Back to Journals » OncoTargets and Therapy » Volume 13
PCSK1 Overexpression in Rectal Cancer Correlates with Poor Response to Preoperative Chemoradiotherapy and Prognosis
Authors Chou CL, Chen TJ, Lin CY, Lee SW ![]() , Wang SC
, Wang SC ![]() , Chu SS, Yang CC
, Chu SS, Yang CC ![]()
Received 25 December 2019
Accepted for publication 30 March 2020
Published 15 April 2020 Volume 2020:13 Pages 3141—3150
DOI https://doi.org/10.2147/OTT.S243750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Chia-Lin Chou,1,2 Tzu-Ju Chen,2– 4 Cheng-Yi Lin,5 Sung-Wei Lee,6 Shih-Chang Wang,7 Shou-Sheng Chu,7 Ching-Chieh Yang7,8
1Division of Colon and Rectal Surgery, Department of Surgery, Chi Mei Medical Center, Tainan, Taiwan; 2Institute of Biomedical Sciences, National Sun Yat-sen University, Kaohsiung, Taiwan; 3Department of Pathology, Chi Mei Medical Center, Tainan, Taiwan; 4Department of Optometry, Chung Hwa University of Medical Technology, Tainan, Taiwan; 5Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan; 6Department of Radiation Oncology, Chi Mei Medical Center, Liouying, Tainan, Taiwan; 7Department of Radiation Oncology, Chi Mei Medical Center, Tainan, Taiwan; 8Department of Pharmacy, Chia-Nan University of Pharmacy and Science, Tainan, Taiwan
Correspondence: Ching-Chieh Yang
Department of Radiation Oncology, Chi-Mei Medical Center, No. 901 Zhonghua Road, Yung Kang District, Tainan City 701, Taiwan
Tel +88662812811-53501
Email [email protected]
Background: In a data mining search for potential therapeutic targets to improve the outcome of rectal cancer, we identified PCSK1 as the cell–cell signaling gene most significantly associated with poor response to concurrent chemoradiotherapy (CCRT). This study aims to investigate the prognostic value of PCSK1 expression in rectal cancer patients who underwent neoadjuvant CCRT.
Methods: Endoscopic biopsy specimens from 172 rectal cancer patients receiving neoadjuvant CCRT followed by curative surgery were assessed immunohistochemically for PCSK1 expression, and H-scores were determined. Expression levels of PCSK1 were further analyzed for correlations with clinicopathologic features, tumor regression grade, metastasis-free survival, disease-specific survival, and recurrence-free survival.
Results: PCKS1 overexpression was significantly associated with pretreatment tumor status (T3– 4; p = 0.009), pretreatment nodal status (N1– 2; p < 0.001), posttreatment tumor status (T3– 4; p < 0.001), posttreatment nodal status (N1– 2; p < 0.001), vascular invasion (p = 0.003), and perineurial invasion (p = 0.023). PCKS1 overexpression was also found to be significantly associated with a lower degree of tumor regression (p < 0.001). In the univariate analysis, PCSK1 overexpression was significantly associated with lower disease-specific survival, metastasis-free survival, and recurrence-free survival (p < 0.005). PCSK1 overexpression remained an independent prognostic factor of lower disease-specific survival (p = 0.003; hazard ratio, 5.478) in the multivariate analysis.
Conclusion: Determination of PCSK1 overexpression may be useful for identifying rectal cancer patients at risk for a poor response and worse survival after CCRT.
Keywords: PCSK1, rectal cancer, chemoradiotherapy, response, survival
Introduction
Colorectal cancer remains one of the most common malignancies and the third-highest cause of cancer-related deaths worldwide.1 Compared to colon cancer, rectal cancer patients often experience worse outcomes because resection is more difficult.2 In recent decades, preoperative concurrent chemoradiotherapy (CCRT) has been shown to provide better local control, greater anal preservation, and lower toxicity over surgery alone.3 However, the effect on a given outcome varies greatly between studies, and 10–20% of patients still experience recurrence or metastasis.4 Therefore, to choose the most suitable treatment option, prognostic biomarkers may be better predictors of response to CCRT and prognosis than cancer stage.
To identify potential biomarkers for rectal cancer, we analyzed a public transcriptomic dataset of rectal cancer (GSE35452) from Gene Expression Omnibus, National Center for Biotechnology Information (GEO, NCBI, Bethesda, MD, USA) and identified convertase subtilisin/kexin-type 1 (PCSK1) as the most significantly upregulated gene among those associated with cell-cell signaling pathways (GO:0007267). As a member of the proprotein convertase family, the PCSK1 protein (also known as PC1/3) plays a vital role in the proteolytic processing of mature bioactive proteins from large prohormones, including pro-opiomelanocortin, proinsulin, proglucagon, pro-islet amyloid polypeptide, and prorenin.5,6 The resulting end products are widely involved in energy balance, glucose metabolism, and blood pressure regulation. In humans, loss-of-function mutations in the PCSK1 gene cause monogenic obesity, impaired glucose tolerance, hypertension, cardiac remodeling, and microvascular damage.7,8 A variety of studies also report a role for PCSK1 expression in human cancers and tumor cell lines.9,10
This study investigates PCSK1 expression and its association with tumor response to preoperative CCRT in patients with rectal cancer. The level of PCSK1 protein expression was determined in 172 pairs of cancer tissue samples, and the role of PCSK1 was elucidated by analyzing the relationships between clinical and pathological features, including tumor response and survival.
Materials and Methods
Ethics Statement
This study was reviewed and approved by the Institutional Review Board of Chi-Mei Medical Center in Taiwan (IRB: CMFHR10501-008). The requirement for informed consent was waived because all identifying information was removed from the dataset before analysis. This manuscript was also designed according to the guidelines of the Helsinki Declaration as revised in 2013.
Analysis of the Published Transcriptome Dataset
To identify potential genes associated with the response to CCRT, data in a public transcriptome database (GSE35452; Gene Expression Omnibus, National Center for Biotechnology Information, GEO, NCBI, Bethesda, MD, USA) comprising 46 patients with rectal cancer treated with preoperative CCRT were analyzed. Raw CEL files were computerized using the Affymetrix Human Genome U133 Plus 2.0 microarray platform with Nexus Expression 3 statistical software (BioDiscovery, Hawthorne, CA, USA). All probe sets were analyzed without pre-selection. Under supervision, the statistical significance of each transcript was examined by comparing responders to non-responders, with special attention to genes involved in cell–cell signaling pathways (GO:0007267). We chose those with p < 0.01 and a difference in log 2-transformed expression of at least +/−0.1-fold for further analysis.
Demographic Characteristics and Tumor Specimens
This retrospective study was performed using formalin-fixed, paraffin-embedded tissue specimens from 172 newly diagnosed rectal adenocarcinoma patients treated at Chi Mei Medical Center between 1998 and 2004. The pretreatment staging was determined by endoscopic ultrasound, abdominal computed tomography, or magnetic resonance imaging findings. Patients received 5-fluorouracil-based chemotherapy concomitant with radiotherapy (45–50 Gy) before surgery, and adjuvant chemotherapy was given if the pretreatment or posttreatment tumor or nodal stage was greater than T3 or N1. Tumors from all patients were re-staged and re-graded according to the 7th edition of the AJCC staging system and the World Health Organization classification of Tumors of the Colon and Rectum. All patients were regularly monitored after diagnosis until death or last follow-up.
Histopathologic Assessment of Tumor Specimens
Tumor specimens were evaluated histologically by two independent pathologists (CF Li and YC Wei) who were blinded to all patient clinical information. The assessment of the tumor response to preoperative CCRT was assessed using the standard 5-point tumor regression grading system.11
PCSK1 Immunohistochemical Analysis
As previously described, tumor specimens at initial diagnosis were routinely deparaffinized, rehydrated, heated, quenched, and washed for immunohistochemical staining.12,13 After epitope retrieval, tumor specimens were incubated for 1 hour with primary antibody recognizing PCSK1 (Sigma, clone 3D2, 1:50). The immunoexpression levels of PCSK1 in all tumor specimens were scored by two independent pathologists of the addition of secondary antibody and hematoxylin staining. For the positive and negative controls, normal bowel tissue treated with or without PCSK1 primary antibody, respectively, were stained in parallel. The immunoexpression levels of PCSK1 in tumor cell nuclei were calculated using the H-score method as follows: H-score = ΣPi (i + 1), where Pi represents the percentage of tumor cells stained at various intensities (0–100%) and i represents the tumor staining intensity (0 - 3+).14 H-scores were used to designate high and low PCSK1 expression (high expression, above or equal to the median; low expression, below the median).
Statistical Analysis
All statistical analyses were performed using SPSS for Windows 22.0 (IBM Corporation, Armonk, NY, USA), with p < 0.05 considered statistically significant. The primary endpoints comprised 5-year disease-specific survival (DSS), local recurrent-free survival (LRFS), and metastases-free survival (MeFS) rates. Deaths due to cancer were defined as valid events, and deaths secondary to other causes were censored. Associations between PCSK1 expression and clinicopathological features were determined using the chi-square test. The 5-year DSS, LRFS, and MeFS rates were described using the Kaplan–Meier method, and differences were compared using log-rank statistics. A multivariate Cox regression model was used after adjusting for other confounding variables.
Results
Upregulation of PCSK1 Gene Is Associated with Poor Response to CCRT
As shown in Table 1 and Figure 1, the top-ranking upregulated genes associated with a poor response to CCRT included PCSK1 and WISP3. However, PCSK1 was the most significantly upregulated (log 2 ration, 1.8447; p < 0.0001). This result motived us to further investigate the expression status and clinical relevance of PCKS1 in rectal cancers treated with CCRT.
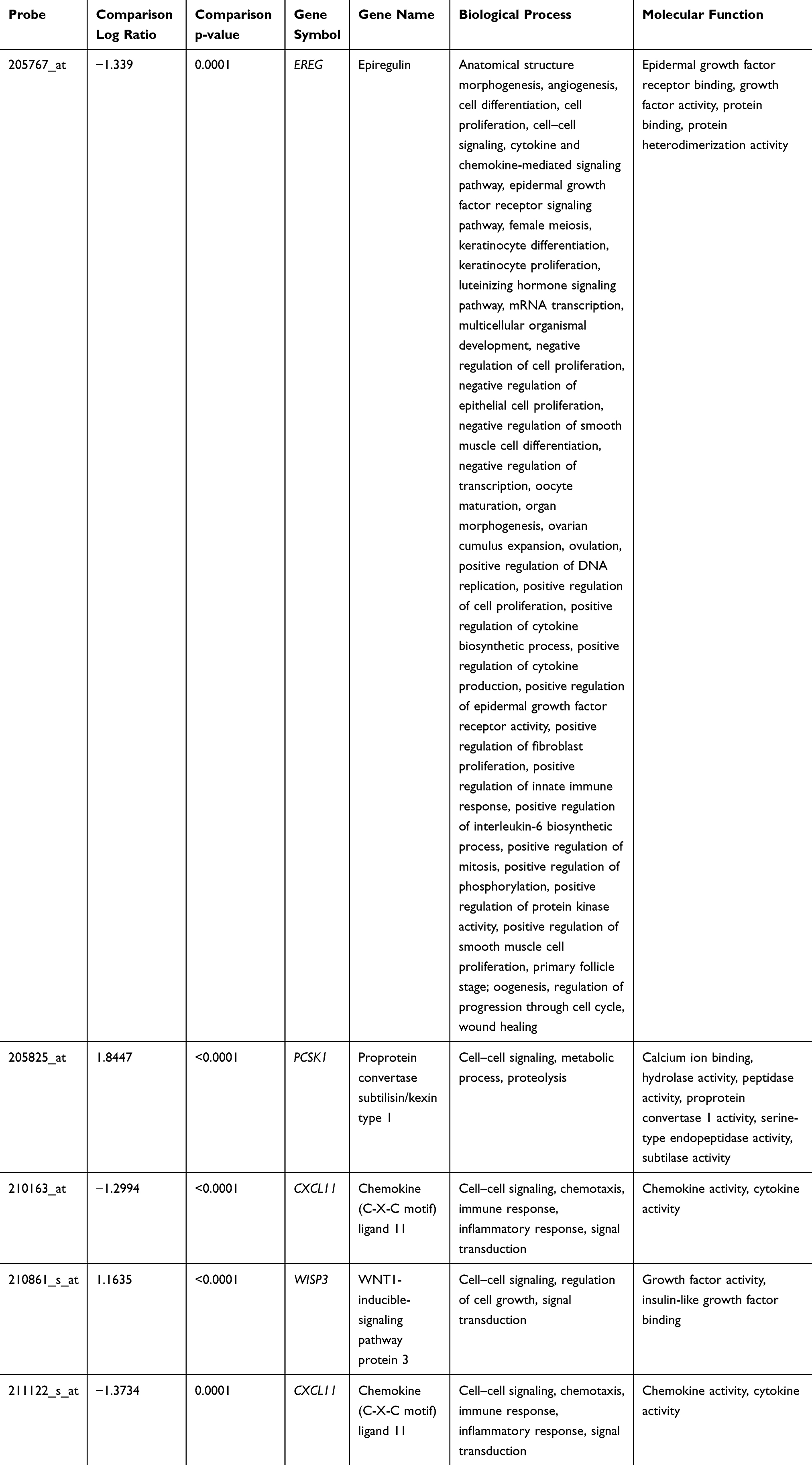 |
Table 1 Summary of Differentially Expressed Genes Associated with Cell–Cell Signaling (GO: 0007267) in Relation to Response to CCRT in Rectal Carcinoma |
 |
Figure 1 Analysis of gene expression in CCRT responders versus non-responders from a published transcriptomic dataset of rectal cancers (GSE35452). Clustering analysis of genes related to cell-cell signaling indicated PCSK1 is the most significantly upregulated gene in patients responsive to CCRT. Tissue specimens from responders (yellow lines) and non-responders (blue lines) are indicated on top of the heatmap, and expression levels of upregulated and downregulated genes are expressed as a spectrum of brightness of red and green, respectively, with those unaltered in mRNA. |
Study Population
A total of 172 patients were enrolled in this study, including 108 (62.8%) males and 64 (37.2%) females (Table 2). The median age was 63 years (range, 22–88 years). The fraction of patients with initial stage I, II, and III disease was 41.9, 29.9, and 28.1%. All stage II and III patients received adjuvant chemotherapy. Fifteen (8.7%) patients presented with vascular invasion, and 5 (2.9%) with perineurial invasion. Of the 172 tumor specimens examined, the response was poor (TRG 0–1, < 25% response) in 37 patients (21.5%), moderate (TRG 2–3) in 118 (68.6%), and complete (no visible tumor in the rectal wall; TRG 4) in 17 (10%) (Table 2).
 |
Table 2 Associations and Comparisons Between PCSK1 Expression and Clinicopathological Factors in 172 Rectal Cancer Patients Receiving Preoperative CCRT |
Immunohistochemical Analysis of PCSK1 Expression and Its Association with Clinicopathologic Features
To determine the relationship between PCSK1 expression level and clinicopathologic characteristics of rectal cancer after neoadjuvant CCRT, immunohistochemical was performed to examine the expression of PCSK1 in 172 rectal cancer specimens. Cytoplasmic expression of PCSK1 was successfully scored in all examined cases, with H-scores varying widely (range, 110–310, Figure 2). High PCKS1 expression was significantly related to pretreatment tumor status (T3-4; p = 0.009), pretreatment nodal status (N1-2; p < 0.001), posttreatment tumor status (T3-4; p < 0.001), posttreatment nodal status (N1-2; p < 0.001), vascular invasion (p = 0.003), and perineurial invasion (p = 0.023) (Table 2). In addition, PCKS1 overexpression was significantly associated with a lower degree of tumor regression (p < 0.001). Among patients with PCSK1 overexpression, we observed a tumor regression grade of 0–1 in 27 (15.7%), grade 2–3 in 56 (32.6%), and grade 4 in 3 (1.7%). These findings indicate that PCSK1 plays a role in modulating rectal tumor progression and CCRT sensitivity.
 |
Figure 2 Immunohistochemical staining for proprotein convertase subtilisin/kexin-type 1 (PCSK1) in rectal cancers. The non-neoplastic colonic mucosa (A) reveals no expression of PCSK1 as compared with rectal cancers with low expression (B) and high expression (C) of PCSK1 in pretreatment specimens, respectively. |
Prognostic Implications of PCSK1 Expression in Rectal Cancer Patients
We further analyzed the prognostic significance of PCSK1 expression in patients with rectal cancer after CCRT. In the univariate analysis (Table 3), clinicopathologic parameters including the pretreatment nodal status, posttreatment tumor status, presence of vascular invasion, and TRG were significantly associated with at least one of the three endpoints of our study. Notably, rectal cancer patients with high PCSK1 expression had significantly lower DSS (p < 0.0001), LRFS (p = 0.0063) and MeFS (p = 0.0008) (Table 3; Figure 3). After multivariate analysis (Table 4), TRG and PCSK1 expression remained as independent prognostic factors. Pretreatment nodal status, posttreatment tumor status and presence of vascular invasion were not significantly associated with DSS, LRFS and MeFS. High PCSK1 expression was an independent predictor of DSS (p = 0.003; hazard ratio [HR], 5.478; 95% confidence interval [CI], 1.789–16.774).
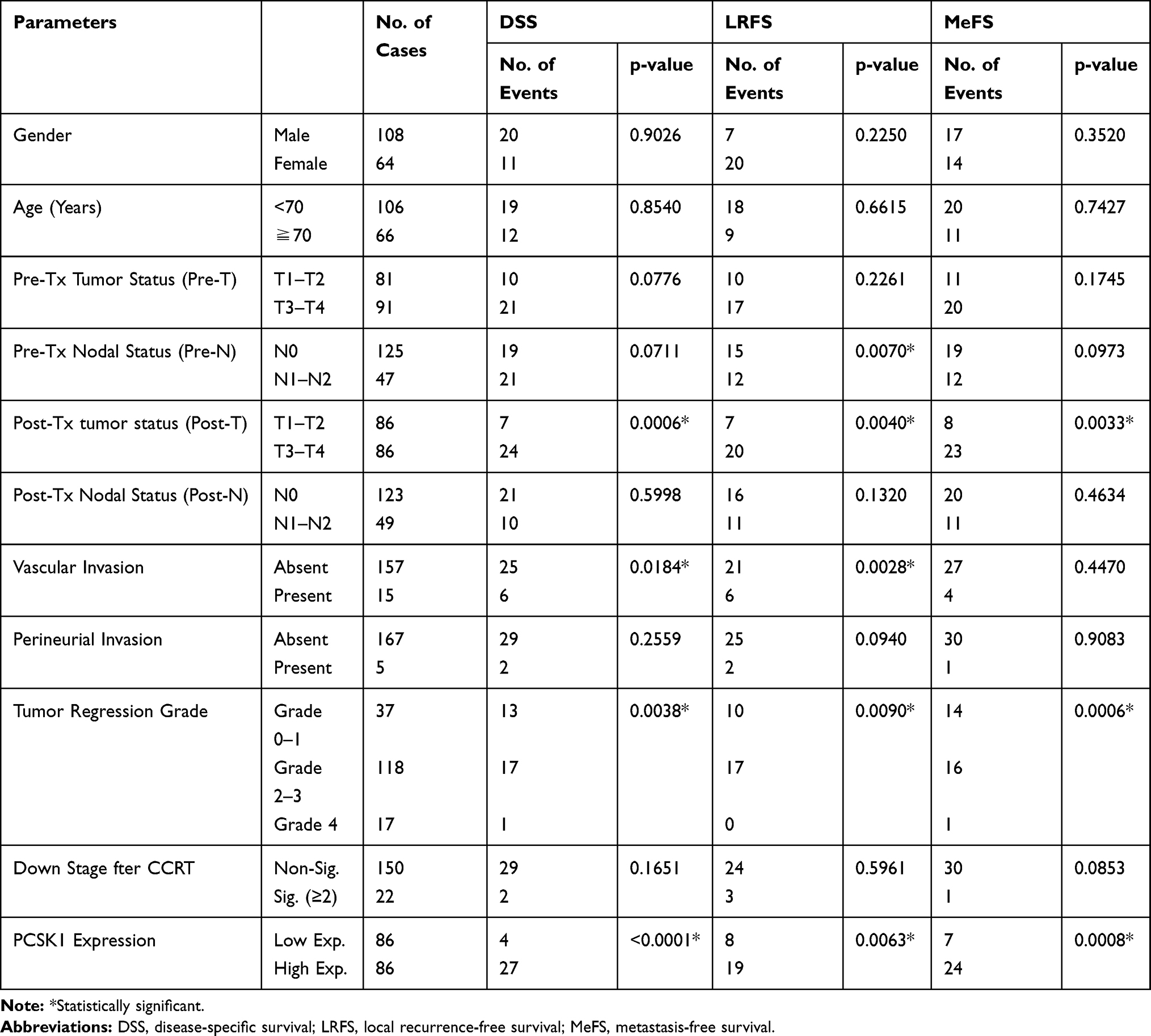 |
Table 3 Univariate Log-Rank Analysis for Important Clinicopathological Variables and PCSK1 Expression |
 |
Table 4 Multivariate Survival Analysis |
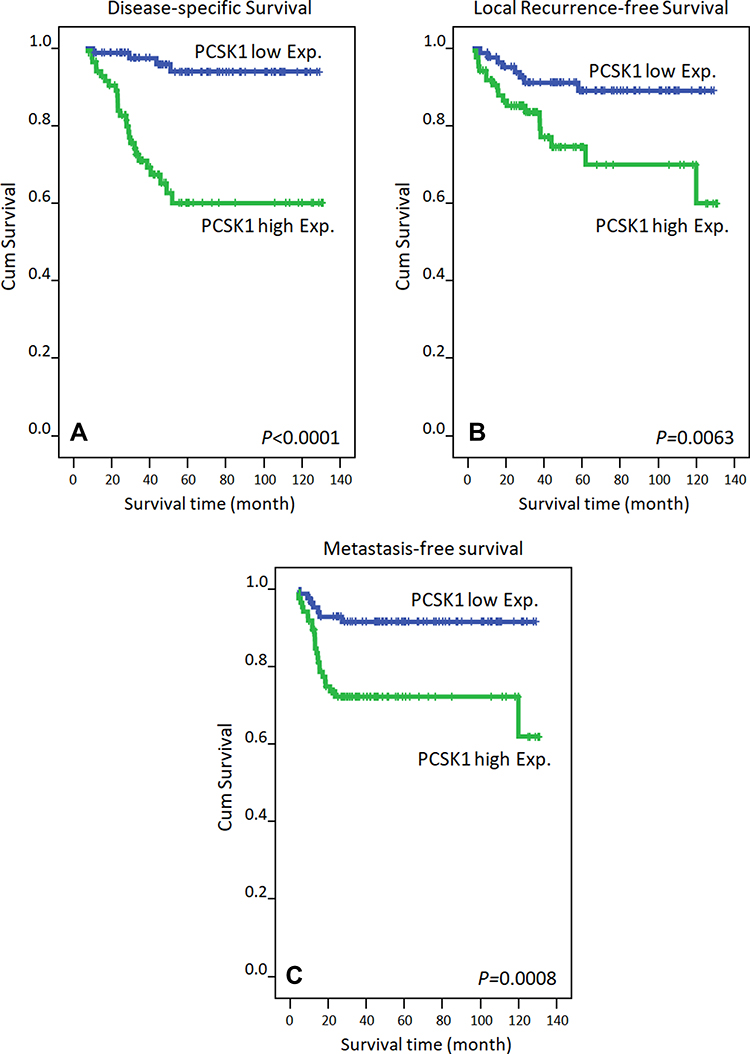 |
Figure 3 Kaplan–Meier survival curves plotted to predict survival. Using the Log rank test, rectal cancer patients with high expression of PCSK1 had an inferior disease-specific survival (A), local recurrence-free survival (B) and metastasis-free survival (C). |
Discussion
Overexpression of proprotein convertases has been demonstrated in multiple cancer types, and is also related to more aggressive tumor behavior.9,15,16 In this study, we observed that high PCSK1 expression is associated with advanced tumor status, poor response to CCRT, and lower survival. To our knowledge, this is the first report describing PCSK1 expression in rectal cancer patients receiving CCRT. More importantly, we also assessed the predisposing clinical and pathological factors influencing survival. These results indicate that PCSK1 may be useful for outcome prediction and may be a potential therapeutic target in rectal cancer.
The proprotein convertase family members convert proproteins into biologically active molecules.17,18 To date, at least nine such enzymes have been identified: furin, PC1/PC3, PC2, PC4, PACE4, PC5/PC6, PC7/LPC/PC8, SKI-1/S1P, and NARC-1/PCSK9.19 In the secretory pathway, proprotein convertases mediate the tissue-specific endoproteolytic activation of precursor proteins, including hormones, neuropeptides, growth factors and their receptors, adhesion molecules, bacterial toxins, and viral glycoproteins. Thus, inhibition of proprotein convertases is associated with many diseases, including Alzheimer’s and endocrinopathies.20
In the early 1990s, proprotein convertases were found to be associated with cancer. Since then, numerous studies have established that PCSK1 contributes to tumor development, invasion, and progression in multiple cancer types, including lung, breast, pancreatic, and intestinal cancer.16,21-24 Mbikay et al reported that small-cell lung cancers often express more mRNA for PC1 and PC2 and less mRNA for the more ubiquitous furin and PACE4, suggesting inverse roles of these convertases in the development of this neoplasm.25 Cheng et al reported elevated expression of furin and PC1, key enzymes needed to activate vasopressin and other growth factors, in human breast tumors.22 All of this evidence supports our findings that high PCSK1 expression is significantly associated with advanced tumor behavior such as, including pretreatment tumor status, pretreatment nodal status, posttreatment tumor status, posttreatment nodal status, vascular invasion, and perineurial invasion. Thus, altered PCSK1 biology could play a role in human tumor formation and progression resulting from the incomplete or absent processing of its target molecules.
Although the association between PCSK1 expression and colorectal cancer outcomes remains largely unclear, our survival analysis shows that high expression of PCSK1 conferred a negative prognostic impact on rectal cancer in terms of lower DFS. In agreement with our findings, Tzimas et al observed that PC1 and PC2 expression and cleavage are altered in colorectal liver metastases and may be associated with worse clinical outcomes.26 Horsch et al report that PC1 and PC2 are also detected in the human anal canal.27 Collectively, these data indicate that high PCSK1 expression not only is associated with a more aggressive phenotype but also acts as a predictor of metastasis.
More importantly, we found that high PCSK1 expression also is significantly associated with lower tumor regression grade, indicating a poor response to CCRT. The possible reasons for this association are as follows. First, PCSK1 plays an important role in the regulation of cytokine secretion and, consequently, is also a regulator of the innate immune response. After irradiation, macrophages receive cellular death signals, leading to the recruitment of more immune cells, including monocytes, which differentiate into macrophages at the injury site.28 With aberrant PCSK1 expression, macrophage activation would be altered, decreasing the production of profibrotic growth factors and anti-inflammatory cytokines, such as TGFβ1, resulting in a poor response to radiation.29 Second, PCSK1 expression is associated with obesity in humans.8,30 Obesity with rectal cancer not only increases the local recurrence rate decreases the possibility of sphincter preservation but also is associated with inflammation, angiogenesis, and chronic oxidative stress, which may affect the response to radiotherapy.31–34 Lee et al recently reported obesity as an independent negative predictive factor for complete response to CCRT in rectal cancer.35,36 As we known, tumor response could reflects early response to treatments and related to late response outcomes including recurrence and survival. Many studies also indicate that obesity is a common risk factor for cardiovascular disease and is an indicator of poor prognosis in multiple cancer types.37,38 Thus, the overexpression of PCSK1 in rectal cancers could be used to identify patients at increased risk of poor response and survival after preoperative CCRT.
The current study has several limitations. First, the number of patients was relatively small; thus, the findings should be verified by larger-scale studies. Second, our study cohort included some early-stage rectal cancer patients because they were undergoing preoperative CCRT with the intention of organ preservation. Further studies in a patient cohort limited to locally advanced rectal cancer should be performed.
Conclusion
In summary, the results of this study indicate that the determination of PCSK1 overexpression may help identify and stratify high-risk patients after preoperative CCRT. The strong inverse correlation observed between TRG and DSS suggests that PCSK1 may be a potential prognostic biomarker and that PCSK1 inhibition may be a novel therapeutic strategy for rectal cancer patients.
Abbreviations
CCRT, concurrent chemoradiotherapy; PCSK1, proprotein convertase subtilisin/kexin-type 1; AJCC, American Joint Committee on Cancer; TRG, tumor regression grade; DSS, disease-specific survival; LRFS, local-recurrence-free survival; MeFS, metastases-free survival; HR, hazard ratio; CI, confidence interval.
Acknowledgments
We acknowledge the support from the following grants: (1) Health and Welfare surcharge on tobacco products (MOHW109-TDU-B-212-134020, WanFang Hospital, Chi Mei Medical Center, and Hualien Tzu-Chi Hospital Joing Cancer Center Grant-Focus on Colon Cancer Research); (2) CMFHR10828 and CMFHR108105 from the Chi Mei Medical center; (3) BioBank of Chi Mei Medical Center for providing the tumor samples and to the translational research laboratory of human cancers at Chi Mei Medical Center (leaded by Prof. Chien-Feng Li) for their invaluable support.
Disclosure
The authors have no declarations of interest to report in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. doi:10.3322/caac.21332
2. Lee YC, Lee YL, Chuang JP, Lee JC. Differences in survival between colon and rectal cancer from SEER data. PLoS One. 2013;8(11):e78709. doi:10.1371/journal.pone.0078709
3. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):1731–1740. doi:10.1056/NEJMoa040694
4. van den Brink M, Stiggelbout AM, van den Hout WB, et al. Clinical nature and prognosis of locally recurrent rectal cancer after total mesorectal excision with or without preoperative radiotherapy. J Clin Oncol. 2004;22(19):3958–3964. doi:10.1200/JCO.2004.01.023
5. Li XM, Ling Y, Lu DR, et al. The obesity-related polymorphism PCSK1 rs6235 is associated with essential hypertension in the Han Chinese population. Hypertens Res. 2012;35(10):994–999. doi:10.1038/hr.2012.79
6. Gu Q, Yazdanpanah M, van Hoek M, et al. Common variants in PCSK1 influence blood pressure and body mass index. J Hum Hypertens. 2015;29(2):82–86. doi:10.1038/jhh.2014.59
7. Choquet H, Stijnen P, Creemers JW. Genetic and functional characterization of PCSK1. Methods Mol Biol. 2011;768:247–253.
8. Ramos-Molina B, Martin MG, Lindberg I. PCSK1 variants and human obesity. Prog Mol Biol Transl Sci. 2016;140:47–74.
9. Khatib AM, Siegfried G, Chretien M, Metrakos P, Seidah NG. Proprotein convertases in tumor progression and malignancy: novel targets in cancer therapy. Am J Pathol. 2002;160(6):1921–1935. doi:10.1016/S0002-9440(10)61140-6
10. Zhang Y, Huang S, Li P, et al. Pancreatic cancer-derived exosomes suppress the production of GIP and GLP-1 from STC-1 cells in vitro by down-regulating the PCSK1/3. Cancer Lett. 2018;431:190–200. doi:10.1016/j.canlet.2018.05.027
11. Rodel C, Martus P, Papadoupolos T, et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol. 2005;23(34):8688–8696. doi:10.1200/JCO.2005.02.1329
12. Li C-F, He H-L, Wang J-Y, et al. Fibroblast growth factor receptor 2 overexpression is predictive of poor prognosis in rectal cancer patients receiving neoadjuvant chemoradiotherapy. J Clin Pathol. 2014;67(12):1056–1061. doi:10.1136/jclinpath-2014-202551
13. Sheu MJ, Li CF, Lin CY, et al. Overexpression of ANXA1 confers independent negative prognostic impact in rectal cancers receiving concurrent chemoradiotherapy. Tumour Biol. 2014;35(8):7755–7763. doi:10.1007/s13277-014-2032-8
14. Rezaeian AH, Li CF, Wu CY, et al. A hypoxia-responsive TRAF6-ATM-H2AX signalling axis promotes HIF1alpha activation, tumorigenesis and metastasis. Nat Cell Biol. 2017;19(1):38–51. doi:10.1038/ncb3445
15. Longuespee R, Couture F, Levesque C, et al. Implications of proprotein convertases in ovarian cancer cell proliferation and tumor progression: insights for PACE4 as a therapeutic target. Transl Oncol. 2014;7(3):410–419. doi:10.1016/j.tranon.2014.04.008
16. Du J, Keegan BP, North WG. Key peptide processing enzymes are expressed by breast cancer cells. Cancer Lett. 2001;165(2):211–218. doi:10.1016/S0304-3835(01)00409-8
17. Chretien M, Mbikay M. 60 YEARS OF POMC: from the prohormone theory to pro-opiomelanocortin and to proprotein convertases (PCSK1 to PCSK9). J Mol Endocrinol. 2016;56(4):T49–T62. doi:10.1530/JME-15-0261
18. Basak A, Chen A, Majumdar S, Smith HP. In vitro assay for protease activity of proprotein convertase subtilisin kexins (PCSKs): an overall review of existing and new methodologies. Methods Mol Biol. 2011;768:127–153.
19. Bassi DE, Fu J, Lopez de Cicco R, Klein-Szanto AJ. Proprotein convertases: “master switches” in the regulation of tumor growth and progression. Mol Carcinog. 2005;44(3):151–161. doi:10.1002/mc.20134
20. Chretien M, Seidah NG, Basak A, Mbikay M. Proprotein convertases as therapeutic targets. Expert Opin Ther Targets. 2008;12(10):1289–1300. doi:10.1517/14728222.12.10.1289
21. Kajiwara H, Itoh Y, Itoh J, Yasuda M, Osamura RY. Immunohistochemical expressions of prohormone convertase (PC)1/3 and PC2 in carcinoids of various organs. Tokai J Exp Clin Med. 1999;24(1):13–20.
22. Cheng M, Watson PH, Paterson JA, Seidah N, Chretien M, Shiu RP. Pro-protein convertase gene expression in human breast cancer. Int J Cancer. 1997;71(6):966–971. doi:10.1002/(SICI)1097-0215(19970611)71:6<966::AID-IJC10>3.0.CO;2-4
23. Yoon J, Beinfeld MC. Prohormone convertase 1 is necessary for the formation of cholecystokinin 8 in Rin5F and STC-1 cells. J Biol Chem. 1997;272(14):9450–9456. doi:10.1074/jbc.272.14.9450
24. Itoh Y, Tanaka S, Takekoshi S, Itoh J, Osamura RY. Prohormone convertases (PC1/3 and PC2) in rat and human pancreas and islet cell tumors: subcellular immunohistochemical analysis. Pathol Int. 1996;46(10):726–737. doi:10.1111/j.1440-1827.1996.tb03541.x
25. Mbikay M, Sirois F, Yao J, Seidah NG, Chretien M. Comparative analysis of expression of the proprotein convertases furin, PACE4, PC1 and PC2 in human lung tumours. Br J Cancer. 1997;75(10):1509–1514. doi:10.1038/bjc.1997.258
26. Tzimas GN, Chevet E, Jenna S, et al. Abnormal expression and processing of the proprotein convertases PC1 and PC2 in human colorectal liver metastases. BMC Cancer. 2005;5:149. doi:10.1186/1471-2407-5-149
27. Horsch D, Day R, Seidah NG, Weihe E, Schafer MK. Immunohistochemical localization of the pro-peptide processing enzymes PC1/PC3 and PC2 in the human anal canal. Peptides. 1997;18(5):755–760. doi:10.1016/S0196-9781(96)00029-0
28. Wynn TA, Ramalingam TR. Mechanisms of fibrosis: therapeutic translation for fibrotic disease. Nat Med. 2012;18(7):1028–1040. doi:10.1038/nm.2807
29. Teresa Pinto A, Laranjeiro Pinto M, Patricia Cardoso A, et al. Ionizing radiation modulates human macrophages towards a pro-inflammatory phenotype preserving their pro-invasive and pro-angiogenic capacities. Sci Rep. 2016;6:18765. doi:10.1038/srep18765
30. Stijnen P, Tuand K, Varga TV, Franks PW, Aertgeerts B, Creemers JW. The association of common variants in PCSK1 with obesity: a HuGE review and meta-analysis. Am J Epidemiol. 2014;180(11):1051–1065. doi:10.1093/aje/kwu237
31. Meyerhardt JA, Tepper JE, Niedzwiecki D, et al. Impact of body mass index on outcomes and treatment-related toxicity in patients with stage II and III rectal cancer: findings from Intergroup Trial 0114. J Clin Oncol. 2004;22(4):648–657. doi:10.1200/JCO.2004.07.121
32. You JF, Tang R, Changchien CR, et al. Effect of body mass index on the outcome of patients with rectal cancer receiving curative anterior resection: disparity between the upper and lower rectum. Ann Surg. 2009;249(5):783–787.
33. Vares G, Wang B, Ishii-Ohba H, Nenoi M, Nakajima T. Diet-induced obesity modulates epigenetic responses to ionizing radiation in mice. PLoS One. 2014;9(8):e106277. doi:10.1371/journal.pone.0106277
34. Incio J, Tam J, Rahbari NN, et al. PlGF/VEGFR-1 Signaling Promotes Macrophage Polarization and Accelerated Tumor Progression in Obesity. Clin Cancer Res. 2016;22(12):2993–3004. doi:10.1158/1078-0432.CCR-15-1839
35. Lee SY, Kim CH, Kim YJ, Kwak HD, Ju JK, Kim HR. Obesity as an independent predictive factor for pathologic complete response after neoadjuvant chemoradiation in rectal cancer. Ann Surg Treat Res. 2019;96(3):116–122.
36. Ho V, Chung L, Singh A, et al. Overexpression of the MRE11-RAD50-NBS1 (MRN) complex in rectal cancer correlates with poor response to neoadjuvant radiotherapy and prognosis. BMC Cancer. 2018;18(1):869. doi:10.1186/s12885-018-4776-9
37. Huang Y, Zhang Y, Li J, Liu G. Charlson comorbidity index for evaluation of the outcomes of elderly patients undergoing laparoscopic surgery for colon cancer. J BUON. 2017;22(3):686–691.
38. Maruoka D, Arai M, Ishigami H, et al. Sporadic nonampullary duodenal adenoma/carcinoma is associated with not only colon adenoma/carcinoma but also gastric cancer: association of location of duodenal lesions with comorbid diseases. Scand J Gastroenterol. 2015;50(3):333–340. doi:10.3109/00365521.2014.1003399
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.