Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Pediatricians’ Knowledge, Attitudes, and Therapeutic Approaches Regarding Diaper Dermatitis: A Common Condition with Many Different Practices
Authors Yildiz I ![]() , Kizilca O, Haksayar A, Hizli Demirkale Z
, Kizilca O, Haksayar A, Hizli Demirkale Z
Received 27 January 2023
Accepted for publication 23 March 2023
Published 5 April 2023 Volume 2023:16 Pages 901—910
DOI https://doi.org/10.2147/CCID.S405414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Ismail Yildiz,1 Ozgur Kizilca,2 Aysen Haksayar,2 Zeynep Hizli Demirkale3
1Department of Pediatrics, Faculty of Medicine, Yalova University, Yalova, Turkey; 2Department of Pediatrics, Faculty of Medicine, Tekirdağ Namık Kemal University, Tekirdağ, Turkey; 3Division of Pediatric Allergy and Immunology, Department of Pediatrics, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkey
Correspondence: Ismail Yildiz, Email [email protected]
Background: Diaper dermatitis is one of the most common skin diseases in early childhood. The prevalence of diaper dermatitis varies between 7% and 35% depending on population and age groups. There may be some differences among the pediatricians about treatment approaches to this common skin condition.
Aim: The purpose of this study is to evaluate the management strategies of pediatricians for diaper dermatitis.
Methods: The questionnaire-based cross-sectional study was conducted between September and December 2021. The questionnaire which contained 21 items aimed to investigate the approaches of pediatricians to diaper dermatitis treatment, follow-up and prevention strategies.
Results: A total of 217 pediatricians (59.4% female, median age 40.0 years) practicing in 32 different provinces of Turkey completed the questionnaire. The most preferred medical treatments in the first visit of children with diaper dermatitis, in respect of frequency, were zinc oxide, panthenol/dexpanthenol, and hamamelis virginiana extract (70.9%, 36.9%, 33.6% respectively). If there was no response to the first-line treatment in the control examination, the treatment was rearranged by adding an antifungal creams, topical low-potency corticosteroids, and/or high concentration zinc oxide creams (67.7%, 57.6%, 28.6%, respectively). Most cases were referred to a dermatologist if these treatments were not effective in the control visits of patients.
Conclusion: Although pediatricians often prefer topical barrier creams for the treatment of diaper dermatitis, options may change depending on the severity of the lesions or the treatment response to the first-line topical treatments.
Keywords: antifungal cream, diaper dermatitis, pediatrics, zinc oxide
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Djaafar has been published for this article.
Introduction
Newborns and infants have a different skin structure, composition, and function compared to adults.1 The stratum corneum, the outer layer of the epidermis is responsible for the skin barrier function, which protects against external irritants and chemicals and regulates the water loss. Infant skin is characterized by a thinner epidermal layer especially stratum corneum and smaller corneocytes.2 Their skin barrier function is less mature, resulting in higher water vapor loss and the absence of an acid mantle on the skin surface.3 This maturation process continues after birth, especially within first year of life, and more closely resembles adult skin in the second year of life.4,5 This immature skin structure and function of newborn and infant skin makes these age groups both more prone to dehydration and more vulnerable to various irritants, including baby wipes, inappropriate diapers, some chemicals including irritating/sensitizing topical products or pathogens.1
Diaper region dermatitis (diaper dermatitis) is defined as inflammations and/or eruptions in the diaper covered area which include the buttocks, perianal, genital, inner thighs, and waistline.6,7 The prevalence of diaper dermatitis varies between 7% and 35% depending on study population and age groups. Approximately 25% of babies in their first four weeks of life have diaper dermatitis, and it is most frequently seen between 9 and 12 months.7,8 It is one of the most common skin diseases in newborns and infants who are not able to control bladder or bowel movements which creates moist environment. A moist environment and defective skin barrier can cause some microorganisms to colonize and proliferate. Candida albicans is the most common cause of candidal superinfection. Less frequently, other pathogenic strains such as S. aureus and S. pyogenes should also be considered in the management of diaper dermatitis.
Determining the severity of the disease is the most crucial aspect of treating diaper dermatitis. Although some scoring scales have been developed for the assessment of the severity of diaper dermatitis, in clinical practice, the severity of diaper dermatitis can be classified as early, mild, moderate, or severe disease based on clinical findings.9,10 The early phase of the disease is characterized by scattered pinpoint erythematous papules. As the disease progresses from the mild to moderate phase, erythema with maceration becomes more prominent, and superficial erosions and discomfort may accompany it. Severe disease is characterized by punched-out lesions or erosions with elevated borders, pseudoverrucous eroded papules, and nodules. Early recognition of the clinical signs of infections is essential for the early treatment of diaper dermatitis. Candidiasis typically presents as fiery-red, sharply marginated patches with satellite papules and pustules. Bacterial superinfections can present in a variety of forms, such as superficial vesicles or bullae, erosions, follicular-based erythematous papules, and pustules.10 Consequently, treatment of diaper dermatitis may vary according to the clinical findings, duration of skin eruptions, accompanying secondary infections, and underlying conditions of the child. Topical barrier preparations (zinc oxide, lanolin, panthenol/dexpanthenol, etc.) for both treatment and prevention; low-potency corticosteroids for inflamed skin, topical antifungal agents (nystatin, clotrimazole, miconazole, ketoconazole, etc.) for candidal superinfection, and topical antibacterials like mupirocin for secondary bacterial infections are generally used for the treatment of diaper dermatitis.11 Some of the other diseases [i. eczematous diseases (contact dermatitis, infantile seborrheic dermatitis, infantile atopic dermatitis), ii. infantile psoriasis, iii. infestations/infections (scabies, candida, streptococci, staphylococci), iv. nutritional disease (acrodermatitis enteropathica), v. autoimmune diseases (lichen sclerosus, Kawasaki disease), vi. malignancy (Langerhans cell histiocytosis) and child abuse] should be strongly considered in the differential diagnosis of diaper dermatitis especially if there is no response to standard treatment.12
The prevention strategies include to protect the skin barrier, avoid harsh cleansing as much as possible, maintain skin surface dryness, and reduce the direct contact with urine and feces. General recommendations for both treatment and prevention are as follows: frequent diaper change, usage of new innovative disposable diapers which are manufactured absorbent and aeration materials, gently cleansing methods while changing the diaper and using barrier creams for minimizing the exposure of urine and feces.11,13
In this study, we aimed to evaluate the treatment, prevention and management strategies of pediatricians in diaper dermatitis which is one of the most common skin eruptions of early childhood.
Materials and Methods
Questionnaire and Collection of Data
A questionnaire-based cross-sectional study was conducted between September and December 2021. The questionnaire was prepared in Google Forms and sent a link to pediatricians. All participants were informed about the study and agreed to fill out the questionnaire.
The first part of the questionnaire inquired data about pediatricians’ demographic characteristics, treatment attitudes (first-line treatment preferences, follow-up visit schedule, alternative treatment options when the first-line treatments fail, time to refer patients to a dermatologist evaluation), and the opinions about when a family seeks medical advice from their pediatricians.
The second part was about pediatricians’ prevention strategies of diaper dermatitis. In this part, general recommendations about prevention of diaper dermatitis, diaper-free time after every diaper change, type of preferred topical barrier preparations and frequency of application of these products, cleaning and drying suggestions of diaper area, diaper change frequencies per day, and diaper tying methods were questioned. Furthermore, opinions about educating caregivers of children and feeding choice during diaper dermatitis were also assessed.
The participants were classified into three groups according to their academic ranks (practitioner vs academician [professor, associate professor, assistant professor]); their median experience lengths (less than 10 years vs more years); and their work settings (private practice vs affiliated with an institute).
Statistical Analysis of Data
Statistical analyses were performed with Jamovi Software 1.6 package program.14 Data were expressed as means with ± standard deviation or medians with 25th and 75th percentiles according to the distribution characteristics of variables. Chi-square test or Fisher’s exact test was used to compare categorical variables. A value of p <0.05 was considered statistically significant.
Ethical Approval
This study was approved by Tekirdağ Namık Kemal University’s Clinical Research Ethics Committee (2021.150.05.23). All participants were informed about the study and informed consent was obtained prior to the study commencement.
Results
Demographic Data
A total of 217 pediatricians in 32 different provinces of Turkey participated in the study. The median age of the pediatricians was 40 years (35–45) (minimum-maximum = 29–70 years) and 59.4% (n: 129) were female. The median duration of practicing as a pediatrician was 10 years (5–16 years).
Treatment of Diaper Dermatitis
Of the pediatricians, 42.9% recommended to visit a physician immediately or within 0–3 days when the family noticed the signs of diaper dermatitis. Topical application of moderate concentration of zinc oxide (20% and below), panthenol/dexpanthenol, and hamamelis virginiana extracts were the most preferred therapies respectively in the first visits of children with diaper dermatitis. Although the length of their experience as a pediatrician did not affect the choice of treatment preparations between the groups, practitioner pediatricians preferred hamamelis virginiana extract (p=0.043) and pediatricians who were affiliated with an institute preferred moderate concentration of zinc oxide (p=0.005) significantly higher than other groups. There was no statistically significant difference between all the groups in terms of other preparations in the treatment of diaper dermatitis. The follow-up visit was recommended within the first week after initial assessment. If there was no response to the first-line treatment in the next physical examination, the treatment was rearranged by adding an antifungal cream, low-potency corticosteroid, and high concentration of zinc oxide (above 20%) respectively. The usage of high concentration of zinc oxide (p=0.014) and anti-bacterial cream (p=0.013) in the patients who did not respond in the first-line therapy was significantly higher in pediatricians with less than a decade of experience. In addition, usage of antifungals in follow-up examination was significantly higher among private practice pediatricians (p=0.048). On the other hand, academic rank did not affect the choice of products in the treatment of patients who fail to respond to the first-line treatment (Table 1). Most of the participants (89.3%) referred to the patient who failed to respond to these treatments to a dermatologist in the follow-up evaluations (Table 2, Figure 1).
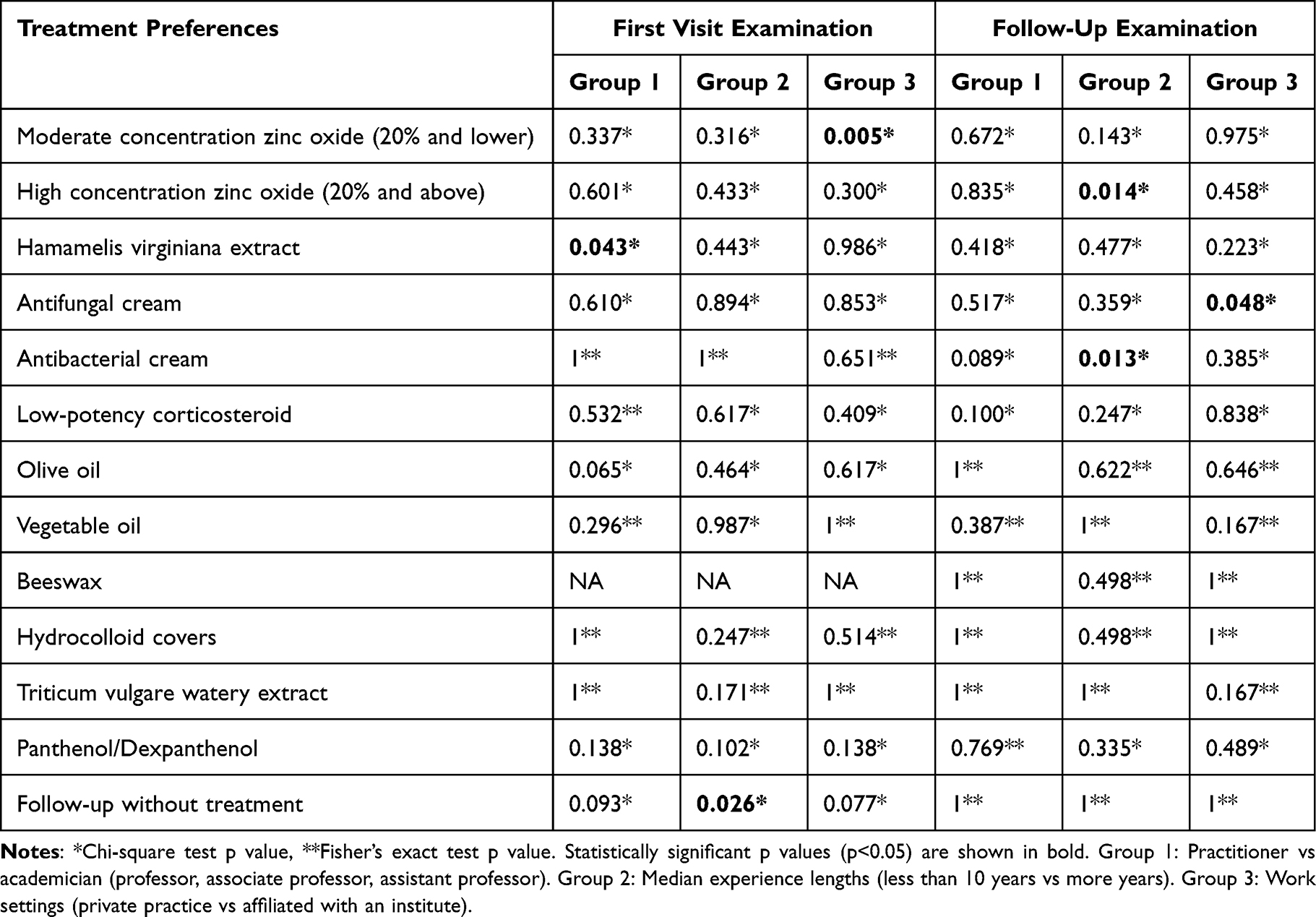 |
Table 1 Treatment Preferences of Pediatrician According to the Groups |
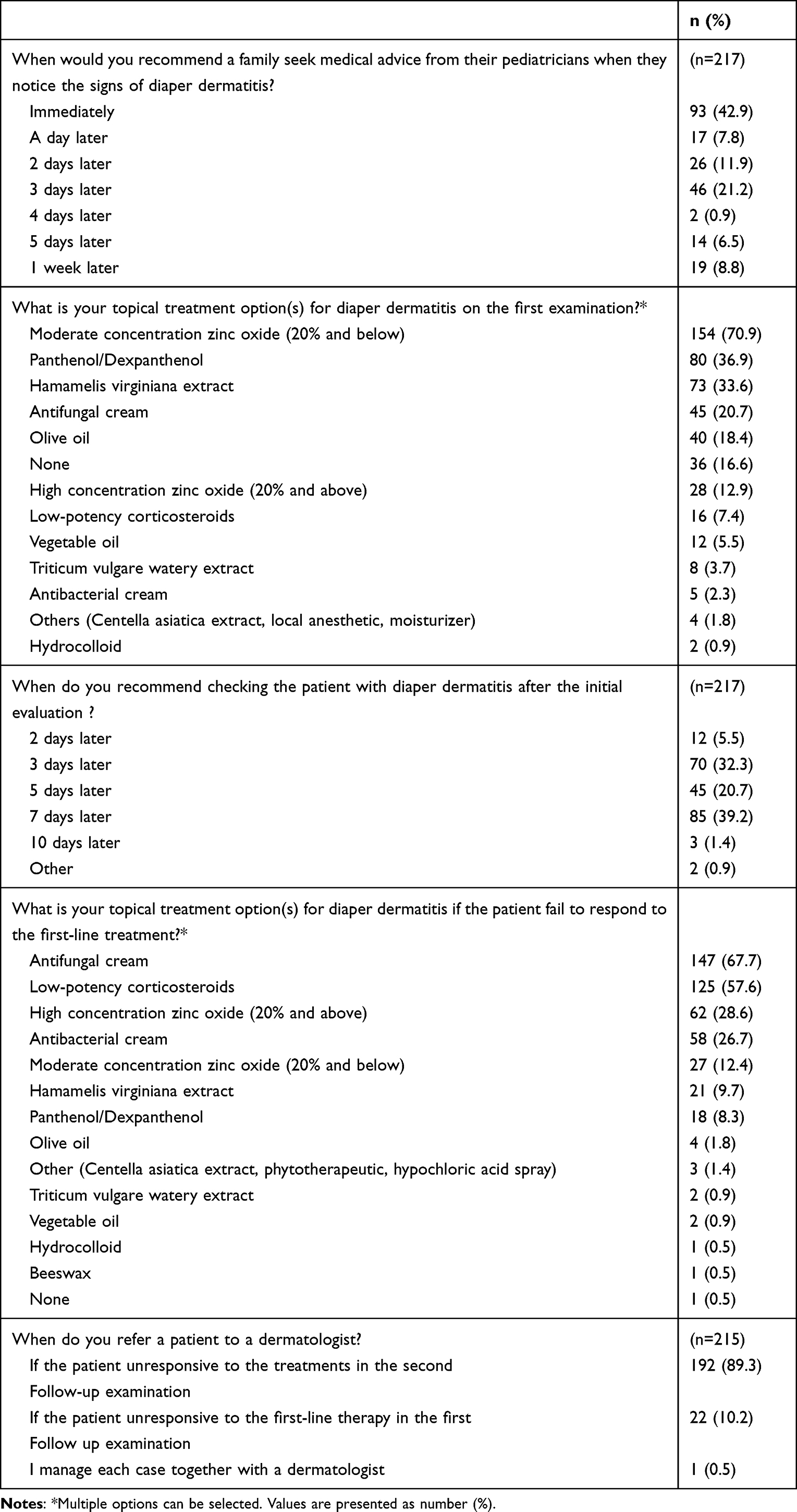 |
Table 2 Diaper Dermatitis Treatment Approaches of Pediatricians |
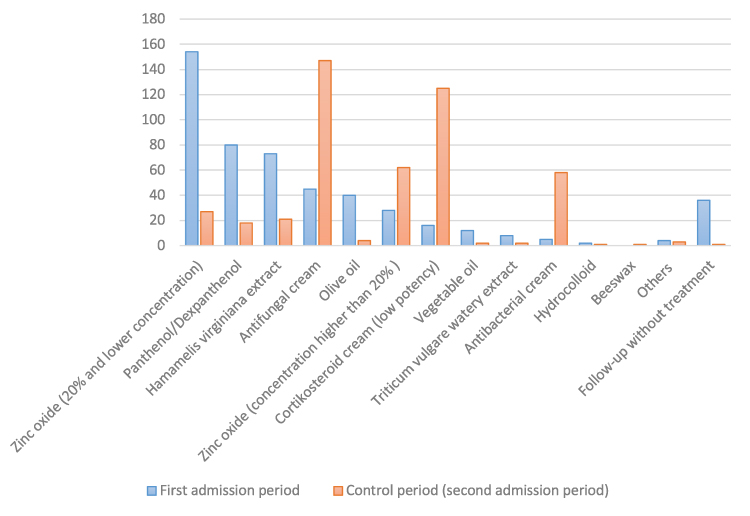 |
Figure 1 Treatment preferences of pediatricians in diaper dermatitis during the first and second admission period. |
Prevention of Diaper Dermatitis
Prevention strategies of the pediatricians were as follows in descending order: aeration of the diaper region, education of the caregivers of babies about diaper dermatitis, gentle cleansing of the diaper area, use of barrier creams and disposable diapers. Most of the participants recommended aeration of diaper region between 0 and 15 minutes after every diaper change which was every 3 to 6 hours. Pediatricians affiliated with an institute recommend aeration of diaper area more than private practice pediatricians (p=0.001). Recommendation for cleaning of diaper area was found to be significantly associated with working health care settings (hospitals, clinics or private practices), academic ranks and length of experience of as a pediatrician. Practitioner pediatricians compared to academician (p=0.012), pediatricians with less than ten years of experience compared to those with more than 10 years of experience (p=0.001), and pediatricians affiliated with an institute compared to private practice pediatricians (p<0.001) suggested to clean the diaper area significantly higher proportion. The sort of topical barrier creams used for treatment (zinc oxide, panthenol/dexpanthenol, hamamelis virginiana extracts) were also the most commonly preferred preparations for the prevention of diaper dermatitis after each diaper change. There was no statistically significant difference in terms of protective agents for prevention for diaper dermatitis between groups. Cleansing with warm water (74.7%) and drying with a clean towel or soft cloth (55.8%) were the most common suggestions. Of the pediatricians, %14,7 reported that they recommend large size diapers according to the weight of the babies, most of them prefer to tie the appropriate size diapers loosely (43.3%) or fit (41.5%). All participants were asked their opinions about continuing breast-feeding or hypoallergenic/standard cow’s milk-based formulas during diaper dermatitis. Almost all of them (98.2%) recommended continuing breastfeeding of babies with diaper dermatitis. In addition, the vast majority of the pediatricians agreed on the necessity of parents and/or caregivers education about the prevention of diaper dermatitis (Table 3).
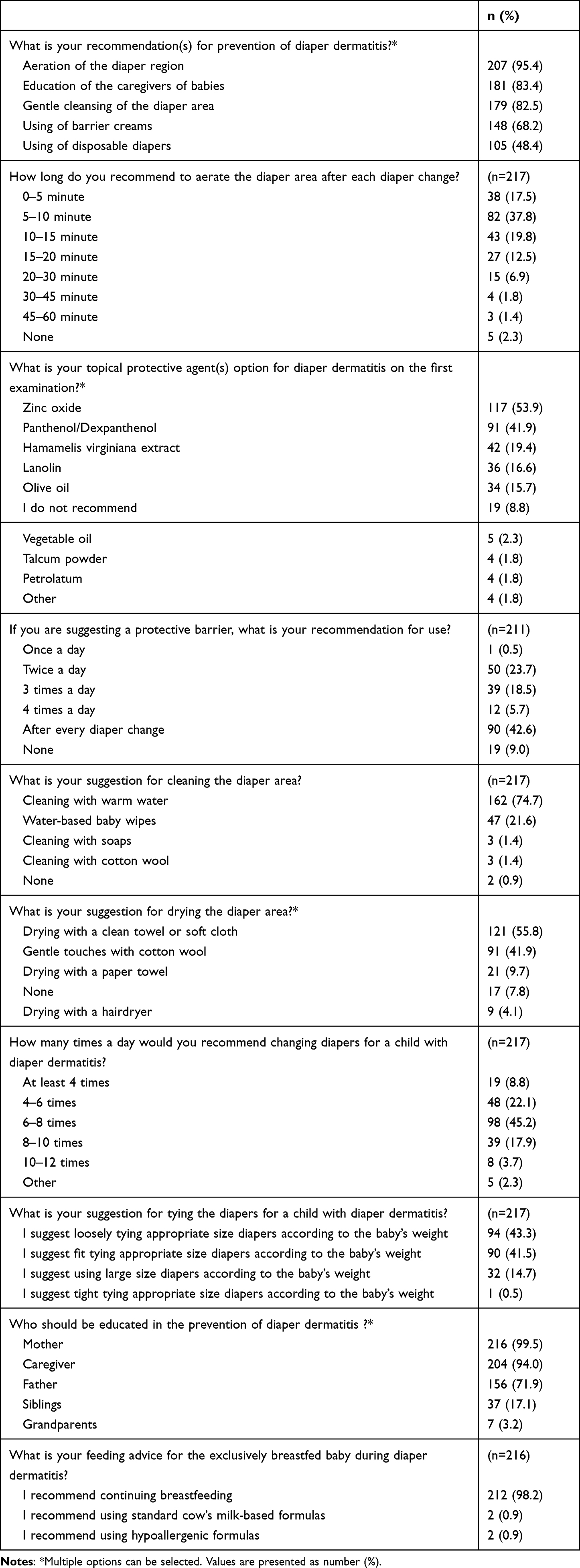 |
Table 3 Diaper Dermatitis Prevention Approaches of Pediatricians |
Discussion
It is well known that topical protective barrier creams are extensively used for both treatment and prevention of diaper dermatitis by physicians and caregivers of infants.15 A variety of topical barrier creams are available in the market such as zinc oxide in various concentrations, petrolatum, lanolin, paraffin, dimethicone and panthenol. Furthermore, these formulations can be used either alone or in combination. Zinc oxide is one of the most effective active ingredients for maintenance of skin health and is frequently used as a topical barrier product.16,17 Previous studies revealed that topical zinc oxide is more effective than or at least as effective as for the other barrier creams in both prevention and treatment of diaper dermatitis.18,19 Preparations with hamamelis virginiana extract are widely used for the treatment of skin conditions including diaper dermatitis. Wolff et al suggested that hamamelis virginiana and dexpanthenol had similar effects in the treatment of skin lesions.20 In this study, moderate concentration of zinc oxide, panthenol/dexpanthenol and hamamelis virginiana extract were the most commonly recommended first-line therapies of diaper dermatitis. This study also demonstrated antifungal creams, low-potency corticosteroids, and high concentration of zinc oxide were commonly preferred by pediatricians in case of unresponsiveness to the first-line treatment.
Candida albicans can colonize within 72 hours in a moist environment and/or defective skin barriers. Satellite lesions that usually affect skinfold areas are common characteristics of superficial candidal infections.10 Although the isolation of Candida albicans in the diaper area is below 4%, it increases up to 70 to 92% in the presence of diaper dermatitis.21 In a study reported that the frequency of candidal infection rate in diaper dermatitis was 77.4% with a long recovery period.22 Secondary bacterial infections may develop due to deterioration of the skin barrier, irritant factors, and changes in pH of the diaper region. Although Staphylococcus aureus is the most common microorganism, diaper dermatitis may complicate by other bacterial pathogens including staphylococci other than Staphylococcus aureus, streptococci, E. coli, and Bacteroides.21,23 Topical antifungals and antibiotics should be considered in the treatment of diaper dermatitis especially if there is no response to the first-line treatment and/or in suspicion of secondary infections. The results of our study were in concordance with general recommendations. Most of the participants considered adding topical antifungal and antibiotic creams to the treatment of diaper dermatitis especially in the case of unresponsiveness to the initial treatment.
Topical low-potency corticosteroids may reduce severe and excessive inflammation of diaper dermatitis.21,24 However, inappropriate or prolonged use of potent corticosteroid creams may potentially cause local and systemic side effects.25 In our study, low-potency corticosteroid creams were used in the treatment of unresponsive cases. Physicians may consider using topical corticosteroids in more severe cases for a limited period of time.
Pediatricians should be aware of the other causes of dermatitis in refractory and/or persistent cases. Consultation of these cases to a dermatologist should be helpful for both follow-up period and management of diaper dermatitis. In our study, most of the participants (89.3%) referred their patients to a dermatologist in the case of unresponsiveness to treatment in the second follow-up examination.
The study of Gözen et al assessed diaper dermatitis prevention and care practices of mothers with 0-2-year-old infants and reported that only 19.3% of mothers routinely used protective creams for their baby’s daily care.26 As stated in this study, it is essential that mothers need to be educated for protection strategies about diaper dermatitis. Besides prevention, it is essential to educate caregivers about getting medical advice for the treatment of diaper dermatitis.11,17,24 The findings of our study demonstrated that nearly all the pediatricians agreed in educating the caregivers of babies about prevention of diaper dermatitis.
A variety of techniques and materials are used to clean the diaper areas such as different kinds of baby wipes, washing with water, cleaning with soaps, and using cotton wool.22 Some kinds of baby wipes may cause allergic contact sensitization and may contribute to inflammation of the diaper area.8 In our study, most pediatricians recommend warm water and water-based baby wipes for cleaning of the diaper region. Algorithm for treating and preventing diaper dermatitis in relation to our study is summarized in Figure 2.
 |
Figure 2 Algorithm for treating and preventing of diaper dermatitis in relation to the study. |
This study has several strengths, but it also has some limitations. The questionnaire was structured only to assess the pharmaceutical ingredients of the topical barrier creams, not their forms, such as creams or ointments. The participants were not asked about the details of the solvent used in the extract, and the active pharmaceutical ingredients of antibacterials and antifungals were not specifically requested. Furthermore, practitioners’ treatment options were queried at the initial examination and when the patient did not respond to first-line treatment. Although this may indirectly provide information about disease severity, directly investigating the relationship between disease severity and treatment options could positively contribute to the study’s outcomes. Lastly, we aimed to evaluate whether pediatricians based their treatment decisions on the severity of skin lesions at the first visit and whether they chose an appropriate preparation based on the efficacy of treatment at the second visit. However, we acknowledge that a more open-ended approach to questioning would have been preferable to avoid potential biases. Future studies should utilize more comprehensive and unbiased approaches to investigate treatment decision-making in the field of pediatrics. Despite these limitations, our findings are significant in evaluating the knowledge, attitudes, and therapeutic approaches of a group of pediatricians which is heterogeneous in terms of experience, academic rank, and affiliations. Another crucial clinical implication of the study is the provision of a comprehensive list of treatment choices for newborns and infants with diaper dermatitis.
Conclusion
In conclusion, our study sheds light on the knowledge, attitudes, and therapeutic approaches of a broad group of pediatricians from different provinces of Turkey regarding diaper dermatitis. Our findings clearly indicate that zinc oxide, panthenol/dexpanthenol, and hamamelis virginiana extract were the most commonly prescribed topical treatments and also the preferred protective options during the first visit. Furthermore, our study revealed that most pediatricians applied topical antimicrobial and anti-inflammatory treatment to their patients when there was no response to first-line treatment, and they sought the opinion of a dermatologist during the second follow-up examination. Overall, our study highlights the different approaches of pediatricians to diaper dermatitis, and we believe that future studies are necessary to demonstrate pediatricians’ management strategies for diaper dermatitis.
Ethical Approval
This study was approved by Tekirdağ Namık Kemal University’s Clinical Research Ethics Committee (2021.150.05.23).
Acknowledgment
The authors would like to thank Dr. İbrahim Kandemir for advice on statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahma A, Lane ME. Skin barrier function in infants: update and outlook. Pharmaceutics. 2022;14(2). doi:10.3390/pharmaceutics14020433
2. Stamatas GN, Nikolovski J, Mack MC, Kollias N. Infant skin physiology and development during the first years of life: a review of recent findings based on in vivo studies. Int J Cosmet Sci. 2011;33(1):17–24. doi:10.1111/j.1468-2494.2010.00611.x
3. Giusti F, Martella A, Bertoni L, Seidenari S. Skin barrier, hydration, and pH of the skin of infants under 2 years of age. Pediatr Dermatol. 2001;18(2):93–96. doi:10.1046/j.1525-1470.2001.018002093.x
4. Stamatas GN, Nikolovski J, Luedtke MA, Kollias N, Wiegand BC. Infant skin microstructure assessed in vivo differs from adult skin in organization and at the cellular level. Pediatr Dermatol. 2010;27(2):125–131. doi:10.1111/j.1525-1470.2009.00973.x
5. Hoeger PH, Enzmann CC. Skin physiology of the neonate and young infant: a prospective study of functional skin parameters during early infancy. Pediatr Dermatol. 2002;19(3):256–262. doi:10.1046/j.1525-1470.2002.00082.x
6. Carr AN, DeWitt T, Cork MJ, et al. Diaper dermatitis prevalence and severity: global perspective on the impact of caregiver behavior. Pediatr Dermatol. 2020;37(1):130–136. doi:10.1111/pde.14047
7. Tüzün Y, Wolf R, Bağlam S, Engin B. Diaper (napkin) dermatitis: a fold (intertriginous) dermatosis. Clin Dermatol. 2015;33(4):477–482. doi:10.1016/j.clindermatol.2015.04.012
8. Mactaggart E, Orchard D, Mui Tam M. Baby wipes and nappy rash - what is the relationship? A review. Australas J Dermatol. 2021;62(4):470–477. doi:10.1111/ajd.13715
9. Buckley BS, Mantaring JB, Dofitas RB, Lapitan MC, Monteagudo A. A new scale for assessing the severity of uncomplicated diaper dermatitis in infants: development and validation. Pediatr Dermatol. 2016;33(6):632–639. doi:10.1111/pde.12988
10. Shin HT. Diagnosis and management of diaper dermatitis. Pediatr Clin North Am. 2014;61(2):367–382. doi:10.1016/j.pcl.2013.11.009
11. Blume-Peytavi U, Kanti V. Prevention and treatment of diaper dermatitis. Pediatr Dermatol. 2018;35(Suppl 1):s19–s23. doi:10.1111/pde.13495
12. Fölster-Holst R. Differential diagnoses of diaper dermatitis. Pediatr Dermatol. 2018;35(Suppl 1):s10–s18. doi:10.1111/pde.13484
13. Blume-Peytavi U, Lavender T, Jenerowicz D, et al. Recommendations from a European roundtable meeting on best practice healthy infant skin care. Pediatr Dermatol. 2016;33(3):311–321. doi:10.1111/pde.12819
14. The jamovi project. Jamovi. (Version 1.6) [Computer Software]; 2021. Available from: https://www.jamovi.org.
15. Pather P, Hines S, Kynoch K, Coyer F. Effectiveness of topical skin products in the treatment and prevention of incontinence-associated dermatitis: a systematic review. JBI Database System Rev Implement Rep. 2017;15(5):1473–1496. doi:10.11124/JBISRIR-2016-003015
16. Gupta M, Mahajan VK, Mehta KS, Chauhan PS. Zinc therapy in dermatology: a review. Dermatol Res Pract. 2014;2014:709152. doi:10.1155/2014/709152
17. Helms LE, Burrows HL. Diaper dermatitis. Pediatr Rev. 2021;42(1):48–50. doi:10.1542/pir.2020-0128
18. Chaithirayanon S. Comparative study between talcum and zinc oxide cream for the prevention of irritant contact diaper dermatitis in infants. J Med Assoc Thai. 2016;99(Suppl 8):S1–S6.
19. Wananukul S, Limpongsanuruk W, Singalavanija S, Wisuthsarewong W. Comparison of dexpanthenol and zinc oxide ointment with ointment base in the treatment of irritant diaper dermatitis from diarrhea: a multicenter study. J Med Assoc Thai. 2006;89(10):1654–1658.
20. Wolff HH, Kieser M. Hamamelis in children with skin disorders and skin injuries: results of an observational study. Eur J Pediatr. 2007;166(9):943–948. doi:10.1007/s00431-006-0363-1
21. Bonifaz A, Rojas R, Tirado-Sánchez A, et al. Superficial mycoses associated with diaper dermatitis. Mycopathologia. 2016;181(9–10):671–679. doi:10.1007/s11046-016-0020-9
22. Ersoy-Evans S, Akıncı H, Doğan S, Atakan N. Diaper dermatitis: a review of 63 children. Pediatr Dermatol. 2016;33(3):332–336. doi:10.1111/pde.12860
23. Šikić Pogačar M, Maver U, Marčun Varda N, Mičetić-Turk D. Diagnosis and management of diaper dermatitis in infants with emphasis on skin microbiota in the diaper area. Int J Dermatol. 2018;57(3):265–275. doi:10.1111/ijd.13748
24. Stamatas GN, Tierney NK. Diaper dermatitis: etiology, manifestations, prevention, and management. Pediatr Dermatol. 2014;31(1):1–7. doi:10.1111/pde.12245
25. Coondoo A, Phiske M, Verma S, Lahiri K. Side-effects of topical steroids: a long overdue revisit. Indian Dermatol Online J. 2014;5(4):416–425. doi:10.4103/2229-5178.142483
26. Gözen D, Çağlar S, Doğan Z. The practice of mothers to prevent and care of diaper dermatitis for their 0–24 months of infants. Istanbul Univ Florence Nightingale J Nurs. 2011;19(1):17–22.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.