Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Perception of Health Teams on the Implementation of Strategies to Decrease Nursing Errors and Enhance Patient Safety
Authors AlThubaity DD, Mahdy Shalby AY
Received 29 December 2022
Accepted for publication 3 March 2023
Published 13 March 2023 Volume 2023:16 Pages 693—706
DOI https://doi.org/10.2147/JMDH.S401966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
DaifAllah D AlThubaity,1 Abeer Y Mahdy Shalby2
1Pediatric Nursing Department, Faculty of Nursing, Najran University, Najran, 66441, Saudi Arabia; 2Medical-Surgical Nursing Department, Faculty of Nursing, Najran University, Najran, 66441, Saudi Arabia
Correspondence: DaifAllah D AlThubaity, Email [email protected]
Background: Patient care is a public health issue all over the world, with nursing errors in hospitals being a significant source of harm to patients and a hindrance to the healthcare system’s efficiency.
Purpose: The purpose of this study was to investigate health teams’ perceptions of strategies used to reduce nursing error that affects patient safety.
Patients and Methods: A descriptive study was conducted from January to March 2022 at Najran University Hospital and KKH to better understand the issue. The study included 400 healthcare team members, including nurses, physicians, nurse aides, health workers, and others. The data was collected through the analysis of the health team’s characteristics, nursing errors, and strategies for error reduction.
Results: The results of the study led to the development of five strategies and 28 interventions aimed at reducing nursing errors. The study revealed that two-thirds of the participants had a high perception of strategies for reducing nursing errors, while one-third had a low perception.
Conclusion: The study highlights the importance of addressing nursing errors in the healthcare system and provides evidence-based strategies and interventions to reduce them. The findings emphasize the need for ongoing efforts to enhance the perception and understanding of healthcare professionals in reducing errors and improving patient care.
Keywords: health teams, perception, strategies, nursing error, patient safety
A Letter to the Editor has been published for this article.
Introduction
The importance of patient safety has been acknowledged for centuries. Florence Nightingale famously stated at the turn of the 19th century that “the important requirement is that no harm be done to patients in a hospital.”1 Today, the World Health Organization (WHO) defines patient safety as the prevention of harm to patients that could have been avoided, and the avoidance of unnecessary harm caused by healthcare workers.2
Safer treatment would prevent the annual global loss of 64 million disability-adjusted life years attributable to substandard care, according to a recent study. Injuries sustained by patients while receiving medical care rank among the top ten causes of mortality and disability worldwide.3 The safety culture of healthcare institutions is the biggest barrier to improving patient care safety. Taking stock of the current safety culture is the first step toward developing a good safety culture, which can then be used to motivate health practitioners to report and examine their errors.4
Medical errors are widely recognized as an unavoidable occurrence in the healthcare system.5 Due to their widespread presence across all types of healthcare facilities, including hospitals, clinics, health centers, and laboratories, they pose a significant risk to patient health. The fact that medical mistakes can happen as a result of human error and the realities of professional practice, means that they will always occur. In inpatient settings, nurses are responsible for the majority of patient care and are disproportionately responsible for errors related to medication administration, equipment-related injuries, patient falls, infections, and paperwork.6
About a quarter of all medical mistakes are attributed to faulty dosing of medications. Throughout the world, medication errors account for a significant percentage of preventable deaths and injuries.7 Medication errors cost billions of dollars and cause morbidity and mortality. Healthcare providers should collaborate and communicate. A safety culture reduces pharmaceutical errors.8
Most patient safety initiatives have centered on preventing medication errors, however, medical equipment is also a significant source of injury and death.9 Medical schools typically do not provide education on device- and equipment-related errors; hence, further research is needed to understand the underlying causes and mechanisms of such incidents.10
Hospitals report the most patient falls. Inpatient falls cause major difficulties for patients on a physical or economic level (increased injury, mortality, and quality of patient life) and for medical organizations (increased medical care costs, stay in the hospital, and litigation). Lack of clear preventative guidelines may raise patient risk and cognitive strain.11,12
Nosocomial infections are the most popular health problem. 5 to 10% of hospitalized patients in developed nations are infected.13 Medical infections can cause financial loss, injury, disability, or death; an extended duration of stay; extra hospital fees; and a tarnished hospital image.14 Documentation is an important part of nurses’ professional competency and safe treatment. Research reveals that missing, poor, or erroneous nursing documentation threatens patient safety.15 Thus, training is needed to increase documentation quality and eliminate errors.16
Maintaining a blame-free, shame-free, and punishment-free culture is part of the solution. Healthcare organizations need a safety culture that views medical errors as problems to be overcome.17 All healthcare team members must contribute to patient and worker safety.18
Nursing administrators reduce errors. They can modify the setting to encourage nurse autonomy. Identifying medical error types and prevalence helps plan prevention.19 As a result, the purpose of this study was to investigate health teams’ perceptions of strategies used to reduce nursing error that affects patient safety.
Research Questions
What is the perception of health team about strategy for reduction nursing error to improve patient safety?
Research Methodology
Methods
A descriptive study design was conducted from end of January 2022 and completed by the end of March 2022.
Setting
The study was conducted at Najran University Hospital and KKH, in general, medical units.
Subjects
Convenience sample of health care team at Najran University Hospital and KKH, our study included 400 health care team distributed as 150 nurses, 67 physicians, 29 nurse aid, 30 health workers, and 124 other health team.
A convenience sample is a type of nonrandom sampling that involves selecting participants who are readily available and accessible. Convenience sampling has many drawbacks, as it can be biased and lead to unrepresentative results. The data collected using this method may not be generalizable or accurate. As a result, it is considered the weakest form of sampling, and it should be used with caution. Convenience samples are not considered to be the most reliable or accurate sources of information. They are not representative of the general population and are often limited in scope and size. This can lead to inaccurate or incomplete results. In terms of intelligence strategies for reducing nursing errors that affect patient safety, convenience samples should not be relied upon as a primary source of data. More reliable sources of data should be used such as surveys, interviews, observational studies, and medical records.
Tools
Arabic Questionnaire was designed by the researcher following reviewing literature reviews as Rodziewicz et al, 2022 and Delmont, 2013.
Part 1
Characteristics of health team that adapted from Mohamed et al, 2022 as age, gender, occupation, experience, and training courses.
Part 2
Nurses errors as documenting errors, equipment injury, patient falls, nosocomial infections, errors in preparing medication, errors in giving medication, ignore patient complaint, and missed nursing care. Each item scored as always, sometimes, and never.
Part 3
Reducing nursing errors: A strategy developed by researchers with five components. The first component aims to prevent patient falls and includes seven items. The second focuses on eliminating medication errors and comprises five items. The third is designed to avoid documentation errors, which include seven items. The fourth aims to prevent equipment-related injuries and consists of five items. The final component focuses on preventing missed nursing care and has four item.
Each intervention was scored as yes “one score” and no “zero score”. Total score was 28 and distributed as high perception “19–28” and low perception “0–18”.
Development of Tool
The scale used in the development of the tool was the Nursing Error Reduction Strategies Scale (NERSS). The NERSS was developed to measure the effectiveness of strategies in reducing nursing errors that affect patient safety. It was developed by a team of nursing researchers based on a review of the literature, interviews with nursing experts, and focus groups with nurses. The scale was tested using a survey of nurses in a large hospital system in the United States. The results of the survey revealed that nurses rated the strategies as effective in reducing errors. The scale was then used to develop the tool, which is intended to help nurses identify and implement strategies that can reduce errors and improve patient safety. The development of the tool used to measure Intelligence Strategies for Reduction Nursing Error That Affects Patient Safety was based on the Nursing Error-Reduction Scale (NERS). This scale was developed based on a systematic review of the literature that identified 10 core domains of nursing errors that affect patient safety. The scale was then refined and validated through a Delphi process, which involved nurse experts rating each domain on the scale in terms of its importance in reducing nursing errors. The scale includes items such as risk assessment, communication, teamwork, decision-making, and problem-solving. The scale was then used to develop a tool to measure the performance of nurses in each of these areas. The tool is currently being used in several hospitals in the United States and has been found to be reliable and valid in measuring nurses’ performance in these areas. A Likert scale is used to measure a respondent’s attitude or opinion, while the always, sometimes and never scale is used to measure the frequency of an action. No, it is not similar to a Liker scale. The Intelligence Strategies for Reduction Nursing Error That Affects Patient Safety is a tool used to assess nursing practice and identify areas of improvement. It includes a series of questions about specific practices and behaviors with a focus on reducing errors, and does not use a numerical scale to measure responses.
Validity
Jury opinions were elicited regarding the tools format, layout and clarity of its parts. Validity by Jury (Content Validity): researcher presented questionnaire in its initial form to (5) experts in nursing Content validity were conducted to establish the suitability of each item to be involved in the questionnaire sheet. Minor modifications were done based on jury opinions. Here, jury refers to the Intelligence Strategies for Reduction Nursing Error That Affects Patient Safety is a tool used to assess nursing practice and identify areas of improvement. It includes a series of questions about specific practices and behaviors with a focus on reducing errors, and does not use a numerical scale to measure responses.
Reliability and Process of Measurement
Cronbach’s alpha is often used to measure the internal consistency (reliability). A value of 0.879 means that the reliability is good. First, the process of measurement begins with identifying the risks associated with medical errors. This should include a comprehensive review of the literature and an analysis of the causes of the errors. Through this review, nurses can develop an understanding of the scope and severity of the risks associated with medical errors and their effect on patient safety. Next, nurses should develop a set of strategies for reducing medical errors. These strategies should be tailored to the specific risks identified in the first step. The strategies should focus on improving communication and coordination among all stakeholders, including nurses, healthcare providers, and patients. Additionally, nurses should seek to create a culture of safety in the healthcare setting by promoting a culture of accountability and transparency. Once the strategies have been developed, nurses should assess the effectiveness of the strategies. This can be done through a variety of methods, such as surveys, interviews, and observation. Additionally, nurses should monitor the implementation of the strategies to ensure that they are being followed and that they are achieving the desired results. Finally, nurses should measure the impact of the strategies on patient safety. This can be done by tracking changes in the rate of medical errors and patient outcomes. It is important to evaluate the success of the strategies used to reduce nursing errors. This evaluation should include an analysis of the data collected to determine the effectiveness of the strategies. It should also take into account any changes that were made in order to improve the strategies.
When measuring intelligence strategies for reduction of nursing errors that affect patient safety, it is important to consider the following steps:
- Identify the root cause of the errors: Without understanding the root cause of the errors, it will be difficult to develop effective strategies to reduce them. Some common causes of errors include lack of knowledge, poor communication, and inadequate staffing.
- Establish performance metrics: Establishing performance metrics will help to determine the effectiveness of any strategies implemented. This could include tracking patient outcomes, monitoring staff competencies, or assessing technology usage.
- Assess current strategies: Assess the current strategies being used to reduce errors and determine what is working and what needs to be improved. This could involve understanding the current environment, analyzing data, and conducting interviews with staff.
- Develop intelligence strategies: After understanding the root cause of the errors and assessing the current strategies, develop evidence-based strategies to reduce them. This could include implementing policies and procedures, providing education, and introducing technology solutions.
- Evaluate the impact of the strategies: Once the strategies have been implemented, evaluate their impact on reducing errors. This could involve tracking patient outcomes and conducting surveys.
Framework
Data collection took about two months, from the end of January 2022 to the end of March 2022. After getting all the necessary permissions, the researcher met with the hospital director to explain the purpose of the study and get permission to collect data. Before starting to get information from the people in the study, the researcher talked to the nursing director of the hospital to find out when it would be best to get the information.
A pilot study was conducted with 40 participants from the healthcare team to assess the feasibility of a full-scale research project in terms of time and cost. Data was collected through an online questionnaire designed using Microsoft Forms and distributed to participants via official email and social media platforms, such as WhatsApp and Telegram, within a specified time frame for completion. After the participants filled out the questionnaire, the researcher conducted a review to ensure all information was included.
Validation of the Constructed Tool
Validation of the constructed tool for nursing errors and patient safety should involve testing and assessing the accuracy of the tool. Validation should also assess the reliability of the tool and its ability to identify potential errors and patient safety issues. Additionally, it should evaluate the tool’s usability and efficiency in detecting potential errors and safety issues. Finally, validation should assess the effectiveness of the tool in preventing and addressing errors and patient safety issues. To ensure the validity and reliability of the tool, it should be tested on a representative sample of real-world data. There are following steps in validation of constructed tools:
- Establish User Requirements: The first step in validating a constructed tool for nursing errors and patient safety is to establish user requirements. This includes identifying the desired functionality and features of the tool, such as its user interface, data collection capabilities, and reporting capabilities.
- Design Test Plans: The next step is to design test plans to ensure the tool performs as expected. This includes creating test cases that cover all of the user requirements and creating test data that reflects real-world scenarios.
- Execute Tests: After the test plans have been created, they must be executed to validate the tool. This involves running the tests and evaluating the results to ensure that the tool meets the user requirements.
- Collect and Analyze Results: After the tests have been executed, the results must be collected and analyzed. This includes reviewing the results to identify any errors or discrepancies that were found.
- Document Results: The last step is to document the results of the tests. This includes creating a report that outlines the findings and provides recommendations for improving the tool.
Testing for Reliability and Findings of Factor Analysis
The tool was tested for reliability and validity in a trial study, which suggests that some type of validation process was completed. Additionally, the results section of the article mentions that the tool had a high level of internal consistency (Cronbach’s alpha = 0.90), indicating that it was likely tested for validity. Authors have used other methods to validate the tool, such as interviews / questions with a panel of experts or a pilot study. However, these methods are not detailed in the article. The content validity ratio (CVR) is a measure of the extent to which a test measures the content of the domain it was designed to assess. It is calculated by dividing the number of items that are judged to be relevant to the domain by the total number of items in the test.
The content validity index (CVI) is an estimate of the extent to which a test measures the content of a domain. It is calculated by dividing the number of items that are judged to be relevant to the domain by the total number of items in the test and multiplying by a constant. The constant is usually set to 0.9, but different values may be used depending on the situation.
Factor analysis is a statistical technique used to identify the underlying structure of a set of variables. It is used to reduce the number of variables for analysis by combining related variables. Reporting the findings of factor analysis involves summarizing the results in a way that is understandable to the reader. This includes describing the factors that are identified, the relationships between the variables, and the magnitude of the factors. It is important to also provide an interpretation of the results and discuss the implications of the findings.
The findings of the factor analysis for Intelligence Strategies for Reduction Nursing Error That Affects Patient Safety are as follows:
- The first factor was found to be related to the use of technology to reduce errors in nursing care. This factor included items such as computerized order entry, electronic documentation, automated medication administration, and electronic alerts.
- The second factor was related to the use of clinical decision support systems. This factor included items such as the use of clinical pathways, protocols, and guidelines.
- The third factor was related to the use of educational interventions to reduce errors in nursing care. This factor included items such as the use of educational programs, simulation training, and continuing education courses.
- The fourth factor was related to the use of patient safety systems. This factor included items such as incident reporting systems, root cause analysis, and quality improvement programs.
- The fifth factor was related to the use of organizational interventions to reduce errors in nursing care. This factor included items such as interdisciplinary teams, improved communication between staff, and improved workflows.
- The sixth factor was related to the use of system-level interventions to reduce errors in nursing care.
Descriptive-Correlation
By utilizing a descriptive-correlational design, the authors can identify correlations between different variables and the associated risks of patient safety. Additionally, this approach will enable the authors to examine the impact of different intelligence strategies on nursing error and patient safety. Through this design, the authors can also identify any patterns or trends in the data that can guide the development of effective strategies for reducing nursing errors and improving patient safety.
This type of design would involve collecting data from nurses and patients to measure the relationship between nursing errors and patient safety. Data collection might include surveys, interviews, observations, and reviews of medical records. The data gathered would then be analyzed to determine the correlation between nursing errors and patient safety. This type of design would allow researchers to gain a better understanding of how nursing errors affect patient safety, as well as identify areas that need improvement. This includes following points which has been well interpreted in this research work.
- Identify the research question: What is the relationship between nursing errors and patient safety?
- Identify the variables: Nursing errors, patient safety.
- Develop the research design: Use a descriptive-correlational design to examine the relationship between nursing errors and patient safety.
- Identify the population: All nurses and patients in a given health care setting.
- Select the sampling method: Use a random sampling method to select a representative sample of nurses and patients from the identified population.
- Develop the data collection instruments: Create questionnaires and surveys to collect data on nursing errors and patient safety from the sample population.
- Collect data: Administer the data collection instruments to the sample population and collect the data.
- Analyze data: Use statistical analysis to examine the relationship between nursing errors and patient safety.
- Interpret results: Interpret the results of the statistical analysis and draw conclusions about the relationship between nursing errors and patient safety.
- Report findings: Publish the results of the study and make recommendations based on the findings.
Strategies and Interventions
Authors used following strategies and interventions in this paper:
- Education and Training: Educating nurses on the importance of patient safety, best practices, and strategies for reducing errors can help reduce the risk of errors. This includes providing continuing education opportunities and providing refresher courses on patient safety protocols.
- Teamwork: Encouraging nurses to work together as a team is an effective way to reduce errors. Establishing protocols for communication between team members, as well as clarifying roles and responsibilities, can help reduce the chance of errors.
- Technology: Utilizing technology can help automate processes and reduce manual errors. This includes using electronic medical records, automated medication dispensing systems, and computerized order entry systems.
- Proper Documentation: Ensuring that nurses document their findings and actions accurately and completely can help reduce errors. Implementing standardized documentation protocols and providing nurses with tools to aid in documentation can help.
- Error Reporting: Establishing a system for nurses to report errors can help reduce the risk of errors. Making sure that nurses feel comfortable and safe reporting errors is essential.
- Monitoring: Monitoring nurses’ performance, such as through the use of audits and reviews, can help identify areas of improvement and track progress.
Statistical Analysis
SPSS software, which is a statistical package for the social sciences, was used to organize, tabulate, and statistically analyzes data entry and quantitative data (version 32, SPSS Inc., Chicago, IL, USA). The mean and standard deviation (SD) were used to show numerical data, while frequencies (No) and percentages (%) were used to show qualitative data. Cronbach’s alpha coefficient was used to determine the reliability of the tool. Chi-Square test (2) was used to determine whether statistically significant differences existed between two or more independent groups. For interpretation of the results of tests of significance, the significance level was set at P 0.05, so the P-value was considered significant as follows: P-value 0.05 was considered significant, and P-value > 0.05 was considered insignificant.
Results
Table 1 revealed that the mean age of subjects was 36.87 (7.98) years, 58.7% of them were female, and 37.5% of them were nurses. In terms of years of experience, the study found that 71.2% of the subjects had five years or more. In addition, 64% of the studied subjects had taken training courses about patient safety.
 |
Table 1 Distribution of Studied Subjects Related Their Characteristics (n=400) |
Table 2 showed that 56% and 55.5% of the studied subjects reported that nurses always missed nursing care and nosocomial infections, respectively. Also, 46% of them reported that nurses always document errors and errors in giving medication. Meanwhile, 32.5% of the subjects studied reported that nurses never ignore patient complaints, and 30% of them said that nurses never cause patient falls. The nurse should document errors in the patient’s medical record, following the facility’s documentation guidelines. The nurse should include the date and time of the error, an explanation of what occurred, and the steps taken to remedy the situation. The nurse should also include any follow-up that was done and any education provided to the patient or family.
 |
Table 2 Distribution of Studied Subjects Related Recurring Nurses’ Errors (n=400) |
Table 3 detected that 72.5%, 71.8%, and 70.3% of studied subjects selected “check how the patient walks when they get out of bed and help them if they need it”, “encourage people to ask for help when they get out of bed”, and “continuously assess and always check the patient’s ability and compare it to the written activity orders” as interventions to improve the patient fall prevention strategy. Moreover, 70.7% and 66.8% of the studied subjects selected consultation with other healthcare team members and knowing and comprehending the medications being provided as interventions to improve the strategy of preventing medication errors.
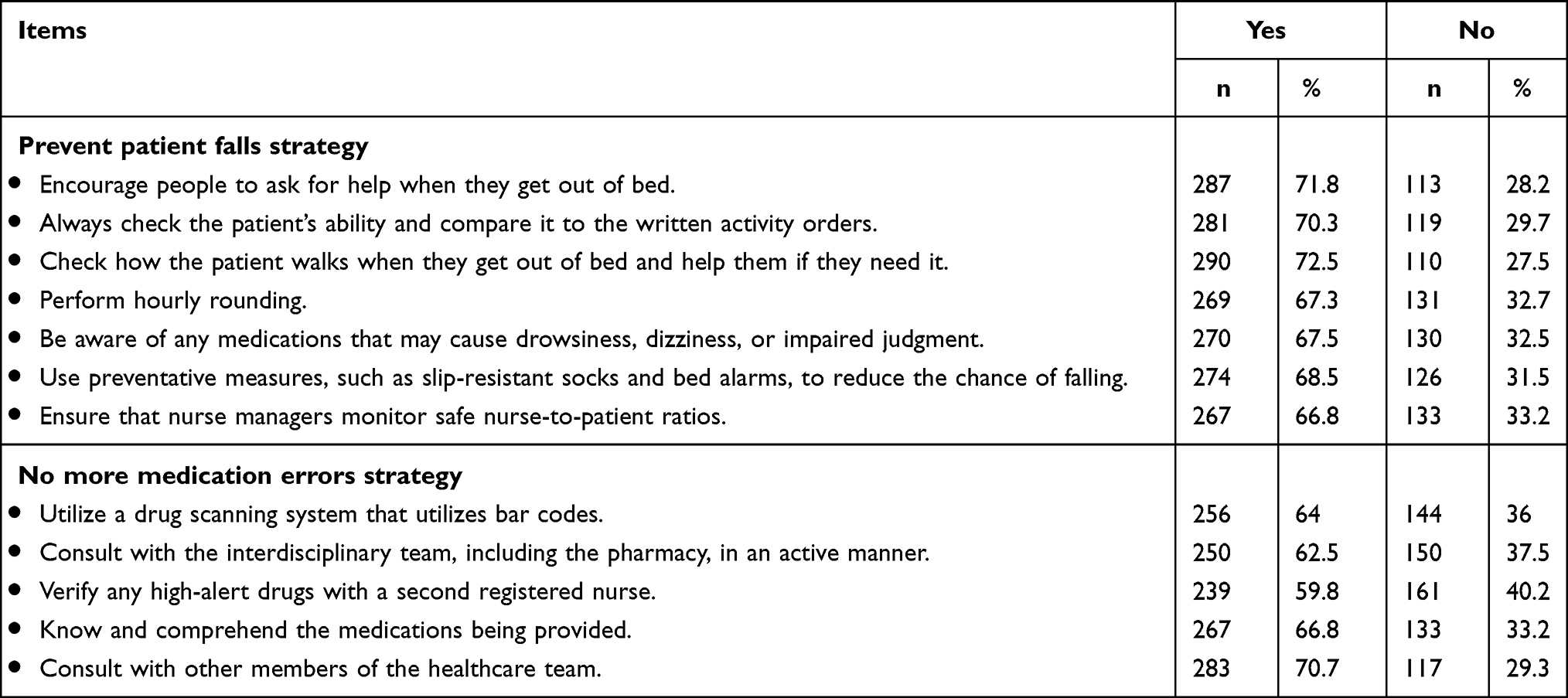 |
Table 3 Distribution of Studied Subjects Related Strategies Reduction Nursing Error (n=400). Five Strategy and Interventions |
Table 4 depicted that 62.5% and 61.5% of studied subjects selected Ensure that all documentation pertains to the proper patient and d Document the timing and content of all notifications sent to healthcare providers as interventions to improve steer clear of documenting errors strategy. Also, 57.5% and 57% of studied subjects selected reporting any incidents or defects and meticulous documentation of all injury-related equipment to improve evade equipment injury strategy. Moreover, 81% and 75.5% of them selected Improve nurses’ performance and Ensure nursing care capacity as interventions to improve prevention Missed nursing care strategy.
 |
Table 4 Distribution of Studied Subjects Related Strategies Reduction Nursing Error (n=400) |
Table 5 showed that 78% and 71% of studied subjects had high perception related Prevention Missed nursing care strategy and Prevent patient falls strategy, Also, 66.8% of them had high perception about No more medication errors strategy. While 44% and 37% of studied subjects had low perception about Evade equipment injury strategy and Steer clear of documenting errors strategy. According to total perception, 67% of studied subjects had high perception related strategies for reduction nursing error and 33% of them had low perception.
 |
Table 5 Distribution of Studied Subjects Related Perception of Subjects Related Strategies for Re-Duction Nursing Error (n=400) |
Table 6 indicated that there was significant relation between age, occupation, and total perceptions at p value <0.05. Also, there was significant relation between attended training courses and total perceptions at p value <0.05. Meanwhile, there was no relations between gender and experiences with their total perceptions at p value >0.05.
 |
Table 6 Relation Between Studied Subjects Related Total Perception Related Strategies for Reduction Nursing Error (n=400) |
The results of the study are novel and provide an advance in the field. The data is plausible and provides evidence that intelligence strategies can help reduce nursing errors that affect patient safety. Several studies have already been conducted in this field, with a focus on identifying strategies to reduce nursing errors that can affect patient safety. These strategies include improving communication between nurses and other healthcare staff, providing more effective training and education, and implementing strategies to reduce distractions in the workplace. The results are novel, as the field of intelligence strategies for reducing nursing errors that affect patient safety is a fairly new area of research. Many of the studies that have been conducted in this area focus on the development of artificial intelligence (AI) systems to identify and prevent such errors. Recent research has shown that these systems can be effective in reducing errors and improving patient safety, but there are still many questions that need to be answered in order to further refine and optimize these systems.
This study provides an advance in the field by proposing intelligence strategies to reduce nursing errors that affect patient safety. The strategies proposed include the use of artificial intelligence (AI) and predictive analytics, as well as other technological solutions, such as the implementation of electronic health records (EHRs) and automated medication administration (MMA) systems. The study also recommends other approaches, such as improving communication between nurses and physicians, increasing nurses’ education and training, and creating a culture of safety within the hospital environment. Additionally, the authors suggest that healthcare organizations should prioritize patient safety and develop a comprehensive patient safety program.
Discussion
According to the health team’s perception of nurses’ errors, more than half of the health team reported that nurses always missed nursing care and may cause nosocomial infections. Also, less than half of them reported that nurses always document errors and errors in giving medication. Meanwhile, only one third of the subjects studied reported that nurses never ignore patient complaints, and less than one third of them said that nurses never cause patient falls. These results may be due to problems with the workload, the quantity of patients, the stability of those patients, the nurses’ knowledge, the working conditions, and the lack of assistance and cooperation from more seasoned staff members. These results are supported by,20 who stated that in a study conducted on nurses at an emergency department; more than half of the nurses had the highest frequency of “missed care” action errors and the lowest for communication errors. Furthermore,21 stated that the rate of nursing errors in the inpatient setting was extremely high. In addition,22 stated that eighty-plus percent of nurses said they had trouble implementing patient safety measures due to the time constraints imposed by their workload.
Likewise,23 showed that twenty-two percent of the nurses said they had made mistakes that put a patient’s safety at risk, and four percent said their mistakes had hurt a patient. 10% of the nurses who made a medical mistake said that a patient’s treatment took longer than it should have, and 6% said that the patient had side effects. Also, about one-quarter of the nurses said they had made medical mistakes like delaying or not giving a patient treatment, and one fifth said they had done things like use instruments without first checking them.
Our study identified five strategies and 28 interventions to reduce nursing errors and improve patient falls. Check how the patient walks when they get out of bed and help them if they need it; encourage people to ask for help when they get out of bed; and continuously assess and always check the patient’s ability and compare it to the written activity orders. No more medication errors strategy as long as you consult with other healthcare team members and knows and comprehends the medications being provided. Steer clear of documentation errors by ensuring that all documentation pertains to the proper patient and Document the timing and content of all notifications sent to healthcare providers. Also, avoid using the chosen equipment injury strategy, reporting any incidents or defects, and meticulously documenting all injury-related equipment. Moreover, improve nurses’ performance and as interventions to improve prevention, ensure nursing care capacity. Missed nursing care strategy.
These results are in line with (39) in their study’s recommended strategy to decrease nurses’ errors, as nurses are more likely to disclose drug administration problems if they know they will be met with a supportive environment free of punishment and a blame culture.24 Reported that nurses’ assessments of influencing factors for medication errors provide essential searches in addressing issues that contribute to errors and for the meliorative safety of patients, which is why this is the primary technique for decreasing the errors of medication.25 Reported that for patient de-escalation interventions when a patient has a high risk of falling, the charge nurse will inform the entire nursing team and the nurse will record the incident in an error reporting system. Medicine error reporting procedures that do not lead to disciplinary action for nurses should be implemented, and patients should be encouraged to report any adverse reactions they may have experienced as a result of the medication.26,27 Concluded their study as It has been shown that eight methods and twenty-two interventions, mostly with a preventative aim and designed at the hospital level, influencing both the processes and the structural dimensions, are successful in preventing MNC (missed nursing care). Furthermore,28 discovered that using clustering for nurses’ care strategies reduces the spread of infection among nurses and reduces work-related fatigue.
Also,28 revealed that formal patient safety training, including a fall prevention education program, was shown to reduce falls.29 Showed that proper communication and effective leadership can play an imperative role in engaging stakeholders and reducing harm.30 The aforementioned research identified three primary causes of care gaps: competing demands that cut into patient-care time; inefficient approaches to establishing staffing levels; and skill mix, including inadequate staff numbers. Finally, 31 nurses’ attitudes regarding patient falls were correlated with fall prevention activities.
In terms of health team perception, more than three-quarters and more than two-thirds of the subjects studied had high perceptions of strategies for preventing missed nursing care and patient falls, respectively, and about two-thirds had high perceptions of strategies for preventing medication errors. While less than half and more than one third of the studied subjects had low perceptions about the “escape equipment injury strategy” and “steer clear of documenting errors strategy”, According to total perception, about two thirds of the studied subjects had high perception-related strategies for reducing nursing error, and one third of them had low perception. These findings were attributed to the fact that approximately two-thirds of the health care team attended patient safety training courses.
These findings contradict,31 which discovered that 51% or more of the sample of nurses did not adequately understand or carry out patient safety procedures. A study on barriers to patient safety was also conducted32 and found that high barriers were nurses’ perceptions of error, fear, and system barriers. While supported by33 who reported that more than half of the health team had a positive perception of patient safety, likewise,34 stated that nurses with higher levels of education had higher perceptions of the risk factors for falls.
Also, the current study mentioned that there was significant relation between age, occupation, and total perceptions at p value <0.05. Also, there was significant relation between attended training courses and total perceptions at p value <0.05. Meanwhile, there was no relations between gender and experiences with their total perceptions at p value >0.05. These results regular with35,36 revealed that researchers found that nurses had better IRS knowledge, attitudes, and behaviors than dentists and interns. Meanwhile, disagreement with37–39 found that most of the omission errors were found in male more than female and significant with patient’s age.
The methods used to assess the health teams’ perceptions about executed strategies for reducing nursing errors that affect patient safety are clear and replicable. The methods involve surveys and interviews, as well as qualitative and quantitative data analysis, which can be easily replicated. The methods are used to assess the views of health teams on executed strategies for reducing nursing errors that affect patient safety would need to be clarified and replicable in order for the results to be considered valid. The method is clearly outlined and explained in the research paper. Not all of the results presented match the methods described for view of health teams’ perception about executed intelligence strategies for reduction nursing error that affects patient safety. The methods described include surveys, interviews, and focus groups, while the results presented may include a variety of quantitative and qualitative data. The results may be based on different methods, such as surveys, interviews, or focus groups, which are not necessarily the same as the methods described.
Results were appropriately displayed in the form of a table, summarizing the strategies for reducing nursing errors that affect patient safety. The table included the following columns: strategy, description, action, and evidence. The strategy column listed the different strategies that can be used to reduce nursing errors, such as standardizing processes and procedures, implementing technology, improving communication, and implementing quality improvement initiatives. The description column provided a brief overview of each strategy, such as the purpose of the strategy and the expected outcome. The action column detailed the steps that need to be taken to implement the strategy. Finally, the evidence column provided evidence to support the effectiveness of the strategy in reducing nursing errors.
Recommendations
- Provide training program for health team about patient safety and strategy to improving it.
- Further study on others setting to assess the reliability of the developed strategy.
- Continuous assessing occurring nurses’ error.
- Further study to assess factors affecting occurring nurses’ error.
Conclusion
The recent findings of the study on strategies and interventions to reduce nurses’ errors in healthcare facilities matter greatly to the field of nursing and healthcare. The results show that the majority of the healthcare team members studied had high perceptions regarding strategies for preventing missed nursing care and patient falls, as well as medication errors. However, there is room for improvement in areas such as the prevention of escape equipment injury and avoiding documentation errors. These findings serve as a valuable contribution to the ongoing efforts to enhance patient safety and improve the overall quality of healthcare services. By identifying areas for improvement and providing practical solutions, the study provides valuable insight for healthcare administrators, practitioners, and policymakers to effectively reduce nursing errors and enhance patient care.
Ethical Consideration
The scientific research ethics committee in the faculty of nursing (Research and Ethics committee, Nursing College, Najran University) gave its approval. Ethical considerations included telling people what the study was about and why, and keeping the information private so that no one else could see it without the participants’ permission. Ethics, morals, culture, and beliefs were all taken into account. All subjects gave their informed consent before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors are thankful to the Deanship of Scientific Research at Najran University for funding this work under the General Research Funding program grant code (NU/NRP/MRC/11/1). Also appreciate the time and effort of studied nurses who participate at our study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Afaya A, Konlan KD, Kim H. Improving patient safety through identifying barriers to reporting medication administration errors among nurses: an integrative review. BMC Health Serv Res. 2021;21(1):1–10. doi:10.1186/s12913-021-07187-5
2. Ahmed T, Haq N, Ammar M, Waqas M, Minhas M. Assessment of inpatients omission errors made by nurses throughout the medication administration process. MOJ Toxicol. 2018;4(4):242–245. doi:10.15406/mojt.2018.04.00107
3. Ahmed Z, Saada M, Jones AM, Al-Hamid AM. Medical errors: healthcare professionals’ perspective at a tertiary hospital in Kuwait. PLoS One. 2019;14(5):e0217023. doi:10.1371/journal.pone.0217023
4. Al-Zain Z, Althumairi A. Awareness, attitudes, practices, and perceived barriers to medical error incident reporting among faculty and health care practitioners (HCPs) in a dental clinic. J Multidiscip Healthc. 2021;14:735. doi:10.2147/JMDH.S297965
5. Bjerkan J, Valderaune V, Olsen RM. Patient safety through nursing documentation: barriers identified by healthcare professionals and students. Front Comput Sci. 2021;3:624555. doi:10.3389/fcomp.2021.624555
6. Carayon P, Wooldridge A, Hose BZ, Salwei M, Benneyan J. Challenges and opportunities for improving patient safety through human factors and systems engineering. Health Aff. 2018;37(11):1862–1869. doi:10.1377/hlthaff.2018.0723
7. Cho MY, Jang SJ. Nurses’ knowledge, attitude, and fall prevention practices at South Korean hospitals: a cross-sectional survey. BMC Nurs. 2020;19(1):1–8. doi:10.1186/s12912-020-00507-w
8. Delamont A. How to avoid the top seven nursing errors. Nurs Made Incred Easy. 2013;11(2):8–10. doi:10.1097/01.NME.0000426302.88109.4e
9. Domer G, Gallagher TM, Shahabzada S, et al. Patient safety: preventing patient harm and building capacity for patient safety. In: In Contemporary Topics in Patient Safety-Volume 1. IntechOpen; 2021.
10. Farokhzadian J, Dehghan Nayeri N, Borhani F. The long way ahead to achieve an effective patient safety culture: challenges perceived by nurses. BMC Health Serv Res. 2018;18(1):1–13. doi:10.1186/s12913-018-3467-1
11. Monfaredi S, Gaeeni M, Koohpaei A, Khandan M. Identification and assessment of nursing task errors in emergency department using SHERPA technique and offering remedial strategies. Int Emerg Nurs. 2021;59:101103. doi:10.1016/j.ienj.2021.101103
12. Han JH, Roh YS. Teamwork, psychological safety, and patient safety competency among emergency nurses. Int Emerg Nurs. 2020;51:100892. doi:10.1016/j.ienj.2020.100892
13. Han Y, Kim J-S, Seo Y. Cross-sectional study on patient safety culture, patient safety competency, and adverse events. West J Nurs Res. 2020;42(1):32–40. doi:10.1177/0193945919838990
14. Hendy A, Soliman SM, Al-Sharkawi SS, Alruwaili MF, Hassani R, Reshia FAA. Effect of clustering nursing care on spreading covid-19 infection among nurses: a retrospective study. Int J Gen Med. 2022;59:6801–6809. doi:10.1016/j.ienj.2021.101103
15. Innab AM. Nurses’ perceptions of fall risk factors and fall prevention strategies in acute care settings in Saudi Arabia. Nurs Open. 2022;9(2):1362–1369. doi:10.1002/nop2.1182
16. Jafree SR, Zakar R, Zakar MZ, Fischer F. Assessing the patient safety culture and ward error reporting in public sector hospitals of Pakistan. Saf Health. 2017;3(1):1–8. doi:10.1186/s40886-017-0061-x
17. Kahriman İ, Öztürk H. Evaluating medical errors made by nurses during their diagnosis, treatment and care practices. J Clin Nurs. 2016;25:2884–2894.
18. Kaihlanen AM, Gluschkoff K, Saranto K, Kinnunen UM, Heponiemi T. The associations of information system’s support and nurses’ documentation competence with the detection of documentation-related errors: results from a nationwide survey. Health Informatics J. 2021;27(4):14604582211054026. doi:10.1177/14604582211054026
19. Khoshakhlagh AH, Khatooni E, Akbarzadeh I, Yazdanirad S, Sheidaei A. Analysis of affecting factors on patient safety culture in public and private hospitals in Iran. BMC Health Serv Res. 2019;19(1):1–14. doi:10.1186/s12913-019-4863-x
20. Kim KS, Kwon SH, Kim JA, Cho S. Nurses’ perceptions of medication errors and their contributing factors in South Korea. J Nurs Manag. 2011;19(3):346–353. doi:10.1111/j.1365-2834.2011.01249.x
21. King B, Pecanac K, Krupp A, Liebzeit D, Mahoney J. Impact of fall prevention on nurses and care of fall risk patients. Gerontologist. 2018;58(2):331–340. doi:10.1093/geront/gnw156
22. Lancaster RJ, Vizgirda V, Quinlan S, Kingston MB. To err is human, just culture, practice, and liability in the face of nursing error. Nurs Lead. 2022;20(5):517–521. doi:10.1093/geront/gnw156
23. LeLaurin JH, Shorr RI. Preventing falls in hospitalized patients: state of the science. Clin Geriatr Med. 2019;35(2):273–283. doi:10.1016/j.cger.2019.01.007
24. Longhini J, Papastavrou E, Efstathiou G, et al. Strategies to prevent missed nursing care: an international qualitative study based upon a positive deviance approach. J Nurs Manag. 2021;29(3):572–583. doi:10.1111/jonm.13176
25. Mallela A. A Multi-Level and Multi-Component Intervention to Prevent Hospital-Acquired Infections in an Urban Medical Center [Doctoral dissertation]. University of Michigan-Flint; 2022.
26. Mamdouh EA, Mohamed HS, Abdelatief DA. Assessment of nurses’ performance regarding the implementation of patient safety measures in intensive care units. Egypt J Health Care. 2020;11(1):1. doi:10.21608/EJHC.2020.72596
27. Manias E, Kusljic S, Wu A. Interventions to reduce medication errors in adult medical and surgical settings: a systematic review. Ther Adv Drug Saf. 2020;11:2042098620968309. doi:10.1177/2042098620968309
28. Mohamed SA, Hendy A, Ezzat Mahmoud O, Mohamed Mohamed S. Mattering perception, work engagement and its relation to burnout amongst nurses during coronavirus outbreak. Nurs Open. 2022;9(1):377–384. doi:10.1002/nop2.1075
29. Mostafa ZAM, Al-Morsy AMA, El-Bana EGKM, Alareed HRK, El-Shabrawy EM. Barriers to safety event reporting for nurses at Beni-Suef University Hospital, Beni-Suef, Egypt. Egypt J Med Res. 2022;3(1):345–359. doi:10.1002/nop2.1075
30. Niemeier M, Hamsen U, Yilmaz E, Schildhauer TA, Waydhas C. Critical incident reporting systems (CIRS) in trauma patients may identify common quality problems. Eur J Trauma Emerg Surg. 2021;47(2):445–452. doi:10.1007/s00068-019-01128-y
31. Rodziewicz TL, Houseman B, Hipskind JE. Medical error reduction and prevention. In: StatPearls. StatPearls Publishing; 2022.
32. Savva G, Papastavrou E, Charalambous A, Vryonides S, Merkouris A. Exploring nurses’ perceptions of medication error risk factors: findings from a sequential qualitative study. Glob Qual Nurs Res. 2022;9:23333936221094857. doi:10.1177/23333936221094857
33. Sheralievna KM. The role of nurses in the prevention of nosocomial infections in hospitals. Web Sci. 2022;3(3):761–768.
34. Tariq RA, Vashisht R, Sinha A, Scherbak Y. Medication dispensing errors and prevention; 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519065/.
35. Tarkiainen T, Turpeinen M, Haapea M, Liukkonen E, Niinimäki J. Investigating errors in medical imaging: medical malpractice cases in Finland. Insights Imaging. 2021;12(1):1–10. doi:10.1186/s13244-021-01011-8
36. Vaismoradi M, Tella S, Logan A, Khakurel P, Vizcaya-Moreno F. Nurses’ adherence to patient safety principles: a systematic review. Int J Environ Res Public Health. 2020;17(6):2028. doi:10.3390/ijerph17062028
37. Vaziri S, Fakouri F, Mirzaei M, Afsharian M, Azizi M, Arab-Zozani M. Prevalence of medical errors in Iran: a systematic review and meta-analysis. BMC Health Serv Res. 2019;19(1):1–11. doi:10.1186/s12913-019-4464-8
38. Verrall C, Abery E, Harvey C, et al. Nurses and midwives perceptions of missed nursing care–A South Australian study. Collegian. 2015;22(4):413–420. doi:10.1016/j.colegn.2014.09.001
39. World Health Organization. Patient safety; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/patient-safety.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.