Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Cemiplimab for the Treatment of Advanced Cutaneous Squamous Cell Carcinoma: Appropriate Patient Selection and Perspectives
Authors Mager L, Gardeen S, Carr DR, Shahwan KT
Received 7 April 2023
Accepted for publication 25 July 2023
Published 9 August 2023 Volume 2023:16 Pages 2135—2142
DOI https://doi.org/10.2147/CCID.S381471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Layna Mager,1,* Samantha Gardeen,2,* David R Carr,3 Kathryn T Shahwan3– 5
1College of Medicine, The Ohio State University, Columbus, OH, USA; 2Division of Dermatology, HealthPartners, Minneapolis, MN, USA; 3Department of Dermatology, The Ohio State University Medical Center, Columbus, OH, USA; 4Department of Dermatology, Altru Health System, Grand Forks, ND, USA; 5Department of Internal Medicine, University of North Dakota, Grand Forks, ND, USA
*These authors contributed equally to this work
Correspondence: Kathryn T Shahwan, Email [email protected]
Abstract: Five percent of patients with cutaneous squamous cell carcinoma develop locally advanced or metastatic disease that is not amenable to definitive surgical or radiation therapy. Cemiplimab, an antibody against programmed death receptor-1, was approved in the United States for the treatment of locally advanced and metastatic cutaneous squamous cell carcinoma in 2018. We performed a literature review on the use of cemiplimab in cutaneous squamous cell carcinoma, with an emphasis on efficacy, safety and tolerability, patient selection, and future directions. Embase and PubMed were searched for relevant terms, and 23 peer-reviewed journal articles presenting primary data on cemiplimab treatment in 5 or more subjects with cutaneous squamous cell carcinoma were included and summarized. Objective response rates in locally advanced and metastatic disease ranged from 42.9% to 50.8% in Phase I/II clinical trials and 32– 77% (median 58%) in post-approval observational studies. Phase II trials looking at neoadjuvant use also had favorable response rates. Real-world studies demonstrated cemiplimab efficacy in periorbital tumors, tumors with large caliber perineural invasion, and tumors in solid organ transplant recipients. Cemiplimab was safe and well-tolerated in most patients. While side effects such as fatigue, diarrhea, pruritus, and rash were fairly common, only 9.8% of adverse events required cessation of therapy in phase II trials. Severe adverse events were primarily immune-mediated, including pneumonitis, myocarditis, myositis, and autoimmune hepatitis; the risk of treatment-related death was 3% in clinical trials. Further research on cemiplimab therapy in cutaneous squamous cell carcinoma is needed, and trials are now underway to obtain Phase IV long-term real-world data, further data on adjuvant and neoadjuvant use, and additional data in special populations such as stem cell and solid organ transplant recipients.
Keywords: cutaneous squamous cell carcinoma, cemiplimab, immunotherapy, immune checkpoint inhibitor, programmed death receptor-1 inhibitor
Introduction
Cutaneous squamous cell carcinoma (CSCC) is the second most common type of skin cancer. Major risk factors for CSCC include chronic sun exposure, immunosuppression, and advancing age.1 Although most CSCCs are low-risk and curable with surgical intervention, a subset of tumors display an aggressive phenotype and have a higher risk of poor outcomes including local recurrence, nodal metastasis, distant metastasis, and disease-specific death. High-risk factors that have been associated with poor outcomes include larger clinical diameter, greater depth of invasion, perineural invasion (PNI), and poor differentiation.2,3 As the incidence of CSCC continues to increase, the morbidity is estimated to surpass that of melanoma over the next 5 years.4
Approximately 5% of patients with advanced cutaneous squamous cell carcinoma (aCSCC), including locally advanced (laCSCC) and metastatic CSCC (mCSCC), are not curable by surgical or radiation therapy.5,6 Previous systemic treatment options for aCSCC were limited to cytotoxic chemotherapy and anti-epidermal growth factor receptor (EGFR) therapy, with significant morbidity and poor durable response rates.7 CSCC has a high mutational burden, and immune surveillance is critical to its pathogenesis,8 leading to the investigation of immunotherapy options for advanced cases. In 2018, cemiplimab (Libtayo®; Regeneron, Tarrytown, New York, United States) - a human IgG4 antibody against programmed death receptor-1 (PD-1) – was approved by the United States Food and Drug Administration (US-FDA) for the treatment of laCSCC and mCSCC not amenable to definitive surgery or radiation.9 We performed a literature review to summarize the data on the use of cemiplimab in CSCC, including effectiveness, safety and tolerability, and appropriate patient selection.
Methods
An electronic literature search was conducted in Embase and PubMed using terms related to cemiplimab and cutaneous squamous cell carcinoma, from database inception through November 7, 2022. Additional articles were identified by searching reference lists of included articles. Articles were included if they were published in peer-reviewed journals and presented primary data on five or more patients with CSCC treated with cemiplimab. Articles were excluded when CSCC data could not be separated from other tumor types, or when cemiplimab data could not be separated from other forms of treatment. The titles and abstracts, followed by the full texts of the remaining articles, were sorted by two reviewers (LM and SG). Conflicts were resolved by a third reviewer (KS).
Results
The database search resulted in 338 articles, 23 of which met criteria and were included in the literature review.
Efficacy of Cemiplimab in Advanced CSCC
Phase I Trial Data
From March 2016 to January 2017, an open-label, multi-institutional phase I study was completed to evaluate the safety and tolerability of cemiplimab in patients with locally advanced or metastatic CSCC.10 Patients with a history of autoimmune disease treated with immunosuppressive medication within the last 5 years, prior anti-PD-1/PD ligand (PDL)-1 therapy, solid organ transplantation, and significant concurrent malignancies were excluded. A total of 26 patients with a median age of 73 years (range 55–88) received intravenous cemiplimab at a dose of 3 mg per kilogram (mg/kg) every 2 weeks for up to 48 weeks, or until they developed unacceptable side effects or disease progression.10 Patients were evaluated by whole-body imaging every 8 weeks, and treatment response was measured by the Response Evaluation Criteria in Solid Tumors (RECIST) system, version 1.1.11 At a median follow-up time of 11 months, the objective response rate (ORR) was 50% (95% confidence interval [CI] 30–70%) with a median observed time to response of 2.3 months (range 1.7–7.3). Additionally, the durable disease control rate (DCR; defined as the percentage of subjects without disease progression at 105 days) was 65% (95% CI 44–83%), and 54% of responders experienced a response lasting over 6 months.10 Table 1 contains a summary of phase I clinical trial data.
 |
Table 1 Efficacy Data from Phase I and Phase II Clinical Trials Evaluating Cemiplimab for the Treatment of Advanced Cutaneous Squamous Cell Carcinoma |
Phase II Trial Data
Phase II trials evaluated the efficacy of cemiplimab for locally advanced CSCC, metastatic CSCC, and neoadjuvant treatment of resectable CSCC. In both the locally advanced and metastatic CSCC trials, subjects were excluded if they were immunosuppressed (including solid organ transplant patients) or had other concurrent malignancies.10,12–14 For locally advanced CSCC not curable with resection or radiotherapy (labeled Group 2 in the combined data), 78 subjects were treated with intravenous cemiplimab 3 mg/kg IV every 2 weeks for up to 96 weeks.12,13 At a median duration of follow-up of 15.5 months, the ORR was 44.9% (95% CI 33.6–56.6%) with a complete response (CR) rate of 12.8% and a partial response (PR) rate of 32.1%. The durable DCR was 62.8% (95% CI 51.1–73.5%), and median time to response was 2.1 months.13 Tumors with a wide range of PDL-1 expression and mutational burden responded to cemiplimab therapy.12
For metastatic CSCC, both weight-based dosing (3 mg/kg every 2 weeks; Group 1) and fixed dosing (350 mg every 3 weeks; Group 3) for up to 96 weeks were evaluated.10,13,14 Group 1 had 59 subjects, and Group 3 had 56. At a median duration of follow-up of 18.5 months for Group 1 and 17.3 months for Group 3, the ORRs were 50.8% (95% CI 37.5–64.1%) and 42.9% (95% CI 29.7–56.8%), respectively.13 This included CR rates of 20.3% for Group 1 and 16.1% for Group 3. The durable DCRs were 61% (95% CI 47.4–73.5%) for Group 1 and 57.1% (95% CI 43.2–70.3%) for Group 3.13 Efficacy was comparable in subjects with nodal and distant metastases.10
In a pooled analysis combining all laCSCC and mCSCC data, median duration of response was not reached by the study end date, and 87.8% (95% CI 78.5–93.3%) of responders were estimated to have an ongoing response at 1 year.13 Median progression-free survival (PFS) and median overall survival (OS) were also not reached by the end of the study. However, Kaplan–Meier curves estimated the median PFS to be 18.4 months (95% CI 10.3–24.3), and the probability of PFS and OS at 24 months to be 44.2% (95% CI 36.1–52.1%) and 73.3% (95% CI 66.1–79.2%), respectively.13 Quality of life scores improved as early as cycle 2, with statistically significant improvement by cycle 3 and clinically meaningful improvement (≥10-point change) by cycle 12. This included significant improvement in emotional functioning, social functioning, and pain.13
Two phase II studies evaluated neoadjuvant cemiplimab therapy for resectable CSCC.15,16 Gross et al included American Joint Commission on Cancer 8th Edition (AJCC-8) stage T2 tumors that were at least 3 cm in diameter, T3 tumors, and T4 tumors located on any anatomic site. Seventy-nine subjects received intravenous cemiplimab 350 mg every 3 weeks for up to 4 cycles prior to definitive resection. The pathologic complete response rate (defined as no tumor cells present on the excision specimen) was 53%, and the pathologic major response rate (defined as tumor cells in up to 10% of the excision specimen) was 13%. ORR by imaging (using RECIST 1.1) was 68%, with 6% having a complete response and 62% a partial response.15 Ferrarotto et al included only T3 and T4 (by AJCC-8) head and neck CSCCs. Twenty subjects (including 13 primary and 7 recurrent tumors) received 2 doses of cemiplimab 350 mg every 3 weeks prior to resection. The ORR was 30% (95% CI 11.9–54.3%), with all having a partial response by RECIST 1.1. A pathologic response was seen in 75% of subjects, including a complete response in 55% and a major response in 20%.16 Table 1 contains a summary of phase II clinical trial data.
Real World Efficacy Data
Post-approval observational studies of cemiplimab for the treatment of CSCC are important to review as they include a broader range of patients treated in real-world settings. This includes patients with advanced age, multiple comorbidities, lower performance status, and immunosuppression. Overall, the ORR ranged from 32% to 77% in observational studies, with a mean of 55% and a median of 58%. This includes partial response rates ranging from 23% to 47% and CR rates ranging from 8% to 33%.17–24 The DCR ranged from 47% to 72% in real-world studies, with a median of 62%.18–20,24,25 Factors associated with higher response rates included age,20 higher performance status, and primary tumors on the head and neck.21,23 Immune status,21 frailty, sex, and body mass index (BMI) did not impact response rates.23 Median duration of response was 12 months in one study,24 and was not reached in others.19,21 Median progression-free survival, when reached by data cut-off, ranged from 5.9 to 9.13 months.19–22 Overall, efficacy in the real-world setting has been comparable to that seen in clinical trials.
One retrospective cohort study evaluated the effect of cemiplimab and radiotherapy combination therapy compared to cemiplimab treatment alone. This resulted in an ORR of 41.6% in the combination therapy group and 47.6% in the cemiplimab monotherapy group. However, the combination therapy group demonstrated an earlier radiologic disease response, with a median duration of 3 months (versus 5.5 months in the monotherapy group) and a prolonged treatment response even after discontinuation of PD-1 blockade.26
Several studies evaluated unique scenarios, such as the use of cemiplimab to treat periorbital CSCC, CSCC with large caliber PNI, and CSCC in SOTRs. For periorbital CSCC, treatment with cemiplimab resulted in response rates between 82% and 100% and negated the need for orbital exenteration in most cases.27–29 In a single center retrospective cohort study evaluating the response of large caliber PNI to immunotherapy, all seven subjects treated with cemiplimab experienced stable or improved neurologic symptoms, one had a complete radiologic response, and five had partial radiologic responses.30 While most real-world studies did not include transplant recipients, Tsung et al studied the use of cemiplimab in six solid organ transplant recipients (SOTRs) with metastatic head and neck CSCC. The DCR in this study was 83%, including one subject with stable disease, three with a partial response, and one with a complete response. Half of the subjects received a systemic steroid regimen as prophylaxis for organ rejection, and one subject in the group that did not receive steroids developed rejection.31
An Italian multi-institutional retrospective study evaluated the impact of the coronavirus-19 (COVID-19) pandemic on cemiplimab treatment in CSCC. In a cohort of 54 patients, 57% continued treatment and 31% stopped due to the pandemic. Only two patients, both of whom were hospitalized at the time, were infected with COVID-19; both patients died of COVID-19 pneumonia. The authors noted the overall safety of immunotherapy during the pandemic and cautioned against stopping treatment due to the risk of tumor progression.32
Finally, two retrospective studies evaluated the use of PET-CT to assess response to cemiplimab treatment. Historically, CT and MRI are used to monitor response to therapy according to the RECIST 1.1 system. In these studies, PET-CT (using the PERCIST 1.0 grading system) performed well in monitoring response to therapy.33,34 McLean et al demonstrated that tumor responses were discordant between CT/MRI and PET-CT, with 73% of subjects achieving a complete response on PET-CT and only 7% achieving a complete response on CT/MRI. They hypothesized that PET-CT is more precise and that in many cases apparent tumor on CT/MRI may actually be scar tissue.34
Safety and Tolerability
Table 2 includes the most common treatment emergent adverse events across all included studies. In phase II clinical trials, 99.5% of the 193 total subjects developed at least one adverse event while on treatment, and 48.7% developed a severe adverse event (National Cancer Institute Grade 3 or higher). However, only 17.1% of severe adverse events were believed to be treatment-related, and only 9.8% of adverse events required cessation of therapy. The most common adverse events were fatigue and GI distress. The most common severe treatment-related adverse effects were pneumonitis (2.6%) and autoimmune hepatitis (1.6%).13 There were six total adverse-event related deaths (3%). Of these, two deaths from pneumonia and one from hypercalcemia and deep vein thrombosis were felt to be related to cemiplimab; the others were not related or only possibly related to treatment.10,12,14
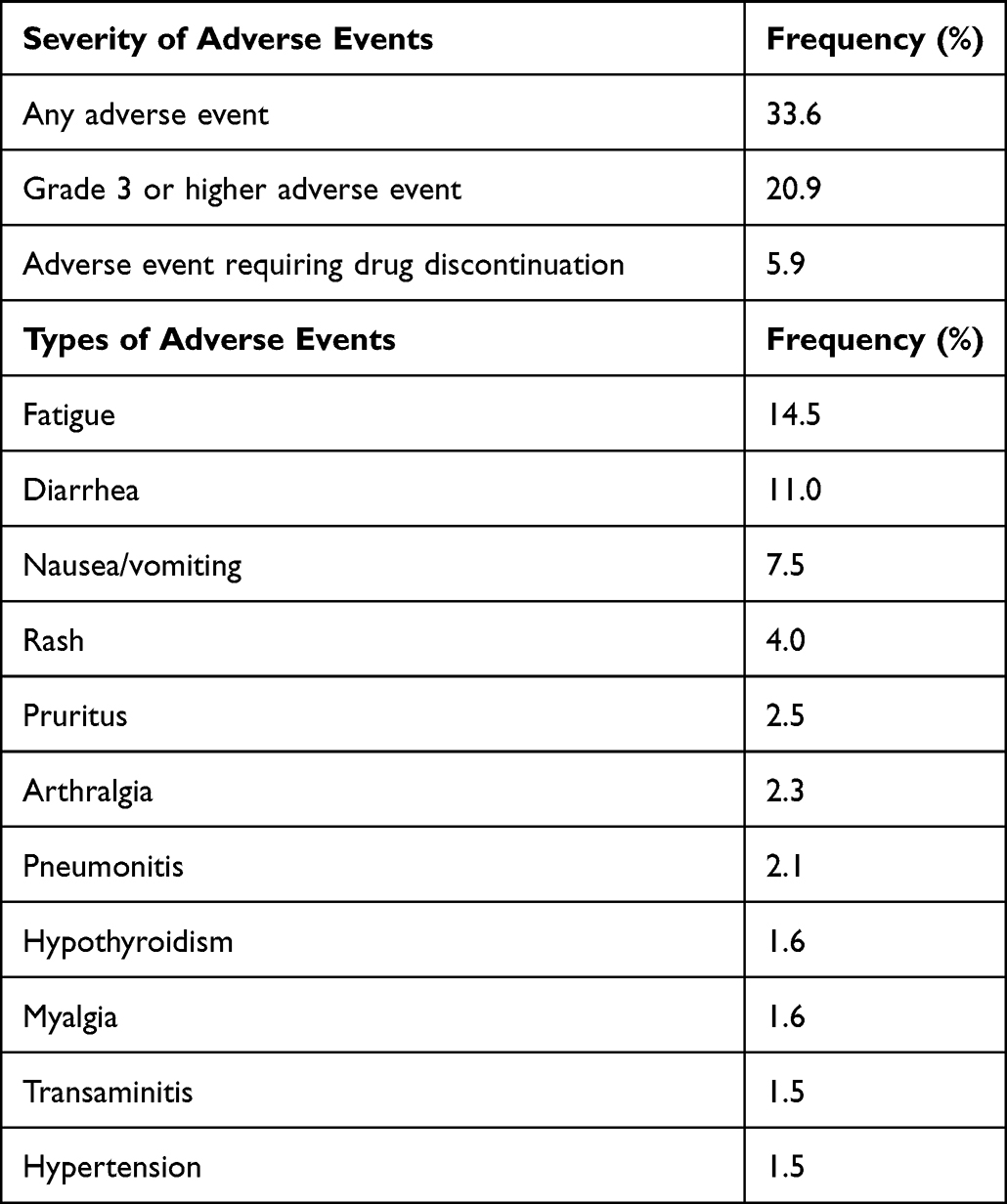 |
Table 2 The Most Common Adverse Events in Clinical Trials and Real-World Observational Studies of Cemiplimab Treatment for Advanced Cutaneous Squamous Cell Carcinoma. Adverse Events with a Frequency of 1.1% or Less are Not Included in This Table |
Safety data in the real-world setting has been comparable to clinical trials, despite inclusion of patients with a broader range of ages and comorbidities. The overall treatment related adverse event rate in larger observational studies ranged from 33% to 58%, 8–9% of which were considered serious events.18,19,21 As in phase II trials, fatigue and diarrhea were most commonly reported, along with pruritus, rash, anemia, pneumonitis, pancreatitis, and musculoskeletal pain.18,19,21 Hepatic disorders were the third most common adverse event in one study;21 another found a 5.1% risk of immune hepatitis and noted that cemiplimab should be considered even in patients with baseline liver disease.25 Interrupted therapy due to side effects occurred in 23.4% of subjects in one study19 and 55% in another.24 Treatment discontinuation rates ranged from 5.3% to 41%.18,19,21,24 Deaths related to cemiplimab treatment were rare and included cases of pneumonitis, myocarditis, toxic epidermal necrolysis, myositis, and pneumonia.18,21,24
Discussion
Immunotherapy has revolutionized the treatment of advanced malignancies, including CSCC. Cemiplimab, a PD-1 immune checkpoint inhibitor, is currently the only FDA-approved systemic treatment for laCSCC and mCSCC not curable with surgery or radiation. Prior to the advent of cemiplimab, systemic therapy options for CSCC were limited to platinum-based chemotherapy and EGFR inhibitors, both of which had limited efficacy and poor tolerability. Phase I and II clinical trials and real-world observational studies have demonstrated that cemiplimab is effective, safe, and well-tolerated in most patients. While adverse events are relatively common, most of these are minor and do not require treatment cessation. Fatal adverse events are rare and tend to be immune-mediated. Overall, the potential benefits of cemiplimab therapy outweigh the risks in patients with advanced CSCC, but patient selection is important.
Patient Selection
Cemiplimab is FDA approved for the treatment of aCSCC. This includes mCSCC and laCSCC, the latter of which is defined as deeply invasive and/or unresectable tumors that are not amenable to definitive treatment with surgery or radiotherapy. Cemiplimab has also shown promise for neoadjuvant treatment of resectable tumors in phase II clinical trials. Although not without risk, cemiplimab therapy has been shown to be well tolerated by most patients, including patients with advanced age, lower functional status, multiple comorbidities, and immunosuppression in real-world studies. In addition, most adverse effects respond well to interruptions in or cessation of treatment.
Phase I and II clinical trials excluded solid organ transplant recipients. Immune checkpoint inhibitors (ICIs) are used with great caution in SOTRs due to the risk of immune-mediated graft rejection. However, these patients are significantly more likely to develop CSCCs and poor CSCC outcomes,35,36 so having treatment options for advanced disease in these patients is critical. Post-approval observational studies of cemiplimab for the treatment of CSCC included 22 SOTRs, and the organ rejection rate across all studies was 13.6%.21,23,25,31
In 2022, a systematic review evaluated the safety of ICIs in advanced malignancies, including 18.5% CSCC. This revealed a 41% risk of organ rejection and a 24% risk of complete graft failure across the entire cohort. However, as subjects were significantly more likely to die of tumor progression (64%) than organ rejection (24%), the benefit of ICI therapy appears to outweigh the risks when no other treatment options are available.37 Limited data suggest that prophylactic systemic steroid regimens may help decrease the risk of rejection in SOTRs.31
Future Directions
Further research on the use of cemiplimab in advanced CSCC is needed. This includes additional long-term and real-world data, further studies in SOTRs (including the best strategy to prevent graft rejection), and additional trials evaluating neoadjuvant and adjuvant use. Future research should also focus on the use of biomarkers to predict treatment response, the timing of treatment cessation in long-term responders, optimal efficacy and safety monitoring, and strategies to prevent and manage adverse events. Finally, other immunotherapy options (including head-to-head clinical trials) and combination therapies should also be explored.
Multiple new trials are now underway to address some of these knowledge gaps. CASE (CemiplimAb-rwlc Survivorship and Epidemiology) is a Phase IV, prospective, non-interventional long-term follow-up study of aCSCC patients treated with cemiplimab in real-world settings (NCT03836105).38 In addition, several clinical trials evaluating the efficacy and safety of cemiplimab in the adjuvant and/or neoadjuvant setting for locally advanced, resectable CSCC are actively enrolling (NCT03969004, NCT03916627, NCT04315701, and NCT4428671).39–42 Finally, NCT04339062 is an open-label, phase I/II trial evaluating the use of cemiplimab in stem cell and renal transplant patients with aCSCC.43
Conclusions
In conclusion, cemiplimab is a promising treatment option for locally advanced and metastatic CSCC and is overall well tolerated. Further research is needed to confirm long-term efficacy and safety in the real-world setting, in special populations, and for adjuvant and neoadjuvant indications.
Funding
There is no funding to report.
Disclosure
Dr. Carr is a trial investigator for Regeneron. The other authors report no conflicts of interest in this work.
References
1. Stratigos A, Garbe C, Lebbe C, et al. Diagnosis and treatment of invasive squamous cell carcinoma of the skin: European consensus-based interdisciplinary guideline. Eur J Cancer. 2015;51(14):1989–2007. doi:10.1016/j.ejca.2015.06.110
2. Brantsch KD, Meisner C, Schönfisch B, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008;9(8):713–720. doi:10.1016/S1470-2045(08)70178-5
3. Thompson AK, Kelley BF, Prokop LJ, et al. Risk factors for cutaneous squamous cell carcinoma recurrence, metastasis, and disease-specific death: a systematic review and meta-analysis. JAMA Dermatol. 2016;152(4):419–428. doi:10.1001/jamadermatol.2015.4994
4. Soleymani T, Brodland DG, Arzeno J, Sharon DJ, Zitelli JA. Clinical outcomes of high-risk cutaneous squamous cell carcinomas treated with Mohs surgery alone: an analysis of local recurrence, regional nodal metastases, progression-free survival, and disease-specific death. J Am Acad Dermatol. 2023;88(1):109–117. doi:10.1016/j.jaad.2022.06.1169
5. European Medicines Agency. Libtayo (cemiplimab): EU public assessment report [homepage on the internet]; 2019. Available from: http://www.ema.europa.eu.
6. Stratigos AJ, Garbe C, Dessinioti C, et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: part 1. Epidemiology, diagnostics and prevention. Eur J Cancer. 2020;128:60–82. doi:10.1016/j.ejca.2020.01.007
7. Maubec E, Petrow P, Scheer-Senyarich I, et al. Phase II study of cetuximab as first-line single-drug therapy in patients with unresectable squamous cell carcinoma of the skin. J Clin Oncol. 2011;29(25):3419–3426. doi:10.1200/JCO.2010.34.1735
8. Corchado-Cobos R, García-Sancha N, González-Sarmiento R, Pérez-Losada J, Cañueto J. Cutaneous squamous cell carcinoma: from biology to therapy. Int J Mol Sci. 2020;21(8):2956. doi:10.3390/ijms21082956
9. Regeneron Pharmaceuticals Inc. Libtayo (cemiplimab): US prescribing information [homepage on the internet]; 2019. Available from: http://www.regeneron.com.
10. Migden MR, Rischin D, Schmults CD, et al. Blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379(4):341–351. doi:10.1056/NEJMoa1805131
11. NCI Dictionaries [homepage on the internet]. USA: RECIST; 2023. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/recist.
12. Migden MR, Khushalani NI, Chang ALS, et al. Cemiplimab in locally advanced cutaneous squamous cell carcinoma: results from an open-label, Phase 2, single-arm trial. Lancet Oncol. 2020;21(2):294–305. doi:10.1016/S1470-2045(19)30728-4
13. Rischin D, Khushalani NI, Schmults CD, et al. Integrated analysis of a phase 2 study of cemiplimab in advanced cutaneous squamous cell carcinoma: extended follow-up of outcomes and quality of life analysis. J Immunother Cancer. 2021;9(8):e002757. doi:10.1136/jitc-2021-002757
14. Rischin D, Migden MR, Lim AM, et al. Phase 2 study of cemiplimab in patients with metastatic cutaneous squamous cell carcinoma: primary analysis of fixed-dosing, long-term outcome of weight-based dosing. J Immunother Cancer. 2020;8(1):e000775. doi:10.1136/jitc-2020-000775
15. Gross ND, Miller DM, Rischin D, et al. Neoadjuvant cemiplimab for stage II to IV cutaneous squamous cell carcinoma. N Engl J Med. 2022;387(17):1557–1568. doi:10.1056/NEJMoa2209813
16. Ferrarotto R, Amit M, Nagarajan P, et al. Pilot Phase II trial of neoadjuvant immunotherapy in locoregionally advanced, resectable cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res. 2021;27(16):4557–4565. doi:10.1158/1078-0432.CCR-21-0585
17. Pham F, Reynaud B, Favier B, Darnis S, Amini-Adle M. Cemiplimab removed from reimbursable drugs in France. Eur J Cancer. 2021;149:11–13. doi:10.1016/j.ejca.2021.02.041
18. Baggi A, Quaglino P, Rubatto M, et al. Real world data of cemiplimab in locally advanced and metastatic cutaneous squamous cell carcinoma. Eur J Cancer. 2021;157:250–258. doi:10.1016/j.ejca.2021.08.018
19. Challapalli A, Watkins S, Cogill G, et al. Cemiplimab in advanced cutaneous squamous cell carcinoma: the UK experience from the Named Patient Scheme. J Eur Acad Dermatol Venereol. 2022;36(7):e590–e592. doi:10.1111/jdv.18082
20. Guillaume T, Puzenat E, Popescu D, Aubin F, Nardin C. Cemiplimab-rwlc in advanced cutaneous squamous cell carcinoma: real-world experience in a French dermatology department. Br J Dermatol. 2021;185(5):1056–1058. doi:10.1111/bjd.20569
21. Hober C, Fredeau L, Pham-Ledard A, et al. Cemiplimab for locally advanced and metastatic cutaneous squamous-cell carcinomas: real-life experience from the French CAREPI Study Group. Cancers. 2021;13(14):3547. doi:10.3390/cancers13143547
22. Ríos-Viñuela E, Álvarez P, Lavernia J, et al. Cemiplimab in advanced cutaneous squamous cell carcinoma: real-world experience in a Monographic Oncology Center. Actas Dermosifiliogr. 2022;113(6):T610–T615. doi:10.1016/j.ad.2022.05.001
23. Strippoli S, Fanizzi A, Quaresmini D, et al. Cemiplimab in an elderly frail population of patients with locally advanced or metastatic cutaneous squamous cell carcinoma: a single-center real-life experience from Italy. Front Oncol. 2021;11:686308. doi:10.3389/fonc.2021.686308
24. Valentin J, Gérard E, Ferte T, et al. Real world safety outcomes using cemiplimab for cutaneous squamous cell carcinoma. J Geriatr Oncol. 2021;12(7):1110–1113. doi:10.1016/j.jgo.2021.02.026
25. Swanson L, Kassab I, Tsung I, Worden FP, Fontana RJ. Infrequent liver injury from cemiplimab in patients with advanced cutaneous squamous cell carcinoma. Immunotherapy. 2022;14(6):409–418. doi:10.2217/imt-2021-0191
26. Bailly-Caillé B, Kottler D, Morello R, et al. Real-life study of the benefit of concomitant radiotherapy with Cemiplimab in advanced cutaneous squamous cell carcinoma (CSCC): a retrospective cohort study. Cancers. 2023;15(2):495. doi:10.3390/cancers15020495
27. Steren B, Burtness B, Bhatia A, et al. Cemiplimab for orbital squamous cell carcinoma in 11 cases. Ophthalmic Plast Reconstr Surg. 2022;38(5):496–502. doi:10.1097/IOP.0000000000002190
28. McLean LS, Lim AM, Webb A, et al. Immunotherapy to avoid orbital exenteration in patients with cutaneous squamous cell carcinoma. Front Oncol. 2022;11:796197. doi:10.3389/fonc.2021.796197
29. Goldfarb JA, Ferrarotto R, Gross N, et al. Immune checkpoint inhibitors for treatment of periorbital squamous cell carcinoma. Br J Ophthalmol. 2023;107(3):320–323. doi:10.1136/bjophthalmol-2021-319417
30. Wu MP, Reinshagen KL, Cunnane MB, et al. Clinical perineural invasion and immunotherapy for head and neck cutaneous squamous cell carcinoma. Laryngoscope. 2022;132(6):1213–1218. doi:10.1002/lary.29953
31. Tsung I, Worden FP, Fontana RJ. A pilot study of checkpoint inhibitors in solid organ transplant recipients with metastatic cutaneous squamous cell carcinoma. Oncologist. 2021;26(2):133–138. doi:10.1002/onco.13539
32. Saponara M, Pala L, Conforti F, et al. Patients with locally advanced and metastatic cutaneous squamous cell carcinoma treated with immunotherapy in the era of COVID-19: stop or go? Data from five Italian referral cancer centers. Ther Adv Med Oncol. 2020;12:1758835920977002. doi:10.1177/1758835920977002
33. Filippi L, Proietti I, Petrozza V, Bagni O, Schillaci O. Cutaneous squamous cell carcinoma subjected to anti PD-1 immunotherapy: monitoring response through serial PET/CT scans with 18F-FDG. Cancer Biother Radiopharm. 2022;37(3):226–232. doi:10.1089/cbr.2021.0368
34. McLean LS, Cavanagh K, Hicks RJ, et al. FDG-PET/CT imaging for evaluating durable responses to immune check point inhibitors in patients with advanced cutaneous squamous cell carcinoma. Cancer Imaging. 2021;21(1):57. doi:10.1186/s40644-021-00426-2
35. Garrett GL, Blanc PD, Boscardin J, et al. Incidence of and risk factors for skin cancer in organ transplant recipients in the United States. JAMA Dermatol. 2017;153(3):296. doi:10.1001/jamadermatol.2016.4920
36. Ritter A, Badir S, Mansour M, et al. Solid organ transplantation worsens the prognosis of patients with cutaneous squamous cell carcinoma of the head and neck region- Comparison between solid organ transplant recipients and immunocompetent patients. Head Neck. 2021;43(3):884–894. doi:10.1002/hed.26546
37. Portuguese AJ, Tykodi SS, Blosser CD, Gooley TA, Thompson JA, Hall ET. Immune checkpoint inhibitor use in solid organ transplant recipients: a systematic review. J Natl Compr Canc Netw. 2022;20(4):406–416.e11. doi:10.6004/jnccn.2022.7009
38. Migden MR, Chandra S, Rabinowits G, et al. CASE (CemiplimAb-rwlc Survivorship and Epidemiology) study in advanced cutaneous squamous cell carcinoma. Future Oncol. 2020;16(4):11–19. doi:10.2217/fon-2019-0762
39. Study of adjuvant cemiplimab versus placebo after surgery and radiation therapy in patients with high risk cutaneous squamous cell carcinoma. Available from: https://clinicaltrials.gov/ct2/show/NCT03969004.
40. Neoadjuvant cemiplimab for the treatment of resectable NSCLC, HCC, and HNSCC. Available from: https://clinicaltrials.gov/ct2/show/NCT03916627.
41. A PD-1 checkpoint inhibitor (Cemiplimab) for high-risk localized, locally recurrent, or regionally advanced skin cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT04315701.
42. Cemiplimab before and after surgery for the treatment of high risk cutaneous squamous cell cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT4428671.
43. Cemiplimab in AlloSCT/SOT recipients with CSCC (CONTRAC). Available from: https://clinicaltrials.gov/ct2/show/NCT04339062.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
PD-L1 Biomolecules Associated with Clinical Features in Non-Melanoma Skin Cancer
Li D, Ma L, Bao J, Cao L, Min W
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1-8
Published Date: 4 January 2023
The Additional Exclusions of ROS1 Fusions (In Addition to EGFR Mutation and ALK Fusions) in the Cemiplimab NSCLC FDA Indication (EMPOWER-Lung 1 and -Lung 3). Catching Up with Current Scientific View of Immunotherapy in Never-Smoker Predominant Actionable Driver Mutation Positive NSCLC?
Brazel D, Ou SI
Lung Cancer: Targets and Therapy 2023, 14:63-69
Published Date: 23 June 2023
Comparison of Neoadjuvant Immunotherapy Plus Chemotherapy versus Neoadjuvant Chemoradiotherapy for Patients with Esophageal Squamous Cell Carcinoma: A Propensity Score Matching Study
Zhao J, Hao S, Tian J, Li Y, Han D
Journal of Inflammation Research 2023, 16:3351-3363
Published Date: 8 August 2023
Real-World Treatment Patterns and Outcomes of Cemiplimab in Patients with Advanced Cutaneous Squamous Cell Carcinoma Treated in US Oncology Practices
Ge W, Wu N, Chen CI, Inocencio TJ, LaFontaine PR, Seebach F, Fury M, Harnett J, Ruiz ES
Cancer Management and Research 2024, 16:841-854
Published Date: 18 July 2024
Synergistic Induction of Immunogenic Cell Death by Biomineralized Manganese and Bisphosphonates Enhances Anti-PD-L1 Therapy in Triple-Negative Breast Cancer
Zhang X, Liu N, Wei M, Yang C, Lin Y, Zeng Y, Li Y, Zhou L, Li T, Zheng Q, Yu H, Zhang J, Gu Y, Xia N, Li S
International Journal of Nanomedicine 2025, 20:5001-5016
Published Date: 17 April 2025