Back to Journals » Risk Management and Healthcare Policy » Volume 13
Perceived Competition and Process of Care in Rural China
Authors Lin X ![]() , Jian W, Yip W, Pan J
, Jian W, Yip W, Pan J ![]()
Received 18 April 2020
Accepted for publication 21 July 2020
Published 14 August 2020 Volume 2020:13 Pages 1161—1173
DOI https://doi.org/10.2147/RMHP.S258812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Xiaojun Lin,1,2 Weiyan Jian,3 Winnie Yip,4 Jay Pan1,2
1West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, People’s Republic of China; 2West China Research Center for Rural Health Development, Sichuan University, Chengdu, People’s Republic of China; 3Department of Health Policy and Management, School of Public Health, Peking University Health Science Center, Beijing, People’s Republic of China; 4Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston, MA, USA
Correspondence: Jay Pan
West China School of Public Health and West China Fourth Hospital, Sichuan University, No. 17, Section 3, Ren Min Nan Road, Chengdu 610041, Sichuan, People’s Republic of China
Tel +86 28 8550 1096
Fax +86 28 8550 1528
Email [email protected]
Purpose: Although there is much debate about the effect of hospital competition on healthcare quality, its impact on the process of care remains unclear. This study aimed to determine whether hospital competition improves the process of care in rural China.
Patients and Methods: The county hospital questionnaire survey data and the randomly sampled medical records of bacterial pneumonia patients in 2015 in rural area of Guizhou, China, were used in this study. The processes of care for bacterial pneumonia were measured by the following three measures: 1) oxygenation assessment, 2) antibiotic treatment, and 3) first antibiotic treatment within 6 hours after admission. Hospital competition was measured by asking hospital directors to rate the competition pressure they perceive from other hospitals. Multivariate logistic regression models were employed to determine the relationship between perceived competition and the processes of care for patients with bacterial pneumonia.
Results: A total of 2167 bacterial pneumonia patients from 24 county hospitals in 2015 were included in our study. Our results suggested that the likelihood of receiving antibiotic treatment and first antibiotic treatment within 6 hours after admission was significantly higher in the hospitals perceiving higher competition pressure. However, no significant relationship was found between perceived competition and oxygenation assessment for patients with bacterial pneumonia.
Conclusion: This study revealed the role of perceived competition in improving the process of care under the fee-for-service payment system and provided empirical evidence to support the pro-competition policies in China’s new round of national healthcare reform.
Keywords: perceived competition, market concentration, process of care, pneumonia, quality, healthcare reform
Introduction
Across the globe, many countries have been introducing competition in the healthcare market to improve healthcare delivery.1,5 However, for decades, there has been ongoing debate about whether the higher market competition is associated with better quality in healthcare, theoretically and practically.2,6 The proponents of competition believe that competition among healthcare providers might potentially benefit the holistic health system as it stimulates innovation, which in turn improves quality.7,8 On the other hand, the opponents argue that the healthcare market differs from the general product markets in several aspects, such as information asymmetry and uncertainty,2,9 which may result in reduced quality.10 A neutral viewpoint is that competition could be either helpful or harmful, depending on the context of the health system and the objectives considered.11
To date, the empirical evidence pertaining to the relationship between competition and quality remains ambiguous: while some studies mainly from the United States and the United Kingdom suggested that more competitive markets have better inpatient healthcare quality,1,12,13 others reported contradictory findings.14,15 Mutter et al16 demonstrated that the measurement of quality may affect the estimation of the relationship between competition and quality.
In China, pro-competition policies have been introduced and implemented in healthcare reform.17 To promote the competition among hospitals, the Chinese government implemented the regulatory reform that enhances hospitals’ autonomy through separating government regulatory and operational control of public hospitals.18 In terms of the competition between public and private hospitals, the Chinese government relaxed the entry and business barriers for private hospitals.19 Over the past decades, China has made substantial progress in improving the quality in health services delivery, but the quality gap remains.20,21 A recent nationally representative study conducted by Jian et al22 reported that the large-scaled tertiary hospitals in China had poor and varied performances in most process-based quality measures for common medical conditions such as acute myocardial infarction (AMI), cerebral ischemic stroke, chronic obstructive pulmonary disease, and bacterial pneumonia, implying that there is still significant room for quality improvement in China. Zhou et al23 also found similar results in patients with AMI admitted to 14 tertiary hospitals in Beijing. Given the daunting challenge of improving quality of care, understanding the potential role of hospital competition on improving the quality of care has become particularly important and would further provide evidence-based implications for China’s healthcare reform.
Compared with abundant theoretical and empirical research from the developed countries, the evidence from China focusing on the impact of competition on the quality of care remains scarce. Pan et al19 investigated whether hospital competition improves healthcare quality and cost using both provincial and individual level data, and found that the hospitals in a more competitive market provide better quality in outpatient services, such as lower observation room mortality and shorter outpatient waiting time. Lin et al24 reported that higher competition was associated with higher mortality for pneumonia inpatients, yet such evidence for patients with AMI was not found. Using the data of stroke inpatients from Sichuan province, Lu and Pan25 also did not find a significant association between competition and inpatient healthcare outcomes. Based on all these previous studies, it is not difficult to conclude that, despite the competition-driven policies in the Chinese healthcare market, whether hospital competition would play a positive role in improving the quality of care remains unclear.
There are two notable research gaps embedded in the existing literature. First, although the process of care is an important dimension of quality measurement,26 the association of competition with the process of care has not received adequate attention. To date, there are a few empirical studies exploring the relationship between competition and process quality, but the consensus has not been reached. Specifically, using the outpatient claims data from 1997 to 2005 in Taiwan, Bennett et al27 found a robust and positive correlation between hospital competition and antibiotic use. Bijlsma et al28 investigated all Dutch general and academic hospitals during 2014–2018 and found that hospital competition had significant effects on increasing the frequency of tests on chronic patients as well as the share of the diagnoses of breast cancer completed within 5 days. Croes et al29 found that higher competition was significantly associated with a higher process-based composite quality score for cataracts and bladder tumors in Dutch. However, Wani et al30 analyzed the longitudinal data from all acute care hospitals in California from 2007 to 2013 and developed a composite measure for assessing the process of care for common and serious medical conditions including AMI, heart failure, pneumonia, and surgical care improvement or the Surgical Care Improvement Project. For example, the components of the process of care for AMI included the percentage of patients given aspirin at discharge, the percentage of patients given fibrinolytic medication within 30 minutes of arrival, and the percentage of patients given percutaneous coronary intervention within 90 minutes of arrival. Through employing the mixed-effects model, they found that greater hospital competition reduced the process of care. Second, previous studies mainly focus on the Western countries, especially the United States and the United Kingdom, with a limited knowledge gained elsewhere. It is noteworthy that there are many structural differences in the healthcare delivery system and policy environment across countries. For example, the public hospitals dominate the healthcare market under regulated prices in China, while the private hospitals serve as the main providers of healthcare services in the United States.19 The hierarchical medical systems have been well-established in the developed countries, while it remains underdeveloped in China.31 Almost the entire population in China were covered by the basic social health insurance programs,32 while about 10.3% of the population under age 65 in the United States remained uninsured in 2017.33 These structural differences inherent in healthcare systems among different countries might potentially complicate the association between hospital competition and quality of care.34
Our study, using the data from county hospitals in rural China, aimed to advance the existing literature on hospital competition and quality of care in two important ways. First, we focused on process-based quality measures for bacterial pneumonia which were not much studied in previous literature. Bacterial pneumonia is known as a common medical condition,22,35 with which patients usually have discretion in choosing hospitals.14 More importantly, payment systems would potentially affect the providers’ incentives to compete in the healthcare market.36 Therefore, our empirical evidence derived from rural China with the fee-for-service payment system was expected to provide implications for other countries with similar settings in healthcare delivery. Second, the Herfindahl-Hirschman Index (HHI) has been commonly used in previous studies to measure hospital competition.1,14,25,37 However, as further described in the following section, the HHI for competition measurement may ignore the potential competitors in the market area.38,39 Based on previous studies,40,42 we developed a county hospital questionnaire and surveyed the hospital directors to measure the degree of perceived competition for each hospital. This measure reflects the competition pressure perceived by hospital directors and could address the drawback of objective competition indicators (ie, HHI), which might explain the hospital behaviors to improve their competitive position in the healthcare market.
Materials and Methods
Data
Guizhou is one of the provinces in southwestern China containing 88 counties. In 2017, there were 19.3 million rural residents and 16.5 million urban residents, with an average gross domestic product (GDP) per capita of 37,956 yuan (about 5622 US dollars).43
The data in this study were retrieved from the Analysis of Provider Payment Reforms on Advancing China’s Health project.44 This project was designed to evaluate the impact of the payment reform that switches the New Rural Cooperative Medical Scheme (NCMS) from paying county hospitals using a fee-for-service scheme (post-payment) to a global budget scheme (prepayment) in rural Guizhou. The first wave of payment reform in Guizhou was implemented in 2016, followed by wave 2 in 2017. A total of 56 counties were initially involved and assigned to treatment and control groups using a matched-pair cluster randomization strategy. Among 28 treatment counties, there were 16 counties that fully accomplished the two waves of payment reform. For the rest of the treatment counties that did not accomplish the payment reform, the whole pairs (including both treatment and control) were excluded from the evaluation. Finally, a total of 32 eligible counties were included for evaluation.
In this study, we focused on the year before the launch of the payment reform in rural Guizhou, because all those county hospitals were under the fee-for-services payment system in 2015, which would be ideal for examining the association between competition and healthcare quality in a market with a single payment system. The county hospital questionnaire was used to collect detailed hospital information, including hospital’s general characteristics (ie, hospital type, hospital level, ownership, profit status), staffing level (ie, the number of doctors, the number of registered nurses), financial statement (ie, total revenue and expense), internal governance (ie, director-in-charge management system, director appointment, director performance assessment), leadership (the intensity of perceived competition, source of competition), and provider payment method (ie, payment method for outpatient and inpatient services). For each county hospital, we conducted chart reviews for patients admitted with bacterial pneumonia using the following strategy. First, the diagnoses in the claims data from county hospitals were recorded in the form of unstandardized disease names (in Chinese) instead of using the International Classification of Diseases codes, and therefore required a thorough review and re-coding process conducted by Chinese clinicians familiar with local clinical practices. Patients with various types of bacterial pneumonia were included in this study, such as pneumonia due to Streptococcus pneumoniae and pneumonia due to Klebsiella pneumoniae. The medical record identification numbers of all patients with bacterial pneumonia for each given hospital were provided by hospitals. Then, 120 cases of bacterial pneumonia were randomly selected. If a hospital had fewer than 120 admissions, all cases were selected. Finally, clinical experts with at least 10 years of clinical experience reviewed all medical records and extracted relevant quality measures for each case from each hospital. Given the limited study budget, we focused on 26 county hospitals that were involved in the first wave of payment reform. The county hospital questionnaire survey data and hospital quality data were linked using the unique hospital identification number.
The following criteria were used to include and exclude observations. First, we included a total of 3072 randomly selected bacterial pneumonia patients who were admitted to the 26 county hospitals in 2015. Second, after the chart reviews, we excluded patients with missing medical records or incorrect principal diagnosis (n=793). Third, patients admitted to two hospitals were excluded (n=112) because these two hospitals had missing data in competition measurement. Finally, a total of 2167 observations from 24 hospitals were included in our final dataset for analysis (Supplementary Table 1).
Process of Care Measurement
We focused on process-based quality measures in this study for the following reasons. First, even though process quality measures are an essential management tool for monitoring hospital performance, the extant literature has paid little attention to the association of competition with process quality. Second, the process of care could recognize the trade-off faced by hospitals in allocating constrained resources.30 Hospitals in a competitive market might allocate more resources and devote more efforts to some aspects of process quality that attract more patients, while other dimensions of process of care would receive less resources and efforts. Third, compared with outcome measures (ie, mortality and readmission), process quality measures are less noisy as they depend less on the exogenous circumstances such as patient demographics and severity of illness.28,30 Thus, an extensive risk adjustment model would be unnecessary for the process of care.
The following process quality measures for bacterial pneumonia were collected in our study: (1) oxygenation assessment, (2) effective dose of sputum culture prior to initial antibiotic treatment, (3) antibiotic treatment, (4) first antibiotic treatment within 6 hours after admission, (5) influenza vaccination, (6) pneumococcal vaccination, and (7) adult suggestion/advice on quitting smoking. These process quality measures for bacterial pneumonia have been commonly used in previous studies22,45,46 and endorsed by the Hospital Quality Alliance framework in the United States35 and the Advancing Quality framework in the United Kingdom.47 In addition, all these measures were consistent with the Tertiary General Hospital Accreditation Criteria,48 the Secondary General Hospital Accreditation Criteria,49 and the clinical guidelines issued by the Chinese Medical Association.50 For example, the clinical guideline for community-acquired pneumonia in China recommended that the first antibiotic treatment should be initiated as soon as possible after the diagnosis,50 and the “Tertiary General Hospital Accreditation Criteria” and the “Secondary General Hospital Accreditation Criteria” specified that the first antibiotic treatment for community-acquired pneumonia should be initiated within 4 hours after the distinct diagnosis.48,49 Considering the time slot between admission and diagnosis, it would be appropriate to use the first antibiotic treatment within 6 hours after admission in this study.
We excluded several process quality measures in our following analyses. Both the “Tertiary General Hospital Accreditation Criteria” and the “Secondary General Hospital Accreditation Criteria” in China have emphasized the “Etiological examination” as an indispensable diagnostic test for serious cases. However, such requirement failed to specify whether the blood or sputum culture should be adopted for checking pathogens.48,49 Therefore in this study, we did not include the sputum culture in our analyses. In addition, since the influenza and pneumococcal vaccines were not recommended as routine treatment for pneumonia patients in China,50,51 the average rate of influenza vaccination and pneumococcal vaccination in our sample were found to be extremely low (0.42% and 0.05%, respectively). Thus, both influenza vaccination and pneumococcal vaccination were excluded from our analyses. Moreover, smoking cessation advice was also excluded from our analyses as more than 90% of observations reported missing data in this aspect. After the abovementioned exclusions, three process quality measures for bacterial pneumonia remained: 1) oxygenation assessment, 2) antibiotic treatment, and 3) first antibiotic treatment within 6 hours after admission. The definitions of these process quality measures are presented in Supplementary Table 2.
The appropriate treatment process would lead to better health outcomes. According to the previous relevant studies,22,45 China’s “Tertiary General Hospital Accreditation Criteria” and the “Secondary General Hospital Accreditation Criteria”,48,49 as well as the quality assessment frameworks in the United States and the United Kingdom,35,47 the hospitals providing antibiotic treatment and first antibiotic treatment within 6 hours after admission for patients diagnosed with bacterial pneumonia would have better quality performance than others.
Competition Measurement
Most studies adopted HHI to measure hospital competition in the healthcare market.1,14,25,37 Defining market area is the first step to calculate HHI. To define market area, various approaches have been proposed and broadly employed in the literature, including geopolitical boundaries (ie, county, city, metropolitan area), fixed radius (ie, 15 miles), and variable radius (ie, 75% of the hospital’s discharges). However, the main drawback embedded in the existing approaches is the incapacity of capturing the potential competitors well.39 Both geopolitical boundaries and fixed radius approaches share the same drawback of assuming that the urban and rural hospitals have the same market area. The urban hospitals may compete with a few close hospitals in a small market area, while rural hospitals may compete with hospitals beyond the geopolitical boundaries or the fixed radius.52 In terms of the variable radius approach, a circular market area for each hospital is defined based on patients’ residence and actual hospital choice, but it would ignore the possible substitution faced by patients. For example, assuming two identical hospitals in a defined market area, the patients always choose the closest hospital, so the two hospital would not compete with each other. However, when the quality of a hospital decreased or costs increased, patients would choose the other hospital, indicating that these two hospitals are competitors.38 Thus, the potential competitors might be different from the competitors identified objectively by various definitions of market area.53 This is particularly true in China’s healthcare market. First, the growing private hospitals tend to pose greater competition pressures to public hospitals, compared with their relatively smaller market shares.19 Second, patients are free to seek care among hospitals, thus the competitors for a hospital are not limited to a specific geopolitical boundary or fixed radius. Third, the development of medical alliances among healthcare providers are encouraged by the government.54 The hospitals in the same medical alliance cooperate with each other rather than compete.
Accounting for the potential limitations of objective competition measures, some studies alternatively employed perceived competition and suggested that competitive behaviors occur when the managers of organizations perceive a threat from competitors, regardless of the objective level of competition.40,42 Following previous studies,40,42 we measured the degree of perceived competition through a questionnaire survey. Hospital directors were asked to rate the competition pressure they perceived from other hospitals in their local market, on a 3-point scale (1=intense, 2=some, 3=no). Among 24 county hospitals in this study, 14 (58.3%) hospitals perceived intense competition pressure, nine (37.5%) reported some competition pressure, while only one hospital (4.2%) responded that they faced no competition. For easy interpretation, we combined “some competition pressure” and “no competition pressure” into the low competition group, as a reference group for the high competition group (“intense competition pressure”). For the hospitals perceiving some or intense competition, we further asked where the competition pressure mainly came from: out-of-county hospitals, within-county hospitals, or other. Eight (34.8%) and 14 (60.9%) hospitals perceived competition from within-county and out-of-county hospitals, respectively, while one hospital responded its competition pressure deriving from false advertisement.
Control Variables
A set of patient- and hospital-level covariates were controlled in our analyses. Due to data limitations, we were only able to include age as a patient-level covariate. Considering that the process of care assesses the extent to which providers adhere to the guidelines and does not require extensive risk adjustment modeling,30,55 we assumed that other patient level covariates such as gender and severity of illness would not affect the process of care.
At the hospital level, in addition to the perceived competition, we included the following covariates: whether a traditional Chinese medicine hospital, whethera tertiary hospital, whether a first-class hospital, the number of hospital beds, the number of doctors and nurses per 100 beds. All hospitals in China are classified into three categories: primary (level 1), secondary (level 2), and tertiary (level 3), and there are three classes for each level: first-class, second-class, and third-class. The traditional Chinese medicine hospitals mainly provide internal medicine services, while the general hospitals provide comprehensive services, including internal medicine and surgery services. All sample hospitals in this study were public and non-profit hospitals. The definitions of all control variables are presented in Supplementary Table 2.
Statistical Analysis
In descriptive analysis, t-test or analysis of variance was used to compare continuous variables, while Chi-square test or Fisher exact test for categorical variables.
In our primary analysis, we used multivariable logistic regressions to analyze the association between perceived competition and three process quality measures for bacterial pneumonia. The model is set as follows:

where  is our main dependent variable of interest, which indicates the process quality of patient
is our main dependent variable of interest, which indicates the process quality of patient  admitted to hospital
admitted to hospital  . For example,
. For example,  equals one for bacterial pneumonia when patient
equals one for bacterial pneumonia when patient  receives first antibiotic treatment within 6 hours after the admission to hospital
receives first antibiotic treatment within 6 hours after the admission to hospital  and zero otherwise.
and zero otherwise.  denotes the competition intensity that the director of hospital
denotes the competition intensity that the director of hospital  perceives.
perceives.  and
and  are the patient- and hospital-level covariates, respectively.
are the patient- and hospital-level covariates, respectively.  is the error term. Clustered robust standard error at hospital level is used to adjust for intra-group correlation when multiple patients were included for the same hospital. Model performance is measured by the c-statistic, which specifies how well a model can differentiate between patients with different outcomes. A value above 0.7 indicates an acceptable discrimination, while above 0.8 an excellent discrimination.56
is the error term. Clustered robust standard error at hospital level is used to adjust for intra-group correlation when multiple patients were included for the same hospital. Model performance is measured by the c-statistic, which specifies how well a model can differentiate between patients with different outcomes. A value above 0.7 indicates an acceptable discrimination, while above 0.8 an excellent discrimination.56
In our secondary analysis, we excluded the patients admitted to the hospitals with “no competition pressure” (n=93) and “inappropriate market competition” (n=29). The competition source was categorized into within-county and out-of-county groups, with the within-county group as the reference. A subsample of 2045 patients in 22 hospitals were included to explore the interaction relationship between perceived competition and competition source.
All data managements were processed in RStudio (Version 1.3.459). The statistical analyses were performed in Stata (Version 14.0 SE, Stata Crop, Chicago, IL, USA). P<0.05 is used to determine statistical significance.
Results
Descriptive Statistics
Table 1 shows the descriptive statistics of patient and hospital characteristics stratified by perceived competition. A total of 2167 bacterial pneumonia patients from 24 hospitals in rural Guizhou in 2015 were identified, with an average age of 20 years old. Compared with the patients admitted to the hospitals perceiving high competition, the patients in the low competition group were younger (Table 1). In total, 1176 patients (54.3%) were treated in the hospitals perceiving high competition, and 1333 (61.5%) in the general hospitals. Most patients (95.2%) received treatments in the secondary hospitals, and 1772 (81.8%) chose the first-class hospitals. There were no significant differences between high and low competition groups in hospital beds, nurses, and doctors.
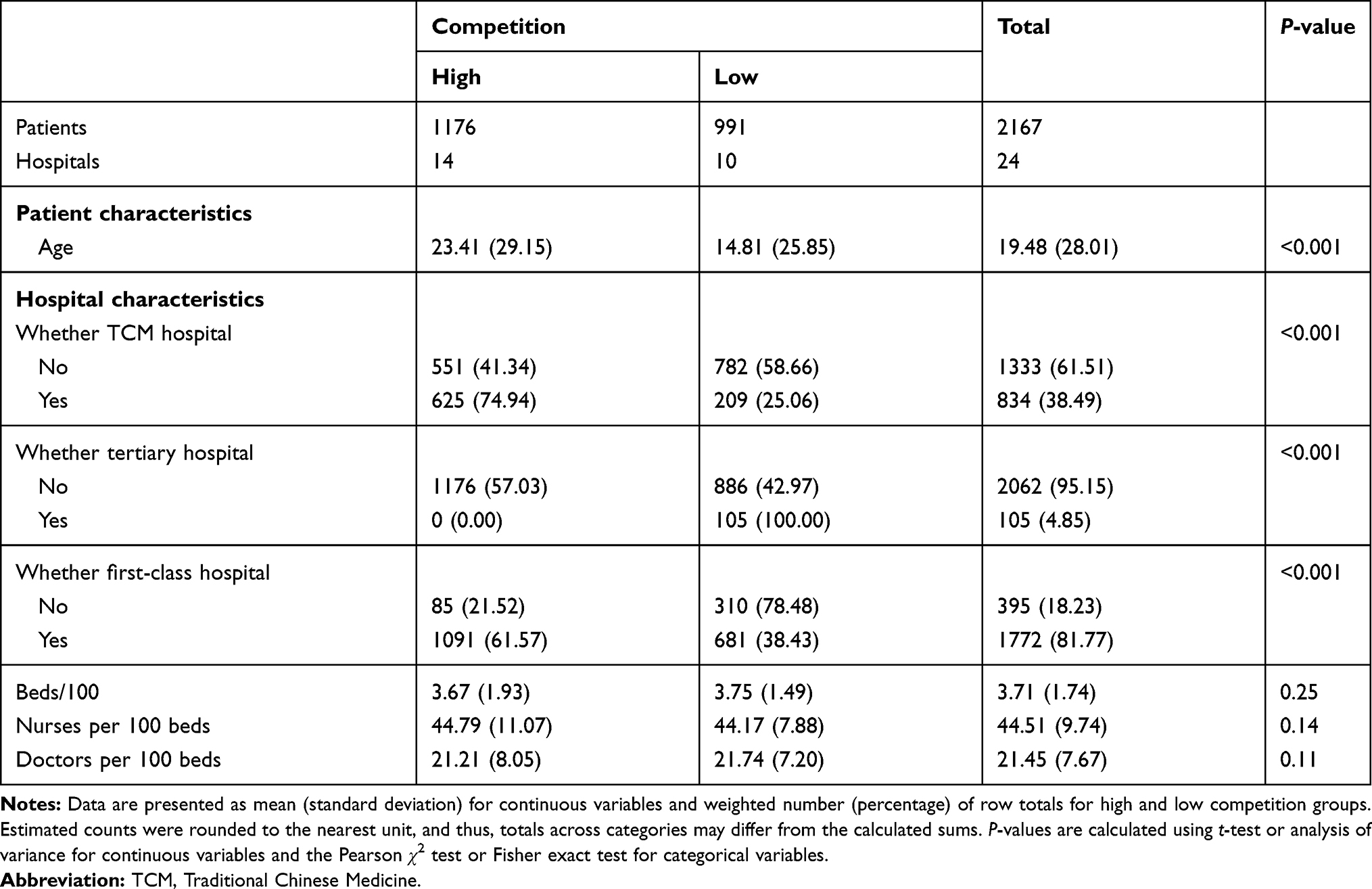 |
Table 1 Patient and Hospital Characteristics |
Table 2 presents the performance of process of care for bacterial pneumonia patients, as well as the comparisons between high and low competition groups. Overall, 49 patients (2.3%) had a documented oxygenation assessment, 2070 patients (95.5%) received antibiotic treatment, and 1975 patients (91.1%) received first antibiotic treatment within 6 hours after admission. Compared with low competition group, the high competition group had significantly better performance in antibiotic treatment (96.9% vs 94.0%, P<0.001) and first antibiotic treatment within 6 hours (94.1% vs 87.7%, P<0.001).
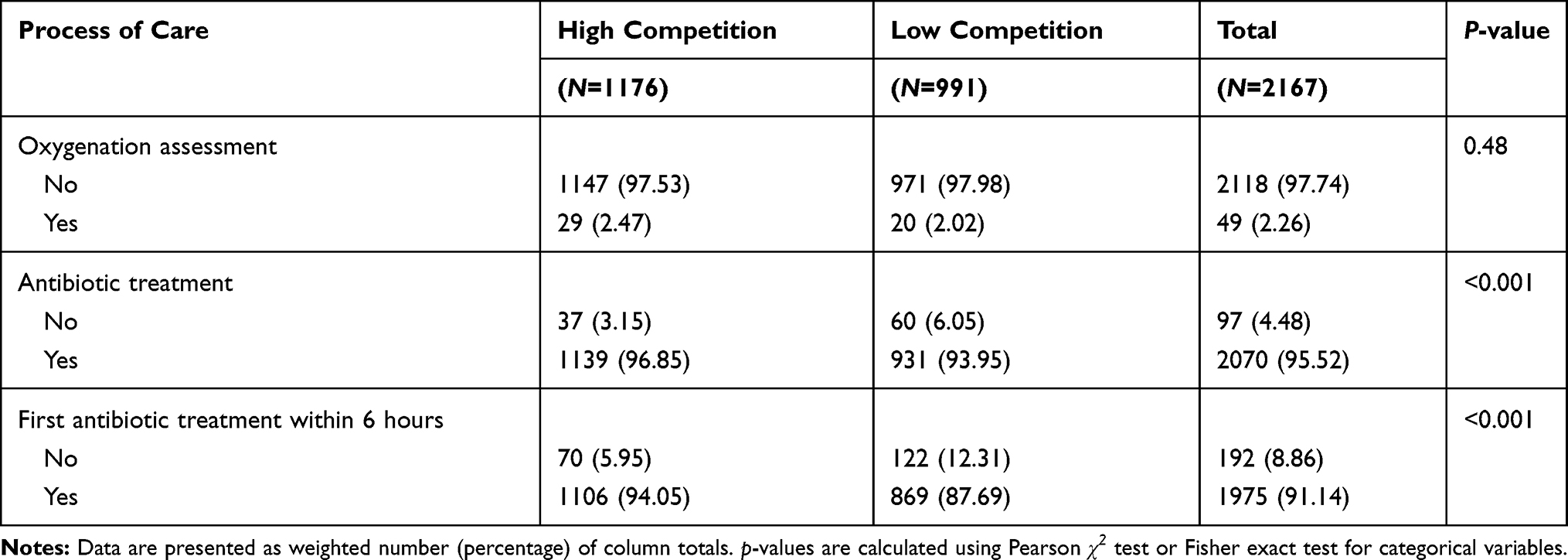 |
Table 2 Performance of Individual Process of Care for Patients with Bacterial Pneumonia |
Regression results
Table 3 reports the association of perceived competition with process of care for bacterial pneumonia after adjusting for the patient- and hospital-level characteristics. The c-statistics are above 0.7 for three regression models, indicating that the models demonstrated excellent performance in differentiating patients who receive appropriate process of care from patients who do not receive. As shown in column 1 of Table 3, there is no significant relationship between perceived competition and oxygenation assessment, with a coefficient of −0.645 (P>0.1). The association of perceived competition with antibiotic treatment is presented in column 2 of Table 3, which indicates hospitals perceiving higher competition are more likely to provide antibiotic treatment for patients with bacterial pneumonia (P<0.05). Our result in column 3 of Table 3 suggests that the likelihood of receiving first antibiotic treatment within 6 hours after admission is significantly higher in the hospitals perceiving higher competition pressure (P<0.001). Patients admitted to hospitals with a higher number of nurses per 100 beds have decreasing odds of receiving antibiotic treatment and first antibiotic treatment within 6 hours (P<0.001).
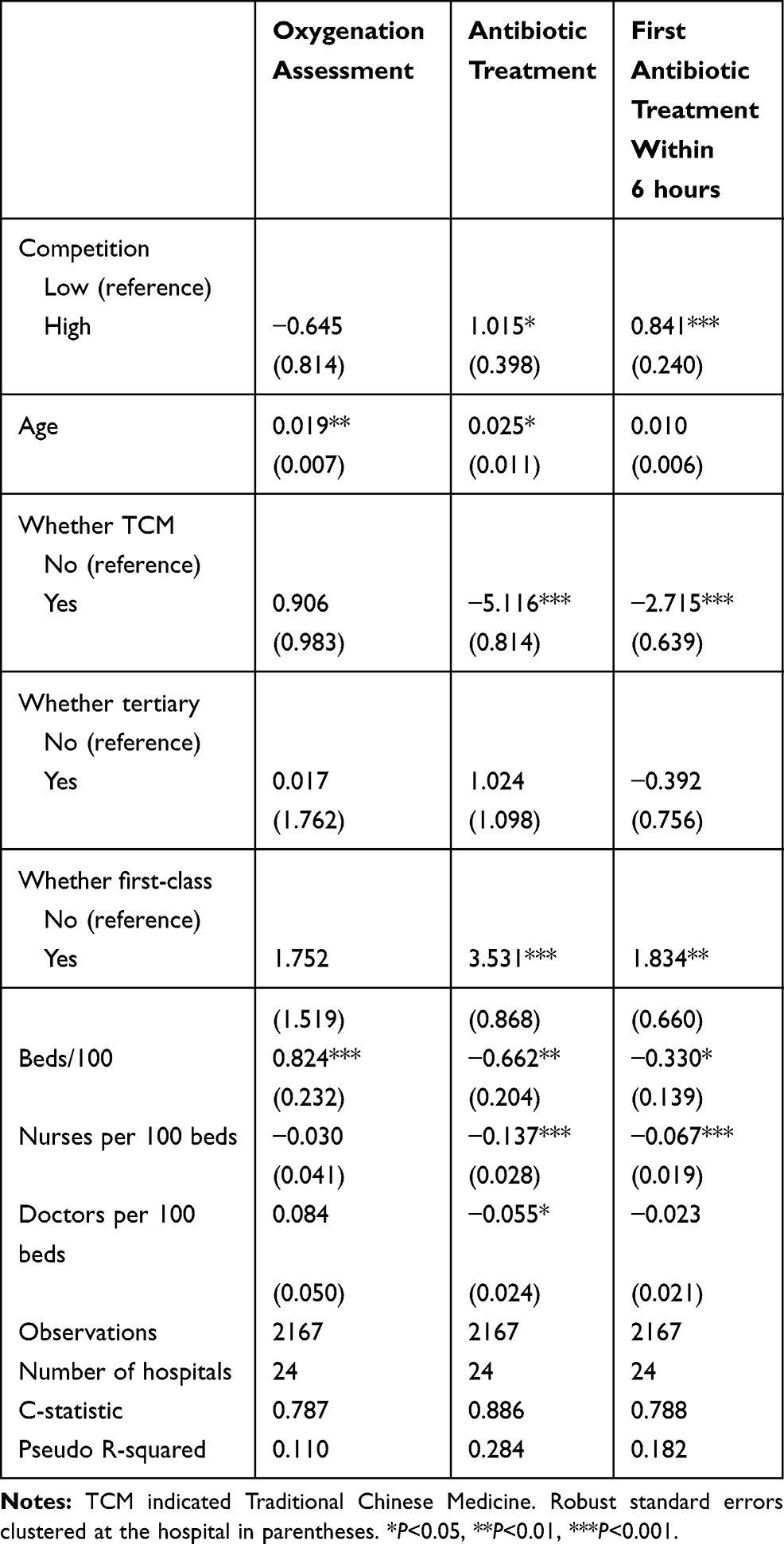 |
Table 3 The Relationship Between Perceived Competition and Process of Care |
Table 4 shows the results of an interaction model adding the interaction term of perceived competition with the source of competition pressure. However, the estimates of all interaction terms are insignificant (P>0.1), which suggests that there is no significant interaction relationship between perceived competition and the source of competition pressure.
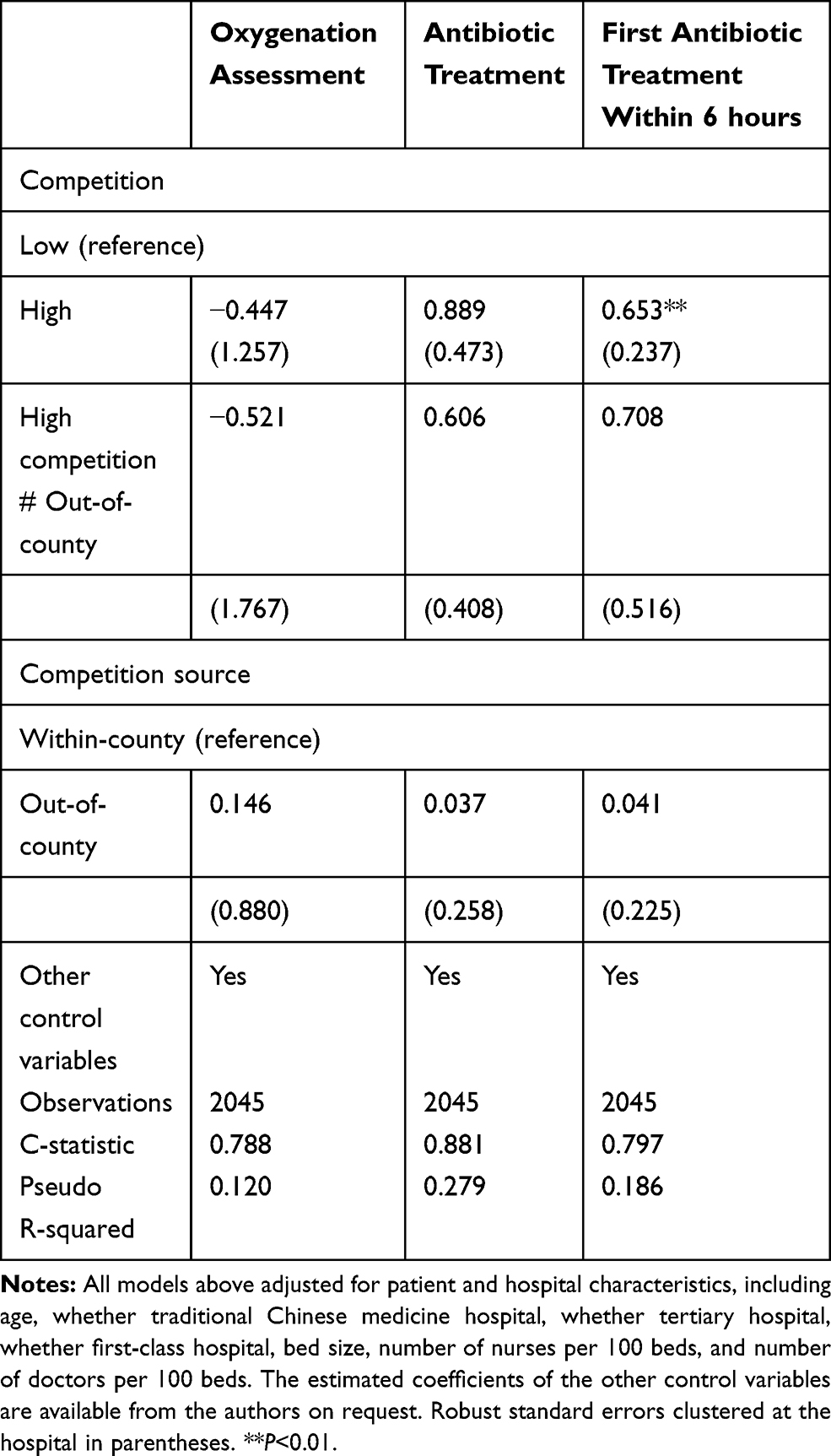 |
Table 4 The Interaction Relationship Between Perceived Competition and Competition Source |
Robustness Checks
For robustness check, we used the following three strategies. First, we combine the hospitals perceiving “some competition pressure” and “no competition pressure” in our primary analysis, which might result in biased estimation of perceived competition effects. Therefore, we repeat our primary analysis after excluding patients admitted to the hospitals perceiving “no competition pressure”. Second, due to the difference in staff qualification between secondary and tertiary hospitals, the treatment guideline adherence of pneumonia in tertiary hospitals might be better than that in secondary hospitals. Thus, we exclude the patients admitted to tertiary hospitals to test the robustness of our findings. Third, we use the cluster standard errors at the county level to account for the dependency of patients in the same county. Table 5 reports the results of robustness checks. For the sake of clarity, we only show the estimated competition coefficients. The results are similar with our primary analysis in terms of the signs and statistical significance of the coefficient estimates, showing the robustness of our primary results.
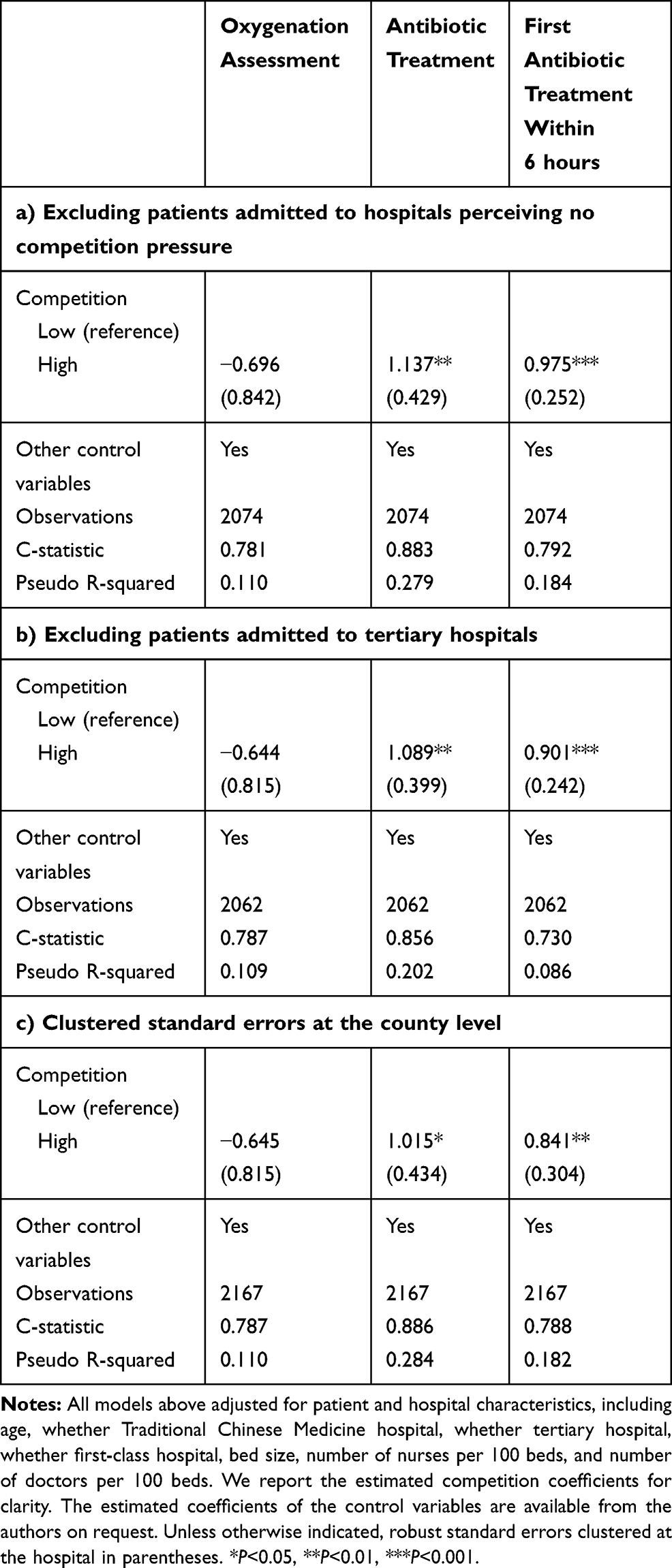 |
Table 5 Robustness Checks |
Discussion
In this study, we investigated the association between perceived competition and the process of care for patients with bacterial pneumonia under the fee-for-service payment system in rural China. Controlling for patient and hospital characteristics, we found that higher perceived competition was positively associated with improved process of care for patients with bacterial pneumonia in terms of antibiotic treatment and first antibiotic treatment within 6 hours after admission, which was consistent with previous studies.28,29 These findings suggested that, under the fee-for-service payment system, a higher level of perceived competition among hospitals might probably serve as an incentive for attracting bacterial pneumonia patients through providing more effective and timely antibiotic treatment. This incentive may be stronger for the care treating the non-acute conditions. Compared with acute symptomatic illnesses such as stroke and AMI, patients with pneumonia tend to have more autonomy in choosing their healthcare providers,24 thus enabling them to seek alternative providers when suffering the delay of antibiotic treatment.
Our findings also indicated that the impact of perceived competition on the process of care varied with quality measures. An unexpected finding was that hospitals with higher perceived competition were less likely to provide oxygenation assessment for patients with bacterial pneumonia, despite the insignificance of such effect in our results. Confronted with intensified market competition, hospitals tend to prioritize the quality that is more easily understood or observed by patients than the unobservable quality.30 For example, Propper et al57 reported that hospitals in competitive markets tend to reduce the patients’ waiting time (observable quality) while having higher AMI mortality (unobservable quality). Likewise, since antibiotic treatment is widely known as an essential treatment method for bacterial pneumonia, it has become much more discernable for patients compared with the oxygenation assessment. As a result, hospitals are much more likely to pay more attention to antibiotic treatment (observable quality) than oxygenation assessment (unobservable quality).
As part of our findings, a strong negative association between the number of nurses per 100 beds and antibiotic use was identified, which differed from previous studies conducted in other settings. Fine et al58 reported that the higher registered nurse-bed ratio is associated with timely antibiotic administration for patients hospitalized with pneumonia in the United States. Haug et al59 also found a similar positive correlation between nursing staffing level and antibiotic use based on the analysis of the data retrieved from health enterprises in Norway. The opposite relationship between nurse staffing and the process of care in our study would represent the fact that the hospitals with poor healthcare quality tend to increase their nurse staffing, which needs further investigation in future studies.
Our study provided empirical evidence that perceived competition was associated with improved process of care for patients with bacterial pneumonia. However, Lin et al24 used predicted HHI to measure hospital competition in Shanxi province, China, and found that higher hospital competition was associated with higher in-hospital mortality for patients with pneumonia. There are two possible explanations for such contradictive findings. First, a better process of care may not lead to better outcomes. Although some observational studies found significant associations between the process of care and the outcomes for patients hospitalized with pneumonia,60–62 contradictive results were also reported by other researchers. For example, Ryan et al63 examined the relationship between Medicare’s process of care quality measures and the mortality for pneumonia, reporting that there was no causal relationship between hospital-level process of care performance and mortality. Another study conducted by Lee et al45 investigated the association between the process of care and the outcomes for pneumonia patients in Connecticut and Pennsylvania and reported similar findings. Second, objective and subjective competition measures may exert different effects on quality of care. Zinn et al40 investigated the predictors of total quality management adoption in nursing homes and found that perceived competition was significantly associated with total quality management adoption, but the objective competition measures (ie, HHI, excess capacity, and availability of substitutes) were not. Their explanation was that the managers of nursing homes tend to take necessary arrangements only when they perceive a competitive threat, regardless of the degree of objective competition.
Under the fee-for-service payment system, the competition perceived by hospital managers in rural China has potential impacts on the process of care. Our empirical findings supported the pro-competition policies in China’s healthcare reform. However, different payment systems might provide different incentives for hospitals in terms of healthcare delivery, which would potentially affect the effects of market competition on quality improvement.36 For example, under the DRGs payment system, the government sets a fee for each diagnosis-related group, regardless of the quality of treatment supplied by the hospitals. As this system is designed for cost containment, hospitals would have an incentive to adopt the most cost-effective treatment and have less concern about the quality of treatment. As a result, hospitals might have no incentive to improve quality of care. In terms of the capitation payment, hospitals are incentivized to provide more preventive care for less treatment expenses in the future. Meanwhile, hospitals have a strong incentive to reduce treatment intensity as more volume means less profit, thus further resulting in reduced quality. The pay-for-performance payment system, as another example, provides financial incentives to healthcare providers, which encourages them to compete with each other based on quality in a more cost-effective way. Moreover, the recent development of medical alliances in China’s healthcare market might complicate the competition among hospitals. At present, there are no tailored payment systems or a clear mechanism of benefit distribution to balance the competition and cooperation among hospitals. Therefore, to fully exert the positive effects of hospital competition on improving quality of care, health policy-makers should recognize the interactions between payment systems and hospital competition and realign incentives to hospitals carefully during the payment systems reform. Our findings were also expected to provide implications for other countries confronted with similar challenges with a fee-for-service payment system.
It should be noted that our study has several limitations. First, this study cannot establish a causal relationship between perceived competition and process of care due to the cross-sectional study design. There would be potential endogenous problems in the estimations, such as simultaneous bias between competition and the process of care. Future research using a causal inference design, such as instrumental variable and regression discontinuity design are warranted. Second, the care for bacterial pneumonia might not be representative of all cares. Our empirical evidence from the rural area of Guizhou only represented China’s lower-income rural regions, thus might not be generalizable to other diseases, urban area, and eastern China. Third, our study was merely conducted under the fee-for-service payment system, thus requiring further investigations on the relationship between competition and the process of care in other settings without a fee-for-service payment system, such as pay-for-performance and DRGs. Further research should also examine whether payment reforms could impact the relationship between hospital competition and quality. Fourth, the robustness of our findings might be reduced due to the lack of other confounding factors such as gender, severity of illness, and socio-economic status. The three-point Likert scale used in this study might also bring potential biases due to lacking response variability. The five-point or seven-point Likert scales would be appropriate to increase the variance of measures. Lastly, the objective competition measures (ie, HHI) are useful in measuring competition intensity, while we only included a subjective competition measure (perceived competition) in this study due to data availability. However, as described in the method section, the objective competition measures have a drawback of capturing potential competitors. It is possible that a hospital perceives high competition pressure in a less competitive market measured by HHI and vice versa. Unlike the objective competition measures, the subjective measure of hospital competition used in this study (perceived competition) emphasized the hospital directors’ perception of market competition rather than the competition per se. It should therefore be highlighted that compared with objective competition measures, perceived competition has its advantages on capturing the potential competitors. Nevertheless, it is noteworthy that several drawbacks embedded in perceived competition might bring potential biases: self-reporting bias, its correlation with respondents’ characteristics, and the unknown relationship between the competition pressure perceived by hospital directors and doctors’ behaviors. As the perceived competition was reported by the hospital directors from a subjective perspective, it might bring self-reporting bias. A list of hospital directors’ characteristics (ie, education background, management experience, competition pressure in last year) might also impact their perceived competition, thus leading to varied competition pressure perceived by different hospital directors even in a same scenario. It remains unknown whether the perceived competition of hospital directors could affect doctors’ behaviors because health services are delivered directly by doctors rather than hospital directors. Since all competition measures have pros and cons, incorporating both objective and subjective measures of competition would be helpful for future research in determining the role of competition in improving the quality of care.
Conclusion
Our findings suggested that higher perceived competition was significantly associated with improved process quality in antibiotic treatment and first antibiotic treatment within 6 hours, but not in oxygenation assessment. Our study provided empirical evidence supporting the pro-competition policies in China’s healthcare reform.
Ethics and Consent Statement
The Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project was led by Harvard University, and the project partners included Fudan University, Sichuan University, Peking University, and Sun Yat-sen University. The preparation work before implementing the project was conducted and finished by Fudan University, therefore this project was reviewed and approved by the School of Public Health Institutional Review Board, Fudan University (Approval number: IRB#2015-08-0561). This project was conducted in accordance with the Declaration of Helsinki. The patient consent to review their medical records was not required by the Institutional Review Board because the medical records we extract from hospitals were de-identified and the use of data cannot result in any damage or distress. Prior to the formal survey, we informed the hospital directors and obtained their oral and written informed consent to take part in our survey.
Acknowledgments
We thank Wen Chen, Min Hu, and Luying Zhang in Fudan University for their great contribution to the preparation of the Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH) project. We are also grateful to two anonymous referees and an anonymous editor for highly valuable comments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kessler DP, McClellan MB. Is hospital competition socially wasteful? Q J Econ. 2000;115(2):577–615. doi:10.1162/003355300554863
2. Gaynor M, Town RJ. Competition in health care markets. In: Handbook of Health Economics. Vol. 2. Elsevier; 2011:499–637.
3. Choné P. Competition policy for health care provision in France. Health Policy (New York). 2017;121(2):111–118. doi:10.1016/j.healthpol.2016.11.015
4. Kifmann M. Competition policy for health care provision in Germany. Health Policy (New York). 2017;121(2):119–125. doi:10.1016/j.healthpol.2016.11.014
5. Propper C. Competition in health care: lessons from the English experience. Health Econ Policy Law. 2018;13(3–4):492–508. doi:10.1017/S1744133117000494
6. Brekke KR, Siciliani L, Straume OR. Hospital Competition and Quality with Regulated Prices. Scand J Econ. 2011;113(2):444–469. doi:10.1111/j.1467-9442.2011.01647.x
7. Xu T, Wu AW, Makary MA. The Potential Hazards of Hospital Consolidation: implications for Quality, Access, and Price. JAMA. 2015;314(13):1337–1338. doi:10.1001/jama.2015.7492
8. Porter ME, Teisberg EO. Redefining competition in health care. Harv Bus Rev. 2004;82(6):64–77.
9. Arrow KJ. Uncertainty and the Welfare Economics of Medical Care. Am Econ Rev. 1963;53(5):941–973.
10. Robinson J. Hospitals respond to Medicare payment shortfalls by both shifting costs and cutting them, based on market concentration. Health Aff. 2011;30(7):1265–1271. doi:10.1377/hlthaff.2011.0220
11. Barros PP, Brouwer WBF, Thomson S, Varkevisser M. Competition among health care providers: helpful or harmful? Eur J Health Econ. 2016;17(3):229–233. doi:10.1007/s10198-015-0736-3
12. Cooper Z, Gibbons S, Jones S, McGuire A. Does Hospital Competition Save Lives? Evidence from the English NHS Patient Choice Reforms. Econ J. 2011;121(554):F228–F260. doi:10.1111/j.1468-0297.2011.02449.x
13. Gaynor M, Moreno-Serra R, Propper C. Death by Market Power: reform, Competition, and Patient Outcomes in the National Health Service. Am Econ J Econ Policy. 2013;5(4):134–166. doi:10.1257/pol.5.4.134
14. Gowrisankaran G, Town RJ. Competition, Payers, and Hospital Quality. Health Serv Res. 2003;38(6p1):1403–1422. doi:10.1111/j.1475-6773.2003.00185.x
15. Propper C, Burgess S, Green K. Does competition between hospitals improve the quality of care? Hospital death rates and the NHS internal market. J Public Econ. 2004;88(7–8):1247–1272. doi:10.1016/S0047-2727(02)00216-5
16. Mutter RL, Wong HS, Goldfarb MG. The effects of hospital competition on inpatient quality of care. Inquiry. 2008;45(3):263–279. doi:10.5034/inquiryjrnl_45.03.263
17. Pan J, Qin X, Hsieh CR. Is the pro-competition policy an effective solution for China’s public hospital reform? Health Econ Policy Law. 2016;11(4):337–357. doi:10.1017/S1744133116000220
18. Pan J, Liu GG, Gao C. How does separating government regulatory and operational control of public hospitals matter to healthcare supply? China Econ Rev. 2013;27:1–14. doi:10.1016/j.chieco.2013.07.002
19. Pan J, Qin X, Li Q, Messina JP, Delamater PL. Does hospital competition improve health care delivery in China? China Econ Rev. 2015;33:179–199. doi:10.1016/j.chieco.2015.02.002
20. Fullman N, Yearwood J, Abay SM, et al. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: a systematic analysis from the Global Burden of Disease Study 2016. Lancet. 2018;391(10136):2236–2271. doi:10.1016/S0140-6736(18)30994-2
21. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
22. Jian W, Figueroa J, Woskie L, et al. Quality of care in large Chinese hospitals: an observational study. BMJ Qual Saf. 2019;28(12):955–958. doi:10.1136/bmjqs-2018-008938
23. Zhou Y, Yao X, Liu G, Jian W, Yip W. Level and variation on quality of care in China: a cross-sectional study for the acute myocardial infarction patients in tertiary hospitals in Beijing. BMC Health Serv Res. 2019;19(1):43. doi:10.1186/s12913-019-3872-0
24. Lin X, Cai M, Fu Q, et al. Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China. Int J Environ Res Public Health. 2018;15(10):2283. doi:10.3390/ijerph15102283
25. Lu L, Pan J. The association of hospital competition with inpatient costs of stroke: evidence from China. Soc Sci Med. 2019;230:234–245. doi:10.1016/j.socscimed.2019.04.017
26. Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q. 2005;83(4):691–729. doi:10.1111/j.1468-0009.2005.00397.x
27. Bennett D, Hung CL, Lauderdale TL. Health Care Competition and Antibiotic Use in Taiwan. J Ind Econ. 2015;63(2):371–393. doi:10.1111/joie.12075
28. Bijlsma MJ, Koning PWC, Shestalova V. The Effect of Competition on Process and Outcome Quality of Hospital Care in the Netherlands. Economist. 2013;161(2):121–155. doi:10.1007/s10645-013-9203-7
29. Croes RR, Krabbe-Alkemade YJFM, Mikkers MC. Competition and quality indicators in the health care sector: empirical evidence from the Dutch hospital sector. Eur J Health Econ. 2018;19(1):5–19. doi:10.1007/s10198-016-0862-6
30. Wani D, Malhotra M, Venkataraman S. Impact of competition on process of care and resource investments. J Oper Manage. 2018;57(1):23–35. doi:10.1016/j.jom.2017.12.002
31. Liu G, Xue Y, Qian Z, et al. Healthcare-seeking behavior among pregnant women in the Chinese hierarchical medical system: a cross-sectional study. Int J Equity Health. 2019;18(1):129. doi:10.1186/s12939-019-1037-8
32. Meng Q, Fang H, Liu X, Yuan B, Xu J. Consolidating the social health insurance schemes in China: towards an equitable and efficient health system. Lancet. 2015;386(10002):1484–1492. doi:10.1016/S0140-6736(15)00342-6
33. Rice T, Unruh LY, van Ginneken E, Rosenau P, Barnes AJ. Universal coverage reforms in the USA: from Obamacare through Trump. Health Policy (New York). 2018;122(7):698–702. doi:10.1016/j.healthpol.2018.05.007
34. Goddard M. Competition in healthcare: good, bad or ugly? Int J Health Policy Manag. 2015;4(9):567–569. doi:10.15171/ijhpm.2015.144
35. Jha AK, Li Z, Orav EJ, Epstein AM. Care in US hospitals—the Hospital Quality Alliance program. N Engl J Med. 2005;353(3):265–274. doi:10.1056/NEJMsa051249
36. Nishida K, Yoshida A. A comparison between two health care delivery systems using a spatial competition model approach. Reg Stud Reg Sci. 2016;3(1):337–354. doi:10.1080/21681376.2016.1209980
37. Moscelli G, Gravelle H, Siciliani L, Santos R. Heterogeneous effects of patient choice and hospital competition on mortality. Soc Sci Med. 2018;216:50–58. doi:10.1016/j.socscimed.2018.09.009
38. Baker LC. Measuring competition in health care markets. Health Serv Res. 2001;36(1 Pt 2):223–251.
39. Wong HS, Zhan C, Mutter R. Do different measures of hospital competition matter in empirical investigations of hospital behavior? Rev Ind Organ. 2005;26(1):61–87. doi:10.1007/s11151-004-6067-7
40. Zinn JS, Weech RJ, Brannon D. Resource dependence and institutional elements in nursing home TQM adoption. Health Serv Res. 1998;33(2 Pt 1):261–273.
41. Özgen Narcı H, Ozcan YA, Şahin İ, Tarcan M, Narcı M. An examination of competition and efficiency for hospital industry in Turkey. Health Care Manag Sci. 2015;18(4):407–418. doi:10.1007/s10729-014-9315-x
42. Choi J-S, Choi S, Lee S, Han E, Kim M-I. Does market competition facilitate resident-centred care among nursing homes? A comparative analysis. Asia Pac J Soc Work. 2016;26(1):15–28. doi:10.1080/02185385.2016.1150874
43. Guizhou Provincial Bureau of Statistics. Guizhou Statistical Yearbook 2018. Beijing, China: China Statistics Press; 2018.
44. Analysis of Provider Payment Reforms on Advancing China’s Health (APPROACH): An Evaluation of County Hospitals (English). Washington, D.C: World Bank Group. http://documents.worldbank.org/curated/en/591771559887831544/An-Evaluation-of-County-Hospitals.
45. Lee JS, Primack BA, Mor MK, et al. Processes of care and outcomes for community-acquired pneumonia. Am J Med. 2011;124(12):
46. Shahian DM, Meyer GS, Mort E, et al. Association of National Hospital Quality Measure adherence with long-term mortality and readmissions. BMJ Qual Saf. 2012;21(4):325–336. doi:10.1136/bmjqs-2011-000615
47. National Quality Forum. Care quality measures. http://www.qualityforum.org/Home.aspx.
48. Ministry of Health. Tertiary General Hospital Accreditation Criteria (2011). http://www.nhc.gov.cn/cmsresources/mohwsyjbgs/cmsrsdocument/doc14029.doc.
49. Ministry of Health. Secondary General Hospital Accreditation Criteria (2012). http://www.nhc.gov.cn/xxgk/pages/publicfiles/business/cmsresources/mohwsyjbgs/cmsrsdocument/doc14022.doc.
50. Thoracic Society of Chinese Medical Association. Diagnosis and treatment guidelines for adult community acquired pneumonia in China (2016 version) (in Chinese). Chin J Tubere Respir Dis. 2016;39(4):253–279.
51. National Health Commission. State Administration of Traditional Chinese Medicine. Guidelines for diagnosis and treatment of community-acquired pneumonia in children (2019 version) (in Chinese). Chin J Clin Infect Dis. 2019;12(1):6–13.
52. Keeler EB, Melnick G, Zwanziger J. The changing effects of competition on non-profit and for-profit hospital pricing behavior. J Health Econ. 1999;18(1):69–86. doi:10.1016/s0167-6296(98)00036-8
53. Bernstein AB, Gauthier AK. Defining competition in markets: why and how? Health Serv Res. 1998;33(5 Pt 2):1421–1438.
54. Song H, Zuo X, Cui C, Meng K. The willingness of patients to make the first visit to primary care institutions and its influencing factors in Beijing medical alliances: a comparative study of Beijing’s medical resource-rich and scarce regions. BMC Health Serv Res. 2019;19(1):361. doi:10.1186/s12913-019-4184-0
55. Jha AK. Measuring hospital quality: what physicians do? How patients fare? Or both? JAMA. 2006;296(1):95–97. doi:10.1001/jama.296.1.95
56. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. Vol. 398. New York: John Wiley & Sons; 2013.
57. Propper C, Burgess S, Gossage D. Competition and Quality: evidence From the NHS Internal Market 1991–9. Econ J. 2008;118(525):138–170. doi:10.1111/j.1468-0297.2007.02107.x
58. Fine JM, Fine MJ, Galusha D, Petrillo M, Meehan TP. Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia: results from the medicare quality indicator system pneumonia module. Arch Intern Med. 2002;162(7):827–833. doi:10.1001/archinte.162.7.827
59. Haug JB, Berild D, Walberg M, Reikvam Å. Hospital- and patient-related factors associated with differences in hospital antibiotic use: analysis of national surveillance results. Antimicrob Resist Infect Control. 2014;3(1):40. doi:10.1186/s13756-014-0040-5
60. Gleason PP, Meehan TP, Fine JM, Galusha DH, Fine MJ. Associations between initial antimicrobial therapy and medical outcomes for hospitalized elderly patients with pneumonia. Arch Intern Med. 1999;159(21):2562–2572. doi:10.1001/archinte.159.21.2562
61. Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med. 2004;164(6):637–644. doi:10.1001/archinte.164.6.637
62. Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA. 1997;278(23):2080–2084. doi:10.1001/jama.1997.03550230056037
63. Ryan AM, Burgess JF, Tompkins CP, Wallack SS. The relationship between Medicare’s process of care quality measures and mortality. Inquiry. 2009;46(3):274–290. doi:10.5034/inquiryjrnl_46.03.274
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.