Back to Journals » Advances in Medical Education and Practice » Volume 14
Peer Role-Play Simulation: A Valuable Alternative to Bedside Teaching During the COVID-19 Pandemic
Authors Elhilu AH ![]() , El-Setouhy M
, El-Setouhy M ![]() , Mobarki AS, Abualgasem MM
, Mobarki AS, Abualgasem MM ![]() , Ahmed MA
, Ahmed MA
Received 13 December 2022
Accepted for publication 7 March 2023
Published 22 March 2023 Volume 2023:14 Pages 257—264
DOI https://doi.org/10.2147/AMEP.S399531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abdelkhalig Hussein Elhilu,1 Maged El-Setouhy,2 Ali Sadeiq Mobarki,2 Mohammed Maki Abualgasem,2 Mohammed Ageel Ahmed1
1Department of Surgery, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia
Correspondence: Abdelkhalig Hussein Elhilu, Tel +966531514032, Email [email protected]; [email protected]
Purpose: The COVID-19 pandemic dramatically affected every aspect of life worldwide. Contact restrictions and social distancing during the epidemic has led to the suspension of bedside teaching (BST) and shifting to online didactic teaching and other methods of active learning. We implemented peer role-play simulation (PRPS) during the pandemic to compensate for the suspended BST. This study aims to explore the effectiveness of PRPS in developing the students’ verbal communication, empathy and clinical reasoning skills compared to BST.
Methods: This is a cross-sectional observational study conducted in Jazan University faculty of medicine with the study sample including all medical students enrolled in 5th and 6th year during the academic year 2020– 21. Data collection involved using a web-based validated questionnaire.
Results: Most of the students (84.1%) rated bedside teaching (BST) as extremely beneficial or beneficial in developing verbal communication skills compared to 73.3% for peer role-play simulation (PRPS). A similar pattern was found in empathy skills development with 84.1% for bedside compared to 72.2% for PRPS. The pattern is reversed with the development of clinical reasoning skills with 77.7% rating BST as beneficial or extremely beneficial compared to 81.2% for PRPS.
Conclusion: Overall, peer role-play is generally a valuable and trustworthy method in the absence of bedside teaching for enhancing clinical reasoning skills of medical students during the COVID-19 pandemic from students’ perspective. It is less efficient than bedside teaching in enhancing communication skills. It cannot wholly replace bedside teaching, although it can be used reliably for that purpose in exceptional circumstances when bedside teaching cannot be implemented.
Keywords: bedside teaching, clinical reasoning, empathy, medical education, peer role-play, verbal communication skills
Introduction
Reform initiatives in medical and health care education curricula during the previous decade have placed a strong emphasis on the use of technology and active learning in raising student engagement and developing their critical thinking abilities.1 According to Bonwell and Elison, active learning is “anything that involves students in doing things and thinking about what they are doing”.2 Active learning strategies include simulations, demonstrations, experiments, debates, role-playing, small group discussions, creating visual representations and models, problem solving, research and presentations, case studies and games.3 Peer role-playing is a simulation-based training method in which medical students take turns playing the roles of patient and clinician.4 Kiger describes role-playing as an experiential learning strategy where students take on different roles in case scenarios and receive feedback to help them refine their skills.5 Role-play training’s instructional goal is to practice scenarios to help learners become more adept at handling similar problems in clinical practice.6 It is a potent intervention that has the potential to improve learners’ cognitive, psychomotor, and affective domains.7 Learning in a real clinical setting, on the other hand, has numerous advantages. It concentrates on actual issues that arise in the course of professional practice. It is the only setting in which the abilities of taking a history, performing a physical examination, using clinical reasoning to make decisions, behaving empathetically, and being professional can be taught and acquired as a cohesive whole.8 “Medicine is learned by the bedside not in the classroom” is one of the famous quotes of Sir William Osler.9 Real patients provide the advantage of genuineness, according to students.10 However, some studies noted a declining interest in bedside teaching.11–13 One reason for this decline is that other methods of active learning have steadily crept into medical curricula at the expense of BST in the students’ timetables. Other explanations for this drop include the rise in hospital patient turnover, perceived patient privacy violations, and a greater dependence on technology during the process of diagnosis.14
The COVID-19 pandemic dramatically affected every aspect of life worldwide. The WHO, UNICEF, and the International Federation of Red Cross and Red Crescent Societies (IFRC) published guidelines on March 10, 2020 that highlight crucial elements and practical checklists to keep schools secure. The guidelines offer guidance for both children and students as well as their parents and caregivers. The next day, the WHO determined that COVID-19 could be considered a pandemic.15 Curfews and social distancing were enforced by the countries all over the world. The pandemic’s effects on preclerkship education have mostly been mitigated by incorporating online and videoconferencing-based didactics that enable students to complete learning objectives remotely.16 Following an initial declaration of school closures and the suspension of teaching at universities and other institutions, with an immediate shift to online virtual learning, Saudi authorities unveiled a mechanism for restarting the new school year 2020/2021 through distance learning programs in all schools while adhering to health instructions and maintaining social distancing.17–19 While bedside teaching remained suspended, on campus practical simulation sessions using small groups were allowed in medical schools with strict health safety protocols. In our institute, we used on-campus peer role-play simulation sessions with small groups of students to promote verbal communication, empathy, and clinical reasoning skills, in addition to practical sessions using mannequins to develop and hone the essential clinical examination skills during the pandemic.
Despite the huge challenges faced in this epidemic, COVID-19 has provided a unique opportunity to assess the efficiency of other methods of active learning in the absence of BST and clinical encounters. This study aims to evaluate PRPS in achieving certain educational outcomes namely, verbal communication skills, empathy and critical thinking skills from the students’ perspective in comparison to the participants’ previous pre-COVID-19 experience with BST.
Materials and Methods
We created a cross-sectional study, using web-based validated anonymous self-reported questionnaire. The target population of the study included all students enrolled in fifth and six year (penultimate and final clinical year) at the Faculty of Medicine, Jazan University during the academic year 2020–21. In order to make up for the pandemic-related suspension of bedside teaching, peer role-play simulation was adopted as an alternative method of teaching in the general surgery, pediatrics, and obstetric modules. Each class was divided into groups of eight to ten students, with a tutor supervising each group. The sessions were conducted following the sequence of preparation, interaction, and discussion. During preparation, the roles of the students are outlined, the setting is prepared, and the context is explained. This is followed by the allocation of roles and handing over the detailed clinical scenarios to the students who are going to play the patient role. The students are then given time to assimilate the case details before the beginning of the interaction which proceeds in similar way to traditional bedside encounters. The session is concluded with the discussion and feedback with participation of the entire group. There was a total of 68 peer-role play sessions with 33 of them in 5th year and 35 sessions in 6th year. All the participants in this study have prior experience with bedside teaching, which was the norm in the previous academic year and before the COVID-19 pandemic rocked the world. We excluded 4th year clinical students from the study because they had no prior experience with bedside teaching. We asked the participants to express their opinions on whether PRPS and BST were beneficial in achieving three educational learning outcomes, namely, verbal communication skills, empathy and critical thinking skills. A 4-point Likert scale was used for this purpose with 1= of no benefit, 2= of little benefit, 3= beneficial and 4= extremely beneficial. The demographic section of the questionnaire covered gender, age and the student level (5th or 6th year).
Data Management and Analysis
We used descriptive and inferential statistics. The data analysis was performed using IBM SPSS statistics software (version 23.0). A P-value of 0.05 or less was used as the cutoff level for statistical significance. First, we tested the reliability of the questionnaire using Cronbach’s alpha. The PRPS scale has a reliability statistic of 0.776, while the BST scale has a reliability statistic of 0.761. This provides evidence that both of these measures can be relied upon for inclusion in any subsequent statistical analysis. Then, we used principle component analysis (PCA) in order to investigate the validity of the dataset of the PRPS and BST scales. According to the component matrix, one factor was extracted from both scales, along with their respective three items. The PRPS scale was found to have an explained variance of 62.82%, while the BST scale has an explained variance of 59.78%. We used the KMO measure of sampling adequacy to assess the appropriateness of factor analysis on the data set. The KMO values for the PRPS and BST scales were 0.78 and 0.69, respectively, indicating that factor analysis was appropriate for our data. The outputs of the component matrices for both scales revealed a loading factor ranging from 0.66 to 0.86 indicating constructs validity.
Results
One hundred seventy-six from the target group responded to the questionnaire (83%). Around 54% of the respondents were males, while (46%) were females (Table 1). Both BST and PRPS were compared across demographic parameters (gender, age, and level) using Mann–Whitney U-test. The BST index rate was not significantly different across any of the studied demographics. Only gender made a difference in PRPS index, with female respondents showing a higher mean than males (Table 2).
 |
Table 1 Background Characteristics of the Study Population |
 |
Table 2 Role of Demographic Characteristics on BST and PRPS Indices |
Verbal Communication
The participants were asked to rate the benefit of BST and PRPS in developing their verbal communication skills from their experience with the two methods of teaching. As can be seen from the data in Figure 1 the vast majority of students rate BST as extremely beneficial or beneficial (36.9%, 47.2% respectively a total sum of 84.1%). The response to the same question regarding PRPS showed 26.7% and 46.6% rating it as extremely beneficial and beneficial respectively (total sum 73.3%). A quarter of the students, see PRPS as of no benefit or of little benefit (26.7%) in developing their communication skills in contrast to 15.9% for BST. A Wilcoxon signed-rank test showed that at the level 0.05 of significance the rating for BST towards beneficial is significantly more than the rating for PRPS in developing verbal communication skills (Z = −2.866, P-value =0.004).
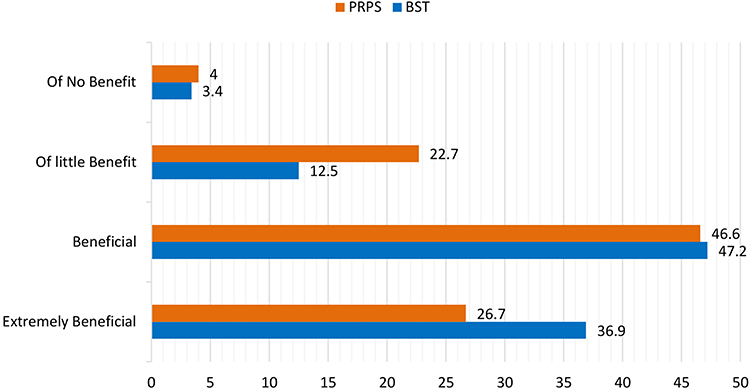 |
Figure 1 Benefit in developing the skills of verbal communication. |
Empathy
The second question was about the development of empathy skills. Figure 2 depicts the details of the participants’ responses. 39.8% rated BST as extremely beneficial and 44.3% as beneficial. Corresponding percentages for PRPS were 25.6% and 46.6% for extremely beneficial and beneficial respectively. Also slightly more than a quarter of the participants see PRPS as of no benefit or of little benefit (27.9%) in developing their empathy skills compared to 15.9% for BST. Interestingly the pattern is similar to the pattern of verbal communication with statistically significant difference in favor of BST (Z = −3.131, P-value =0.002).
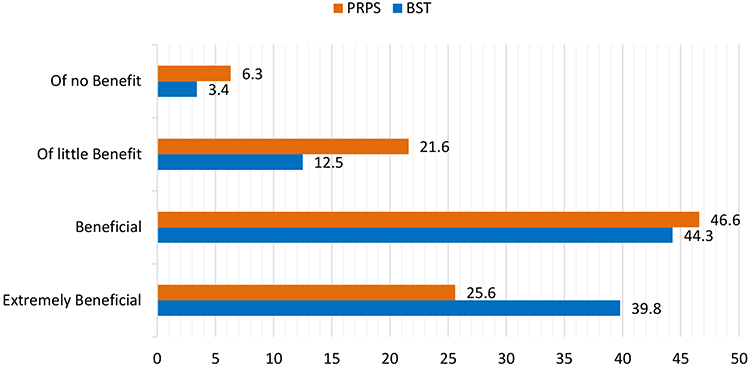 |
Figure 2 Benefit in developing the empathy skills. |
Clinical Reasoning Skills
When asked to rate the benefit of BST and PRPS in developing their skills of clinical reasoning, 30.1% of the participants rated BST as extremely beneficial while 47.7% rated it as beneficial. PRPS is rated to be extremely beneficial by 29.5% of the participants while 51.7% rated it as beneficial. 17% see BST as of little benefit while 5.1% see it as of no benefit. PRPS is seen as of little benefit by 17% of the participants while only 1.7% see it as of no benefit in achieving clinical reasoning skills (Figure 3). There is no significant statistical difference between BST and PRPS in achieving of the clinical reasoning skills (Z = −0.641, P-value = 0.522).
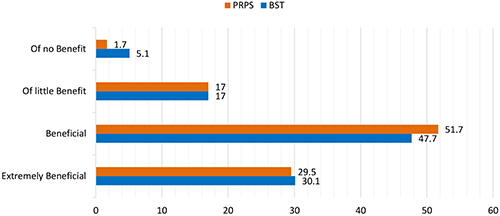 |
Figure 3 Benefit in developing the skills of clinical reasoning. |
Discussion
The suspension of clinical placements and bedside teaching was one of the most significant challenges to medical education during the COVID-19 pandemic. Many innovative teaching methods were used during the pandemic to compensate for the absence of clinical encounters. Online bank of patient interviews and interactive cases, video-conferencing or telephone interviews, telemedicine, virtual consultations with simulated patients, virtual bedside tutorials, and virtual ward rounds are among the many teaching formats utilized during the COVID-19 pandemic.20–23 Most of the studies claimed success with these formats of teaching. However, the principal weaknesses of virtual teaching methods are the technical difficulties and the loss of face-to-face teaching.24 During the pandemic, we substituted the PRPS method for the BST, and the goal of this study was to assess how well PRPS promoted verbal communication, empathy, and clinical reasoning skills as compared to BST.
In medicine, communication skills cover a wide range of competencies, such as information collection, relationship-building, empathetic behavior, and/or planning and explanation.25 The way and extent to which communication skills are taught and assessed varies greatly between medical schools.26 Students appeared to prefer hands-on methods of learning communication skills, such as role-playing with simulated patients and interacting with real patients in a clinical setting.27 Verbal communication and empathy are the two aspects of communication skills, which we targeted in this study. Verbal communication is defined as the human interaction through the use of words, or messages in linguistic form.28 It incorporates the appropriate choice of words and relevant tone in addition to active listening.29 Empathy, on the other hand, is a type of disciplined caring in which patients perceive their doctor’s consistent, professional concern for their feelings.30 It has a cognitive component that entails being aware of, cognizant and respectful of the patient’s worries and anxieties without joining and sharing in the feeling of their suffering.31 Our results show that both PRPS and BST are efficient in developing verbal communication skills. BST appears superior to PRPS in this respect with statistically significant difference (P-value =0.004) (Figure 1). A similar pattern was detected in empathy development (P-value =0.002) (Figure 2). Some studies attribute this trend to the realism of BST compared to the artificial nature and lack of authenticity associated with simulation-based medical education methods.4,32,33 Mansfield highlighted the students’ initial resistance to participating in role-plays through shyness and fear of exposure as a disadvantage that may face the trainers.34 In addition, the patient-centered approach and the increased learners’ motivation provided by BST makes it outstanding and provides the learners’ with more excitement, as noted by Asani.35
Clinical reasoning is the methodical, analytical, scientific approach that considers all pertinent data in the search for the most appropriate course of treatment and diagnosis for any given patient.36 Different approaches to teaching clinical reasoning may benefit students at various stages of their training.37 The best strategy to begin clinical training for junior medical students is to teach clinical reasoning in a systematic manner with an emphasis on creating an accurate and thorough differential diagnosis.38 The most effective way to accomplish this seems to be to have students prepare and present a case in a small group setting under the supervision of a clinical tutor.38 Activities that improve memory retention, clinical experience, and opportunities to exercise reasoning in actual or simulated clinical settings are all necessary for the development of analytical and non-analytical clinical reasoning skills.39 The majority of the participants in our sample think that both bedside teaching and peer role-play are either extremely beneficial or beneficial in developing their clinical reasoning skills. There is no statistically significant difference between the two methods (P-value = 0.522). The fact that peer role-play simulation sessions can be structured and customized, allowing the possibility to cover a larger and more diverse number of clinical scenarios makes it a useful method for promoting clinical reasoning skills. During role-play sessions, the students’ groups can be uniformly exposed to the same clinical scenarios, insuring homogeneity. On the other hand, patient experience is crucial for forging new links in memory between taught materials and clinical presentations, for creating illness scripts, and for honing the capacity to reason flexibly by using analytic reasoning and pattern recognition.40
The gender difference in the PRPS index (Table 2) can be explained by a possible difference in the setting, as female and male campuses are separate.
Limitations
This study’s findings would have been more generalizable if it had included multiple institutions. Furthermore, the study did not address additional outcome measurements, such as student evaluation outcomes compared to previous cohorts, and this should be considered when interpreting the findings.
Conclusion
Overall, peer role-play is generally a valuable and trustworthy method in the absence of bedside teaching for enhancing clinical reasoning skills of medical students during the COVID-19 pandemic from students’ perspective. It is less efficient than bedside teaching in enhancing communication skills. It cannot wholly replace bedside teaching, although it can be used reliably for that purpose in exceptional circumstances when bedside teaching cannot be implemented.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available upon reasonable request from the corresponding author.
Ethics Approval and Informed Consent
We obtained ethical approval for this study from the Scientific Research Ethics Committee - Jazan University (Reference No.: REC-43/02/002). Participation was voluntary, the anonymity of participants was emphasized, and confidentiality was strictly maintained on all collected questionnaires. All participants provided informed consent.
Acknowledgment
The authors would like to thank everyone who participated in the survey, as well as Dr. Siddig Ibrahim Abdelwahab for his insightful comments and suggestions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific funding from public, commercial, or non-profit funding agencies.
Disclosure
The authors report no competing interest in this work.
References
1. McCoy L, Pettit RK, Kellar C, Morgan C. Tracking active learning in the medical school curriculum: a learning-centered approach. J Med Educ Curric Dev. 2018;5:2382120518765135. doi:10.1177/2382120518765135
2. Bonwell CC, Eison JA. Active learning: creating excitement in the classroom. 1991 ASHE-ERIC higher education reports. One Dupont Circle, Suite 630, Washington, DC 20036-1183: ERIC Clearinghouse on Higher Education, The George Washington University; 1991.
3. Kanthan R, Mills S. Active learning strategies in undergraduate medical education of pathology: a Saskatoon experience. J Int Assoc Med Sci Educ. 2005;15(20):12–18.
4. Gelis A, Cervello S, Rey R, et al. Peer role-play for training communication skills in medical students: a systematic review. Simul Healthc. 2020;15(2):106–111. doi:10.1097/SIH.0000000000000412
5. Kiger A. Teaching for Health. Elsevier Health Sciences; 2004.
6. Nestel D, Kelly M, Jolly B, Watson M. Healthcare Simulation Education: Evidence, Theory and Practice. John Wiley & Sons; 2017.
7. Manzoor I, Mukhtar F, Hashmi NR. Medical students’ perspective about role-plays as a teaching strategy in community medicine. J Coll Physicians Surg Pak. 2012;22(4):222–225.
8. Spencer J. Learning and teaching in the clinical environment. BMJ. 2003;326(7389):591–594. doi:10.1136/bmj.326.7389.591
9. Stone MJ. The wisdom of sir William Osler. Am J Cardiol. 1995;75(4):269–276. doi:10.1016/0002-9149(95)80034-P
10. Bokken L, Rethans JJ, Jöbsis Q, Duvivier R, Scherpbier A, van der Vleuten C. Instructiveness of real patients and simulated patients in undergraduate medical education: a randomized experiment. Acad Med. 2010;85(1):148–154. doi:10.1097/ACM.0b013e3181c48130
11. Garout M, Nuqali A, Alhazmi A, Almoallim H. Bedside teaching: an underutilized tool in medical education. Int J Med Educ. 2016;7:261. doi:10.5116/ijme.5780.bdba
12. Qureshi Z, Maxwell S. Has bedside teaching had its day? Adv Health Sci Educ. 2012;17(2):301–304. doi:10.1007/s10459-011-9308-1
13. Ahmed K. What is happening to bedside clinical teaching? Med Edu. 2002;36(12):1185–1188. doi:10.1046/j.1365-2923.2002.01372.x
14. Peters M, Ten Cate O. Bedside teaching in medical education: a literature review. Perspect Med Educ. 2014;3(2):76–88. doi:10.1007/S40037-013-0083-Y
15. Listing of WHO‘s response to covid-19. Available from: https://www.who.int/news/item/29-06-2020-covidtimeline.
16. Sukumar S, Zakaria A, Lai CJ, Sakumoto M, Khanna R, Choi N. Designing and implementing a novel virtual rounds curriculum for medical students’ internal medicine clerkship during the COVID-19 pandemic. MedEdPORTAL. 2021;17:11106. doi:10.15766/mep_2374-8265.11106
17. Yezli S, Khan A. COVID-19 social distancing in the Kingdom of Saudi Arabia: bold measures in the face of political, economic, social and religious challenges. Travel Med Infect Dis. 2020;37:101692. doi:10.1016/j.tmaid.2020.101692
18. The Kingdom of Saudi Arabia's experience in health preparedness and response to COVID-19 pandemic, Saudi Arabia Ministry of Health 2020.Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Documents/COVID-19-NATIONAL.pdf.
19. Saudi Arabia to apply distance learning for first seven weeks of new school year 2020–2021, Saudi Arabia Press Agency; 2020. Available from: https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2120909.
20. Monaghan AM. Medical teaching and assessment in the era of COVID-19. J Med Educ Curric Dev. 2020;7:2382120520965255. doi:10.1177/2382120520965255
21. Feeley A, Feeley I, Carroll A, Hehir DJ. Student acceptance of virtual bedside surgical tutorials during COVID-19; A randomized control trial. J Surg Res. 2022;270:261–265. doi:10.1016/j.jss.2021.09.029
22. Sani I, Hamza Y, Chedid Y, Amalendran J, Hamza N. Understanding the consequence of COVID-19 on undergraduate medical education: medical students’ perspective. Ann Med Surg. 2020;58:117–119. doi:10.1016/j.amsu.2020.08.045
23. Hofmann H, Harding C, Youm J, Wiechmann W. Virtual bedside teaching rounds with patients with COVID-19. Med Educ. 2020;54(10):959–960. doi:10.1111/medu.14223
24. Wilcha RJ. Effectiveness of virtual medical teaching during the COVID-19 crisis: systematic review. JMIR Med Educ. 2020;6(2):e20963. doi:10.2196/20963
25. Kurtz S, Silverman J, Draper J, van Dalen J, Platt FW. Teaching and Learning Communication Skills in Medicine. CRC press; 2017.
26. Hargie O, Dickson D, Boohan M, Hughes K. A survey of communication skills training in UK schools of medicine: present practices and prospective proposals. Med Edu. 1998;32(1):25–34. doi:10.1046/j.1365-2923.1998.00154.x
27. Rees C, Sheard C, McPherson A. Medical students’ views and experiences of methods of teaching and learning communication skills. Patient Educ Couns. 2004;54(1):119–121. doi:10.1016/S0738-3991(03)00196-4
28. Definition of verbal communication in the Oxford reference, Oxford University Press. Available from: https://www.oxfordreference.com/view/10.1093/oi/authority.20110803115457102.
29. Kee JW, Khoo HS, Lim I, Koh MY. Communication skills in patient-doctor interactions: learning from patient complaints. Health Prof Educ. 2018;4(2):97–106. doi:10.1016/j.hpe.2017.03.006
30. Dyche L. Interpersonal skill in medicine: the essential partner of verbal communication. J Gen Intern Med. 2007;22(7):1035–1039. doi:10.1007/s11606-007-0153-0
31. Han JL, Pappas TN. A review of empathy, its importance, and its teaching in surgical training. J Surg Educ. 2018;75(1):88–94. doi:10.1016/j.jsurg.2017.06.035
32. Narayanan V, Nair BR. The value of bedside teaching in undergraduate medical education: a literature review. Med Ed Publish. 2020;9(1):1.
33. Lane C, Rollnick S. The use of simulated patients and role-play in communication skills training: a review of the literature to August 2005. Patient Educ Couns. 2007;67(1–2):13–20. doi:10.1016/j.pec.2007.02.011
34. Mansfield F. Supervised role‐play in the teaching of the process of consultation. Med Edu. 1991;25(6):485–490. doi:10.1111/j.1365-2923.1991.tb00102.x
35. Asani M. Bedside teaching: an indispensable model of patient-centred teaching in undergraduate medical education. NJBCS. 2014;11(2):57. doi:10.4103/0331-8540.140305
36. Sniderman AD, LaChapelle KJ, Rachon NA, Furberg CD. The necessity for clinical reasoning in the era of evidence-based medicine. Mayo Clin Proc. 2013;88(10):1108–1114. doi:10.1016/j.mayocp.2013.07.012
37. Schmidt HG, Mamede S. How to improve the teaching of clinical reasoning: a narrative review and a proposal. Med Edu. 2015;49(10):961–973. doi:10.1111/medu.12775
38. Custers EJ. Training clinical reasoning: historical and theoretical background. Principles and practice of case-based clinical reasoning education; 2018.
39. Richmond A, Cooper N, Gay S, Atiomo W, Patel R. The student is key: a realist review of educational interventions to develop analytical and non‐analytical clinical reasoning ability. Med Edu. 2020;54(8):709–719. doi:10.1111/medu.14137
40. Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217–2225. doi:10.1056/NEJMra054782
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Commercial Learning Platforms in UK Undergraduate Medical Education: A Qualitative Study of Benefits, Limitations, and Integration

Phillips R, Coleman JJ
Advances in Medical Education and Practice 2025, 16:2191-2205
Published Date: 28 November 2025
AI Use for Medical Students: Impact on Clinical Skill Acquisition and Retention. A Systematic Review
Turney J, Young TM, Chauhan DR, Beeharry R, Mahmud M
Advances in Medical Education and Practice 2026, 17:583763
Published Date: 11 April 2026
When Clinical AI and Learner Reasoning Conflict: An Emerging Educational Blind Spot and a Framework for Pedagogical Response
Heslin SM
Advances in Medical Education and Practice 2026, 17:592114
Published Date: 7 May 2026
Teaching Jugular Venous Pressure (JVP) Ultrasound: Methods That Improved Medical Students’ Knowledge and Confidence in Performing JVP Assessment
Patel B, Montgomery MW, Callahan DG, Chen HX, Osman NY, Engel-Rebitzer E, Pelletier SR, Shields HM
Advances in Medical Education and Practice 2026, 17:599200
Published Date: 8 May 2026
Enhancing Cognitive Reflection in Medical Trainees and Physicians: An EBM–CBL–PBL Integrated Teaching Model
Chen X, Xu L, Xu M, Liu D, Yang F, Xu G, Feng Q, Yang H
Advances in Medical Education and Practice 2026, 17:607106
Published Date: 9 July 2026