Back to Journals » Patient Preference and Adherence » Volume 17
Peer Support in Rheumatic Diseases: A Narrative Literature Review
Authors Karp N, Yazdany J, Schmajuk G
Received 4 March 2023
Accepted for publication 8 September 2023
Published 2 October 2023 Volume 2023:17 Pages 2433—2449
DOI https://doi.org/10.2147/PPA.S391396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Nathan Karp,1 Jinoos Yazdany,1,2 Gabriela Schmajuk1– 3
1Department of Medicine, Division of Rheumatology, University of California, San Francisco, CA, USA; 2Institute for Health Policy Research, University of California, San Francisco, CA, USA; 3Department of Medicine, Division of Rheumatology, San Francisco Veterans Affairs Health System, San Francisco, CA, USA
Correspondence: Nathan Karp, Department of Medicine, Division of Rheumatology, University of California, 4150 Clement St. (111R), San Francisco, CA, 94121, USA, Tel +1 415 221 4810 ext. 23857, Email [email protected]
Abstract: Rheumatic diseases are a group of chronic conditions that are associated with significant morbidity, impaired physical function, psychosocial stress, and cost to the healthcare system. Peer support interventions have been shown to have a positive impact on health outcomes in several chronic conditions, but no review has specifically assessed the impact of peer support on rheumatic conditions. The aim of this narrative literature review was to understand how peer support has been applied in the field of rheumatology, with a specific focus on the impact of observational and randomized studies of direct peer support interventions on various outcome measures across rheumatic conditions. We also examined studies exploring patient attitudes and preferences toward peer support. The majority of studies included focused on peer support in rheumatoid arthritis and systemic lupus erythematosus. Generally, patients across the spectrum of rheumatic disease perceive peer support as a useful tool. Peer support interventions, while highly variable, were generally associated with positive impacts on health-related quality of life metrics (both perceived and measured), although these differences were not always statistically significant. Important limitations include variability in study design, selection bias among study participants, and short follow-up periods across most peer support interventions.
Keywords: rheumatology, patient preferences, peer navigation, peer support, self-management
Introduction
Rheumatic diseases are a heterogenous group of chronic inflammatory conditions that are associated with significant morbidity, mortality, and cost—to both patients and the healthcare system. Rheumatoid arthritis (RA), for example, affects 0.5% to 1% of adults in the United States, and represents a total annual societal cost in excess of $39 billion (in 2005 United States dollars).1–3 Systemic lupus erythematosus (SLE), while less prevalent, also exerts a significant financial burden; the average annual direct health care costs for individuals with severe disease may exceed $50,000.4–6
In addition to the physical symptoms associated with these conditions, living with a rheumatic disease can have profound ramifications for an individuals’ emotional and psychological well-being. A new diagnosis of RA may leave patients feeling isolated and ill-equipped to cope with their disease7,8 Patients living with SLE are subject to disease flares that can lead to organ- or life-threatening complications; these patients can experience severe psychological stress and have a high incidence of comorbid anxiety, depression and psychiatric disease.9,10
Individualized needs assessments, patient education and self-management strategies are foundational components of chronic disease management, and these have been incorporated into guidelines for the treatment of rheumatic disease.11,12 Peer support may represent an opportunity for achieving some of these goals by leveraging individuals’ experience living with a disease to support others attempting to do the same. As described in one conceptual analysis, the objective of peer support is the provision of emotional, appraisal and informational assistance by a created social network member who possesses experiential knowledge of a specific behaviour or stressor and similar characteristics as the target population.13 The introduction of such peer support measures may, through direct or indirect effects, improve health outcomes and foster a sense of community and belonging for patients that could help reduce the burden on care providers (ie, family and friends) and the healthcare system as a whole.14,15
While peer support interventions have been shown to be effective in the management of several chronic conditions (including HIV, chronic kidney disease, diabetes mellitus, and malignancy),16–22 there is considerable variability in how peer support is defined or applied across studies, even within the same condition. A recent systematic review attempted to categorize peer support interventions and assess their efficacy in chronic conditions; this review found significant inconsistencies in how “peers” and “peer support” are defined, ambiguous study designs, and widely variable outcome measurement.15 Furthermore, to our knowledge, no literature review has queried the specific impacts of peer support interventions for rheumatic conditions. As such, the exploration of peer support interventions in rheumatic disease represents a key knowledge gap and is the focus of this review article.
While rheumatology-focused literature reviews may be lacking, peer support has emerged as a key component of self-management programs—with demonstrated efficacy in the realm of rheumatology. Foundational research by Lorig et al showed that both a generic Chronic Disease Self-Management program and an Arthritis Self-Management Program were efficacious interventions for patients with arthritis.23,24 These programs may be considered a form of peer support, as the highly structured programming is administered in a group setting by trained peer leaders. While these programs have been shown to be cost effective,25 they are considerably resource-intensive. Direct peer support tools may represent a less resource-intensive intervention—requiring less programmatic structure and peer training—with applications in rheumatic disease. Increasingly, the internet has become a popular destination for patients to seek information and support,26 inviting new ideas for web-based peer support applications. This is particularly relevant for more rare rheumatic conditions, where the internet could facilitate peer-to-peer interactions that would not otherwise be feasible in person.
In this review, we have examined recent literature on peer support interventions in rheumatic disease, with an emphasis on direct peer support interventions rather than those that co-occur within comprehensive disease management programs. We aimed to summarize the documented effects of peer support on rheumatic disease outcomes such as functional status, disease activity, medication adherence, patient knowledge, health care utilization and cost, and other self-efficacy and quality-of-life metrics from both observational and randomized studies of peer support interventions. We also reviewed qualitative interview, survey, and focus-group based studies exploring patient and provider attitudes toward peer support.
Methods
We searched PubMed for English-language articles published between 2000 and 2023 that examined peer support in rheumatic diseases. The year 2000 was selected to help capture more recent studies that explore novel, internet-based approaches to peer support. Search terms included rheumatologic disease states (inflammatory arthritis, rheumatoid arthritis, systemic lupus erythematosus, mixed connective tissue disease, systemic sclerosis, ankylosing spondylitis, psoriatic arthritis, vasculitis, dermatomyositis, polymyositis, gout) and their corresponding MeSH terms in conjunction with terms related to peer support (peer support, peer navigator, peer mentor, peer-led, and peer-to-peer).
After the initial PubMed search, one author (NK) reviewed the titles of all articles and applied the following selection criteria: we excluded studies that were unrelated to rheumatic disease or the topic of peer support in rheumatic disease, primarily about pediatric-aged populations, or focused on non-inflammatory conditions, such as osteoarthritis, fibromyalgia, or chronic back pain. While many articles referenced peer support, or discussed interventions that indirectly incorporated peer support modalities, we focused our review on those studies where peer support was a central focus. We reviewed abstracts of the remaining articles (and reference lists from included articles) to identify studies investigating specific peer support interventions and other articles exploring patient and provider preferences and attitudes toward peer support.
Results
Our initial search yielded 103 full text articles (Figure 1). After applying our exclusion criteria, 52 articles were selected for abstract review. Following review of these abstracts and associated reference lists, we identified 30 articles for inclusion. The majority of these articles focused on peer support interventions (n=9) and attitudes toward peer support (n=8) in RA and other forms of inflammatory arthritis (IA); we identified a smaller body of literature examining the same (n=5, n=1, respectively) in SLE. We also identified articles (n=7) investigating peer support in the context of rarer rheumatic conditions, including vasculitis and systemic sclerosis (SSc). The results of our analysis are organized into the following four sections: peer support interventions in RA/IA, attitudes toward peer support in RA/IA, peer support in SLE, and peer support in other rheumatic diseases.
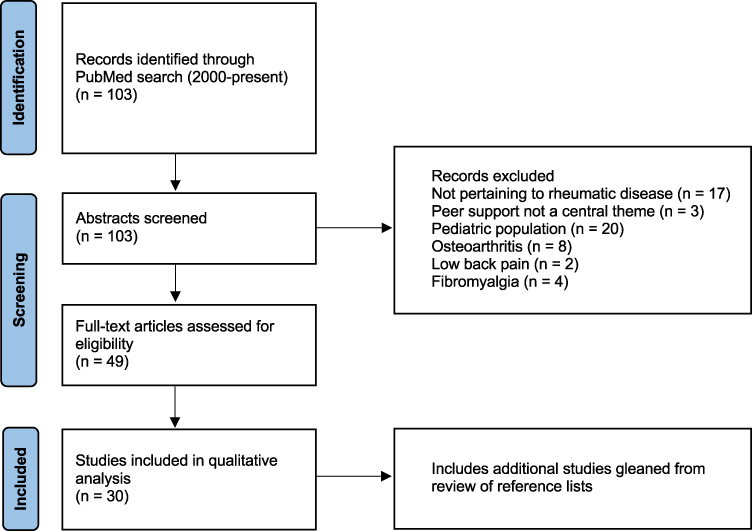 |
Figure 1 Study selection flow diagram. Note: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. |
Peer Support Interventions in RA/IA
Nine articles described peer support interventions in patients with IA; seven of these studies focused primarily on RA, while two examined patients with ankylosing spondylitis (see Table 1).27–35 Peer support interventions included online message boards and support groups, peer-to-peer telephone support, in-person support groups, and peer-led educational efforts. Patients with RA included in these studies were predominantly female and greater than 50 years old; those with AS were predominantly male, and younger than 50 years old.
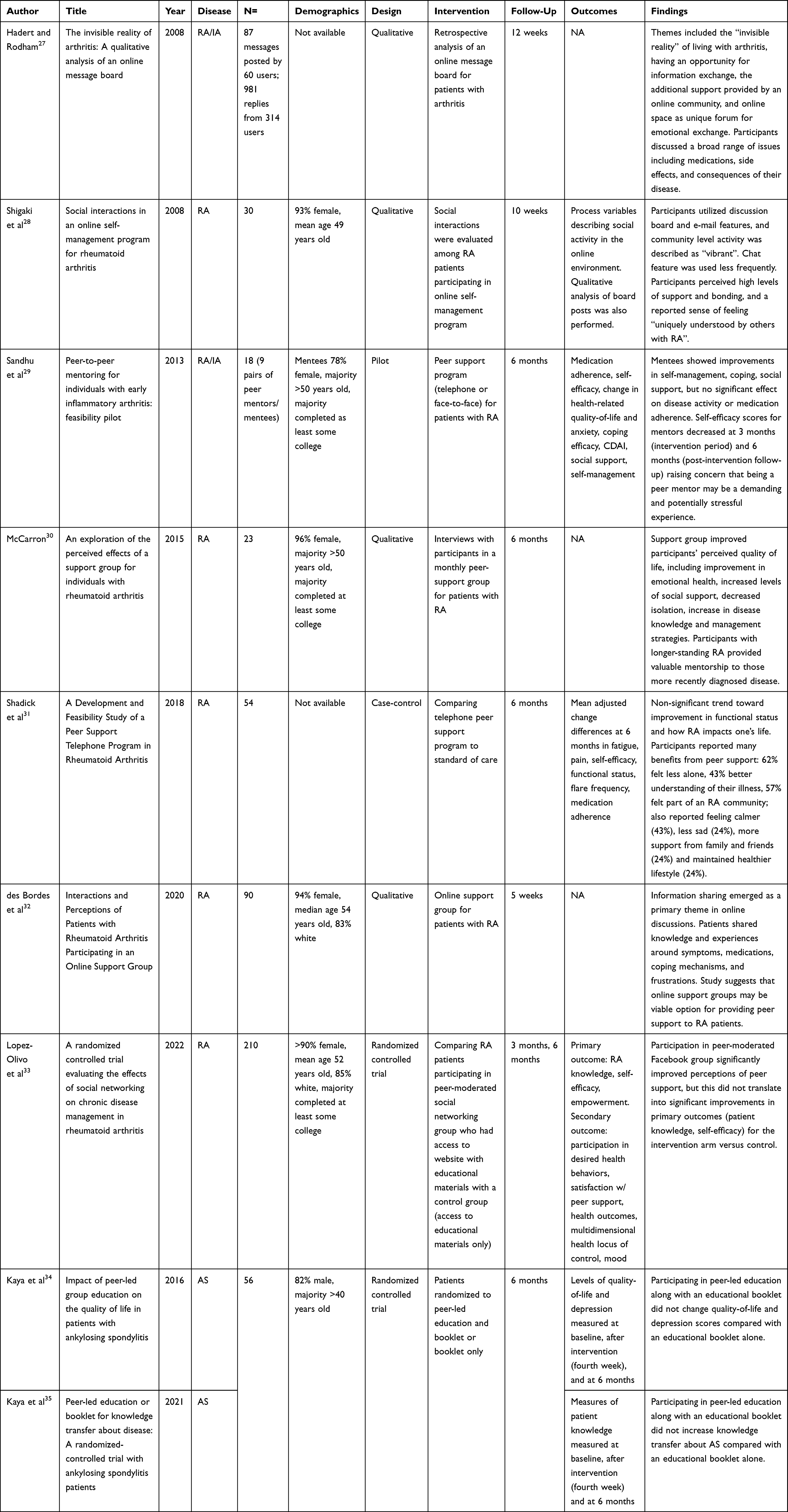 |
Table 1 Peer Support Interventions in RA/IA |
Of the nine total articles, three qualitative studies and one RCT explored online peer support interventions for patients with RA, including social interaction via online discussion board and participation in online support groups.27,28,32,33 Participants found these internet-based interventions to provide unique and valuable opportunities for information exchange, psychosocial support, and fostering a sense of community among patients with shared experiences living with RA. The one RCT in this category also demonstrated improved perceptions of peer support among participants, though these findings did not translate into significant improvements in the primary outcomes of patient knowledge or self-efficacy.33 Three additional studies (two feasibility pilots, one qualitative analysis) examined telephone and in-person peer support interventions, either individually or in a group setting.29–31 Participants reported many benefits in terms of improved social support, coping skills, and disease knowledge. One study showed a non-significant trend toward improvement in measures of functional status and how RA impacts one’s life.31 The only study that assessed the impact of peer support on disease activity and medication adherence did not show any significant effect for those outcomes.29
The two studies in ankylosing spondylitis patients reviewed findings from a single RCT investigating the impact of a peer-led education program. Neither of these studies showed benefit of the peer-led intervention over the control group in terms of quality-of-life metrics, depression scores, or knowledge transfer.34,35
In sum, peer support interventions in RA demonstrated some degree of improvement in self-management skills, quality of life metrics, and a trend toward improvement in functional status, though they have not been shown to modify disease activity or medication adherence, and these findings are not necessarily generalizable to patients with other forms of inflammatory arthritis.
Attitudes Toward Peer Support in RA/IA
Eight articles addressed patient perspectives on peer support in the context of their RA or other IA (see Table 2).36–43 As above, the patients with RA were primarily female and over the age of 50 years old. Several themes emerged, including a general interest in peer support groups, a belief that peer mentoring was important (especially in the setting of a new diagnosis), the importance of seeking support from others living with RA (as opposed to family and friends without the disease), and the ability of peer support to help foster group participation (eg in an organized exercise program). One study also assessed the attitudes of clinicians and nurses toward peer support programs, and identified concerns regarding the potential for lack of control and oversight over information that might be shared in peer support settings.42 In summary, patients living with RA/IA value peer support as an important tool to improve self-efficacy, though there remains some concern from providers about potential negative consequences of these interventions.
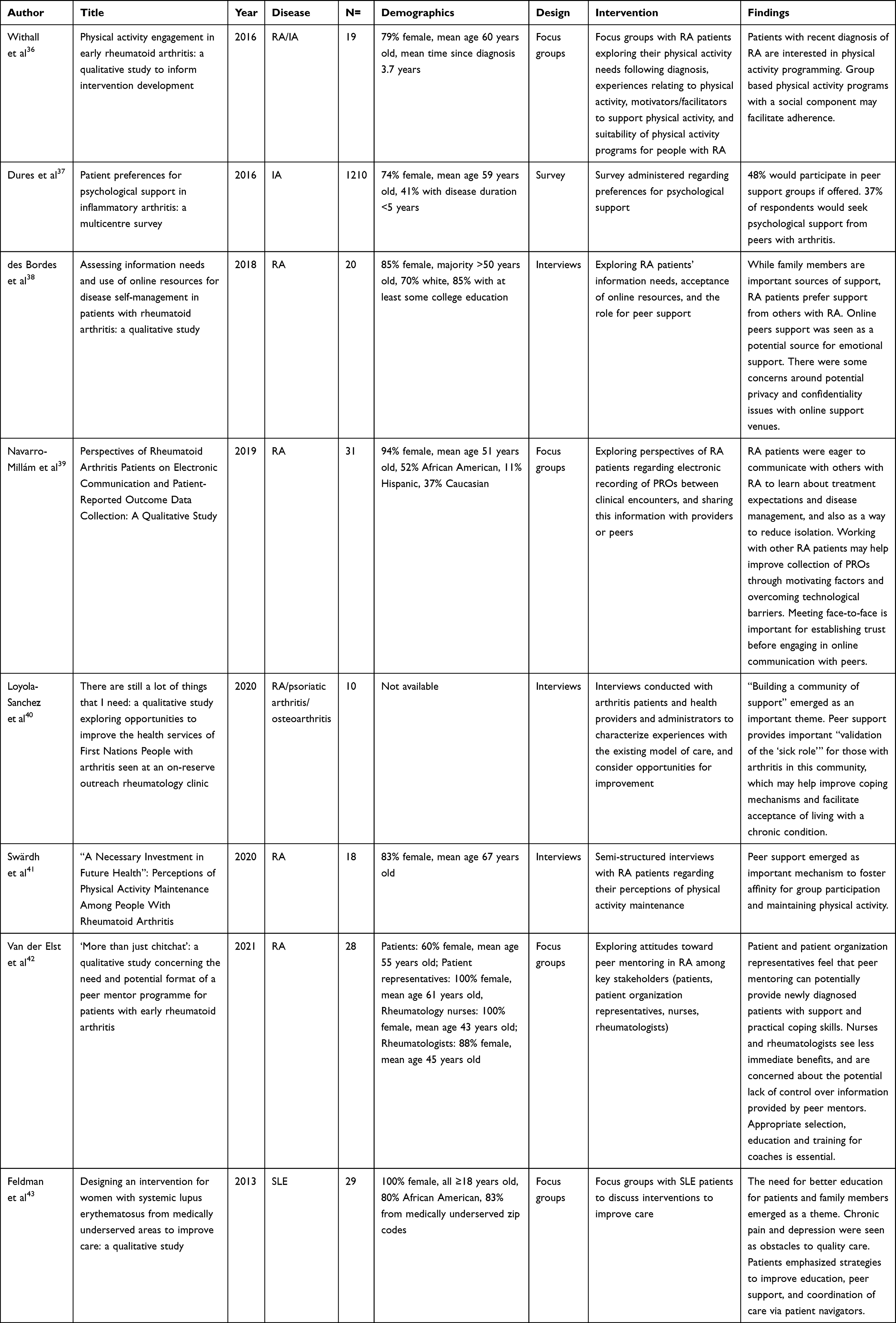 |
Table 2 Attitudes Toward Peer Support in Rheumatic Diseases |
Peer Support in SLE
Six publications, encompassing two patient cohorts, described peer support interventions among patients with SLE (see Table 3).44–49 The patients in these cohorts were predominantly African American women. Five articles reviewed findings from the Peer Approaches to Lupus Self-Management (PALS) project, a three-month feasibility pilot investigating a weekly, telephone-based peer mentoring intervention for African American women with SLE.45–49 One abstract evaluated a long-standing telephone-based peer counseling service for woman with SLE.44
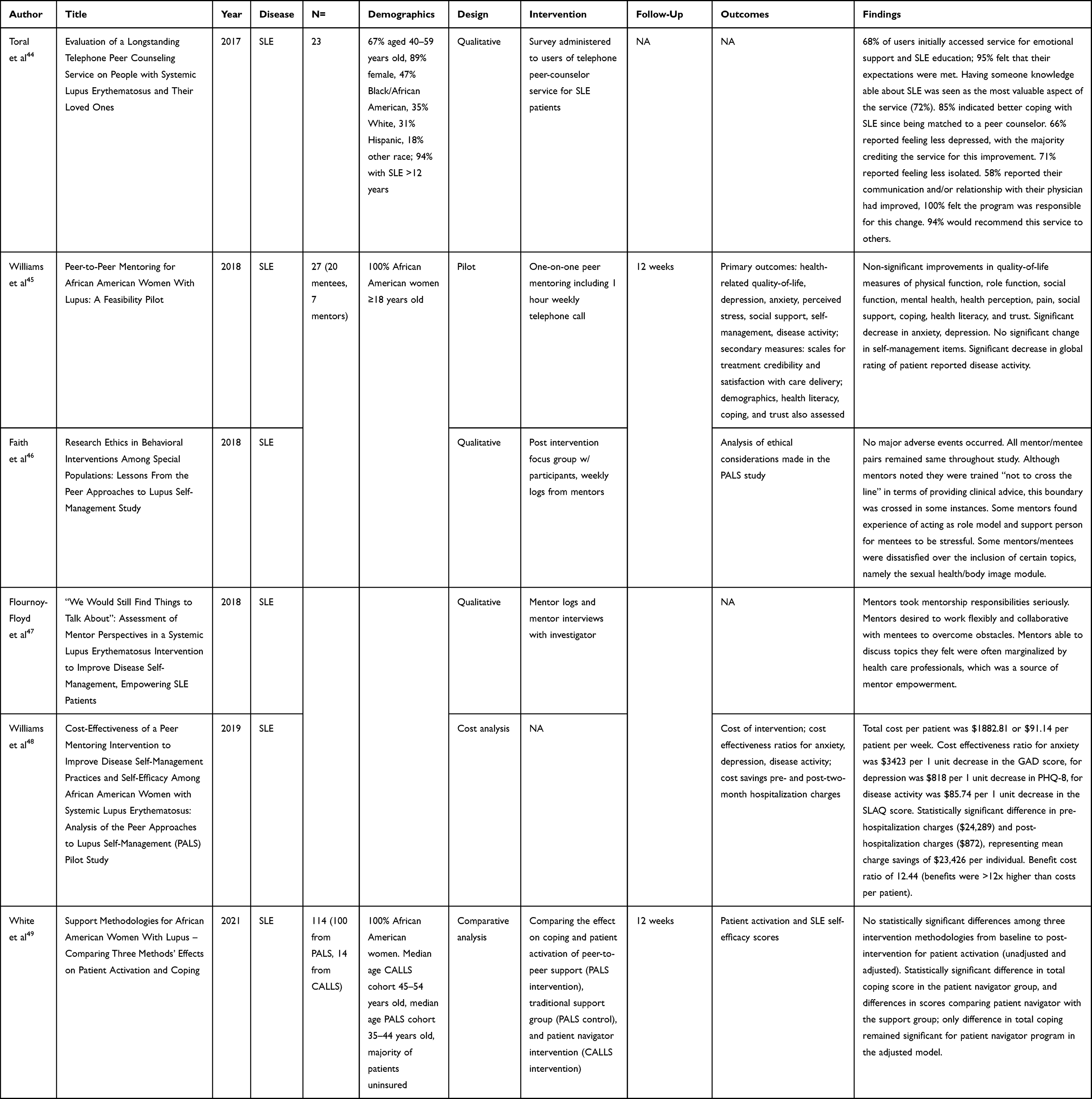 |
Table 3 Peer Support Interventions in SLE |
The PALS pilot study showed statistically significant improvements in participants’ anxiety and self-reported disease activity, non-significant improvements in various quality of life measures, including physical function, pain, coping, health literacy, trust, mental health, and trust.45 Peer mentors were also empowered by participation in this study, and found they were able to discuss topics with mentees that they felt were often ignored or minimized by health care providers.47 Interesting, preliminary data from this pilot also suggested significant cost savings for participants driven by decreased acute care utilization, including a benefit-cost ratio of >12x (meaning the cost savings to the health care system were greater than twelve times the cost of the program per patient),48 but the small sample size precluded definitive conclusions. There were no major adverse events during the study, though some mentors found the experience of acting as a role mode/support person to be stressful; mentors were also found to have inappropriately provided clinical advice in some instances.46 An article comparing the PALS cohort with another, patient navigator-based intervention, found that participants in the patient navigator group had significantly increased self-efficacy scores when compared with those in the peer-to-peer intervention.49
One study explored SLE patients’ attitudes toward peer support. Focus groups were conducted with SLE patients, predominantly from medically underserved areas, regarding potential interventions to improve care. Patients reported feeling isolated at the time of diagnosis, needing assistance to navigate the health care system, and a desire for SLE education. Nearly 70% of those surveyed favored a peer support intervention.43
To summarize, peer support interventions in SLE appear to improve —at least in the short term—self-reported disease activity, anxiety and depression, and to yield healthcare cost savings. Patients living with SLE also appear to have a favorable view of these interventions.
Peer Support in Other Rheumatic Diseases
Seven publications included in our analysis addressed peer support in rarer rheumatologic conditions (see Table 4). One study, a survey of patients with vasculitis, explored the relationship between peer support, medication adherence, and quality of life measures. At three months, an adherence-related peer support intervention was neither predictive of medication adherence nor improvements in quality of life.50 The other six studies, all qualitative analyses of survey data or focus groups, examined attitudes toward peer support groups among different cohorts of SSc patients in Europe and North America.
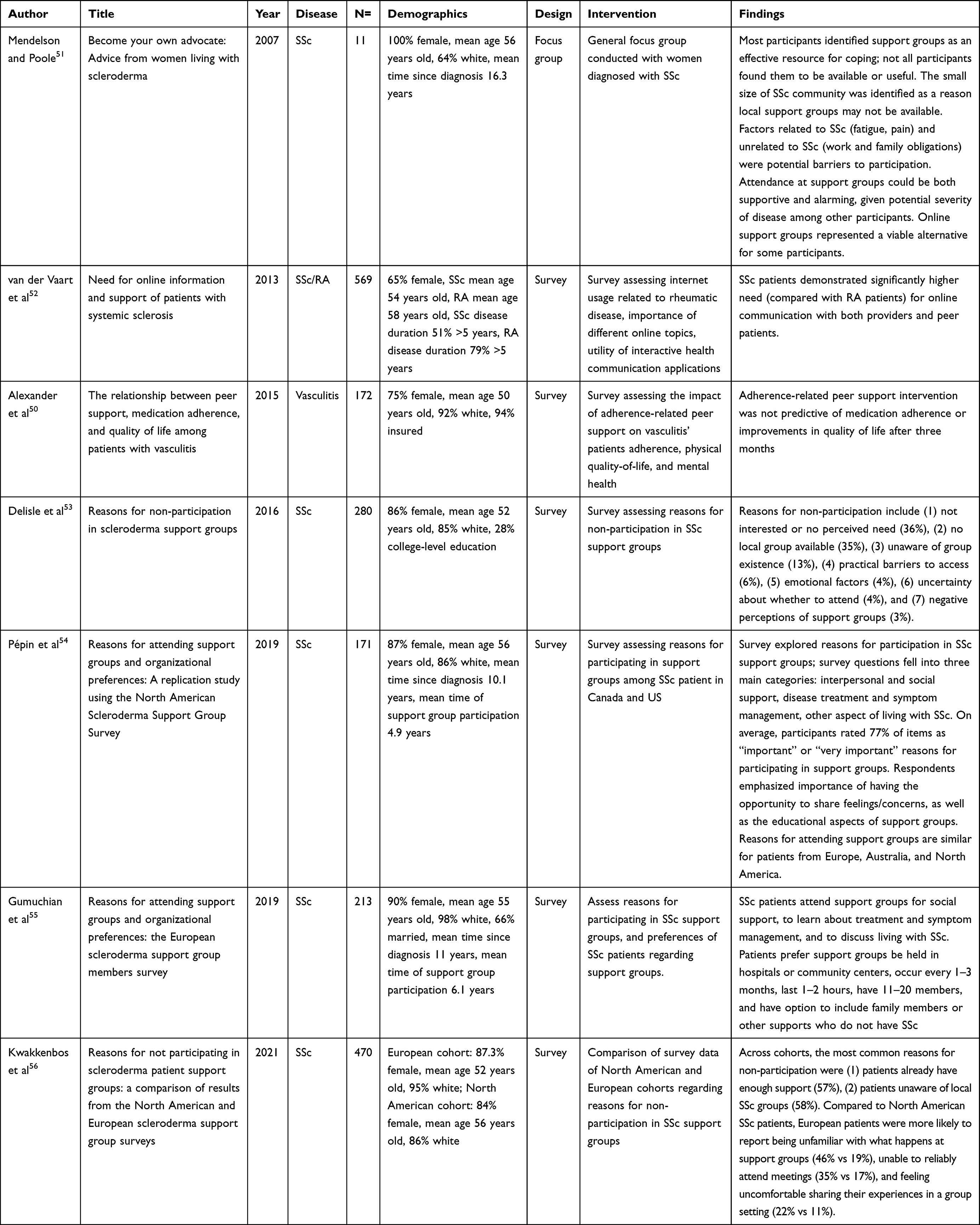 |
Table 4 Peer Support in Other Rheumatic Diseases |
All studies examining peer support in SSc encompassed predominantly white, female patients with a mean age greater than 50 years old. Two of the six studies explored reasons for participation in SSc support groups in Canada, the United States, and Europe. Across cohorts, patients attended support groups for similar reasons: to gain social support, to learn about treatment and symptom management, and to discuss other aspects of living with SSc.54,55 A focus group with SSc patients identified online support groups as a viable alternative for those who might not have local access to an in-person support group.51 Compared with RA patients, SSc patients have demonstrated a significantly higher need for online communication with both providers and their peers.52 Two other survey-based studies and one focus group also explored reasons for non-participation in SSc support.56,57 The most common reason for non-participation was lack of interest or no perceived need. A lack of in person support groups (attributed to the relative rarity of the disease) was also a common reason for non-participation. European respondents were relatively less aware of what happens at support groups, and reported feeling less comfortable sharing their experiences in a group setting.56 Even among focus group respondents who found group attendance to be supportive, there were concerns about potential adverse impacts, including exposure to severe disease complications that may be frightening or cause illness anxiety among those with less advanced disease.51
In sum, peer support groups are an important resource for patients living with more rare rheumatologic conditions, like systemic sclerosis, though the impact of these support groups on health outcomes remains unclear.
Discussion
We performed a narrative review of recent studies exploring peer support interventions and attitudes toward peer support in the context of rheumatic disease. Although there was significant heterogeneity in what constitutes peer support (and the mechanisms by which peer support is delivered), we found that patients’ perceptions of peer support were generally favorable across rheumatic conditions, and there exists some signal toward benefit with regard to self-management skills and functional status (in RA/IA) and quality-of-life metrics and health care utilization/costs (in SLE).
Our findings are consistent with existing literature on peer support interventions in the management of other chronic diseases. Studies of peer support for those living with chronic conditions tend to focus on quality of life and self-efficacy outcomes, with most studies reporting positive but non-significant findings.15 The heterogeneity of peer support, however, poses a significant and foundational challenge to this area of study. Peer support can be incredibly variable; interventions may include professionally-led group sessions, peer-led self-management trainings, peer coaches, community health workers, in-person support groups, as well as telephone- and internet based peer support.58 Although many studies on self-management include some type of peer-based intervention, these interventions do not occur in a vacuum, and it can be difficult to parse direct effect of peer support from co-occurring disease management strategies. This is particularly challenging when peer support occurs as part of a robust, resource-intensive self-management program. A systematic review of internet-based peer support interventions across conditions, for example, was unable to draw any meaningful conclusions on the effect of web-based peer support interventions.59 In this review we have attempted to highlight the potential impact of direct peer support interventions, but heterogeneity in peer support intervention, study design, level of peer mentor training and education, and outcomes measured limited the conclusions we could draw about many of the interventions.
The studies of peer support interventions in RA and SLE included in this review are limited by the specific outcomes assessed, selection bias of patients willing to participate, and relatively short follow-up periods—all of which can hinder our ability to detect the true impact of peer support interventions in these conditions. The patients with RA who participated in the studies in this review represent a homogenous patient population of older, white women. The lack of signal for peer support interventions impacting disease activity or medication adherence may illustrate that this particular patient population is less likely to benefit in these domains or that these outcomes to not capture the benefits conferred by peer support. Alternatively, the potential benefits of peer support in this group may require a longer time scale—months to years, rather than days to weeks—before they appear. Conversely, most of the data we reviewed on peer support in SLE emerges from a single cohort of African American patients. While the data is impressive, the patients in these studies may represent a more vulnerable patient-population relative to the studies involving people with RA and may not be generalizable to all patients with SLE. Peer support has been posited to be particularly beneficial intervention for African American patients with SLE.9 However, it is important to note that available data suggest benefits in the short term; the durability of this response over time remains unknown.
Much of the data in this review focuses on patient and provider perspectives, though some studies do highlight significant findings with respect to peer mentors themselves. While providing peer support can be a source of empowerment for mentors, it may also carry some risk—particularly when mentors themselves constitute a vulnerable patient populating trying to cope with a chronic disease.46 Prior qualitative reviews of peer support interventions have similarly highlighted the need to be vigilant for any negative effects from these interventions, including the potential impact on both mentors and mentees.14 Understanding not only the impact of peer support interventions on patients but also potential unintended consequences to mentors is therefore a high priority for future work.
Conclusion
The literature on peer support in rheumatic diseases is still nascent and the variability in peer support interventions make it challenging to fully evaluate their efficacy or draw comparisons across studies. Future studies should aim to clearly define the intervention, characterize the study population, and identify a minimum set of outcomes, including measures of self-efficacy, shared decision making, and patient satisfaction. To date it has been difficult to detect measurable differences in outcomes, though patients living with rheumatic diseases generally view peer support as a favorable and necessary tool for helping manage their conditions. In addition to perceived benefits to patients, the limited available data suggests that direct peer support may improve self-management skills in patients with RA and help reduce psychological stress in patients with SLE (along with potential cost savings to the healthcare system). The internet will increasingly be utilized as a venue for providing both synchronous and asynchronous peer support, but it should not necessarily supplant more conventional modalities, including telephone and in-person applications. Peer support interventions have the potential to serve as an accessible and dynamic resource for patients with rheumatic diseases, but future studies must attempt to quantify their benefits to justify more wide-spread use.
Disclosure
Dr Jinoos Yazdany reports grants from Aurinia, Gilead, Astra Zeneca; personal fees from AbbVie, outside the submitted work. The authors report no other conflicts of interest relevant to this work.
References
1. Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising?: results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010;62(6):1576–1582. doi:10.1002/art.27425
2. Hunter TM, Boytsov NN, Zhang X, Schroeder K, Michaud K, Araujo AB. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004-2014. Rheumatol Int. 2017;37(9):1551–1557. doi:10.1007/s00296-017-3726-1
3. Birnbaum H, Pike C, Kaufman R, Maynchenko M, Kidolezi Y, Cifaldi M. Societal cost of rheumatoid arthritis patients in the US. Curr Med Res Opin. 2010;26(1):77–90. doi:10.1185/03007990903422307
4. Barber MRW, Clarke AE. Socioeconomic consequences of systemic lupus erythematosus. Curr Opin Rheumatol. 2017;29(5):480–485. doi:10.1097/BOR.0000000000000416
5. Murimi-Worstell IB, Lin DH, Kan H, et al. Healthcare Utilization and Costs of Systemic Lupus Erythematosus by Disease Severity in the United States. J Rheumatol. 2021;48(3):385–393. doi:10.3899/jrheum.191187
6. Carter EE, Barr SG, Clarke AE. The global burden of SLE: prevalence, health disparities and socioeconomic impact. Nat Rev Rheumatol. 2016;12(10):605–620. doi:10.1038/nrrheum.2016.137
7. Griffith J, Carr A. What is the impact of early rheumatoid arthritis on the individual? Best Pract Res Clin Rheumatol. 2001;15(1):77–90. doi:10.1053/berh.2000.0127
8. Radford S, Carr M, Hehir M, et al. “It’s quite hard to grasp the enormity of it”: perceived needs of people upon diagnosis of rheumatoid arthritis. Musculoskeletal Care. 2008;6(3):155–167. doi:10.1002/msc.132
9. Williams EM, Egede L, Faith T, Oates J. Effective Self-Management Interventions for Patients With Lupus: potential Impact of Peer Mentoring. Am J Med Sci. 2017;353(6):580–592. doi:10.1016/j.amjms.2017.01.011
10. Bachen EA, Chesney MA, Criswell LA. Prevalence of mood and anxiety disorders in women with systemic lupus erythematosus. Arthritis Rheum. 2009;61(6):822–829. doi:10.1002/art.24519
11. Nikiphorou E, Santos EJF, Marques A, et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann Rheum Dis. 2021;80(10):1278–1285. doi:10.1136/annrheumdis-2021-220249
12. Iversen MD, Hammond A, Betteridge N. Self-management of rheumatic diseases: state of the art and future perspectives. Ann Rheum Dis. 2010;69(6):955–963. doi:10.1136/ard.2010.129270
13. Dennis CL. Peer support within a health care context: a concept analysis. Int J Nurs Stud. 2003;40(3):321–332. doi:10.1016/s0020-7489(02)00092-5
14. Embuldeniya G, Veinot P, Bell E, et al. The experience and impact of chronic disease peer support interventions: a qualitative synthesis. Patient Educ Couns. 2013;92(1):3–12. doi:10.1016/j.pec.2013.02.002
15. Thompson D. Peer support for people with chronic conditions: a systematic review of reviews. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-07816-7
16. Morisky DE, Ang A, Coly A, Tiglao TV. A model HIV/AIDS risk reduction programme in the Philippines: a comprehensive community-based approach through participatory action research. Health Promot Int. 2004;19(1):69–76. doi:10.1093/heapro/dah109
17. Keyserling TC, Samuel-Hodge CD, Ammerman AS, et al. A randomized trial of an intervention to improve self-care behaviors of African-American women with type 2 diabetes: impact on physical activity. Diabetes Care. 2002;25(9):1576–1583. doi:10.2337/diacare.25.9.1576
18. Elliott MJ, Love S, Fox DE, et al. ’It’s the empathy’-defining a role for peer support among people living with chronic kidney disease: a qualitative study. BMJ Open. 2022;12(5):e057518. doi:10.1136/bmjopen-2021-057518
19. Ghahramani N. Potential impact of peer mentoring on treatment choice in patients with chronic kidney disease: a review. Arch Iran Med. 2015;18(4):239–243.
20. Brownson CA, Heisler M. The role of peer support in diabetes care and self-management. Patient. 2009;2(1):5–17. doi:10.2165/01312067-200902010-00002
21. Helgeson VS, Cohen S, Schulz R, Yasko J. Group support interventions for women with breast cancer: who benefits from what? Health Psychol off J Div Health Psychol Am Psychol Assoc. 2000;19(2):107–114. doi:10.1037//0278-6133.19.2.107
22. Helgeson VS, Cohen S, Schulz R, Yasko J. Long-term effects of educational and peer discussion group interventions on adjustment to breast cancer. Health Psychol off J Div Health Psychol Am Psychol Assoc. 2001;20(5):387–392. doi:10.1037//0278-6133.20.5.387
23. Lorig K, Lubeck D, Kraines RG, Seleznick M, Holman HR. Outcomes of self-help education for patients with arthritis. Arthritis Rheum. 1985;28(6):680–685. doi:10.1002/art.1780280612
24. Lorig K, Ritter PL, Plant K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients. Arthritis Care Res. 2005;53(6):950–957. doi:10.1002/art.21604
25. Kruger JMS, Helmick CG, Callahan LF, Haddix AC. Cost-effectiveness of the Arthritis Self-Help Course. Arch Intern Med. 1998;158(11):1245–1249. doi:10.1001/archinte.158.11.1245
26. Berland GK, Elliott MN, Morales LS, et al. Health Information on the Internet: accessibility, Quality, and Readability in English and Spanish. JAMA. 2001;285(20):2612–2621. doi:10.1001/jama.285.20.2612
27. Hadert A, Rodham K. The invisible reality of arthritis: a qualitative analysis of an online message board. Musculoskeletal Care. 2008;6(3):181–196. doi:10.1002/msc.131
28. Shigaki CL, Smarr KL, Gong Y, et al. Social interactions in an online self-management program for rheumatoid arthritis. Chronic Illn. 2008;4(4):239–246. doi:10.1177/1742395308097862
29. Sandhu S, Veinot P, Embuldeniya G, et al. Peer-to-peer mentoring for individuals with early inflammatory arthritis: feasibility pilot. BMJ Open. 2013;3(3):e002267. doi:10.1136/bmjopen-2012-002267
30. McCarron A. An exploration of the perceived effects of a support group for individuals with rheumatoid arthritis. J Am Assoc Nurse Pract. 2015;27(3):160–166. doi:10.1002/2327-6924.12146
31. Shadick NA, Zibit MJ, Iannaccone CK, et al. A Development and Feasibility Study of a Peer Support Telephone Program in Rheumatoid Arthritis. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis. 2018;24(6):346–349. doi:10.1097/RHU.0000000000000661
32. Des Bordes JKA, Foreman J, Westrich-Robertson T, et al. Interactions and Perceptions of Patients with Rheumatoid Arthritis Participating in an Online Support Group. Clin Rheumatol. 2020;39(6):1775–1782. doi:10.1007/s10067-020-04967-y
33. Lopez-Olivo MA, Foreman JT, Leung C, et al. A randomized controlled trial evaluating the effects of social networking on chronic disease management in rheumatoid arthritis. Semin Arthritis Rheum. 2022;56:152072. doi:10.1016/j.semarthrit.2022.152072
34. Kaya T, Goksel Karatepe A, Atici Ozturk P, Gunaydin R. Impact of peer-led group education on the quality of life in patients with ankylosing spondylitis. Int J Rheum Dis. 2016;19(2):184–191. doi:10.1111/1756-185X.12256
35. Kaya T, Atıcı P, Karatepe AG, Günaydın R. Peer-led education or booklet for knowledge transfer about disease: a randomized-controlled trial with ankylosing spondylitis patients. Arch Rheumatol. 2021;36(4):560–569. doi:10.46497/ArchRheumatol.2021.8334
36. Withall J, Haase AM, Walsh NE, Young A, Cramp F. Physical activity engagement in early rheumatoid arthritis: a qualitative study to inform intervention development. Physiotherapy. 2016;102(3):264–271. doi:10.1016/j.physio.2015.07.002
37. Dures E, Almeida C, Caesley J, et al. Patient preferences for psychological support in inflammatory arthritis: a multicentre survey. Ann Rheum Dis. 2016;75(1):142–147. doi:10.1136/annrheumdis-2014-205636
38. Des Bordes JKA, Gonzalez E, Lopez-Olivo MA, Shethia M, Nayak P, Suarez-Almazor ME. Assessing information needs and use of online resources for disease self-management in patients with rheumatoid arthritis: a qualitative study. Clin Rheumatol. 2018;37(7):1791–1797. doi:10.1007/s10067-018-4047-9
39. Navarro-Millán I, Zinski A, Shurbaji S, et al. Perspectives of Rheumatoid Arthritis Patients on Electronic Communication and Patient-Reported Outcome Data Collection: a Qualitative Study. Arthritis Care Res. 2019;71(1):80–87. doi:10.1002/acr.23580
40. Loyola-Sanchez A, Pelaez-Ballestas I, Crowshoe L, et al. “There are still a lot of things that I need”: a qualitative study exploring opportunities to improve the health services of First Nations People with arthritis seen at an on-reserve outreach rheumatology clinic. BMC Health Serv Res. 2020;20(1):1076. doi:10.1186/s12913-020-05909-9
41. Swärdh E, Nordgren B, Opava CH, Demmelmaier I. “A Necessary Investment in Future Health”: perceptions of Physical Activity Maintenance Among People With Rheumatoid Arthritis. Phys Ther. 2020;100(12):2144–2153. doi:10.1093/ptj/pzaa176
42. Van der Elst K, De Cock D, Bangels L, et al. “More than just chitchat”: a qualitative study concerning the need and potential format of a peer mentor programme for patients with early rheumatoid arthritis. RMD Open. 2021;7(3):e001795. doi:10.1136/rmdopen-2021-001795
43. Feldman C, Bermas B, Zibit M, et al. Designing an intervention for women with systemic lupus erythematosus from medically underserved areas to improve care: a qualitative study. Lupus. 2013;22(1):52–62. doi:10.1177/0961203312463979
44. Toral P, Flores MT, Horton R, Rose J Evaluation of a Longstanding Telephone Peer Counseling Service on People with Systemic Lupus Erythematosus and Their Loved Ones. ACR Meeting Abstracts. Available from: https://acrabstracts.org/abstract/evaluation-of-a-longstanding-telephone-peer-counseling-service-on-people-with-systemic-lupus-erythematosus-and-their-loved-ones/.
45. Williams EM, Hyer JM, Viswanathan R, et al. Peer-to-Peer Mentoring for African American Women With Lupus: a Feasibility Pilot. Arthritis Care Res. 2018;70(6):908–917. doi:10.1002/acr.23412
46. Faith TD, Egede L, Williams EM. Research Ethics in Behavioral Interventions Among Special Populations: lessons From the Peer Approaches to Lupus Self-Management Study. Am J Med Sci. 2018;355(2):104–112. doi:10.1016/j.amjms.2017.08.021
47. Flournoy-Floyd M, Ortiz K, Egede L, Oates JC, Faith TD, Williams EM. “We Would Still Find Things to Talk About”: assessment of Mentor Perspectives in a Systemic Lupus Erythematosus Intervention to Improve Disease Self-Management, Empowering SLE Patients. J Natl Med Assoc. 2018;110(2):182–189. doi:10.1016/j.jnma.2017.05.003
48. Williams EM, Dismuke CL, Faith TD, et al. Cost-effectiveness of a peer mentoring intervention to improve disease self-management practices and self-efficacy among African American women with systemic lupus erythematosus: analysis of the Peer Approaches to Lupus Self-management (PALS) pilot study. Lupus. 2019;28(8):937–944. doi:10.1177/0961203319851559
49. White A, Faith TD, Ba A, et al. Support Methodologies for African American Women With Lupus – comparing Three Methods’ Effects on Patient Activation and Coping. Front Psychol. 2021;12:734390. doi:10.3389/fpsyg.2021.734390
50. Alexander DS, Hogan SL, Jordan JM, Devellis RF, Carpenter DM. The relationship between peer support, medication adherence, and quality of life among patients with vasculitis. Clin Exp Rheumatol. 2015;33(2 Suppl 89):S1856.
51. Mendelson C, Poole JL. Become your own advocate: advice from women living with scleroderma. Disabil Rehabil. 2007;29(19):1492–1501. doi:10.1080/09638280601029480
52. van der Vaart R, Repping-Wuts H, Drossaert CHC, Taal E, Knaapen-Hans HKA, van de Laar MAFJ. Need for online information and support of patients with systemic sclerosis. Arthritis Care Res. 2013;65(4):594–600. doi:10.1002/acr.21875
53. Delisle VC, Gumuchian ST, El-Baalbaki G, et al. Training and support needs of scleroderma support group facilitators: the North American Scleroderma Support Group Facilitators Survey. Disabil Rehabil. 2019;41(20):2477–2482. doi:10.1080/09638288.2018.1467970
54. Pépin M, Kwakkenbos L, Carrier ME, et al. Reasons for attending support groups and organizational preferences: a replication study using the North American Scleroderma Support Group Survey. J Scleroderma Relat Disord. 2019;4(3):173–186. doi:10.1177/2397198319849806
55. Gumuchian ST, Delisle VC, Kwakkenbos L, et al. Reasons for attending support groups and organizational preferences: the European scleroderma support group members survey. Disabil Rehabil. 2019;41(8):974–982. doi:10.1080/09638288.2017.1416497
56. Kwakkenbos L, Carboni-Jiménez A, Carrier ME, et al. Reasons for not participating in scleroderma patient support groups: a comparison of results from the North American and European scleroderma support group surveys. Disabil Rehabil. 2021;43(9):1279–1286. doi:10.1080/09638288.2019.1656292
57. Delisle VC, Gumuchian ST, Pelaez S, et al. Reasons for non-participation in scleroderma support groups. Clin Exp Rheumatol. 2016;34 Suppl 100(5):56–62.
58. Heisler M. Building Peer Support Programs to Manage Chronic Disease: seven Models for Success. California Health Care Foundation. 2006:67.
59. Eysenbach G, Powell J, Englesakis M, Rizo C, Stern A. Health related virtual communities and electronic support groups: systematic review of the effects of online peer to peer interactions. BMJ. 2004;328(7449):1166. doi:10.1136/bmj.328.7449.1166
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.