Back to Journals » International Journal of Women's Health » Volume 17
Perception and Childbirth Decision-Making in Unintended Pregnancy: A Qualitative Study
Authors Qiu D, Zou Y, Xiong H, Huang J, Geng L, Zhai J
Received 25 June 2025
Accepted for publication 17 October 2025
Published 5 December 2025 Volume 2025:17 Pages 5181—5193
DOI https://doi.org/10.2147/IJWH.S546376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Dan Qiu,1,* Yinting Zou,2,* Haiyan Xiong,2 Jingyi Huang,1 Lingling Geng,1 Jinguo Zhai3
1DongGuan Maternal and Child Health Care Hospital, Dongguan, 523057, People’s Republic of China; 2School of Nursing, Guangdong Maoming Health Vocational College, Maoming, 525400, People’s Republic of China; 3School of Nursing, Southern Medical University, Guangzhou, 510515, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinguo Zhai, School of Nursing, Southern Medical University, Guangzhou, 510515, People’s Republic of China, Tel +8618620287620, Email [email protected]
Introduction: It’s estimated that about 121 million unintended pregnancies occur worldwide every year, which has significant impacts on individuals, families, and society. It’s important to explore the factors influencing the childbirth decision in these women, thereby informing midwifery practice.
Methods: A qualitative study was performed on women with unintended pregnancies via focus group discussion. The thematic analysis was guided by the theory of planned behavior. Data were analyzed using a combination of deductive and inductive content analysis.
Results: The analysis revealed three main themes and several subthemes: attitudes toward behavior (changes in fertility concepts, impact of fertility policies, conflicts in women’s roles), subjective norms (influence from friends, family, societal attitudes towards fertility), and perceived behavioral control (health-related pregnancy factors, pressures of child-rearing responsibilities, concerns about family, workplace support).
Discussion: Women are eager to make informed decisions regarding unintended pregnancies. A collaborative effort from society, healthcare providers, and families is essential to support these women in making appropriate decisions. Healthcare providers hold a pivotal role in caring for pregnant women. Additional studies are required to assess and integrate strategies within healthcare practice.
Trial Registration: The study received the approval from the Ethics Committee at Dongguan Maternal and Child Health Care Hospital (No. 2024– 14) on 12 April 2024.
Keywords: unintended pregnancy, decision-making, reproductive health, midwifery practice
Introduction
Unintended pregnancy occurs when a woman is not ready to have a child and is characterized as an unplanned, unwanted, or mistimed pregnancy.1 Such pregnancies can cause considerable distress and exert significant health, emotional, financial, and social impacts on individuals and their families.2 The reproductive choices of women experiencing unintended pregnancies vary widely and are influenced by a range of cultural and social factors. Their perceptions and experiences could let clinicians better understand the requirements to deliver appropriate healthcare services and foster personalized, evidence-based decision-making in these women. This understanding is particularly vital in China, where the country faces a dramatic demographic transformation, with an aging population, a shrinking workforce, and declining birth rates.3
Unintended pregnancy has become an important worldwide public health issue, with an annual global incidence of approximately 121 million cases from 2015 to 2019.4 After awareness of the unintended pregnancy, the pregnant woman has to make the reproductive choice regarding whether to have the child or not.5 Previous research has found that many women with unintended pregnancies experienced difficulty in making decision on whether to continue or terminate them.5–7 They needed time, support, and guidance from healthcare providers to weigh their intentions, wishes, and emotions.6 Yet, little research has explored the specific factors that could shape their process of decision-making during this difficult period.6 In China, several studies have investigated the factors that influence women’s fertility decisions under the national childbirth policy.8,9 However, the decision-making process among women with unintended pregnancies was rarely addressed.5,6 Midwives are at a unique position to support and care women with pregnancies. Acquiring insights into the experiences and factors that shape childbirth decision-making can provide evidence-based support to midwifery practice for better reproductive health in women facing unintended pregnancies.
The decision-making process in women with unintended pregnancies is complex, encompassing women’s living situations, relationships with sexual partners, future plans, and moral responsibilities on abortion or motherhood.10–12 Childbirth decisions were made from an economic perspective and were influenced by subjective emotions and beliefs.10 The theory of planned behavior (TPB) is a psychological model explaining the impact of various factors on people’s intention to engage in a particular behavior.13,14 According to the TPB, fertility intention is determined by three core components: attitude toward childbearing, subjective norm regarding childbirth, and perceived control over childbearing.15 The TPB has been applied to understand the fertility intention in various situations and provide valuable insights on the process of fertility decision-making, enabling in-depth exploration of attitudes, perceived behavioral control, and intentions in these women, thus providing a thorough understanding of factors shaping the reproductive choices.16–18
Here, we utilized the TPB as a conceptual framework to conduct a qualitative study among women with unintended pregnancies. We aimed to investigate the experiences and perceptions of these women, focusing on identifying factors that influence childbirth decision-making, thereby informing healthcare practice.
Methods
Study Design
The study employed a qualitative descriptive design, in which face-to-face individual interviews were conducted at Dongguan Maternal and Child Health Care Hospital in China between May and July 2024. The study protocol was approved by the local hospital’s ethics committee. Participation was voluntary, and all participants provided written informed consent. This study’s reporting complies with the COREQ guidelines.19 The conduction of the study complied with the Declaration of Helsinki.
Participant Selection and Recruitment
The purposive and theoretical sampling methods were adopted to enroll study participants. The inclusion criteria were 1) married and parous women ≥18 years old; 2) unintended pregnancy (ie, without a pregnancy planning); 3) intrauterine pregnancy confirmed by ultrasound; 4) women with a recent abortion or antenatal check-ups at family planning clinics or obstetric clinics; and 4) ability to communicate effectively. Following the maximum variation sampling strategy in qualitative research, participants were selected based on their age, education, occupation, and reproductive history. The participant recruitment was stopped when data saturation was reached and no new information emerged.
Data Collection
The semi-structured interview was designed following the TPB principles (Figure 1 and Table 1).13 Face-to-face semi-structured interviews were conducted by two professionally trained obstetricians, each with more than 10 years’ clinical experience. Both of them also had conducted qualitative research previously. The interviews were scheduled after 12 weeks of pregnancy or after induced abortion. Prior to commencement, participants were presented with the choice of being interviewed jointly with their spouse, friend, or relative. Of the 12 participants, three agreed to the jointed interviews, while one participant was accompanied by her spouse, two participants were accompanied by their mothers, and nine participants opted for solo interviews. Prior to the study, participants were informed of the study purpose, process, and format. Semi-structured, open-ended interviews were carried out in a quiet room, aiming to capture interviewees’ genuine perspectives while ensuring each question in the outline was addressed fully and truthfully without straying from the topic. In addition, vocal cues, intonation, pauses, facial expressions, and body language were also recorded. Each session lasted 20–30 minutes. Both brief written notes and audio recordings were analyzed.
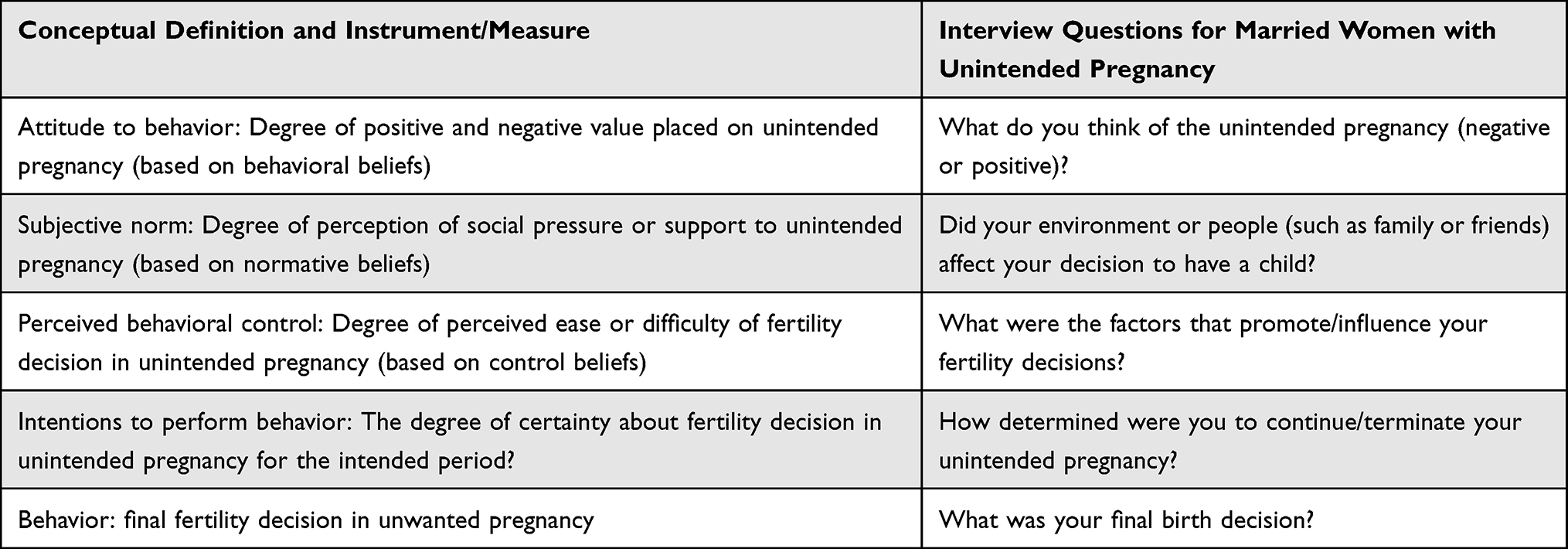 |
Table 1 Interview Questions Based on the Theory of Planned Behavior |
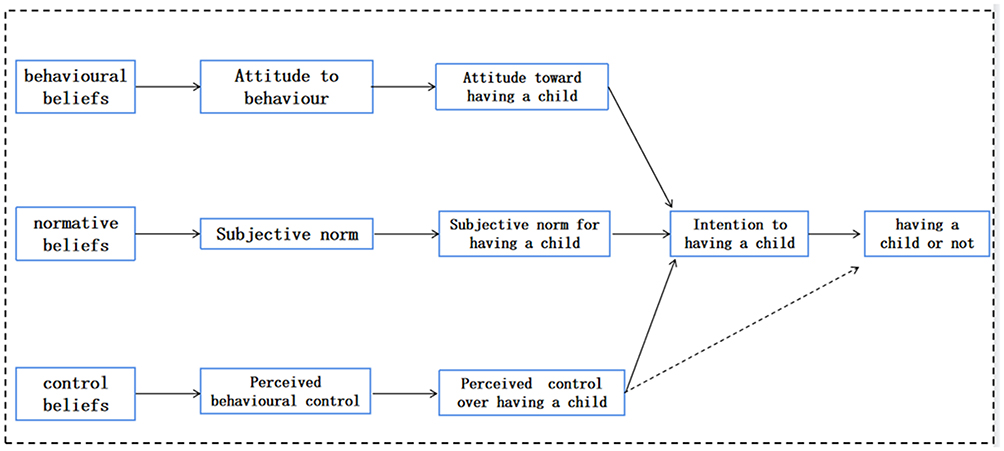 |
Figure 1 Conceptual model to understand experience and perspectives on childbirth choice in women with unintended pregnancy based on the theory of planned behavior. |
Data Analysis
Combined deductive and inductive methods were applied for repeated content analysis.20,21 Within 24 hours post-interview, audio recordings were transcribed verbatim alongside their transcripts, then coded using according to the three elements of the TPB. Initially, open coding was used to deconstruct the information, seeking codes to extract and develop categories through comparative analysis. During axial coding, interrelationships between categories were identified, with thematic connections verified against the data. Selective coding was then employed to refine the core categories and establish as many connections as possible between the core and other categories.
To ensure the accuracy, interview results were transcribed word-for-word in the original languages (Chinese), and then all chosen Chinese quotes were translated into English by two bilingual researchers and back-translated by a third one. This translation procedure standardized the textual data into English transcript to facilitate the subsequent analysis.
To maintain the rigor of the data collection and analysis process, we strictly adhered to the COREQ guidelines.19 The authors (ZYT and ZJG), with substantial expertise in maternal health education and qualitative research,22,23 designed research questions and analyzed data aligning with the current knowledge and skills in maternal health research. All authors participated throughout the study procedure of data collection and analysis to ensure that data interpretation remained consistent. In addition, researchers held several meetings to deliberate on the emerging categories and themes. Furthermore, the study’s credibility was boosted by the purposive sampling method to collect a diverse sample of women.24 The selection and characteristics of participants, as well as data collection and analysis processes, were clearly described to facilitate transferability. All data analyses and interpretation findings were considered provisional until supported and validated by data.
Ethical Considerations
The Ethics Committee of DongGuan Maternal and Child Health Care Hospital approved the study (No. 2024–14) on 12 April 2024. Every participant was made aware of the study’s process and explained the voluntary nature of the study. Written informed consent was acquired from participants prior to data collection. Participants retained the right to withdraw from the study at any time without any impact on their clinical care. All data collected were held in strict confidence, with access to the audio recordings and transcripts restricted solely to the researchers.
Results
A total of 12 married and parous women (aged 25 to 43, 32.7 ± 5.7 years) with unintended pregnancies participated in the semi-structured, face-to-face interviews. They had between zero to two children and had experienced zero to three miscarriages previously. Their clinical characteristics are detailed in Table 2. Analysis of the interview data generated three primary themes and nine sub-themes associated with childbirth decision-making among these women (Table 3).
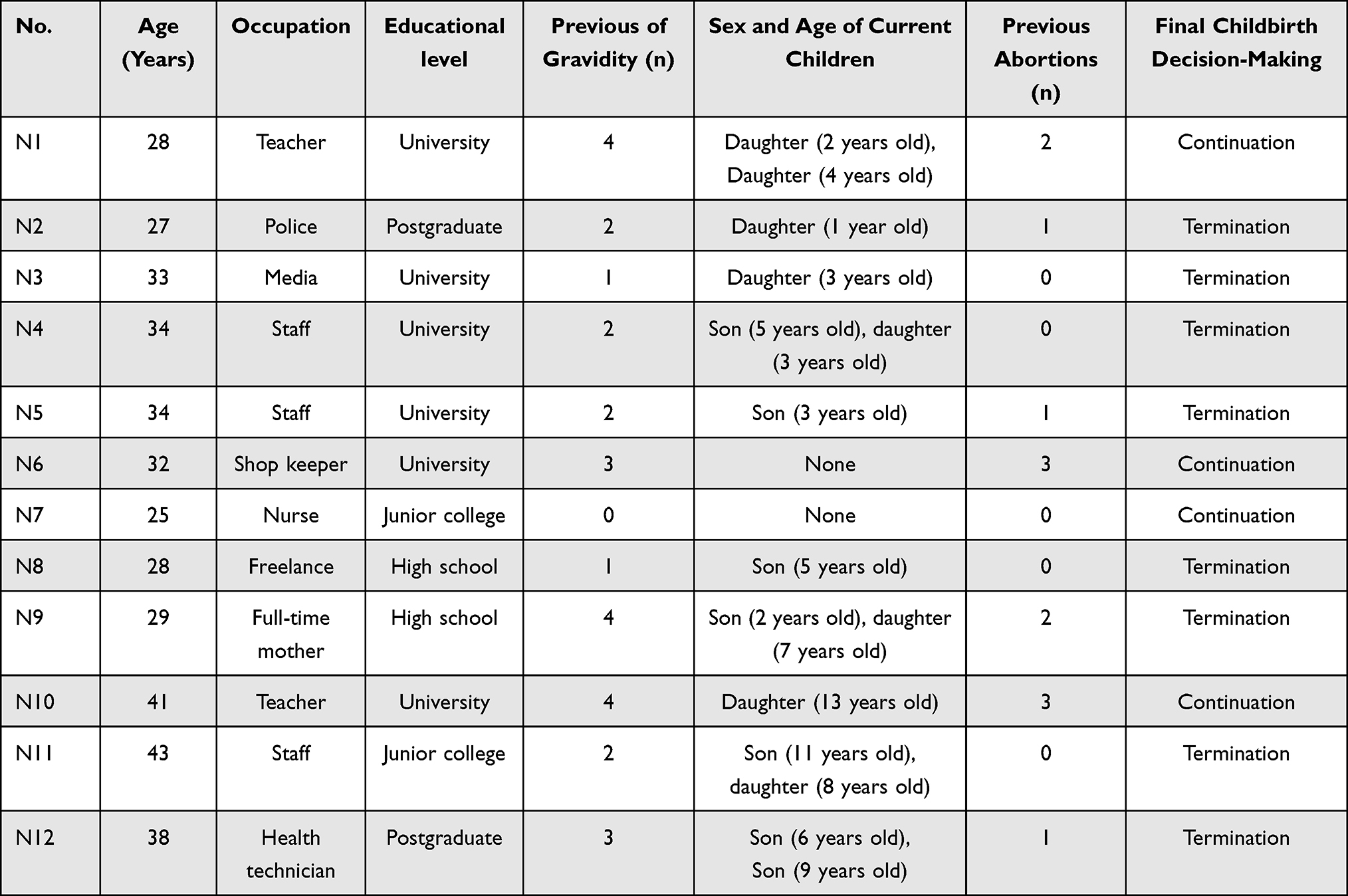 |
Table 2 Clinical Characteristics of Study Participants (n = 12) |
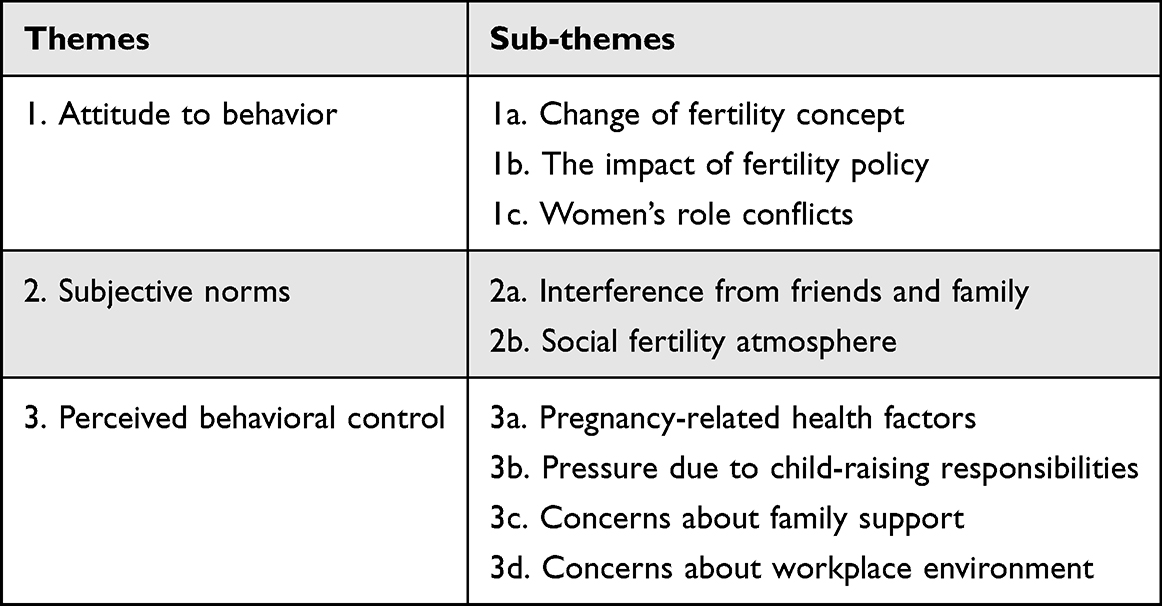 |
Table 3 Themes and Sub-Themes of Childbirth Decision-Making Among Women with Unintended Pregnancy |
Attitude Behavior
Behavioral beliefs represent the individual’s subjective evaluations and value judgments about fertility. Women’s behavioral beliefs about fertility, whether positive or negative, are directly linked to their intentions regarding childbirth, thereby influencing their decision-making processes. Positive behavioral beliefs may arise from the perceived benefits of fertility or personal emotional needs. Conversely, negative behavioral beliefs often stem from entrenched personal fertility concepts and the impact of fertility policies and are associated with adverse value judgments regarding fertility outcomes.
Change in Fertility Concept
Most married women did not desire an additional child, although they might change their minds later.
Despite the pressure of raising two children, I will still choose to have an additional child. I like kids, and they have company when they group up. (continue pregnancy) (N1)
I like two children, a boy and a girl, but I never consider three children. (terminate pregnancy) (N4)
I wish I had two children, but I already have a boy. I’m worried that another one will still be a boy. (terminate pregnancy) (N8)
Two children are just right, preferably a boy and a girl. One more child will give us a lot of pressure. (terminate pregnancy) (N9)
The individual emotional effect was prominent. The influences of traditional fertility values varied significantly. The influence of traditional fertility culture, such as “raising children for old age” and “more blessings with more children” on fertility intention was gradually fading.
One child is enough. I don’t want to have another child. When we get old, my husband and I will accompany each other. When the child grows up, he will have his wonderful world. I can’t think of relying on him for retirement. (terminate pregnancy) (N3)
My husband and I have a very good relationship. We hope to raise two children, a boy and a girl, together. The pregnancy came like a sudden, but we were looking forward to the baby. (continue pregnancy) (N7)
A child can’t live in a loveless family. My husband and I are not close together and always argue. I won’t consider having another child. (terminate pregnancy) (N2)
However, a significant number of women was vague or undermined on whether to have a child. When facing an unintended pregnancy, they appeared highly anxious and agitated.
Oh, I’m really stuck with work right now—I’m swamped and not sure what to do. It is difficult to decide. (continuation pregnancy) (N6)
I don’t know if my husband still wants any kids! I didn’t expect to get an unintended pregnancy. It is a little hard to choose. (terminate pregnancy) (N8)
I truly wish to have another child, yet I’m worried that I am too old to do so. I’m not sure if I have the courage to go through with it! (continue pregnancy) (N10)
Impact of Fertility Policies
Under the influence of the previous national one-child policy, some married women have developed a fixed fertility concept.
My parents have only one child, me. I feel very happy. At present, my child is still young, so I don’t consider having one more child. If I change my mind later on, I’m not too late to get pregnancy again. (terminate pregnancy) (N2)
Everyone around me has only one child. I think the children in these families are very happy and can get the love of their parents. So, I’m not thinking about to have an additional child. (terminate pregnancy) (N5)
Women’s Role Conflicts
Due to traditional culture in China, child and family care is typically thought to the responsibilities of women. When suddenly realizing they were pregnant, they had to incorporate the roles of pregnant woman and nursing mother into their already balanced family roles. Such conflicts often affected their childbirth choice.
The family burden between men and women is unfair right now. I don’t want to be a fertility machine. I have my life pursuit and ideals. Now, if I have a baby, everything could change. (terminate pregnancy) (N4)
Is my value just being to have children? Do I have to give up my job and take care of my family? I want be like a man to work through my value. (terminate pregnancy) (N5)
Subjective Norms
Subjective norms are expectations or stresses individuals observe and perceive from spouses, parents, friends, and society. Women’s perception of spouses, parents, friends, society, and other close members about the attitude towards having children, particularly the spouse’s reproductive preference and emotional support degree, can affect their fertility intentions, thus affecting their reproductive decisions.
Perspectives of Friends and Family
Women’s perceptions of their spouse, children, parents, and other close family members play a significant role in decisions about childbirth. Specifically, a spouse’s reproductive preferences and emotional support can significantly influence reproductive choices. Women may also consider the opinions and experiences of other women within their age group.
My husband and I are looking forward to this baby. Unplanned pregnancy gave us a huge surprise. (Continue pregnancy) (N7)
My parents are getting old. Although they say they will help to take care of my children, I don’t want to bother them. (terminate pregnancy) (N9)
My family wants me to have another child, but no family around us have three children. It would always feel weird if we have one additional child. (terminate pregnancy) (N11)
Most of my friends say that one child is good enough. I also agree with this. (terminate pregnancy) (N12)
Social Fertility Atmosphere
Women may internalize societal norms about fertility, incorporating these into their values and adjusting their desire to have children accordingly. Public opinion can also influence their reproductive choices. Meanwhile, social media platforms, such as TikTok, can also significantly influence women’s perception on potential reproductive risks, thereby shaping their reproductive choice-making.
Currently, television and online media extensively emphasize the pressure associated with raising boys, particularly the pressure of purchasing housing in large cities. I have two boys now. I really can’t afford to have an additional child. (terminate pregnancy) (N12)
I have encountered claims on TikTok stating that men are the primary beneficiaries of marriage, while the greatest injustice faced by women in marriage is childbirth. I believe that my decision was influenced by these claims. (terminate pregnancy) (N3)
I saw women who gave birth to children in the TikTok. Their hair is messy, completely do not pay attention to their figures. I don’t want to become an out-shaped, middle-aged woman. (terminate pregnancy) (N11)
Perceived Behavioral Control
Perceived behavioral control denotes an individual’s awareness of the factors that might enable or hinder their ability to achieve certain behavioral objectives. This concept encapsulates women’s assessment of the direct and indirect costs associated with childbirth and their evaluations of their capacity to surmount these cost-related challenges.
Pregnancy-Related Health Factors
Previous negative reproductive experiences and concerns about potential adverse pregnancy outcomes may lead women to prefer opting out of childbirth altogether. The fact that some pregnancies occur despite the use of contraception has led women to worry about the health of their fetuses. More critically, a decline in physical fitness and reproductive capability associated with aging can weaken their intention to conceive. Several women described their desire of more support from health professionals to make reproductive decisions.
I had an extremely terrible experience when I gave birth to my son. These memories are so miserable. The memories are so scary. I fear that an abortion is also painful. (terminate pregnancy) (N5)
I’m 38 years old and in an advanced maternal age. I have great concerns regarding the potential development of severe complications during pregnancy and childbirth. Furthermore, my current pregnancy is unplanned, despite having used contraceptive medications. I am worried that continuing with this pregnancy may have adverse impacts on the fetal health. (terminate pregnancy) (N12)
I had cesarean sections and two induced abortions before. This unintended pregnancy makes me worried about my body, and I desperately need someone to help me. An induced abortion may be the best option. In any case, no one can be certain whether prior contraceptive measures can have any impact on the fetus. (terminate pregnancy) (N9)
During the delivery of my daughter last year, I experienced some unpleasant incidents at home and also had a poor postnatal recovery. Currently, my physical condition, particularly my mental state, does not allow me to have a second child. (terminate pregnancy) (N2)
Women with unintended pregnancies might use medication during conception. In addition, the impact of advanced age on the fetus was another concern in these women. All of these factors could make them concerned about the child’s physical well-being and mental growth.
I desire to have a baby, yet I had no option. Having just received the cervical cancer vaccine, I feared it might harm the baby. (terminate pregnancy) (N2)
I am very busy at work during this time. I often stay up late and drink a lot of coffee. I dare not to have a child, what if it has an impact on the child? (terminate pregnancy) (N4)
I am too old to have another child. Doctors also said that advanced age is very dangerous! It will bring a lot of trouble if the child has a congenital disease. (terminate pregnancy) (N11)
Financial Pressure of Child-Rearing
The childbirth decision-making could be marked impacted by the monetary situations. Raising a child could cause considerable financial burden. High expected costs could weaken and restrict the fertility desire of women.
I already have two children. The family is very crowded. We can’t afford to buy another house. My financial condition does not allow me to have one more child. (terminate pregnancy) (N4)
I already have two boys now. The cost of raising children in modern society is getting higher and higher, especially for the education. With our family’s current financial condition, we can’t afford it. (terminate pregnancy) (N12)
Now, with only one child, I already have a lot of pressure. If we have another child, our living standard would definitely decline. (terminate pregnancy) (N8)
Concerns About Family Care
Spousal involvement in child-rearing and parental assistance can enhance women’s control beliefs and encourage their desire to continue a pregnancy. Conversely, the lack of such support can diminish their desire to have another child.
If the child’s grandparents are willing to help take care of the child, I will consider having another child. (Continue pregnancy) (N1)
There are many problems with the elderly taking care of children. I am not particularly relieved. (terminate pregnancy) (N9)
My husband is too busy to help take care of the children. (terminate pregnancy) (N11)
Lack of Supportive Work Environment
The work environment represents an uncontrollable factor when women decide to have another child. Work-family imbalances can reduce satisfaction both at home and at work. When faced with a less favorable work environment, women often opt to terminate their pregnancies.
My job is a teacher. Having one more child has little impact on my work. (Continue pregnancy) (N10)
I want to get promoted in my career. Having a baby will seriously affect my career plans. (terminate pregnancy) (N3)
Taking maternity leave may lead to a significant reduction in my income. After going back to work, I can only find less desirable jobs with low pay. This will greatly reduce my quality of life. (terminate pregnancy) (N9)
Discussion
In this qualitative study, we utilized the TPB framework and interviewed women with unintended pregnancies to understand their childbirth decision-making process. Various factors can affect decision-making processes in these women. These results could provide a foundation for healthcare providers to enhance the healthcare and support available to these women and their families, who require assistance and guidance when making difficult childbirth decisions under the circumstances of unintended pregnancy.
Our study found that all these women with unintended pregnancies experienced a tough decision-making process. They were eager to decide on this important issue, reflecting a positive coping and help-seeking process.5,6 Prior relevant studies have demonstrated that the assessment and decision-making process could be influenced by diverse factors in women with unintended pregnancies.11 The women commonly described this experience as an isolated journey, during which their values might not be fully appreciated.25 In order to help women make appropriate decisions to meet their personal and family needs, health professionals need to be aware of the loneliness described by the women.25 However, this was often overlooked during the decision-making, especially not in the literature related to the medical care.
With the implementation of the childbirth encouragement policy in China, family planning has a new connotation. Women are provided with comprehensive, full-course, and multi-angle reproductive health services, including necessary contraception and birth control, prenatal and postnatal care guidance, fertility assessment, infertility diagnosis and treatment, and disease prevention and treatment to enhance their fertility care.26 This also aligned with the mission of the International Fertility Education Initiative, which encourages educational efforts to boost fertility and reproductive health awareness.27 With this situation in mind, healthcare providers should further strengthen their focus on the reproductive health of women with unintended pregnancies and incorporate its protection into key service areas. On the one hand, they should offer standardized pregnancy counselling, necessary prenatal examinations, and when indicated, safe protocols for pregnancy termination to maximize the safety of pregnancy. On the other hand, they should systematic and reliable health education on contraception and offer long-term support to help women prevent future unintended pregnancies and achieve autonomous fertility planning in the future.
Notably, in this study, “quality of marriage and partnerships” was identified as a significant factor influencing attitudes toward unintended pregnancy. Marital satisfaction and the strength of spousal relationships played a crucial role in the decision to continue a pregnancy.28 In-depth interviews by Wei et al with ten mothers in Chongqing, China, revealed that women dissatisfied with their marriages and partner relationships were hesitant to have more children, even if they had sufficient financial resources, healthcare, and workplace support.29 Besides, regarding fertility concepts, Chinese women increasingly embrace delayed marriage and childbearing, opting for fewer but better-quality births, and show no preference for the child’s sex.30 The concept of childbirth among Chinese women has evolved from traditional views of “passing on the family line” and “bringing up children for being looked after in old age” to modern perspectives that emphasize childbirth as an “emotional experience”, “spiritual needs”, and “the pledge of love”.31,32 Cultural concepts, rather than the cost of living, were the primary factors influencing childbirth decisions in women with unintended pregnancies.30,33 Although previous research reported that most married Chinese women did not plan to have large families, they were open to the idea of an additional child if it occurred,9 a finding supported by our study here. Healthcare providers should acknowledge the impact of emotional and reproductive attitudes on women’s reproductive decision-making and provide more targeted support measures to help women make informed and appropriate choices regarding their reproductive health.
Moreover, some participants displayed hesitant or uncertain fertility intentions, reflecting the complex emotions and confusion faced by these women in their reproductive decision-making.34 In such uncertain environments, ambivalence and hesitation in making fertility decisions are common.7 From the perspective of fertility support, unintended pregnant women who were “may be born” or “not fully considered yet” were more likely to adjust or change their birth plan compared with those who were “definitely not born”.35 Accurate capture of this information is essential to assess the desire for childbirth intention and help pregnant women make appropriate decisions. Adequate support from partners could play a crucial role in alleviating the pressure on women to make reproductive choices.5 It is essential for women experiencing an unintended pregnancy to have adequate access to reliable, targeted, and evidence-based counseling services and strong supportive care to facilitate their informed decision-making regarding the future of the pregnancy.
Procreation is not only an individual or family decision-making process but also a social issue. Women’s reproductive decisions are influenced not only by their spouses, relatives, and friends but also by the broader social fertility atmosphere.10,11,36 Our study indicates that while the fertility views of spouses and parents exert minimal influence on these norms, the impact of social fertility atmospheres and media platforms is increasingly pronounced. In recent years, some new media platforms have significantly altered some women’s fertility values.37 Social media channels disseminate information about the challenges of childbirth and parenting, controversial policies, and negative news about marriage and fertility.38,39 Women may consider the opinions and experiences of their peers and even internalize popular internet-based fertility concepts into their personal values, continually adjusting their fertility intentions.32 Additionally, the quest for independence and equality among women can lead them to be particularly susceptible to influence by information found online.32 As an informal communication platform, the internet significantly boosts women’s awareness of potential fertility risks.32 It may also unintentionally change their perceptions of fertility and exert a biased impact on their fertility intentions.38–40 A study found that the perception of childbirth in China was more pessimistic, even though the fertility rate was already low.33 In China, women not only underestimated the changes in the fertility rate but also held negative attitudes toward childbirth, which could restrict the women’s fertility intention. Our study also confirmed this. Thus, healthcare professionals should promptly acknowledge women’s concerns and anxieties, and respond in a timely manner to their worries about any questions related to fertility. Moreover, healthcare providers can use the fertility network information service platform to deliver high-quality fertility education, thereby effectively addressing women’s needs, facilitating access to parenting resources, and alleviating fertility-related anxiety,5,41 which might be more important for women with unintended pregnancy who are trying to make an appropriate decision.
Past childbirth experience and uncertainty about future delivery would act as a perceived behavior, prompting unintended pregnant women to make a trade-off between “cost” and “benefit”, which in turn affected their reproductive decisions.15 In this study, we found that decreased physical fitness and reproductive ability, child-raising responsibility pressure, concerns about family support, and lack of friendly workplace environments weakened the fertility control beliefs of unintended pregnant women. Among them, “health status” became the negative control belief that influenced the reproductive decision of women with unwilling pregnancy. Some studies have shown that the incidences of abnormal menstrual cycles, psychological anxiety, and depression in women with several children were significantly higher than those of women with one child.42,43 Other studies have also shown that the high psychological stress level of women during pregnancy was an important factor causing spontaneous abortion, and the most important psychological pressure came from worrying about the health of their children and work pressure.44,45 Healthcare practitioners can acknowledge their experiences and alleviate the discomfort associated with pregnancy and childbirth by discussing and applying appropriate labor analgesia.46 In addition, during the prenatal visit, care should be taken to detect and monitor potential pregnancy complications for prompt management.5
Work-family conflict could present a major challenge for pregnant women who continued working during pregnancy.5 Roughly 75% of mothers indicated experiencing moderate to severe tensions between their jobs and raising children.47 This conflict is particularly acute for women with unintended pregnancies, as the sudden realization of pregnancy forces them to consider additional burdens and limitations on their career development. Consequently, a large number of women opt to have fewer children to minimize their challenges in the labor market. Therefore, in addition to the proactive measures taken by the government, healthcare providers should provide more effective parenting support to women with unintended pregnancy and their families, in order to alleviate work-family conflicts, enabling them to make well-informed reproductive health decisions.
Limitations
Our study has certain limitations. Firstly, the research participants were enrolled exclusively from a tertiary hospital in China, restricting the result generalizability. Additional investigations across different countries and cultural contexts are necessary to gain insight into regional and cultural variations in how women with unintended pregnancies make decisions. Secondly, this study focused on married and parous women. Unmarried or nulliparous women with unintended pregnancies may face different burdens and pressures, resulting in distinct experiences and childbirth decisions that require further exploration. Thirdly, we did not consider demographic factors that might influence participants. Future research could explore how different demographic characteristics impact reproductive decisions among women with unintended pregnancies.
Conclusion
Women are eager to make informed decisions regarding unintended pregnancies. Factors such as fertility values, social fertility atmosphere, health, financial and work status, and family support significantly influence their decisions. A collaborative effort from society, healthcare providers, and families is essential to support these women in making appropriate decisions. Healthcare providers should receive necessary training to expand their skills and knowledge, enabling them to provide adequate support and care for unwanted pregnant women in making well-informed, suitable decisions regarding their reproductive health.
Data Sharing Statement
The datasets produced and analyzed in this study are kept confidential in order to safeguard participants’ anonymity. However, they can be obtained from the corresponding author with a reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was granted by the Ethics Committee of DongGuan Maternal and Child Health Care Hospital (No. 2024-14) on 12 April 2024, and informed consent was obtained from each participant. Interview participants were provided with a study fact sheet and informed consent was obtained at the beginning of each interview. Participants consented to participation and audio recording of the interview. The conduction of the study complied with the Declared of Helsinki.
Consent for Publication
All data published here are under the consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by 2025 Higher Education Reform Project of Guangdong Province (202430553), 2025 Natural Science Foundation of Guangdong Province, Guangdong (2025), 2023 Guangdong Postgraduate Education Innovation Program Project (Grant No. 2023ANLK_018), 2022 Teaching Quality and Teaching Reform Project (Grant No. ZL2022007), 2021 Educational Science Planning Project (Higher Education) (Grant No. 2021GXJK163), Humanities and Social Sciences Project of Guangdong Maoming Health Vocational College (Grant No. MJZYr2022008).
Disclosure
Dan Qiu and Yinting Zou are co-first authors for this study. The authors declare no competing interests in this work.
References
1. Eftekhariyazdi M, Mehrbakhsh M, Neamatshahi M, Moghadam MY. Comparison of pregnancy complications in unintended and intended pregnancy: a prospective follow-up study. Biomedicine. 2021;11(4):51–56. doi:10.37796/2211-8039.1192
2. Nelson HD, Darney BG, Ahrens K, et al. Associations of unintended pregnancy with maternal and infant health outcomes: a systematic review and meta-analysis. JAMA. 2022;328(17):1714–1729. doi:10.1001/jama.2022.19097
3. Navigating the demographic shift: an examination of China’s new fertility policy and its implications. Front Political Sci. 2023.
4. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020;8(9):e1152–e1161. doi:10.1016/S2214-109X(20)30315-6
5. Zhang Y, Jin A, Zhu J. Stress response to fertility decisions of married and parous women with unexpected pregnancy: a three month study at tertiary suzhou hospital, China. Clin Exp Obstet Gynecol. 2023;10(50):208. doi:10.31083/j.ceog5010208
6. Brauer M, Van Ditzhuijzen J, Boeije H, van Nijnatten C. Understanding decision-making and decision difficulty in women with an unintended pregnancy in the Netherlands. Qual Health Res. 2019;29(8):1084–1095. doi:10.1177/1049732318810435
7. Kirkman BL, Chen G, Farh JL. Individual power distance orientation and follower reactions to transformational leaders: a cross-level, cross-cultural examination. Acad Manage J. 2009;52(4):744–764. doi:10.5465/amj.2009.43669971
8. Jing W, Liu J, Ma Q, Zhang S, Li Y, Liu M. Fertility intentions to have a second or third child under China’s three-child policy: a national cross-sectional study. Hum Reprod. 2022;37(8):1907–1918. doi:10.1093/humrep/deac101
9. Yao Y. Research on influencing factors of college teachers’ second child fertility intentions--Taking Jinan as an example. PLoS One. 2024;19(5):e0299838. doi:10.1371/journal.pone.0299838
10. Yong MQY, Yeo Y, Shorey S. Factors affecting unintended pregnancy resolution from the perspectives of pregnant women and people: a systematic review of qualitative evidence. Midwifery. 2023;127:103866. doi:10.1016/j.midw.2023.103866
11. Klann EM, Wong YJ. A pregnancy decision-making model: psychological, relational, and cultural factors affecting unintended pregnancy. Psychol Women Q. 2020;2(44):170–186. doi:10.1093/jbi/wbz051
12. Boivin J, Buntin L, Kalebic N, Harrison C. What makes people ready to conceive? Findings from the International Fertility Decision-Making Study. Reprod Biomed Soc Online. 2018;6:90–101. doi:10.1016/j.rbms.2018.10.012
13. Ajzen I. The theory of planned behavior. Organ Behav Human Decision Processes. 1991;2(50):179–211. doi:10.1016/0749-5978(91)90020-T
14. Bosnjak M, Ajzen I, Schmidt P. The theory of planned behavior: selected recent advances and applications. Eur J Psychol. 2020;16(3):352–356. doi:10.5964/ejop.v16i3.3107
15. I A, K J. Fertility intentions: an approach based on the theory of planned behavior. Demograph Res. 2013;29:203–232.
16. Alizadeh T, Moodi M, Salmani F, Moudi A. Factors affecting childbearing intention in women employees in Birjand: application of the theory of planned behavior. J Educ Health Promot. 2023;12:446. doi:10.4103/jehp.jehp_1379_22
17. Sahraei M, Kohan S, Mohebbi-Dehnavi Z, AbdiShahshahani M. The effect of single-child couples’ education based on the theory of planned behavior on their intention to have next child. J Educ Health Promot. 2024;13:183. doi:10.4103/jehp.jehp_505_23
18. Matera C, Dommermuth L, Bacci S, Bertaccini B, Minello A, Vignoli D. Perceived Economic Uncertainty and Fertility Intentions in Couples: a Dyadic Extension of the Theory of Planned Behaviour. J Fam Econ Issues. 2022;44(4):1–17. doi:10.1007/s10834-022-09872-x
19. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
20. Yr K. Case Study Research: Design and Methods. Sage; 2009.
21. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
22. Zou Y, Lan Q, Chen L, Yao Z, Zhai J. Undergraduate midwifery students’ experiential learning of perinatal bereavement care: a qualitative analysis. Nurse Educ Today. 2024;141:106324. doi:10.1016/j.nedt.2024.106324
23. Chen W, Zhai J, Yuan C, et al. Dietary habit and lifestyle of postpartum women in South China: a mixed methods research. BMJ Open. 2024;14(10):e082998. doi:10.1136/bmjopen-2023-082998
24. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice.
25. Kjelsvik M, Sekse R, Moi AL. Women’s experiences when unsure about whether or not to have an abortion in the first trimester. Health Care Women Int. 2018;39(7):784–807. doi:10.1080/07399332.2018.1465945
26. Gu XY, Zhang YS. Chinese journal of practical gynecology and obstetrics. Chin J Practical Gynecol Obstetrics. 2021;08(37):793–794.
27. Harper JC, Hammarberg K, Simopoulou M, et al. The international fertility education initiative: research and action to improve fertility awareness. Hum Reprod Open. 2021;2021(4):hoab031. doi:10.1093/hropen/hoab031
28. Li Z, Wu YJ. Studies on socialism with Chinese characteristics. Studies Social Chinese Characteristics. 2022;(Z1):84–94.
29. Yang T, Wu YJ, Han N. Chinese women’s concept of childbirth based on the social media topic “what does childbirth mean to a woman”: content and thematic analysis. JMIR Pediatr Parent. 2024;
30. L L, W P. Factors influencing fertility intentions among Chinese women: policy changes, feminist values, and considerations of personal benefit. J Simul. 2024;12(1):13.
31. Ranjbar M, Rahimi MK, Heidari E, et al. What factors influence couples’ decisions to have children? Evidence from a systematic scoping review. BMC Pregnancy Childbirth. 2024;24(1):223. doi:10.1186/s12884-024-06385-3
32. Chen SJ, Shen JH, Jiang QJ. Underestimating others’ fertility attitudes and behaviors hinders the fertility intentions of childless individuals in Gen Z. Acta Psychologica Sinica. 2024;06(56):759–779.
33. Chen W, Lm M. Research on the problem of low birth rate of youth under the background of three-child policy. China Youth Study. 2022;03:5–14.
34. Qs S, Wen M. Chinese Journal of Population Science. Chin J Population Sci. 2024;38(02):82–97.
35. Jones RK. Are Uncertain Fertility Intentions a Temporary or Long-term Outlook? Findings from a Panel Study. Womens Health Issues. 2017;27(1):21–28. doi:10.1016/j.whi.2016.10.001
36. Harvey-Knowles JA. An examination of women’s decision-making processes during unplanned pregnancy. Qual Res Rep Commun. 2012;1(13):80–87. doi:10.1080/17459435.2012.722165
37. Liu P, Cao J, Nie W, Wang X, Tian Y, Ma C. The influence of Internet usage frequency on women’s fertility intentions-the mediating effects of gender role attitudes. Int J Environ Res Public Health. 2021;18(9).
38. Ning C, Wu J, Ye Y, Yang N, Pei H, Gao H. How media use influences the fertility intentions among Chinese women of reproductive age: a perspective of social trust. Front Public Health. 2022;10:882009. doi:10.3389/fpubh.2022.882009
39. Li L, L F. Traditional gender concept, information dissemination, women’s fertility desire: a questionnaire survey based on women of childbearing age. J Southwest Univ Nationalities. 2021;(12):146–152.
40. Liu J, Anxiety? TSR. Research on social media usage and female childbirth risk perception. Media Observer. 2022;6:79–86.
41. Yu X, Liang J. Social norms and fertility intentions: evidence from China. Front Psychol. 2022;13:947134. doi:10.3389/fpsyg.2022.947134
42. Bedaso A, Adams J, Peng W, Sibbritt D. The relationship between social support and mental health problems during pregnancy: a systematic review and meta-analysis. Reprod Health. 2021;18(1):162. doi:10.1186/s12978-021-01209-5
43. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
44. Jiang Q, Guo Y, Zhang E, et al. Perinatal mental health problems in Rural China: the role of social factors. Front Psychiatry. 2021;12:636875. doi:10.3389/fpsyt.2021.636875
45. Zhao T, Jhangri GS, Dobson KS, et al. The impact of prenatal mental health on birth outcomes before and during the COVID-19 pandemic in Anhui, China. PLoS One. 2024;19(8):e0308327. doi:10.1371/journal.pone.0308327
46. Qiao J, Wang Y, Li X, et al. A Lancet Commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet. 2021;397(10293):2497–2536. doi:10.1016/S0140-6736(20)32708-2
47. Liu J, Zhou Z. Mothers’ subjective well-being after having a second child in current China: a case study of Xi’an City. Int J Environ Res Public Health. 2019;16(20).
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.