Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Pediatric Radiation-Induced Alopecia Post Intracranial Vascular Malformation Embolization: A Case Report with Dermoscopic Findings
Received 2 December 2025
Accepted for publication 15 February 2026
Published 24 February 2026 Volume 2026:19 584194
DOI https://doi.org/10.2147/CCID.S584194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Chen Sun, Xiao Yang
Department of Dermatology, Children’s Hospital of Nanjing Medical University, Nanjing, People’s Republic of China
Correspondence: Xiao Yang, Email [email protected]
Abstract: Radiation-induced alopecia (RIA) is an uncommon complication associated with fluoroscopy-guided neurointerventional procedures. We present a case of a 7-year-old female child who developed a well-demarcated square alopecic patch on the occipital scalp 18 days after undergoing intracranial vascular malformation embolization. Dermoscopic examination revealed multiple characteristic findings, including black dots, yellow dots, Pohl-Pinkus constrictions, tapered hairs, flame hairs, and upright regrowing hairs. The geometric shape of the alopecic patch was completely consistent with the intraoperative radiation exposure field, confirming the diagnosis of RIA. Notably, the presence of Pohl-Pinkus constrictions and tapered hairs suggests a dystrophic anagen response pattern, reflecting a less severe form of follicular damage that permits eventual hair regrowth. This case underscores the diagnostic value of dermoscopy in differentiating RIA from other common alopecic disorders, particularly in pediatric patients who have undergone neurointerventional procedures.
Keywords: radiation-induced alopecia, RIA, dermoscopy, Pohl-Pinkus constrictions, tapered hairs, flame hairs, intracranial vascular malformation, endovascular embolization
Introduction
Endovascular embolization of intracranial vascular malformations is a commonly used minimally invasive neurointerventional procedure.1 It occludes abnormal intracranial vascular malformations through endovascular techniques, which can effectively reduce the risk of intracranial hemorrhage and improve neurological dysfunction. This procedure requires real-time fluoroscopic guidance, often involving prolonged and repeated radiation exposure, thus inevitably exposing patients to ionizing radiation. Radiation-induced alopecia (RIA) is one of the rare complications following such interventional therapy,1 and there is currently no clear data on its clinical incidence. To our knowledge, pediatric RIA cases with detailed dermoscopic findings remain rarely documented, leading to insufficient awareness among pediatricians, neurosurgeons, and dermatologists. Children have poor tolerance for invasive pathological examinations, while dermoscopy, as a non-invasive detection method, plays an important role in the clinical diagnosis of various alopecic disorders. This study aims to explore the clinical and dermoscopic features of RIA in children after endovascular embolization of intracranial vascular malformations, and to provide a reference for early clinical identification and diagnosis of this disease.
Case Presentation
A 7-year-old female patient was admitted emergently 25 days prior due to a sudden fall with unconsciousness. After completing relevant examinations, she urgently underwent combined transcatheter embolization, resection, and intracranial hematoma evacuation for an intracranial vascular malformation. Preoperative whole-scalp shaving was performed. Postoperatively, the scalp healed well, and hair grew back uniformly to approximately 5 mm in length. Seven days prior to presentation (postoperative day 18), the parents noticed alopecia in the occipital region, which gradually formed a square-shaped patch. There was no scalp erythema, pain, ulceration, or other discomfort, prompting a visit to the dermatology clinic.
Specialized physical examination revealed a well-defined, square alopecic patch measuring approximately 7 cm × 9 cm on the occipital scalp. The skin in the affected area was smooth, without atrophy, scarring, or signs of inflammation. The hair pull test was negative (Figure 1).
 |
Figure 1 A square-shaped alopecic patch measuring approximately 7 cm × 9 cm on the occipital scalp. |
Dermoscopic examination (Beining Dermoscope Image Processing Workstation, Model: BN-PFMF-8001D) of the alopecic area showed black dots, yellow dots, Pohl-Pinkus constrictions, tapered hairs, flame hairs, and upright regrowing hairs (Figures 2 and 3).
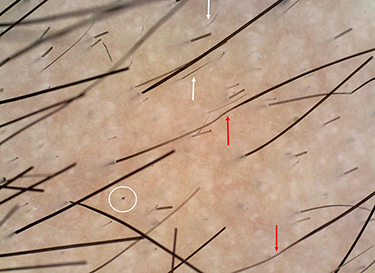 |
Figure 2 Red arrows: Pohl-Pinkus constrictions; white arrows: upright regrowing hairs; white circles: black dots (magnification ×40). |
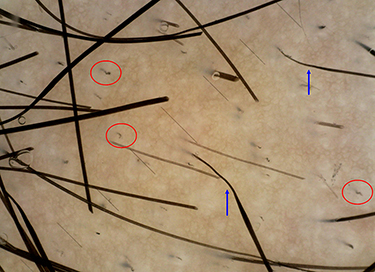 |
Figure 3 Blue arrows: tapered hairs; red circles: flame hairs (magnification ×50). |
Diagnosis: Radiation-induced alopecia.
Treatment: Topical mucopolysaccharide polysulfate cream was prescribed three times daily. At the 2-month follow-up, gradual hair regrowth was observed in the alopecic area.
This study was approved by the Ethics Committee of Children’s Hospital of Nanjing Medical University (Approval No.: 202510072-1), with explicit permission for the publication of this case report. Written informed consent for case publication was obtained from the patient’s legal guardians.
Discussion
RIA is characterized by typical clinical manifestations, usually presenting as square or rectangular alopecic patches on the occipital or parietal scalp. This characteristic feature is closely associated with the geometric irradiation range of the intraoperative radiation beam and the patient’s prolonged fixed position during surgery.2 The occurrence of RIA is closely related to radiation dose and exposure duration. A radiation dose of 3–6 Gray (Gy) can induce temporary alopecia, while doses exceeding 7 Gy may result in permanent hair loss.3 Clinically, alopecia typically occurs 1–2 weeks after radiation exposure, and spontaneous hair regrowth mostly occurs within 2–24 weeks post-exposure, with some cases having a prolonged regrowth period of up to 12 months.4 The child in this case presented with a typical square alopecic patch, which was completely consistent with the intraoperative fluoroscopic radiation exposure field, thus confirming the clinical diagnosis of RIA.
The core pathogenesis of RIA is closely related to differences in the radiation sensitivity of hair follicle cells and radiation-induced hair follicle damage responses. There is a significant gradient in the radiation sensitivity of different hair follicle cells: actively proliferating matrix cells are the most sensitive, followed by outer root sheath and lower proximal cup cells with relatively inactive mitosis, while quiescent bulge epithelial hair follicle stem cells (eHFSCs) are the least sensitive.5 Ionizing radiation primarily targets actively proliferating matrix cells, causing acute damage that inhibits cell proliferation and renewal, leading to thinning of the proximal hair shaft, increased fragility, and subsequent breakage.
Studies have indicated that the final damage phenotype of hair follicles is mainly mediated by radiation dose, specifically manifesting as two distinct damage response patterns: dystrophic anagen response and dystrophic catagen response.6 When hair follicle radiation damage is mild and the radiation dose is low, a dystrophic anagen response is predominantly induced. At this stage, outer root sheath and lower proximal cup cells with low radiation sensitivity can act as reserve progenitor cells, promptly replenishing the number of damaged and apoptotic matrix cells, thereby enabling the hair follicle to barely maintain anagen activity and resulting in relatively mild clinical alopecia. In contrast, when hair follicle radiation damage is severe and the radiation dose is high, a dystrophic catagen response is triggered. This process requires the recruitment of outer root sheath cells and bulge eHFSCs for repair, which is time-consuming; meanwhile, hair canal dilatation induced by apoptosis impairs the normal attachment of the hair shaft, leading to significant alopecia.6 If the radiation dose further increases, irreversible damage to the hair follicle structure will occur, ultimately resulting in permanent RIA.6
As a non-invasive detection method, dermoscopy holds important clinical value in the auxiliary diagnosis of alopecic disorders, particularly for pediatric patients with poor tolerance for invasive pathological examinations. Previous studies on adult RIA have shown that its main dermoscopic manifestations include yellow dots, black dots, vellus hairs, and broken hairs.1,2,4,7 Yellow dots correspond to dilated hair follicle infundibula obstructed by sebaceous gland secretions and keratin, while black dots represent residual intrafollicular hair roots after hair shaft breakage. However, the dermoscopic manifestations of adult RIA are non-specific and overlap significantly with those of alopecia areata, easily leading to clinical misdiagnosis. Since RIA usually resolves spontaneously within a few months and the clinical treatment regimens for these two alopecic disorders differ significantly, accurate clinical differentiation is of great importance for clinical diagnosis and management.
Currently, reports on the clinical and dermoscopic features of pediatric RIA are relatively limited. The dermoscopic manifestations of the pediatric patient in this case are notably characteristic, with the concurrent detection of the triad of Pohl-Pinkus constrictions, tapered hairs, and flame hairs, which merits clinical attention. Pohl-Pinkus constrictions are characterized by focal narrowing of the hair shaft diameter, serving as a marker of rapid and repeated inhibition of hair follicle metabolism and mitotic activity, and directly reflecting hair follicle radiation damage. If radiation damage occurs repeatedly, multiple progressive and irregular narrowing may appear on the hair shaft, presenting a characteristic beaded appearance.8 This finding can be observed in various diseases, including alopecia areata, chemotherapy-induced alopecia, cicatricial alopecia, severe systemic infections, massive blood loss, nutritional deficiencies, interferon therapy, and localized hereditary hypotrichosis.8
Tapered hairs are a morphological variant of Pohl-Pinkus constrictions, characterized by narrowing of the proximal hair shaft. The narrowed area may be beyond the dermoscopic field of view or present as intact terminal hairs, which are also referred to as “coudability hairs” in the literature.8 Only sporadic case reports have mentioned the presence of tapered hairs and continuous irregular narrowing of the hair shaft in RIA.6 Clinically, it is essential to distinguish tapered hairs from exclamation mark hairs; the latter are characterized by thinning and hypopigmentation of the proximal segment and thickening and hyperpigmentation of the distal segment. To date, there are no reports of exclamation mark hairs in patients with RIA.4 The detection of Pohl-Pinkus constrictions and tapered hairs in this patient indicates a mild, radiation-induced dystrophic anagen response. As an incomplete form of hair follicle tissue repair, this mechanism primarily serves to maintain the activity of damaged follicles within their compromised anagen phase, rather than triggering the reconstruction of new anagen hair follicles. This favorable repair profile may be attributed to the stronger hair follicle regenerative capacity of children compared with adults, as well as the low cumulative intraoperative radiation dose and short exposure duration.
Flame hairs were also detected in this child, which are pigmented hair remnants characterized by slender, curled distal ends resembling flames. Histologically, this finding corresponds to a single hair follicle with abnormal hair shaft morphology at the infundibular level.9 Flame hairs were once considered a characteristic dermoscopic finding of trichotillomania; however, studies by Miteva et al10 have confirmed that they represent a form of anagen hair breakage and are not specific to trichotillomania. They can also be observed in alopecia areata, traction alopecia, central centrifugal cicatricial alopecia, and other diseases, with a detection rate of 100% in acute chemotherapy- or radiation-induced alopecia.
It must be acknowledged that this study has certain limitations. This report only describes a single pediatric case of RIA, and thus cannot confirm whether the dermoscopic triad (Pohl-Pinkus constrictions, tapered hairs, and flame hairs) is a specific manifestation of pediatric RIA compared with adult RIA, nor can it confirm whether there is a correlation between dermoscopic findings and radiation dose. These findings need to be verified in a larger cohort of pediatric patients with RIA. In addition, based solely on this single case and short-term follow-up, we cannot reliably determine the efficacy of topical mucopolysaccharide polysulfate cream in the treatment of RIA; its therapeutic effect requires further verification through well-designed, larger-scale clinical studies with longer follow-up periods.
Conclusion
With the increasing application of intracranial endovascular interventional therapy in pediatric patients, the incidence of postoperative radiation-induced alopecia (RIA) is expected to rise. As a valuable non-invasive preliminary diagnostic tool, dermoscopy—particularly when used to identify the characteristic dermoscopic triad of Pohl-Pinkus constrictions, tapered hairs, and flame hairs —when combined with the patient’s medical history and clinical manifestations, can assist in accurate diagnosis, assess the degree of hair follicle damage, and guide subsequent treatment. This triad, observed in our pediatric case, provides important diagnostic clues that enhance dermoscopy’s utility in distinguishing RIA from other common alopecic disorders in children.
Data Sharing Statement
Research data are not shared.
Ethics Statement
Approved by the Ethics Committee of Children’s Hospital of Nanjing Medical University (Approval No.: 202510072-1).
Patient Consent
Written patient consent for publication was obtained from the patient’s parents.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chen X, Xie Y, Wei A. Combined corticosteroid and minoxidil therapy for early recovery in radiation-induced alopecia: a case report. Clin Cosmet Invest Dermatol. 2025;18:1495–5. doi:10.2147/CCID.S520575
2. Cho S, Choi MJ, Lee JS, et al. Dermoscopic findings in radiation-induced alopecia after angioembolization. Dermatology. 2014;229(2):141–145. doi:10.1159/000362810
3. Ednalino KAG, Yap-Silva C. Alopecia induced by fluoroscopy-guided embolization: a case report. Acta Med Philipp. 2024;58(17):106–109. doi:10.47895/amp.v58i17.7501
4. Guerrero-Putz MD, Flores-Dominguez AC, Castillo-de la Garza RJ, et al. Anagen effluvium after neurointerventional radiation: trichoscopy as a diagnostic ally. Skin Appendage Disord. 2022;8(2):102–107. doi:10.1159/000518743
5. Huang WY, Lai SF, Chiu HY, et al. Mobilizing transit-amplifying cell-derived ectopic progenitors prevents hair loss from chemotherapy or radiation therapy. Cancer Res. 2017;77(22):6083–6096. doi:10.1158/0008-5472.CAN-17-0667
6. Lin SJ, Yue Z, Paus R. Clinical pathobiology of radiotherapy-induced alopecia: a guide toward more effective prevention and hair follicle repair. J Invest Dermatol. 2023;143(9):1646–1656. doi:10.1016/j.jid.2023.02.041
7. Seol JE, Kim DH, Park SH, et al. Three cases of radiation-induced temporary alopecia with hair microscopic examination: “Coudability Hair” might not be specific for alopecia areata. Int J Trichol. 2018;10(1):40–43. doi:10.4103/ijt.ijt_74_17
8. Rudnicka L, Rakowska A, Kerzeja M, et al. Hair shafts in trichoscopy: clues for diagnosis of hair and scalp diseases. Dermatol Clin. 2013;31(4):695–708. doi:10.1016/j.det.2013.06.007
9. Lima ABS, Rocha FT, Perecin FAMC, et al. Flame hair: auxiliary trichoscopic finding in radiotherapy-induced alopecia. Skin Appendage Disord. 2021;7(3):224–226. doi:10.1159/000513578
10. Miteva M, Tosti A. Flame hair. Skin Appendage Disord. 2015;1(2):105–109. doi:10.1159/000438995
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Prospective Study of Dermoscopic and Ultrastructural Features of Vitiligo-Associated Leukotrichia
Li M, Wang F, Li X, Ding X, Du J
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3673-3680
Published Date: 21 December 2023