")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Perceived Health Status and Medical Conditions Among US Active-Duty Service Members
Authors Olapeju B , Ahmed AE , Chu K, Yoon J, Mancuso JD
Received 7 July 2023
Accepted for publication 27 November 2023
Published 21 December 2023 Volume 2023:16 Pages 5121—5138
DOI https://doi.org/10.2147/PRBM.S429341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Bolanle Olapeju, Anwar E Ahmed, Kasi Chu, Jangho Yoon, James D Mancuso
Department of Preventive Medicine and Biostatistics, Uniformed Services University of the Health Sciences, Bethesda, MD, USA
Correspondence: Bolanle Olapeju, Department of Preventive Medicine and Biostatistics, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Road, Bethesda, MD, 20814, USA, Tel +1 301-295-1585, Email [email protected]
Purpose: This paper investigates the association between self-reported perceived health status and doctor-informed medical conditions among US active duty service members (ADSM).
Methods: Data are from the 2018 Health-Related Behaviors Survey – a cross-sectional survey weighted to represent the US military (N = 17166). Perceived good health status was defined as having a response choice of “good”, “very good”, or “excellent” to the question: Would you say your overall physical health is ___? Medical conditions were based on self-reported presence of nine clinical conditions. Analysis included weighted prevalence and log-binomial regression models to explore relationships between ADSM characteristics with perceived good health status as well as concordance between perceived status and medical conditions.
Results: ADSM rated their health to be excellent (14.6%), very good (37.7%), good (36.2%), fair (9.7%) and poor (1.7%). About 88.5% perceived a good (to excellent) health status. Perceived good health status was negatively associated with the number of medical conditions present (adjusted odds ratio (aOR): ranging from 0.78 to 0.92) as well as several health behaviors (aOR): ranging from 0.86 to 0.98) and other sociodemographic factors. Among all ADSMs, 51% perceived good health in the absence of medical conditions, while 8% perceived poor health status in the presence of medical conditions. Concordance between perceived health status and medical conditions was significantly lower among ADSM who were older (aOR: 0.61; 95% CI: 0.54– 0.69), with dependent children (aOR: 0.89; 95% CI: 0.84– 0.95), or had been deployed (aOR: 0.89, 95% CI: 0.84-0.95).
Conclusion: The prevalence of perceived good health status among ADSMs was consistent with those documented in the general US population. The interrelationships between ADSM’s perceptions, medical conditions and sociodemographic characteristics may have implications for their health literacy and utilization of health services. Study findings suggest that interventions promoting healthy behaviors, health literacy and treatment-seeking may influence perceived health status and mitigate medical conditions among ADSM, thus improving the US Military readiness, resilience and mission success.
Keywords: active duty service members, health status, medical conditions, risk behaviors, United States
Introduction
Self-reported indices of health status or have been frequently used in health surveys.1,2 Perceived health status is usually measured by asking the individual to rate their health on a four- or five-point ordinal scale or in comparison to peers.3,4 Such evaluations are typically based on a person’s subjective assumption about their physical, mental and social well-being in addition to actual information about the diseases or injuries they have.5 Self-perceived health has been used to evaluate population-level health status, health inequities and general health care needs among diverse populations.1–5
Perceived Health Status in the US
According to the National Center for Health Statistics in 2020, about 14% of Americans rated their health as fair or poor in general, ranking the US low among high-income countries.6 In addition, self-perceived poor health in the US varied substantially by sex, age, region, socioeconomic status and race. Specifically, perceived poor health was higher among adults 65 years or older, females and race/ethnic minority groups.7 Although perceived health status is often used as a proxy measure for disease and health behavior, research has demonstrated discordance between perceived and actual health status in the US.8,9 Higher levels of this discordance have been reported among older, wealthier and ethnic minority sub-groups.8,9
Review of Relevant Literature
Evidence indicates positive psychological states—such as having a sense of purpose, being satisfied with life, or having a sense of optimism—are associated with good physical and mental health, a key principle of positive epidemiology.10 Self-perceived health status is demonstrated to be a valid predictor of actual health status and outcomes.11 Perceived health status could also be considered a proxy for psychosocial constructs in behavioral theories such as the Health Belief Model12 and Theory of Planned Behavior,13 used to understand population-level health behaviors. Specifically, perceived health status may be a measure of perceived vulnerability (susceptibility to adverse health outcomes) and perceived severity (how serious such adverse outcomes would be in the event that they occur).14 Perceived health status may also reflect perceived community norms such regarding the population health status as well as personal values related to health. Thus, perceived health status may not only reflect actual health status but also a correlate of health behavior such as substance use or risky sexual behaviors.15
Study Rationale
The active-duty military population is generally considered to be fitter than the general population. Lower rates of obesity (18 versus 37%) and hypertension (13% versus 30%) were seen among ADSM compared to the overall US population.16,17 It is unclear the extent to which the prevalence and correlates of perceived health status would be similar across US military and general populations. Limited research among active duty Air Force recruits and Army personnel suggests that perceived health status was associated with harmful substance use, obesity, depression, poor sleep quality as well as outcomes such as increased risk of future hospitalization and illness-related ambulatory care visits.18,19 In addition, military members may be in a unique position to have differences in perceived versus actual health status due to prevailing expectations of health standards and ideals of self-image.20 However, no study has systematically explored the concordance between perceived health status and presence of medical conditions or the interconnections between self-perceived, actual health status and risk behaviors among all the Nation’s servicemen and women including the US Air Force, Army, Marine Corps, Navy and Coast Guard.
Study Aims and Conceptual Framework
The primary aim is to assess demographic, medical and behavioral risk factors associated with perceived health status among active duty military. The secondary aim is to explore the concordance between perceived health status and actual medical conditions as well as its correlates among ADSM. This analysis will enhance our current understanding of the utility, correlates and interpretation of self-perceived health status and inform the design of relevant preventive measures and provide recommendations that may support the design of timely health or behavioral interventions for service members.
The study’s conceptual framework draws from available data in the Health-Related Behaviors Survey (HBRS) as well as psychosocial constructs from behavioral theories such as the Health Belief Model and Theory of Reasoned Action. Using a positive epidemiologic approach focused on health assets and a broader range of health-related states,10 the study hypothesizes relationships between measures available in HRBS such as sociodemographic factors, risk behaviors, medical conditions and perceived health status as shown in Figure 1. We posit perceived good health status is negatively associated with the presence of medical conditions and engagement in risk behaviors. In addition, sociodemographic factors of ADSM such as their age, sex, race and ethnicity, housing status, education, etc., may be distal factors influencing perceived health status.21 The study hypothesizes that perceived good health status is negatively associated with older age, race/ethnic minorities, lower socioeconomic or education levels. We also hypothesize that an arbitrary proportion of three quarters of ADSM would demonstrate concordance between their perceived health status and medical conditions.
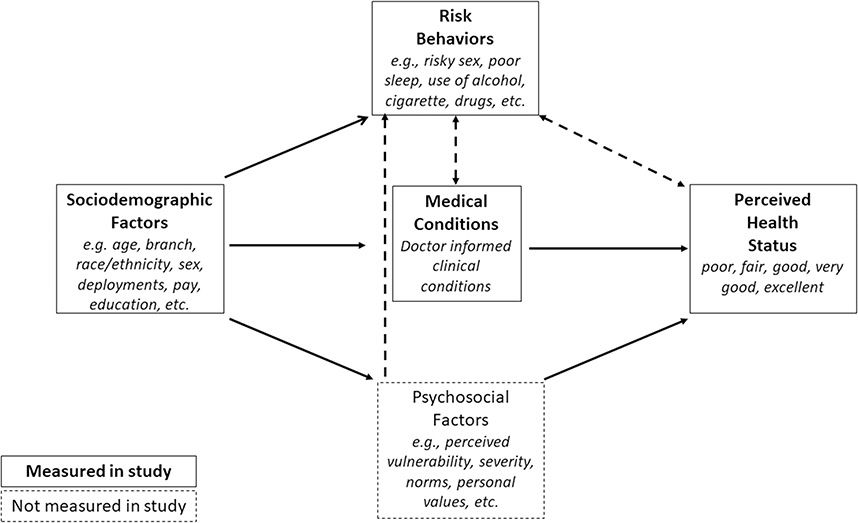 |
Figure 1 Study Conceptual Framework Showing Relationships between Perceived Health Status, Medical Conditions and Risk Behaviors. |
Materials and Methods
Study Design and Population
The Health-Related Behaviors Survey (HRBS) is a recurring cross-sectional survey instituted by the Department of Defense (DoD) since 1980 and currently sponsored by the Defense Health Agency (DHA). It is the DoD’s flagship survey for understanding the health, health-related behaviors, and well-being of service members which utilizes existing, validated measures that facilitate comparisons with civilian populations.22 The 2018 HRBS is the most recent iteration for which publicly available data have been released. This study excludes the reserve (not on active duty) component. The total sampling frame was 1,357,219 active component service members. The sampling frame utilized 50 strata based on the interaction of service branch (five categories), pay grade (five categories), and gender (two categories). By considering anticipated response rates that differ across these strata, the sampling plan attempted to minimize the survey design effect (ie, loss of precision). From the sampling frame of 1,357,219 service members, 199,996 active-duty service members were approached to complete the online survey. A total of 17,166 surveys were completed, resulting in a weighted response rate of 9.6% (N = 17,166 ADSM). First, design weights were employed to counteract the survey design, which slightly oversampled Marines, women, and junior enlisted personnel to guarantee enough of those groups to yield reliable estimates. Next, nonresponse weights were used to make the respondents representative of those who were selected for sampling. The final analytic weights were the product of the design and nonresponse weights to make the analytic sample representative of the eligible service member population. Missing data typically introduce bias due to unreported values being systematically different from reported ones. However, the missingness rates in the HRBS 2018 data ranged from less than 0.1% to 7%, and this was addressed by imputation to result in a data set that is more representative of the inferential population and makes more-efficient use of the available data for all cases even where they did not complete every survey item.22
Measurements
Perceived Health Status
The HRBS includes the question: “Would you say your overall physical health is ___?” Response options were excellent, very good, good, fair or poor. This variable was explored as an ordinal variable as well as dichotomized into perceived good (good to excellent) versus poor (fair or poor) health status in keeping with other relevant nationally representative research.23,24
Medical Conditions
This was self-reported based on 8 survey questions: “In the PAST 12 MONTHS has a doctor or other health professional told you that you had”: i) High blood pressure; ii) High blood sugar or diabetes; iii) High cholesterol; iv) Asthma; v) Angina or coronary heart disease; vi) Heart attack; vii) Back pain; viii) Bone, joint, or muscle injury or condition. Obesity was based on the self-reported height (inches) and weight (pounds) of ADSM (BMI>30kg/m2).22 The number of doctor-informed medical conditions and obesity status were explored as continuous (ranging from 0 to 9), categorical (none, 1–2, 3+) and dichotomous variables (0 versus 1+ conditions). This manuscript focuses on self-reported data, typically considered subjective instead of the more objective confirmed medical status, because this is a secondary analysis of confidential survey data that is not linked to the medical records of participants.
Mental Health Status
The HRBS also included a measure of an ADSM’s mental health based on the validated Kessler Mental Health Scale (K6) battery of questions to assess nonspecific serious psychological distress.25 The score ranges between 0 and 24 with “serious distress” being identified as a mean K6 score greater than 12.
Risky Behaviors
This included the following five short-term and two long-term self-reported behaviors within the past 30 days and 12 months, respectively:
- Infrequent physical activity and/or strength training in the past 30 days defined as less than three days per week of strength training, moderate or vigorous physical activity.
- Screen time (spent using a device with a screen for activities other than for work or school) over than two hours/day in past 30 days.
- Bad sleeping habits in past 30 days defined as a composite measure of all of the following: a) sleeping less than seven hours/day, b) self-rated quality of sleep as insufficient, c) the use of prescription medications to go to sleep, d) use of energy drinks, caffeinated beverages, or over-the-counter medications to stay awake.
- Weekly binge drinking of alcohol in the past 30 days. This is defined as consumption of five or more drinks on the same occasion for men and consumption of four or more drinks on the same occasion for women.
- Current smoker or substance (marijuana or hashish, synthetic cannabis, other illegal drugs, inhalants, synthetic stimulants, non-prescription cough or cold medicine to get high) user in past 30 days.
- No visit to the doctor for a routine checkup in past 12 months.
- Risky sexual behavior in past 12 months defined as two or more sexual partners or sex with a new partner without a condom.
Covariates
These included sociodemographic variables identified from the literature or a priori understanding to be associated with risk behaviors and health outcomes. They included i) service branch, ii) sex, iii) age group, iv) pay grade, v) race/ethnicity, vi) education level, vii) marital status, viii) having dependent children, ix) number of deployments, x) current housing status and xi) sexual orientation (lesbian, gay or bisexual versus not).
Statistical Analysis
Weighted prevalence and standard error (SE) were reported for the ADSM characteristics, perceived health status and doctor-informed medical conditions. Bivariate associations were tested using weighted Rao-Scott tests. Concordance in actual versus perceived health status was explored based on dichotomous variables of perceived health (good (defined as good, very good or excellent) versus poor (defined as fair or poor) and medical conditions (0 versus 1+ conditions). Crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using weighted log-binomial regression models to assess associations between ADSM characteristics and perceived good health status as well concordance between health status and the presence of medical conditions (defined as perceived good health in the absence of medical conditions or perceived less than good health status in the presence of medical conditions). Adjusted models controlled for all the sociodemographic covariates listed above. This model was used due to the high prevalence of perceived good health status. Ordered logistic regressions were used to explore the associations between ADSM characteristics and perceived health status as an ordinal variable. Statistical significance was set at 0.05 for all statistical tests. STATA 17.0 (College Station, TX: StataCorp LLC.) and SAS 9.4 (RTI International, Research Triangle Park, NC) were employed to confirm all analyses.
Results
Description of Study Population
Table 1 shows the characteristics of the study population of ADSMs by their perceived health status. ADSM were mostly male (83.3%), less than 35 years old (77.7%), with a high school level of education or less (64.4%), non-Hispanic White (57.6%), with no dependent children (60.3%), and deployed at least once (60.4%). Of note, 14.6% of ADSM perceived their health status to be excellent, 37.7% considered their status was very good, 36.2% thought their status was good, while 9.7% identified their status as fair and 1.7% described it as being poor. Thus, 88.5% perceived their health status to be good (or very good or excellent), while 11.5% perceived their health status to be poor (or fair). In addition, the majority of ADSM characteristics differed significantly by perceived health status.
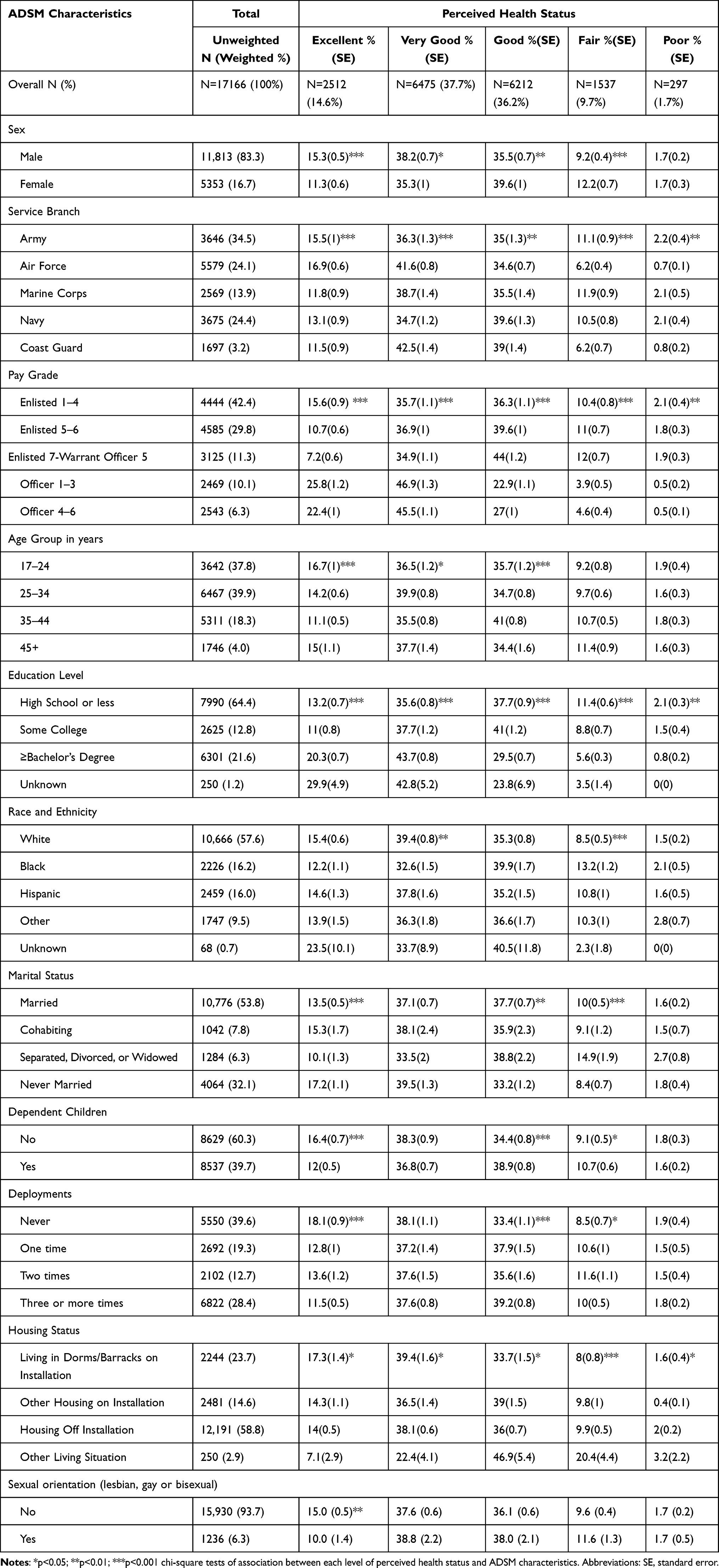 |
Table 1 ADSM Characteristics by Their Perceived Health Status, 2018 Department of Defense Health-Related Behaviors Survey (N = 17166) |
Medical Conditions and Risk Behaviors by Perceived Health Status
Table 2 highlights the prevalence of doctor-informed medical conditions and risk behaviors among ADSMs as well as by their perceived health status. The most prevalent medical conditions were bone, joint, or muscle injury or condition (26.4%), back pain (24.6%), obesity (14.4%) and high blood pressure (9.1%). Other medical conditions included high cholesterol (4.2%), asthma (1.7%), high blood sugar (0.9%), angina or coronary heart disease (0.3%), and heart attack (0.1%). Furthermore, there was a significant association between all medical conditions and ADSM perceived health status. The overall mental health distress (mean k6) score was 5.7 (range 0 to 24). With regard to risk behaviors, many ADSM had high levels of screen time use (65.0%), bad sleeping habits (53.1%) in the past month, while 41.7% reported risky sexual behavior in the past year and 29.7% did not have a routine health check-up in the past year.
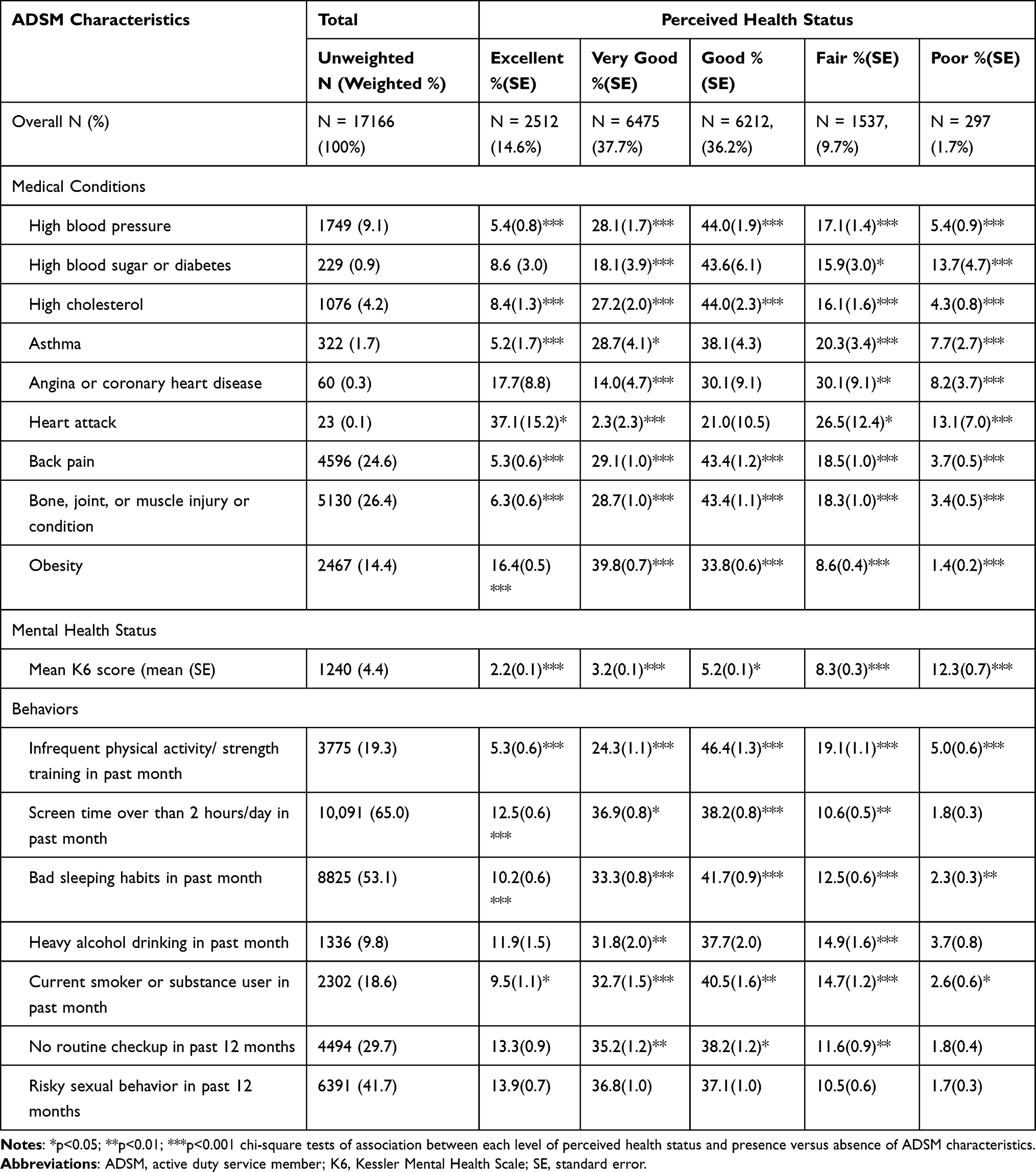 |
Table 2 Medical Conditions and Risk Behaviors Among ADSM by Their Perceived Health Status, 2018 Department of Defense Health-Related Behaviors Survey (N = 17,166) |
Figure 2 summarizes the average number of medical conditions and risk behaviors among ADSMs by their perceived health status. As perceived health status changed from excellent to poor, the percentage of ADSMs with no medical conditions reduced (78% to 19%), while the percentage with three or more conditions increased (2% to 31%). Similarly, the percentage of ADSMs engaging in three or more risk behaviors increased from 35% to 57% among those who perceived their health status to be excellent and poor, respectively.
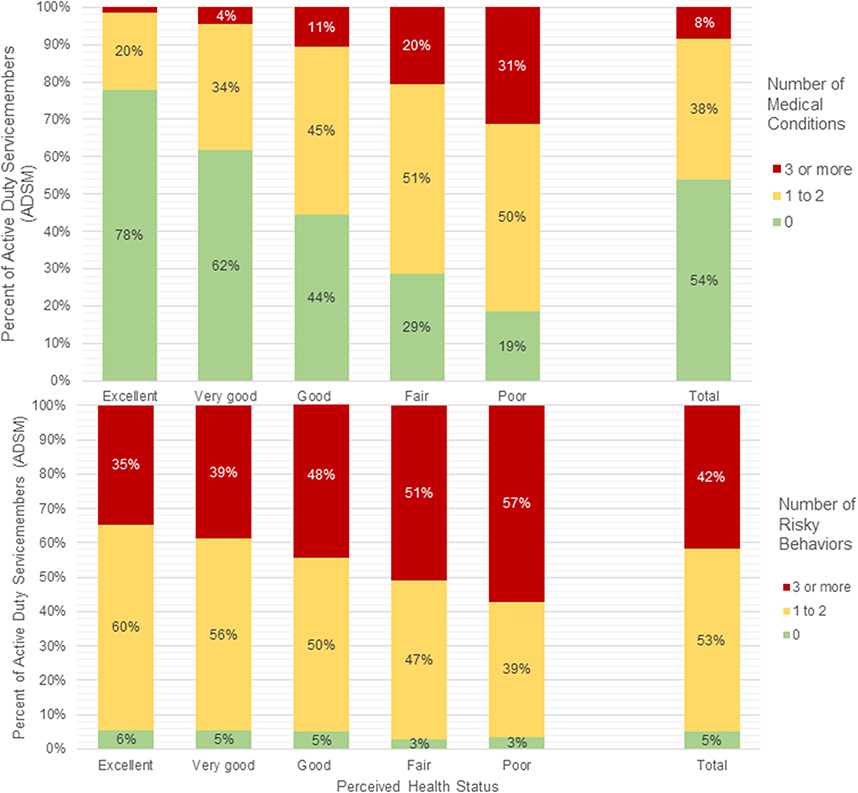 |
Figure 2 Number of Medical Conditions and Risky Behaviors among US Active Duty Service Members by their Perceived Health Status, 2018 Department of Defense Health-Related Behaviors Survey (N = 17,166). |
ADSM Characteristics Associated with Perceived Good Health Status
Table 3 shows the crude and adjusted odds ratios using logistic regressions of ADSM characteristics associated with perceived good health status. Sociodemographic factors positively associated with perceived good health included being in the Air Force, Navy, and Coast Guard compared with the Army, increasing pay grade and levels of education. Conversely, being female, older age, and Black, and housing off the installation were associated with reduced odds of perceiving good health status.
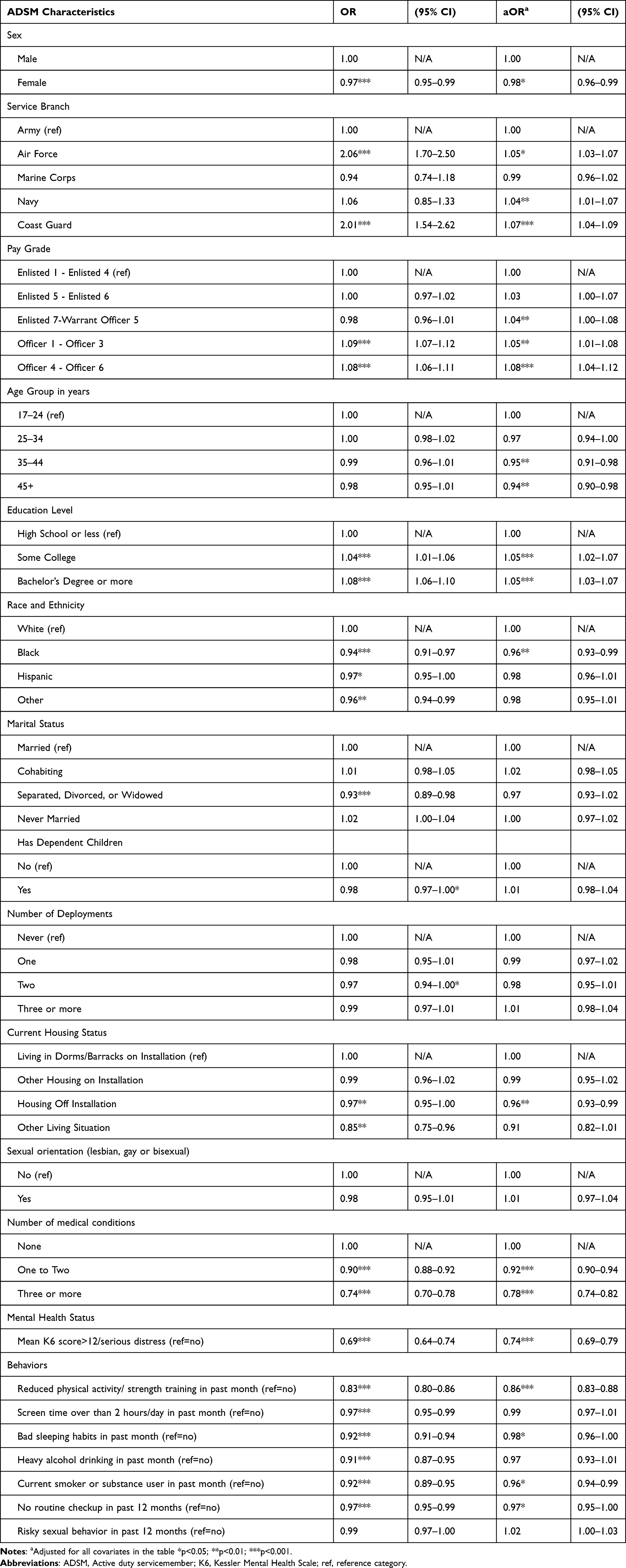 |
Table 3 Crude and Adjusted Odds Ratios of Perceived Good Health, 2018 Department of Defense Health-Related Behaviors Survey (N = 17166) |
The likelihood of perceiving good health status was lower as the number of medical conditions increased from zero to one/two (adjusted odds ratio (aOR): 0.92; 95% Confidence Interval (CI): 0.92, 0.94) and to three or more medical conditions (aOR: 0.78; 95% CI: 0.74, 0.82).
In addition, a K6-score greater than 12 and many risk behaviors were associated with reduced odds of perceiving a good health status (aOR ranging from 0.98 among ADSM with bad sleeping habits to an aOR of 0.86 among ADSM with reduced physical activity/strength training). On the other hand, screen time, heavy alcohol drinking or risky sexual behavior were not significantly associated with perceived good health status. Additional results from ordered logistic regression of perceived health as an ordinal variable by ADSM characteristics are presented in Supplemental Table 1. Similarly, perceived health status was progressively better (each unit increase from poor to excellent) with increasing pay grade and education level, worsening with presence of medical conditions and engagement in risk behaviors.
Concordance in Perceived Health Status and Medical Conditions
Figure 3 displays the concordance between perceived health status and medical conditions. Among all ADSMs, 50.8% accurately perceived good health (in the absence of medical conditions), 37.8% inaccurately perceived or overestimated their good health (perceived good health with medical conditions present), 8.3% accurately perceived less than good health status (in the presence of medical conditions), while 3.1% inaccurately perceived or underestimated their poor health (perceived poor health in the absence of medical conditions). Of note, the correlation between presence of medical conditions and perceived good health status was 0.40.
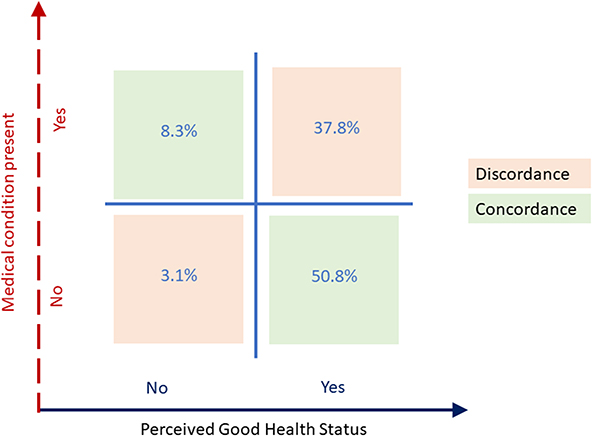 |
Figure 3 Concordance in Perceived Health Status and Medical Conditions Present among US Active Duty Service Members, 2018 Department of Defense Health-Related Behaviors Survey (N=17,166). |
Table 4 presents the crude and adjusted odds ratios of concordance between ADSM perceived health status and medical conditions. Concordance is defined as perceived good health in the absence of medical conditions or perceived less than good health status in the presence of medical conditions. Factors associated with increased odds of concordance included coast guard service branch (aOR: 1.14; 95% CI: 1.06–1.21), Officer 1–3 pay grade (aOR: 1.10; 95% CI: 1.02–1.18) and not having a routine medical checkup in the past year (aOR: 1.09; 95% CI: 1.04–1.13). On the other hand, the odds of concordance was reduced among the following: older ADSM aged 35–44 years (aOR: 0.75; 95% CI: 0.68–0.81) or 45 years and above (aOR: 0.61; 95% CI: 0.54–0.69); those with dependent children (aOR: 0.89; 95% CI: 0.84–0.95); having one (aOR: 0.94; 95% CI: 0.89–1.00) or three or more deployments (aOR: 0.89; 95% CI: 0.84–0.95); living in other housing on (aOR: 0.92; 95% CI: 0.85–0.99) or off installation (aOR: 0.93; 95% CI: 0.88–0.99); screen time more than two hours per day (aOR: 0.94; 95% CI: 0.90–0.98) or bad sleeping habits in the past month (aOR: 0.85; 95% CI: 0.82–0.89).
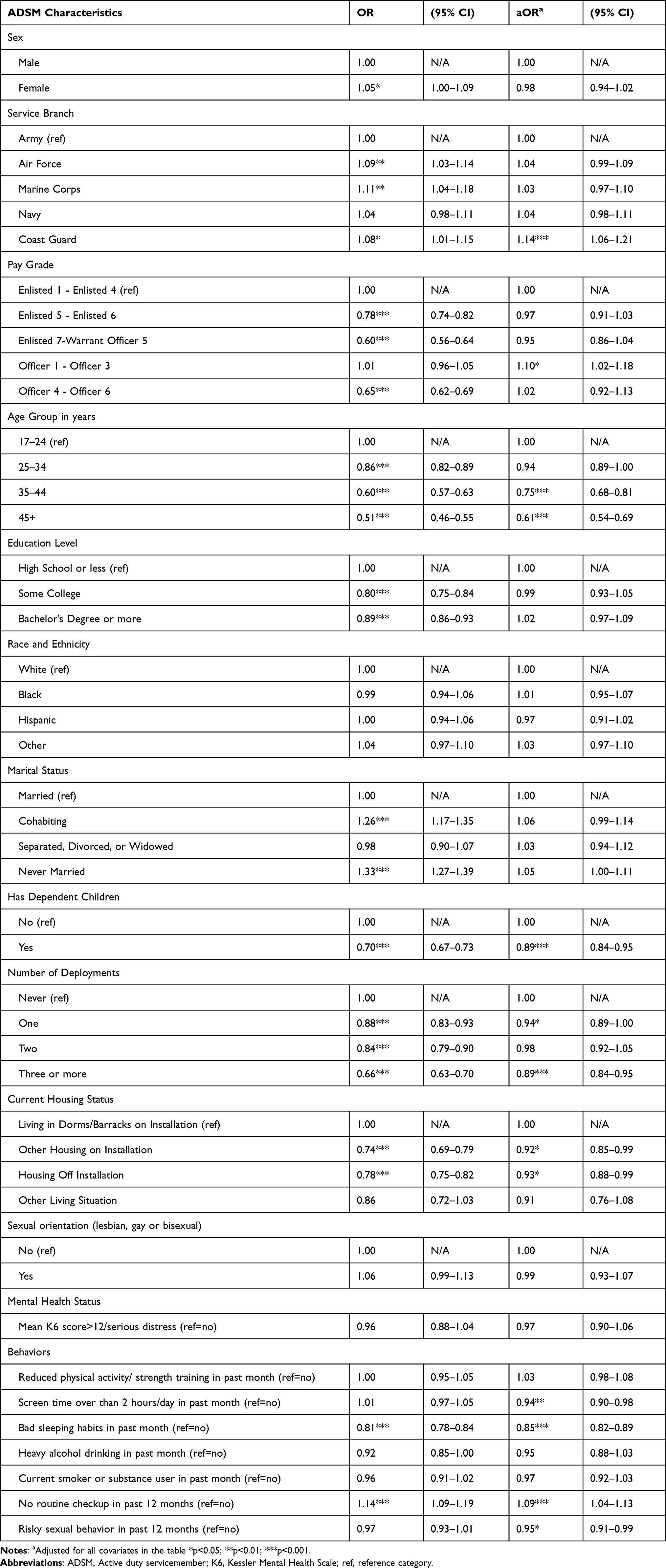 |
Table 4 Crude and Adjusted Odds Ratios of Concordance Between Perceived Health Status and Medical Conditions, 2018 Department of Defense Health-Related Behaviors Survey (N = 17166) |
Discussion
This exploratory study assessed prevalence of perceived health status and its interconnections with doctor-informed medical conditions, risk behaviors and sociodemographic characteristics among ADSMs in the US Military. Per the conceptual framework, this study hypothesized that ADSM’s perceived good health status was negatively associated with the presence of medical conditions, engagement in risk behaviors as well as certain sociodemographic characteristics. The high prevalence of perceived good health status observed in this study may corroborate prevailing expectations of health standards, ideals of self-image and other social norms within the military.26 However, the rates of perceived good health status among ADSMs were comparable with the age-adjusted rates among the general US population in 2018 at 88.5%,6 and 90%, respectively, which challenges the healthy soldier effect assumption in which military populations’ are presumed to be fitter and healthier than the general population due to initial physical screenings for service, requirements to maintain a certain standard of physical well-being, and better access to medical care during and after military service.27 However, comparability in perceived health status across US ADSM and general populations does not appear to translate to a similar comparability in actual health status as rates of chronic medical conditions such as obesity, hypertension and diabetes were notably lower among ADSM compared to the general US population. Among ADSM, the most prevalent doctor-informed medical conditions included back pain, bone, joint, or muscle injury or condition as well as obesity. These musculoskeletal medical conditions may be attributable to the fact that ADSMs engage in high levels of physical activity.28 In addition, obesity assessed using body mass index might reflect high muscle mass and not a true measure of nutrition or physical fitness.29
Study findings demonstrate a relationship between perceived health status, doctor-informed medical conditions and behaviors. Specifically, presence of an increasing number of medical conditions, reduced physical activity, poor sleeping habits, current smoking/substance use, and lack of routine medical checkup were inversely associated with perceiving a good health status. These associations may reflect ADSM beliefs that these risk behaviors result in poorer health. These findings emphasize the promotion of healthy behaviors and prevention of health conditions as important to perceived health. Engaging in healthy behaviors might help ADSM feel better about themselves and perhaps be more focused on the mission and able to fulfill assigned military duties and overall readiness. Alternatively, ADSM who feel healthy may wish to avoid risky behaviors in order to maintain their perceived good health status.30 Thus, the directionality and temporality of the relationship between risk behaviors and perceived good health status needs to be further explored using longitudinal studies. Of note, the study did not reveal any association between screen time, heavy alcohol use or risky sexual behaviors with perceived health status, warranting future exploration to understand this phenomenon.
The study also demonstrated concordance or agreement between perceived health status and medical conditions among two-thirds of ADSM. However, the remaining third of ADSM had incorrect perceptions of their health status when compared with actual medical conditions present. It is unclear if this is comparable with the general populations, prompting the need for further research. Furthermore, concordance was seen to be reduced among presumably more experienced ADSM (who were older, with dependent children or had been deployed). It is worth researching the degree to which such aspects of the military experiences might be impacting ADSM’s ability to correctly assess their health status.
The interrelationships between behaviors, perceptions and medical conditions have implications for the health literacy and seeking of health services among ADSM. This paper posits that perceived health status may be an indirect measure of health literacy.31 This is important in an increasingly fiscally restrained Military Health System where access can be positively impacted by informed self-care measures.32 If an active-duty service member (ADSM) perceives their health status correctly or has high health literacy, s/h/they can judiciously use limited health resources.32 Interventions that promote health literacy, address treatment-seeking stigma31 and demand-generation for needed health services need to be complemented with interventions that ensure access and supply of health services for ADSMs.32 This is particularly important given the fiscal austerity measures faced within the military health system.33 In addition, it is to the US Military’s advantage to cultivate an environment where wellness is prioritized as study findings highlight the role of mental health in perceived health status. This includes the implementation of relevant policies and interventions that reduce mental health distress and promote work/life balance within the military population.34 Additional research on how to promote resilience is needed as this remains a potential mitigating factor for mental distress and other downstream effects including health status.35
This study also highlighted heterogeneity in perceived health status within ADSMs with perceived worse health status among women, enlisted, and black service members despite adjusting for a large variety of factors, including those which are intermediates in causal pathways. The military population is typically considered to be an equal access environment in which there are substantially less health disparities. However, persisting race, ethnicity and social differences suggest the need to further explore ADSM intersectionality,36 the role of social determinants of health37 and their influence on readiness as well as the need for targeted interventions to such sub-groups.
This novel study exploring interrelationships between perceived health status, medical conditions and risk behaviors within the US military boasts a few strengths, including the use of a large, nationally representative sample with robust sociodemographic, medical and behavioral data and a conceptual framework detailing hypothesized pathways. The large sample size allowed a detailed examination of perceived health status (as an ordinal scale) by ADSM characteristics. However, key limitations include the use of self-reported data which may be subject to social desirability or recall bias, the cross-sectional study design which limits the ability to make causal inferences, and unmeasured confounding from other mental health conditions and psychosocial factors which might influence perceived health status. As with most of HRBS, we noted a suboptimal response rate (9.6% weighted). However, sample weights were used to generate similar estimates of ADSM population characteristics. Thus, this study is positioned as a simple exploratory study to inform the design of future research and/or longitudinal studies to corroborate study findings and further elucidate hypothesized causal pathways. Additional qualitative research may explore how ADSM perceive their health status, what it means to them and how it is influenced by internal and external factors. We also acknowledge that unmeasured psychosocial constructs identified in the conceptual framework may be associated with ADSM’s perceptions of their health status.38 Such constructs include perceived vulnerability, perceived severity of medical conditions, perceived norms regarding health status within the military as well as ADSM’s personal values relating to health.39 Future prospective studies should aim to better explore psychosocial factors influencing perceived health status in order to identify additional opportunities for relevant interventions.
Conclusion
In conclusion, this study employed a positive epidemiology approach to assess correlates of perceived good health status among US ADSM, which was negatively associated with the presence of doctor informed medical conditions and engagement in risky behaviors. Most ADSM demonstrated concordance between their perceived health status and medical conditions, but this was significantly lower among ADSM who were older, with dependent children or had been deployed. Study findings suggest that interventions promoting healthy behaviors, health literacy and treatment-seeking may influence perceived health status and mitigate medical conditions among ADSM, thus improving the US Military readiness, resilience and mission success.
Data Sharing Statement
The data that support the findings of this study are available from RAND and DOD but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of RAND and DOD.
Ethical Approval and Informed Consent
This secondary data analysis research was reviewed by the Uniformed Services University (USU) Human Research Protections Program (HRPP) which granted ethical approval waiver for the study with a determination of Research Not Involving Human Subjects (Protocol DBS.2022.408). The HRBS study protocol and all methods were carried out in accordance with the Declaration of Helsinki and other relevant guidelines and regulations. Informed consent was obtained from all study participants. The HRBS study were approved by RAND’s Institutional Review Board (known as the Human Subjects Protection Committee), the Westat Institutional Review Board, the Coast Guard’s Institutional Review Board, the Office of People Analytics, the Office of the Under Secretary of Defense for Personnel and Readiness’s Research Regulatory Oversight Office, the Office of the Assistant Secretary of Defense for Health Affairs and the Defense Health Agency’s Human Research Protection Office, and the DoD Security Office. All survey materials included the survey report control system license number: DD-HA(BE)2189.
Acknowledgments
The authors thank all the active duty service members who participated in this study.
The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the Department of Defense.
Author Contributions
BO Conceptualized the study while BO and AA conducted all data analysis and drafted the manuscript. KC, JY and JM provided technical feedback to the manuscript. All authors read and approved the final version of the manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funding for this study.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Axon DR, Jang A, Son L, Pham T. Determining the association of perceived health status among United States older adults with self-reported pain. Aging Health Res. 2022;2(1):100051. doi:10.1016/j.ahr.2021.100051
2. Piko BF. Self-perceived health among adolescents: the role of gender and psychosocial factors. Eur J Pediatr. 2007;166(7):701–708. doi:10.1007/s00431-006-0311-0
3. Benyamini Y, Blumstein T, Lusky A, Modan B. Gender differences in the self-rated health–mortality association: is it poor self-rated health that predicts mortality or excellent self-rated health that predicts survival? Gerontologist. 2003;43(3):396–405. doi:10.1093/geront/43.3.396
4. Umar N, Aliyu MH, Otado J, Gillum RF, Obisesan TO. ethnic-based differences in the association of self-perceived health status and doctor’s office utilization: longitudinal study on aging. Clin Int Aging. 2011;6:295. doi:10.2147/CIA.S19935
5. Brandon LJ, Proctor L. Comparison of health perceptions and health status in African Americans and Caucasians. J Natl Med Assoc. 2010;102(7):590–597. doi:10.1016/s0027-9684(15)30636-2
6. Organization for Economic Co-operation and Development. OECD.Stat. Perceived health status; 2022. Available from: https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_STAT.
7. Escalera C, Strassle PD, Quintero SM, et al. Perceived general, mental, and physical health of Latinos in the United States following adoption of immigrant-inclusive state-level driver’s license policies: a time-series analysis. BMC Public Health. 2022;22(1):1609. doi:10.1186/s12889-022-14022-x
8. Ely GE, Miller K, Dignan M. The disconnect between perceptions of health and measures of health in a rural Appalachian sample: implications for public health social workers. Soc Work Health Care. 2011;50(4):292–304. doi:10.1080/00981389.2010.534342
9. Loprinzi PD. Factors influencing the disconnect between self-perceived health status and actual health profile: implications for improving self-awareness of health status. Preventive Medicine. 2015;73:37–39. doi:10.1016/j.ypmed.2015.01.002
10. VanderWeele TJ, Chen Y, Long K, Kim ES, Trudel-Fitzgerald C, Kubzansky LD. Positive Epidemiology? Epidemiology. 2020;31(2):189–193. doi:10.1097/EDE.0000000000001147
11. Haddock CK, Poston WS, Pyle SA, et al. The validity of self-rated health as a measure of health status among young military personnel: evidence from a cross-sectional survey. Health Qual Life Outcomes. 2006;4(1):57. doi:10.1186/1477-7525-4-57
12. Strecher VJ, Rosenstock IM. The health belief model. Cambridge Handbook Psychol Health Med. 1997;113:117.
13. Ajzen I. The theory of planned behavior. Organ Behav Human Dec Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
14. Rosenstock IM Health Belief Model; 2000.
15. Rosenstock IM, Strecher VJ, Becker MH. The health belief model and HIV risk behavior change. In: Preventing Aids. Springer; 1994:5–24.
16. Hollerbach BS, Haddock CK, Kukić F, et al. Comparisons of baseline obesity prevalence and its association with perceived health and physical performance in military officers. Biology. 2022;11(12). doi:10.3390/biology11121789
17. Ostchega Y, Fryar CD, Nwankwo T, Nguyen DT Hypertension prevalence among adults aged 18 and over: United States, 2017–2018; 2020.
18. Golenbock S, Kazman JB, Krauss S, Deuster PA. General health status in army personnel: relations with health behaviors and psychosocial variables. Qual Life Res. 2017;26(7):1839–1851. doi:10.1007/s11136-017-1523-7
19. Trump DH. Self-rated health and health care utilization after military deployments. Mil Med. 2006;171(7):662–668. doi:10.7205/MILMED.171.7.662
20. Kümmel G. Military identity and identity within the military. In: Handbook of the Sociology of the Military. Springer; 2018:477–493.
21. Gallo LC, Smith TW, Cox CM. Socioeconomic status, psychosocial processes, and perceived health: an interpersonal perspective. Ann Behav Med. 2006;31(2):109–119. doi:10.1207/s15324796abm3102_2
22. Meadows SO, Engel CC, Collins RL, et al. 2018 Department of Defense Health Related Behaviors Survey (HRBS): Results for the Reserve Component. Santa Monica, CA: RAND Corporation; 2021.
23. Covert EC, Baker AM, Gilani O. Evaluating clinical and demographic influences on health perception: a translation of the SF-12 for use with NHANES. SSM Popul Health. 2022;18:101081. doi:10.1016/j.ssmph.2022.101081
24. Nguyen HA, Anderson CAM, Miracle CM, Rifkin DE. The association between depression, perceived health status, and quality of life among individuals with chronic kidney disease: an analysis of the national health and nutrition examination survey 2011–2012. Nephron. 2017;136(2):127–135. doi:10.1159/000455750
25. Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Aust N Z J Public Health. 2001;25(6):494–497. doi:10.1111/j.1467-842X.2001.tb00310.x
26. Hamilton JA, Danish SJ, Perrin PB, McDonald SD. Exploring the social norms of help seeking in the military. Mil Behav. 2015;3(2):145–150. doi:10.1080/21635781.2015.1009213
27. McLaughlin R, Nielsen L, Waller M. An evaluation of the effect of military service on mortality: quantifying the healthy soldier effect. Ann Epidemiol. 2008;18(12):928–936. doi:10.1016/j.annepidem.2008.09.002
28. Roy TC, Springer BA, McNulty V, Butler NL. Physical fitness. Mil Med. 2010;175(suppl_8):14–20. doi:10.7205/MILMED-D-10-00058
29. Nevill AM, Stewart AD, Olds T, Holder R. Relationship between adiposity and body size reveals limitations of BMI. Am J Phys Anthropol. 2006;129(1):151–156. doi:10.1002/ajpa.20262
30. Herbenick D, Reece M, Schick V, Sanders SA, Dodge B, Fortenberry JD. Sexual behaviors, relationships, and perceived health status among adult women in the United States: results from a national probability sample. J Sex Med. 2010;7(Suppl 5):277–290. doi:10.1111/j.1743-6109.2010.02010.x
31. Williston SK, Bramande EA, Vogt DS, et al. An examination of the roles of mental health literacy, treatment-seeking stigma, and perceived need for care in female veterans’ service use. Psychiatr Serv. 2020;71(2):144–150. doi:10.1176/appi.ps.201800405
32. Ringel JS, Hosek SD, Vollaard BA, Mahnovski S. The elasticity of demand for health care. A Review of the Literature and Its Application Military Health System. 2002
33. Mender BH. FY2021 Budget Request for the Military Health System. Congressional Research Service Washington United States; 2020.
34. Bartone PT. Resilience under military operational stress: can leaders influence hardiness? Mil Psychol. 2006;18(sup1):S131–S148. doi:10.1207/s15327876mp1803s_10
35. Cooper DC, Bates MJ. Military health provider training and evaluation of a problem-solving intervention to reduce distress and enhance readiness among service members. Mil Med. 2018;184:5–6.
36. Eichler M. Seeing Sex, Gender, and Intersectionality in Military, Veteran, and Family Health Research. Vol. 7. University of Toronto Press; 2021:1–2.
37. Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129(1_suppl2):19–31. doi:10.1177/00333549141291S206
38. Cohen S, Kaplan GA, Salonen JT. The role of psychological characteristics in the relation between socioeconomic status and perceived health 1. J Appl Soc Psychol. 1999;29(3):445–468. doi:10.1111/j.1559-1816.1999.tb01396.x
39. Piko BF, Keresztes N. Self‐perceived health among early adolescents: role of psychosocial factors. Pediatr Int. 2007;49(5):577–583. doi:10.1111/j.1442-200X.2007.02430.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.