Back to Journals » Infection and Drug Resistance » Volume 19
Pediatric Submandibular Lymphadenitis Caused by Mycobacterium houstonense: A Case Report and Literature Review
Authors Liu M, Guo J, Chen Y, Hu X, Luo X, Ma L, Huang L
Received 18 January 2026
Accepted for publication 12 March 2026
Published 7 April 2026 Volume 2026:19 593959
DOI https://doi.org/10.2147/IDR.S593959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Minxue Liu,1,* Jing Guo,1,* Yan Chen,1 Xuehua Hu,1 Xiaocheng Luo,2 Lian Ma,2 Liying Huang1
1Department of Laboratory Medicine, Maternal and Child Health Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 2Department of Laboratory Medicine, Nanning Fourth People’s Hospital, Guangxi AIDS Clinical Treatment Center (Nanning), Nanning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liying Huang, Department of Laboratory Medicine, Maternal and Child Health Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China, Email [email protected]
Abstract: Infection caused by Mycobacterium houstonense is rare. A literature review suggested that M. houstonense infections mainly affect adults with open fractures or wounds. Here, we report a pediatric case of submandibular lymphadenitis caused by M. houstonense. The strain was identified using Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS) and 16S rRNA gene sequencing. The patient was successfully treated with a six-month combination regimen of linezolid, clarithromycin, amikacin, and cefoxitin, with the modification that trimethoprim-sulfamethoxazole was used instead of cefoxitin for the final four months. The pediatric patient was monitored monthly with complete blood counts and liver function tests throughout the treatment course. No adverse events were observed, and clinical cure was achieved.
Keywords: Mycobacteria houstonense, pediatric patient, infection, lymphadenitis, case report
Introduction
Mycobacterium houstonense is classified as a non-tuberculous mycobacterium (NTM) and belongs to Mycobacterium fortuitum third biovariant complex. It is a sorbitol-positive, acid-fast, and rapidly growing mycobacterium (RGM).1,2 M. houstonense was first reported in 2004 in the facial wound of a patient from Houston, Texas; hence, the name Mycobacterium houstonense.2,3 To date, reports on M. houstonense infections remain limited, primarily documenting wounds and osteomyelitis in adults.4–7 Here, we report a case of M. houstonense-related submandibular lymphadenitis in a pediatric patient from Guangxi, China. Standard management of NTM cervical lymphadenitis in children requires antimicrobial susceptibility testing (AST)-guided antibiotic selection for the specific isolate and an adequate treatment duration; surgical intervention or debridement may be necessary when abscess formation occurs or antibiotic efficacy is poor. In addition, we reviewed published cases of M. houstonense infection. This study broadens our knowledge on M. houstonense-related infections.
Case Presentation
An 11-year-old boy was admitted to the Maternal and Child Health Hospital of the Guangxi Zhuang Autonomous Region (Guangxi, China). He had a two-month history of mild pain and progressive right submandibular lymphadenopathy of an unknown origin. Physical examination showed a 3×5 cm lymph node on the right submandibular with a rubbery texture; the overlying skin was warm and of normal color (Figure 1A). His temperature was 36.5 °C. Subsequent laboratory investigations revealed that inflammatory markers were within normal limits, with a white blood cell count of 6.24 × 109/L and a C-reactive protein level of 1.06 mg/L. Ultrasonography revealed inflammatory changes in the right submandibular lymph node. Computed tomography revealed lymphadenitis. However, the interferon-gamma release assay results were negative.
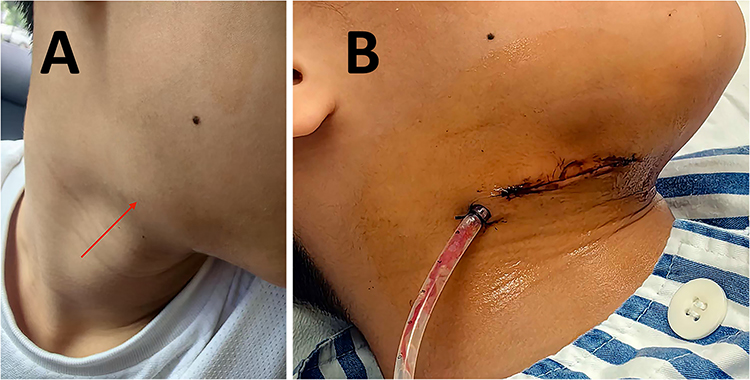 |
Figure 1 (A) A 3×5 cm, rubbery lymph node in the right submandibular region (indicated by red arrows). The overlying skin appears warm and normally colored. (B) Lymphadenectomy was performed. |
Subsequently, lymphadenectomy was performed for definitive diagnosis and therapeutic excision (Figure 1B). Pathological examination of the lymph nodes revealed caseous necrosis and granuloma formation (Figure 2A) with positive acid-fast bacilli (AFB) staining (Figure 2B). In addition, lymph tissues were cultured on blood agar plates at 35 °C with 5% CO2. After 72 h of incubation, small diameter colonies were observed. After subculturing on blood and chocolate agar plates at 35 °C with 5% CO2 for 96 h, the colonies appeared as slightly beige, mucoid, convex, round, and entire-edged with no aerial hyphae (Figure 2C and D). The strain appeared as light-colored, string-of-beads bacilli on Gram staining (Figure 2E) and was confirmed to be acid-fast positive (Figure 2F).
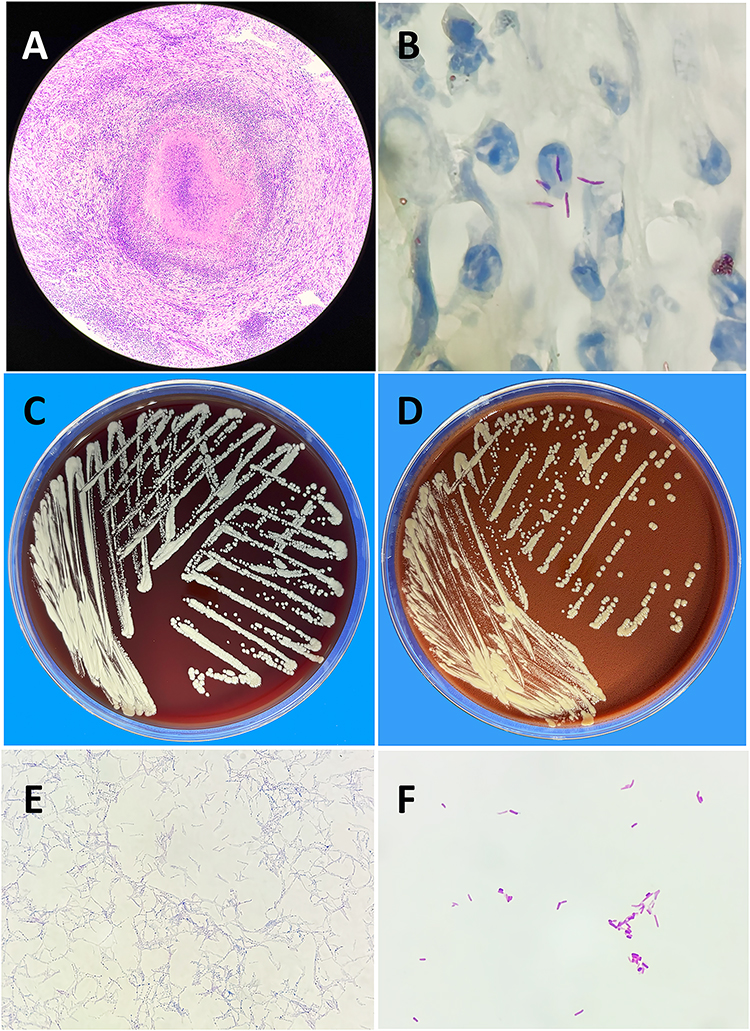 |
Figure 2 (A) Pathological examination of the lymph node showed caseous necrosis with granuloma formation. (B) Acid-fast bacilli staining of the lymph node biopsy section was positive. (C and D) After 96 hours of subculture on blood and chocolate agar plates at 35 °C under 5% CO2, colonies appeared slightly beige, mucoid, convex, round, and entire-edged, without aerial hyphae. (E) Gram staining revealed lightly stained bacilli arranged in a beaded-chain morphology. (F) The strain tested positive on acid-fast staining. |
The clinical strain was identified as M. houstonense using Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS, Antobio MS 600, Zhengzhou, China), achieving a confidence score of 9.3, and 16S rRNA gene sequencing, which showed 99.93% nucleotide identity with reference sequences in the NCBI GenBank rRNA/ITS databases. The 16S rRNA sequence of this M. houstonense isolate was deposited in GenBank (accession number: PV707975).
Antimicrobial susceptibility testing (AST) was performed by using Drug susceptibility test kit for Mycobacteria (Yinke, Zhuhai, China), which is based on the broth microdilution method and includes 15 antibiotics (rifampin, rifabutin, ethambutol, linezolid, clarithromycin, amikacin, imipenem, azithromycin, cefoxitin, tobramycin, moxifloxacin, gatifloxacin, doxycycline, minocycline, and sulfamethoxazole). All procedures were performed according to the manufacturer’s instructions. The minimum inhibitory concentrations (MICs) of the 15 antibiotics were determined after incubation at 37°C for 7 to 10 days. Mycobacterium kansasii BNCC360707 was used as the quality control strain. The results showed that the isolate was susceptible to linezolid, clarithromycin, amikacin, cefoxitin, moxifloxacin, and sulfamethoxazole but resistant to imipenem, tobramycin, and doxycycline according to the breakpoints for RGM in CLSI M24S 2nd Edition8 (Table 1).
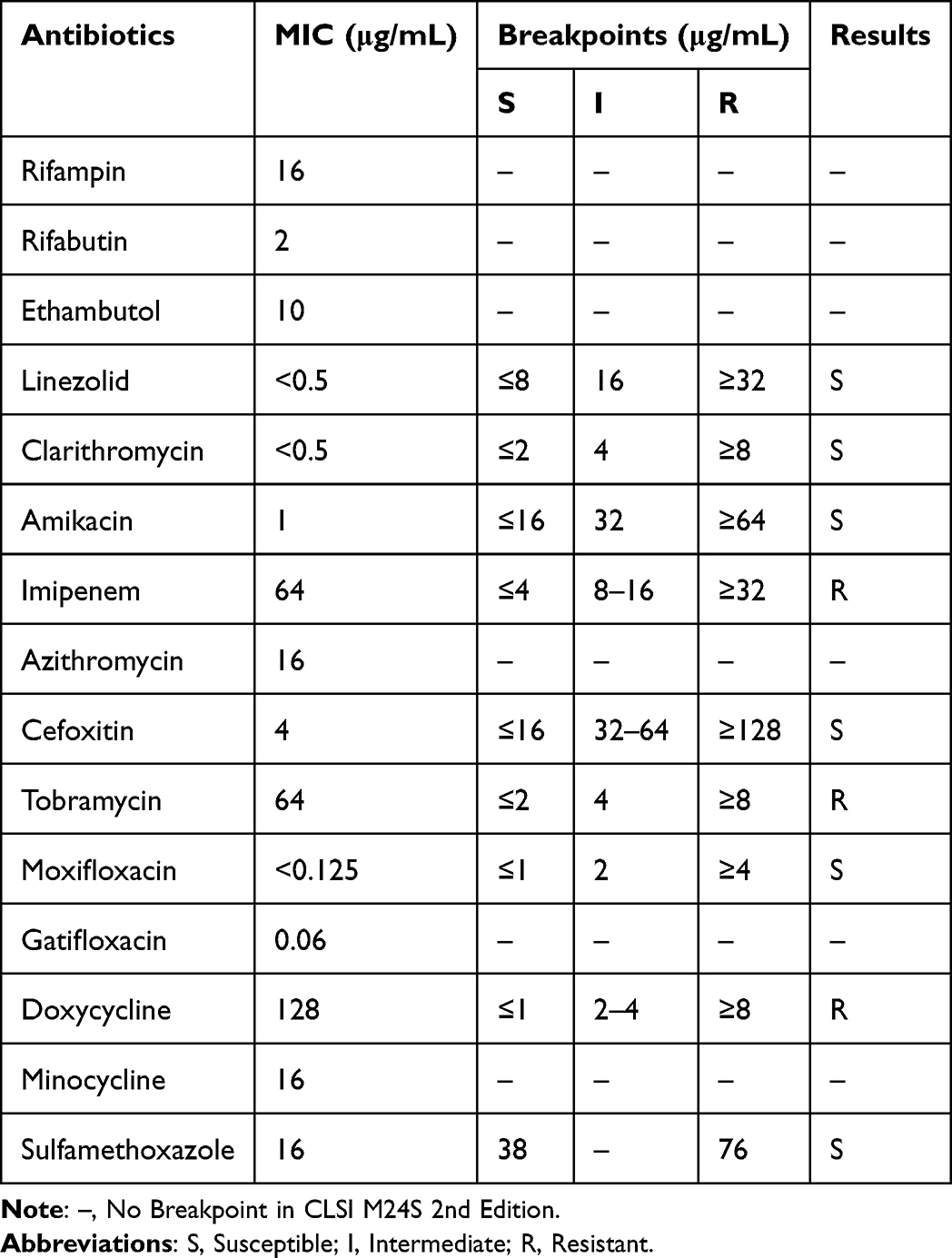 |
Table 1 In vitro Antibiotic Susceptibility Testing Results of the Clinical Mycobacterium houstonense Isolate |
Before formal reports on bacterial identification and AST were obtained, the child was transferred to Nanning Fourth People’s Hospital (Guangxi, China), an infectious disease prevention and control hospital. Subsequent culture of the wound secretion was negative. Given the pathological findings and positive AFB results, tuberculosis could not be excluded from pediatric patients. He was therefore started on empiric anti-tuberculosis therapy with the standard four-drug oral regimen: isoniazid 0.3 g daily, rifampin 0.45 g daily, ethambutol 0.5 g daily and pyrazinamide 0.25 g daily. The surgical wound showed no improvement and exhibited persistent exudate after one month of empiric anti-tuberculosis therapy (Figure 3A). Subsequently, an unstained pathological specimen from the lymphadenectomy performed at the admitting hospital was sent to the Dian Diagnostics Laboratory (Hangzhou, China) for metagenomic next-generation sequencing (mNGS, MGISEQ-200/G99, BGI) analysis. However, the mNGS results were negative.
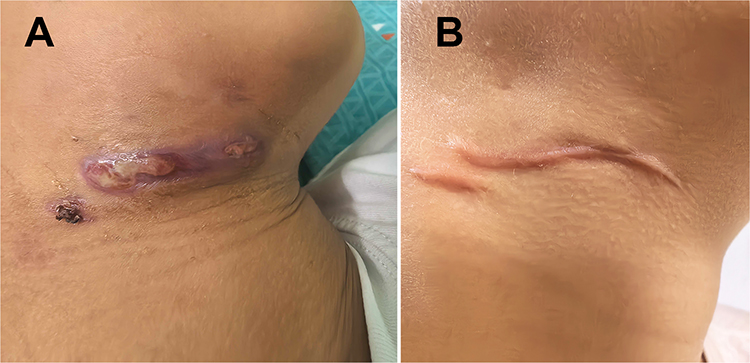 |
Figure 3 (A) After one month of empiric antituberculosis therapy, the surgical wound showed no improvement and continued to produce exudate. (B) Following six months of anti-M. houstonense therapy, the wound healed completely with no residual exudate. |
Based on the pathological examination findings, a positive AFB result, M. houstonense isolation in culture during the initial hospitalization, and the patient’s lack of response to empiric anti-tuberculosis therapy, he was diagnosed with M. houstonense submandibular lymphadenitis. The AST and Chinese guidelines for nontuberculous mycobacterial diseases guide further management.9 Accordingly, the child was initially treated in the hospital with a regimen consisting of oral linezolid (20 mg/kg, once daily), oral clarithromycin (0.5 g twice daily for children weighing 30–40 kg), intravenous amikacin (15–20 mg/kg, once daily), and intravenous cefoxitin (200 mg/kg daily, in three divided doses). After two months of therapy, the wound showed significant improvement. Subsequently, the child was discharged with a regimen of oral linezolid (10 mg/kg daily), oral clarithromycin (0.5 g twice daily for children weighing 30–40 kg), and oral trimethoprim-sulfamethoxazole (15 mg/kg twice daily) to be taken at home, and received once daily intramuscular injections of amikacin (15–20 mg/kg) at a nearby local clinic. After a further four-month course of therapy, the wound exhibited complete resolution, with no evidence of exudate (Figure 3B). Additionally, no abnormal blood flow signals or lymphadenopathy were detected on ultrasonography. During prolonged therapy, the pediatric patient was monitored monthly with complete blood counts and liver function tests (including aspartate aminotransferase and alanine aminotransferase). No adverse events were observed. The onset, diagnosis, and treatment of the disease in this patient are shown in Figure 4.
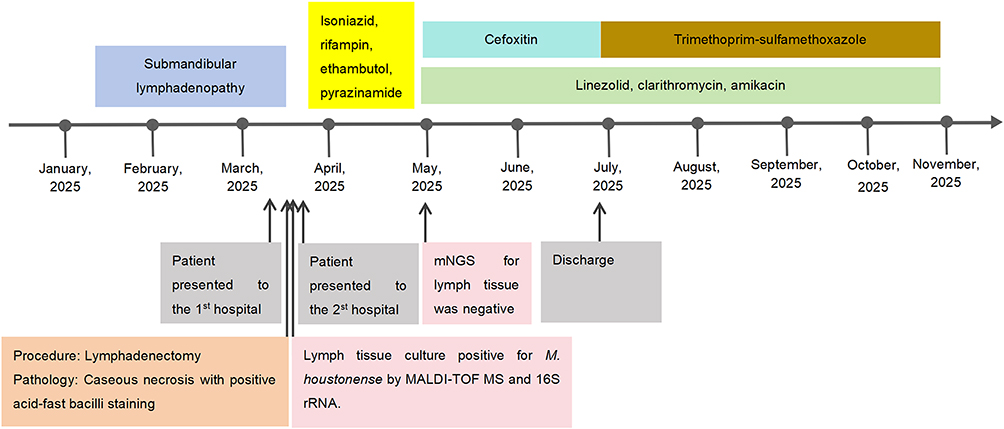 |
Figure 4 Timeline of the patient’s clinical presentation and key events. mNGS, Metagenomic next-generation sequencing; MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry. |
Discussion
In this case, an immunocompetent child developed M. houstonense infection despite having no history of trauma or surgery. Although pediatric submandibular lymphadenitis caused by NTM has been documented,10,11 this is the first reported case of M. houstonense. Alena et al detected sequences closely related to M. houstonense in consumed fish.12 However, in this case, the pediatric patient denied any contact with fish products. The mechanism by which M. houstonense causes pediatric lymphadenitis has not yet been fully elucidated. Further studies are required to clarify the exact pathogenic pathway involved.
M. houstonense is a gram-positive, pleomorphic bacillus; however, its pale Gram staining can lead to false-negative results. Therefore, careful examination and considerable experience in microscopic specimen screening are essential. And M. houstonense is an acid-fast, rapidly growing NTM that can be cultured on blood agar at 35°C for 2 to 4 d. Culture methods remain the gold standard for the diagnosis of NTM infections. Although cultures frequently yield negative results, several published studies have highlighted mNGS’s robust diagnostic potential of mNGS in such contexts.7,13 We agree that mNGS is not routinely necessary when culture results are positive. However, in our case, the positive culture was obtained at the initial hospital, while a subsequent culture of the wound secretion was negative in the second hospital. Therefore, mNGS was subsequently performed on pathological specimens from the original hospital to confirm M. houstonense infection and to rule out the possibility of co-infection with other pathogens. Notably, mNGS was negative despite a positive culture, probably because the sensitivity of mNGS for pathological specimens is often reduced by DNA degradation. In a study by Wang et al,13 mNGS testing of cerebrospinal fluid was performed four times, with only one positive result. This discrepancy may be associated with sampling quality, nucleic acid extraction efficiency, or limitations in the sequencing database. Thus, traditional microbiological culture combined with molecular diagnosis remains essential for the diagnosis M. houstonense infection.
Due to the similar symptoms and pathological findings between NTM infections and tuberculosis, NTM infections are often misdiagnosed as tuberculosis, as seen in our case and in two other case reports.7,13 However, antibiotic therapies for NTM and Mycobacterium tuberculosis differ significantly.9,14–16 Misdiagnosis leading to inappropriate anti-tuberculosis treatment can delay the correct management of NTM infections. Additionally, unnecessary treatment exposes patients to the burdensome toxic side effects of anti-tuberculosis drugs, particularly in children. However, divergent antimicrobial susceptibility patterns have been observed across NTM and intra-species strains.17–21 Therefore, pathogen identification and AST are crucial for guiding treatment.
We also conducted a literature review of documented M. houstonense infection cases by searching PubMed and Web of Science using the search terms “rapidly growing mycobacteria” OR “RGM” OR “nontuberculous mycobacteria” OR “NTM” OR “Mycobacterium fortuitum complex” OR “Mycobacterium houstonense” for publications up to November 2025. The inclusion criteria were: (1) infection caused by M. houstonense; (2) cases with adequate clinical information; (3) articles published in English. After systematic screening, eight reported cases4–7,13,22 were identified (Table 2). All individuals infected with M. houstonense were adults, seven of whom had open wounds. The infections included: one case of endophthalmitis, one central nervous system infection, two surgical incision infections, and four osteoarthritis infections. Five M. houstonense strains, including the first isolate from Houston and the isolate from our patient, were subjected to AST. The results demonstrated that these strains were susceptible to amikacin and quinolones but resistant to doxycycline and tobramycin. The susceptibility to clarithromycin, imipenem, linezolid, and trimethoprim-sulfamethoxazole varied. Therefore, when cultures are positive, AST is crucial for guiding subsequent treatment decisions. The importance of AST-guided therapy in NTM infection is also emphasized in the Chinese Expert Consensus on Diagnosis and Management of Cutaneous NTM Diseases.14 The use of quinolone antibiotics has been restricted in children owing to their potential to cause adverse musculoskeletal events.23 However, studies have shown that arthralgia and arthropathy are relatively uncommon in children and resolve after discontinuation of quinolones, without long-term sequelae.24,25 Therefore, quinolones may be considered for the treatment of M. houstonense infections in children when susceptibility is confirmed by AST and clinically appropriate. Additionally, among the eight reported cases, seven of eight (7/8) underwent surgical intervention, such as wound debridement. Therefore, surgical intervention may be a useful therapeutic approach in addition to antibiotic administration. As recommended by the International Pediatric Otolaryngology Group (IPOG) consensus guidelines, the management options for nontuberculous mycobacterial cervicofacial lymphadenitis include surgical excision and prolonged antimicrobial therapy.26
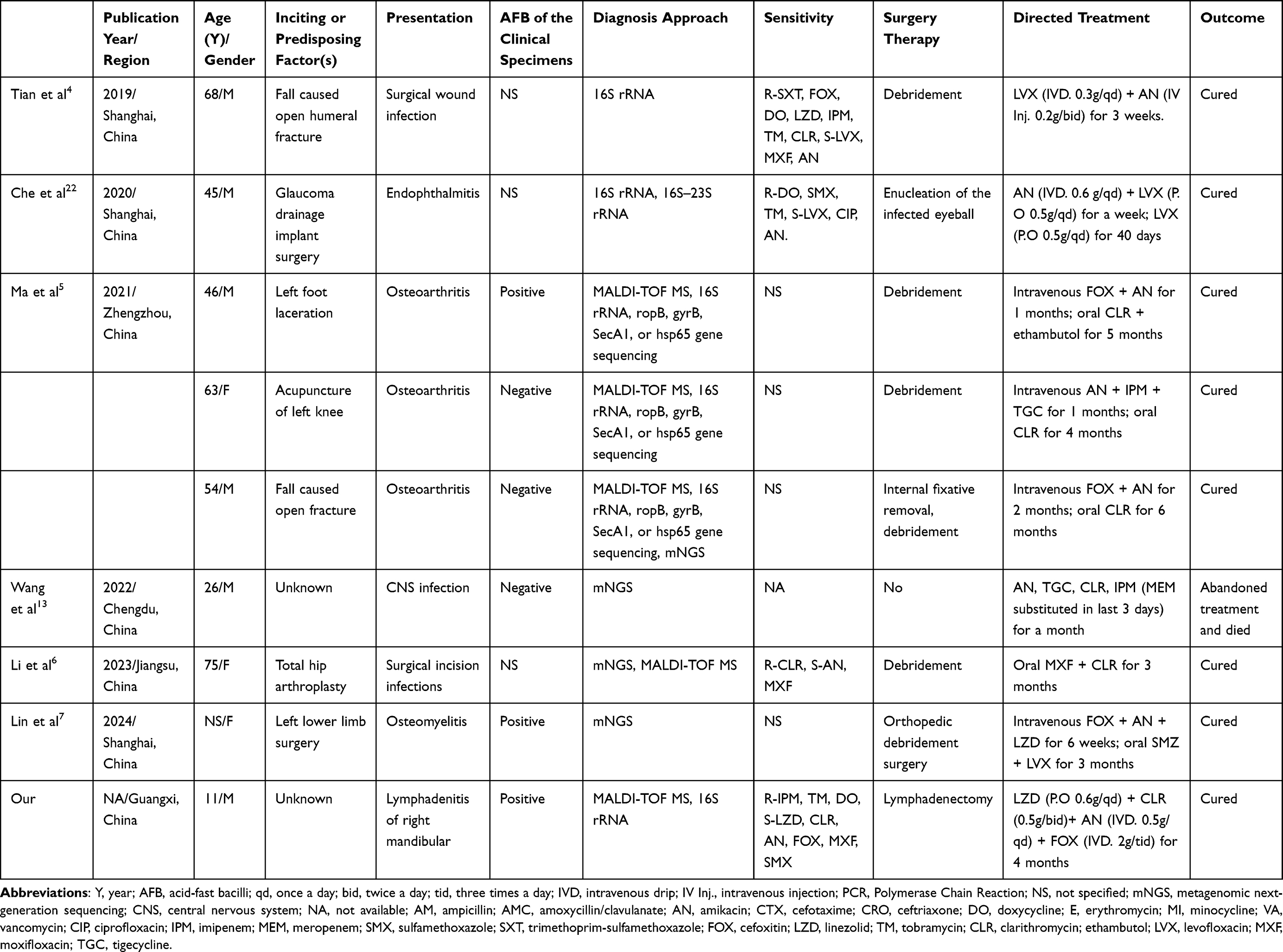 |
Table 2 Cases of Infection Caused by Mycobacterium houstonense Reported in the Literature |
Among the nine patients with M. houstonense infection, eight cases involving the skin and soft tissue recovered following appropriate treatment. However, one patient with central nervous system infection died because of an inadequate treatment course and intracranial infection. For NTM infections, guidelines recommend a minimum of 4 months of therapy for skin and soft tissue infections, and 6 months for bone infections.9,14 However, a study focusing on RGM-induced CNS infections reported survivor treatment durations ranging from 2.5 months to greater than 16 months.27 Therefore, an adequate treatment course is essential for a favorable prognosis.
Our study has a limitation. While 16S rRNA sequencing is useful, it may not reliably identify species within the M. fortuitum complex. More accurate methods, such as sequencing of the 16S–23S rRNA internal transcribed spacer (ITS) region or whole-genome sequencing,28 could provide definitive molecular identification. In recent years, MALDI-TOF MS has continued to be valued for microbial identification. However, its identification accuracy is dependent on the comprehensiveness and currency of the reference mass spectral database. In our study, M. houstonense was included in the MALDI-TOF MS database (Antobio MS 600, Zhengzhou, China). The clinical strain was identified as M. houstonense by both MALDI-TOF MS and 16S rRNA sequencing. The concordant results from these two distinct platforms significantly strengthened the reliability of our identification.
Conclusions
This case report describes submandibular lymphadenitis caused by M. houstonense in a child. Clinicians should maintain a high index of suspicion for this organism in pediatric cervicofacial lymphadenitis. Accurate species identification is essential. Treatment should be guided by validated antimicrobial susceptibility testing, with meticulous attention to pediatric dosing and safety monitoring. Broad-spectrum empiric regimens should be avoided, as M. houstonense exhibits diverse resistance patterns that necessitate targeted therapy to optimize efficacy and minimize toxicity in children.
Abbreviations
MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; NTM, Non-tuberculous Mycobacteria; MIC, Minimum Inhibitory Concentration; RGM, Rapidly growing mycobacteria; AFB, Positive acid-fast bacilli; AST, Antimicrobial susceptibility testing; mNGS, Metagenomic next-generation sequencing.
Data Sharing Statement
The sequencing data can be accessed from GenBank (accession number: PV707975). The datasets analyzed and used in our study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the local Ethics Committee of The Maternal and Child Health Hospital of Guangxi Zhuang Autonomous Region.
Consent for Publication
As the patient was 11 years old, consent for the publication of case details and the accompanying images was obtained from the patient’s guardian. The publication of the case details were approved by the medical ethics committee of The Maternal and Child Health Hospital of Guangxi Zhuang Autonomous Region.
Acknowledgment
The authors thank all staff who assisted us with this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the “Seedling plan” of The Maternal and Child Health Hospital of Guangxi Zhuang Autonomous Region Foundation (No. GXWCH-YMJH-2018008), the self-funded project of the Health Commission of Guangxi Zhuang Autonomous Region (No. Z-A20220265 and No. Z20210134), and the Major Departments (Department of Laboratory Medicine) Construction Project of Guangxi province.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Brown-Elliott BA, Wallace RJ. Clinical and taxonomic status of pathogenic nonpigmented or late-pigmenting rapidly growing mycobacteria. Clin Microbiol Rev. 2002;15(4):716–9. doi:10.1128/cmr.15.4.716-746.2002
2. Schinsky MF, Morey RE, Steigerwalt AG, et al. Taxonomic variation in the Mycobacterium fortuitum third biovariant complex: description of Mycobacterium boenickei sp. nov. Mycobacterium houstonense sp. nov. Mycobacterium neworleansense sp. nov. and Mycobacterium brisbanense sp. nov. and recognition of Mycobacterium porcinum from human clinical isolates. Int J Syst Evol Microbiol. 2004;54(Pt 5):1653–1667. doi:10.1099/ijs.0.02743-0
3. Levasseur A, Asmar S, Robert C, Drancourt M. Draft genome sequence of Mycobacterium houstonense strain ATCC 49403T. Genome Announc. 2016;4(3):10–128. doi:10.1128/genomeA.00443-16
4. Tian L, Zhang Z, Chen Z, Sun Z. Surgical wound infection following open humeral fracture caused by Mycobacterium houstonense: a case report. BMC Infect Dis. 2019;19(1):333. doi:10.1186/s12879-019-3979-2
5. Ma Q, Chen R, Yang E, et al. Non-tuberculous mycobacterial infection of the musculoskeletal system detected at two tertiary medical centres in Henan, China, 2016–2020. Front Microbiol. 2021;12:791918. doi:10.3389/fmicb.2021.791918
6. Li Z, Yuan Z, Cao H, et al. A case report on Mycobacterium houstonense infection after total Hip arthroplasty. BMC Infect Dis. 2023;23(1):722. doi:10.1186/s12879-023-08705-y
7. Lin HY, Tan QH. Metagenomic next-generation sequencing may assist diagnosis of osteomyelitis caused by Mycobacterium houstonense: a case report. World J Orthop. 2024;15(11):1095–1100. doi:10.5312/wjo.v15.i11.1095
8. CLSI. Performance standards for susceptibility testing of Mycobacteria, Nocardiae spp. and other Aerobic Actinomycetes. 2nd edition. CLSI supplement M24S. Clinical and Laboratory Standards Institute; 2023.
9. Tang JS, Li L, Yan XF, Wu SM. [Guidelines for diagnosis and treatment of non-tuberculous mycobacteria disease]. Chin J Tuberc Respir Dis. 2020;43:918–946.
10. Meoli A, Deolmi M, Iannarella R, Esposito S. Non-tuberculous mycobacterial diseases in children. Pathogens. 2020;9(7):553. doi:10.3390/pathogens9070553
11. Leow O, Aoyama R, Loh WS, et al. Non-tuberculous mycobacterial cervicofacial lymphadenitis in children-10-year experience in a tertiary pediatric center. J Pediatric Infect Dis Soc. 2023;12(7):406–412. doi:10.1093/jpids/piad043
12. Lorencova A, Klanicova B, Makovcova J, et al. Nontuberculous mycobacteria in freshwater fish and fish products intended for human consumption. Foodborne Pathog Dis. 2013;10(6):573–576. doi:10.1089/fpd.2012.1419
13. Wang L, Wang F, Yang C, Luo F. Central nervous system infection caused by Mycobacterium houstonense: a case report. Front Neurol. 2022;13:908086. doi:10.3389/fneur.2022.908086
14. Mycobacteriosis Research Group CBaRDA, & Division of Dermatology and STI Diagnosis, Chinese Association on Leprosy. [Expert consensus on the diagnosis and treatment of cutaneous nontuberculous mycobacterial diseases in China]. Chin J Dermatol. 2024;57(2):109–118.
15. Alsayed SSR, Gunosewoyo H. Tuberculosis: pathogenesis, current treatment regimens and new drug targets. Int J Mol Sci. 2023;24(6):5202. doi:10.3390/ijms24065202
16. Martínez-Campreciós J, Espinosa-Pereiro J, Sánchez-Montalvá A. Update on the treatment of tuberculosis. Med Clin. 2024;163(5):245–252. doi:10.1016/j.medcli.2024.02.030
17. Zimenkov D. Variability of mycobacterium avium complex isolates drug susceptibility testing by broth microdilution. Antibiotics. 2022;11(12):1756. doi:10.3390/antibiotics11121756
18. Lin S, Hua W, Wang S, et al. In vitro assessment of 17 antimicrobial agents against clinical Mycobacterium avium complex isolates. BMC Microbiol. 2022;22(1):175. doi:10.1186/s12866-022-02582-2
19. Ying R, Yang J, Wu X, Yu F, Sha W. Antimicrobial susceptibility testing using the MYCO test system and MIC distribution of 8 drugs against clinical isolates of nontuberculous mycobacteria from Shanghai. Microbiol Spectr. 2023;11(2):e0254922. doi:10.1128/spectrum.02549-22
20. Tunesi S, Zelazny A, Awad Z, Mougari F, Buyck JM, Cambau E. Antimicrobial susceptibility of Mycobacterium abscessus and treatment of pulmonary and extra-pulmonary infections. Clin Microbiol Infect. 2024;30(6):718–725. doi:10.1016/j.cmi.2023.09.019
21. Aono A, Morimoto K, Chikamatsu K, et al. Antimicrobial susceptibility testing of Mycobacteroides (Mycobacterium) abscessus complex, Mycolicibacterium (Mycobacterium) fortuitum, and Mycobacteroides (Mycobacterium) chelonae. J Infect Chemother. 2019;25(2):117–123. doi:10.1016/j.jiac.2018.10.010
22. Che X, Li Q, Wang L, et al. Endophthalmitis caused by Mycobacterium houstonense: case report. BMC Infect Dis. 2020;20(1):849. doi:10.1186/s12879-020-05590-7
23. Wu Junyan SS. Expert consensus on the use of fluoroquinolone antibacterial drugs in children. Today Med. 2018;28(1):1–10.
24. Wang JG, Cui HR, Hu YS, Tang HB. Assessment of the risk of musculoskeletal adverse events associated with fluoroquinolone use in children: a meta-analysis. Medicine. 2020;99(34):e21860. doi:10.1097/md.0000000000021860
25. Patel K, Goldman JL. Safety Concerns Surrounding Quinolone Use in Children. J Clin Pharmacol. 2016;56(9):1060–1075. doi:10.1002/jcph.715
26. Roy CF, Balakrishnan K, Boudewyns A, et al. International Pediatric Otolaryngology Group: consensus guidelines on the diagnosis and management of non-tuberculous mycobacterial cervicofacial lymphadenitis. Int J Pediatr Otorhinolaryngol. 2023;166:111469. doi:10.1016/j.ijporl.2023.111469
27. Talati NJ, Rouphael N, Kuppalli K, Franco-Paredes C. Spectrum of CNS disease caused by rapidly growing mycobacteria. Lancet Infect Dis. 2008;8(6):390–398. doi:10.1016/s1473-3099(08)70127-0
28. Xu A, Pan N, Zhang B, et al. Genomic analysis of a clinical Mycolicibacterium houstonense isolate reveals dual escalation in adaptability and virulence. BMC Microbiol. 2025;26(1):86. doi:10.1186/s12866-025-04637-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.