Back to Journals » Psychology Research and Behavior Management » Volume 19
Perceived Control in the NICU: Implications for Maternal Mental Health and Parenting in the NICU
Authors Aokalani MC, Wisner KL, Ngwa J, Ottolini KM, Andescavage NN, Limperopoulos C
Received 20 December 2025
Accepted for publication 1 May 2026
Published 12 June 2026 Volume 2026:19 590477
DOI https://doi.org/10.2147/PRBM.S590477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Mariana Cerqueira Aokalani,1 Katherine Leah Wisner,1,2 Julius Ngwa,1 Katherine Marie Ottolini,1,3,4 Nickie Niforatos Andescavage,1,3– 5 Catherine Limperopoulos1,4,5
1Developing Brain Institute, Children’s National Hospital, Washington, DC, USA; 2Department of Psychiatry, George Washington University School of Medicine and Health Sciences, Washington, DC, USA; 3Department of Neonatology, Children’s National Hospital, Washington, DC, USA; 4Department of Pediatrics, George Washington University School of Medicine and Health Sciences, Washington, DC, USA; 5Department of Obstetrics & Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, USA
Correspondence: Nickie Niforatos Andescavage, Email [email protected]
Purpose: We examined whether maternal stress in the Neonatal Intensive Care Unit (NICU) predicts parental involvement, measured as functional parenting (FP) and physical contact (PC), during hospitalization. We hypothesized that higher stress, particularly related to perceived lack of control, would be associated with reduced FP and PC.
Patients and Methods: A retrospective analysis was conducted on 51 parent–preterm infant dyads from a prospective longitudinal cohort in a level IV NICU. Maternal stress and anxiety were assessed within 2 weeks of birth using a reduced version of the Parental Stressor Scale: NICU (PSS: NICU), the Perceived Stress Scale (PSS), and the State–Trait Anxiety Inventory (STAI). FP and PC were extracted from medical chart logs and adjusted for hospitalization length. Multivariable regression models were tested, with best-fit models determined by Bayesian Information Criterion (BIC), and adjusted for gestational age of infant at delivery, caregiver education, and infant sex.
Results: Maternal stress associated with perceived lack of control over the infant’s medical care was significantly related to reduced FP (β = – 0.55, p < 0.001, BIC = – 10.78) and PC (β = – 0.50, p < 0.001, BIC = – 15.38), when controlling for gestational age at birth and maternal education. PSS and STAI were not associated with FP or PC in unadjusted or adjusted models, p > 0.35.
Conclusion: Elevated maternal stress linked to lack of control in the NICU predicts lower caregiver involvement, placing families at risk for disrupted bonding and poorer long-term outcomes. Findings underscore the need for dyadic interventions that reduce maternal stress, enhance caregiver agency, and promote parent–infant connection in the NICU. Findings are limited by the retrospective design, potential measurement variability in chart-documented parental involvement, small sample size, and single-site setting, which further limit generalizability.
Keywords: parental involvement, prematurity, maternal stress, relational health
Introduction
Approximately 12% of pregnant women worldwide deliver preterm, or before 37 weeks of gestation.1,2 Preterm birth (PTB) is associated with neonatal illness, death, and long-term neurodevelopmental challenges,3,4 with increasing rates over the period between 2016 and 2023, representing a significant public health issue. For parents and infants, being in the neonatal intensive care unit (NICU) is particularly stressful due to the consistent, frequent disruption, early separation, invasive medical procedures, and medical outcome uncertainty. Higher levels of toxic stress and co-regulation difficulties in infants admitted to the NICU occur in part from early separation and limited access of infants to nurturing caregiving. Infants requiring NCU admissions are prone to challenges in self-regulation, attention, and socioemotional development, with up to 26.4% experiencing developmental delays.5 During adolescence, children who were hospitalized in the NICU show higher rates of psychiatric disorders, including attention deficit hyperactivity disorder (ADHD), depression, anxiety, and autism spectrum disorder (ASD).2 These developmental outcomes likely result from both medical exposures related to underlying prematurity as well as relational risks from disrupted caregiving and attachment.
Parents of infants in the NICU also face significant psychological risks. Early separation due to NICU admission can interfere with the transition to parenthood and weaken early bonding.6,7 Compared to the general perinatal population, caregivers of infants admitted to the NICU are 30% more likely to develop perinatal mood and anxiety disorders.8 PTB disrupts parental attachment representations—the internal models through which they interpret their relationship with their infants9—as well as caregiver sensitivity (ability to understand their infant cues) and organize caregiving behavior.10 Parents of preterm infants are also more likely to exhibit disengaged or distorted attachment representations,11 which in turn predict less effective parenting behaviors. For example, in a review of 52 studies comparing preterm to full-term dyads,12 approximately half of those studies, a decrease in maternal sensitivity and an increase in intrusiveness were observed. Similarly, heightened parental perceptions of child vulnerability—referred to as the vulnerable child syndrome—are common after preterm birth, affecting up to 27% of NICU parents.13,14 High parental perception of child vulnerability is linked to impaired parenting, increased healthcare use, and adverse developmental and behavioral outcomes for the child.13
Despite these known risks to parental mental health and disruptions to early caregiving and attachment, less is known about the associations between parental mental health and developmental care (ie, medical-led treatments centered on emotional and developmental needs, such as decreasing auditory and visual stimulation, and Kangaroo care) within the NICU admission. Integrated, dyadic NICU interventions may benefit from combining developmental care with mental health support for caregivers. This study explored whether maternal stress related to the NICU experience was associated with physical contact (PC; eg, holding, skin-to-skin, touch) and functional parenting (FP; eg, feeding, diaper changing) behaviors. We hypothesized that higher maternal stress levels would correlate with lower FP and PC.
Prior studies have linked global maternal stress to caregiving behaviors in the NICU.15–17 Most of this work has assessed stress using standardized self-report measures, such as the Parental Stressor Scale: Neonatal Intensive Care Unit (PSS: NICU) and has relied on self-reported indicators of parental participation (eg, Assessment of Mothers’ Participation in Caregiving Scale15). While these studies have identified significant associations between higher maternal stress and lower caregiving involvement, they are limited by their reliance on subjective reports and relatively limited use of objective, behavioral measures of parent engagement (eg, chart-derived indicators of caregiving involvement). Furthermore, the literature has largely focused on global measures of psychological distress, with comparatively limited attention to NICU-specific dimensions of stress. In particular, perceived control within the NICU context has been understudied as a distinct and potentially significant factor influencing parental involvement. This represents an important gap, as perceived lack of control may more directly reflect the caregiving environment and day-to-day constraints shaping parent–infant interaction than global distress measures. Building on this literature, the present study differentiates between global maternal stress and NICU-specific perceived control and examines perceived control as a context-sensitive predictor of parental involvement. In doing so, it identifies a targeted, potentially modifiable mechanism underlying parent engagement in the NICU.
Materials and Methods
This study is a retrospective analysis of data from a prospective longitudinal cohort on brain development in preterm infants admitted to a level IV Neonatal Intensive Care Unit (NICU) conducted at Children’s National Hospital (CNH) in Washington, DC. Study procedures were approved by the CNH Institutional Review Board (Project PROTECT IRB Pro00002391), and written informed consent was obtained by at least one parent or legal guardian. This study complies with the Declaration of Helsinki.
Participants
Inclusion criteria for enrollment were premature infants, born before 37 weeks of gestational age (GA), whose parents spoke English or Spanish. Participants were excluded from the study if they presented the following: dysmorphic features or congenital anomalies suggestive of a genetic syndrome, metabolic disorders, chromosomal abnormalities, or congenital infection. By doing so, we aimed to reduce the biological confounders of parental involvement in the NICU while avoiding systematic biases in parental involvement associated with high prognostic uncertainty.
Parental Care in the NICU
Parent-newborn involvement was recorded as part of routine clinical care each shift by the bedside nurse in the electronic health record as follows:
Parent visited, parent called, caregiver interacted with care team, parent held patient, parent did skin-to-skin with patient, parent diapered patient, caregiver involvement in child care, parent bottle-fed patient, parent breastfed patient, caregivers at bedside, parent bathed patient, parent touched patient.
Parental care events were extracted from the medical record and categorized into two main groups: functional parenting (FP, ie, task-oriented caregiving, focused on meeting the infant’s basic physiological and medical needs, without requiring emotional attunement or relational engagement), which included bottle-feeding, diaper change, and bathing and physical contact (PC), which included the following caring behaviors: touch, holding, breastfeeding, and skin-to-skin. The number of days with at least one event in each group, classified as either FP or PC, was summed, and the total for each category was divided by the length of hospitalization. Caregiving involvement data were extracted from the electronic medical record using a standardized protocol defining specific caregiving activities (eg, feeding, holding, diapering) based on structured chart fields and nursing documentation. Data extraction was conducted by a single trained reviewer, and a subset of records was reviewed to ensure consistency in coding. Caregiving involvement is documented in the electronic medical records by the bedside nurse using a standardized protocol defining specific caregiving activities (eg, feeding, holding, diapering) under structured chart fields. Data extraction was conducted by business analytic tools of the identified chart field. A single trained reviewer conducted a second review of 10% of the records, selected randomly, to ensure consistency in coding. No inconsistencies were found. Each instance of PC and FP documented in the medical record was coded as present (1) or absent (0) for each hospital day. Scores were added and normalized by total length of stay to generate a standardized measure of caregiving involvement per day. This standardized approach ensured consistent application of extraction procedures across all records and improved reproducibility.
Caregiver Questionnaires
Standardized mental health assessments were administered to newborns’ mothers in the first two weeks after birth and are detailed below.
Perceived Stress Scale (PSS)
The PSS16 is a widely psychometrically sound tool to measure how stressful situations in one’s life are perceived. Each item is a statement that participants rate based on their feelings and experiences, and on how unpredictable, uncontrollable, and overloaded they perceive their lives to be over the past month. The scale is designed to be easy to understand and use across diverse populations.17
The PSS has multiple validated forms, with the 10- and 14-item versions being most common, each using a 5-point Likert scale with ten and fourteen items, respectively. In this study, we used the PSS-10 because of its higher psychometric properties compared to other versions, with Cronbach’s alpha and test-retest reliability above 0.70.
State-Trait Anxiety Inventory (STAI)
The STAI18 comprises two 4-point Likert scales of 20 items each, differentiating between state anxiety (short-term experience of anxiety) and trait anxiety (long-lasting experience of anxiety associated with a personality trait). This scale has an internal consistency coefficient that ranges from 0.86 to 0.95; test–retest reliability coefficients from 0.65 to 0.75 over a 2-month interval. Considerable evidence attests to the construct and concurrent validity of the scale.19
The State-Anxiety Scale is a sensitive indicator of changes in transitory anxiety experienced by patients in counseling, psychotherapy, and behavior-modification programs. It has been used to assess the level of anxiety induced by unavoidable real-life stressors. The Trait-Anxiety scale has proven helpful in identifying people who differ in motivation or drive level. STAI has been widely used in clinical research with parents, including studies of parental anxiety when a child is hospitalized in a pediatric ICU,20 maternal anxiety in the NICU setting and its impact on bonding,21 and the assessment of anxiety during pregnancy in relation to early attachment.22
The Parental Stressor Scale: Neonatal Intensive Care Unit (PSS:NICU)
The PSS: NICU23 is a 47-item 5-point Likert scale to measure the unique stressors experienced by parents of infants hospitalized in a neonatal intensive care unit. It is widely used in both clinical and research settings. It has three subscales: 1) Sights and Sounds (eg, monitors, alarms, and unfamiliar medical environment), 2) Infant Behavior and Appearance (eg, baby’s fragile or altered appearance), and 3) Parental Role Alteration (eg, inability to hold, feed, or comfort one’s baby). Internal consistency coefficients for the subscales range from 0.73 to 0.94, and test–retest reliability has been reported as satisfactory.
For this study, we used a 10-item adapted PSS: NICU for brevity and feasibility (Supplement B). We divided this questionnaire into two subscales: PSS: NICU A (Medical Vulnerability: stress associated with parents’ perception of their infant’s vulnerability, n=3 items), and PSS: NICU B (Parental Control: stress associated with parents’ perception of their lack of control over their infant’s condition and care, n=7 items).
Statistical Plan
Descriptive statistics were used to characterize the study sample. Continuous variables (eg, gestational age at birth, postmenstrual age at scan, maternal age, gravida, para, total hospitalization days, stress scores, and parenting involvement scores) were summarized using medians and interquartile ranges (IQR) when not normally distributed and using means and standard deviations when normally distributed. Categorical variables (eg, infant sex, delivery mode, maternal education) were summarized as frequencies and percentages.
PSS: NICU internal consistency was calculated to demonstrate acceptable internal consistency for both subscales Medical Vulnerability and Parental Control. We used PSS: NICU as predictors and adjusted for covariates (eg, gestational age, hospitalization days, infant sex, maternal parity). PSS: NICU scales were assessed as continuous variables and categorical variables (eg, level of anxiety) where appropriate. Both parenting involvement variables, FP and PC, were assessed separately. We compared the distribution of variables for both FP and PC (eg, differences by infant sex, postmenstrual age at PSS: NICU on FP and PC groups) using Fisher’s exact tests for categorical outcomes or the Kruskal–Wallis test for non-normal continuous data.
To test the central hypothesis, we conducted primary analysis using unadjusted models, followed by a secondary analysis with a multivariable regression model adjusted for infant gestational age at birth, maternal education, and potential confounders. Finally, we conducted an exploratory analysis through a backward stepwise regression. We calculated BIC and standardized betas for all models. No corrections for multiple testing were applied, given the exploratory nature of this study.
All statistical analyses were performed in R, version 4.5.0 (R Core Team, 2025). Linear regression models were computed using the stats package. Stepwise model selection was performed using the step() function. Bayesian Information Criterion (BIC) was calculated using the BIC() function, and standardized beta coefficients were obtained with the lm.beta package (version 1.5–1). Tables summarizing model coefficients and fit statistics were generated using sjPlot (version 2.8.12). Data manipulation and visualization were conducted using dplyr (version 1.2.1) and ggplot2 (version 3.5.3). Significance was set at p <0.05 (two-tailed).
Results
Sample Characteristics
From the initial 136 subjects enrolled, 51 mothers completed the PSS: NICU within the first 2 weeks of birth and were included in the primary analyses. Maternal age at delivery ranged from 19 to 38 years. Gestational age at birth was available for 51 infants, ranging from 24.00 to 34.57 weeks, with a median of 30.4 weeks (IQR = 6.9). Delivery mode was vaginal in 45.1% (n = 23), cesarean in 47.1% (n = 24), and unknown in 7.8% (n = 4). Among the infants, 52.9% (n = 27) were male. Median length of hospitalization was 56 days (IQR = 57). FP events (without a normal distribution), normalized to length of stay, had a median of 0.403 (IQR = 0.485), and PC (with a normal distribution) events had a mean of 0.625 and a standard deviation of 0.302. We then categorized these into low-moderate-high through a distribution-based approach, ±1 standard deviation (SD). Low parental involvement levels were assigned to values <1 SD, moderate levels for values between −1 and 1 SD, and high levels for values >1 SD (see Table 1 and Supplemental Tables 1a and 1b). Forty-five percent of infants did not have additional comorbdities beyond prematurity. Additional single comorbditiy was present in 15.7% of the cases, dual diagnoses in 13.7% of the cases, and three or more additional diagnoses in 25.6% of cases (see Table 2).
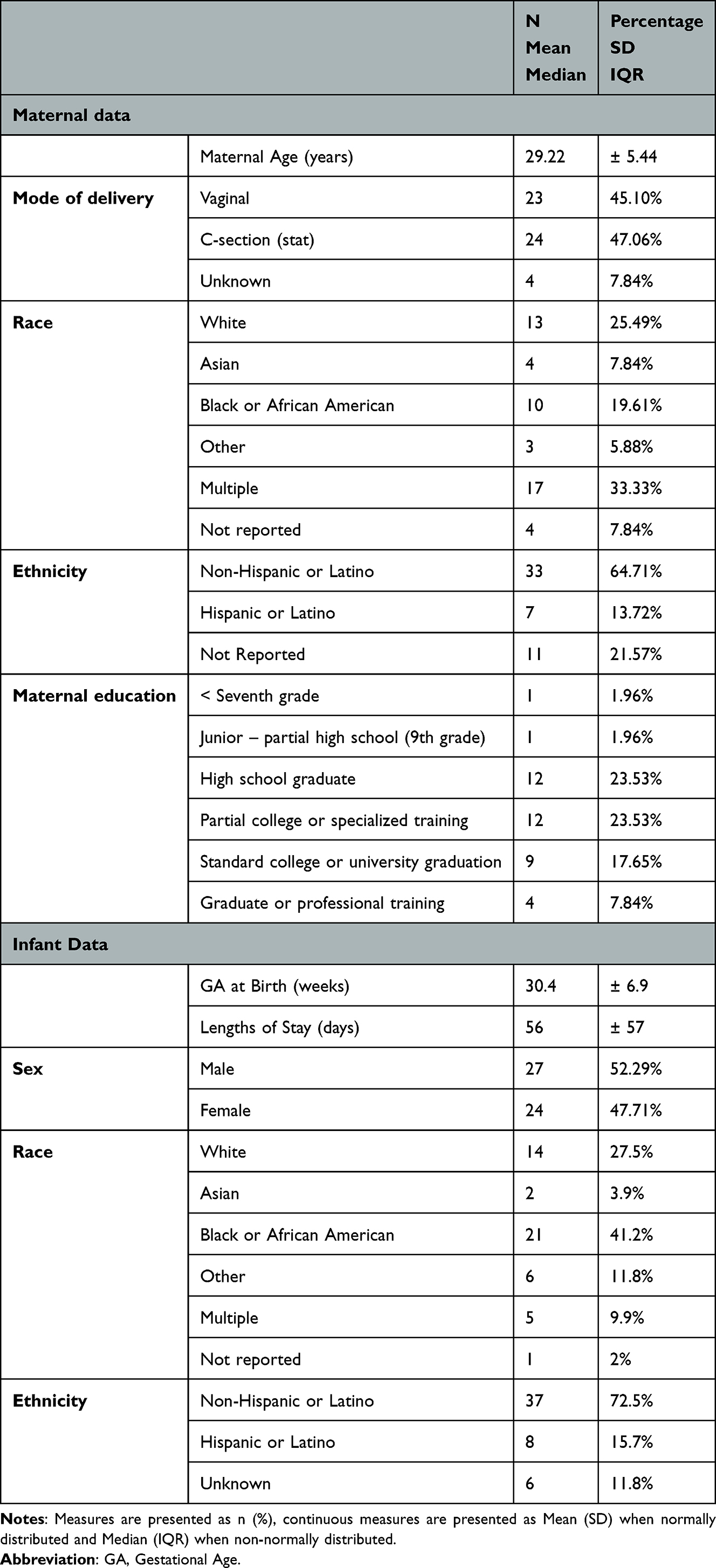 |
Table 1 Patient Characteristics |
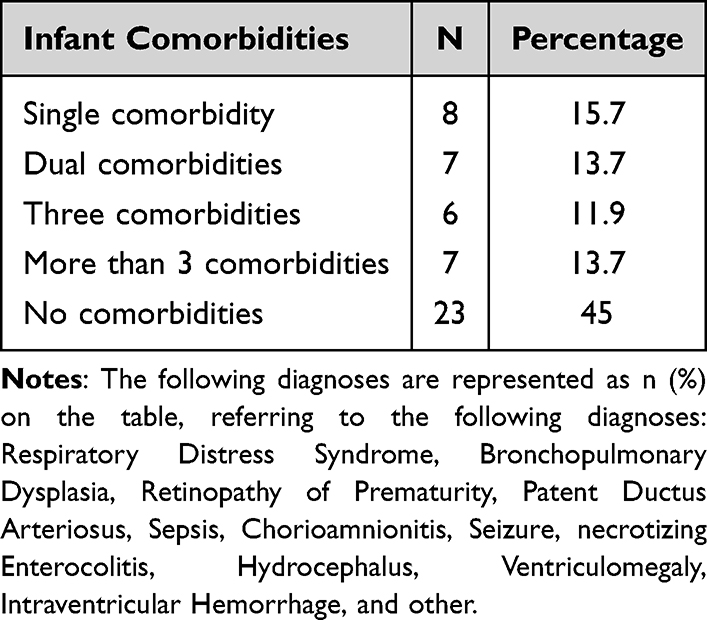 |
Table 2 Infants’ Comorbidities Characteristics |
The adapted PSS: NICU subscales demonstrated acceptable to excellent internal consistency for our sample. Cronbach’s α for PSS: NICU A (medical vulnerability) was α = 0.741, and for PSS: NICU B (lack of control) was α = 0.916. The two subscales, PSS: NICU A (associated with stress due to parental perception of the infant’s vulnerability, without a normal distribution), had a median of 25 (IQR 15.5), and PSS: NICU B (associated with stress due to parental perception of lack of control, with a normal distribution) had a mean of 6.593 and a standard deviation of 3.092.
The PSS had a mean of 19.86 (SD = 7.49). STAI-State had a mean of 44.73 (SD = 12.23), and STAI-Trait had a mean of 41.9 (SD = 10.80). The distribution of these stress measures is compressed toward the moderate range, with up to 71% of participants in this category. To mitigate the impact of this range restriction, we will treat these measures as continuous variables in all analyses (see Table 3).
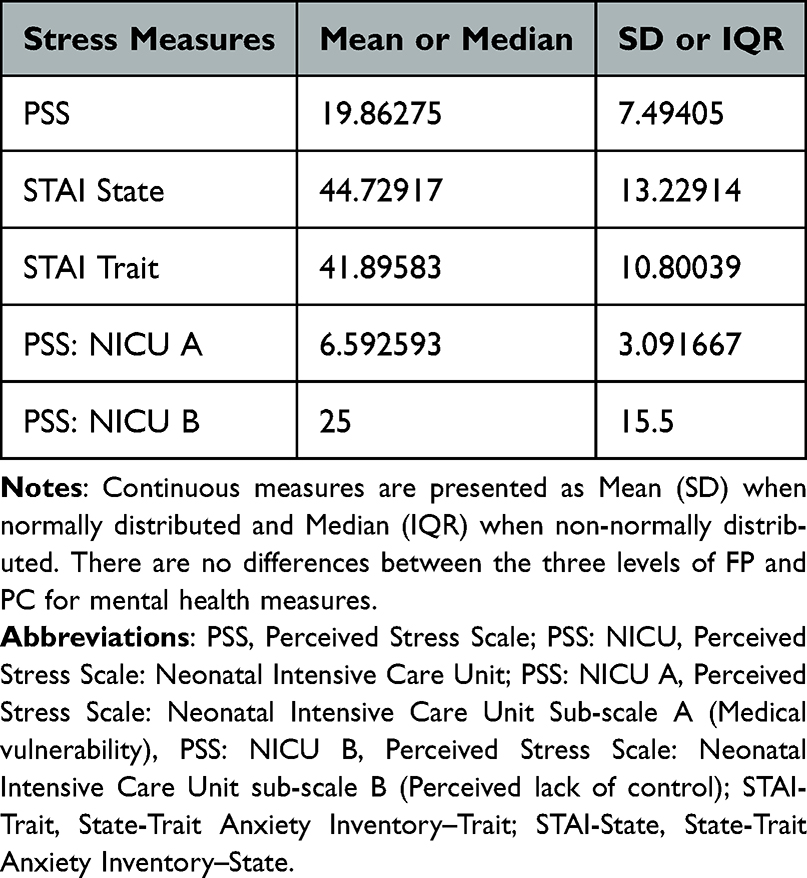 |
Table 3 Patient’s Mental Health Characteristics |
Associations Between Parental Stress and Anxiety with Parenting Involvement
To test our central hypothesis, we first examined whether individual measures of maternal stress or anxiety predicted parental involvement (see Supplemental Table 3). We examined whether maternal stress predicted parenting involvement using multivariable linear regression models with FP and PC as dependent variables. Predictor variables included PSS: NICU subscales (A and B), overall PSS scores, and maternal anxiety (STAI-State and STAI-Trait). Linear regressions indicated that FP was not significantly associated with PSS, STAI State, STAI Trait, NICU: PSS. Similarly, PC was not significantly associated with PSS, STAI, or PSS: NICU B. These findings suggest that maternal stress, in isolation, did not predict parenting involvement.
To estimate the effect of maternal stress while accounting for potential confounding variables, we developed models controlling for infant gestational age at birth, infant sex, and maternal education (see Supplemental Table 4). Because maternal stress (PSS, STAI-State, STAI-Trait) was colinear with maternal stress related to infant NICU hospitalization, these variables were analyzed separately in the adjusted models. To identify the most parsimonious set of predictors, we calculated each model’s Bayesian Information Criterion (BIC) as a measure of fit (see Table 4). Only maternal education (p < 0.003) and PSS: NICU B (Parental Control) (<.001) showed significant associations across all models. For both FP and PC, Model 4—which included GA at birth, maternal education, and PSS: NICU B (Parental Control)—offered the best fit, with BIC values of –10.78 and –15.38, respectively. These outperformed the next best models by ΔBIC = 13.90 and 13.63, providing strong evidence that this is the optimal model. For FP, the final model explained 66% of the variance (adjusted R2 = 0.66, p < 0.001). Significant predictors included maternal education (p < 0.001), gestational age at birth (p = 0.004), and PSS: NICU B (p < 0.001). Higher education and greater gestational age were linked to higher FP levels, while higher PSS: NICU B (Parental Control) scores were associated with lower FP levels. For PC, the final model explained 76% of the variance (adjusted R2 = 0.76, p < 0.001). Significant predictors included maternal education (p < 0.001), gestational age at birth (p < 0.001), and PSS: NICU B (Parental Control) (p < 0.001). Higher education and greater gestational age were associated with higher PC levels, whereas higher PSS: NICU B scores correlated with lower PC levels.
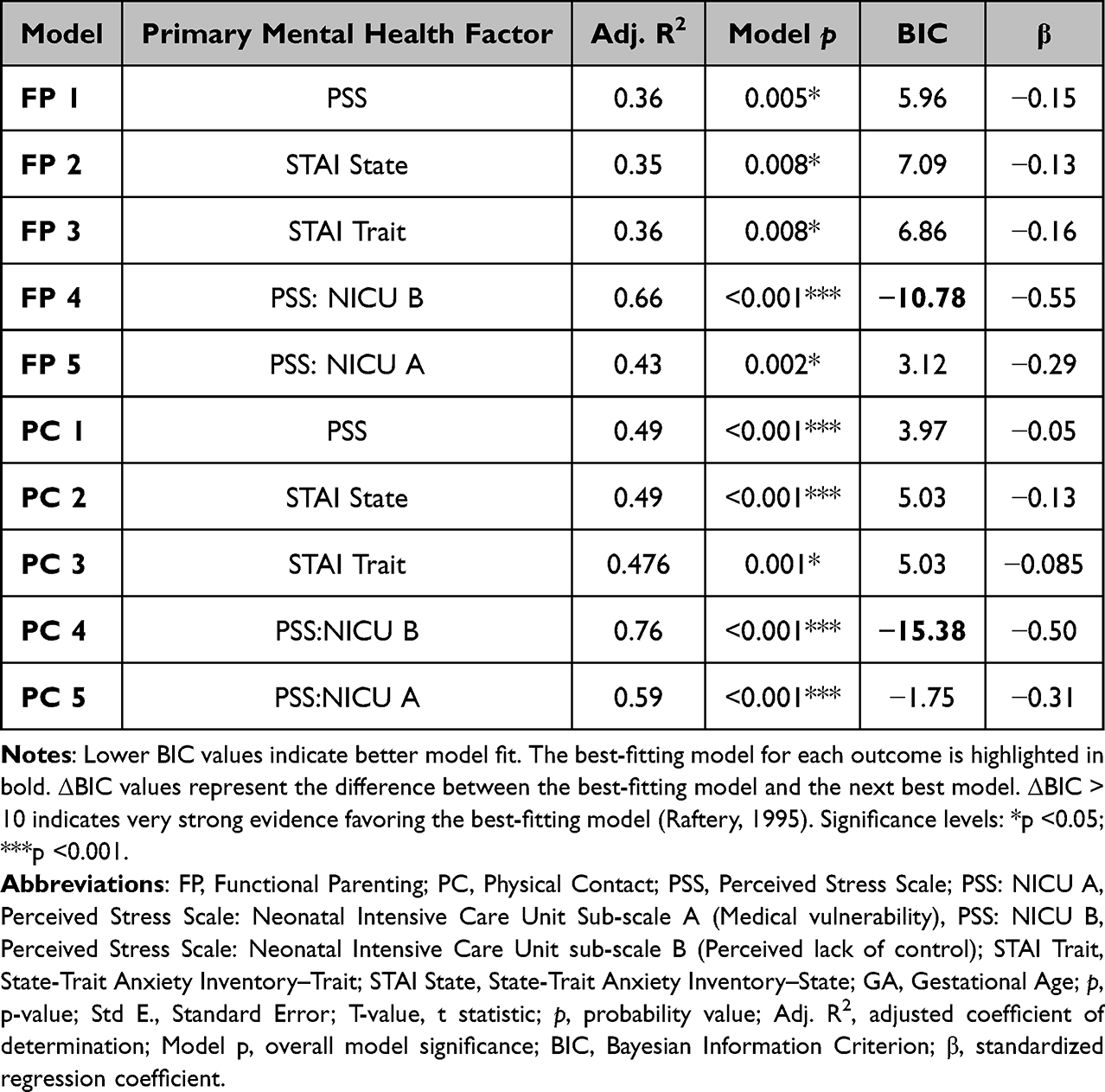 |
Table 4 Adjusted Models |
Exploratory Analysis Stepwise Regression
To explore both theory-driven models and data-driven selection procedures and identify the most parsimonious model, we perform an exploratory stepwise regression. Due to the colinear impact of maternal stress (PSS, STAI-State, STAI-Trait) on maternal stress related to infant NICU hospitalization, these variables were excluded from the adjusted models (see Tables 5 and 6). The results aligned with BIC-based model comparison, supporting Model 4 as the best-fitting and most parsimonious model.
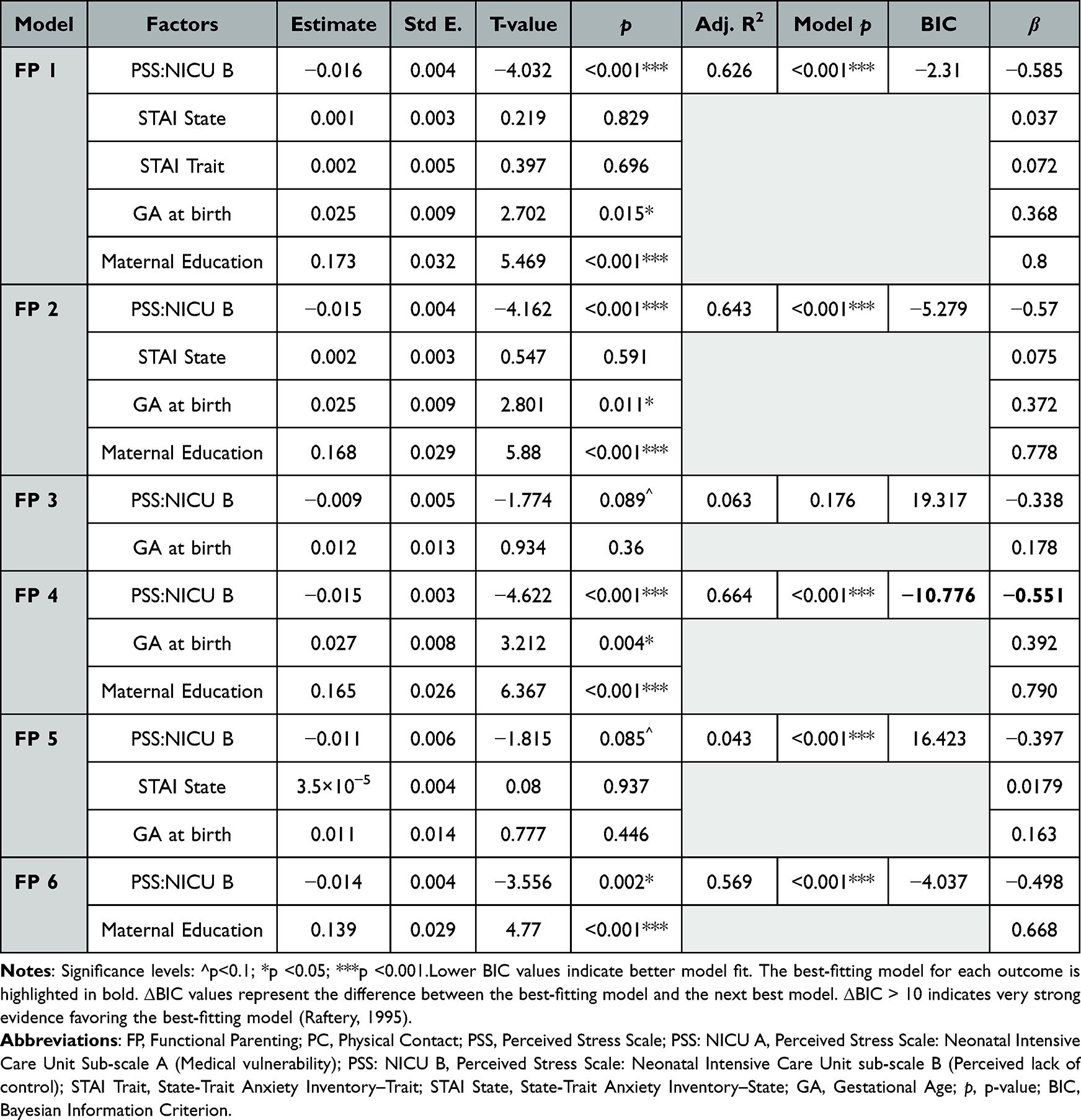 |
Table 5 Stepwise Regression for Functional Parenting |
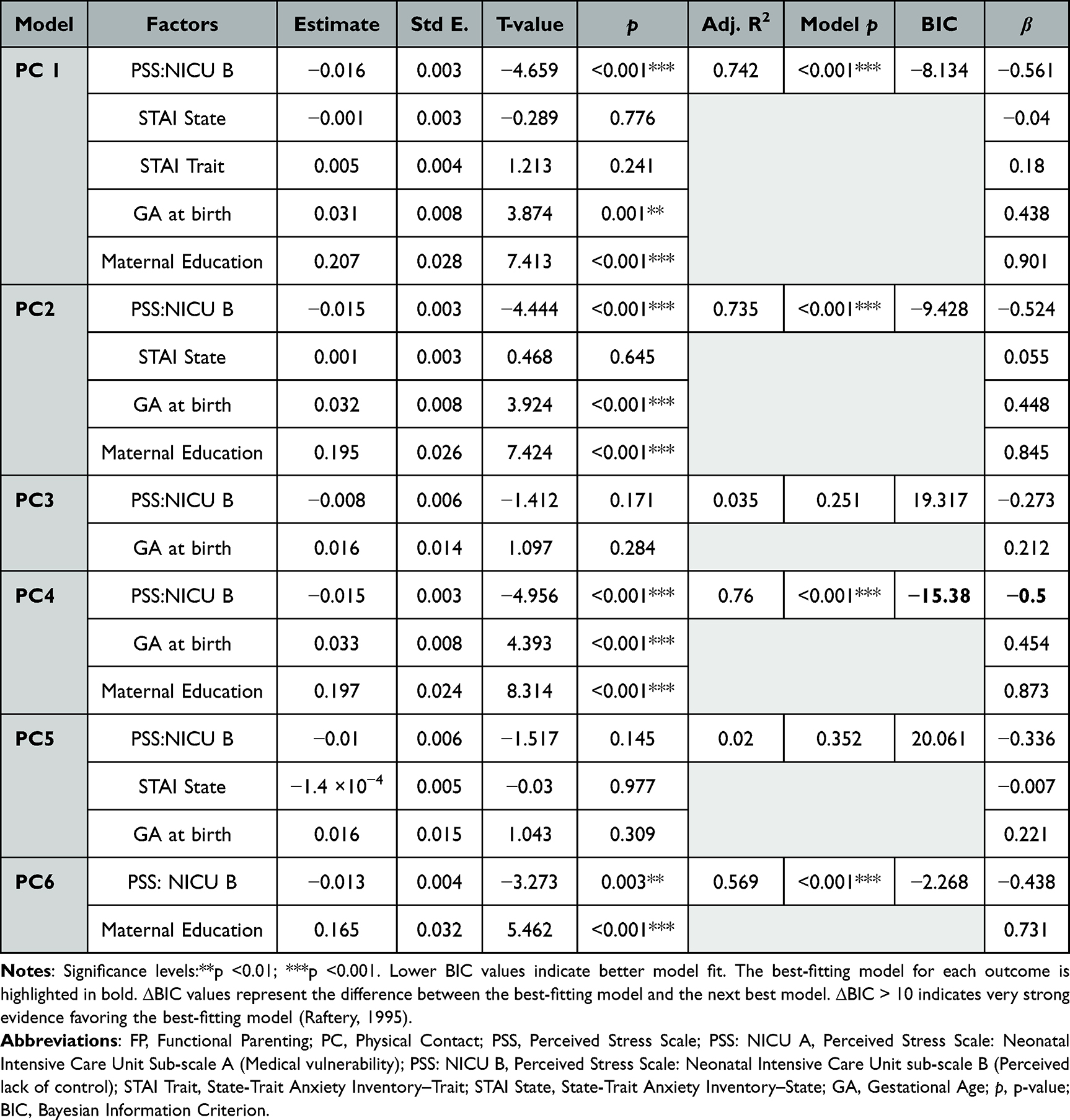 |
Table 6 Stepwise Regression for Physical Contact |
For functional parenting, the final model explained 66.4% of the variance (adjusted R2 = 0.664, model p < 0.001). Significant predictors included maternal education (p < 0.001), gestational age at birth (p = 0.004), and PSS: NICU B (Parental Control) (model p < 0.001). Higher education and greater gestational age were linked to higher levels of functional parenting, while higher PSS: NICU B scores, consistent with higher scores of maternal stress surrounding perceived control, were linked to lower levels of functional parenting. For physical contact, the final model explained 76% of the variance (adjusted R2 = 0.76, model p < 0.001). Maternal education (p < 0.001), gestational age at birth (p < 0.001), and PSS: NICU B (p < 0.001) were significant predictors. Similar to functional parenting, higher education and gestational age predicted more frequent physical contact, while higher PSS: NICU B scores predicted less physical contact. The regression analysis demonstrated adequate statistical power (power = 0.99; df = 47; critical t = 1.678) for both FC and PC. This study identifies NICU-specific perceived maternal control (PSS: NICU B), rather than global maternal stress, as a key predictor of parental involvement in the NICU.
Discussion
Main Findings
Parental involvement in the NICU, whether expressed as FP or PC, is influenced by multiple factors, particularly infant gestational age and maternal education. Stepwise regression revealed that both FP and PC were negatively related to maternal stress associated with perceived lack of control over their infant’s medical condition and care. The model fit for FP (BIC = –10.78) and PC (BIC = –15.38) surpassed the best alternative models by more than 13 BIC units, providing solid evidence for these final models. Maternal stress related to perceived lack of control was strongly and negatively associated with both functional parenting (β = –0.55, p < 0.001) and physical contact (β = –0.50, p < 0.001), indicating that parents who felt more helpless and with minimal control were less likely to engage in hands-on caregiving and physical bonding activities. This represents a large effect size, underscoring the central role of parental perceptions of helplessness in shaping real-time caregiving behaviors in the NICU. Interestingly, we found no significant association between parental involvement in the NICU and scores on the PSS or STAI. These measures reflect mothers’ global perceptions of stress and anxiety in daily life, which may not directly translate to caregiving behaviors in the NICU. Global measures of stress and anxiety may fail to predict parental involvement because: (1) they are not context-specific, (2) coping strategies and motivation can buffer general distress, (3) situational constraints in the NICU influencing behavior (eg, hospital policies, limited parental leave), and (4) infant-specific stress is more proximally related to hands-on caregiving and bonding.24 Additionally, the unique environment of a Level 4 NICU and our relatively small sample may limit the ability to detect associations between global stress measures and parental involvement.
Previous research has shown maternal stress in the NICU is associated with several factors: 1) parents’ mental health, 2) parents’ perception of infants’ vulnerability, 3) attachment representation, 4) parental self-efficacy, and 5) medically fragile infants’ characteristics (eg, communication, level of discomfort or distress).25,26 These factors impact parental emotional availability to connect with their infant, as well as the quality and quantity of their interactions.27,28 Indeed, premature newborns are often perceived as difficult and fussier than term newborns. Caregivers of premature infants have difficulties discerning their newborn’s cues and therefore responding to their needs appropriately, which impacts their sense of parenting self-efficacy. All these components add to the stress of having a newborn in the NICU, parents’ representation of their baby and, consequently, on their parenting behaviors, described as intrusive, controlling, or withdrawal and avoidant.29–31 In contrast, our findings showed no significant associations between global stress measures (PSS, STAI) and parental involvement. This divergence may reflect the difference between generalized distress and context-specific stress related to the NICU environment. Consistent with studies that emphasize context-stressors,24,32,33 our results suggest that infant-specific stress (PSS: NICU) is a stronger predictor to parental engagement in caregiving within a specific multifactorial environment. Parents may experience elevated global stress yet remain actively involved in caregiving when hospital context or use engagement as coping resources. This distinction underscores the importance of assessing contextualized stress constructs when predicting parental behavior in intensive care settings.
PC may be influenced by infant medical stability,34 unit policies and staffing,35 and practical or structural barriers such as transportation, leave, and visiting hours. Parental psychological readiness is important, but structural and infant clinical factors often have a larger impact on uptake.36 Parental involvement in the NICU is inversely related to GA at birth, meaning that greater prematurity is associated with lower parental involvement rates, both in FC and PC. This may be due to more complex medical conditions for the infant, which are closely associated with GA at birth, as well as structural barriers that may limit extended employment leave. This contrasts with FP, which is strongly connected to parental skills/education,37 training/support from staff to involve parents in their infant’s care,38 and validation of caregivers’ emotional experiences, leading to an empowering transition into parenthood.39 Reduced time at the bedside is paramount for opportunities for PC, which requires more extended visits than FP, for which trained parents can participate in care tasks during shorter visits. Parents with higher education can have more resources (eg, parental leave, childcare support, enhanced medical literacy), thereby predicting greater engagement in functional tasks (such as feeding and diapering) when invited/supported, and in PC. While previous studies have identified predictors of maternal stress and correlates of involvement (eg, infant illness severity, NICU structure, parental education), few have connected specific dimensions of stress—particularly perceived loss of control—to observable, moment-to-moment caregiving behaviors (functional and physical contact).
GA at birth is linked to higher parental negative feelings and maternal stress, which predict lower quality in parent–infant interactions (eg, sensitivity, responsiveness, warmth, reciprocity, involvement).29 Our findings highlight caregiver perception of lack of control, as well as their infant condition and maternal stress, as key factors affecting their behavior. Caregiver sense of a lack of control diminishes as staff manage the daily care of premature infants. Parents often feel helpless and excluded, struggling with the transition into their new roles as parents.40 The stress related to caregivers’ lack of control in the NICU undermines parental identity and self-efficacy. As a result, it reduces engagement in both essential PC and FP and may lead to maladaptive parenting styles such as withdrawal or overprotection.7
Maternal stress caused by a lack of control in the NICU, prematurity level, and caregivers’ educational level all affect parental involvement during the infant’s hospitalization. Within established psychological frameworks, perceived lack of control may influence caregiving behavior through several mechanisms. According to stress appraisal theory, parents who perceive the NICU environment as unpredictable and uncontrollable are more likely to experience heightened stress and emotional dysregulation.41 In parallel, reduced perceived control may undermine parental self-efficacy, lowering confidence in engaging in caregiving tasks.42 Over time, this diminished sense of agency may contribute to behavioral disengagement, whereby parents defer caregiving responsibilities to medical staff, further limiting active participation. Together, these processes provide a plausible mechanism linking perceived control to parental involvement in the NICU. These mechanisms are particularly relevant in the NICU, where medical complexity and role disruption may amplify the impact of perceived control on caregiving engagement. The degree of prematurity in infants may worsen parental stress related to a lack of control. Premature infants are more easily dysregulated, and their communication methods are unfamiliar to parents.43 This can further decrease maternal self-efficacy and raise stress levels, which are connected to parental involvement and overall maternal psychological distress. Consequently, this impacts infant–parent interactions.7 Intrusive or disengaged parenting behaviors can, in turn, further increase infant disengagement or distress, resulting in feedback loop for parents and infants. Together, this can lead to higher rates of insecure attachment and maladaptive parenting behaviors,44–46 and consequently long-lasting psychiatric (eg, ADHD, personality disorders) and health consequences.45 By identifying control-related stress as a behavioral inflection point, our study refines the pathway from NICU stress to long-term relational and regulatory outcomes, providing a concrete target for early intervention within high-acuity NICU contexts.
To our knowledge, this is among the first studies to demonstrate that NICU-specific perceived maternal control rather than global maternal stress, is a key and potentially modifiable predictor of parental involvement in the NICU.
Strengths and Limitations
Our study highlights several strengths that support a novel, real-time understanding of maternal stress related to their NICU experience and their level of involvement. Specifically, a perceived lack of control significantly impacts their involvement in bonding and routine care activities in the unit. To account for significant variation in hospitalization length and control for exposure time, we normalized parental involvement on a given day based on hospitalization length. Additionally, we reduced recall bias using objective observational logs on participants’ charts. Applying a multistep analytical approach improves transparency of the baseline relationships between variables, accounts for confounding effects, strengthens causal inference, and reliably identifies the most parsimonious best-fitting model.
The retrospective nature of this analysis imposes several limitations. Data were collected from existing records, limiting the establishment of causal relationships between maternal stress and caregiving behaviors to association inferences only. Documentation of parental involvement relied on medical chart review, which may have introduced variability in measurement. In addition, stress measures were completed by the mother, while the parental involvement in the medical chart was often documented undifferentiable (eg, parent). Although our models adjusted for important covariates, other unmeasured factors (eg, staffing patterns, parental leave, social support) may have influenced both maternal stress and parental involvement. The modest sample size and recruitment from a single level IV NICU limit the generalizability of our findings, as they may not reflect experiences in lower-acuity NICU settings. Although post hoc power estimates were high, this likely reflects the large observed effect size. While the final model included a limited number of predictors, the modest sample size and use of stepwise model selection may still contribute to inflation of effect estimates. Findings should therefore be interpreted with caution pending replication in larger samples.
While the PSS: NICU subscales demonstrated excellent internal consistency in our sample, very high reliability coefficients can sometimes indicate item redundancy. Infant medical comorbidities and treatment characteristics may influence maternal stress and perceptions of control in the NICU. While those were documented in the clinical record, they were not incorporated in the present analyses. Given the modest sample size, gestational age at birth was selected as a robust and widely used proxy for overall neonatal medical risk to maintain model parsimony and avoid overfitting. Gestational age does not fully reflect the clinical heterogeneity or treatment intensity characteristic of infants cared for in a level IV NICU. Future studies should also incorporate standardized medical severity indices or detailed comorbidity profiles to more precisely account for infant health status in modeling parental involvement. The retrospective study design precluded the ability to assess changes in caregiving involvement post-discharge, or longer-term parenting and infant outcomes. The impact of NICU specific stress and early caregiving activities on long-term parent and infant outcomes warrants additional study.
Clinical Implications and Future Directions
Identifying caregiver stress levels related to the lack of control over the NICU environment and infant care is essential for establishing dyadic NICU interventions. Screening caregivers in the NICU can enhance parent-infant involvement and emotional bonding, leading to long-term benefits for the infant’s attachment and neurodevelopmental progress. Implementing standardized screening for caregiver risk factors associated with decreased parental involvement is vital for improving parental self-efficacy and caregivers’ sensitivity. Early dyadic interventions, such as the Family Nurture Intervention and Kangaroo Care, are positive parent-infant relational outcomes (eg, increased parental attunement and reflective capacity) and infant neurodevelopmental benefits.39 Using a trauma-informed approach, parents can be supported by enhancing their sense of predictability, agency, and self-efficacy in the NICU. While parents cannot control many aspects of medical care, offering choices over small, immediate decisions that do not interfere with infant care can increase a realistic sense of control and competence. For example, parents could decide which intervention to prioritize when multiple procedures are scheduled, the order of feeding or diapering, when to engage in skin-to-skin or holding sessions, or whether to participate in comforting activities such as reading, singing, or gentle touch during procedures. Combining these choices with predictable schedules and clear communication about upcoming care tasks helps parents anticipate routines, feel empowered, and remain actively engaged in caregiving, even in a high-stress, medicalized environment. By doing so, parental involvement is enhanced, which may support parents in cultivating greater tolerance for uncertainty and practicing radical acceptance of their infants’ medical condition. Several strategies could be implemented within existing family-centered NICU care models. Introducing structured bedside protocols and nursing-led communication routines that identify and facilitate opportunities for parental participation in daily care, while increasing parental choice, may enhance tolerance of uncertainty by strengthening parents’ sense of control. Embedding these practices into routine workflows—such as multidisciplinary rounds or scheduled caregiving sessions—may promote consistent implementation across providers and improve feasibility within standard NICU practice.
In addition to individual psychological factors, parental involvement in the NICU is also shaped by different strategies could be implemented within that were not directly measured in the present study. Institutional policies, such as visitation guidelines, staffing models, and unit-level caregiving practices, may facilitate or constrain opportunities for parental engagement. Similarly, socio-economic conditions, including parental leave availability, work demands, transportation barriers, and financial stressors, may influence the extent to which parents are able to participate in caregiving activities. Social support systems, including partner involvement and extended family support, may further buffer or exacerbate these constraints. These external factors likely interact with perceived control and stress appraisals to shape parental involvement and represent important directions for future research. Parental involvement practices are influenced by cultural norms surrounding caregiving roles, family structure, and expectations for parental presence in medical settings. In addition, institutional policies, resource availability, and models of family-centered care vary across hospitals and health systems, which may shape opportunities for parental engagement. As this study was conducted within a single clinical setting, findings may not fully extend to NICUs with different organizational structures or socio-cultural contexts. Future multi-site and cross-cultural studies are needed to examine the robustness of these associations across diverse care environments.
In addition to include a larger and more diverse NICU population to replicate our findings, to future studies should incorporate longitudinal outcomes (eg, attachment, neurodevelopment, and readmission rates) would provide a more comprehensive understanding of how caregivers’ perceived lack of control in the NICU impacts the parent–infant relationship and child development. To gain a better understanding of these relationships, dual EEG and functional connectivity (fMRI) could offer deeper insights into parent–infant interactions.
Conclusion
This study demonstrates that parental involvement in the NICU, whether expressed as functional parenting or physical contact, is shaped by infant prematurity, maternal education, and, most critically, parents’ perceived lack of control. Consistent with prior research, greater gestational maturity and higher maternal education were associated with increased involvement. Early premature infants in less educated families are especially vulnerable, with higher maternal stress due to a lack of control in the NICU. These families face fewer opportunities for engagement and, therefore, are at greater risk of poorer long-term attachment and development. Heightened stress related to lack of control was strongly associated with reduced caregiving behaviors. The strength and robustness of our models underscore the clinical relevance of these findings.
By elucidating that situated stress appraisals (control over infant care) are more proximal determinants of caregiving behavior than global distress measures, our findings can directly inform NICU-based programs to include structured opportunities for caregiving and decision-making that strengthen control and competence. Despite several interventions developed to improve parent–infant bonding in the NICU (eg, Kangaroo Care, Family Nurture Intervention), these follow standardized behavioral protocols with limited attention to maternal readiness, stress, or emotional needs.47 These results highlight the importance of early, dyadic interventions that reduce maternal stress, enhance caregiver agency, and promote positive parent–infant bonding, ultimately aiming to improve long-term developmental and attachment outcomes.
Our findings should be interpreted in light of several limitations. The use of retrospective records precludes causal inference, and reliance on chart-documented parental involvement may have introduced measurement variability, particularly given the lack of differentiation between caregivers. Although models adjusted for key covariates, unmeasured factors (eg, staffing, parental leave, social support) may have influenced results. Finally, the modest sample size and single-site design limit generalizability beyond a level IV NICU context.
Data Sharing Statement
Participants provided informed consent that allows for the sharing of de-identified data. Accordingly, de-identified datasets generated during this study may be made available from the corresponding author upon reasonable request and in accordance with IRB approval.
Acknowledgments
We thank the clinical staff of the Neonatal Intensive Care Unit at Children’s National Hospital for their support and assistance with recruitment and data collection. We are grateful to the infants and families whose participation made this research possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
All phases of this study were supported by NIH grants, T32 HD098066/HD/NICHD NIH HHS/United States and R01 HD099393/HD/NICHD NIH HHS/United States.
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. da Fonseca EB, Damião R, Moreira DA. Preterm birth prevention. Best Pract Res Clin Obstet Gynaecol. 2020;69:40–15.
2. Griggs KM, Hrelic DA, Williams N, McEwen-Campbell M, Cypher R. Preterm labor and birth: a clinical review. MCN Am J Matern Child Nurs. 2020;45:328–337.
3. Bernabe-Zuñiga JE, Rodriguez-Lucenilla MI, Alias-Castillo AJ, et al. Early interventions with parental participation and their implications on the neurodevelopment of premature children: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2025;34:853–865.
4. Warnier H, Dauby J, De Halleux V, et al. [Prevention of prematurity’s complications]. Revue Medicale de Liege. 2024;79(5–6):436–441. French.
5. Saboktakin L. Developmental delay in preterm infants during the first twelve months after birth and its risk factors. J Educ Health Promot. 2024;13:48.
6. Caporali C, Pisoni C, Gasparini L, et al. A global perspective on parental stress in the neonatal intensive care unit: a meta-analytic study. J Perinatol. 2020;40:1739–1752.
7. Givrad S, Hartzell G, Scala M. Promoting infant mental health in the neonatal intensive care unit (NICU): a review of nurturing factors and interventions for NICU infant-parent relationships. Early Hum Dev. 2021;154:105281.
8. Shaw RJ, Givrad S, Poe C, et al. Neurodevelopmental, mental health, and parenting issues in preterm infants. Children. 2023;10:1565.
9. Madigan S, Hawkins E, Plamondon A, Moran G, Benoit D. Maternal representations and infant attachment: an examination of the prototype hypothesis. Infant Ment Health J. 2015;36:459–468.
10. Tooten A, Hall RAS, Hoffenkamp HN, et al. Maternal and paternal infant representations: a comparison between parents of term and preterm infants. Infant Behav Dev. 2014;37:366–379.
11. Forcada-Guex M, Borghini A, Pierrehumbert B, Ansermet F, Muller-Nix C. Prematurity, maternal posttraumatic stress and consequences on the mother-infant relationship. Early Hum Dev. 2011;87:21–26.
12. Hartzell G, Shaw RJ, Givrad S. Preterm infant mental health in the neonatal intensive care unit: a review of research on NICU parent-infant interactions and maternal sensitivity. Infant Ment Health J. 2023;44:837–856.
13. Allen EC, Manuel JC, Legault C, Naughton MJ, Pivor C, O’shea TM. Perception of child vulnerability among mothers of former premature infants. Pediatrics. 2004;113(2):267–273.
14. Hoge MK, Heyne E, Nicholson TDF, et al. Vulnerable child syndrome in the neonatal intensive care unit: a review and a new preventative intervention with feasibility and parental satisfaction data. Early Hum Dev. 2021;154:105283.
15. Özçalık HB, Akin B. The relationship between participation in caregiving, maternal stress and maternal role among mothers whose babies are hospitalized in the neonatal intensive care unit. J Neonatal Nurs. 2025;31:101721.
16. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–396.
17. Lee EH. Review of the psychometric evidence of the perceived stress scale. Asian Nurs Res. 2012;6:121–127.
18. Speilberger CD, Gorsuch R, Lushene R, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory (Form Y1 – Y2). Palo Alto, CA: Consulting Psychologists Press; 1983.
19. Spielberger CD. State-Trait Anxiety Inventory Bibliography.
20. Rojas-Carrasco KE. [Levels of state-trait anxiety between mothers and fathers who have children in an intensive care unit]. Rev Méd Inst Mex Seguro Soc. 2013;51(6):606–609. Spanish.
21. Kraft KE, Jaschke AC, Ravensbergen A-G, et al. Maternal anxiety, infant stress, and the role of live-performed music therapy during NICU Stay in The Netherlands. Int J Environ Res Public Health. 2021;18:7077.
22. Dennis CL, Coghlan M, Vigod S. Can we identify mothers at-risk for postpartum anxiety in the immediate postpartum period using the state-trait anxiety inventory? J Affect Disord. 2013;150:1217–1220.
23. Miles MS, Funk SG, Carlson J. Parental stressor scale: neonatal intensive care unit. Nursing Research. 1993;42(3):148–152.
24. Obeidat HM, Bond EA, Callister LC. The parental experience of having an infant in the newborn intensive care unit. J Perinat Educ. 2009;18:23–29.
25. Klein CC, McDonald NM. Parenting stress following a neonatal intensive care unit hospitalization: a longitudinal study of mothers and fathers. Int J Environ Res Public Health. 2024;21:970.
26. Pavlyshun H, Sarapuk I, Saturska U. Maternal stress experience in the neonatal intensive care unit after preterm delivery. Am J Perinatol. 2024;41:1155–1162.
27. Hane AA, Henderson HA, Reeb-Sutherland BC, Fox NA. Ordinary variations in human maternal caregiving in infancy and biobehavioral development in early childhood: a follow-up study. Dev Psychobiol. 2010;52:558–567.
28. Hane AA, Fox NA. Early caregiving and human biobehavioral development: a comparative physiology approach. Curr Opin Behav Sci. 2016;7:82.
29. Ionio C, Colombo C, Brazzoduro V, et al. Mothers and Fathers in NICU: the impact of preterm birth on parental distress. Eur J Psychol. 2016;12:604–621.
30. Welch MG, Myers MM. Advances in family-based interventions in the neonatal ICU. Curr Opin Pediatr. 2016;28:163–169.
31. Welch MG, Hofer MA, Brunelli SA, et al. Family nurture intervention (FNI): methods and treatment protocol of a randomized controlled trial in the NICU. BMC Pediatr. 2012;12:14.
32. Yu NKK, Shum KK, Lam YY, et al. Sensitivity training for mothers with premature infants: a randomized controlled trial. J Pediatr Psychol. 2022;47:1167–1184.
33. Rodrigues SM, Shin S, Pinto MD, et al. Parenting self-efficacy moderates the association between unmet parenting expectations and NICU-Related PTSD symptoms reported by mothers 1–5 years post-infant NICU Hospitalization. Issues Ment Health Nurs. 2025;46:58–69.
34. Lewis TP, Andrews KG, Shenberger E, et al. Caregiving can be costly: a qualitative study of barriers and facilitators to conducting kangaroo mother care in a US tertiary hospital neonatal intensive care unit. BMC Pregnancy Childbirth. 2019;19:227.
35. Newborn health. Available from: https://www.who.int/health-topics/newborn-health/#tab=tab_1.
36. Ekwueme MC, Girma AZ, Gobezayehu AG, Young MF, Cranmer JN. Predictors of effective kangaroo mother care, exclusive breastfeeding, and skin-to-skin contact among low birthweight newborns in Amhara, Ethiopia. J Glob Health. 2024;14:04114.
37. Reiter A, De Meulemeester J, Kenya-Mugisha N, et al. Parental participation in the care of hospitalized neonates in low- and middle-income countries: a systematic review and meta-analysis. Front Pediatr. 2022;10:987228.
38. Ferreira A, Ferretti E, Curtis K, et al. Parents’ views to strengthen partnerships in newborn intensive care. Front Pediatr. 2021;9:721835.
39. Darilek U, Finley E, McGrath J. A narrative review of NICU implementation of evidence-based early relational health interventions. Adv Neonatal Care. 2024;24:253–267.
40. Heo YJ, Oh WO. The effectiveness of a parent participation improvement program for parents on partnership, attachment infant growth in a neonatal intensive care unit: a randomized controlled trial. Int J Nurs Stud. 2019;95:19–27.
41. Folkman S, Lazarus RS. If it changes it must be a process: study of emotion and coping during three stages of a college examination. J Pers Soc Psychol. 1985;48:150–170.
42. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Adv Behav Res Ther. 1978;1:139–161.
43. Gerstein ED, Poehlmann-Tynan J, Clark R. Mother-child interactions in the NICU: relevance and implications for later parenting. J Pediatr Psychol. 2015;40:33–44.
44. Emami M, Moghadasin M, Mastour H, Tayebi A. Early maladaptive schema, attachment style, and parenting style in a clinical population with personality disorder and normal individuals: a discriminant analysis model. BMC Psychol. 2024;12:78.
45. Gajula R, Yeshala V, Gogikar N, Kotha R. NICU graduates and psychosocial problems in childhood: a systematic review. Cureus. 2024;16.
46. Mehler K, Heine E, Kribs A, et al. High rate of insecure attachment patterns in preterm infants at early school age. Acta Paediatr. 2023;112:977–983.
47. Jaekel J, Dathe A-K, Brasseler M, et al. Infant regulatory problems and the quality of dyadic emotional connection—a proof-of-concept study in a multilingual sample. Front Child Adolesc Psychiatry. 2023;2:1304235.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.