Back to Journals » International Journal of General Medicine » Volume 17
Perceived Knowledge, Guidelines Concordance, and Practices of Physicians for Management of Recurrent Urinary Tract Infections in Women
Authors Aldabeeb D ![]() , Alenzi EO
, Alenzi EO ![]() , Alhaizan M
, Alhaizan M ![]() , Alkhattabi M, Barry M
, Alkhattabi M, Barry M ![]() , Alalshaikh NK, Temsah MH
, Alalshaikh NK, Temsah MH ![]() , Al-Tawfiq JA
, Al-Tawfiq JA ![]() , Alshaikh G
, Alshaikh G
Received 20 March 2024
Accepted for publication 20 July 2024
Published 14 August 2024 Volume 2024:17 Pages 3521—3530
DOI https://doi.org/10.2147/IJGM.S469821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Dana Aldabeeb,1 Ebtihag O Alenzi,2 Maysoon Alhaizan,3 Mashael Alkhattabi,3 Mazin Barry,4,5 Nouf Khalid Alalshaikh,6 Mohamad-Hani Temsah,7,8 Jaffar A Al-Tawfiq,9– 11 Ghadeer Alshaikh1
1Department of Obstetrics and Gynecology, King Saud University, Riyadh, 11587, Saudi Arabia; 2Family and Community Medicine Department, College of Medicine, Princess Nourah bint Abdulrahman University 11671, Riyadh, Saudi Arabia; 3Department of Obstetrics and Gynecology, King Saud University Medical City, King Saud University, Riyadh, 11587, Saudi Arabia; 4Department of Internal Medicine College of Medicine, King Saud University, Riyadh, 11587, Saudi Arabia; 5Department of Internal Medicine, College of Medicine, University of Ottawa, Ottawa, ON, K1H 8M5, Canada; 6College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, 6660, Saudi Arabia; 7Pediatric Department, College of Medicine, King Saud University, Riyadh, 11587, Saudi Arabia; 8Evidence-Based Health Care & Knowledge Translation Research Chair, King Saud University, Riyadh, 11587, Saudi Arabia; 9Infectious Disease Unit, Specialty Internal Medicine, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia; 10Division of Infectious Diseases, Indiana University School of Medicine, Indianapolis, IN, USA; 11Division of Infectious Diseases, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Dana Aldabeeb, Department of Obstetrics and Gynecology, King Saud University, Riyadh, Saudi Arabia, PO Box 2549-12434, Tel +966505375606, Email [email protected] Mohamad-Hani Temsah, Evidence-Based Health Care & Knowledge Translation Research Chair, Family & Community Medicine Department, College of Medicine, King Saud University, Riyadh, 11362, Saudi Arabia, Tel +966554124457, Email [email protected]
Background: Recurrent urinary tract infections (rUTIs) are common complaints that burden the healthcare system. Reporting perceived knowledge and guidelines in concordance regarding the management of (rUTI) is essential for providing better healthcare and higher treatment rate. This study assesses the perceived knowledge, guidelines concordance, and physicians’ practices toward treatment of (rUTI) among physicians with different specialties.
Study Design: This questionnaire-based survey included residents, fellows, and consultants of various specialties across several regions in Saudi Arabia.
Results: A total of 419 physicians were included in the final analysis. In terms of age distribution, the majority were 28– 38 years of age (159, 37.9%), followed by 18– 28 years (99, 23.6%). Gender distribution was nearly balanced. The sample included a significant number of residents (182, 43.4%), consultants (173, 41.3%), and fellows (64, 15.3%). OBS/GYNE shows a significant presence of females (40.6%) and is notably represented in private hospitals or clinics (52.5%) and among fellows (40.6%) and consultants (32.4%). Infectious disease physicians had the highest perceived knowledge scores (3.83 ± 0.09), followed closely by urologists/urogynecologists (3.67 ± 0.48). Urologists/urogynecologists also reported the highest satisfaction (4.24 ± 0.83) and familiarity (2.89 ± 1.11) with new rUTI guidelines. Infectious disease physicians were most confident (3.50 ± 0.71) in communicating with patients about rUTI treatment options. In terms of practices and guideline adherence, obstetricians/gynaecologists were more likely to repeat urine sample tests for suspected contamination (3.73 ± 1.00) and less likely to treat asymptomatic bacteriuria (1.33 ± 0.59) the same as UTIs compared to other physicians. They also scored highest in conducting post-treatment tests for asymptomatic patients (3.21 ± 1.37) and recommending vaginal estrogen therapy for peri- and post-menopausal women to prevent UTIs (3.59 ± 1.06) among all specialties. Conversely, urologists and urogynecologists were more likely to discuss antibiotic prophylaxis (3.79 ± 0.89) and cranberry prophylaxis (3.71 ± 0.73) with their rUTI patients.
Conclusion: The findings highlight variations in knowledge, satisfaction, familiarity with guidelines, confidence in communication, and guideline concordance among different physician specialities regarding the management of UTIs and rUTIs.
Keywords: recurrent urinary tract infection, urologist, Saudi Arabia, gynecologists
Introduction
Urinary tract infections (UTI) are frequent urological complaints affecting approximately 60% of women at some point in their lifespan.1 Nearly 50% of women report a recurrence of UTI within 6–12 months, which not only causes discomfort but also leads to financial strain and a negative impact on their quality of life.2,3 In Saudi Arabia, UTIs significantly burden the healthcare system, accounting 10% of all infections and it is the second most common reason for emergency department admissions4,5 Recurrent UTIs (rUTIs) are defined as at least 2 episodes of culture-positive acute bacterial cystitis in 6 months or a minimum of 3 episodes in 1 year,6,7 and the recurrence is directly proportional to the impact of the infections on the patients’ lives.8,9 Women are more prone to rUTI than men because of their shorter urethral length, anatomical proximity of the urethra to the anal canal, vaginal bacterial colonization, and post-menopausal status.1
rUTIs can have a significant impact on patient’s daily lives and emotional well-being. Studies have shown that rUTIs can lead to disruptions in daily activities, reduced productivity, and impaired quality of life.1,10 Patients often experience persistent symptoms, such as pain, discomfort, and the need for frequent urination, which can interfere with their ability to work, engage in social activities, and maintain their usual routines. The emotional burden of rUTIs should not be overlooked. Patients with rUTIs have been found to experience higher levels of anxiety, depression, and frustration compared to those without recurrent infections.11,12
In addition, females are at a higher risk of Multidrug-resistant (MDR) and Pandrug-resistant (PDR) bacterial colonization when frequently exposed to antibiotics, the management of which can therefore become a challenge.13 One local study in Saudi Arabia reported that antimicrobial susceptibility testing (AST) for E. coli resulted in more than fifty percent resistance to 10 out of 18 tested antibiotics. It showed the most resistance rates to aztreonam 85.2%, ampicillin 78.8%, and cephalexin 71.2%.14 It is essential for physicians to fully understand the management of rUTI and the specific diagnostic criteria to provide better evidence-based healthcare to patients diagnosed with the infection.
The American Urologic Association (AUA), the Canadian Urological Association (CUA), the Society of Urodynamics, and the Female Pelvic Medicine & Urogenital Reconstruction (SUFU) recently published new guidelines for the care of female patients with uncomplicated rUTI in 2019.15 They included 16 recommendations for the evaluation and management of patients with symptoms of rUTI, including a comprehensive assessment with an initial review of patient symptoms, asymptomatic bacteriuria, and choice of antibiotic drugs and prophylaxis. The guidelines also include non-antibiotic prophylaxis, follow-up management, and the application of vaginal estrogen. Moreover, they highlighted the importance of shared decision-making between patients and their physicians when discussing the treatment options for rUTI, as physicians should be familiar with the guidelines.
A recent study assessed the awareness of participants from different levels, including medical students, residents, and fellows, of the new guidelines and examined the degree of education and certainty in treating rUTI according to recent guidelines.16 The study found that the knowledge increased with advanced training and reported that most urology trainees were aware of the 2019 rUTI guidelines, compared to other residents, fellows, and medical students.
Understanding the degree of knowledge regarding the recent guidelines and the patterns of rUTI management is essential for providing better healthcare and a higher treatment rate. Thus, this study aims to explore the general awareness and confidence of medical trainees and physicians regarding the treatment of female patients with rUTI. It also aims to evaluate any differences in the perceptions of participants regarding rUTI management for pre-and post-menopausal women. These results can be used to facilitate further training and increase awareness among trainees when helping female patients reporting rUTI for the first time.
Materials and Methods
Study Design
This questionnaire-based study included physicians working in hospitals in several regions of Saudi Arabia. Physicians from several specialties at different training levels, including, residents, fellows, and consultants, were invited through Email to participate in the research between 1 March and 31 July 2022.
Study Processes and Data Source
The study aim was explained to all participants, who also provided informed consent before taking the questionnaire. Participation was voluntary and privacy was ensured.
Data was collected using an online questionnaire. The questionnaires were adopted from a previous study,16 with a few items modified and adjusted for the Saudi population, such as place of residence, ethnicity, and race. Adaptation processes include providing culturally sensitive content and appropriate local work settings and environments. The final draft was piloted on ten participants at the xxxxxxxxxxxxxx to ensure clarity and check the time required for completion, and they were excluded from the final results. Minor changes were made to each of the feedback items. The required sample size was calculated using Raosoft. Based on a confidence level of 95%, a confidence interval of 0.05, the minimum required sample size was 278.
The questionnaire consisted of the following sections: (1) Informed consent; (2) Demographic information, including age, gender, level of training (residents, fellows, and consultants), current work setting, and work region/province;2 specialties which were grouped into urology/urogynecology, obstetrics/gynecology, infectious diseases, and other specialties; and3 UTI and rUTI management-related factors including number of patients with UTI and rUTI that a physician have seen per month, perceived level of knowledge about rUTI treatment, satisfaction with the new rUTI guidelines, the believe that rUTI guidelines will reduce the recurrence of UTIs and the financial burden, perceived familiarity with the updated rUTI guideline, perceived confidence in the effectiveness of communication with patients about rUTI treatment options, and physicians’ practices and guideline concordance for management of UTI and rUTI. The perceived level of knowledge about rUTI treatment and perceived familiarity with the updated rUTI guideline was assessed using a scale from 1 to 4 where 1 = no knowledge at all; 2= A little knowledge; 3= A moderate amount of knowledge; 4= A great deal of knowledge. The answers to satisfaction with the new rUTI guidelines consisted of 1 “very dissatisfied”, 2 “somewhat dissatisfied”, 3 “neither satisfied or dissatisfied”, 4 “somewhat satisfied”, and 5 “very satisfied”. Agreement with the belief that rUTI guidelines will reduce the recurrence of UTIs and the financial burden was estimated with 5 replies (from 1 “disagree” to 5 “agree”). Perceived confidence in the effectiveness of communication with patients about rUTI treatment options was answered based on the options ranging from 1” not at all confident” to 4 “very confident. For physicians’ practices and guideline concordance for the management of UTI and rUTI, there were 6 items “repeating urine sample test when an initial urine specimen is suspect for contamination, treating asymptomatic bacteriuria, the same as UTIs, discussing prescribing antibiotic prophylaxis with rUTI patients, suggesting cranberry prophylaxis to women with rUTIs, performing a post-treatment test of cure urinalysis/culture for asymptomatic patients, and recommending vaginal estrogen therapy to reduce risk of future UTIs for peri- and post-menopause. The participants provided answers for each of these practice-related statements based on 5 Likert scales (1=never, 2=almost never, 3= sometimes, 4=almost always, 5=always).
This study was approved by the Institutional Review Board (IRB) of KSUMC under Project Number No E-22-6783.
Statistical Analysis
Data was analyzed using the SPSS 24.0 version statistical software. Descriptive statistics (frequencies and percentages) were used to outline categorical variables while means with standard deviations (SD) were reported for continuous data. Bivariate statistical analysis was performed using the appropriate statistical tests (chi-square or Fisher’s exact test). One-way analysis of variance (ANOVA) tests were used to test the differences in the UTI treatment-related factors (perceived knowledge, satisfaction, believe, perceived familiarity, perceived confidence, and disease management) between different specialities (urology/urogynecology, obstetrics/gynecology, infectious diseases, other specialties). P-value of <0.05 and 95% CI were used to report the statistical significance and precision of the results.
Results
Study Sample’s Characteristics
Of the 744 healthcare workers who received the survey, 419 (56.32%) physicians were included in the analysis (Figure 1). The characteristics of the included participants are listed in Table 1.
 |
Table 1 Main Characteristics of the Study Sample (N=419) |
 |
Figure 1 Sample flow chart. |
The study included 419 participants with the majority aged 28–38 years (n=159, 37.9%), followed by those aged 18–28 years (n=99, 23.6%), 38–48 years (n=81, 19.3%), and those >48 years (n=80, 19.1%). Gender distribution was nearly balanced. The sample included a significant number of residents (n=182, 43.4%), consultants (n=173, 41.3%), and fellows (n=64, 15.3%). Approximately one-third of participants have seen more than 10 patients with UTIs per month while 10% of them have seen more than 10 patients with rUTIs per month (not tabulated).
Differences in the Physicians’ Characteristics by Their Specialities
Table 2 demonstrates the main difference in our sample of physicians based on their specialities. Factors that were significantly different across specialities (urology/urogynecology, obstetrics/gynaecology, infectious diseases, and other specialities) included age, gender, medical position, current work setting, and work region.
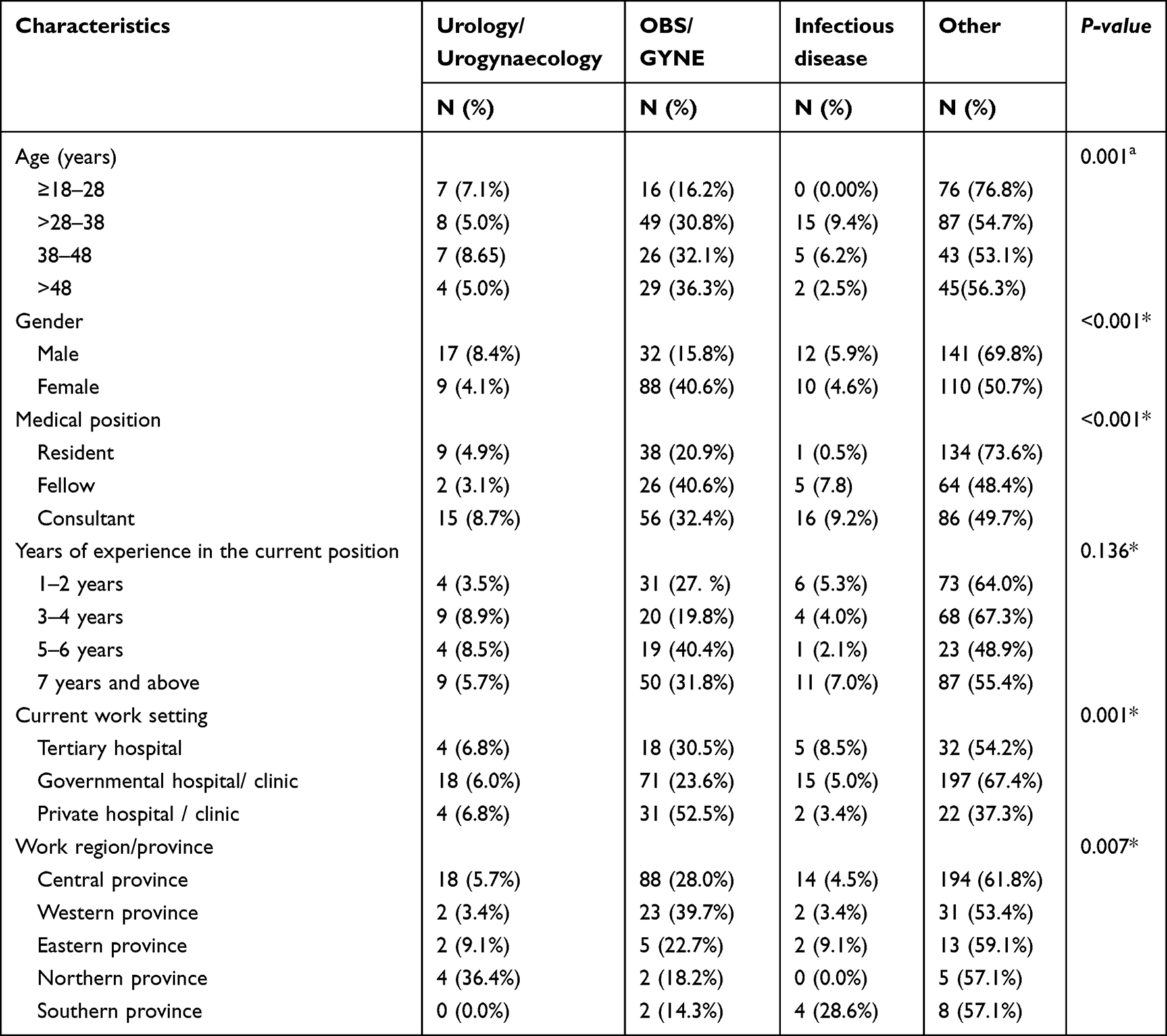 |
Table 2 Differences in the Physicians’ Characteristics by Their Specialities (N=419) |
Differences in UTI and rUTI Management -Related Factors Based on Speciality
The differences in all UTI management-related factors between the groups of different specialities are presented in Table 3. Factors that were significantly associated with the type of speciality included number of patients seen with UTI and rUTI per month, perceived level of knowledge about rUTI treatment, satisfaction with the new rUTI guidelines, perceived familiarity with the updated rUTI guideline, perceived confidence in the effectiveness of communication with patients about rUTI treatment options, and physicians’ practices and guideline concordance for management of UTI and rUTI.
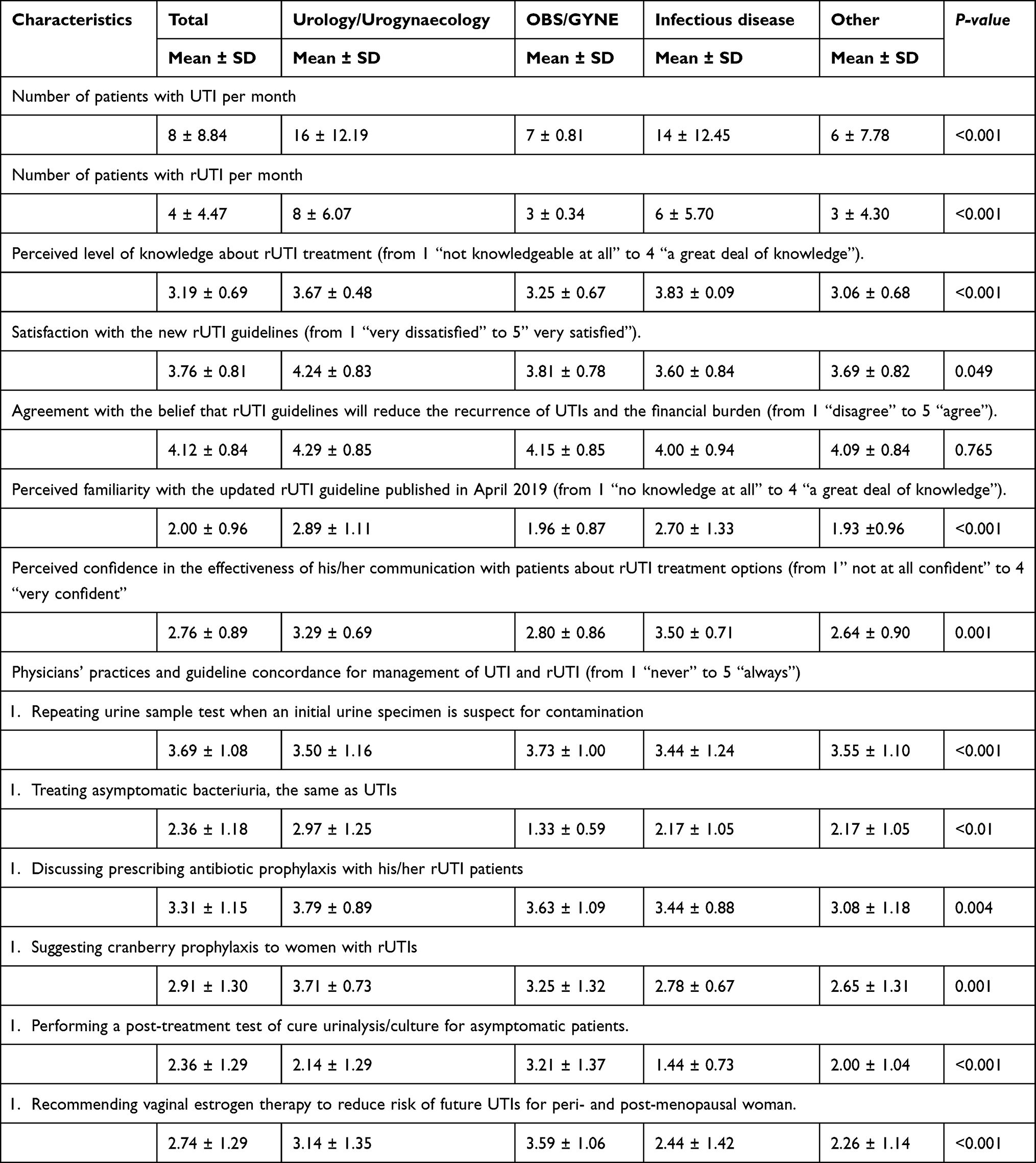 |
Table 3 Differences in the Urinary Tract Infection (UTI) Treatment Related Factors (Perceived Knowledge, Satisfaction, Believe, Perceived Familiarity, Perceived Confidence, and Disease Management) Based on Physicians’ Specialities (N=419) |
Overall, the average number of UTI cases that physicians have seen per month was 8 cases while the average number of rUTI cases was 4 cases. On average, physicians who have seen the highest number of cases with UTI specialized in urology or urogynecology (16 ± 12.19) followed by physicians who specialized in infectious diseases (14 ± 12.45). Likewise, physicians who have seen the highest number of cases with rUTI were urologists or uro-gynecologists (8 ± 6.07) followed by physicians who specialized in infectious diseases (6 ± 5.70). In general, physicians were moderately knowledgeable (3.19 ± 0.69) about rUTI treatment, somewhat satisfied (3.76 ± 0.81) with the new rUTI guidelines, a little familiar (2.00 ± 0.96) with the updated rUTI guideline, confident (2.76 ± 0.89) in the effectiveness of their communication with patients about rUTI treatment options. Infectious diseases physicians had the highest score (3.83 ± 0.09) of perceived knowledge followed by urologists and uro-gynecologists (3.67 ± 0.48). Urologists and uro-gynecologists had highest scores in satisfaction (4.24 ± 0.83) and familiarity (2.89 ± 1.11) with the new rUTI guidelines compared to other specialties. However, infectious disease physicians had the highest scores of confidence (3.50 ± 0.71) in the effectiveness of their communication with patients about rUTI treatment options.
Regarding physicians’ practices and guideline concordance for the management of UTI and rUTI, obstetricians/gynaecologists were more likely to repeat urine sample tests when an initial urine specimen is suspect for contamination as compared to the average score of physicians (3.73 vs 3.69). On the other hand, obstetricians/gynaecologists were less likely to treat asymptomatic bacteriuria, the same as UTIs (1.33 vs 2.36) as compared to other physicians in the sample. Also, obstetricians/gynaecologists reported the highest scores of performing a post-treatment test of cure urinalysis/culture for asymptomatic patients (3.21 ± 1.37) and recommending vaginal estrogen therapy to reduce the risk of future UTIs for peri- and post-menopausal woman (3.59 ± 1.06) as compared to other specialities. However, urologists and urogynecologists had the highest scores for discussing prescribing antibiotic prophylaxis with their rUTI patients (3.79 ± 0.89) and offering cranberry prophylaxis to women with rUTIs (3.71 ± 0.73).
Discussion
Antimicrobial resistance (AMR) and the emergence of multi-drug-resistant organisms are global problems which are becoming more significant due to the misuse of antibiotics in hospitals and communities. In Saudi Arabia, there has been a steady increase in extended-spectrum beta-lactamases Escherichia coli and Klebsiella pneumonia, the two most common causes of UTI.17 The emergence of AMR in Saudi Arabia is of particular global public health importance due to the annual Hajj.18 The use of antibiotics and treatment of common infections, such as UTI, are affected by numerous factors, including the knowledge and practice of physicians towards antibiotic use.19
Assessing physicians’ knowledge of rUTI guidelines is valuable from a scientific perspective, as it can help identify knowledge gaps, inform clinical practice, and evaluate the effectiveness and uptake of these guidelines in real-world settings. Evaluating physicians’ knowledge can also reveal potential barriers and facilitators to the implementation of rUTI guidelines, which can guide the design and focus of future research studies aimed at improving the management of this common and recurrent condition. By understanding the current knowledge and practices of physicians, researchers and policymakers can develop more effective strategies to enhance clinical decision-making and ultimately lead to better patient outcomes.
The release of the 2019 guidelines (AUA/CUA/SUFU) provides physicians with an evidence-based management plan of rUTI aimed at decreasing the risk of antibiotic resistance. Additionally, it offers options for both antibiotic and non-antibiotic treatments and enhances the overall quality of life for patients with rUTIs.15 This study highlights the current perceived knowledge of physicians in the treatment process of rUTI patients, as well as their familiarity, satisfaction, and concordance with these guidelines among different specialties.
On average, physicians in our sample have seen about 8 cases of UTI and 4 cases of rUTI per month. They perceived their knowledge about rUTI treatment as moderate, were somewhat familiar with the new rUTI guidelines, and expressed satisfaction with them. Additionally, they were confident in the effectiveness of their communication with patients about rUTI treatment options.
Specialties of physicians who have seen the highest numbers of cases with UTI and rUTI were urology/urogynecology and infectious disease. Physicians with these specialties perceived their knowledge about rUTI treatment as a great deal of knowledge and they thought that they were familiar with new guidelines of rUTI treatment. Also, they were confident in the effectiveness of their communication with patients about rUTI treatment options. Consistent with this finding, a previous study reported that most urology trainees were more knowledgeable of recent guidelines than non-urology residents and fellows.16 However, other physicians may see at least 3 cases of rUTI per month so raising awareness and knowledge among them is essential for a robust healthcare system, especially primary healthcare physicians as they represent the first line of approach for patients with simple UTI or rUTI.
When it comes to guidelines concordance, obstetricians/gynaecologists and urologists/urogynecologists were more likely to follow guidelines as compared to other specialists. Obstetricians/gynaecologists almost always repeat urine sample tests when an initial urine specimen is suspected of contamination (3.73 ± 1.00). Also, obstetricians/gynecologists had never treated asymptomatic bacteriuria (ASB) the same as UTI cases (1.33 ± 0.59). For the management of rUTI, non-pharmacological modalities have been shown to decrease antibiotic resistance in patients with rUTI. In 2015, the World Health Organization (WHO) released a global action plan aimed at decreasing the AMR.20 Recently, cranberries have been widely studied in randomized clinical trials.21 Current study showed that physicians in general were sometimes prescribing cranberry prophylaxis to women with rUTI while urologists/urogynecologists almost always recommended cranberry prophylaxis for women with rUTI (3.79 ± 0.73).
This suggests a lack of knowledge among other specialities regarding the mechanism of action of proanthocyanidins (PACs) present in cranberries and their ability to prevent the adhesion of bacteria to the urothelium.22–24 Thus, physicians should be aware of non-pharmacological options, such as different cranberry formulas, including oral juice and tablet formulations.
Regarding the management of rUTI in post-menopausal women, vaginal topical estrogen has been proven to reduce the risk of rUTI.22 However, only obstetricians/gynaecologists almost always recommended vaginal estrogen therapy to reduce the risk of UTIs for peri- and post-menopausal women (3.59 ± 1.06), while other specialists sometimes (urologists/urogynecologists) or almost never (all other physicians) suggested this therapy for peri- and post-menopausal women.
Consistent with our results, a study conducted among physicians in the United States showed that specialties except obstetrics/gynaecology and urology had low rates of guideline concordance during the management of uncomplicated UTI cases.25 Also, a study in general medical wards of New Zealand demonstrated that the prescribers had low rates of guidelines concordant in their diagnosis and treatment of UTI cases.26
This could be explained by the fact that they were less exposed to patients who need topical vaginal estrogen and therefore less familiar with the advantages of this preventive therapy for the post-menopausal group.
The current study provides valuable insights, but it has several limitations, including response bias, selection bias, geographic limitation, cross-sectional design, lack of objective assessment, limited depth of responses, and potential non-response. To address these limitations, future research could incorporate more robust methodologies, such as objective assessments, longitudinal designs, and a broader geographic representation, to provide a more comprehensive understanding of physicians’ knowledge and practices regarding UTI therapy guidelines. Addressing these limitations could enhance the robustness and applicability of the findings, leading to a more accurate and actionable understanding of the challenges and opportunities in improving UTI therapy guidelines adherence among healthcare providers in Saudi Arabia. The recent guidelines were released three years ago, and responses may be affected by recall bias. Further research analyzing qualitative data may provide a better understanding of physicians’ knowledge about the management of rUTI and the gaps that need to be filled to provide patients with an optimal healthcare plan. Enhancing adherence to guidelines and increasing knowledge among physicians can be achieved by increasing education among physicians through campaigns, ground rounds and emphasizing on national awareness UTI day (November 21st). Since patients diagnosed with rUTI may seek medical care from any physician, it is essential to increase awareness about the recent guidelines to manage cases with rUTI and promote guidelines concordance in physicians’ practices for optimal women’s health care.
Conclusions
The AUA/CUA/SUFU guidelines have provided a great understanding of how to manage patients with rUTI, together with clear instructions on how to decrease the uncertainty surrounding rUTI management for various medical specialities in Saudi Arabia. Notably, urologists/urogynecologists and physicians specializing in infectious diseases are more likely to treat rUTI cases and possess a high level of perceived knowledge. In contrast, obstetricians/gynaecologists are more adherent to guidelines in their rUTI management practices. However, other physicians report low perceived knowledge and familiarity with updated guidelines, indicating a need for targeted educational activities and self-directed learning to ensure they provide evidence-based rUTI treatment plans. Enhancing the knowledge and guideline adherence among all specialities could significantly improve patient outcomes by ensuring consistent and effective management of rUTIs, ultimately contributing to a reduction in antibiotic resistance and enhancing the overall quality of care for women suffering from this condition.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) of KSUMC under Project Number No E-22-6783.
Informed Consent Statement
The study aimed explained to all participants, who also provided informed consent before taking the questionnaire. Participation was voluntary and privacy was ensured.
Acknowledgment
The authors are grateful to the Deanship of Scientific Research, King Saud University, for funding through the Vice Deanship of Scientific Research Chairs.
We thank “Prince Naif Health Research Center”, Investigator Support Unit at King Saud University, Riyadh, Saudi Arabia, for their statistical analysis efforts. The authors extend their appreciation to the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research (IFKSURC-1-3103).
Disclosure
The authors report no personal or financial conflicts of interest to declare.
References
1. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28(1):1–13. doi:10.1016/j.idc.2013.09.003
2. Ikähelmo R, Siitonen A, Heiskanen T, et al. Recurrence of urinary tract infection in a primary care setting: analysis of a I-year follow-up of 179 women. Clinl Infect Dis. 1996;22(1):91–99. doi:10.1093/clinids/22.1.91
3. Wagenlehner F, Wullt B, Ballarini S, Zingg D, Naber KG. Social and economic burden of recurrent urinary tract infections and quality of life: a patient web-based study (GESPRIT). Expert Rev Pharmacoecon Outcomes Res. 2018;18(1):107–117. doi:10.1080/14737167.2017.1359543
4. Alrashid S, Ashoor R, Alruhaimi S, Hamed A, Alzahrani S, Al Sayyari A. Urinary tract infection as the diagnosis for admission through the emergency department: its prevalence, seasonality, diagnostic methods, and diagnostic decisions. Cureus. 2022;14(8). doi:10.7759/cureus.27808
5. Alanazi MQ, Al-Jeraisy MI, Salam M. Prevalence and predictors of antibiotic prescription errors in an emergency department, Central Saudi Arabia. In: Drug, Healthcare and Patient Safety. Taylor and Francis; 2015:103–111.
6. Dason S, Dason JT, Kapoor A. Guidelines for the diagnosis and management of recurrent urinary tract infection in women. Canadian Urolog Assoc J. 2011;5(5):316. doi:10.5489/cuaj.687
7. Finucane TE. “Urinary tract infection”—requiem for a heavyweight. J Am Geriatr Soc. 2017;65(8):1650–1655. doi:10.1111/jgs.14907
8. Geerlings SE. Clinical presentations and epidemiology of urinary tract infections. Microbiol Spectr. 2016;4(5). doi:10.1128/microbiolspec.UTI-0002-2012
9. Gupta K, Trautner BW. Diagnosis and management of recurrent urinary tract infections in non-pregnant women. BMJ. 2013;346(may29 4):f3140–f3140. doi:10.1136/bmj.f3140
10. Eriksson I, Gustafson Y, Fagerström L, Olofsson B. Urinary tract infection in very old women is associated with delirium. Int Psychogeriatr. 2011;23(3):496–502. doi:10.1017/S1041610210001456
11. Thomas-White K, Navarro P, Wever F, King L, Dillard LR, Krapf J. Psychosocial impact of recurrent urogenital infections: a review. Women's Health. 2023;19:17455057231216537.
12. Jo SB, Kim HJ, Ahn ST, Oh MM. Level of Anxiety Shows a Positive Correlation With the Frequency of Acute Cystitis Recurrence in Women. Int Neurourol J. 2024;28(2):156–161. doi:10.5213/inj.2448096.048
13. Simmering JE, Tang F, Cavanaugh JE, Polgreen LA, Polgreen PM. The increase in hospitalizations for urinary tract infections and the associated costs in the United States, 1998–2011. In: Open Forum Infectious Diseases. Oxford University Press; 2017.
14. Almutawif YA, Eid HMA. Prevalence and antimicrobial susceptibility pattern of bacterial uropathogens among adult patients in Madinah, Saudi Arabia. BMC Infect Dis. 2023;23(1):582. doi:10.1186/s12879-023-08578-1
15. Anger J, Lee U, Ackerman AL, et al. Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. J Urol. 2019;202(2):282–289. doi:10.1097/JU.0000000000000296
16. Ingram A, Yudovich M, Payne N, Bellows F, Posid T. Knowledge is Key: viewpoints of New Recurrent Urinary Tract Infections Guidelines. Urology. 2021;158:45–51. doi:10.1016/j.urology.2021.08.035
17. Al-Tawfiq JA, Rabaan AA, Saunar JV, Bazzi AM. Antimicrobial resistance of gram-negative bacteria: a six-year longitudinal study in a hospital in Saudi Arabia. J Infect Public Health. 2020;13(5):737–745. doi:10.1016/j.jiph.2020.01.004
18. Al-Tawfiq JA, Memish ZA. The emergence, persistence, and dissemination of antimicrobial-resistant bacteria in environmental Hajj settings and implications for public health. Trop Med Infect Dis. 2021;6(1):33. doi:10.3390/tropicalmed6010033
19. Alnasser AHA, Al-Tawfiq JA, Ahmed HAA, et al. Public knowledge, attitude and practice towards antibiotics use and antimicrobial resistance in Saudi Arabia: a web-based cross-sectional survey. J Public Health Res. 2021;10(4):
20. WHO. World Health Organization: antimicrobial resistance; 2015. Available from: https://www.who.int/health-topics/antimicrobial-resistance.
21. Valente J, Pendry BA, Galante E. Cranberry (Vaccinium macrocarpon) as a prophylaxis for urinary tract infections in women: a Systematic Review with Meta-Analysis. J Herbal Med. 2022;36:100602. doi:10.1016/j.hermed.2022.100602
22. Foo LY, Lu Y, Howell AB, Vorsa N. A-Type Proanthocyanidin Trimers from Cranberry that Inhibit Adherence of Uropathogenic P-Fimbriated Escherichia coli. J Natural Prod. 2000;63(9):1225–1228. doi:10.1021/np000128u
23. Howell AB, Reed JD, Krueger CG, Winterbottom R, Cunningham DG, Leahy M. A-type cranberry proanthocyanidins and uropathogenic bacterial anti-adhesion activity. Phytochemistry. 2005;66(18):2281–2291. doi:10.1016/j.phytochem.2005.05.022
24. Lavigne J-P, Vitrac X, Bernard L, Bruyère F, Sotto A. Propolis can potentialise the anti-adhesion activity of proanthocyanidins on uropathogenic Escherichia coli in the prevention of recurrent urinary tract infections. BMC Res Notes. 2011;4(1):522. doi:10.1186/1756-0500-4-522
25. Langner JL, Chiang KF, Stafford RS. Current prescribing practices and guideline concordance for the treatment of uncomplicated urinary tract infections in women. Am J Clin Exp Obstet Gynecol. 2021;225(3):272.e1–272.e11. doi:10.1016/j.ajog.2021.04.218
26. Chen AK, Duffy EJ, Ritchie SR, Thomas MG. Diagnostic accuracy and adherence to treatment guidelines in adult inpatients with urinary tract infections in a tertiary hospital. J Pharm Pract Res. 2019;49(3):246–253. doi:10.1002/jppr.1508
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.