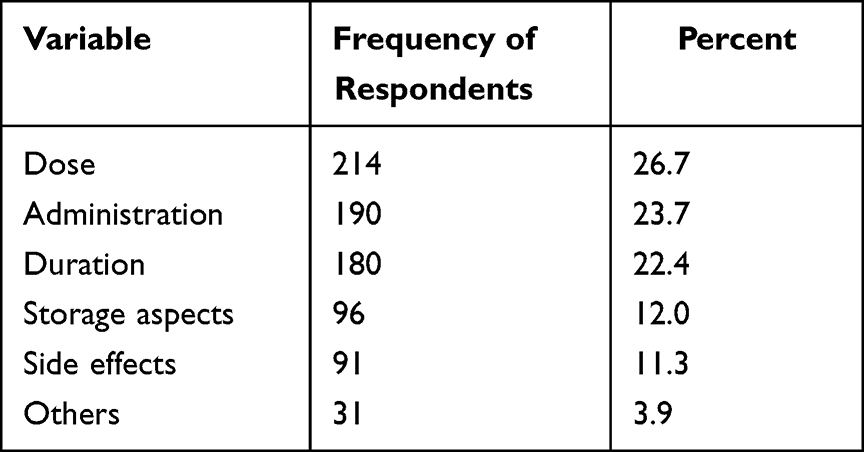 |
Table 4 Type of Information Provided by Community Pharmacists During Counseling |
The Most Common Questions Asked by the Patients
Regarding the questions asked to community pharmacists by the patients, the cost was the most asked question 28.2% followed by asking about the dose 20.4%, and the administration 20.1%, while 8.8% of the patients asked about the side effects of their medications. Further details are shown in Table 5.
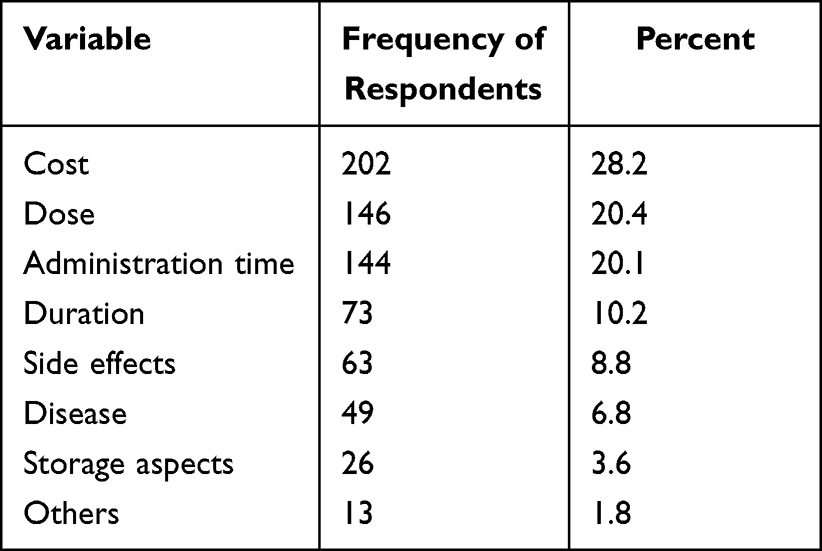 |
Table 5 Questions Frequently Asked by the Patients |
Barriers Encountered by Community Pharmacists During Patient Counseling and Strategies to Overcome the Barriers
The major barrier that faced the community pharmacists during patient counseling was the lack of patients’ interest, as 55% (n=131) of pharmacists felt that, followed by the lack of time 47.9% (n=114), and lack of knowledge 36.6% (n=87). To overcome these barriers 29.8% (n=128) of the community pharmacists suggested providing separate spaces for counseling, and 26.6% (n=114) of them suggested providing continuing education programs (Table 6).
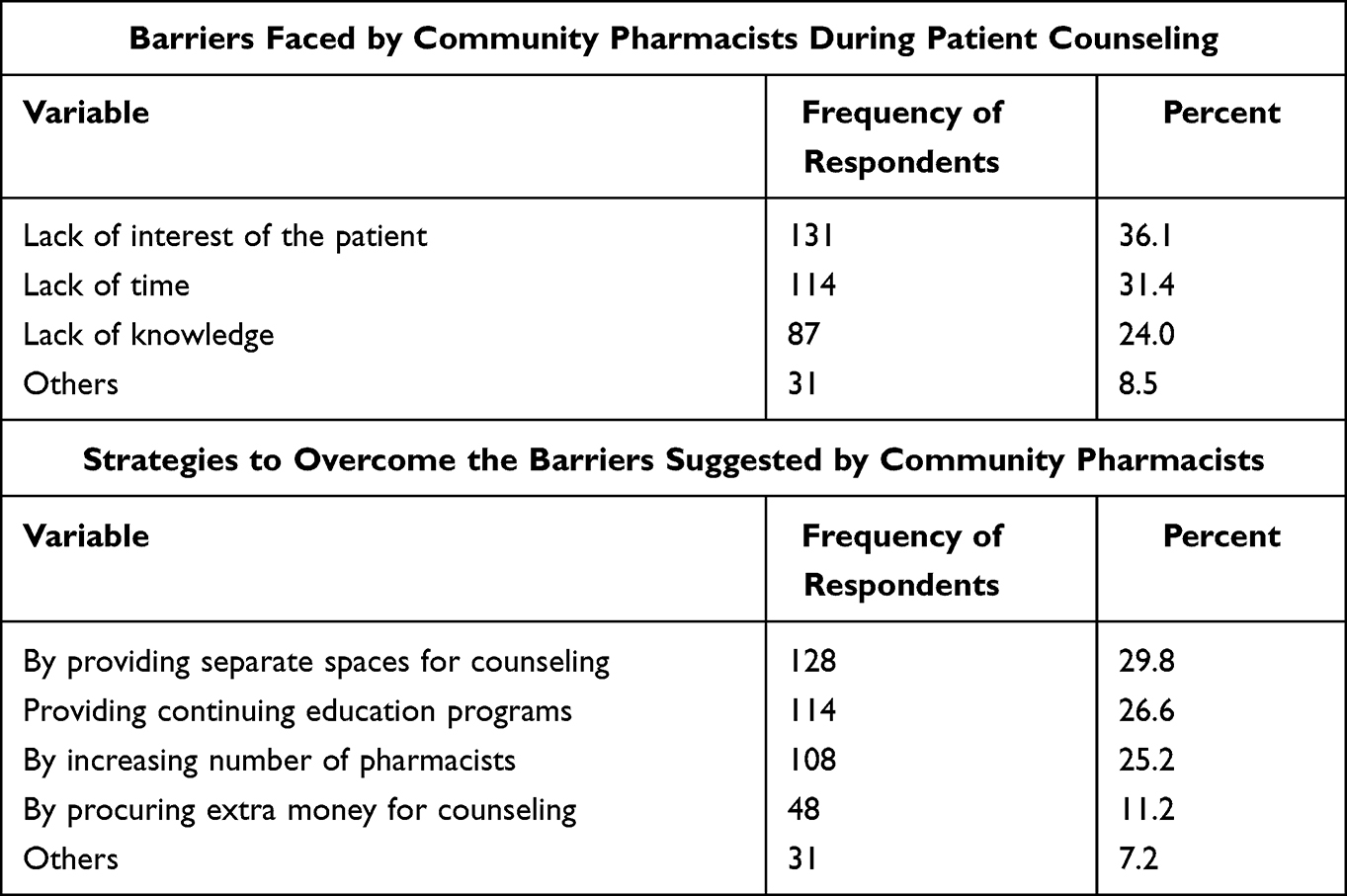 |
Table 6 Barriers Faced by Community Pharmacists During Counseling and Their Suggestions to Overcome Them |
Community Pharmacists’ Interest in the Continuing Pharmacy Education Programs
Almost all (96.2%) of the respondent pharmacists were interested in continuing pharmacy education, they also believed continuing pharmacy education programs is important to improve their knowledge and maximize their practice. They were interested more in educational programs related to common diseases (36.6%), followed by common drugs (30.3%), lifestyle (21.4%), and others (11.7%).
Discussion
Safe, rational, and effective use of medicines by the community can be achieved only through patient counseling which is believed to be the responsibility of the pharmacists.22,23 In the current study, almost all community pharmacists have a positive perception regarding patient counseling. This result is similar to the results of other comparable studies.24,25 In contrast, in a study from South India that aimed to know the perceptions and attitudes of community pharmacists’ toward patient counseling, a devastating result was obtained as 76% of the pharmacists were not interested in providing patient counseling.26
To provide good counseling pharmacists must spend more time with patients, the WHO specified that the pharmacist should spend at least three minutes providing counseling.27 In our study, more than two-third of the community pharmacists took 1–5 minutes to dispense a prescription which is per what was found in two similar studies conducted in Iraq,24 where almost 51% of the pharmacists spent from 1–5 minutes, and Nepal,21 where 56.6% of the participant took 1–5 minutes with each patient during the dispensing process.
Regarding the sources of drug information available in the community pharmacies. The most common source of drug information was the BNF, which provides information about all the medicines available on the National Health Service (NHS). It covers aspects like prescribing, dosage and administration, pharmacology, and side effects, and includes a section on drug interactions. The Sudan Medicine Handbook (SMH), which was used by many pharmacists mimics the BNF in many details but only contains drugs registered in Sudan, and both provide great assistance to community pharmacists. What was observed in this study is that almost a quarter of the community pharmacists did not have any source of information in their pharmacies or even use any online resources to obtain information about drugs. Community pharmacists encounter many situations during their daily practice such as drug interactions, adverse drug reactions, and drug use during pregnancy, in these situations, it is vital to provide the correct use of drugs. Hence accessing an adequate source of drug information is important.28 A pharmacist must not rely only on his or her memory as with every day new information is added to the field of pharmacy, and it would be impossible for the community pharmacists to get all this new information regarding patient care.29
Regarding patient counseling, almost one-third of community pharmacists believe that giving counseling improves the patient’s compliance. Non-compliance to medications is attributed to poor patient counseling.30 The result of the present study is different from the study by Poudel et al,21 where the major reason for giving counseling to patients is believing that it is the duty of the pharmacist. During counseling, most of the pharmacists in this study focus on providing information regarding the dose, administration, and duration of the treatment, which is similar to the observations of other studies.24,25 Although the side effects of drugs are considered an important factor that affects patient adherence,31 only 11.3% of pharmacists provide counseling regarding it, and the reason for this might be that pharmacists may decrease the given information during counseling due to lack of patients’ interest. On the other hand, regarding questions that patients usually asked during counseling, the highest percentage of the patients ask about the cost of the medication which is similar to the results of a previous study in Nepal,21 and this is maybe explained by the deteriorating financial status of the individuals in our country due to the economic inflation.
To understand the counseling practices of pharmacists in community pharmacies it is necessary to identify and assess counseling barriers, many studies have already identified different aspects including the attitude of the pharmacists and the crowdedness of the pharmacies.23 In the current study, the major barrier encountered by the community pharmacists was the lack of patients’ interest which might be due to patients’ ignorance regarding the importance of counseling, this result is in agreement with what was found in a similar study from Iraq,24 and another study from Northwest China.32
The lack of patients’ interest might be overcome by promoting public education regarding the importance of counseling and the information that they should know regarding their medications during the counseling process. In addition to the lack of patients’ interest, according to other pharmacists’ lack of time and knowledge also can influence their counseling practice which is similar to the findings observed in studies from Malaysia,25 Iraq,24 and Nepal.21 While in a study conducted to explore the perception of community pharmacy personnel towards patient counseling in Aden,33 poor patient counseling was attributed to the absence of professionally qualified pharmacists in the community pharmacies.
Some strategies were deemed to overcome the problem of poor counseling, in this study the highest strategy suggested by most of the respondents was providing separate spaces for counseling, followed by attending continuing pharmacy education programs, and increasing the number of pharmacists in the pharmacies. Some studies found that attendance in continuing pharmacy education programs was the commonest solution mentioned by pharmacists to overcome counseling barriers, as increasing pharmacists’ knowledge can be useful in reducing these barriers.24,26,34 While in another two studies, pharmacists felt that promoting public education will ease the counseling process.33,35
Regarding pharmacists’ perception toward continuing pharmacy education, the present revealed that almost all participants were interested in continuing pharmacy education programs, and they declared that these educational programs would help in improving their knowledge. This result is in agreement with the findings of previous studies conducted in Nepal,21 Iraq,24 Yemen,33 and Malaysia.25 Pharmacists’ interest in these programs was more focused on common diseases and common drugs. Continuing pharmacy education has been demonstrated to be beneficial in enhancing pharmacists’ competencies, to improve patient outcomes.35,36 For developing and implementing an effective continuing pharmacy education, its essential to consider both, the local context as well as best models for continuing professional development. The seven items Harden model acronymized as CRISIS (convenience, relevance, individualization, self-assessment, interest, speculation, and systematic) summarized the criteria required for an effective professional development program.37
This study has a few limitations, one of them is the limited generalizability as this study was conducted only in Khartoum locality, so it does not reflect the perception of the entire community of pharmacists in Sudan. Another limitation is that this study did not investigate the pharmacists’ opinions on the availability of pharmacy education programs in the country, and the barriers to not participating in them.
Conclusion
Our study showed that the majority of the participant had positive perceptions toward patients’ counseling. Different drug information sources were used by community pharmacists, nevertheless, a considerable proportion did not have or use any drug information sources. Community pharmacists had mentioned lack of time, and lack of interest of the patient as the main barriers that affect their professional counseling. Issues such as common diseases and common drugs were highlighted to be addressed in the pharmacy education programs. This study provided a clue about what is supposed to be implemented to improve the counseling process. Given the evolving nature of healthcare, stakeholders should endorse regular and effective continuing pharmacy educational programs. It's important to identify what learning programs are required for professional practice through future research and self-assessment. In addition, the regulatory bodies need to integrate appropriate continuing pharmacy education programs as a requirement for licensure update. Furthermore, it is imperative to use the media to spread awareness among patients about the importance of counseling and how it impacts their lives.
Acknowledgments
The authors acknowledge all community pharmacists who agreed to participate in this study.
Funding
There is no funding to report.
Disclosure
All authors declare that there are no conflicts of interest in this work.
References
1. Alfadl AA, Alrasheedy AA, Alhassun MS. Evaluation of medication counseling practice at community pharmacies in Qassim region, Saudi Arabia. Saudi Pharm J. 2018;26(2):258–262. doi:10.1016/j.jsps.2017.12.002
2. Ibrahim A, Scott J. Community pharmacists in Khartoum State, Sudan: their current roles and perspectives on pharmaceutical care implementation. Int J Clin Pharm. 2013;35:236–243. doi:10.1007/s11096-012-9736-x
3. Lias N, Lindholm T, Pohjanoksa-Mäntylä M, Westerholm A, Airaksinen M. Developing and piloting a self-assessment tool for medication review competence of practicing pharmacists based on nationally set competence criteria. BMC Health Serv Res. 2021;21(1):1–12. doi:10.1186/s12913-021-07291-6
4. Fatima F, Sherazi BA. Evolutionary role of the community pharmacist A review. Asian Pacific J Health Sci. 2017;4(4):136–139. doi:10.21276/apjhs.2017.4.4.33
5. Puspitasari HP, Sc B, Phil M, et al. A review of counseling practices on prescription medicines in community pharmacies. Res Soc Adm Pharm. 2009;5(3):197–210. doi:10.1016/j.sapharm.2008.08.006
6. Surur AS, Getachew E, Teressa E, Hailemeskel B, Getaw NS, Erku DA. Self-reported and actual involvement of community pharmacists in patient counseling: a cross-sectional and simulated patient study in Gondar, Ethiopia. Pharm Pract (Granada). 2017;15(1):1–7. doi:10.18549/PharmPract.2017.01.890
7. Asmelashe Gelayee D, Binega Mekonnen G. Perception of community pharmacists towards dispensing errors in community pharmacy setting in Gondar Town, Northwest Ethiopia. Biomed Res Int. 2017;2017:2137981. doi:10.1155/2017/2137981
8. American Society of Health-System Pharmacists. ”ASHP” guidelines on pharmacist-conducted patient education and counseling. Am J Health Syst Pharm. 1997;54:431–434. doi:10.1093/ajhp/54.4.431
9. Wiedenmayer K, Summers RS, Mackie CA, et al. (2006). Developing Pharmacy Practice: A Focus on Patient Care: Handbook.
10. Al Aqeel S, Abanmy N, AlShaya H, Almeshari A. Interventions for improving pharmacist-led patient counselling in the community setting: a systematic review. Syst Rev. 2018;7(1):1–13. doi:10.1186/s13643-018-0727-4
11. Langer B, Bull E, Burgsthaler T, Glawe J, Schwobeda M, Simon K. Assessment of counselling for acute diarrhoea in German pharmacies: a simulated patient study. Int J Pharm Pract. 2018;26(4):310–317. doi:10.1111/ijpp.12405
12. Santos AP, Mesquita AR, Oliveira KS, Lyra DP. Assessment of community pharmacists´ counselling skills on headache management by using the simulated patient approach: a pilot study. Pharm Pract. 2013;11(1):3–7.
13. Hamadouk RM, Albashair ED, Mohammed FM, Yousef BA. The practice of the community pharmacists in managing potential drug-drug interactions: a simulated patient visits. Integr Pharm Res Pract. 2022;11:71–84. doi:10.2147/IPRP.S355675
14. Alaqeel S, Abanmy NO. Counselling practices in community pharmacies in Riyadh, Saudi Arabia: a cross-sectional study. BMC Health Serv Res. 2015;15(1):1–9. doi:10.1186/s12913-015-1220-6
15. Blalock SJ, Roberts AW, Lauffenburger JC, Thompson T, O’Connor SK. The effect of community pharmacy-based interventions on patient health outcomes: a systematic review. Med Care Res Rev. 2013;70(3):235–266. doi:10.1177/1077558712459215
16. Van Wijk BLG, Klungel OH, Heerdink ER, De Boer A. Effectiveness of interventions by community pharmacists to improve patient adherence to chronic medication: a systematic review. Ann Pharmacother. 2005;39(2):319–328. doi:10.1345/aph.1E027
17. North K. Quality and forms of medication information provided to patients by community pharmacists. WJPR. 2016;5(4):332–358.
18. Marfo AF, Owusu-Daaku FT, Kyerewaa-Akromah E. Patient knowledge of medicines dispensed from Ghanaian community pharmacies. Pharm Pract. 2013;11(2):66–70.
19. Ameh D, Wallymahmmed A, Mackenzie G. Patient Knowledge of their Dispensed Drugs in Rural Gambia. Int J Sci Basic Appl Res. 2014;16(2):61–85.
20. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):1623–1627. doi:10.1371/journal.pmed.0040296
21. Poudel A, Khanal S, Kadir A, Palaian S. Perception of Nepalese community pharmacists towards patient counseling and continuing pharmacy education program: a multicentric study. J Clin Diagnostic Res. 2009;3(2):1408–1413.
22. Bizri E, El Bizri L, Dimassi A. Lebanese community pharmacy: the role of the pharmacist in the health care. Eur J Pharm Med Res. 2019;6(1):149–158.
23. Javed B, Kheir N, Yousif A. Patient counseling practices among community pharmacists in Qatar.
24. Mohammed SI, Dawood EB, Abaas IS. Perceptions and attitudes of community pharmacists’ towards patient counseling and continuing pharmacy education programs in Iraq. Iraqi J Pharm Sci. 2019;28(2):30–36.
25. Rajiah K, Preet Kaur K, Sivarasa S, Leowyeow M. Perception of community pharmacists towards patient counseling and continuing pharmacy education program in Kuala Lumpur and Selangor states of Malaysia. Am J Pharm Heal Res. 2014;2(1):49–56.
26. Palaian S, Rao PGM, Nair NM, Nair NM, Alam K. Perception of community pharmacists towards patient counseling in South India. Pharma J Kenya. 2008;19:13–17.
27. Gokcekus L, Toklu HZ, Demirdamar R, Gumusel B. Dispensing practice in the community pharmacies in the Turkish Republic of Northern Cyprus. Int J Clin Pharm. 2012;34:312–324. doi:10.1007/s11096-011-9605-z
28. Zehnder S, Beutler M, Bruppacher R, Ehrenhöfer T, Hersberger KE. Needs and use of drug information sources in community pharmacies: a questionnaire-based survey in German-speaking Switzerland. Harm World Sci. 2004;26(4):197–202. doi:10.1023/B:PHAR.0000035881.17853.e0
29. Iwanowicz SL, Marciniak MW, Zeolla MM. Obtaining and providing health information in the community pharmacy setting. Am J Pharm Educ. 2006;70(3):57. doi:10.5688/aj700357
30. Ibrahim MI, Palaian S, Al-Sulaiti F, El-Shami S. Evaluating community pharmacy practice in Qatar using simulated patient method: acute gastroenteritis management. Pharm Pract. 2016;14(4):800. doi:10.18549/PharmPract.2016.04.800
31. Juste M. Medication adherence. Pharmacien Hospitalier Et Clinicien. 2019;54:107–108. doi:10.1016/j.phclin.2019.05.001
32. Fang Y, Yang S, Feng B, Ni Y, Zhang K. Pharmacists’ perception of pharmaceutical care in community pharmacy: a questionnaire survey in Northwest China. Heal Soc Care Commun. 2011;19(2):189–197.
33. Alshakka M, Bahattab A, Ravi Shankar P, Ansari M, Ali HS, Ibrahim MIM. Perception of community pharmacy personnel towards patient counseling and continuing pharmacy education programs in Aden, Yemen. J Clin Diagnostic Res. 2018;12(7):LC18–22.
34. Sancar M, Okuyan B, Apikoglu-Rabus S, Izzettin FV. Opinion and knowledge towards pharmaceutical care of the pharmacists participated in clinical pharmacy and pharmaceutical care continuing education program. Turk J Pharm Sci. 2013;10(2):245–253.
35. Schindel TJ, Kehrer JP, Yuksel N, Hughes CA. University-based continuing education for pharmacists. Am J Pharm Educ. 2012;76(2):1–7. doi:10.5688/ajpe76220
36. Kennerly J, Weber R. Role of pharmacy education in growing the pharmacy practice model. 48. Hosp Pharm. 2013;48(4):338–342. doi:10.1310/hpj4804-338
37. Harden RM, Laidlaw JM. Effective continuing education: the CRISIS criteria. Med Edu. 1992;26(5):407–422. doi:10.1111/j.1365-2923.1992.tb00194.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.