Back to Journals » International Journal of General Medicine » Volume 16
Pediatric and Adolescent Flatfoot: A Questionnaire Based Middle East and North Africa Study
Authors Yasin MS ![]() , Al-Labadi GM
, Al-Labadi GM ![]() , Alshrouf MA
, Alshrouf MA ![]() , AlRaie BA
, AlRaie BA ![]() , Ibrahim RA
, Ibrahim RA ![]() , AlRaie LA
, AlRaie LA ![]()
Received 8 December 2022
Accepted for publication 7 March 2023
Published 29 May 2023 Volume 2023:16 Pages 2055—2061
DOI https://doi.org/10.2147/IJGM.S400720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Mohamad S Yasin, Ghayda’a M Al-Labadi, Mohammad Ali Alshrouf, Bayan A AlRaie, Raneem A Ibrahim, Lana A AlRaie
Department of Special Surgery, Division of Orthopedics, The University of Jordan, Amman, 11942, Jordan
Correspondence: Lana A AlRaie, Department of Special Surgery, Division of Orthopedics, The University of Jordan, Amman, 11942, Jordan, Tel +962776129370, Email [email protected]
Background: Flatfoot is commonly seen in the community and is a common cause of concern for parents because it could become symptomatic and lead to decreased quality of life. One of the most used management approaches is foot orthoses, although no clear evidence supports their use. We aimed to study flatfoot symptoms’ prevalence, effect on activities of daily living, and the use and effectiveness of orthoses.
Methodology: This was a cross‐sectional study that included five countries from the Middle East and North Africa region (Jordan, Palestine, Syria, Egypt, and Iraq). Data were collected using an online questionnaire directed toward parents of children aged 0 to 16 from September to December 2020. The demographic factors were expressed as frequencies (percentages) using standard descriptive statistical parameters, and Pearson’s chi-square test was used to examine the relationship between study factors.
Results: 1256 participants were recruited using this online survey. The majority (29.6%) of children were diagnosed in the age group of 0 to 2. The abnormal appearance of the foot was the most common (78.7%) complaint. Overall, 54.2% of patients were prescribed orthoses, of which 36.8% noticed improvement in flatness and 37.6% reported relief of symptoms.
Conclusion: This study demonstrated that most participants have no or minimal symptoms and that there is a mismatch between participants’ expectations and the actual effectiveness of orthoses. Taking into consideration that there is no clear evidence to support the corrective effect of orthoses, we recommend that physicians prescribing them adhere more to their proper indications and spend more time and effort counseling and addressing patients’ and parents’ concerns about this developmental stage.
Keywords: flatfoot, foot deformity, pediatric, foot orthoses, cross-sectional
Introduction
Foot problems in children are a common cause of parental concern, with foot posture and flatfoot in particular being the ones that lead to frequent orthopedic assessments.1 Flatfoot, which is also known as pes planus, is a condition in which the medial longitudinal arch is lower than normal with or without hind foot eversion.2 The condition can be rigid or flexible, and the difference between them is crucial for diagnosis and treatment. The flexible type, which is the most common, is physiological and considered part of the normal development of the child.3 The rigid subtype is more complex and indicates a pathology that usually requires surgical correction.4 If the longitudinal arch disappears in the weight-bearing position and becomes visible at rest, then it’s considered flexible, whereas the rigid one implies the loss of arch height in both positions.5
The diagnosis of flatfoot is based on clinical assessment and sometimes supplemented by X-rays and gait analysis.6 Patients with flatfoot can present with symptoms or be completely asymptomatic. Functions of the foot including distributing the weight of the body, facilitating its forward movement during walking, and absorbing shock are dependent on its structure and foot kinetics.2
Flatfoot is usually first noticed and reported by parents as a result of the abnormal shape of the foot, and less commonly because of shoe wear or limited physical activity,7 which is more frequently seen in younger children and in males.5 The prevalence can vary with age, gender, body mass index, and many other variables.6,8,9
There are several measures that could be taken to manage flatfoot, ranging from parental reassurance and prescribing foot orthoses to surgical correction, which is occasionally needed if conservative measures fail.10 Foot orthoses remain the most common form of management, despite the fact that their effectiveness is questionable.5,11 This article’s primary aim was to study pediatric flatfoot and its epidemiology in the Middle East and North Africa (MENA) region, to investigate the reasons that make parents seek medical attention, the prevalence of using foot orthoses, and if there was a reported improvement after using them.
Methods
Study Design and Population
This was a questionnaire-based cross-sectional study that included 1256 patients who met our inclusion criteria. The study aimed to determine the prevalence of symptoms associated with this condition, and the effectiveness of orthoses when used. It was conducted over a period of 3 months, from September to December 2020. Our study population consisted of participants from five Middle East and North Africa (MENA) countries including Jordan, Syria, Iraq, Palestine, and Egypt. The participant’s age was between 0 to 16 years. Those older than 16 years and/or residing outside the five countries were excluded.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Jordan University Hospital. Ethical approval for this study was granted by the Institutional Review Board (IRB) of Jordan University Hospital (reference number 1020234148). The first page of the questionnaire included a clear explanation of the research objectives and aims, which were clarified in Arabic, the official language in the previously mentioned countries, and then consent was obtained from subjects enrolled in the study. Participants were able to withdraw from the questionnaire at any point. No identifying information were obtained, and all collected data were solely used for statistical analysis.
Data Collection Tool and Process
The online questionnaire was purpose-built for this study by a panel of consultant pediatric orthopedic surgeons, it was created using Google Forms and filled out by the participant’s parents. The parents were requested to fill out the Pediatric and Adolescent Flatfoot Questionnaire. The questionnaire (available in English in the Supplementary Materials) consisted of 20 items that assessed foot pain, activity limitation, and physical and social problems caused by the flatfoot. The survey had four sections: general demographics were first assessed, including country of residence, gender, and age (3 questions). Then, participants were asked about the diagnostic journey, including how and at what age it was first noticed, as well as the investigations carried out to reach/confirm the diagnosis if any (5 questions). The study also covered the participants’ symptoms, their level of awareness about their condition, and the impact of the deformity on their lives (6 questions). Finally, we focused on the measures participants took to improve their condition, including getting regular medical care, using orthoses, the expectations prior to orthoses use, and whether improvement in both symptoms and shape of the foot was noticed following their use (6 questions). Participants were classified into four age groups (0–2, 3–5, 6–10, 11–16).
Participants were recruited using an internet-based questionnaire, and they were selected based on being the parent of a child or adolescent with a flat foot. The questionnaire was distributed to participants via social media platforms that included Facebook, WhatsApp, and Twitter. In total, 1256 participants from five countries in the MENA region (Jordan, Syria, Iraq, Palestine, and Egypt) took part in this study.
Statistical Analysis
SPSS version 28.0 (Chicago, IL, USA) was used in our analysis. The demographic factors were calculated and provided as frequencies (percentages) using standard descriptive statistical parameters. Pearson’s chi-square test (χ2) was used to examine the relationship between study factors. Chi-square test with OR (95% CI) was used to determine the association between the likelihood of visiting a doctor and its impact on life. Statistical significance was defined as a p-value of less than 0.05.
Results
In total, there was 1256 participants in this study, 54.2% males and 45.8% females. Most of them (63.9%) were 11 to 16 years old at the time of the study. Almost one-third (29.6%) of diagnoses were made or parents noticed it within the first two years of life. The participants were from 5 different countries: Syria 40%, Jordan 24.3%, Palestine 18.2%, Iraq 14.5%, and Egypt 3%. Table 1 demonstrates the demographic and clinical characteristics of the participants.
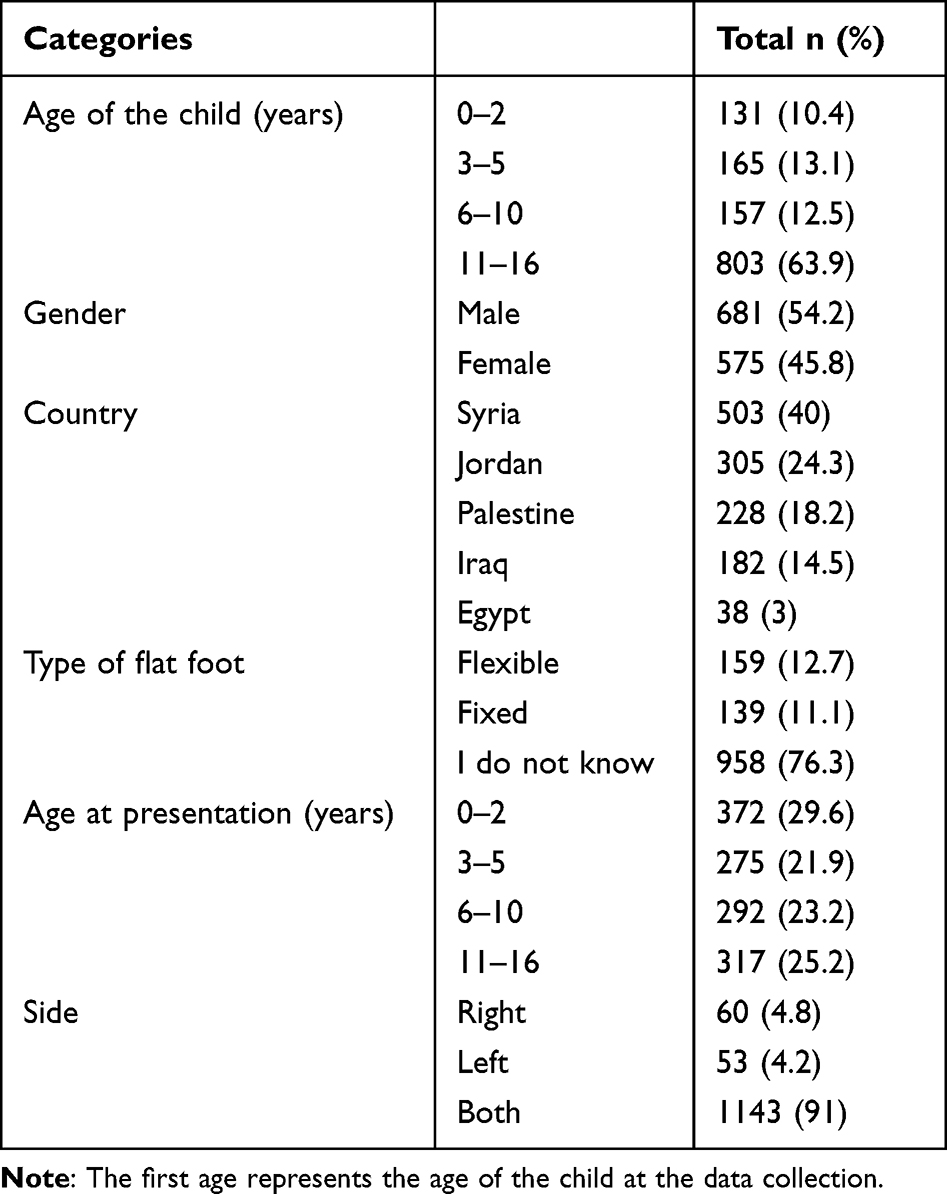 |
Table 1 Characteristics of the Study Population |
The most common presenting symptoms were an abnormal external appearance (78.7%), shoe wearing out (24.8%), and being uncomfortable wearing shoes (24.3%) (Figure 1). In most cases (91%), the deformity was bilateral (Table 2). Only 23.7% of participants had pain as a presenting symptom. However, 68.6% of them complained of pain at the time of the study, with 74.8% having experienced symptoms for years, and the pain was more common (47.3%) on the inner side of the foot (Table 3). There was no significant difference in terms of pain between patients with flexible or rigid flatfoot (p = 0.934). Moreover, there was a significant trend toward having more pain as the age of diagnosis increased from 7.5% in 0 to 2 years, to 40.4% in 11 to 16 years (p < 0.001). Children who were diagnosed at a younger age were more likely to visit the doctor (p < 0.001).
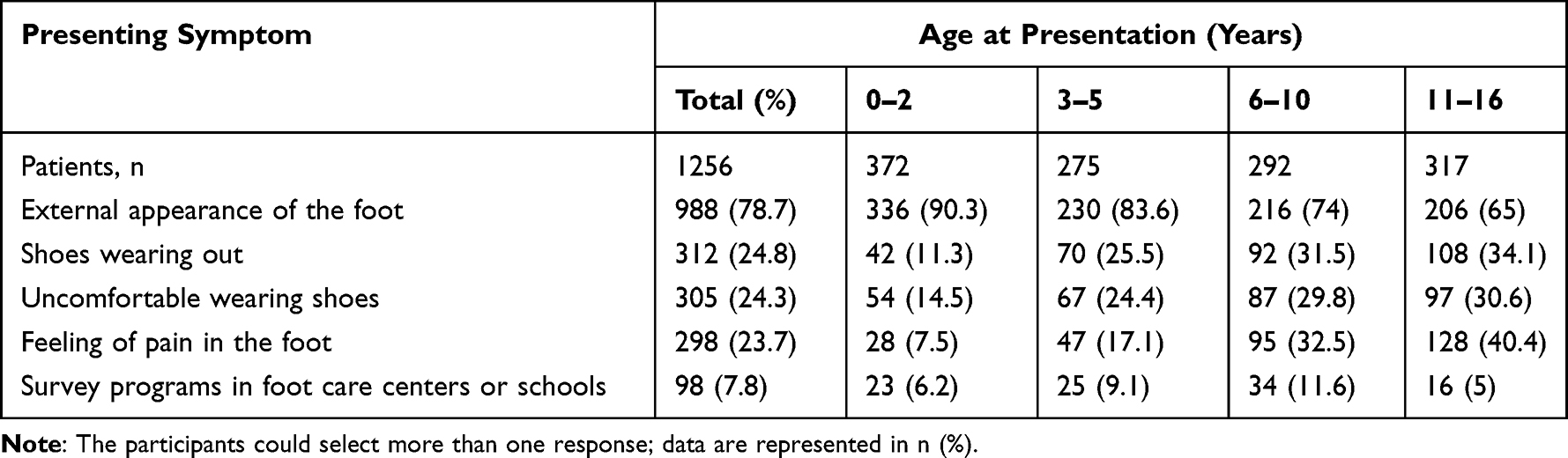 |
Table 2 Presenting Symptoms According to the Age at Presentation |
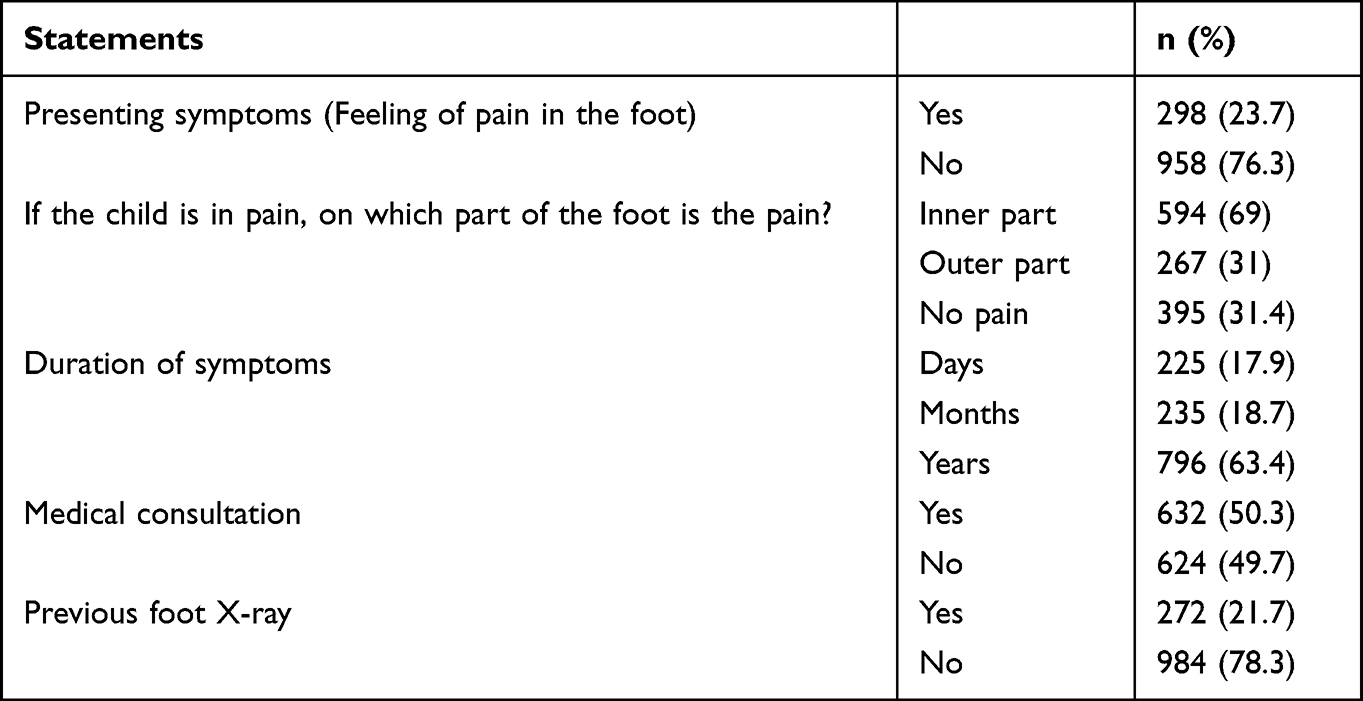 |
Table 3 Description of the Symptoms of the Patients |
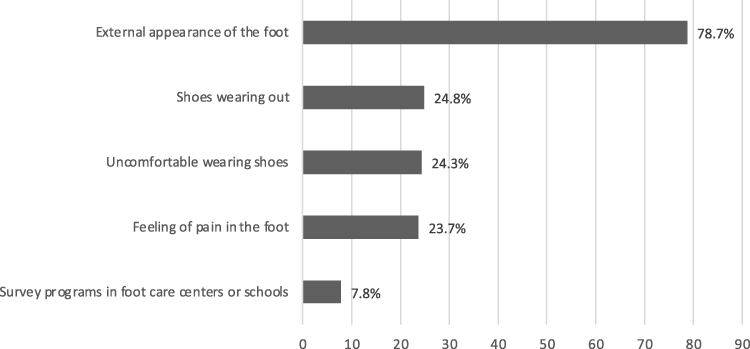 |
Figure 1 Presenting symptoms of the patients. |
Only 50.3% of the participants were seen by a doctor. More than half (54.2%) of our participants were prescribed orthoses; 31.8% were prescribed by an orthopedic surgeon, 11.9% by medical equipment and supply companies, and in 7.2%, they were recommended by relatives and friends. More than half (58.1%) of those who wore orthoses were told that they would correct the flatness, but only 36.8% reported an improvement in the flatness. Furthermore, 37.6% of orthosis users reported improvements in their child’s symptoms in general. Table 4 summarizes the prescription of orthosis and symptoms improvement.
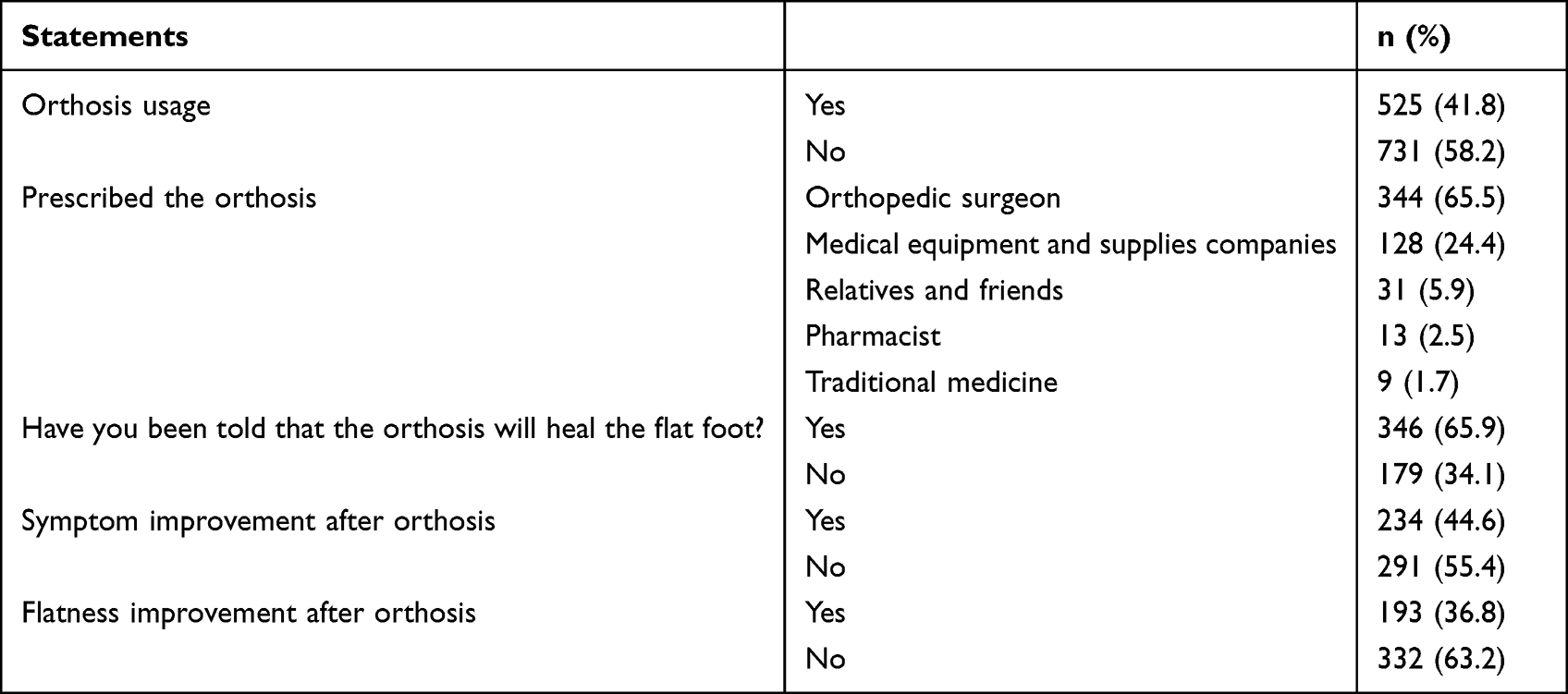 |
Table 4 The Prescription of Orthosis and Symptoms Improvement |
More than a third (35%) complained of severe symptoms that affected their activities of daily living, and 47.1% of our participants had symptoms bad enough to impact their sports or social activities. Participants who had symptoms affecting their daily living activities were significantly more likely to visit a doctor (OR = 1.41, CI 95% 1.12–1.78, p = 0.004). Likewise, participants who had symptoms that had an impact on their sports or social activities were more likely to visit a doctor (OR = 1.36, CI 95% 1.09–1.7, p = 0.007). In the long run, only 15.3% of patients had some form of regular medical visits with an orthopedic surgeon.
Discussion
Our findings showed that the most common presenting symptom was the abnormal appearance of the foot (78.7%), and pain was only present in 23.7% of cases. In addition, 54.2% of participants were prescribed orthoses, with 36.8% reported improvement in flatness and 37.6% reported improvement in symptoms.
It is assumed that the physiological maturation of the medial longitudinal arch occurs by the age of 10.12 In our study, 25.2% of the participants were first noticed/diagnosed to have flatfoot after the age of 10. Park et al studied children 15 years old and younger who presented to the hospital primarily due to parental concern and followed them up for more than a year and found that the improvement of flatfoot over time, as assessed by radiographic measurements, gets slower and more restricted as children become older than 10 years of ag.13 In addition, it has been reported that wearing insoles helps reduce the signs and symptoms of flatfoot, especially if used before the age of five.14 Therefore, age-appropriate treatment initiation is crucial for the success of the therapy. However, in a systemic review, they were unable to come to a definite conclusion on the age at which children’s foot posture stops to develop further.15 Moreover, the trend between the flatness improvement with age was found to be non-linear and within a wide range.16
In this study, 50.3% of the children were seen by a doctor, with the remaining being labeled with flatfoot without receiving a actual diagnosis from an orthopedic surgeon. Moreover, the most common presenting symptom was the abnormal external appearance of the foot among all age groups (78%). Other symptoms included shoes wearing out (24.8%), uncomfortable wearing shoes (24.3%), and pain (23.7%). Our findings are consistent with the literature, as most cases of flat foot are asymptomatic and parental concern about the external appearance is the most common cause of presentation to physicians.1,9,13,17 Furthermore, a third of the participants (35%) reported experiencing severe symptoms that interfered with their everyday activities, and 47.1% reported experiencing symptoms severe enough to prevent them from participating in sports or social events. In a cross-sectional study that included children aged between 5 and 18 years, it was found that there were significant decreases in the quality of life in the school functioning domain among children younger than 11 years of age.18 In addition, it has been reported previously that children with flexible flatfoot had significantly increased hindfoot eversion and forefoot supination during gait, which were significantly correlated with decreased quality of life.19
Among patients who were prescribed orthoses, 65.9% were told that orthoses would correct the flat foot. This inconsistency could be due to a lack of established evidence about the efficacy of orthoses. In a recent meta-analysis, they were unable to reach a conclusion on the effectiveness of foot orthoses in flatfoot; however, they did indicate that it may have a role in the reduction of pain in adults.11 Moreover, a recent study performed by Shin et al suggested that explaining to families that flatfoot spontaneously improves with time in addition to showing the expected time of skeletal maturity of the foot using calculations that include radiographic indices along with recognizing the factors that play a role in the rate of correction will help in preventing the financial and psychological burden on both parents and children caused by unnecessary treatment.20 Overall, 65.5% of the orthoses were prescribed by orthopedic surgeons and 24.4% by medical equipment and supply companies. The trend toward using orthoses could be attributed to clinicians’ intent to relieve parental concern. However, its excessive use can make children rely on them21 and lead to long-lasting negative psychological effects, as reported by adults who wore orthoses during childhood.22 Pfeiffer et al found that the vast majority of prescribed orthoses were not absolutely needed as only 1–2% of the children were symptomatic when they conducted the study.23 A recent Cochrane review conducted by Evans et al found that using foot orthoses to treat asymptomatic patients with flexible flatfoot is low to very low in evidence, whether they used custom-made orthoses or regular orthoses, supporting the idea that foot orthoses should not be used to correct the flatness.24
In our study, we found that 37.6% of the patient reported improvement in symptoms, indicating that more than half of patients did not benefit from this practice. However, the estimation of pain improvement is subjective and hard to validate because this may depend on parental personal characteristics and the child’s self-perception of pain. In a randomized control trial, Hsieh et al included 52 children with symptomatic flexible flatfeet and followed them up after 3 months; the interventional group was prescribed customized foot orthoses made by a senior physiatrist and instructed to wear them for at least 5 hours per day, and the study concluded that the intervention group improved significantly in terms of pain; however, the study lacks adequate sample size with a short-term follow-up period.25 Furthermore, a randomized control experiment found that custom-made orthoses were no superior to conventional orthoses, and prescription foot orthoses for asymptomatic individuals is only weakly supported by evidence.26 A much lower percentage (36.8%) of our studied patients reported a structural improvement in the shape of the foot after using foot orthoses. Two case-control studies compared radiographic parameters after applying custom-made orthopedic shoes to children aged 1 and 6 years7 and medial arch support insole to children aged 10 to 11 years27 to an age-controlled group. They found that structural radiographic improvements were found in both groups; nevertheless, the radiographic parameters remained in the abnormal range, and there was no significant changes between the flatfoot group compared to the controls.
The main limitation of this study is its cross-sectional design, which limited our ability to determine causal relationships. Although the questionnaire collected information from a wide geographical area, there was no exclusion criteria for any underlying medical condition, no control group, and no specific clinical assessment to measure the original deformity and/or improvement. Moreover, the study is subjected to recall bias since the data was self-reported and as this was an online survey, the flatfoot was self-reported, and no clinical examination or imaging was performed to confirm the diagnosis.
Conclusion
Our findings, in agreement with the literature, show that most of the participants have no or minimal symptoms, with the most prevalent presentation being an abnormal appearance of the foot. We also found a noticeable mismatch between patients’ expectations and the actual effectiveness of orthoses when used, where only around one-third noticed improvement in flatness and a little more in their symptoms. We recommend that physicians prescribing orthoses adhere more to their proper indications and spend more time and effort counseling and addressing patients’ and parents’ concerns about this developmental stage.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evans AM, Rome K, Peet L. Screening for foot problems in children: is this practice justifiable? J Foot Ankle Res. 2012;5(1):1–10. doi:10.1186/1757-1146-5-18
2. Aenumulapalli A, Kulkarni MM, Gandotra AR. Prevalence of flexible flat foot in adults: a cross-sectional study. J Clin Diagnos Res. 2017;11(6):AC17–AC20. doi:10.7860/JCDR/2017/26566.10059
3. Halabchi F, Mazaheri R, Mirshahi M, Abbasian L. Pediatric flexible flatfoot; clinical aspects and algorithmic approach. Iran J Pediatr. 2013;23(3):247–260.
4. Harris EJ, Vanore JV, Thomas JL, et al. Diagnosis and treatment of pediatric flatfoot. J Foot Ankle Surg. 2004;43(6):341–373. doi:10.1053/j.jfas.2004.09.013
5. Dars S, Uden H, Banwell HA, Kumar S. The effectiveness of non-surgical intervention (Foot Orthoses) for paediatric flexible pes planus: a systematic review: update. PLoS One. 2018;13(2):1–17. doi:10.1371/journal.pone.0193060
6. Pita-Fernandez S, Gonzalez-Martin C, Alonso-Tajes F, et al. Flat foot in a random population and its impact on quality of life and functionality. J Clin Diagn Res. 2017;11(4):LC22–LC27. doi:10.7860/JCDR/2017/24362.9697
7. Kanatlı U, Aktas E, Yetkin H. Do corrective shoes improve the development of the medial longitudinal arch in children with flexible flat feet? J Orthopaed Sci. 2016;21(5):662–666. doi:10.1016/j.jos.2016.04.014
8. Xu L, Gu H, Zhang Y, Sun T, Yu J. Risk factors of flatfoot in children: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(14):8247. doi:10.3390/ijerph19148247
9. Bouchard M, Mosca VS. Flatfoot deformity in children and adolescents: surgical indications and management. J Am Acad Orthopaed Surg. 2014;22(10):623–632. doi:10.5435/JAAOS-22-10-623
10. Bok SK, Kim BO, Lim JH, Ahn SY. Effects of custom-made rigid foot orthosis on pes planus in children over 6 years old. Ann Rehabil Med. 2014;38(3):369–375. doi:10.5535/arm.2014.38.3.369
11. Oerlemans LNT, Peeters CMM, Munnik-Hagewoud R, Nijholt IM, Witlox A, Verheyen CC. Foot orthoses for flexible flatfeet in children and adults: a systematic review and meta-analysis of patient-reported outcomes. BMC Musculoskelet Disord. 2023;24(1):16. doi:10.1186/s12891-022-06044-8
12. Choi JY, Hong WH, Suh JS, Han JH, Lee DJ, Lee YJ. The long-term structural effect of orthoses for pediatric flexible flat foot: a systematic review. Foot Ankle Surg. 2020;26(2):181–188. doi:10.1016/j.fas.2019.01.007
13. Park MS, Kwon SS, Lee SY, Lee KM, Kim TG, Chung CY. Spontaneous improvement of radiographic indices for idiopathic planovalgus with age. J Bone Joint Surg. 2013;95(24):1–8. doi:10.2106/JBJS.M.00301
14. Chen KC, Chen YC, Yeh CJ, Hsieh CL, Wang CH. The effect of insoles on symptomatic flatfoot in preschool-aged children: a prospective 1-year follow-up study. Medicine. 2019;98(36):e17074. doi:10.1097/MD.0000000000017074
15. Uden H, Scharfbillig R, Causby R. The typically developing paediatric foot: how flat should it be? A systematic review. J Foot Ankle Res. 2017;10:37. doi:10.1186/s13047-017-0218-1
16. Gijon-Nogueron G, Martinez-Nova A, Alfageme-Garcia P, Montes-Alguacil J, Evans AM. International normative data for paediatric foot posture assessment: a cross-sectional investigation. BMJ Open. 2019;9(4):e023341. doi:10.1136/bmjopen-2018-023341
17. Carr JB, Yang S, Lather LA. Pediatric pes planus: a state of the-art review. Pediatrics. 2016;137(3). doi:10.1542/peds.2015-1230
18. Damayanti Y, Hadisoemarto PF, Defi IR. Flatfoot decreases school functioning among children < 11 years of age. Universa Medicina. 2018;37:50–56. doi:10.18051/UnivMed.2018.v37.50-56
19. Kothari A, Dixon PC, Stebbins J, Zavatsky AB, Theologis T. The relationship between quality of life and foot function in children with flexible flatfeet. Gait Posture. 2015;41(3):786–790. doi:10.1016/j.gaitpost.2015.02.012
20. Shin BJ, Lee KM, Chung CY, et al. Analysis of factors influencing improvement of idiopathic flatfoot. Medicine. 2021;100(32):e26894. doi:10.1097/MD.0000000000026894
21. Helfet AJ. A new way of treating flat feet in children. Lancet. 1956;267(6922):578. doi:10.1016/S0140-6736(56)90627-4
22. Dare DM, Dodwell ER. Pediatric flatfoot: cause, epidemiology, assessment, and treatment. Curr Opin Pediatr. 2014;26(1):93–100. doi:10.1097/MOP.0000000000000039
23. Pfeiffer M, Kotz R, Ledl T, Hauser G, Sluga M. Prevalence of flat foot in preschool-aged children. Pediatrics. 2006;118(2):634–639. doi:10.1542/peds.2005-2126
24. Evans AM, Rome K, Carroll M, Hawke F. Foot orthoses for treating paediatric flat feet. Cochrane Database System Rev. 2022;2022(1). doi:10.1002/14651858.CD006311.pub3
25. Hsieh RL, Peng HL, Lee WC. Short-term effects of customized arch support insoles on symptomatic flexible flatfoot in children. Medicine. 2018;97(20). doi:10.1097/MD.0000000000010655
26. Whitford D, Esterman A. A randomized controlled trial of two types of in-shoe orthoses in children with flexible excess pronation of the feet. Foot Ankle Int. 2007;28(6):715–723. doi:10.3113/FAI.2007.0715
27. Choi JY, Lee DJ, Kim SJ, Suh JS. Does the long-term use of medial arch support insole induce the radiographic structural changes for pediatric flexible flat foot? — a prospective comparative study. Foot Ankle Surg. 2020;26(4):449–456. doi:10.1016/j.fas.2019.05.017
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.