Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Perceived Stigma and Associated Factors Among People Living with HIV Attending ART Clinics in Public Health Facilities of Dessie City, Ethiopia
Authors Adane B ![]() , Yalew M
, Yalew M ![]() , Damtie Y
, Damtie Y ![]() , Kefale B
, Kefale B ![]()
Received 27 July 2020
Accepted for publication 9 September 2020
Published 7 October 2020 Volume 2020:12 Pages 551—557
DOI https://doi.org/10.2147/HIV.S274019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Bezawit Adane,1 Melaku Yalew,2 Yitayish Damtie,2 Bereket Kefale2
1Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Reproductive and Family Health, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Bezawit Adane
Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Wollo University, PO Box: 1145, Dessie, Ethiopia
Tel +251933558106
Fax +251331190586
Email [email protected]
Introduction: Despite the fact that responses to epidemics of human immune-deficiency virus (HIV) have gradually improved; it remains one of the world’s public health challenges, particularly in low- and middle-income countries. Evidence is still limited in this area and this study aimed to assess the magnitude of perceived stigma and associated factors among people living with HIV (PLWH) in public health facilities of Dessie city, Ethiopia.
Methods: A health facility-based cross-sectional study was conducted among a total of 422 PLWH from September 1 to October 30, 2019 in Dessie city. A pretested structured interviewer-administered questionnaire was used to collect the data and it was analyzed using Stata/SE 14. Multivariable binary logistic regression analysis was used to identify factors associated with perceived stigma. The adjusted odds ratio (AOR) along with 95% confidence interval (CI) was estimated to measure the strength and direction of the association. Statistical significance was declared at P value less than 0.05.
Results: The overall magnitude of perceived stigma among people living with HIV in public health facilities of Dessie city was 41.93% [95% CI: (37.25, 46.75)]. Perceived stigma was positively associated with being female [AOR=2.08, 95% CI: (1.26, 3.46)], living in rural areas [AOR=1.80, 95% CI: (1.10, 2.94)] and not disclosing HIV status [AOR=2.36, 95% CI: (1.19, 4.66)].
Conclusion: In this study, the magnitude of perceived stigma was high as compared to UNAIDS standard, and sex, place of residence, and disclosure of HIV serostatus were significantly associated with perceived stigma. The findings suggested that special emphasis should be placed on rural residents in order to reduce perceived stigma. Moreover, counseling should focus on disclosing HIV serostatus to anyone else interested to disclose particularly for females.
Keywords: stigma, sexually transmitted infections, HIV prevention, HIV, Dessie Ethiopia
Introduction
HIV remains one of the world’s public health challenges, particularly in low- and middle-income countries like Ethiopia.1,2 According to the 2016 Ethiopian Demographic and Health survey, the prevalence of HIV in Ethiopia was 1.2%.3 PLWH faced not only medical problems but also social problems associated with the disease. One of these problems is HIV related stigma which means: prejudice, discounting, discrediting and discrimination directed toward persons having HIV.4,5 Perceived stigma is how PLWH feel when they are negatively treated by partners, family, friends, health care providers and members of their community due to their HIV status and.6,7
A recent study found that evidence-based effective programming to reduce stigma and discrimination had expanded.8 Efforts to reduce stigma related to HIV/AIDS will not only help countries to achieve key strategies of Sustainable Developmental Goal (SDG), it will also protect and promote human rights. Studies conducted in India indicated that perceived stigma ranged from 10% to 97% whereas, only 26% of the PLWH had experienced stigma.7,9 In Iran, a study witnessed that 62% and 98% of participants experienced external and internal stigma, respectively.10 Stigma also reached up to 67.2% in Cameroon and 35% in Nigeria.4,11 Studies conducted in Jimma hospital revealed that 72.2% experienced perceived stigma whereas it was 49.4% in Hawassa.12,13
Perceived stigma greatly affects the quality of life of PLWH, their family members and the healthcare providers who work with them.10 Stigma causes serious care limitations for PLWH and this is an important factor for the HIV epidemic throughout the world.10–12 People who experienced stigma report a range of negative effects, including loss of income or job, isolation from communities, and inability to participate as a productive member of society.14 Stigma also hinders adherence to antiretroviral treatment (ART) and accelerates disease progression.15–17 They were also more likely to develop low self-esteem, accompanied by feelings of anger and revenge, and emotional stress.18 They had a high risk of developing anxiety and other mental disorders.13,19
Those who also experienced felt stigma related to a disruption of their personal lives while mediated by depression were likely to report poor overall health.20 Stigma affects the overall quality of life of PLWH and isolates them from the community.21–25 A study conducted in Cameroon indicated that 23% of the victims lost their job due to stigma and discrimination.26 They are also at a higher risk of suicide.27 It is due to stigma that HIV positive people do not disclose their HIV status.5 A study conducted in Amhara, Ethiopia showed that those who felt stigmatized were more likely to develop distress and depression.7,28–30 A study also indicated that stigma affects access to health care.31 Some studies have shown that aspects of stigma have been reported as factors constituting a serious obstacle for HIV counseling and testing (VCT) service utilization and HIV prevention.32,33
To end the epidemic of HIV by the year 2030, the joint united nation program on HIV/AIDS has set a broad goal agenda calling for the three zeros: no new HIV infection, no new HIV related death and no HIV related stigma and discrimination.34 Perceived stigma could be influenced by socio-demographic characteristics of HIV infected people,6,11,35–37 duration of ART11,37 and time since being diagnosed,14,35,38 family size and wealth,6 CD4 count and being on ART,39 social and family support.38,40,41 Although large numbers of PLWH are found in Ethiopia, the situation of perceived stigma related to HIV has not been addressed. Therefore, this study aimed to assess the magnitude of perceived stigma and associated factors among people living with HIV attending ART clinics in public health facilities of Dessie City, Ethiopia.
Materials and Methods
Study Area, Study Design and Participants
A cross-sectional study was conducted in ART clinics of Dessie city from September 1 to October 30, 2019. Dessie is the center of South Wollo zone located 401 km away from Addis Ababa, the capital city of Ethiopia and 480 km away from Bahir Dar. According to the 2019 Dessie town Administrative Health Office report, two government hospitals and three health centers were providing ART services. Nine thousand seven hundred and forty seven HIV positive people were registered in all public health facilities (5818 in Dessie referral hospital, 904 in Boru hospital, 2152 in Dessie health center, 422 in Buanbwuha health center and 541 in Segnogebeya health center) of Dessie city. All HIV positive people who were registered in ART logbook and who were on ART were included and those participants aged less than 18 were excluded from the study.
Sample Size and Sampling Procedure
The sample size was calculated using a single population proportion formula by taking the proportion of perceived stigma as 49.4% which was conducted in Hawassa.13 Thus, adding 10% for non-response, the minimum required sample size was 422. The sample size was proportionately allocated to each health facility providing ART services based on the average number of client flow per month. Then, the study participants were selected systematically until reaching the sample size.
Data Collection Tools and Measurements
Data were collected by face to face interview using a structured and pretested Amharic version questionnaire. Medical records were also reviewed to identify clinical markers like CD4 count, viral load and World Health Organization (WHO) clinical staging. A very reliable and valid 40-point HIV stigma psychometric assessment scale employed elsewhere was used to measure perceived stigma.42 A score of 0 was given for those who answered “strongly disagree” and “disagree”. A score of 1 was given for those who chose “agree” and “strongly agree”. The scores were summated and a total score greater or equal to 50% was considered as having a stigma. A total score less than 50% was considered as not having a stigma.12
Statistical Analysis
Data were coded and entered into Epi-Data Version 3.1 and exported to STATA/14 for statistical analysis. Descriptive statistics such as frequency, proportion and figure were computed. All independent variables having a p-value less than 0.2 were included in the multivariable binary logistic regression model. Multicollinearity was checked using the standard error and variance inflation factor (VIF). Variables having P value of less than 0.05 were considered as statistically significant predictors of perceived stigma and adjusted odds ratios with 95% confidence interval were also computed to see the strength and direction of association.
Ethical Approval and Consent to Participate
The data were collected after getting Ethical clearance from the Ethical Review Committee of Wollo University College of Medicine and Health Sciences (CMHS). Official letter of cooperation was obtained from each health facility administration. An informed verbal consent was obtained from each participant before their enrollment and the Ethical Review Committee also approved verbal consent with the ethical approval number CMHS/398/02/2011. This study was conducted in accordance with Helsinki Declaration and the data collection procedure was anonymous for keeping the privacy and confidentiality of any information.
Result
Socio-Demographic Characteristics of Participants
Four hundred and fifteen people living with HIV participated in this study, making the response rate 98.3%. More than half (50.36%) of the respondents were aged less than 35 years and one out of ten were aged greater than 44 years. Again more than half (55.90%) of the participants were females. Three hundred and twenty three (77.83%) of the respondents were urban dwellers. Concerning their educational status, nearly one quarter (23.37%) of the participants was not formally educated. Lastly, one hundred and ninety two (46.26%) of the respondents were below the middle wealth quintile (Table 1).
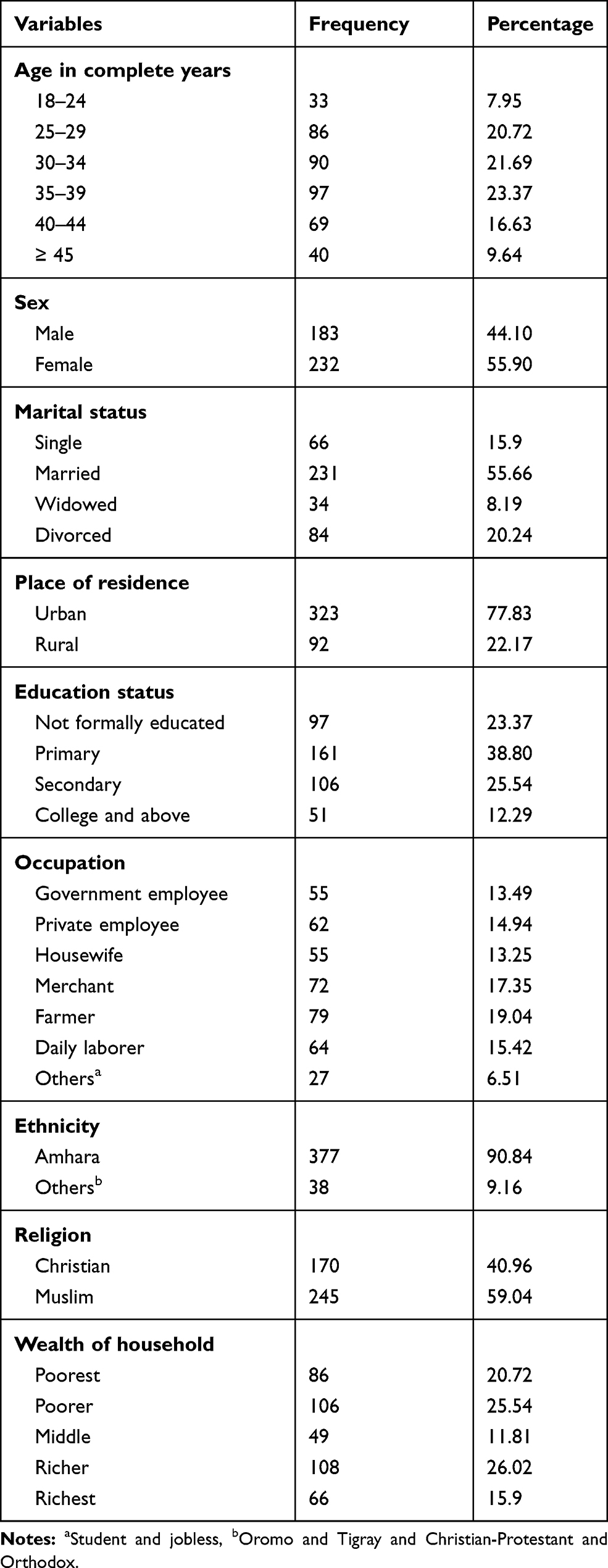 |
Table 1 Socio-Demographic Characteristics of People Living with HIV in Public Health Facilities of Dessie City, Ethiopia, 2019 |
Magnitude of Perceived Stigma Among People Living with HIV
The overall magnitude of perceived stigma among people living with HIV was 41.93% [95% CI: (37.25, 46.75)] (Figure 1).
 |
Figure 1 Magnitude of perceived stigma among people living with HIV in public health facilities of Dessie city, Ethiopia, 2019. |
Factors Associated with Perceived Stigma Among PLWH
The multivariable analysis result showed that sex and residence of participants and disclosing HIV status to anyone else interested were found to have a significant statistical association with perceived stigma in PLWH. The odds of perceived stigma among female people living with HIV were 2 times higher than their counterparts [AOR=2.08, 95% CI: (1.26, 3.46)]. Those HIV infected people who lived in rural area also had 1.7 times higher risk of developing perceived stigma as compared to urban dwellers [AOR=1.80, 95% CI: (1.10, 2.94)]. Lastly, the odds of developing perceived stigma were 2 times higher in those who did not disclose their HIV serostatus [AOR=2.36, 95% CI: (1.19, 4.66)] (Table 2).
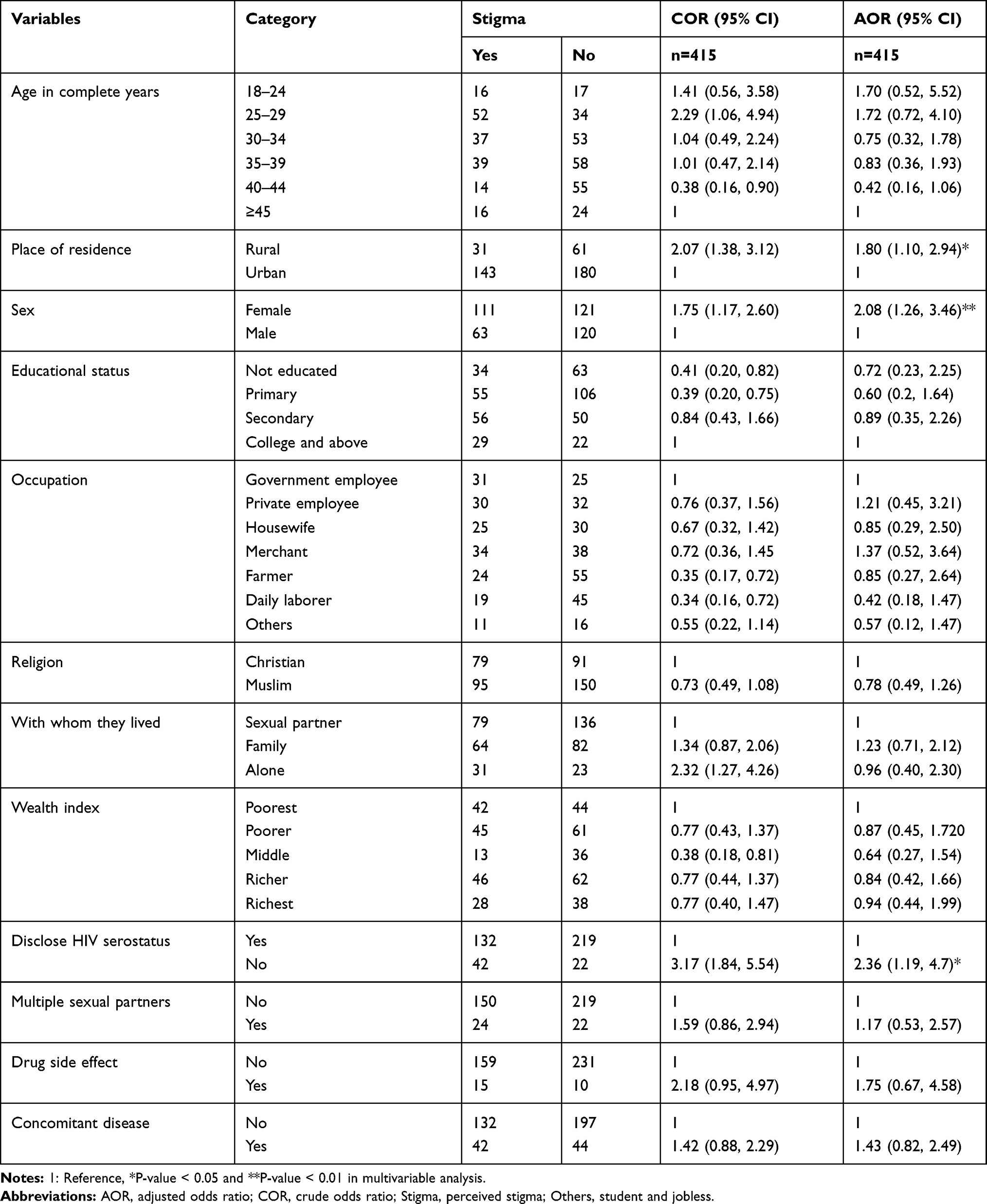 |
Table 2 Regression Model for Factors Associated with Perceived Stigma Among People Living with HIV in Health Facilities of Dessie City, 2019 |
Discussion
In this study the magnitude of perceived stigma was 41.93% [95% CI: (37.25, 46.75)]. Variables like sex and place of residence of respondents and disclosing HIV serostatus were significantly associated with perceived stigma. The magnitude of perceived stigma is lower than in the previous studies conducted in Hawassa and Jimma, Ethiopia.12,13 But, it is higher than a study conducted in Nigeria and Botswana.4,43 Whereas, it is also lower than studies conducted in Cameroon and Iran.10,11 The possible reason for this discrepancy may be due to time variation and different context especially with those studies being outside Ethiopia. It may also be due to different governmental and non-government interventions.
The finding also revealed that females were more likely to have perceived stigma. This is also supported by a previous study conducted in Jimma, Ethiopia.6 The finding is also in line with a study conducted in Uganda.37 The possible reason for this association may be due to frequent history of exposure to high risk things and females were less stable emotionally and had low self-esteem as compared to males.44
The odds of perceived stigma among rural residents were more than that of their counterparts. The finding is in agreement with a study conducted in Arbaminch, Ethiopia.45 It is also similar to a study conducted in Iran.38 The possible reason for this association may be due to cultural beliefs and practices that would magnify its effect which may persist in rural residents. It may also be due to poor knowledge regarding its cause as they may think of it as a sign of sin, and different misconceptions were found in rural residents. Even though cultures should be respected, all cultural practices and beliefs are not useful, particularly in Ethiopia. So, information, education, communication, and behavioral change communication would be necessary to address those bad cultural practices.
The other finding was that those who did not disclose their HIV positive serostatus were more likely to have perceived stigma. The reason for this association may be due to fear of being HIV positive and every misunderstanding was mistakenly interpreted as it was due to their HIV serostatus. Despite the fact that this study tried to investigate all possible factors of perceived stigma, it is not without limitations. It was only facility based, which will not be representative of community based studies. In addition, as it was conducted through face to face interview, the study may be prone to social desirability biases.
Conclusion
In this study, the magnitude of perceived stigma was high as compared to UNAIDS standard, and sex of respondent, place of residence and disclosure of HIV serostatus were significantly associated with perceived stigma. The findings suggested that special emphasis should be placed on rural residents in order to reduce perceived stigma. Moreover, counseling should focus on disclosing HIV serostatus to anyone else interested to disclose particularly for females.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; CD4, cluster of differentiation; HIV, human immune-deficiency virus; PLWH, people living with HIV; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during this study will not be shared.
Acknowledgments
We would like to extend our deepest gratitude to Wollo University, public health facilities of Dessie city and study participants for creating different opportunities and providing important information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Oku AO, Owoaje ET, Ige OK, Oyo-ita A. Prevalence and determinants of adherence to HAART amongst PLHIV in a tertiary health facility in south-south Nigeria. BMC infect dis. 2013;3:1–9.
2. The Impact Of International Organizations On The Aids Epidemic In Sub-Saharan Africa Christopher Richins *. 2008;
3. Central Statistical Agency (CSA) [Ethiopia] and ICF. 2016. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
4. Sekoni AO, Obidike OR, Balogun MR. Stigma, medication adherence and coping mechanism among people living with HIV attending General Hospital, Lagos Island, Nigeria. African J Prim Heal Care Fam Med. 2012;4(1):1–10.
5. Lifson AR, Demissie W, Tadesse A, et al. Barriers to retention in care as perceived by persons living with HIV in rural Ethiopia: focus group results and recommended strategies. J Int Assoc Provid AIDS Care. 2013;12(1):32–38.
6. Fido NN, Aman M, Brihnu Z. HIV stigma and associated factors among antiretroviral treatment clients in Jimma Town, Southwest Ethiopia. HIV/AIDS Res Palliat Care. 2016;8:183–193. doi:10.2147/HIV.S114177
7. Mohite VR, Mohite RV, George J. Correlates of perceived stigma and depression among the women with HIV/AIDS infection. Bangladesh J Med Sci. 2015;14(2):151–158. doi:10.3329/bjms.v14i2.21864
8. Gausset Q, Overgaard H, Maurice W, Yameogo E, Berthé A, Konaté B. Social Science & Medicine The ambivalence of stigma and the double-edged sword of HIV/AIDS intervention in Burkina Faso. Soc Sci Med. 2012;74(7):1037–1044. doi:http://dx.doi.10.1016/j.socscimed.2011.11.044
9. Thomas BE, Rehman F, Suryanarayanan D, Josephine K. AIDS Care: psychological and Socio- medical Aspects of AIDS/HIV How stigmatizing is Stigma in the life of people living with HIV: A study on HIV positive individuals from Chennai. (December 2014). AIDS care. 2014;37–41.
10. SeyedAlinaghi S, Paydary K, Afsar Kazerooni P, et al. Evaluation of Stigma Index Among People Living With HIV/AIDS (PLWHA) in Six Cities in Iran. Thrita J Med Sci. 2013;2(2):69–75. doi:10.5812/thrita.11801
11. Ajong AB, Njotang PN, Nghoniji NE, et al. Quantification and factors associated with HIV-related stigma among persons living with HIV/AIDS on antiretroviral therapy at the HIV-day care unit of the Bamenda Regional Hospital, North West Region of Cameroon. Globalization health. 2018;14(1):1–7.
12. Solomon T, Haileamlak A, Girma B. Original Article Effect Of Acess To Antiretroviral Therapy On Stigma, Jimma University Hospital, Southwest Ethiopia. Ethiopian J Health Sci. 2008;18:25–32.
13. Therapy A, Hospital R. Factors Associated with Anxiety Disorder among ART Clients attending Factors Associated with Anxiety Disorder among ART Clients attending Antiretroviral Therapy Clinic at Hawassa University Referral Hospital, Hawassa. 2016.
14. Ml M, Kruger P, Mellors SE, Wolvaardt G. An exploratory survey measuring stigma and discrimination experienced by people living with HIV/AIDS in South Africa: the People Living with HIV Stigma Index. BMC public health. 2014;14:80.
15. Leddy AM, Turan JM, Johnson MO, et al. Poverty stigma is associated with suboptimal HIV care and treatment outcomes among women living with HIV in the United States. AIDS. 2019;33(8):1379–1384. doi:10.1097/QAD.0000000000002189
16. Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM, Bimirew MA, Kassie DM. Barriers and Facilitators of Adherence to Antiretroviral Drug Therapy and Retention in Care among Adult HIV- Positive Patients: A Qualitative Study from Ethiopia. PloS one. 2014;9:5.
17. Katz IT, Ryu AE, Onuegbu AG, et al. Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis. J Int AIDS Soc. 2013;16(Suppl):2.
18. Rahmati-Najarkolaei F, Niknami S, Aminshokravi F, et al. Experiences of stigma in healthcare settings among adults living with HIV in the Islamic Republic of Iran. J Int AIDS Soc. 2010;13(1):1–11. doi:10.1186/1758-2652-13-27
19. Yi S, Chhoun P, Suong S, Thin K, Brody C. AIDS-Related Stigma and Mental Disorders among People Living with HIV: A Cross- Sectional Study in Cambodia. PloS one. 2015;10:1–16.
20. Individuals AH, Hiv S, Reece M, et al. Impact of Internalized Stigma on HIV Prevention Behaviors. AIDS Patient Care STDs. 2012;26:12.
21. Miller AN, Rubin DL. Factors Leading to Self-Disclosure of a Positive HIV Diagnosis in Nairobi, Kenya: people Living With HIV/AIDS in the Sub-Sahara. Qualitative health res. 2007;75:254.
22. Campbell C. Dying Twice ’ A Multi-level Model of the Roots of AIDS Stigma in Two South African Communities. J health psycholy. 2007.
23. Rankin WW, Brennan S, Schell E, Laviwa J, Rankin SH. The Stigma of Being HIV-Positive in Africa. PLoS Med. 2005;2(8):702–704.
24. Phetlhu R, Naidoo JR, Makoae LN, Dlamini PS, Chirwa ML, Holzemer WL. Disclosure of HIV Status: experiences and Perceptions of Persons Living With HIV/AIDS and Nurses Involved in Their Care in Africa. Qualitative health res. 2008;18:311–324.
25. Wu X, Chen J, Huang H, Liu Z, Li X, Wang H. Perceived stigma, medical social support and quality of life among people living with HIV/AIDS in Hunan, China. Appl Nurs Res. 2014.
26. Hsin L, Kleinman A, Link BG, Phelan JC, Lee S, Good B. Culture and stigma: adding moral experience to stigma theory. AIDS. 2007;64:1524–1535.
27. Joy O, Akahomen S, Lawani AO, James BO. Stigma and suicidality among people living with HIV attending a secondary healthcare facility in Nigeria. Perspect psychiatric care. 2018;3(June).
28. Logie CH, Marcus N, Wang Y, et al. RESEARCH ARTICLE A longitudinal study of associations between HIV-related stigma, recent violence and depression among women living with HIV in a Canadian cohort study. J int AIDS soc. 2019;22:1–12.
29. Basha EA, Derseh BT, Gebre Y, Haile E, Tafere G. Factors Affecting Psychological Distress among People Living with HIV/AIDS at Selected Hospitals of North Shewa Zone, Amhara Region, Ethiopia. AIDS res treatment. 2019;2019.
30. Binduru R. Prevalence Of Hiv Related Stigma And Associated Factors Among Hiv. 2018.
31. Sayles JN, Wong MD, Kinsler JJ, Martins D, Cunningham WE. The association of stigma with self-reported access to medical care and antiretroviral therapy adherence in persons living with HIV/AIDS. J Gen Intern Med. 2009;24(10):1101–1108. doi:10.1007/s11606-009-1068-8
32. Muoghalu CO, Jegede SA. The Role of Cultural Practices and the Family in the Care for People Living With HIV/AIDS Among the Igbo of Anambra State, Nigeria. Social work health care. 2010;49:981–1006.
33. Golub, S. The Impact of Anticipated HIV Stigma on Delays in HIV Testing Behaviors: findings from a Community-Based Sample of Men Who Have Sex with Men and Transgender Women in New York City. AIDS. 2013;27:11
34. Joint United Nations Programme on HIV/AIDS (UNAIDS). On the Fast-Track to End AIDS by 2030: Focus on Location and Population. Geneva: UNAIDS:2014.
35. Dlamini PS, Ph D, Wantland D, et al. HIV Stigma and Missed Medications in HIV-Positive People in Five African Countries.AIDS patient care STDs. 2009;23:5.
36. Asgary R, Amin S, Grigoryan Z. Perceived stigma and discrimination towards people living with HIV and AIDS in Addis Ababa, Ethiopia: a qualitative approach. J Public Health. 2013;21:155–162.
37. Nattabi B, Li J, Thompson SC, Orach CG, Earnest J. Factors associated with perceived stigma among people living with HIV/AIDS in post-conflict northern Uganda. AIDS. 2011;23(3):193–205.
38. Pourmarzi D, Sc M, Khoramirad A, Sc M, Gaeeni M, Ph D. Perceived Stigma in People Living With HIV in Qom. J family rep health. 2017;11:4.
39. Article O, Datta S, Bhattacherjee S, Sherpa PL, Banik S. Perceived HIV Related Stigma among Patients Attending ART Center of a Tertiary Care Center in Rural West. J Public Health. 2020;25:9–12.
40. Xu X, Clark K. Factors Predicting Internalized Stigma Among Men Who Have Sex with Men Living with HIV in Beijing, China. J Assoc Nurses AIDS Care. 2016;24:1–12.
41. Monjok E, Smesny A, Essien EJ. ORIGINAL RESEARCH ARTICLE HIV/AIDS - Related Stigma and Discrimination in Nigeria: review of Research Studies and future directions for Prevention Strategies. Pers Individ Dif. 2009;13(3):21–35.
42. Berger BE, Ferrans CE, Lashley R. Measuring Stigma in People With HIV: psychometric Assessment of the HIV Stigma Scale. Res nurs health. 2001;24:518–529.
43. Wolfe WR, Weiser SD, Leiter K, Steward WT, Korte FP. The Impact of Universal Access to Antiretroviral Therapy on HIV Stigma in Botswana. Am J Public Health. 2008;98(10):1865–1871.
44. Moksnes UK, Moljord IEO, Espnes GA, Byrne DG. The association between stress and emotional states in adolescents: the role of gender and self-esteem. Pers Individ Dif. 2010;49(5):430–435. doi:10.1016/j.paid.2010.04.012
45. Lifson AR, Demissie W, Tadesse A, et al. HIV/AIDS stigma-associated attitudes in a rural Ethiopian community: characteristics, correlation with HIV knowledge and other factors, and implications for community intervention. BMC. 2012;1–8.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.