Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Perceptions and Expectations of Advanced Geriatric Nursing Role Development in Primary Health Care: A Qualitative Study Exploring Staff’s Perspectives
Authors Li Y ![]() , Chen M, Lin R, Li H
, Chen M, Lin R, Li H
Received 9 October 2021
Accepted for publication 14 December 2021
Published 30 December 2021 Volume 2021:14 Pages 3607—3619
DOI https://doi.org/10.2147/JMDH.S343622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yulian Li,1 Meirong Chen,2 Rong Lin,1,3 Hong Li1,3
1The School of Nursing, Fujian Medical University, Fuzhou City, Fujian Province, People’s Republic of China; 2Department of Nursing, Fujian Provincial Hospital, Fuzhou City, Fujian Province, People’s Republic of China; 3Research Center for Nursing Theory and Practice, Fujian Provincial Hospital, Fuzhou City, Fujian Province, People’s Republic of China
Correspondence: Hong Li Tel +86 13705070219
Fax +86 591-87532356
Email [email protected]
Purpose: This qualitative study aimed to explore multidisciplinary members’ perceptions and expectations of advanced geriatric nursing role development in primary health care.
Patients and Methods: A multi-center, cross-sectional study based on semi-structured individual interviews was conducted with registered nurses, general physicians, and managers involved in the care of older people in primary health care between September 2020 and January 2021. Recruitment was purposive and the framework method was used to inductively analyze the data. The Consolidated Criteria for Reporting Qualitative research (COREQ) served to structure our manuscript.
Results: In total, 29 registered nurses, 6 general physicians, and 10 managers from 8 health centers were interviewed. The relevant themes interpreted from the interview data were as follows: (1) the current roles of registered nurses in the care of older people; (2) the factors affect the advanced geriatric nursing role development; (3) expectations of the advanced geriatric nursing roles.
Conclusion: There is a need for appropriate educational programs, well-established laws, and regulations to support the sustainable development of advanced geriatric nursing roles. To build the expected role model, the nursing education program in the future should integrate gerontological nursing, public health nursing, and nursing management to maximize the role of gerontological nurse practitioners in primary health care.
Keywords: advanced nurse practitioner, older people, primary care, qualitative approaches
Introduction
The consequences of the growing aging population have become a worldwide phenomenon, and the pace is particularly fast in China. In 2019, older adults made up 18.1% of the Chinese population, and this proportion is projected to peak by 2058.1,2 Since the prevalence of frailty, multi-morbidity, and disability increases with age, the number of older adults living at home with complex primary healthcare needs, multiple comorbid health problems, and polypharmacy is growing.3 The World Health Organization (WHO) emphasizes how critical it is to develop a person-centered integrated care system that has primary care as a central element to achieve Healthy Aging.4,5 The Chinese government has introduced a series of policies to build a Three-Tiered Aged Care System that is “home-based, community-supported, institutional-supplemented old-age care system, and integrated with medical care system”, which aims to integrate existing medical care and long-term care resources across care settings and providers to meet both the health care and long-term care needs of older people.6 However, the ability of the integrated care system to meet the expanding need for older people will be limited by the ongoing shortage of proficient medical and nursing staff specialized in geriatric care.
Preview studies from the United States, Australia, and other countries reported that considerable physician/nursing staff shortages exist in primary health care settings due to the retirement of older professionals, lack of clear career pathways, few professional development opportunities, and inconsistent role definition.7–9 In China, primary health care is also facing the challenge of inadequate physicians because of high turnover intention and poor training.10 Demand scale of nursing staff specializing in geriatric care in China is projected to reach 0.56 million in 2025.11 However, according to the report of “ China Civil Affairs Statistical Yearbook 2017 ”, the number of the certified nursing staff was less than 20 thousand in 2016, which indicated that there would be a massive gap in China’s nursing staff in the future. Additionally, the shortage of nurses/physicians has been proved to be associated with adverse effects on fragmented care, increased hospital admission rates, and increased health care costs.12,13 Therefore, exploring effective ways to maximize the utilization of professionals and re-conceptualize roles and responsibilities of all health care professionals, including the registered nurse (RN), are optimized in the reimagined integrated care model.
Many countries have taken strategies to introduce Advanced Practice Nurse (APN) to alleviate shortages of staff, decrease health care costs, and respond to the increasing aging population in primary health care.14–16 The gerontological nurse practitioner (GNP) role was developed in the United States in 1975, which also has been introduced recently by Australia, Israel, Norway, and other countries, to meet the needs of the health systems in providing general services to older adults and their family members.17–22 The development has led to a situation where GNPs’ educational requirements and scope of work vary greatly across countries. Nevertheless, in most countries, APN specializing in the care of older adults have been introduced as follows: they are registered nurses (RNs) with additional education and training, who have professional autonomy, advanced knowledge, and skills to apply a variety of health promotion activities such as disease prevention, health education and counseling into nursing in acute and primary care settings, and implement effective care for older adults utilizes evidence-based practice to achieve quality outcomes.23 Additionally, preview studies have demonstrated that APN with a substitute or supplemental role to physicians in multiple settings generate better health outcomes for a broad range of older people conditions, and improve the satisfaction of both older people and health care providers.24–26 Wherefore, the implementation of APN has been a new model to promote integrated care coordination for older people with complex needs in primary healthcare.
The advanced nursing practice did not emerge in China until the early 2000s. In particular, the gerontological nurse specialist (GNS) has been recently introduced in 2005 by China.27 The roles of the GNS are usually categorized into different types based on chronic disease, generally in hospitals to guide geriatric practices. However, the role of the GNS has not been extended to primary health care, such as community or long-term care facilities. RNs are key performers in the care of older people in various primary healthcare settings, however, are commonly characterized by low levels of education, poor professional quality, and high turnover rates.28 Several studies reported that the nursing staff working with older people was of low social status and did not require specialized knowledge or skills.29 While the Chinese government and nursing associations have taken action to promote the development of NPs to address the above issues for RNs in the primary health care system, the GNP roles are not well established. There are no regulations, central frameworks, or guidelines to guide the development of GNP roles. Hence, exploring appropriate ways to support the development of GNP roles in the context of China, are a necessary process to expand the role of RNs and improve the integrated care within primary health care.
We conducted this qualitative study to explore multidisciplinary members’ perceptions on the role of RNs in the care of older people, to investigate the factors affecting the development of advanced geriatric nursing roles in primary health care, and to identify multidisciplinary members’ expectations of the role of GNP in the future. Preview studies have identified several barriers and facilitators to role development for APNs and highlighted a clear definition of the specific features of the role as a crucial determinant for successful interprofessional collaboration when implementing these roles into practice.30 However, there is a lack of clarity about how RNs and other staff perceive their work with older people, and the literature is missing recently professional providers’ perceptions on the development of GNP role in the context of China. Their perceptions can provide insights into the areas of deficiency in ways that nursing educators and policy makers cannot as they can perceive the nursing role and nursing practice environment in the care of older people within primary health care. Thus, this study was designed to provide information about a gap in the literature related to providers’ perceptions about what is needed to enhance RNs’ role in the care of older people and to guide development related to advanced geriatric nursing roles and gerontological nursing education in developing countries.
Materials and Methods
Study Design
A qualitative, descriptive, and exploratory approach was adopted. We carried out a multi-center, cross-sectional study based on face-to-face interviews with professionals and managers involved in geriatric care in the primary healthcare system. The Consolidated Criteria for Reporting Qualitative research (COREQ) served to structure our manuscript.
Research Team
Our research team consisted of senior researchers and Ph.D. students in nursing. The interview was conducted by a Ph.D. student who was trained in qualitative interviewing. Before the interview, the Ph.D. student was fully familiar with the working environment of the participants and had established a good relationship with them. All researchers directly involved in data collection and analysis are well-experienced in qualitative interviewing and/or thematic analysis.
Recruitment and Participants
The senior managers of the participating health centers were contacted by email in September 2020. They were informed of the purpose of the study and the inclusion criteria and agreed to participate. Shortly after, the first author contacted potential participants to confirm voluntary participation, give further information on the study, and set a date for the interview. RNs, general physicians (GPs), and managers from the primary healthcare system were targeted as participants for this study due to their collaborative responsibility for the care of older adults. Participants fulfilled the following inclusion criteria: (a) had to work in primary health care for more than one year; (b) had to have expertise and experience in primary geriatric care; (c) were willing to talk about their experiences. Purposeful strategies and maximum variation based on differences in organizational levels such as staff, head nurses, matron, and supervisors as well as different experience levels, were used to recruit participants. The sample size itself was dependent upon reaching data saturation in the themes that emerged during data analysis.
Data Collection
A pilot study was conducted in a health center providing a similar contextual setting as the current study to test the data collection methods. Experiences and findings from the pilot study resulted in a more detailed interview guide. No data from the pilot study were used in the current study.
The data were collected from September 2020 until January 2021, through in-depth semi-structured interviews using an interview guide. The interviews were conducted by the same researcher in a quiet room and were audio-recorded and transcribed verbatim. Additionally, the transcripts were returned to participants for comment. The duration of interviews was between 20–55 min. During the interviews, participants were encouraged to freely share their views on the attitudes, factors, and exceptions regarding the development of GNPs in primary health care. An interview guide was developed after reviewing the research literature on the development of GNPs’ role in primary health care. The interview guide in Table 1 was used to structure the interviews.
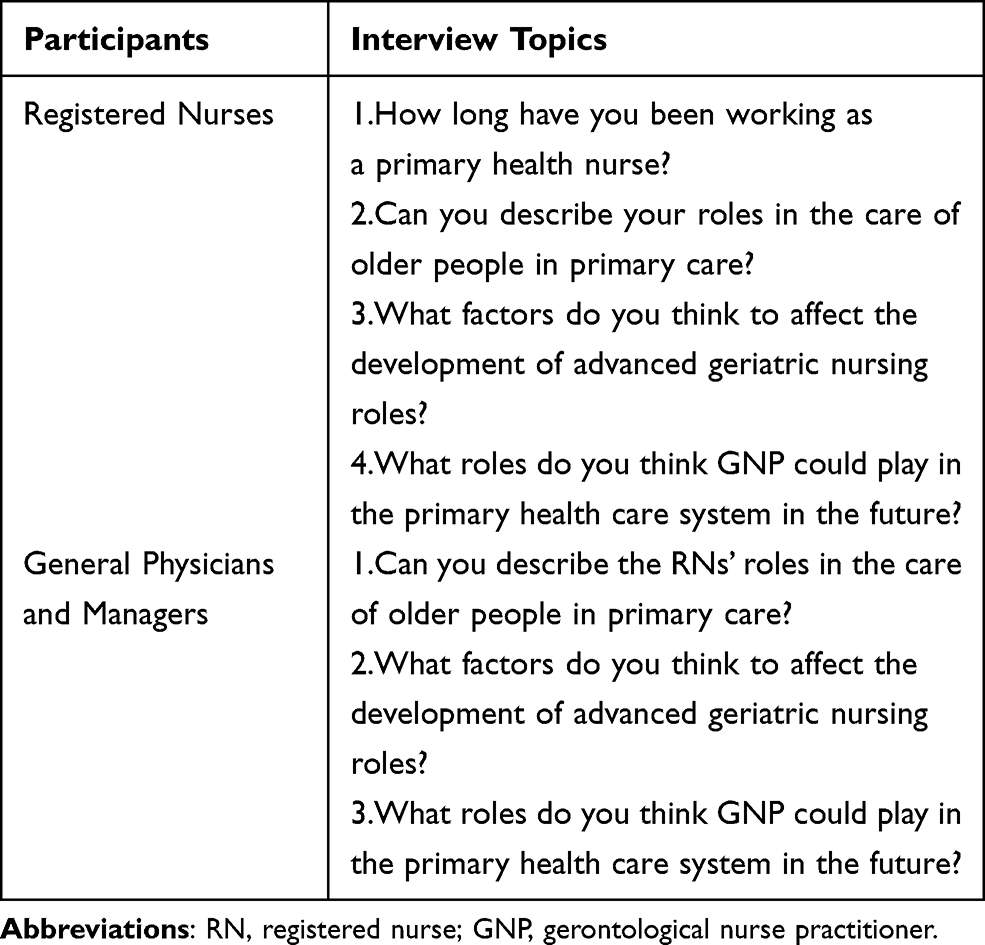 |
Table 1 Interview Guide |
The participant information sheet was also provided to collect detailed information on the participants. Participants were asked to sign the consent form and complete an initial demographic survey to collect data on age, sex, highest degree attained, and years of primary health practice.
Data Analysis
An inductive content analysis approach was used to analyze the data. Content analysis is a systematic coding and categorizing approach used for unobtrusively exploring large amounts of textual information to determine trends and patterns of words used, their frequency, their relationships, and the structures and discourses of communication.31 Inductive content analysis was conducted in this study because there have been insufficient studies dealing with this phenomenon, and therefore the coded categories are derived directly from the text data.
NVivo 11 was used to code and organize the data. All audiotaped interviews were transcribed verbatim in the initial data analysis.32 Next, the study team read through all the transcripts several times to obtain a sense of the overall data. Initial open coding was done, which was then developed into various categories. Key concepts and phrases that arose in the transcripts were manually highlighted, extracted, and collated to generate the codes and subthemes. As the process continued, labels for codes emerged as they were grouped into final categorical themes. The process of data collection and analysis was concurrent until the analysis yielded varying perceptions, and there were no new themes emerging, at which point data saturation was assumed to be achieved.33
Ethical Considerations
This study was approved by the Ethics and Research Committee of Fujian Province Hospital and was validated by each of the participating centers. Data confidentiality was guaranteed by assigning a code to each participant that only the study researchers had access to. Before each interview, the researchers explained the purpose, process, and requirements of the study to the participants. The researchers also assured the participants of the voluntary nature of the study and their rights to discontinue the study at any given time. All participants provided written informed consent and agreed that their anonymous data may be used for publication.
Rigor
Credibility, dependability, confirmability, and transferability are the most common measures necessary to achieve rigor in qualitative studies.34 Several techniques were used to ensure data validity and rigor in this study. First, data coding was conducted simultaneously by two team members to maintain dependability.35 In cases of disagreement about key themes during the coding and analysis process, the team discussed the issue until reaching a consensus. If no consensus was reached, the principal investigator’s decision prevailed. Credibility was maintained by debriefing participants on the study findings and asking them if these were or were not consistent with their views and opinions. In addition, field notes were taken during the interview to enhance self‐awareness and ongoing reflection of the interaction process with the participants.36 Transferability was achieved by analyzing the experiences of the different participants working in the eight primary care centers in China. Sufficient information (based on a China context) was provided to highlight identical contextual details and attain a high level of transferability. Confirmability can be attained by achieving good credibility, transferability, and dependability in the experimental process.34
Results
Participants’ Characteristics
Table 2 summarizes the participant’s demographic characteristics. There were 29 RNs from four urban community health centers and four township health centers, six GPs, and 10 managers. Most participants were female, between 25 and 46 years old. Most participants also had more than two years of experience in geriatric nursing practice and had graduated with a college degree (82%).
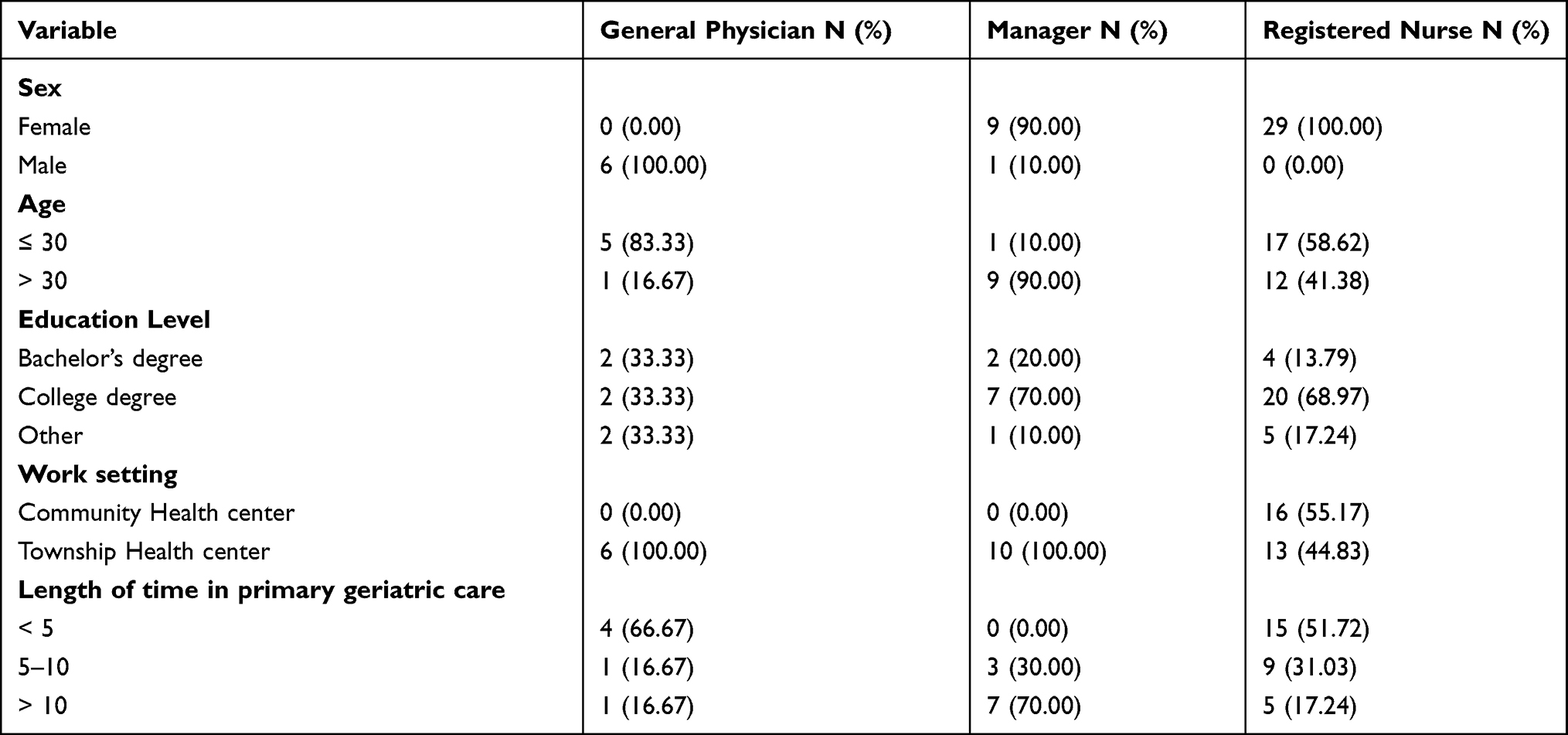 |
Table 2 Sociodemographic Characteristics of Participants |
Three core themes were identified in the data: current roles of RNs in the care of older people; factors that affect the advanced geriatric nursing role development; and expectations of the GNPs’ roles in primary health care. The themes, subthemes, and sample quotes are presented in Table 3.
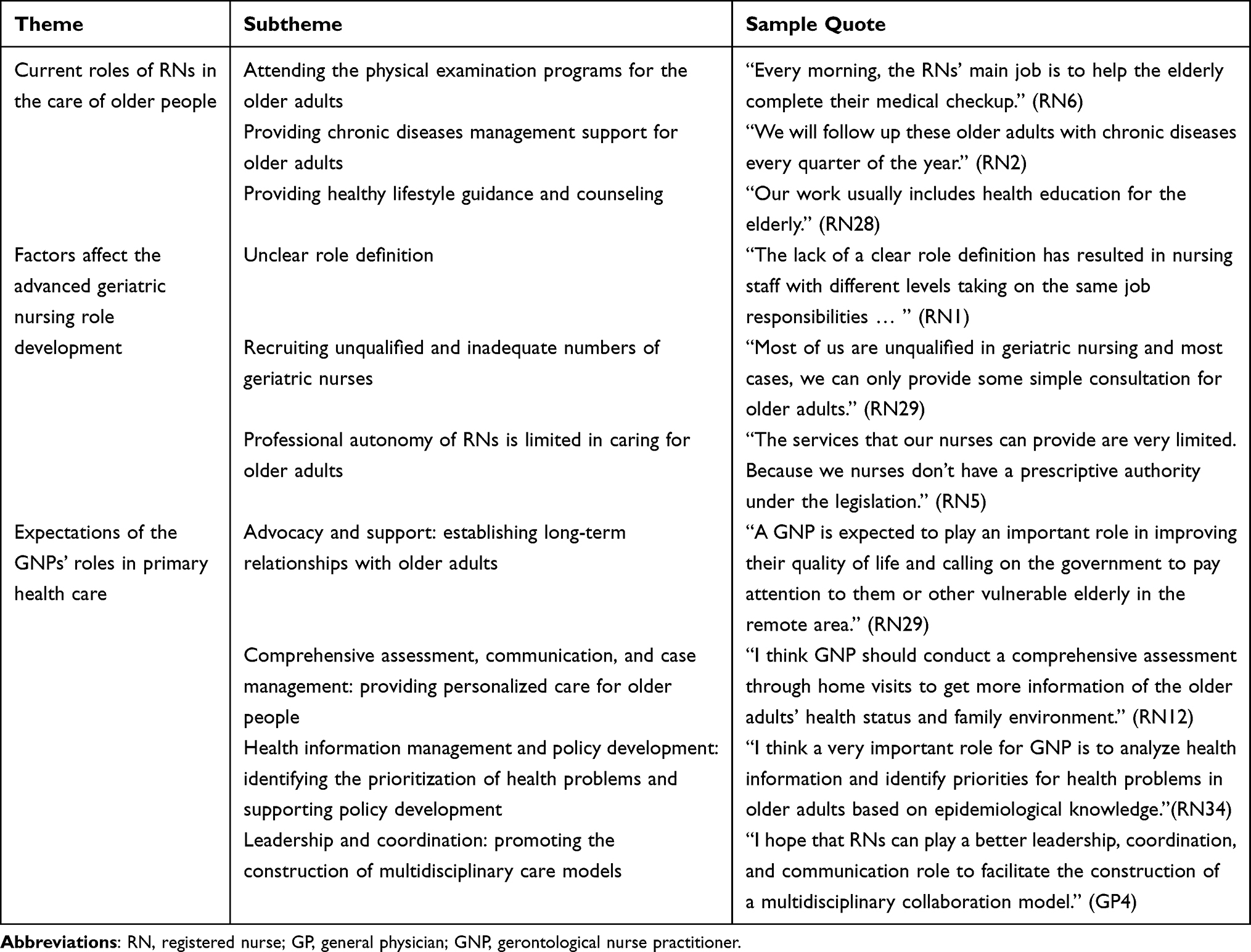 |
Table 3 The Themes, Subthemes, and Sample Quotes |
Current Roles of RNs in the Care of Older People
Even though the Three-tier Aged Care Model has been initially developed, there is no well-developed framework to guide RNs’ work in primary health care. When exploring the current roles of RNs in the care of older people, the results are all related to performing the Basic Public Health Services (BPHS). As the main executors of BPHS, RNs mainly participate in the health checkup, the management of chronic diseases, and health education for older adults. The examples provided by the participants illustrate the role of RNs in elderly care within the primary healthcare system mainly focusing on public health nursing activities that the organization requires of them.
Attending the Physical Examination Programs for the Older Adults
The annual free physical check-up is one of the BPHS offered for older adults in China. Usually, both the RNs from urban community health centers and township health centers play a key role in informing and guiding the elderly to complete all check-up items. As described by one RN:
Every morning, the RNs’ main job is to help the elderly complete their medical checkups. We take blood pressure, electrocardiogram, height and weight, and questionnaires on Chinese medicine for the elderly. Then in the afternoon, we record the report, file entry. (RN6, urban, community health center)
Providing Chronic Diseases Management Support for Older Adults
Across the three groups, there was a view that it is a major responsibility for RNs to provide support for the elderly in chronic disease management. In particular RNs aid in managing hypertension and diabetes, which are supported by the Public Health Fund. As one RN described:
We will follow up these older adults with chronic diseases every quarter of the year. If they are not satisfied with diabetes control, health centers will provide free blood glucose measurement service once a quarter. (RN2, urban, community health center)
Providing Healthy Lifestyle Guidance and Counseling
When RNs, physicians, and managers described the daily work in the care of older people, the key words were always related to health education. The RNs provide health knowledge and lifestyle guidance for the elderly through different means, to promote the prevention of chronic diseases.
Our work usually includes health education for the elderly. For example, we need to prevent him from falling. Additionally, we need to make elderly people who are prone to itching pay attention to hygiene during the season change … there are also long-term bedridden patients in their own homes. We also need to provide education and guidance on personal care skills. (RN28, rural, township health center)
Factors Affect the Advanced Geriatric Nursing Role Development
Unclear Role Definition
Although RNs play important roles in chronic diseases management and health promotion as one of the multidisciplinary team, their specific roles and activities are not well defined due to there being no full-time position for RNs working with older people within the primary healthcare system. Most of the RNs are part-time general nurses and usually need to attend to additional nursing practice for other specific populations, such as women and children.
There is no such a full-time position for us to provide services for older adults. Most of us are general nurses and have not graduated from gerontology nursing education program. (RN27, rural, township health center)
Moreover, in the absence of well-defined job descriptions, the RNs’ role providing care for older adults lacked clarity, as all RNs were considered as a homogeneous group regardless of individual education, skills, or clinical experience. As one RN complained:
It has nothing to do with our major within multidisciplinary team … Because we are often spent a lot of time collating information on health checkups for the elderly, which leads to the feeling that the professional knowledge we have learned is not useful. (RN6, urban, community health center)
Furthermore, unclear role definition also resulted in unclear career pathways, which is a key factor affecting the advanced nursing role development. One RN suggested that managers should provide different professional role development opportunities based on the education and competency levels of each individual.
The lack of a clear role definition has resulted in nursing staff with different levels taking on the same job responsibilities, which has had a significant impact on our career development. In my opinion, an RN with a bachelor’s degree should get more opportunities to develop advanced geriatric nursing roles. (RN1, urban, community health center)
Recruiting Unqualified and Inadequate Numbers of Geriatric Nurses
When reflecting on the factor that affects advanced role development, RNs, GPs, and managers all reported that the lack of geriatrically-trained RNs is an obstacle to the provision of high-quality aged-care services in primary healthcare. These findings indicated that RNs in caring for older adults have relatively low academic qualifications and lack knowledge and competence.
“Most of us are unqualified in geriatric nursing and in most cases, we can only provide some simple consultation for older adults.” (RN29, rural, township health center)
Additionally, challenges in recruiting competent staff were mentioned, especially in rural areas.
We are in short supply of nursing staff in the primary healthcare system. The nursing staff we can recruit now are all graduates from technical secondary schools, which has seriously affected the development of the advanced geriatric nursing roles. (GP2, rural, township health center)
Some GPs expressed the view that the lack of professional nurses is related to the absence of appropriate educational programs. Some physicians and managers emphasized the integration of geriatric nursing into nursing education to ensure that there is ongoing qualified RNs preparation.
Geriatric nursing education should be integrated into undergraduate education under regular and policy so that they can start training from school and graduate with the appropriate competencies. (M10)
The pre-graduation training program should be developed to start nurse students’ learning about how to be a professional nurse before they left school. Participating in home visits and other nursing activities in the care of older adults in their third year of undergraduate study is conducive to nursing students’ adaptation to their jobs following graduation. (GP3, rural, township health center)
Professional Autonomy of RNs is Limited in Caring for Older Adults
Professional autonomy is defined
as the practice of one’s occupation by one’s education, with members of that occupation governing, defining and controlling their activities in the absence of external control.
Most of the respondents stated that the professional autonomy of RNs is limited in primary healthcare under China legislation. As one RN described:
The services that our nurses can provide are very limited. Because we nurses don’t have a prescriptive authority under the legislation. In addition, there is no such a professional nursing body to guide geriatric nursing practice in primary health care. (RN5, urban, community health center)
When exploring the possibility of the development of advanced geriatric nursing roles, the managers recognized that it is necessary to develop laws and regulations to guide the geriatric nursing practice in primary health care.
If the advanced geriatric nursing role is to be developed, sufficient laws and regulations are required to ensure that RNs can work independently. Obviously, it is still imperfect at this stage … (M1, urban, Government Pension Service)
Expectations of the GNPs’ Roles in Primary Health Care
Participants identifying themselves as members of a multidisciplinary team which included RNs were asked to identify what they thought were the key aspects of the advanced geriatric nursing roles in primary healthcare. The responses of participants were coded to minor categories from which four main categories were derived – “support and advocacy”, “comprehensive assessment, communication and case management”, “health information management and policy development”, and “leadership and coordination”. Figure 1 presents participants’ expectations of the role of GNP in the primary health care system.
 |
Figure 1 Expected role model of gerontological nurse practitioners (GNPs) in primary health care. |
Advocacy and Support: Establishing Long-Term Relationships with Older Adults
The provision of advocacy and support to older adults and their families were considered to be important aspects of the GNPs’ roles in primary health care. Participants considered that the GNP is the one who has more time to spend with the older adults and is able to develop a close and long-term relationship with older adults. The role of GNP as an advocate for the “empty-nest” older adults within a multidisciplinary team was highlighted by several participants with examples provided.
Most empty-nest elderly are unable to live independently and lack care support from their family. Therefore, a GNP is expected to play an important role in improving their quality of life and calling on the government to pay attention to them or other vulnerable elderly in the remote area. (RN29, rural, township health center)
Due to children being away from home for study or work, “empty-nest” elderly lack opportunities for face-to-face communication with their children, which weakens the emotional family bond. Respondents reported that GNP should play the role of supporters and establish friendly relationships with the elderly through listening and communication to alleviate the loneliness and depression of the older adults.
For GNP, it is necessary to provide psychological counseling for older adults. GNP can establish a long-term relationship with older adults and as an alternative role for their children to ease their loneliness. (RN36, rural, township health center)
Comprehensive Assessment, Communication, and Case Management: Providing Personalized Care for Older People
The processes of assessment and case management are considered to be among the GNPs’ responsibilities identified by participants. The GNP is expected to be responsible for utilizing case-finding to target at-risk older people by conducting a comprehensive assessment. Case management was also identified by participants as a key aspect of the GNP role with participant examples provided:
I think GNP should conduct a comprehensive assessment through home visits to get more information of the older adults’ health status and family environment. Only then can we detect the elderly at high risk in time, and intervene early. (RN12, urban, community health center)
Case management is also a very important aspect of the role of GNPs. It is necessary to develop a personalized health care plan based on elderly persons’ medical, psychosocial and functional capabilities. Also, health education is very important. After all, the improvement of chronic diseases requires long-term medication and lifestyle changes. (GP3, rural, township health center)
A GNP is expected to acquire not only technical knowledge but also basic knowledge to serve as a health communicator. Among the views expressed by the participants, how to communicate with the elderly and provide older people with basic information about diseases and prevention to raise their awareness to provide information about the disease, was also crucial.
Very often, the delivery of health information is challenging for older adults due to well-known language, low literacy, and cultural barriers. Therefore, I think GNP should acquire knowledge to understand the local cultural background and overcome language barriers to provide effective health education. (GP1, urban, community health center)
Health Information Management and Policy Development: Identifying the Prioritization of Health Problems and Supporting Policy Development
Most of the participants stated that GNPs are the preferred professionals to perform health information management to identify the prioritization of health problems of older adults. The examples provided by the participants illustrate that the abilities of GNP to collect and analyze health information on older adults are essential in the primary health care system.
I think a very important role for GNP is to analyze health information and identify priorities for health problems in older adults based on epidemiological knowledge. It is a key way to inform GPs or other professionals of treatment adjustments. (RN34, rural, township health center)
Additionally, the management of health information was considered as a key aspect of the advanced geriatric nursing role in the primary healthcare system to promote health conditions and reduce risk factors.
GNP needs to effectively analyze the health information to understand the diseases with high incidence and their influencing factors among the community-home elderly, to prevent these diseases in time. (GP2, rural, township health center)
Furthermore, some participants reported that GNPs need to identify the actual needs of older adults to support policy development.
“GNP should clarify the needs of the elderly through the collection and analysis of health information to support the development of national policies.” (M2, rural, township health center)
Leadership and Coordination: Promoting the Construction of Multidisciplinary Care Models
GNPs were identified as conduits of communication between members of the multidisciplinary team, between the multidisciplinary team and primary care providers, and between the multidisciplinary team and the older adults. The role of the GNP as coordinator and leader was particularly valued by multidisciplinary team members when there is a lack of standard guiding the care of older people in primary health care.
Geriatric care requires multidisciplinary cooperation. However, we do not have a standard model to guide our division of staff at this stage. Therefore, I hope that RNs can play a better leadership, coordination, and communication role to facilitate the construction of a multidisciplinary collaboration model.(GP4, rural, township health center)
Discussion
The main findings in our study indicate that the RN has a central role in caring for older people within the primary health care system, however, several factors have limited their development into advanced geriatric nursing roles in China context. Additionally, our study built an expected role model of GNPs to guide the development of educational programs for GNP while supporting GNPs’ sustainability and scalability in primary health care. These findings are congruent with the first national guidelines for health promotion, Healthy China 2030, and the corresponding Three-Tiered Age Care System, which highlights the importance of integrated care within the primary health care system.
Initially, our study re-examined the existing role of RNs in elderly care from the different perspectives of physicians, RNs, and managers. According to the results, we found that role of RNs in elderly care with more responsibility for health screening, chronic disease management, and health education. However, the roles of RNs involved in the care of older adults are limited to implementing BPHS programs or activities that the organization requires them to complete. Moreover, most of the participants expressed a view that RNs spend much time on activities that are not related to gerontological nursing, such as medical examination guidance and entry of health information. The move of the Three-Tiered Aged Care System requires advanced knowledge and competencies from RNs to coordinate and manage older adults with complex conditions among home, community, and long-term institutions. Indeed, findings from a survey investigating the demand for gerontological nurses in 35 hospitals, 284 community and 253 long-term care facilities in Zhejiang Province indicated that all institutions have a great need on skill-mix RNs equipped with advanced gerontological nursing knowledge and competency.37 Moreover, other countrie’s experience with an integrated model that combines APNs and RNs shows that interdisciplinary care approaches are effective for the care of older adults.38 Therefore, in this context, attention needs to be shifted from hospital to the primary health care to develop and optimize the gerontological nursing staff when implementing integrated care.
The absence of a full-time position, role ambiguity, lack of professional staff, and limited professional autonomy were all identified by participants as important factors affecting the development of advanced geriatric nursing roles in the current primary health care system. These findings align with the preview literature, which emphasized the role clarification and support practice should be considered to guarantee the development of the APN role, including the clear job description, independent decision-making, and adequate preparation of APN.29,39 Among these identified factors, ensuring sufficient RNs with adequate knowledge and competence to care for older adults is considered to be critical to the development of advanced geriatric nursing roles in primary health care. Preview literature also emphasized the importance of educational programs of making the advanced knowledge and skills of RNs involved in caring for older adults, due to the complexity and prevalence of the aging population in nursing practice.40,41 To cope with the continuing shortage of RNs educated to care for older adults, competency-based education programs both at Bachelor’s and Master’s level had been developed in the USA and other countries.42,43 However, in China, the development of geriatric care is relatively late and there is no established framework or standards for gerontological nursing education.44 Moreover, previous studies have indicated that nursing education is one significant way to enhance students’ interest in pursuing a career in caring for older people.45 Therefore, gerontological nursing education is an important way to prepare future GNPs and to promote this field as a career choice. Thus, we suggest that the Chinese government should adopt a whole education approach to prepare adequately for the development of GNP including undergraduate education, master’s education, and continuing professional development.
Another factor also emphasized by the participants in our study was the limited professional autonomy of the RNs. NPs in other countries have legal rights to diagnostic authority, prescriptive authority, independent practice authority, and multi-specialty practice authority.46 However, whether NPs are suitable for multi-site practice is still being debated in China. Therefore, there is a need to refine policies to establish a clear career framework and promote the authority of GNP for independent practice. Taken together, the above factors should be highlighted to promote the development of GNP roles and to prepare qualified GNPs in an integrated care model that can effectively address the needs of older adults in a variety of primary health care settings.
Furthermore, our study also explored expectations of the GNPs’ roles from different perspectives. These roles were emerged into four domains, including “support and advocacy”, “comprehensive assessment, communication, and case management”, “health information management and policy development”, and “leadership and coordination”. Due to practice conditions and time are not yet ripe for GNP development in China, the roles identified by participants in our study were based on participants’ perceptions of the current practice environment in primary health care and the characteristics of older adults. GNPs in our study are expected to play central roles in comprehensive assessment, case management, and better coordinate collaboration among primary health care settings, which are recognized as key components to meeting the complex needs in other countries that have implemented the GNP in primary health care.19,47,48 These findings are also consistent with the elements involved in integrated care models, which usually include comprehensive assessment, case management, systematic risk factor screening, patient education, professional education, home visits, and medication review.49 However, compared with the findings from preview studies, the roles of GNP in our study focused more on supporting and advocating for vulnerable groups, especially for empty-nest older adults who remained in the community. These views are associated with the high number of empty-nest older adults in rural and remote areas of China that have a low quality of life and are at high risk for mental illness.50,51 Thus, GNP in our study is expected to be a suitable professional to build long-term relationships with empty-nest older adults and to promote health equity. Additionally, health information management is also emphasized by participants to highlight the importance of collecting data to assess community health status and aging population needs in primary healthcare systems. These findings align with the health care systems to meet the needs of older adults, which represent the core thrusts of a global strategy and action plan on aging and health. The World Health Organization with other health promotion institutions have launched an age-friendly care framework to advance the momentum of age-friendly communities, health care, and public health. The preview literature reported that gerontological nurses should enhance their knowledge about age-friendly movements and advance their competencies in caring for older adults.52 Additionally, the COVID-19 pandemic has placed older adults at high risk and placed greater demands on nurses’ public health nursing competencies and knowledge. Thus, future education programs for GNPs should consider integrating gerontological nursing, public health nursing, and nursing management to better meet the integrated and complex needs of older adults in the primary health care system.
Nursing in primary health care settings, particularly the client’s home is notably different from hospital settings because of higher levels of isolation and autonomy.53 Identically, caring for older people in primary health care requires higher competencies and knowledge from RNs. Not only advanced geriatric care knowledge and skills are required, but also stronger communication, coordination, and public health nursing skills are needed to ensure that older adults in different institutions can receive continuing care. In conclusion, our findings can provide a role model framework for guiding the future development of GNPs, also provide new perspectives on the future development of competency frameworks and educational programs.
Limitations
This study has a few limitations. Because the sample size and geographic distribution were limited, we must be cautious in generalizing the conclusions. Data collection was performed by a single researcher with a nursing background, which may introduce bias. In further, the majority of participants in our study were recruited from community health centers and township health centers, and the staff in long-term institutions were not included. The long-term institution plays a supplementary role in the three-tier aged care system in China, and future research can be conducted to further explore the role of GNPs in long-term institutions, and to make the GNP role model a better fit with China’s aged care system.
Conclusion
The current roles of RNs in caring for older adults are more limited in the primary health care system. There is a need for developing appropriate educational programs, well-established laws, and regulations to support the sustainable development of GNPs. To build the expected role model, the nursing education program in the future should integrate gerontological nursing, public health nursing, and nursing management to maximize the role of gerontological nurse practitioners in primary health care.
Acknowledgments
The authors thank the RNs, GPs, and managers who participated in this study for their time and feedback; and Fujian Provincial Hospital and all health centers participated in this study for supporting the interview conduct.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhai Z, Chen J, Long L. Future trends of China’s population and aging: 2015~2100. Popul Res. 2017;41(4):60–71.
2. Statistical Bulletin of the People’s Republic of China on National Economic and Social Development in 2019. Statistical bulletin of the People’s Republic of China; 2020. Available from: www.stats.gov.cn/tjsj/zxfb/202002/t20200228_1728913.html.
3. Lewis C, Moore Z, Doyle F, et al. A community virtual ward model to support older persons with complex health care and social care needs. Clin Interv Aging. 2017;12:985–993. doi:10.2147/CIA.S130876
4. Briggs A, Carvalho I. Actions required to implement integrated care for older people in the community using the World Health Organization’s ICOPE approach: a global Delphi consensus study. PLoS One. 2018;13(10):e0205533. doi:10.1371/journal.pone.0205533
5. Briggs A, Valentijn PP, Thiyagarajan JA, Carvalho I. Elements of integrated care approaches for older people: a review of reviews. BMJ Open. 2018;8(4):e021194. doi:10.1136/bmjopen-2017-021194
6. Zhou Y, Li Y, Zhu X, Ma L. Medical and old-age care integration model and implementation of the Integrated Care of Older People (ICOPE) in China: opportunities and Challenges. J Nutr Health Aging. 2021;25(6):720–723. doi:10.1007/s12603-021-1595-5
7. Nkomazana O, Mash R, Shaibu S, Nthabiseng P. Stakeholders’ perceptions on shortage of healthcare workers in primary healthcare in botswana: focus group discussions. PLoS One. 2015;10(8):e0135846. doi:10.1371/journal.pone.0135846
8. Holveck Casandra A, Wick Jeannette Y. Addressing the shortage of geriatric specialists. Consult Pharm. 2018;33(3):130–138. doi:10.4140/TCP.n.2018.130
9. Bloomfield JG, Christina A, Thomas THT, et al. Factors associated with final year nursing students’ desire to work in the primary health care setting: findings from a national cross-sectional survey. Nurse Educ Today. 2018;61:9–14. doi:10.1016/j.nedt.2017.10.001
10. Li W, Xu A, Lu M, et al. Influence of primary health care physicians’ perceived overqualification on turnover intention in China. Qual Manag Health Care. 2020;29(3):158–163. doi:10.1097/QMH.0000000000000259
11. Zhang L, Shen S, Guo Y, et al. Forecasting future demand of nursing staff for the oldest-old in china by 2025 based on markov model. Int J Health Policy Manag. 2021. doi:10.34172/ijhpm.2021.63
12. Storm M, Siemsen Inger Margrete D, Laugaland K, Dyrstad DN, Aase K. Quality in transitional care of the elderly: key challenges and relevant improvement measures. Int J Integr Care. 2014;14:e013. doi:10.5334/ijic.1194
13. Pellegrin Karen L, Krenk L, S j O, Ciarleglio A, J. L. Reductions in medication-related hospitalizations in older adults with medication management by hospital and community pharmacists: a quasi-experimental study. J Am Geriatr Soc. 2017;65(1):212–219. doi:10.1111/jgs.14518
14. Martínez-González NA, Djalali S, Tandjung R, et al. Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. BMC Health Serv Res. 2014;14:214. doi:10.1186/1472-6963-14-214
15. Maier C, Aiken L. Task shifting from physicians to nurses in primary care in 39 countries: a cross-country comparative study. Eur J Public Health. 2016;26(6):927–934. doi:10.1093/eurpub/ckw09826
16. Fougère B, Morley J, Decavel F, et al. Development and implementation of the advanced practice nurse worldwide with an interest in geriatric care. J Am Med Dir Assoc. 2016;17(9):782–788. doi:10.1016/j.jamda.2016.05.009
17. Duffy E. The future of the gerontological nurse practitioner and GAPNA. Geriatr Nurs (Minneap). 2012;33(5):410–415. doi:10.1016/j.gerinurse.2012.07.008
18. Ljungbeck B, Forss K. Advanced nurse practitioners in municipal healthcare as a way to meet the growing healthcare needs of the frail elderly: a qualitative interview study with managers, doctors and specialist nurses. BMC Nurs. 2017;16:63. doi:10.1186/s12912-017-0258-7
19. Yafa H, Dorit R, Shoshana R. Gerontological nurse practitioners (GNPs) for the first time in Israel: physician and nurse attitudes. J Am Assoc Nurse Pract. 2016;28(8):415–422. doi:10.1002/2327-6924.12343
20. King A, Boyd M, Dagley L, Raphael D. Implementation of a gerontology nurse specialist role in primary health care: health professional and older adult perspectives. J Clin Nurs. 2018;27:807–818. doi:10.1111/jocn.1411027
21. Hungerford C, Prosser B, Davey R, Clark S. The Australian “grey nomad” and aged care nurse practitioner models of practice: a case study analysis. Rural Remote Health. 2016;16(2):3647. doi:10.22605/RRH3647
22. Henni SH, Kirkevold M, Antypas K, Foss C. The role of advanced geriatric nurses in Norway: a descriptive exploratory study. Int J Older People Nurs. 2018;13(3):e12188. doi:10.1111/opn.12188
23. Greenberg S, Squires A, Adams J, et al. A post-master’s advanced certificate in gerontology for NPs. Nurse Pract. 2017;42(9):18–23. doi:10.1097/01.NPR.0000521992.53558.73
24. Prajankett O, Markaki A. Integrated older people care and advanced practice nursing: an evidence-based review. Int Nurs Rev. 2020;68(1):67–77. doi:10.1111/inr.12606
25. Morilla-Herrera JC, García-Mayor S, Martín-Santos F, et al. A systematic review of the effectiveness and roles of advanced practice nursing in older people. Int J Nurs Stud. 2016;53:290–307. doi:10.1016/j.ijnurstu.2015.10.010
26. Chavez KS, Dwyer A, Ramelet A. International practice settings, interventions and outcomes of nurse practitioners in geriatric care: a scoping review. Int J Nurs Stud. 2018;78:61–75. doi:10.1016/j.ijnurstu.2017.09.010
27. Chen H-X, Pu L, Chen Q, Xu X, Bai C, Hu X. Instrument development for evaluation of gerontological nurse specialists core competencies in China. Clin Nurse Spec. 2019;33(5):217–227. doi:10.1097/NUR.0000000000000469
28. Mao Y, He R, Liu J, Zhang N, Zhu BL. Turnover intention of primary health workers in China: a systematic review. BMJ Open. 2018;10(10):e037117. doi:10.1136/bmjopen-2020-037117
29. Cao L, Wang J, Liang Y, Chen Y. The level of gerontological care competencies of community nurses in Shanghai. J Nurs Sci. 2018;033(017):81–84.
30. Torrens C, Campbell P, Hoskins G, et al. Barriers and facilitators to the implementation of the advanced nurse practitioner role in primary care settings: a scoping review. Int J Nurs Stud. 2019;104:103443. doi:10.1016/j.ijnurstu.2019.103443104
31. Hsieh H, Shannon S. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
32. Nvivo software (Version11.0). Available from: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/about/nvivo.
33. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(18):59–82. doi:10.1177/1525822X05279903
34. Lincoln G, Guba E, Lincoln Y, Guba Y. Naturalistic inquiry guba lincoln. J Neuroendocrinol. 2019;31. doi:10.1111/jne.12694
35. Rgn SC. Content analysis: concepts, methods and applications. applications. Nurse Res. 1997;4(3):5. doi:10.7748/nr.4.3.5.s2
36. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
37. Chen L, Zhang L. Investigation on the demands for geriatric nurses and major provision. Chin Nurs Manage. 2013;14(8):845–848.
38. Josi R, Bianchi M. Advanced practice nurses, registered nurses and medical practice assistants in new care models in Swiss primary care: a focused ethnography of their professional roles. BMJ Open. 2019;9(12):e033929. doi:10.1136/bmjopen-2019-0339299
39. Brault I, Kilpatrick K, D’amour D, et al. Role clarification processes for better integration of nurse practitioners into primary healthcare teams: a multiple-case study. Nurs Res Pract. 2014;2014:170514. doi:10.1155/2014/170514
40. Henni SH, Kirkevold M, Antypas K, Foss C. The integration of new nurse practitioners into care of older adults: a survey study. J Clin Nurs. 2019;28:2911–2923. doi:10.1111/jocn.14889
41. Dahlke SA, Kalogirou MR, Swoboda NL. Registered nurses reflections on their educational preparation to work with older people. Int J Older People Nurs. 2021;16(2):e12363. doi:10.1111/opn.12363
42. Bednash GP, Mezey MD, Tagliareni EJ. The hartford geriatric nursing initiative experience in geriatric nursing education: looking back, looking forward. Nurs Outlook. 2011;59(4):228–235. doi:10.1016/j.outlook.2011.05.01259
43. Backhaus R, Verbeek H, van Rossum E, Capezuti EA, Hamers JP. Future distinguishing competencies of baccalaureate-educated registered nurses in nursing homes. Geriatr Nurs. 2015;36(6):438–444. doi:10.1016/j.gerinurse.2015.06.01236
44. Wang F, Department M, University S. Current situation and countermeasures on geriatric nursing education in China. Med Philosophy. 2014;35(1A):77–79.
45. Koskinen S, Salminen L, Stolt M, Leino-Kilpi H. The education received by nursing students regarding nursing older people: a scoping literature review. Scand J Caring. 2015;29(1):15–29. doi:10.1111/scs.1213529
46. Kroezen M, Dijk L, Groenewegen P, Francke A. Nurse prescribing of medicines in Western European and Anglo-Saxon countries: a systematic review of the literature. BMC Health Serv Res. 2011;11:127. doi:10.1186/1472-6963-11-127
47. King AII, Boyd M, Raphael D, Jull A. The effect of a gerontology nurse specialist for high needs older people in the community on healthcare utilisation: a controlled before-after study. BMC Geriatr. 2018;18(1):22. doi:10.1186/s12877-018-0717-3
48. Buerhaus P, Chang Y, DesRoches CM, Guzikowski S, Norman LD, Donelan K. The roles and clinical activities of registered nurses and nurse practitioners in practices caring for older adults. Nurs Outlook. 2021;69(3):380–388. doi:10.1016/j.outlook.2020.11.011
49. Goodwin N, Dixon A, Anderson GM, Wodchis WP. Providing Integrated Care for Older People with Complex Needs Lessons from Seven International Case Studies. London:King’s Fund; 2014.
50. Huang G, Duan Y, Guo F, Chen G. Prevalence and related influencing factors of depression symptoms among empty-nest older adults in China. Arch Gerontol Geriatr. 2020;91:104183. doi:10.1016/j.archger.2020.10418391
51. Gao Y, Wei YB, Shen YD. China’s empty nest elderly need better care. J Am Geriatr Soc. 2014;62(9):1821–1822. doi:10.1111/jgs.1299762
52. Carmody J, Black K, Bonner AF, Wolfe M, Fulmer T. Advancing gerontological nursing at the intersection of age-friendly communities, health systems, and public health. J Gerontol Nurs. 2021;47(3):13–17. doi:10.3928/00989134-20210125-01
53. Smolowitz J, Speakman E, Wojnar DM, et al. Role of the registered nurse in primary health care: meeting health care needs in the 21st century. Nurs Outlook. 2014;63(2):130–136. doi:10.1016/j.outlook.2014.08.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.