Back to Journals » Risk Management and Healthcare Policy » Volume 16
Perceived Utilization of Leadership Styles Among Nurses
Authors Gashaye M, Tilahun D ![]() , Belay A
, Belay A ![]() , Bereka B
, Bereka B
Received 6 September 2022
Accepted for publication 2 February 2023
Published 11 February 2023 Volume 2023:16 Pages 215—224
DOI https://doi.org/10.2147/RMHP.S388966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Mihret Gashaye,1 Desalew Tilahun,2 Admasu Belay,2 Bayisa Bereka2
1Jimma Medical Center, Institute of Health, Jimma University, Jimma Town, Ethiopia; 2Nursing School, Faculty of Health Science, Institute of Health, Jimma University, Jimma Town, Ethiopia
Correspondence: Mihret Gashaye, Tel +251918314503 ; +251917557279, Email [email protected]
Background: Nurses´ perceptions of leaders´ leadership styles has a significant impact on their well-being. Effective leadership in health care is crucial for improving and enhancing the effectiveness of health care systems. This study aimed to assess the perceived utilization of leadership styles among nurses at Jimma town public health facilities, Ethiopia.
Methods: This facility-based cross-sectional study was conducted with 403 nurses. Data were collected through a self-administered structured questionnaire. Data were entered into Epi-Data version 4.6 and then exported to SPSS version 25. The strength of association was described using unstandardized adjusted β with a 95% confidence interval (CI) and p-value < 0.05.
Results: Of the 422 participants, 403 completed and returned the questionnaire correctly, thus achieving a response rate of 95.5%. Staff nurses perceived that their head nurses fairly often or commonly used transformational leadership styles, with a mean of 2.77± 0.60. The multivariable linear regression analysis model indicated that there was a positive relationship between perceived leadership style and gender, overall organizational commitment, overall job-related stress, overall innovative work behavior, and overall leadership practice. However, there was a negative relationship between perceived leadership style and nurses who had not received previous training on leadership.
Conclusion: This study highlights that transformational leadership is a commonly utilized leadership style by leader nurses. Effective and balanced use of various leadership styles requires knowledge (training), organizational commitment, and innovative work behavior from both leaders and staff nurses. Therefore, a transformational leadership style is key to achieving organizational goals and increasing staff nurses’ productivity.
Keywords: organizational commitment, job-related stress, innovative work behavior, leadership, leadership style, nurses, Jimma, Ethiopia
Introduction
Leadership is a multidimensional process of recognizing goals, influencing people to act, and providing support and motivation to achieve mutually negotiated goals.1 Leadership has a strong relationship with employees, leaders, and accomplishments of organizational goals.2 Leadership style is the way a leader provides direction, motivates people, and implements plans.3 There are different types of leadership style that nurse leaders use when leading staff nurses at health facilities. These styles are autocratic, democratic, bureaucratic, situational, charismatic, visionary, coaching, laissez-faire, transactional, and transformational.4,5 However, most studies group leadership style as a full range leadership model which is categorized into three types of leadership style, transformational, transactional, and laissez-faire,6,7 among which the most preferred and effective is the transformational leadership style.8,9
Transformational leadership style influences followers towards achieving more than what they have planned by using leaders´ skills to influence followers towards achieving goals by changing followers’ beliefs, values and needs.10 It is classified into five categories: idealized influence attributed, idealized influence behaviors, inspirational motivation, intellectual stimulation, and individual consideration.11 The transactional leadership style motivates and directs followers to the leader using rewards and punishment. It is divided into three categories: contingent rewards, active management-by-exception, and passive management.11 A laissez-faire or hands-off leadership style is one in which there is little or no guidance from the leader and the leader gives employees all authority and freedom to work independently.12
The leadership style used by nurse leaders in the healthcare sector influences job satisfaction, job performance, and quality of services.8 Leadership style also influences nurses’ retention in organizations; when leadership style is unfavorable it increases intention to leave; when leadership style is favorable, indicating that a transformational leadership style is in place, it enhances staff retention.13 The lack of an effective leadership style for nurse leaders is a contributing factor for lack of morale and led to staff turnover, staff shortage, and an increase in healthcare setting costs.4,5
Healthcare systems in the world are facing a lot of complex challenges in providing high-quality, safe, and cost-effective care due to ever-changing systems, increases in the costs of healthcare, technology innovation, and patients’ increased disease acuity.14 Nurse leaders are challenged to solve these problems using critical thinking, especially through their leadership style in healthcare.15 In a previous study, the annual turnover rate from nursing jobs was high: for certified nurse assistants it was 74.5% and for registered nurses, 56.1%.16 In addition, intention to leave or stay in the nursing profession is associated with nurse leaders’ utilization of leadership styles.17 However, nurses’ working conditions remain a challenge faced by current healthcare systems because of the shortage of nurses, staff burn-out, and poor leadership in retaining and attracting nurses.18 The current shortage of nurses requires strong, supportive, encouraging, advocating, and inspirational nurse leaders, so an effective leadership style is very important to fight against the current shortage of nurses and minimize stressors in the nursing profession.19 However, many nurse leaders lack the necessary leadership skills to deal with such problems; furthermore, some nurse leaders assume a leadership role by chance as they are appointed based on their clinical expertise rather than leadership skills.20
A study conducted in Saudi Arabia has shown that nurse leaders who use effective leadership styles promote better outcomes, including staff nurses’ job satisfaction and work effectiveness.21 In addition, studies have shown that the transformational leadership style of nurse leaders brings positive outcomes among staff nurses and leads to high quality nursing care and staff nurse satisfaction.4
In African countries, nurse shortages as a result of different factors contributes to the challenge of the role of nurse leaders to utilize effective leadership styles.22,23 Healthcare system failures in sub-Saharan Africa (SSA) are due to weak or ineffective leadership capacity.13,15 Lack of effective leadership style has been identified as a major constraint to scaling up and providing affordable services in low-income countries.24 A study in East Africa indicated that nurse leaders’ participation in health policy was important to influence, communicate effectively, build relationships, feel empowered, and demonstrate professional credibility. However, a significant number are still excluded from making policies and decisions that influence nurse leaders’ abilities.25
Ineffective utilization of leadership style can cause staff turnover of 21%, and low staff nurse satisfaction, reduced productivity, and low effectiveness by 17%, 17.1%, and 17.7%, respectively.26,27 Effective utilization of leadership style has been associated with reduced length of hospital stay and lower rates of medication errors, patient falls, urinary tract infections, and pneumonia. Additionally, it improves the quality of care and patient outcomes, and lowers patient mortality.28,29 There is a dearth of published studies in Ethiopia regarding perceived utilization of leadership style among nurses, to our extent of searching. Thus, the purpose of this study was to assess perceived utilization of leadership style and associated factors among nurses.
Methods and Materials
Study Design, Setting and Period
The study was conducted from August 16 to September 16, 2021 at Jimma town public health facilities. Jimma town is located in Jimma zone, Oromia regional State, at 352 km southwest of Addis Ababa. According to the Central Statistical Agency (CSA, 2012), the total population of Jimma town was 207,573. In the study town, there were 4 public health centers, one general hospital, and one medical center. According to data from the Jimma town health office, there were a total of 39 nurses in the health center. There were 641 nurses in JMC and 57 nurses in Shenen Gibe hospital as reported by human resource management. The total number of nurses in the Jimma town public health facility was 737.
Source of Population and Study Population
This facility-based cross-sectional study was conducted with nurses. Nurses who were working during the study period and worked at least six months before data collection at Jimma town public health facilities were included. However, staff nurses who were on sick leave, annual leave, and maternal leave and head nurses or nurse leaders were excluded.
Sample Size Determination and Sampling Techniques
Sample Size Determination
A single population proportion formula was applied to determine the sample size for this study by considering 95% confidence interval (Z=1.96), 5% margin of error (d=0.05), and 50% population proportion (p=0.5) due to the dearth of published study on this particular topic in Ethiopia. The initial calculated sample size was 384 considering a 10% non-response rate; the final sample size was 422.
Sampling Techniques and Data Collection
To select the study participants, the sampling frame was prepared by having lists of nurses from nursing service director for JMC, matron for Shenen Gibe Hospital, and human resource management for health centers. Finally, study participants were selected using a simple random sampling technique using lottery methods after proportional allocation to each unit. The sample size was distributed to each public health facility proportional to size allocation by using proportional allocation formula.
Data were collected by three trained BSc midwives and supervised by one trained health officer for facilitating data collection and explaining the purpose of the study to each study participant. Continuous monitoring was made by supervisor during data collection. Before actual data collection, the data collection tools were pretested on 21 nurses working at Agaro hospital and health center to measure the internal consistency of the tools, to estimate data collection time, and to make modifications as needed. The internal consistency was checked using Cronbach’s alpha and it was 0.81.
Operational Definition
Mean values of perceived leadership style used between 3.21–4.00 = frequently, 2.41–3.20 = fairly often, 1.61–2.40 = sometimes, 0.81–1.60 = once in a while, and 0.00–0.80 = no leadership styles utilized.30
Study Instruments
Data were collected through a self-administered structured questionnaire. It was adapted from a valid and reliable tool called the Multifactorial Leadership Questionnaire (MLQ-5x),31 job-related stress tools,32 innovative work behavior tools,33,34 organizational commitment tools,35 and leadership practice inventory tools.36 The questionnaire was prepared in English language. The questionnaire contains six sections; the first covers socio-demographic characteristics of the participants (12 items); the second covers MLQ (33 items) and is mainly grouped under three domains (transformational, transactional, and laissez-faire leadership style). The perceived utilization of leadership style was assessed using the MLQ, which is a five-point Likert scale: 0 = not at all, 1 = once, 2 = sometimes, 3 = often, and 4 = frequently. The third section covers organizational commitment (18 items) and is a five-point Likert scale ranging from 1 = very dissatisfied to 5 = very satisfied. The fourth section covers job-related stress (24 items) and is a four-point Likert scale between 1 = never stressful to 4 = always stressful. The fifth section is innovative work behavior (11 items) and is a five-point Likert scale ranging from 1 = never to 5 = very often. The last section contains leadership practice (25 items) rated on a five-point Likert scale between 1 = almost never to 5 = frequently.
Data Quality Assurance
Data collectors were selected from health facilities that were not working in Jimma town’s public health facilities and did not participate in the study. Data collectors and supervisor were trained for one day on the objectives, contents, and procedures of data collection ahead of data collection by principal investigator. The questionnaire was pre-tested on 5% (21 nurses) of the final sample size at Agaro hospital and health center one week a head of the actual data collection period to assess clarity, flow, completeness, and internal consistency. The reliability of the MLQ tool was verified using Cronbach’s alpha and it was 0.81. The completeness and appropriateness of the collected data were cross-checked and reported by supervisor daily. The principal investigator and supervisor closely supervised the process of data collection.
Data Processing, Analysis and Presentation
Data were checked for completeness and consistency, and coded by the principal investigator. Next, they were entered into Epidata manager version 4.6 and then exported to SPSS version 25.0 for analysis. Normality assumption for multiple linear regression was checked and it was at a maximum. VIF was 2.20. Model adequacy was checked using the Kolmogorov–Smirnov test (p-value was 0.097) and it fitted. Both descriptive and analytic analyses were performed. In the descriptive analysis, means, frequencies, and percentages were calculated. In analytic statistics, simple linear regression analysis was used to select candidate variables for multiple linear regression. All variables having p-value <0.25 during simple linear regression were selected for the multiple linear regression. Variables having p-values <0.05 were considered as significant associations with nurses’ perceived utilization of leadership style. The strength of association was described using unstandardized β with 95% CI and p-value. Finally, the results were presented in text, tables, and graphs.
Ethical Considerations
The study was reviewed and approved by Jimma University‘s Ethical Institutional Review Board, Ref. No. IHFPG/368/21. A formal letter from the Institute of Health was obtained and submitted to Jimma town public health facilities to facilitate and acquire their co-operation and permission. All participants were provided with written informed consent to participate in the study. The participation was voluntary and the data obtained was kept confidentially.
Results
Socio-Demographic Characteristics
Although 422 participants planned to be included in this study, only 403 completed the questionnaire fully, which makes a response rate of 95.5%. Among the total study participants, more than half (57.1%) were female. Regarding marital status, 248 (61.5%) of nurses who participated in this study were married. Slightly less than two-thirds (63.8%) of study participants were Oromo in ethnicity. Concerning working units, the top four units in which nurses were working were surgical, medical, pediatric, and emergency, which accounted for 17.4%, 15.9%, 13.9%, and 13.4%, respectively. Regarding leadership training, the majority (89.1%) of nurses had not received training. The mean age of the study participants was 29.20±5.49, with a minimum age of 20 and maximum age of 48 years. The average service years of the study population were 5.36±3.57 years, having a minimum of 10 months and a maximum of 18 years. The minimum monthly salary was 3000 and the maximum was 10,095ETB, with a mean salary of 6345.52±1400.55 (Table 1).
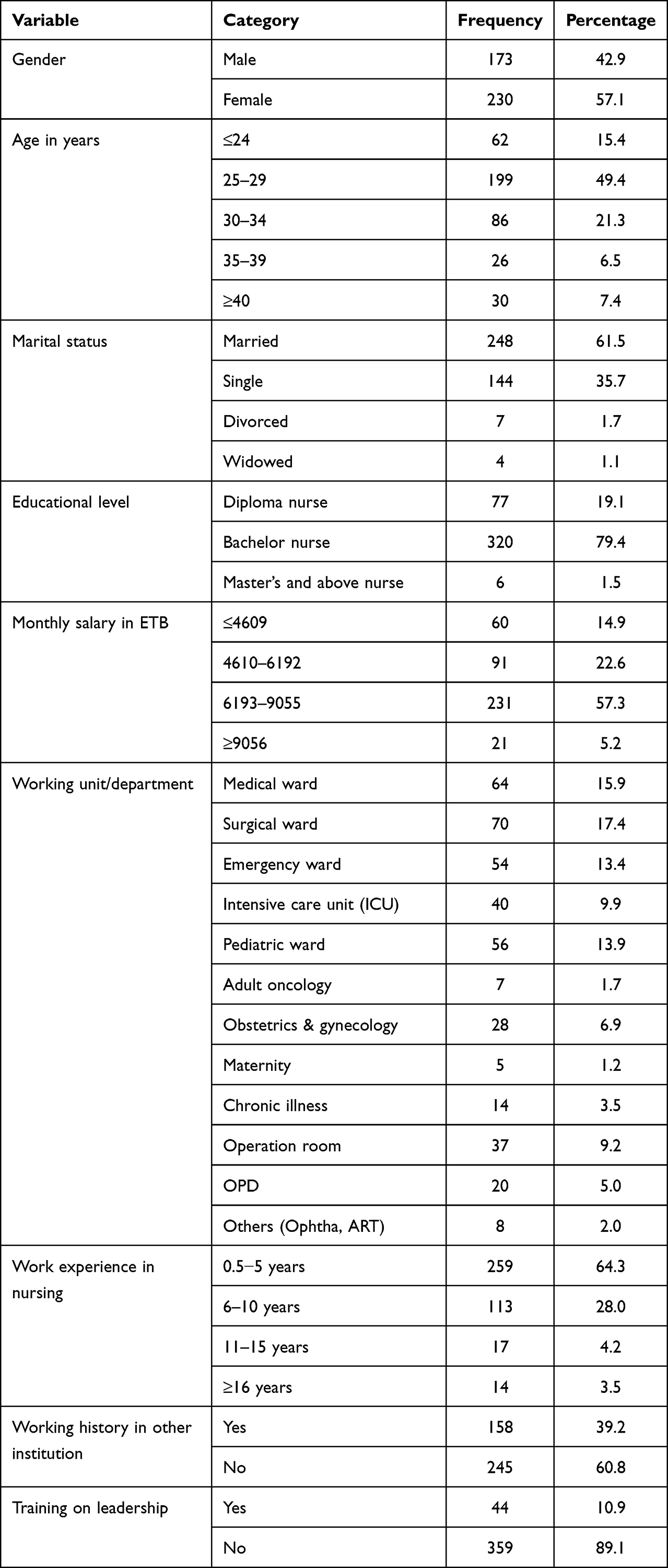 |
Table 1 Socio-Demographic Characteristics of Nurses Working at Jimma Town Public Health Facilities in 2022 |
Perceived Utilization of Leadership Style
As shown in Table 2, the analysis showed that nurses’ perception of their leaders’ utilization of leadership style according to the three leadership styles is as follows: the head nurses fairly often or commonly used the transformational leadership style, with a mean of 2.77±0.60; they used transactional leadership style sometimes, with a mean of 2.23±0.58 and they used laissez-faire leadership style once in a while, with a mean of 1.31±0.56. Moreover, the analysis showed that nurses indicated that their head nurses had used all domains of transformational leadership style equally, with a mean between 2.69 and 2.83, and domains of transactional leadership style in a variable way, ranging from fairly often to sometimes, with a mean score between 1.73 and 2.74. Among the transformational leadership styles, inspirational motivation and idealized influence behavior had highest mean scores. The head nurses had fairly often used a contingent reward leadership style, while they sometimes used active and passive management by exception. The result infers that nurses perceived that their head nurses were using a transformational leadership style more often than transactional and laissez-faire leadership styles (Table 2).
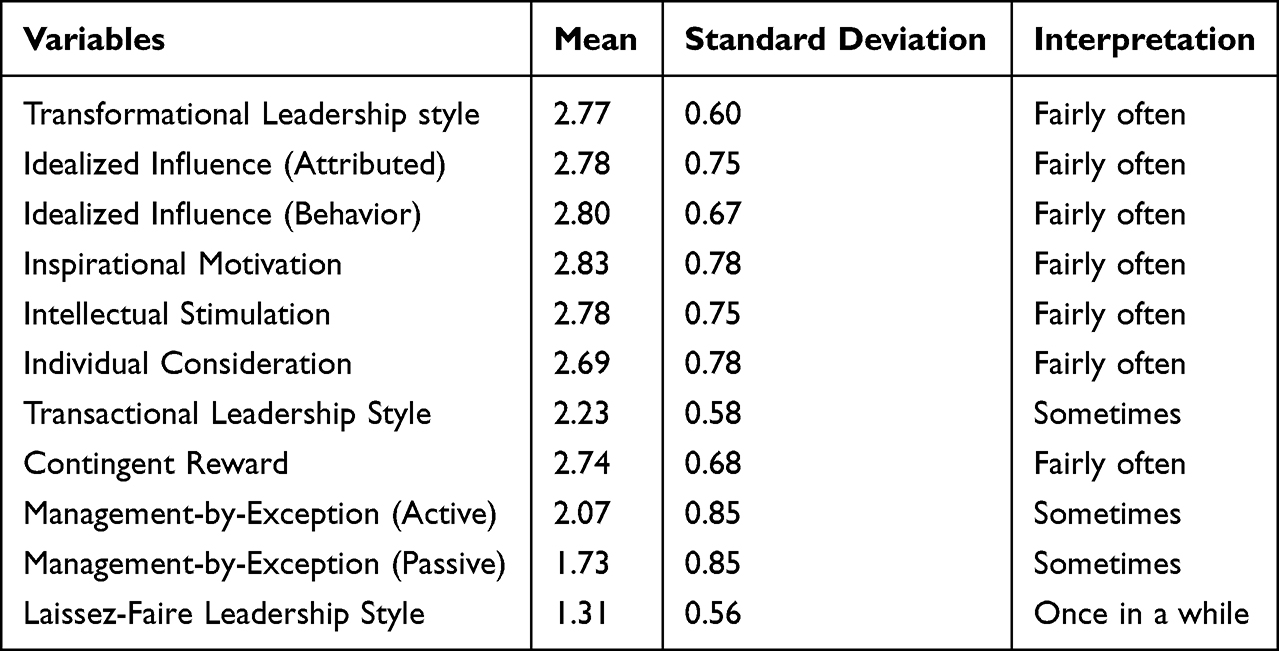 |
Table 2 Descriptive Statistics of Perceived Utilization of Leadership Styles at Jimma Town Public Health Facilities in 2022 |
Factors Associated with Perceived Utilization of Leadership Style Among Nurses
Simple linear regression analysis was done to identify candidate variables for multivariable linear regression. A total of 14 variables were entered one by one: 10 socio-demographic, 1 overall organizational commitment, 1 overall leadership style, 1 overall job-related stress, and 1 overall innovative leadership behavior. From these, 9 variables were selected for multivariable linear regression having a p-value less than 0.25. Accordingly, level of education, marital status, level of healthcare facilities, training on leadership, monthly salary, overall organizational commitment, total job-related stress, overall innovative leadership behavior, and perceived overall leadership practice were candidate variables for multivariable linear regression.
The candidate variables were entered in a multivariable linear regression model and the enter method was used for variable selection. Then, variables having P-values <0.05 were considered as significantly associated with perceived utilization of leadership style. Out of the nine selected candidate variables from simple linear regression analysis, four of them were identified as associated factors with perceived utilization of leadership style on the final model. These include: training on leadership, organizational commitment, innovative work behavior, and job-related stress. However, level of education, marital status, monthly salary, level of healthcare facilities, and perceived leadership practice were not associated with perceived utilization of leadership style.
Accordingly, being a female nurse increased the perceived utilization of leadership style by their leader by 3.87 times more than being a male nurse by keeping the other variables constant (β=3.87 95% CI=1.47, 6.27; p=0.002). An increase in organizational commitment of nurses increases perceived utilization of leadership style by 0.37 (β=0.37 95% CI=0.17, 0.56; p<0.001). The result also showed that increase in innovative work behavior of nurses increases perceived utilization of leadership practice by 039 (β=0.39, 95% CI=0.17, 0.61; p=0.001). However, there was a negative association between nurses who had not received training on leadership and job-related stress with perceived utilization of leadership style. An increase in job-related stress decreases nurses’ perceived utilization of leadership style by 0.13 (β=−0.13, 95% CI=0.02, 0.24; p=0.021). The lack of leadership training for nurses lowers perceived utilization of leadership style by 5.89 times compared to those who had received training (β=−5.89, 95% CI=−9.76, −2.03; p=0.003) (Table 3).
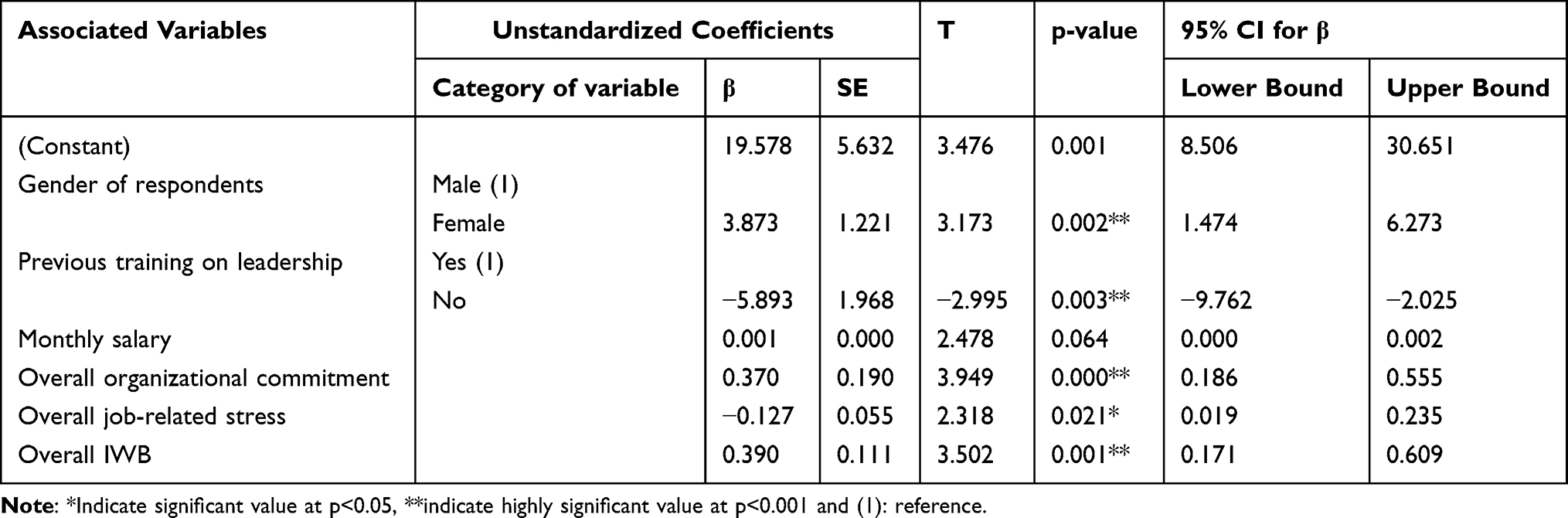 |
Table 3 Multivariable Linear Regression Analysis of Final Model for Study of Perceived Utilization of Leadership Style |
Discussion
The results of this study indicate that the commonly perceived leadership style among nurses at Jimma town’s public health facilities is a transformational leadership style that is fairly often utilized. This indicates that transformational leadership improves client care by increasing staff nurses’ motivation. This result is congruent with studies conducted in Saudi Arabia19,30 and the United States37 but incongruent with a study conducted in Iran, which stated that the dominant head nurses’ “utilized leadership style from [the perspective of] nurses” was transactional leadership.38 This difference may be due to the setup of health institutions and policies. The results of this study demonstrate that staff nurses perceived a transformational leadership style to be utilized more often than transactional and laissez-faire leadership styles. This result is similar to that of previous studies in different areas of Saudi Arabia19,30,39 and the United States.37 Moreover, the results showed that nurses perceived that their head nurses had fairly often used all domains of the transformational leadership style. Among the transformational leadership style inspirational motivation has highest mean score, which is similar to studies conducted in Indonesia40 and Saudi Arabia41 but incongruent with studies conducted in Nigeria9 and the United States;37 while domains of transactional leadership style vary, ranging from sometimes to fairly often. Head nurses have sometimes used active and passive management by exception style and fairly often used a contingent reward style, which is similar to a study conducted in Saudi Arabia.30
The results infers that nurses perceived that their head nurses were using a transformational leadership style more often than transactional and laissez-faire leadership styles. Nevertheless, nurses still have low scores of perception for frequently using these leadership styles since the mean scores of leadership styles in all domains range from once to fairly often.
This study shows that being a female nurse is significantly associated with perceived utilization of leadership style (β=3.87, p=0.002), which is congruent with the study conducted in Spain which states that men obtained lower results than women in perceived leadership style, with p-value 0.015.43 Similarly, a study conducted in Saudi Arabia showed a significant difference in terms of gender between female and male nurses, with p=0.039.19 However, this study result was in contrast to a study conducted in Saudi Arabia which found that male nurses had higher scores than female nurses, with p<0.001.30 This difference may be due to female nurses preferring to emphasize connection and relatedness, whereas male nurses emphasize their power or type of industry in which the makeup of the workforce plays a part in the perception of leadership style utilization.
The findings of this study also show that there is a significant negative association between nurses who had not received previous training on leadership and perceived utilization of leadership style (β=−5.89, p=0.003). Nurses who had not received previous training on leadership had a decreased perception of their leader’s leadership style whereas nurses who had received training had an increased perception of the leadership style utilized in the workplace by head nurses. This result was supported by the study conducted in Saudi Arabia which indicates significant difference in the perception of staff nurses on the nurse managers’ leadership style in terms of training, with p=0.014,19,24 and a study conducted in Arizona has noted the role of education including training on leadership has a positive association.44
This study shows that organizational commitment is statistically significant and positively related to perceived utilization of leadership style (β=0.37, p<0.001), which indicates that nurses who have organizational commitment have increased perceptions of leadership style of their leaders. This finding is consistent with a study conducted in Saudi Arabia that organizational commitment was positively related to transformational leadership style.45 This might be the generation of open communication with leaders that encourages staff satisfaction and retention. Moreover, the results showed that organizational commitment is statistically significant and positively related to transformational and transactional leadership styles but negatively significant with laissez-faire leadership style. This result was similar to that of studies conducted in Saudi Arabia,45 Singapore,42 and Egypt.46
The findings in this study show that job-related stress was a significantly associated factor with the outcome variable of perceived utilization of leadership style (β=-0.127, p=0.021) which was congruent with a study conducted in Pakistan.47 This study result was incongruent with studies conducted in Indonesia48 and Iran.38 This may be due to differences in working settings or climate and healthcare systems.
This study showed that nurses’ innovative work behavior was significantly associated with perceived utilization of leadership style (β=0.39, p=0.001), which is congruent with the study conducted in Pakistan49,50 showing a positive relationship between transformational leadership style and innovative work behavior of nurses. This finding was supported by a study conducted in Egypt,46,51 which stated that there was a statistically significant association between innovative work behavior of nurses and utilization of leadership style. This might be because nurse leaders provide staff nurses with the freedom and autonomy to share creative thoughts and opinions, which fosters the development of nurses’ innovative work behaviors.
In conclusion, the leadership style commonly utilized in the Jimma town public health facility is transformational leadership. Gender, previous training on leadership, organizational commitment, innovative work behavior, and job-related stresses were identified as factors significantly associated with nurses’ perceived utilization of leadership style.
The findings of this study contribute to the body of knowledge on leadership style. Effective and balanced use of various leadership styles requires knowledge (training), organizational commitment, and innovative work behavior from both leader and staff nurses, relevant to client satisfaction. A collaborative approach is needed to employ the most effective leadership styles to improve the quality of nursing care, staff satisfaction, and creation of suitable working environments.
Abbreviations
JMC, Jimma medical center; SPSS, Statistical Package for Social Sciences; CI, confidence interval; SSA, sub-Saharan Africa; WHO, World Health Organization; CSA, Central Statistical Agency; HCs, health centers; IWB, innovative work behavior; MLQ-5x, Multifactorial Leadership Questionnaires; VIF, variance of inflation factor; IRB, institutional review board; ETB, Ethiopian birr; SD, standard of deviation; Df, degree of freedom; SE, standard of error; β, beta; IHFPG, institute of heath facility of post graduate.
Data Sharing Statement
The datasets used in this study are available from the corresponding author upon request.
Acknowledgment
We are grateful to Jimma University, Jimma town public health facility administrative body, and data collectors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Jimma University. This funding organization hadn’t involved or had any role in the design of the study, collection, analysis, interpretation of the data, or and in writing of the manuscript.
Disclosure
All authors declare that they have no competing interests.
References
1. Northouse PG. Leadership: Theory and Practice. SAGE Publications, Incorporated; 2021.
2. Elhajj S. Importance of leadership in administration. Course Fall. 2013;24:548.
3. Memon KR. Effects of leadership styles on employee performance: integrating the mediating role of culture, gender and moderating role of communication. Int J Manag Sci Bus Res. 2014;3:18.
4. Dassanayake D. Leadership style of Nurse Managers. Int J Sci Res Publ. 2014;27:205.
5. Alshahrani M, Baig LA. Effect of Leadership Styles on Job Satisfaction Among Critical Care Nurses in Aseer, Saudi Arabia. J Coll Physicians Surg. 2016;26(5):366–370.
6. Phd DMA, Mohammad P, Almukhtar M. Review: effects of Leadership Styles on Quality of Services in Healthcare. Eur Sci J. 2014;10:18
7. Bass BM, Riggio RE. Transformational Leadership. Psychology Press; 2006:279.
8. Alloubani AM, Abdelhafiz IM, Abughalyun Y, Edris EEM, Almukhtar MM. Impact of Leadership Styles On Leadership Outcome (Effectiveness, Satisfaction And Extra Effort) In The Private Healthcare Sector In Jordan. Int Sci Forum. 2015;13:548.
9. Olu-Abiodun O, Abiodun O. Perception of transformational leadership behaviour among general hospital nurses in Ogun State, Nigeria. Int J Afr Nurs Sci. 2017;6:22–27.
10. Ahmad AR, Adi MNM, Noor HM, Rahman AGA, Yushuang T. The Influence of Leadership Style on Job Satisfaction among Nurses. Asian Soc Sci. 2013;9(9):172. doi:10.5539/ass.v9n9p172
11. Alkahtani AH. The Influence of Leadership Styles on Organizational Commitment: the Moderating Effect of Emotional Intelligence. Bus Manag Stud. 2015;2(1):23. doi:10.11114/bms.v2i1.1091
12. Bass BM, Bass R. The Bass Handbook of Leadership: Theory, Research, and Managerial Applications. Simon and Schuster; 2009.
13. Muhangi B. Leadership style and staff retention in organisations. Int J Sci Res IJSR. 2016;7(5):412.
14. Porter-OGrady T, Malloch K. Quantum Leadership. Advancing Innovation, Transforming Health Care. 3. Painos. Jones & Bartlett Learning, Sudburu MA; 2011.
15. Ledlow GJR, Coppola MN. Leadership for Health Professionals. Jones & Bartlett Learning; 2013.
16. Donoghue C. Nursing Home Staff Turnover and Retention: an Analysis of National Level Data. J Appl Gerontol. 2010;29(1):89–106. doi:10.1177/0733464809334899
17. Cummings GG, Tate K, Lee S, et al. Leadership styles and outcome patterns for the nursing workforce and work environment: a systematic review. Int J Nurs Stud. 2018;85:19–60. doi:10.1016/j.ijnurstu.2018.04.016
18. Wong CA, Spence Laschinger HK, Macdonald-Rencz S, et al. Part 2: nurses’ career aspirations to management roles: qualitative findings from a national study of C anadian nurses. J Nurs Manag. 2013;21(2):231–241. doi:10.1111/j.1365-2834.2012.01451.x
19. Albagawi B, Laput V, Pacis C, AlMahmoud T. Nurses’ perceptions of nurse manager leadership styles. Am J Nurs Res. 2017;5(1):22–31. doi:10.12691/ajnr-5-1-3
20. Perez JWL. Impact of Nurse Managers’ Leadership Styles on Staff Nurses’ Intent to Turnover. Gardner-Webb University; 2014. 46.
21. Asiri SA, Rohrer WW, Al-Surimi K, Da’ar OO, Ahmed A. The association of leadership styles and empowerment with nurses’ organizational commitment in an acute health care setting: a cross-sectional study. BMC Nurs. 2016;15(1):38. doi:10.1186/s12912-016-0161-7
22. Crisp N, Chen L. Global supply of health professionals. N Engl J Med. 2014;370(10):950–957. doi:10.1056/NEJMra1111610
23. Egenes KJ. The nursing shortage in the US: a historical perspective. Chart. 2012;110(4):18–22.
24. Mutale W, Vardoy-Mutale A-T, Kachemba A, Mukendi R, Clarke K, Mulenga D. Leadership and management training as a catalyst to health system strengthening in low-income settings: evidence from implementation of the Zambia Management and Leadership course for district health managers in Zambia. PLoS One. 2017;12(7):e0174536. doi:10.1371/journal.pone.0174536
25. Shariff N. Factors that act as facilitators and barriers to nurse leaders’ participation in health policy development. BMC Nurs. 2014;13(1):1–13. doi:10.1186/1472-6955-13-20
26. Cummings GG, MacGregor T, Davey M, et al. Leadership styles and outcome patterns for the nursing workforce and work environment: a systematic review. Int J Nurs Stud. 2010;47(3):363–385. doi:10.1016/j.ijnurstu.2009.08.006
27. Nyirazigama A. Transformational Leadership Styles and Its Outcomes Among Nursing Staff at Rwanda Military Hospital [Phd Thesis]. University of Rwanda; 2017.
28. Wong CA, Cummings GG, Ducharme L. The relationship between nursing leadership and patient outcomes: a systematic review update. J Nurs Manag. 2013;21(5):709–724. doi:10.1111/jonm.12116
29. JESUS, JESSICA C PARKER. Staff nurse perceptions of nurse manager leadership styles and outcomes - CASIDA - 2011 - Journal of Nursing Management - Wiley Online Library [Internet]. Available from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1365-2834.2011.01252.x.
30. Aboshaiqah AE, Hamdan-Mansour AM, Sherrod DR, Alkhaibary A, Alkhaibary S. Nurses’ perception of managers’ leadership styles and its associated outcomes. Am J Nurs Res. 2014;2(4):57–62.
31. Avolio BJ, Bass BM. Multifactor leadership questionnaire (TM). Mind Gard Inc Menlo Park CA. 2004.
32. Dagget T, Molla A, Belachew T. Job related stress among nurses working in Jimma Zone public hospitals, South West Ethiopia: a cross sectional study. BMC Nurs. 2016;15(1):1–10. doi:10.1186/s12912-016-0158-2
33. Jong JPJ. Individual innovation: the connection between leadership and employees’ innovative work behavior. ZoetermeerEIM; 2007.
34. Kleysen RF, Street CT. Toward a multi-dimensional measure of individual innovative behavior. J Intellect Cap. 2001;2(3):284–296. doi:10.1108/EUM0000000005660
35. Swanepoel H. The Relationship Between Workplace Spirituality and Work Related Attitudes [Phd Thesis]. Welkom: Central University of Technology, Free State; 2015.
36. Kouzes JM, Posner BZ. The Leadership Practices Inventory (LPI): Self Instrument. Vol. 52. John Wiley & Sons; 2003.
37. Bush S, Michalek D, Francis L. Perceived Leadership Styles, Outcomes of Leadership, and Self-Efficacy Among Nurse Leaders:: a Hospital-Based Survey to Inform Leadership Development at a US Regional Medical Center. Nurse Lead. 2020. doi:10.1016/j.mnl.2020.07.010
38. Atashzadeh Shoorideh F, Afshar A, Naderi M. Correlation of head nurses leadership style from nurses’ perspective and nurses’ job stress. J Health Promot Manag. 2015;4(1):72–79.
39. Albagawi B. Leadership styles of nurse managers and job satisfaction of staff nurses: correlational design study. Eur Sci J. 2019;15(3):254–275.
40. Suratno K. The relationship between transformational leadership and quality of nursing work life in hospital. Int J Caring Sci. 2018;11(3):1416–1422.
41. Dahshan DMEAE, Youssef DHAM, Aljouaid M, Babkeir RA, Hassan DWB. Effect of Nurse Managers Leadership Styles on Organizational Commitment of Nurses Working at Taif Governmental Hospitals in Kingdom of Saudi Arabia. Glob J Manag Bus Res. 2017;1:548.
42. Goh AMJ, Ang SY, Della PR. Leadership style of nurse managers as perceived by registered nurses: a cross-sectional survey. Proc Singap Healthc. 2018;27(3):205–210. doi:10.1177/2010105817751742
43. Jodar I Solà G, Gené I Badia J, Hito PD, Osaba MAC, Del Val García JL. Self-perception of leadership styles and behaviour in primary health care. BMC Health Serv Res. 2016;16(1):572. doi:10.1186/s12913-016-1819-2
44. Kelly LA, Wicker TL, Gerkin RD. The relationship of training and education to leadership practices in frontline nurse leaders. JONA J Nurs Adm. 2014;44(3):158–163. doi:10.1097/NNA.0000000000000044
45. Al-Yami M, Galdas P, Watson R. Leadership style and organisational commitment among nursing staff in Saudi Arabia. J Nurs Manag. 2018;26(5):531–539. doi:10.1111/jonm.12578
46. Abd El Muksoud NO, Metwally FG, Ata AA. Leadership Behaviors, Organizational Commitment and Innovative Work Behaviors among Nurses. Ann Romanian Soc Cell Biol. 2021;4227–4245.
47. Hussain M, Akhtar S, Inayatullah MA, Gillani SA. Impact of Leadership Styles on Work Related Stress among Nurses. Saudi J Med Pharm Sci. 2017;907–916.
48. Rindu R, Lukman S, Hardisman H, Hafizurrachman M, Bachtiar A. The Relationship between Transformational Leadership, Organizational Commitment, Work Stress, and Turnover Intentions of Nurse at Private Hospital in Indonesia. Open Access Maced J Med Sci. 2020;8(E):551–557. doi:10.3889/oamjms.2020.4425
49. Umrani WA, Afsar B. How transformational leadership impacts innovative work behaviour among nurses. Br J Healthc Manag. 2019;25(12):1–16. doi:10.12968/bjhc.2018.0069
50. Masood M, Afsar B. Transformational leadership and innovative work behavior among nursing staff. Nurs Inq. 2017;24(4):e12188. doi:10.1111/nin.12188
51. Ahmed AK, Ata AA, Abd-Elhamid ZN. Relationship between the leadership behaviors, organizational climate, and innovative work behavior among nurses. Am J Nurs. 2019;7(5):870–878.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Empowering Leadership: A Journey of Growth and Insight Through a Mentoring Program for Nurses in Leadership Positions
Lysfjord EM, Skarstein S
Journal of Healthcare Leadership 2024, 16:443-454
Published Date: 1 November 2024
Perceptions of Organisational Readiness for Change in Nurse- and Midwifery-Led Quality Improvement Initiatives
Atenchong N, Maweu DM, Wanyama PA, Uwimana C, Ewing H, Ndaimani A
Journal of Healthcare Leadership 2025, 17:851-861
Published Date: 27 December 2025