Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
PD-L1 Biomolecules Associated with Clinical Features in Non-Melanoma Skin Cancer
Authors Li D, Ma L, Bao J, Cao L, Min W
Received 4 August 2022
Accepted for publication 18 November 2022
Published 4 January 2023 Volume 2023:16 Pages 1—8
DOI https://doi.org/10.2147/CCID.S383481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Dan Li,1 Liwen Ma,1 Jun Bao,1 Lei Cao,2 Wei Min3
1Department of Dermatology, the Affiliated Hospital of Nanjing University Medical School, Nanjing, People’s Republic of China; 2Clinical Immunology Laboratory, the First Affiliated Hospital of Soochow University, Soochow University, Suzhou, People’s Republic of China; 3Department of Dermatology, the First Affiliated Hospital of Soochow University, Soochow University, Suzhou, People’s Republic of China
Correspondence: Wei Min, Email [email protected]
Background: Increasing evidence has indicated that several B7 family members play critical roles in the progress of many cancers. However, the clinical significance of the B7 family in cutaneous squamous cell carcinoma (cSCC) is still elusive. The purpose of this study is to investigate the potential role of B7-H1 biomolecules (PD-L1) in regulating the tumorigenesis and progression of cSCC, the most common non-melanoma skin cancer.
Methods: We collected transcriptome data of cSCC patients from TCGA databases (n = 496) and subjected the transcription data to bioinformatical analysis. Differential expression of B7-H1 genes with a grade-dependent pattern was identified. We collected paraffin sections of skin squamous carcinoma and analyzed by immunohistochemical staining. We further examined the PD-L1 levels of CD14+ cells in peripheral blood of each cSCC patient and normal subjects by flow cytometry.
Results: It was found that higher expression of PD-L1 was associated with poor prognosis of cSCC patients and shorter overall survival. These observations were further verified in the clinical paraffin sections and in peripheral blood T cells.
Conclusion: Our study reveals that PD-L1 is a potential prognostic marker in clinical prognosis for cSCC patients and could be valuable for cSCC treatment.
Keywords: PD-L1, cutaneous squamous cell carcinoma, tumour progression, immunotherapy
Corrigendum for this paper has been published.
Introduction
Cutaneous squamous cell carcinoma (cSCC) is the second most common malignant tumor of the skin after basal cell carcinoma. The most common disease progression is from actinic keratosis (AK), which then develops into squamous cell carcinoma in situ, invasive cSCC, and finally metastatic cSCC.1 The incidence of cSCC is mainly related to long-term cumulative ultraviolet radiation, and other risk factors include virus infection, genetic and immune factors. In recent years, new targeted therapy drugs such as epidermal growth factor receptor inhibitors cetuximab, gefitinib and erlotinib, and PD-L1 inhibitor cimiprizumab, have been gradually applied in the clinical treatment of advanced metastatic cSCC and achieved certain effects.2,3 Although the majority of cSCC cases have a good prognosis, some cSCCs are highly metastatic and invasive, and their incidence is increasing at the rate of 2–4% per year.4 Therefore, new biological targets with anti-tumor metastatic invasion are needed to delay the late metastasis of cSCC and delay the survival of the disease.
Induced programmed death ligand 1(PD-L1, PD-L1, CD274), an inhibitory molecule of the B7 family.5 In 1999, Dong Haidong discovered this type I transmembrane protein structure, which is homologous to B7-1 and B7-2 and consists of immunoglobulin V and C-like domains, hydrophobic transmembrane protein domains and 30 amino acids, and named it as “PD-L1”.6 In chronic infections and tumors, PD-L1 binds to programmed cell death 1 (PD-1) to induce “failure” of T cells.7 According to Latchman et al, the effect of PD-L1 and PD-1 is to accelerate T cell apoptosis by blocking cell cycle rather than inducing cell death.8 In addition, PD-L1 has been reported to be highly expressed in various solid tumors including lung cancer,9 breast cancer,10 pancreatic cancer,11 renal cancer,12 colorectal cancer,13 gastric cancer,14 and cervical cancer,15 and it was found that the expression level of PD-L1 was significantly correlated with clinical performance. At present, immune checkpoint inhibitors targeting PD-1/PD-L1 and CTLA-4/B7 have been reported to be successfully used in cancer treatment.16,17 However, the expression and mechanism of PD-L1 in cutaneous non-dark skin cancer, especially squamous cell carcinoma, remain unclear.
Immune escape plays an important role in the recognition and regulation of immune checkpoint escape. Immune checkpoints include classical CTLA-4 and PD-1, and some of the molecules that discovered recently, such as B7-H3, CD47, and members of the SigLec-family (SigLec-7/9).18 They play an important role in initiating defensive immunity and maintaining immune tolerance.19 Immunosuppression mediated by the PD-L1/PD-1 signaling pathway has been shown to increase the apoptosis of antigen-specific human T cell clones in tumor tissues and cells and inhibit the activation of CD4+/CD8+T cells in vitro, thereby enhancing the immune tolerance of tumor cells and promoting immune escape.20,21 At present, PD-L1 inhibitors have been used in the evaluation of the efficacy of immunotherapy for patients with metastatic melanoma,22 which will bring a new direction for tumor immunotherapy.
In this study, we found that the negative costimulatory molecule PD-L1 was abnormally high expressed in skin squamous cell carcinoma tissues and peripheral blood CD14+ cells. PD-1 receptor was also highly expressed in peripheral blood T cells. In addition, we also analyzed the relationship between the expression level of PD-L1 and clinicopathological variables such as age, site, tumor size and pathological grade.
Materials and Methods
Bioinformatic Analysis
Transcriptome data that showed differential expression of cSCC were downloaded from TCGA cohorts. The genes expressed in the (807 over-expressed and 559 over-expressed genes) in cSCC were subjected to KEGG enrichment analysis. Kyoto Encyclopedia of Genes and Genomes (KEGG, http://www.kegg.jp/kegg/pathway.html). Gene Set Variation Analysis (GSVA package of R http://www.bioconductor.org/) was used to explore the correlation between B7-H1 and the prognosis predictor.
Patients and Clinical Specimens
Tissue samples were analyzed immunohistochemically. Primary tumor tissues specimens and control group tissues specimens were obtained by surgery and pathological diagnosis from 136 paraffin sections (96 cSCC, 20 AK, 20 Normal) without any chemotherapy or radiation therapy before surgery in the Dermatology and Orthopedics Department of the First Affiliated Hospital of Soochow University between 2009 and 2015. Cutaneous squamous cell carcinoma and actinic keratosis were confirmed by hematoxylin and eosin (H&E) staining after surgical resection. The average age ranged from 20 to 85 years (47 males,49 females). This study was approved by the Ethics Committee of our hospital, and all patients provided written informed consent before enrolment.
Blood Samples
Blood samples were collected from 15 patients with cutaneous squamous cell carcinoma and 10 health people in the wards of the First Affiliated Hospital of Soochow University. All patients with skin squamous cell carcinoma were first diagnosed with skin squamous cell carcinoma. Exclusion criteria include the following:
I) patients with autoimmune diseases;
II) patients taking immunosuppressive drugs;
III) HIV-positive patients;
IV) patients with other tumors.
Separation of PBMCs
Peripheral blood mononuclear cells (PBMCs) were isolated from EDTA-treated peripheral blood by a standard density gradient centrifugation (Ficoll R&D, USA) (25 min, 400 g, 22°C). The cells were washed twice in phosphate buffered saline (PBS).
Immunohistochemistry
Immunohistochemistry was used to detect the expression of PD-L1 in cSCC, actinic keratosis, and normal skin tissue. All the surgically resected specimens were fixed with 10% neutral buffer formalin and made into 4-cm serial paraffin-embedded sections. The paraffin section was dipped into the repair solution for deparaffinating and rinsed with PBS every 30 min for 3 min each time. After dehydration with alcohol, the tissue slices were incubated with hydrogen peroxide at 25 °C to block endogenous peroxidase and rinsed with PBS every 10 min for three times. The deparaffined tissues were co-incubated with 5% BSA solution for 1 h. Sections were incubated with PD-L1 primary antibody followed by secondary antibody and colored by diaminobenzidine (DAB). PBS was rinsed to remove the excess antibodies. Diaminobenzene was used as the chromogen and hematoxylin as the nuclear counterstain. Sections were dehydrated, cleared and mounted.
Immunohistochemical results were evaluated by microscopic observation. The score was quantified by the the tumor tissue staining intensity multiplied by the percentage of positive tumor cells. Tumor tissue-staining intensity was determined as follows:1, pale yellow; 2, brown yellow; 3, tan. The percentage of positive tumor cells was determined as follows: 0, <5%; 1, 5–25%; 2, 50–70%; 3, >70%. Three certified pathologists were blinded to evaluate the scores and achieved the consensus results.
Flow Cytometry
Peripheral blood were collected and incubated with anti-PD-L1, CD3, CD4, CD8 and CD14 monoclonal antibodies (R&D Systems, Abingdon, UK & Europe) at room temperature for 30 min. The labeled cells were resuspended in a 0.5 mL cell staining buffer and examined by flow cytometry. The analysis was performed using flow cytometry (Flowjo software, USA). Isotype controls were set for each stain.
Statistical Analysis
The χ2 test was used to analyze the associations between the expression of PD-L1 and clinical parameters (gender, age, and tumor risk factors). Statistical analysis and mapping were performed using SPSS 11.0 and GraphPad Prism 8.0 software. Statistical significance was set at P<0.05.
Results
PD-L1 Expression in Normal, AK, and cSCC Tissue Simples
To understand the function of PD-L1 and obtain comprehensive insights into their clinical correlations with cSCC, we firstly analyzed the RNA expression data of 496 patients from The Cancer Genome Atlas (TCGA) database. We identified differential expression of PD-L1 genes with a grade-dependent pattern. The results show that B7-H1 was frequently expressed in cSCC (Figure 1A). It is also worth noting that the expression level of PD-L1 significantly correlates with the survival times of cSCC patients (Figure 1B). Higher expression of PD-L1 was associated with poor outcomes in cSCC patients. These results indicate that the expression of PD-L1 may play important regulatory role in the progress of cSCC tumors.
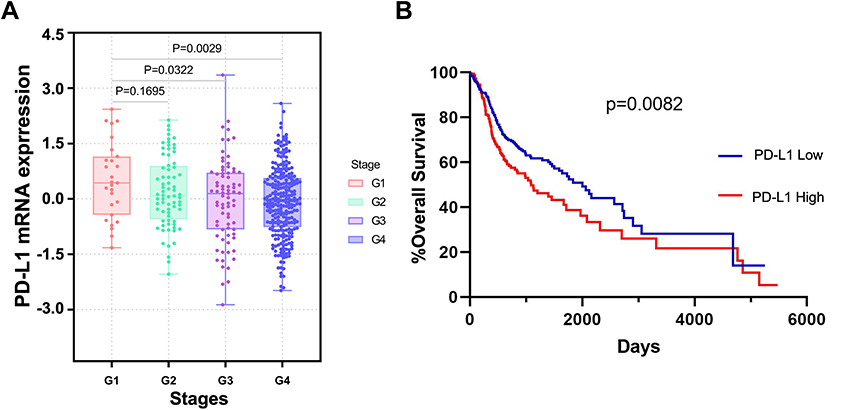 |
Figure 1 The expression of PD-L1 in cSCC in TCGA dataset. (A) The expression of PD-L1 in each grade of cSCC. (B) Kaplan-Meier analysis showed the prognosis value of PD-L1 in cSCC. |
To further delineate the clinical significance of the PD-L1 gene signature expressed in cSCC, 96 cases of paraffin sections of skin squamous carcinoma, 20 cases of solar keratosis (precancerous lesion), and 20 cases of normal epithelial tissue were analyzed by immunohistochemical staining. Immunohistochemical staining showed that the expression of PD-L1 in normal skin tissues, actinic keratosis tissues, and cSCC tissues. The results showed that the expression of PD-L1 was higher in actinic keratosis and cSCC tissues, but lower in normal skin tissues (Figure 2A-C). Immunohistochemical results were evaluated by microscopic observation. The score was based on the degree of staining of the tumor tissue, and the proportion of positive cells was then scored using a secondary scoring system (Figure 2D). However, PD-L1 with pathologic correlation analysis found that PD-L1 levels in cSCC patients with occurrence and development of tumor low risk factors such as age, gender, and high-risk factors such as whether the tumor is located in the exposed parts, tumor size, and whether lymph node metastasis and tumor cell differentiation degree had no correlation (P>0.05; Table 1).
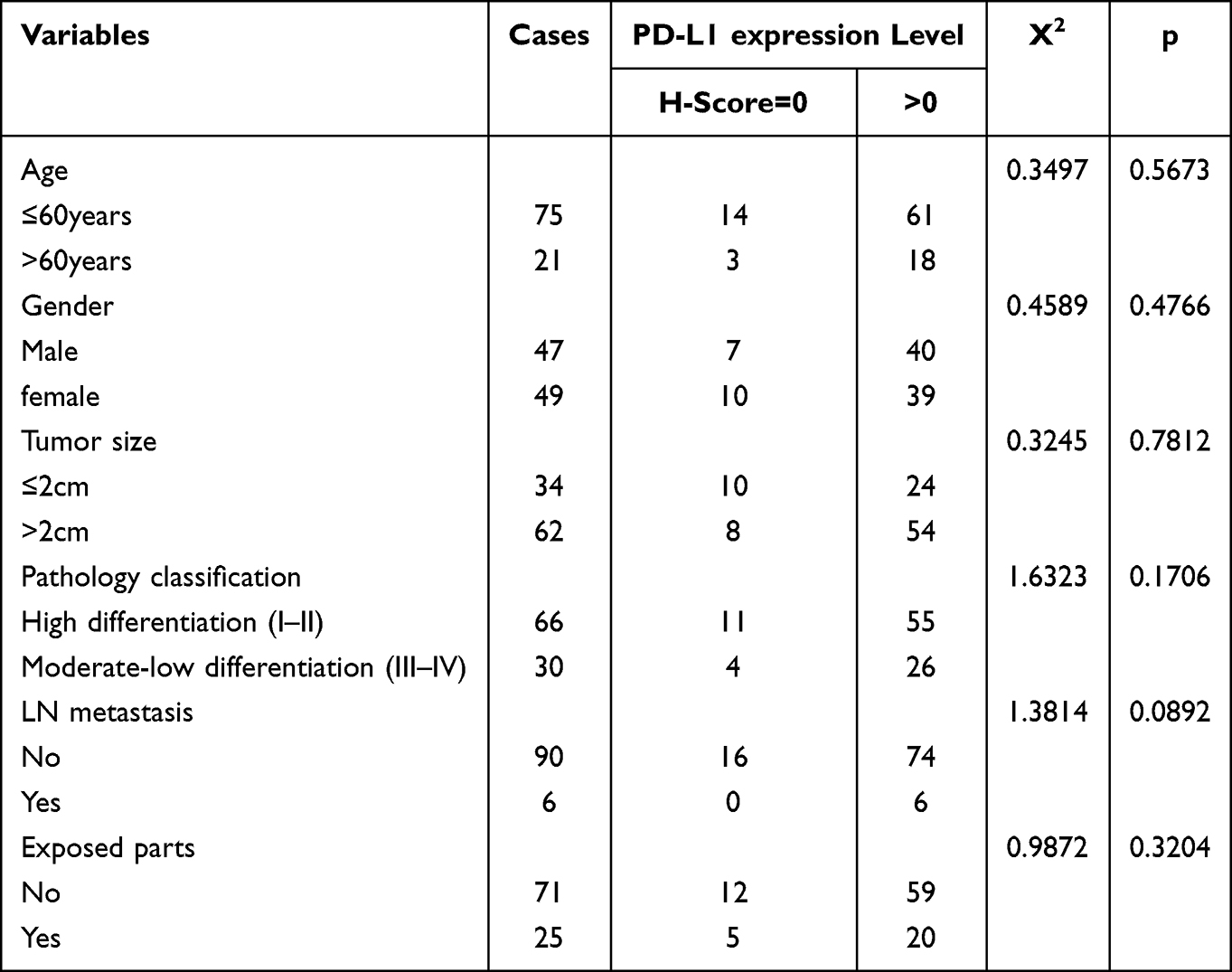 |
Table 1 Correlation Between PD-L1 Expression and Pathological Findings of cSCC Patients |
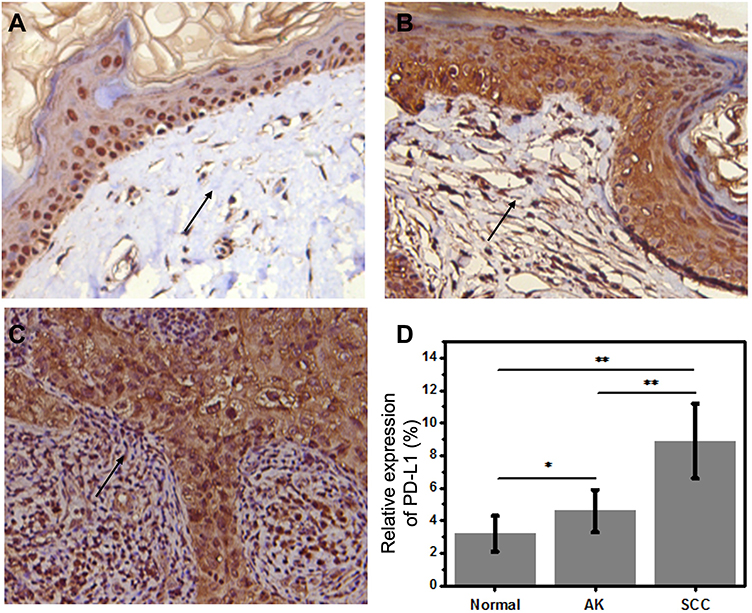 |
Figure 2 Immunohistochemical staining of expression of the PD-L1 molecule in different skin tissues (IHC). (A) PD-L1 negative expression in normal skin tissues. (B and C) PD-L1 positive expression in actinic keratosis and cSCC tissues. Magnification: 400×. (D) PD-L1 level as shown by a secondary scoring system. Arrows show the expression of PD-L1 in the tissue. (*P<0.05; **P<0.01). |
Expression of PD-L1 in CD14+ Cells in Peripheral Blood of Patients with cSCC
In order to evaluate the immune status especially the immune escape in cSCC, we first examined the PD-L1 levels of CD14+ monocyte cells in peripheral blood of each cSCC patient and normal subjects by flow cytometry. Compared to normal subjects, the results showed that PD-L1 was highly expressed on CD14+ cells in the peripheral blood of patients with cutaneous squamous cell carcinoma (Figure 3A). The flow cytometry results were analyzed statistically (Figure 3B).
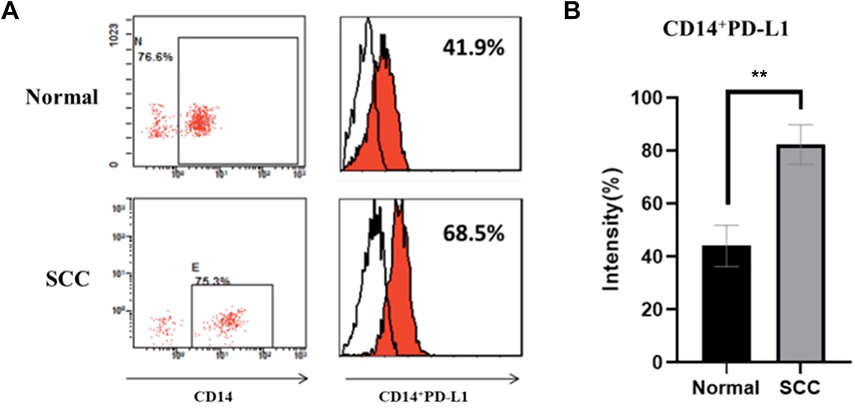 |
Figure 3 Flow cytometric analysis of PD-L1 molecules on CD14+ cells in peripheral blood of normal and cSCC patients. (A) The expression of PD-L1 on CD14+ cells in peripheral blood of healthy controls and skin squamous cell carcinoma patients. (B) Statistical analysis of flow cytometry results showed a significant difference in PD-L1 expression between patients with squamous cell carcinoma and the control group.(**P<0.01). |
Expression of PD-1 in CD3+CD4+/CD3+CD8+ in Peripheral Blood T Cells of Patients with cSCC
PD-1 expression level of CD3+CD4+/CD3+CD8 in peripheral blood T cells of normal person and patients with cutaneous squamous cell carcinoma was detected by flow cytometry (Figure 4A and B). Our results showed that PD-1 was also highly expressed in peripheral blood T cells of patients with skin squamous cell carcinoma (Figure 4C and D).
 |
Figure 4 Flow cytometric analysis of CD3+CD4+ PD-1 and CD3+CD8+ PD-1 expression in peripheral blood T cells of normal and cSCC patients. (A) peripheral blood T cells of normal persons. (B) peripheral blood T cells of cSCC. (C) Statistical analysis of flow cytometry results showed abnormally high expression of CD3+CD4+ PD-1 in peripheral blood T cells of patients with cSCC.(*P<0.05;**P<0.01). (D) Statistical analysis of flow cytometry results showed abnormally high expression of CD3+CD8+ PD-1 in peripheral blood T cells of patients with skin squamous cell carcinoma. (**P<0.01). |
Discussion
As a type I transmembrane protein, PD-L1 is a hot molecule of the B7 family in recent years. It is expressed in hematopoietic cells, B cells, T cells, dendritic cells (DCs) and macrophages, and acts with the PD-1 receptor on activated T cells, B cells and bone marrow cells.5 In 1999, Dong et al reported for the first time that PD-L1 was involved in the negative regulation of specific cellular immune response.6 Tyler J. Curiel et al also demonstrated that blocking PD-L1 on myeloid dendritic cells (MDC) in the tumor microenvironment enhances T cell activation.23 In addition, the use of PD-L1 blocking antibodies increases the number of tumor-infiltrating immune cells, especially CD8+T cells.24,25 It has recently been reported that the interaction between PD-L1 on multiple myeloma cells and PD-1 on NK cells can limit NK cell-mediated anti-tumor response.26 Therefore, we concluded that tumors may escape anti-tumor immunity through two independent PD-L1 pathways:1. The effector T cells producing IFN-c were reduced by PD-L1; 2. Reduction of NK cell response by PD-L1.
The expression of PD-L1 in 96 patients with cSCC was studied at cell, blood and tissue levels. Our results showed that PD-L1 was highly expressed in the precancerous lesions of skin cancer and cSCC tissues, and the expression level was not significantly correlated with the age, gender, and tumor risk factors of the patients. This is consistent with findings in patients with melanoma and non-small cell lung cancer.27 It is suggested that PD-L1 plays an important role in the process from normal skin tissue to precancerous lesions and then to cutaneous squamous cell carcinoma, but it cannot be used as an indicator for the recurrence and prognosis of skin cancer. We also found that the ligand PD-1 of PD-L1 was also highly expressed on peripheral blood T cells of patients with cSCC, which further suggested that the PD-L1 molecule may transmit inhibitory signals through the receptor PD-1, reduce the immune effector of T cells in the local microenvironment, make the immune escape of mutated cells, and promote the occurrence and development of cutaneous squamous cell carcinoma.28,29 Previous studies have demonstrated that the PD-L1 molecule promotes tumorigenesis through antiapoptosis and epithelial to mesenchymal transition (EMT) of tumor cells. Azum’s study also showed that PD-L1 molecules can transmit growth-inhibiting signals to tumors.30 The PD-1 suggest the tolerance signal on immune system. The highly expressed PD-1 in CD3+CD4+/CD3+CD8 cells can lead to T death and thus inducing the tumor escape from T cells. It has also been well established that PD-L1 is an immunosuppressive molecule, so it is no surprise to find that expression of PD-L1 on CD14 + cells is upregulated and contributes to the potent suppressor activity of the cells. Previous studies have demonstrated that monocytes exposed to glioma tumor have immunosuppressive properties and a higher level of B7-H1 (PD-L1) expression. Therefore, PD-L1 expression in CD14 + cells may confer additional immunosuppressive properties to these patients with cSCC. Therefore, we speculated that PD-L1 may be involved in the biological behavior of cSCC as a functional molecule, playing a role in maintaining its proliferation and invasion. This suggests that targeting PD-L1 inhibitors may provide a new target for immunotherapy of skin squamous cell carcinoma.
In the development of tumor immunotherapy, drug resistance of immune checkpoint inhibitors has been gradually discovered and become an urgent problem to be solved. Liye Zhou et al found that in the process of targeting PD-1-blocking drugs for head and neck squamous cell carcinoma, patients showed a good prognosis, but the clinical response rate was very low. They believed that the mechanism of drug resistance might be related to the disorder of tumor cell antigen presentation mediated by the missing HLA-I antigen. In patients with cervical cancer, only 17% of patients with tumor responded to PD-L1 antagonist therapy, and this result was inversely correlated to the PD-L1 expression level. Therefore, the role of PD-L1 in tumor drug resistance remains to be further studied.
Conclusions
Overall, our study provides preliminary evidence that PD-L1 is highly expressed in cSCC and is correlated with the outcomes of cSCC. PD-L1 could be a potential indicator for the prognosis of cSCC. Our findings have important implications for the understanding of the carcinogenesis and progression of cSCC, which will provide an important indicator for the clinical diagnosis and therapeutic strategies for cSCC.
Ethics Statement
This study complies with the Declaration of Helsinki. All samples were collected from The First Affiliated Hospital of Soochow University. Informed consent was obtained from all patients, and ethical approval was obtained from the Ethics Committee of The First Affiliated Hospital of Soochow University (approval No. 2020-280).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We gratefully acknowledge the support of the Jiangsu Institute of Clinical Immunology of The First Affiliated Hospital of Soochow University and Dr. Lei Cao.
Funding
This research was supported by grants from the Jiangsu National Science Foundation (BK2012170), science project from the traditional Chinese Medicine Bureau of Jiangsu Province (LZ1109).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cheng R, Chen Y, Zhou H, Wang B, Du Q, Chen Y. B7-H3 expression and its correlation with clinicopathologic features, angiogenesis, and prognosis in intrahepatic cholangiocarcinoma. Apmis. 2018;126:396–402.
2. Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma: incidence, risk factors, diagnosis, and staging. J Am Acad Dermatol. 2018;78:237–247. doi:10.1016/j.jaad.2017.08.059
3. Migden MR, Rischin D, Schmults CD, et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N Engl J Med. 2018;379:341–351. doi:10.1056/nejmoa1805131
4. Soura E, Gagari E, Stratigos A. Advanced cutaneous squamous cell carcinoma: how is it defined and what new therapeutic approaches are available? Curr Opin Oncol. 2019;31:461–468. doi:10.1097/CCO.0000000000000566
5. Kythreotou A, Siddique A, Mauri FA, Bower M, Pinato DJ. Pd-L1. J Clin Pathol. 2018;71:189–194. doi:10.1136/jclinpath-2017-204853
6. Dong H, Zhu G, Tamada K, Chen L. PD-L1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nat Med. 1999;5:1365–1369. doi:10.1038/70932
7. Wherry EJ, Kurachi M. Molecular and cellular insights into T cell exhaustion. Nat Rev Immunol. 2015;15:486–499. doi:10.1038/nri3862
8. Latchman Y, Wood CR, Chernova T, et al. PD-L2 is a second ligand for PD-1 and inhibits T cell activation. Nat Immunol. 2001;2:261–268. doi:10.1038/85330
9. Wrona A. Role of immunotherapy in stage III nonsmall cell lung cancer. Curr Opin Oncol. 2019;31:18–23. doi:10.1097/CCO.0000000000000493
10. Karasar P, Esendagli G. T helper responses are maintained by basal-like breast cancer cells and confer to immune modulation via upregulation of PD-1 ligands. Breast Cancer Res Treat. 2014;145:605–614. doi:10.1007/s10549-014-2984-9
11. Wang L, Ma Q, Li D, et al. Indoleamine 2, 3-dioxygenase and PD-L1 expressions as prognostic and follow-up markers in human pancreatic carcinoma. Pathol Res Pract. 2018;214(9):1309–1314. doi:10.1016/j.prp.2018.02.016
12. Safaei HR, Rostamzadeh A, Rahmani O, et al. Prognostic investigations of PD-L1 and B7-H4 expression levels as independent predictor markers of renal cell carcinoma. Tumor Biol. 2016;37(6):7583–7587. doi:10.1007/s13277-015-4652-z
13. Zhao L, Li C, Zhang R-L, et al. PD-L1 and B7-H4 expression in colorectal carcinoma: correlation with tumor FOXP3+ regulatory T-cell infiltration. Acta Histochem. 2014;116:1163–1168. doi:10.1016/j.acthis.2014.06.003
14. Geng Y, Wang H, Lu C, et al. Expression of costimulatory molecules PD-L1, B7-H4 and Foxp3+ Tregs in gastric cancer and its clinical significance. Int J Clin Oncol. 2015;20:273–281. doi:10.1007/s10147-014-0701-7
15. Tao J, Dai J, Hou S. Association between PD-L1 and cervical cancer: PD-L1 impairs the immune response in human cervical cancer cells. Exp Ther Med. 2017;14:4125–4133. doi:10.3892/etm.2017.5100
16. Barrios DM, Do MH, Phillips GS, et al. Immune checkpoint inhibitors to treat cutaneous malignancies. J Am Acad Dermatol. 2020;83:1239–1253. doi:10.1016/j.jaad.2020.03.131
17. Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28:3167–3175. doi:10.1200/JCO.2009.26.7609
18. Khan M, Arooj S, Wang H, Cell-Based Immune NK. Checkpoint Inhibition. Front Immunol. 2020;11:548.
19. Haanen JBAG, Robert C. Immune Checkpoint Inhibitors. Prog Tumor Res. 2015;42:55–66.
20. Jiang X, Wang J, Deng X, et al. Role of the tumor microenvironment in PD-L1/PD-1-mediated tumor immune escape. Mol Cancer. 2019;18:1–17. doi:10.1186/s12943-018-0928-4
21. Watanabe N, Gavrieli M, Sedy JR, et al. BTLA is a lymphocyte inhibitory receptor with similarities to CTLA-4 and PD-1. Nat Immunol. 2003;4:670–679. doi:10.1038/ni944
22. Kakavand H, Rawson RV, Pupo GM, et al. PD-L1 expression and immune escape in melanoma resistance to MAPK inhibitors. Clin Cancer Res. 2017;23:6054–6061. doi:10.1158/1078-0432.CCR-16-1688
23. Curiel TJ, Wei S, Dong H, et al. Blockade of PD-L1 improves myeloid dendritic cell-mediated antitumor immunity. Nat Med. 2003;9:562–567. doi:10.1038/nm863
24. Raez LE, Cassileth PA, Schlesselman JJ, et al. Allogeneic vaccination with a B7.1 HLA-A gene-modified adenocarcinoma cell line in patients with advanced non-small-cell lung cancer. J Clin Oncol. 2004;22:2800–2807. doi:10.1200/JCO.2004.10.197
25. Taube JM, Anders RA, Young GD, et al. Colocalization of inflammatory response with PD-L1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med. 2012;4. doi:10.1126/scitranslmed.3003689
26. Benson DM, Bakan CE, Mishra A, et al. The PD-1/PD-L1 axis modulates the natural killer cell versus multiple myeloma effect: a therapeutic target for CT-011, a novel monoclonal anti-PD-1 antibody. Blood. 2010;116:2286–2294. doi:10.1182/blood-2010-02-271874
27. Gadiot J, Hooijkaas AI, Kaiser ADM, et al. Overall survival and PD-L1 expression in metastasized malignant melanoma. Cancer. 2011;117(10):2192–2201. doi:10.1002/cncr.25747
28. Alsaab HO, Sau S, Alzhrani R, et al. PD-1 and PD-L1 checkpoint signaling inhibition for cancer immunotherapy: mechanism, combinations, and clinical outcome. Front Pharmacol. 2017;8:1–15. doi:10.3389/fphar.2017.00561
29. Bagir EK, Acikalin A, Avci A, Gumurdulu D, Paydas S. PD-1 and PD-L1 expression in thymic epithelial tumours and non-neoplastic thymus. J Clin Pathol. 2018;71:637–641. doi:10.1136/jclinpath-2017-204788
30. Yao Y, Tao R, Wang X, et al. PD-L1 is correlated with malignancy-grade gliomas but is not expressed exclusively on tumor stem-like cells. Neuro Oncol. 2009;11:757–766. doi:10.1215/15228517-2009-014
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cemiplimab for the Treatment of Advanced Cutaneous Squamous Cell Carcinoma: Appropriate Patient Selection and Perspectives
Mager L, Gardeen S, Carr DR, Shahwan KT
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2135-2142
Published Date: 9 August 2023