Back to Journals » Advances in Medical Education and Practice » Volume 17
Perceptions from a Single Virtual Near-Peer Mock SBA Examination: A Retrospective Pre–Post Study Among Undergraduate Medical Students
Authors Dalavaye N ![]() , Baskaran R
, Baskaran R ![]() , Ng VWS
, Ng VWS ![]() , Vyas R, Leveridge B, Hodgson M, Mukhopadhyay S
, Vyas R, Leveridge B, Hodgson M, Mukhopadhyay S ![]() , Peramuna Gamage M
, Peramuna Gamage M ![]() , Somani BK
, Somani BK ![]() , Hassoulas A
, Hassoulas A
Received 4 August 2025
Accepted for publication 10 December 2025
Published 20 January 2026 Volume 2026:17 558158
DOI https://doi.org/10.2147/AMEP.S558158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Nishaanth Dalavaye,1,* Ravanth Baskaran,2,* Vincent Wing Sum Ng,3 Rohan Vyas,4 Becky Leveridge,5 Megan Hodgson,6 Srinjay Mukhopadhyay,7 Movin Peramuna Gamage,8 Bhaskar Kumar Somani,2 Athanasios Hassoulas5
1Bolton NHS Foundation Trust, Bolton, UK; 2University Hospital Southampton NHS Foundation Trust, Southampton, UK; 3University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK; 4Royal Free NHS Foundation Trust, London, UK; 5School of Medicine, Cardiff University, Cardiff, UK; 6East Kent Hospitals University NHS Foundation, Kent, UK; 7London North West University Healthcare NHS Trust, London, UK; 8University Hospitals of North Midlands, Stoke-on-Trent, UK
*These authors contributed equally to this work
Correspondence: Athanasios Hassoulas, Email [email protected]
Background: Formative mock examinations are increasingly used to help medical students transition from theoretical learning to clinical application. Delivering such assessments through virtual near-peer formats may enhance accessibility and engagement, yet evidence remains limited regarding student perceptions and confidence outcomes.
Methods: A single live virtual near-peer mock single-best-answer (SBA) examination was conducted in March 2023 using an interactive polling platform. Senior medical students developed 30 SBA questions aligned with the UK Medical Licensing Assessment content map. Participants completed a post-session questionnaire containing retrospective pre- and post-ratings of confidence and anxiety, and items assessing perceived preparedness, question difficulty, time allocation, and platform usability. Data were analysed using the Wilcoxon signed-rank test and Pearson’s chi-squared test.
Results: A total of 198 students participated, with 82.8% from Cardiff University. Median self-reported confidence for sitting final examinations increased from 5 (IQR 4– 6) to 6 (IQR 4– 7) (p < 0.001), while anxiety remained unchanged at 8 (IQR 6– 9) (p = 0.054). Participants rated the mock as moderately beneficial for exam preparation (median 5 [IQR 4– 6]) and judged the 90-second question limit appropriate (median 8 [IQR 7– 10]). Most respondents (65.7%) preferred the live-polling platform for future mock assessments.
Conclusion: A single virtual near-peer mock SBA examination was feasible and well received, and was associated with a small but measurable gain in students’ self-reported confidence without a change in anxiety. These findings highlight the value of virtual near-peer formats as accessible formative tools within undergraduate medical education. However, the generalisability of results should be interpreted cautiously given the retrospective pre–post design and sampling concentration.
Keywords: formative assessment, near-peer teaching, live polling, medical finals preparation, student perceptions
Introduction
The pursuit of innovative pedagogical strategies remains an ongoing endeavour as medical educators strive to enhance learning experiences and outcomes.1 The journey from theoretical knowledge acquisition to clinical competence is a multifaceted and demanding process.2 Formative assessment has emerged as a key component of effective education, providing structured opportunities for feedback, encouraging continuous improvement, and fostering active engagement with learning materials.3–5 Through regular feedback and coaching, formative assessment promotes metacognitive awareness and supports the development of a growth mindset that fulfils lifelong professional learning.5
When applied consistently, formative assessments can enhance motivation and improve knowledge retention through repetition and retrieval practice.6–9 Testing itself functions as a learning tool that strengthens recall and facilitates the transfer of information into long-term memory.10,11 These assessments also encourage self-regulated learning behaviours, helping students identify weaknesses and integrate feedback into their study strategies.12–14 Within medical education, this process of feedback and reflection contributes to the development of lifelong learning habits and professional accountability.13
In recent years, advances in educational technology and the widespread disruption caused by the COVID-19 pandemic have reshaped how medical education is delivered. The rapid transition to online and hybrid formats required educators to maintain assessment quality while ensuring accessibility and inclusivity in virtual settings.15,16 This transformation aligns with the broader mission of universities across Europe to embed innovation and flexibility within their curricula, preparing graduates for evolving professional demands.17 For medical schools, this shift has driven the search for digital assessment models that preserve pedagogical integrity while expanding reach and scalability.
One approach that reflects these aims is near-peer teaching, in which senior students provide structured learning experiences for their junior peers. The method draws upon cognitive and social congruence, as tutors who recently mastered similar material can explain complex concepts in ways that are relatable and accessible.18,19 Near-peer teaching benefits both learners and tutors, enhancing knowledge consolidation, confidence, and communication skills while fostering collaboration and mutual support. When integrated into formative assessment, the near-peer approach combines realistic examination practice with feedback and reflection in a supportive learning environment.20–22
With the growing reliance on digital learning, near-peer teaching has expanded into virtual environments, leading to virtual mock examinations that simulate assessment conditions using interactive technologies such as live polling platforms.23–26 These sessions offer accessible opportunities for practice and immediate feedback, but they also pose challenges in maintaining engagement and replicating authentic exam conditions.27,28 While virtual near-peer formats have been used effectively in Objective Structured Clinical Examinations (OSCE) and anatomy teaching, limited evidence exists regarding their use in single-best-answer (SBA) examinations. The SBA format is central to undergraduate finals and forms a major component of the forthcoming United Kingdom Medical Licensing Assessment (UKMLA). Few studies have explored how students perceive the realism, difficulty, and psychological impact of virtual near-peer SBA assessments, or how these experiences influence confidence and preparedness for high-stakes examinations.
Understanding these perceptions is important for near-peer educators aiming to design formative assessments that are both pedagogically robust and technologically feasible. Insights into students’ views on timing, question difficulty, and platform usability can inform best practices for future implementation and help balance authenticity with accessibility. The present study therefore aimed to evaluate medical students’ perceptions of a single virtual near-peer mock SBA examination delivered through a live-polling platform. It examined self-reported changes in confidence and anxiety before and after the session, as well as perceptions of preparedness, question difficulty, and platform usability.
Materials and Methods
Study Design
This study employed a cross-sectional descriptive design to evaluate the perceptions of undergraduate medical students who participated in a virtual near-peer mock single-best-answer (SBA) examination. Data were collected using a single post-session questionnaire that included retrospective pre–post ratings of students’ confidence and anxiety toward their final examinations. Because these self-assessments were collected retrospectively within the same survey, the design is susceptible to response-shift and recall bias. Consequently, findings are interpreted strictly as self-reported perceptions rather than objective measures of performance or learning gain. The research adhered to the STROBE guidelines to ensure transparency and methodological rigour.29
Setting
The educational session, titled Virtual Finals Mock Exam, was conducted as a single 90-minute event in March 2023 via the Zoom™ videoconferencing platform. Question delivery and response collection were managed through Vevox®, a live-polling application that enabled synchronous participation. The session was hosted by one senior medical student (ND) acting as the near-peer tutor, supported by several co-tutors who moderated the chat and handled technical queries in real time. The format simulated a finals-style written SBA paper. Thirty SBA questions were displayed simultaneously on the Zoom™ screen and participants’ devices, each with a 90-second time limit for answering before poll closure. The ninety-second limit was selected to reflect common SBA pacing while maintaining engagement and session flow for a large virtual audience. Timing was manually enforced using a digital stopwatch—a fixed, host-controlled approach that differs from self-paced exam conditions. After all questions were completed, participants were shown anonymous aggregate response distributions, followed by a concise explanation phase in which each question and its correct answer were discussed.
Participants and Recruitment
Participation was open to all undergraduate medical students in the United Kingdom. The event was advertised publicly on OSCEazy’s social media channels, an international student-led teaching initiative.30 Although the session was accessible globally, only responses from students enrolled at UK medical schools were included in the analysis. A total of 198 medical students completed the post-session questionnaire and met the inclusion criteria. The largest subgroup comprised Year 5 students, and 82.8% of respondents were enrolled at Cardiff University. The session was scheduled in March, ahead of the end of the academic year when summative exams typically take place, to maximise its relevance and impact on students’ final preparations.
Question Development
The thirty SBA items were authored by senior medical students and mapped to the UKMLA content domains to ensure curricular relevance.31 Each item underwent internal peer review to confirm clarity, accuracy and appropriate difficulty before inclusion in the session. The complete text of all items, together with their correct options, is available in Supplementary Material 1. Interactive polling was used to present these questions as it has been demonstrated to be a valuable educational tool.32–34
Data Collection
Data collection was conducted through a single post-session questionnaire (Supplementary Material 2), distributed via the ZoomTM chat function. This questionnaire, comprising 10-point Likert-scale questions and single-item questions, was designed to evaluate participants’ perceptions of the teaching session. It assessed participant confidence and anxiety levels in preparation for final exams, both before and after the teaching session. It evaluated the perceived helpfulness of the examination in aiding exam readiness and alignment with typical exam questions. Preferences for examination format, engagement incentives, and platform suitability were explored. The responses were compiled into an Excel spreadsheet for data management. Given the exploratory nature of the study, formal sample size calculations were omitted, and extensive efforts were made to maximise participant recruitment for enhanced generalisability and statistical power.
Statistical Analysis
Survey data were exported to Microsoft Excel for preprocessing and analysed using Jamovi version 2.3.28. Descriptive statistics summarised the data as medians and interquartile ranges (IQRs). Given the non-normal distribution, Wilcoxon signed-rank tests were applied to paired retrospective pre- and post-ratings of confidence and anxiety. Effect sizes were calculated as rank-biserial correlations, with positive values indicating increased post-session ratings. 95% confidence intervals for effect sizes were not retained in the original analysis and are therefore not presented. Associations between categorical variables (for example, preferred number of questions and time per question) were tested using Pearson’s chi-square. Preferred item-count (eg, <30, 30, >30) and time-per-item (eg, <90s, 90s, >90s) categories were pre-specified for chi-square analysis. All analyses were exploratory, and no corrections for multiple comparisons were applied. Analyses used complete cases; no imputation was performed.
Ethical Considerations
Drawing guidance from the United Kingdom Health Research Authority’s online decision tool, the study concluded that formal ethics committee approval was not requisite. Participants provided informed consent, thereby granting permission for their anonymised data to be used in future publications. Participation was voluntary, with no compensation offered. The study strictly adhered to General Data Protection Regulation (GDPR) guidelines concerning secure data storage and privacy. The research involved no access or collection of private, personal or sensitive data, and participants accessed the ZoomTM meeting link without incurring any cost. No identifiable personal data were collected via the polling platform or survey.
Results
Participant Demographics
A total of 198 medical students completed the post-session questionnaire and were included in the analysis. The majority (n = 164; 82.8%) were enrolled at Cardiff University, with the remainder representing other UK medical schools (Table 1). Most respondents were in Year 5 (n = 75; 37.9). Demographic variables were self-reported, and no personally identifiable information was collected.
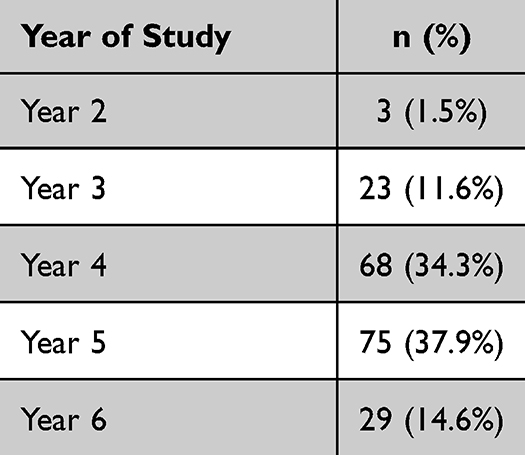 |
Table 1 Participants’ Distribution by Year of Study |
Confidence and Exam Preparedness
Following participation in the virtual mock examination, students reported a significant increase in self-rated confidence for sitting final examinations. The median confidence score rose from 5 (IQR 4–6) before the session to 6 (IQR 4–7) after the session (Wilcoxon signed-rank Z = −4.62, p < 0.001, rank-biserial r = +0.35), representing a small-to-moderate positive effect. In contrast, median anxiety scores remained unchanged at 8 (IQR 6–9) both before and after the session (Z = −1.93, p = 0.054, r = −0.20), indicating no significant change. Participants’ perception of overall preparedness for their final examinations following the session was moderate, with a median rating of 5 (IQR 4–6).
Question Difficulty and Time Allocation
Students perceived the difficulty of the SBA questions to be moderately aligned with that of their institutional final examinations, with a median rating of 7 (IQR 6–9). The 90-second response time per question was viewed as realistic and appropriate, with a median rating of 8 (IQR 7–10). Preferences regarding the number of questions and time allocation varied (Table 2). A little over half of the participants (n = 104; 52.5%) favoured the existing structure of 30 questions, each with 90 seconds. A smaller proportion (n = 25; 12.6%) preferred fewer questions with shorter time limits, while 22 (11.1%) favoured a longer examination with more questions and extended time per item. A statistically significant association was identified between the preferred number of questions and the preferred time per question (χ2 = 79.13, df = 4, p < 0.001), indicating a diversity of pacing preferences among students.
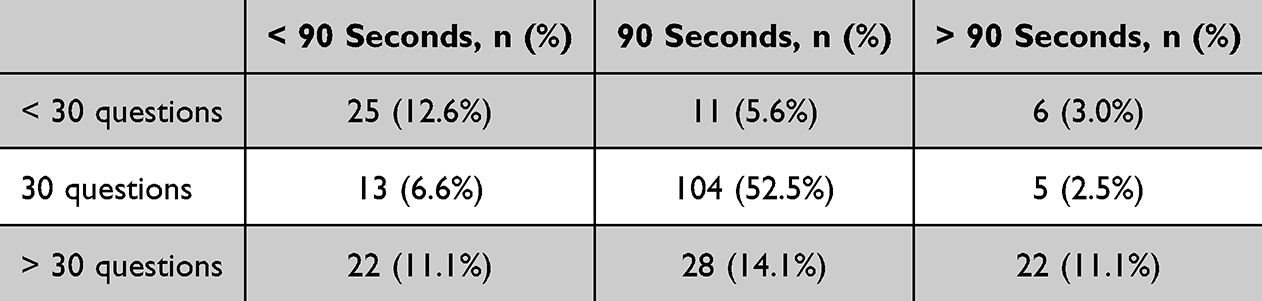 |
Table 2 Distribution of Ideal Number of Questions and Time per Question |
Examination Platform and Preferences
Participants rated the Vevox® polling platform highly for usability and effectiveness in delivering the virtual mock examination, with a median rating of 9 (IQR 8–10). When asked about preferred platforms for future mock examinations, 130 participants (65.7%) selected Vevox® as their first choice (Table 3). Opinions regarding competitive features were mixed: the presence of a leaderboard was rated as moderately motivating (median 7, IQR 5–9), whereas providing prizes for top performers was viewed less favourably (median 5, IQR 2–8).
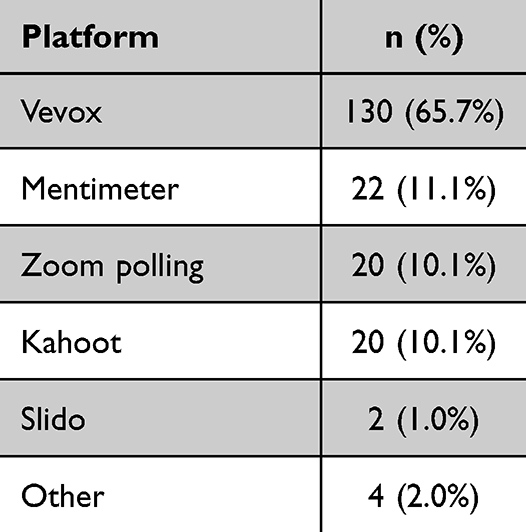 |
Table 3 Participants’ Preferences for Platform to Deliver a Virtual Mock Examination |
Discussion
This study explored students’ perceptions of a single virtual near-peer mock SBA examination delivered via live polling. Participants reported a modest increase in self-rated confidence for finals while anxiety remained unchanged, and they endorsed the general realism of item difficulty and a 30-item/90-second cadence. In line with recent shifts toward technology-enabled assessment precipitated by remote and hybrid learning, these findings suggest that virtual near-peer SBA sessions are a feasible and acceptable adjunct in medical education; however, they should be interpreted explicitly as perception-level outcomes rather than evidence of educational effectiveness or performance gains.35,36
The observed confidence gain is consistent with literature showing that formative assessment and near-peer learning can support preparedness by structuring practice, feedback, and reflection.3–7,18–22 Near-peer delivery likely leveraged social and cognitive congruence, enabling recently successful students to pitch explanations at an accessible level and frame questions in relatable ways.37–39 That anxiety did not change may reflect persistent, trait-like exam stress and the deliberately challenging item standard, which was intended to stimulate clinical reasoning rather than provide reassurance. From a psychological standpoint, an increase in confidence without heightened anxiety can still be seen as a favourable affective signal before high-stakes exams. The perceived benefit of the virtual mock examination for exam preparation aligns with the multifaceted nature of student resources, in which various pedagogical strategies contribute to holistic learning.40–42
A recurring theme is that immediate, specific feedback strengthens learning by correcting misconceptions while material is still salient.43,44 The post-item explanation segment here, which highlighted distractor rationale and pointing to further study, aligns with this principle and may have supported the confidence shift reported, even in the absence of measured performance outcomes. At the same time, the scope of formative benefit depends on question quality and breadth. Our 30-item blueprint prioritised core internal-medicine topics for inclusivity across schools, but this breadth-over-depth trade-off may have limited coverage of clinical reasoning nuances; future iterations could expand the item pool and include more red-flags/high-value items to increase practical salience.45–47
The 90-second time limit per item was selected as a pragmatic value based on the facilitators’ prior experience with similar assessments. While this duration was somewhat arbitrary, our collective experience suggested that it would allow most participants sufficient time to read, interpret, and respond to each single-best-answer question without feeling rushed, particularly in a large live session where timing uniformity was important. We recognise, however, that this approach departs from the authentic pacing of summative examinations, where students can allocate time strategically across items. This includes answering familiar questions rapidly to preserve time for those they find more challenging. By enforcing a fixed window, our design prioritised inclusivity and logistical synchrony over individual pacing autonomy. This trade-off likely influenced perceptions of difficulty and realism and represents an important consideration for future iterations of live virtual formative assessments.
Students perceived the 90-second limit as realistic, which is in keeping with typical SBA pacing and cognitive constraints on reading, comprehension, and decisional latency.9,48 Still, the host-controlled, fixed timing used to keep a large session synchronised diverges from authentic exam conditions where candidates self-allocate time across items. This ecological-validity limitation may attenuate transfer to real test-taking strategies and should be considered when interpreting perceptions of difficulty and time pressure. More broadly, timing and item count remain levers with pedagogical trade-offs: additional time risks overthinking, whereas tighter limits can suppress analytic processing; the optimal setting depends on whether the goal is coverage or depth of reasoning.9,47,48 An additional potential benefit of delivering the assessment live was that it created a more immersive and synchronous experience, more closely replicating the atmosphere of a summative examination than an asynchronous format would have achieved.
Technology played an enabling role by providing a simple, interactive platform that allowed hundreds of students to take part simultaneously. Participants rated the live polling format as easy to use and effective for engagement, which echoes findings from other studies using similar tools.32–34 These advantages are not necessarily unique to any one platform but relate instead to the principles of good design: accessibility, clarity and immediate feedback. While technology can make assessments scalable and inclusive, their educational value ultimately depends on the quality of the content and the guidance of facilitators.49 The session also encompassed core internal medicine specialities to ensure the relevance of content to all clinical year students.46
The mixed reactions to competitive features such as leaderboards and prizes highlight the complexity of student motivation. Some participants found competition motivating, while others were cautious about its potential to heighten stress or feelings of inadequacy. Previous studies have shown that visible rankings can encourage engagement but may also reinforce imposter feelings or excessive self-comparison.50–56 Keeping results anonymous, as was done here, may help reduce such effects. Evidence suggests that extrinsic incentives may shift attention away from learning and may even encourage dishonest behaviour.53 Thoughtful use of gamified elements can make assessments enjoyable, but these features should remain supportive rather than pressurising.
Several limitations should be acknowledged. The study relied on a single post-session survey using retrospective ratings, which is susceptible to recall and response bias. The sample was self-selected and mostly from one institution, so the findings may not represent the experiences of students elsewhere. The analysis was exploratory and based on perception data rather than objective outcomes, with no adjustment for multiple comparisons. The lack of substantial changes in anxiety levels towards final exams might also be influenced by broader stress sources, emphasising the importance of addressing stress management and wellbeing alongside examination interventions.57 SBAs mainly test factual knowledge and pattern recognition and have been criticised for their propensity for test-taking behaviours.58 Other formats such as very short answer questions could provide a more accurate assessment of applied understanding, though these are more resource-intensive to develop.59–61
Importantly, our study did not attempt to measure performance or knowledge gain, as its intent was to describe feasibility and self-reported perceptions in a large virtual cohort. Cross-checking self-reported improvements in performance with actual scores is useful, as studies indicate that medical students often have poor self-assessment skills; high-achieving students tend to underestimate their performance, while those struggling may overestimate theirs.62,63 Establishing a causal link between participation in virtual near-peer assessments and summative outcomes would require a different study design. Recent meta-analytic evidence from other educational technologies underscores why this distinction matters: for example, Bevizová et al reported that virtual-reality-based anatomy teaching produced a moderate pooled improvement in learning outcomes compared with lecture-based teaching, though results were highly heterogeneous and VR did not outperform physical models or clinical experience. This illustrates that while advanced technologies can yield measurable performance gains under specific conditions, such outcomes are not automatic.64 In contrast, the present study occupies an earlier point on that evidence continuum which is evaluating acceptability and feasibility of a scalable virtual near-peer SBA model rather than its effect on objective performance.
Future research could build on these findings by introducing pre-registered designs with baseline measures, comparator groups and repeated sessions over time. The inclusion of detailed qualitative feedback and exploration of confounding variables such as faculty familiarity with technology and perceptions from other polling platforms could enhance future studies. It would also be valuable to explore how such sessions affect wellbeing and engagement in the longer term, given the ongoing concerns about stress and burnout among medical students.54,55,57 Emerging tools such as large language models may eventually assist tutors in generating or analysing assessment content, but these technologies must be implemented responsibly and evaluated rigorously to ensure that educational integrity is maintained.65–69
Conclusion
This study found that a single virtual near-peer mock single best answer examination was well received by medical students and associated with a modest increase in self-reported confidence without a change in anxiety. The session was viewed as realistic, accessible and valuable for examination preparation, demonstrating the feasibility of virtual near-peer formative assessment. However, the findings reflect perceptions rather than objective measures of learning or performance and are limited by the single-institution sample and retrospective design. Future research should include comparator groups and links to summative outcomes to clarify the educational impact of virtual near-peer formats within undergraduate medical training.
Author Contributions
Nishaanth Dalavaye and Ravanth Baskaran are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boms O, Shi Z, Mallipeddi N, et al. Integrating innovation as a core objective in medical training. Nat Biotechnol. 2022;40(3):434–10. doi:10.1038/s41587-022-01253-x
2. Dong H, Lio J, Sherer R, Jiang I. Some learning theories for medical educators. Med Sci Educ. 2021;31(3):1157–1172. doi:10.1007/s40670-021-01270-6
3. Morris R, Perry T, Wardle L. Formative assessment and feedback for learning in higher education: a systematic review. Rev Educ. 2021;9(3):e3292. doi:10.1002/rev3.3292
4. Gedye S. Formative assessment and feedback: a review. Planet. 2010;23(1):40–45. doi:10.11120/plan.2010.00230040
5. Atkinson A, Watling CJ, Brand PLP. Feedback and coaching. Eur J Pediatr. 2022;181(2):441–446. doi:10.1007/s00431-021-04118-8
6. Evans DJR, Zeun P, Stanier RA. Motivating student learning using a formative assessment journey. J Anat. 2014;224(3):296–303. doi:10.1111/joa.12117
7. Ismail SM, Rahul DR, Patra I, Rezvani E. Formative vs. summative assessment: impacts on academic motivation, attitude toward learning, test anxiety, and self-regulation skill. Lang Test Asia. 2022;12(1):40. doi:10.1186/s40468-022-00191-4
8. Darling-Hammond L, Flook L, Cook-Harvey C, Barron B, Osher D. Implications for educational practice of the science of learning and development. Appl Develop Sci. 2020;24(2):97–140. doi:10.1080/10888691.2018.1537791
9. Yang BW, Razo J, Persky AM. Using Testing as a Learning Tool. Am J Pharm Educ. 2019;83(9):7324. doi:10.5688/ajpe7324
10. Dunlosky J, Rawson KA, Marsh EJ, Nathan MJ, Willingham DT. Improving students’ learning with effective learning techniques: promising directions from cognitive and educational psychology. Psychol Sci Public Interest. 2013;14(1):4–58. doi:10.1177/1529100612453266
11. Roediger HL, Karpicke JD. Test-enhanced learning: taking memory tests improves long-term retention. Psychol Sci. 2006;17(3):249–255. doi:10.1111/j.1467-9280.2006.01693.x
12. Schellekens LH, Bok HGJ, de Jong LH, van der Schaaf MF, Kremer WDJ, van der Vleuten CPM. A scoping review on the notions of Assessment as Learning (AaL), Assessment for Learning (AfL), and Assessment of Learning (AoL). Stud in Educ Eval. 2021;71:101094. doi:10.1016/j.stueduc.2021.101094
13. Hauer KE, Iverson N, Quach A, Yuan P, Kaner S, Boscardin C. Fostering medical students’ lifelong learning skills with a dashboard, coaching and learning planning. Perspect Med Educ. 2018;7(5):311–317. doi:10.1007/S40037-018-0449-2
14. Carless D. Feedback loops and the longer-term: towards feedback spirals. Assess Eval Higher Educ. 2019;44(5):705–714. doi:10.1080/02602938.2018.1531108
15. Chan EHY, Chan VHY, Roed J, Chen JY. Observed interactions, challenges, and opportunities in student-led, web-based near-peer teaching for medical students: interview study among peer learners and peer teachers. JMIR Med Educ. 2023;9:e40716–e40716. doi:10.2196/40716
16. Chan SCC, Choa G, Kelly J, Maru D, Rashid MA. Implementation of virtual OSCE in health professions education: a systematic review. Med Educ. 2023;57(9):833–843. doi:10.1111/medu.15089
17. Ostatníková D, Hopkins MA, Riles T, Robinson E, Hnilicová S. Universities and their educational mission in the 21st century: medical education innovations at Comenius university faculty of medicine. Bratisl Lek Listy. 2019;120(9):617–620. PMID:31475541. doi:10.4149/BLL_2019_101
18. Baskaran R, Mukhopadhyay S, Ganesananthan S, et al. Enhancing medical students` confidence and performance in integrated structured clinical examinations (ISCE) through a novel near-peer, mixed model approach during the COVID-19 pandemic. BMC Medical Educ. 2023;23(1):128. doi:10.1186/s12909-022-03970-y
19. Bowyer E, Shaw SK. Informal near-peer teaching in medical education: a scoping review. Educ Health. 2021;34(1):29. doi:10.4103/efh.EfH_20_18
20. Dalavaye N, Baskaran R, Mukhopadhyay S, et al. Exploring the educational value of popular culture in web-based medical education: pre-post study on teaching jaundice using “The Simpsons”. JMIR Med Educ. 2023;9(1):e44789. doi:10.2196/44789
21. Sioufi J, Hall B, Antel R. Near-peer tutoring: an effective adjunct for virtual anatomy learning. Can Med Educ J. 2023;14(3):119–121. doi:10.36834/cmej.75632
22. Sader J, Cerutti B, Meynard L, et al. The pedagogical value of near-peer feedback in online OSCEs. BMC Med Educ. 2022;22(1):572. doi:10.1186/s12909-022-03629-8
23. Calisi O, King S, Berger DJ, Nasir M, Nickolich S. Comparing the perceptions of reciprocal- and near-peer Objective Structured Clinical Examinations (OSCEs) in medical students. Cureus. 2023;15(2):e35535. doi:10.7759/cureus.35535
24. Chan J, Ang Jing Shi A, Chua D, Foo J, Tay SM. Benefits of a near-peer-led practice Objective Structured Clinical Examination (OSCE) in Teaching Physical Examination (PE) skills. 2020.
25. Grover S, Pandya M, Ranasinghe C, Ramji SP, Bola H, Raj S. Assessing the utility of virtual OSCE sessions as an educational tool: a national pilot study. BMC Med Educ. 2022;22(1):178. doi:10.1186/s12909-022-03248-3
26. Shah S. Evaluation of online near-peer teaching for penultimate-year objective structured clinical examinations in the COVID-19 era: longitudinal study. JMIR Med Educ. 2022;8(2):e37872–e37872. doi:10.2196/37872
27. Braier-Lorimer DA, Warren-Miell H. A peer-led mock OSCE improves student confidence for summative OSCE assessments in a traditional medical course. Med Teach. 2022;44(5):535–540. doi:10.1080/0142159X.2021.2004306
28. Hollister B, Nair P, Hill-Lindsay S, Chukoskie L. Engagement in online learning: student attitudes and behavior during COVID-19. Front Educ. 2022;7. doi:10.3389/feduc.2022.851019
29. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(5):31. doi:10.4103/sja.SJA_543_18
30. Mukhopadhyay S, Baskaran R, Peramuna Gamage M, et al. Assessing the publicity and reach of peer-led online medical teaching: a single-event evaluation. Adv Med Educ Pract. 2022;13:781–788. doi:10.2147/AMEP.S368218
31. General Medical Council [Internet]. MLA content map. 2019. Available from: gmc-uk.org/mla.
32. Bawazeer MA, Aamir S, Othman F, Alkahtani R. Students engagement using polls in virtual sessions of physiology, pathology, and pharmacology at King Saud bin Abdulaziz University for Health Sciences during COVID-19 pandemic: a cross-sectional study. BMC Med Educ. 2023;23:276. doi:10.1186/s12909-023-04253-w
33. Mayhew E, Davies M, Millmore A, Thompson L, Bizama AP. The impact of audience response platform mentimeter on the student and staff learning experience. Res Learn Technol. 2020;28.
34. Díez-Pascual AM, García Díaz MPG. Audience response software as a learning tool in university courses. Educ Sci. 2020;10(12):350. doi:10.3390/educsci10120350
35. Atwa H, Shehata MH, Al-Ansari A, et al. Online, face-to-face, or blended learning? Faculty and medical students’ perceptions during the COVID-19 pandemic: a mixed-method study. Front Med. 2022;9.
36. Barche A, Nayak V, Pandey A, Bhandarkar A, nayak SG, Nayak K. Student perceptions towards online learning in medical education during the COVID-19 pandemic: a mixed-methods study. F1000Res. 2022;11:979. doi:10.12688/f1000research.123582.1
37. Lockspeiser TM, O’Sullivan P, Teherani A, Muller J. Understanding the experience of being taught by peers: the value of social and cognitive congruence. Adv Health Sci Educ. 2008;13(3):361–372. doi:10.1007/s10459-006-9049-8
38. Loda T, Erschens R, Loenneker H, et al. Cognitive and social congruence in peer-assisted learning – a scoping review. PLoS One. 2019;14(9):e0222224–e0222224. doi:10.1371/journal.pone.0222224
39. Loda T, Erschens R, Nikendei C, et al. A novel instrument of cognitive and social congruence within peer-assisted learning in medical training: construction of a questionnaire by factor analyses. BMC Med Educ. 2020;20(1):214. doi:10.1186/s12909-020-02129-x
40. Bauzon J, Alver A, Ravikumar V, et al. The impact of educational resources and perceived preparedness on medical education performance. Med Sci Educator. 2021;31(4):1319–1326. doi:10.1007/s40670-021-01306-x
41. Finn E, Ayres F, Goldberg S, Hortsch M. Brave new E‐world: medical students’ preferences for and usage of electronic learning resources during two different phases of their education. FASEB BioAdv. 2022;4(5):298–308. doi:10.1096/fba.2021-00124
42. Wynter L, Burgess A, Kalman E, Heron JE, Bleasel J. Medical students: what educational resources are they using? BMC Med Educ. 2019;19(1):36. doi:10.1186/s12909-019-1462-9
43. Badyal DK, Bala S, Singh T, Gulrez G. Impact of immediate feedback on the learning of medical students in pharmacology. J Adv Med Educ Prof. 2019;7(1):1–6. doi:10.30476/JAMP.2019.41036
44. Dihoff RE, Brosvic GM, Epstein ML. The role of feedback during academic testing: the delay retention effect revisited. Psychol Rec. 2003;53(4):533–548. doi:10.1007/BF03395451
45. Devine OP, Harborne AC, McManus IC. Assessment at UK medical schools varies substantially in volume, type and intensity and correlates with postgraduate attainment. BMC Med Educ. 2015;15(1):146. doi:10.1186/s12909-015-0428-9
46. Devine OP, Harborne AC, Horsfall HL, et al. The Analysis of Teaching of Medical Schools (AToMS) survey: an analysis of 47,258 timetabled teaching events in 25 UK medical schools relating to timing, duration, teaching formats, teaching content, and problem-based learning. BMC Med. 2020;18(1):126. doi:10.1186/s12916-020-01571-4
47. Rush BR, Rankin DC, White BJ. The impact of item-writing flaws and item complexity on examination item difficulty and discrimination value. BMC Med Educ. 2016;16:250. doi:10.1186/s12909-016-0773-3
48. Kyllonen PC, Zu J. Use of response time for measuring cognitive ability. J Intell. 2016;4(4):14. doi:10.3390/jintelligence4040014
49. Regmi K, Jones L. A systematic review of the factors – enablers and barriers – affecting e-learning in health sciences education. BMC Med Educ. 2020;20(1):91. doi:10.1186/s12909-020-02007-6
50. Corell A, Regueras LM, Verdú E, Verdú MJ, de Castro JP. Effects of competitive learning tools on medical students: a case study. PLoS One. 2018;13(3):e0194096. doi:10.1371/journal.pone.0194096
51. Chodoff A, Conyers L, Wright S, Levine R. “I never should have been a doctor”: a qualitative study of imposter phenomenon among internal medicine residents. BMC Med Educ. 2023;23(1):57. doi:10.1186/s12909-022-03982-8
52. Khan M. Imposter syndrome—a particular problem for medical students. BMJ. 2021;375:n3048. doi:10.1136/bmj.n3048
53. Kirsch J, Spreckelsen C. Caution with competitive gamification in medical education: unexpected results of a randomised cross-over study. BMC Med Educ. 2023;23(1):259. doi:10.1186/s12909-023-04258-5
54. Bergmann C, Muth T, Loerbroks A. Medical students’ perceptions of stress due to academic studies and its interrelationships with other domains of life: a qualitative study. Med Educ Online. 2019;24(1):1603526. doi:10.1080/10872981.2019.1603526
55. Voltmer E, Köslich-Strumann S, Voltmer JB, Kötter T. Stress and behavior patterns throughout medical education – a six year longitudinal study. BMC Med Educ. 2021;21(1):454. doi:10.1186/s12909-021-02862-x
56. Kaushik M, Singh V, Chakravarty S. Experimental evidence of the effect of financial incentives and detection on dishonesty. Sci Rep. 2022;12:2680. doi:10.1038/s41598-022-06072-3
57. Rich A, Viney R, Silkens M, Griffin A, Medisauskaite A. UK medical students’ mental health during the COVID-19 pandemic: a qualitative interview study. BMJ Open. 2023;13(4):e070528. doi:10.1136/bmjopen-2022-070528
58. Kilgour JM, Tayyaba S. An investigation into the optimal number of distractors in single-best answer exams. Adv Health Sci Educ. 2016;21(3):571–585. doi:10.1007/s10459-015-9652-7
59. Sam AH, Westacott R, Gurnell M, Wilson R, Meeran K, Brown C. Comparing single-best-answer and very-short-answer questions for the assessment of applied medical knowledge in 20 UK medical schools: cross-sectional study. BMJ Open. 2019;9(9):e032550–e032550. doi:10.1136/bmjopen-2019-032550
60. Bala L, Westacott RJ, Brown C, Sam AH. Twelve tips for introducing very short answer questions (VSAQs) into your medical curriculum. Med Teach. 2023;45(4):360–367. doi:10.1080/0142159X.2022.2093706
61. Sam AH, Millar KR, Westacott R, Melville CR, Brown CA. Standard setting Very Short Answer Questions (VSAQs) relative to Single Best Answer Questions (SBAQs): does having access to the answers make a difference? BMC Med Educ. 2022;22(1):640. doi:10.1186/s12909-022-03693-0
62. Urrizola A, Santiago R, Gea A, et al. What medical students with better academic results do: a cross-sectional analysis. BMC Med Educ. 2023;23(1):19. doi:10.1186/s12909-023-03999-7
63. Park KH, Kam BS, Yune SJ, Lee SY, Im SJ. Changes in self-reflective thinking level in writing and educational needs of medical students: a longitudinal study. PLoS One. 2022;17(1):e0262250. doi:10.1371/journal.pone.0262250
64. Bevizová K, Falougy HE, Thurzo A, et al. Is virtual reality enhancing dental anatomy education? A systematic review and meta-analysis. BMC Med Educ. 2024;24:1395. doi:10.1186/s12909-024-06233-0
65. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. doi:10.1371/journal.pdig.0000198
66. Totlis T, Natsis K, Filos D, et al. The potential role of ChatGPT and artificial intelligence in anatomy education: a conversation with ChatGPT. Surg Radiol Anat. 2023;45(10):1321–1329. doi:10.1007/s00276-023-03229-1
67. Khan RA, Jawaid M, Khan AR, Sajjad M. ChatGPT - reshaping medical education and clinical management. Pak J Med Sci. 2023;39(2):605–607. doi:10.12669/pjms.39.2.7653
68. Safranek CW, Sidamon-Eristoff AE, Gilson A, Chartash D. The role of large language models in medical education: applications and implications. JMIR Med Educ. 2023;9(1):e50945. doi:10.2196/50945
69. Yang D, Wang H, Metwally AHS, Huang R. Student engagement during emergency remote teaching: a scoping review. Smart Learn Environ. 2023;10(1):24. doi:10.1186/s40561-023-00240-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.