Back to Journals » Open Access Emergency Medicine » Volume 13
Pattern of Traumatic Dental Injuries Among Adults
Authors Ramachandran A, Khan SIR, Al-maslamani M, Baskaradoss JK ![]()
Received 14 March 2021
Accepted for publication 28 April 2021
Published 21 May 2021 Volume 2021:13 Pages 201—206
DOI https://doi.org/10.2147/OAEM.S311113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Anupama Ramachandran,1 Sulthan Ibrahim Raja Khan,2 Manal Al-maslamani,3 Jagan Kumar Baskaradoss4
1Department of Conservative Dentistry & Endodontics, Chettinad Dental College & Research Institute, Tamil Nadu, India; 2Restorative & Endodontics, Department of Restorative & Prosthetic Dental Sciences, College of Dentistry, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia; 3Department of Restorative Sciences, Faculty of Dentistry, Kuwait University, Safat, Kuwait; 4Department of Developmental and Preventive Sciences, Faculty of Dentistry, Kuwait University, Safat, Kuwait
Correspondence: Jagan Kumar Baskaradoss
Department of Developmental and Preventive Sciences, Faculty of Dentistry, Kuwait University, P.O. Box: 24923, Safat, 13110, Kuwait
Tel +965 2463-6807
Fax +965 25326049
Email [email protected]
Background: The etiology, presentation and management of traumatic dental injuries (TDIs) vary significantly between the adult and the younger population. Most epidemiological studies on TDIs have focused on the pediatric age group. This study aims to report and compare the distributions of TDIs among adults in a sub-population in India.
Methods: This prospective observational study was performed on 1562 consecutively selected patients (1218 males and 344 females) from a university dental hospital in India, between July 2014 and June 2018. The clinical examinations were performed by a single trained and calibrated endodontist. Only TDIs to anterior teeth were recorded (canine to canine in the maxilla and mandible) and classified using a modified version of the World Health Organization’s (WHO’s) classification. Periapical and panoramic radiographs were taken for all the subjects.
Results: A total of 1562 patients aged between 20 and 73 years, with a mean age of 36 years, were examined during the study period. The total number of teeth with TDIs was 3044. Males (78%) clearly outnumbered the females (22%) in all the age groups. The most common type of injury occurring in both the genders is uncomplicated crown fractures (male=31.0% and female=36.6%). Avulsion injuries are more likely to be seen by a dentist within 1 hour post-trauma. About two-third of the TDIs were caused by road traffic accidents (RTAs) followed by falls in about 20% of the patients.
Conclusion: Uncomplicated crown fracture was the most commonly observed type of TDI, and RTAs were the primary cause of TDI.
Keywords: adults, dental injuries, trauma
Background
Traumatic dental injuries (TDIs) are very frequent with an estimated world average prevalence of 18% in the permanent dentition, with higher prevalence being reported from the Americas and South-East Asian Regions (about 22% and 16%, respectively).1 Oral injuries are most frequent during the first 10 years of life, are decreasing gradually with age, and are very rare after the age of 30.2 Almost ninety percent of TDIs occur before the age of 20.3 Data from the National Health and Nutrition Examination Survey (NHANES)-III showed that 1 in every 5 children aged 6–20 experienced trauma to their incisors.4
Several epidemiological studies on TDIs have focused on the pediatric age group.5–7 Very few studies have focused on describing TDIs in an adult population (>20yrs).8–10 Studies focusing on the adult population are required especially as the etiology of TDIs is different between adults and children. The main causes for dental trauma in children are falls and injuries sustained during play, whereas in adolescents and adults, more complex traumas may occur caused by sport accidents, fights, and road traffic accidents (RTAs).11 As the etiology of TDI is different, the impact of trauma will manifest itself differently in children and adults. Equally important is the difference in the tooth and bone structure between a child and an adult, which plays a vital role in the mechanism and nature of the energy transmission following an impact to a tooth.
Studies from Europe have shown higher frequencies of crown–root fractures, root fractures, and lateral luxations among adults as compared to adolescents and children.11 The NHANES-III study examined more than 7700 individuals in the age group of 5–60 years and reports higher prevalence of incisal trauma, of both maxillary and mandibular incisors, in both the younger and older age groups.4 Similar data on TDIs among adults in India is not available.
In India, RTA injuries and deaths have increased dramatically in the last two decades. There has been more than a three-fold increase in the number of persons injured per 100,000 of population from 13 in 1970 to 42.3 in 2011.12 India also tops the global list of fatalities from road traffic accidents with the State of Tamil Nadu topping the list by accounting for almost 11.5% of the total RTA fatalities in the country.13 This study aims to report and compare the distributions of TDIs among adults in a sub-population in India.
Methods
The study received ethical approval from the Institutional Ethics Committee of the Chettinad Academy of Research and Education, Tamil Nadu, India, and is reported based on the guidelines of the strengthening the reporting of observational studies in epidemiology (STROBE) statement.14 The study was conducted in accordance with the World Medical Association Declaration of Helsinki, and written consent was obtained from each of the participants before commencement of the study.
Using 30% as the estimated prevalence of patients with traumatic dental injuries, with a precision of the estimate at 10% level, it was calculated that 896 patients would be required.1 Accounting for an assumed design effect of 1.2 and also the non-response rates, the final sample size was fixed at 1500 patients. The study included 1562 consecutively selected patients (1218 males and 344 females) at the Chettinad Dental College and Research Institute, Tamil Nadu, in India, during the period from July 2014 to June 2018. Cases with incomplete documentation or TDI affecting primary dentition were excluded.
The clinical examinations were performed by a single trained and calibrated endodontist. Excellent intra-examiner reliability (kappa=0.90) for TDI classification was observed, as assessed in a subsample of 10 patients, who were not part of the final sample. The following data were obtained from each patient: 1) age; 2) gender; 3) cause of TDI; 4) tooth involved; 5) classification of TDIs; and 6) and time elapsed before seeking dental care. Only TDIs to anterior teeth were recorded (canine to canine in the maxilla and mandible) and classified using a modified version of the WHO’s classification.15 Intraoral periapical and panoramic radiographs were also taken for all the subjects.
TDI data was tabulated as frequency distributions in percentages. The data management and analysis were carried out, using statistical software SPSS 22.0 (Statistical Package for the Social Sciences for Windows; SPSS Inc., Chicago, IL, USA).
Results
A total of 1562 patients aged between 20 and 73 years, with a mean age of 36 years, were examined during the study period. A total of 1562 panoramic radiographs and 3457 periapical radiographs were assessed in this study. The total number of teeth with TDIs was 3044, and males (78%) clearly outnumbered the females (22%) in all the age groups (Figure 1). The number of TDIs in conjunction with other bodily injuries was 42.2% (n= 662).
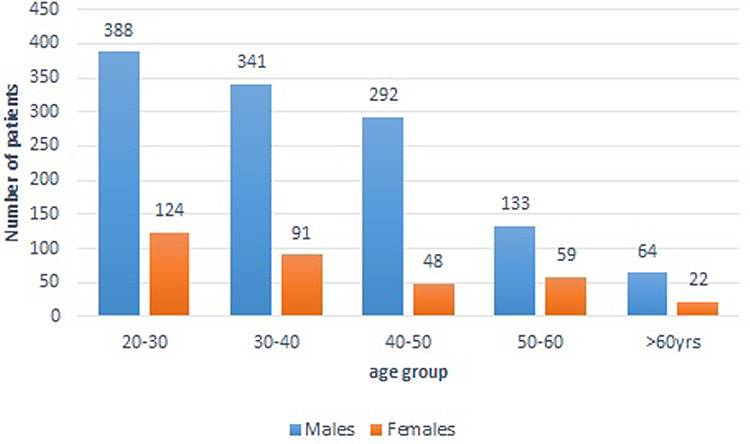 |
Figure 1 Age distribution of male and female participants. |
The most common type of injury occurring in both the genders is uncomplicated crown fractures (male=31.0% and female=36.6%) (Table 1). Table 2 presents the distribution of TDIs among 1562 patients by cause of injury and teeth involved. The most commonly affected tooth was the upper left maxillary incisor (38.5%) followed by the upper right maxillary incisor (33.9%). About two-third of the TDIs were caused by road traffic accidents (RTA) followed by falls (20%). Fight/interpersonal violence and sports-related injuries accounted for approximately 6% and 7% of the patients, respectively. Other causes of TDIs included epileptic seizures, drowsiness due to prescription medications and unknown etiology which comprised only a small fraction of the total TDIs.
 |
Table 1 Frequency Distribution of Teeth with Fractures and Luxations by Gender |
 |
Table 2 Distribution of TDIs Among 1562 Patients by Cause of Injury and Teeth Involved |
The type of injury most frequently seen within the first hour post-trauma was avulsion (Table 3). Uncomplicated crown fractures were mostly seen 1 week post-trauma, in contrast to complicated crown fractures which were seen within 1–6 hours post-trauma. Most tooth fractures were reported to the dentist after a considerable delay, and most of the luxation injuries were seen within the first 24 hours post-trauma.
 |
Table 3 Frequency Distribution of the Type of Injury and the Time Elapsed to Seek Dental Treatment |
Discussion
This study reports the distributions of TDIs among adults in a sub-population in southern India. Several epidemiological studies investigating traumatic injuries are retrospective studies.8,16–19 However, the present study is a prospective observational study, conducted over a period of 4 years. The advantage of such study over a retrospective one is that the data is more reliable as the data is collected as the incident occurs and therefore recall bias is less.20
This study found out that TDI is more prevalent in males than in females. Similar results have been reported from studies across the world.18,19,21 This underscores the fact that outdoor activities/travel and sports are promoted more among males rather than females, more so in India. Maxillary central incisor is the most frequently injured teeth in our study, and our finding is in accordance with several previous studies.4,8,17 The primary reason for the higher incidence of trauma in the central incisors is its position in the jaw, especially in cases with an increased overjet.22
The results reveal that the commonest etiology of TDI in this population is due to road traffic accidents. Chaotic traffic and poor implementation of road safety rules in the developing countries contributes towards the high incidence of TDIs. Driving under the influence of alcohol and infrequent use of protective headgear/helmet can contribute towards the higher incidence of TDIs in this population.23 Another possible explanation of RTA topping the etiology of TDIs are linked to the prevalence of higher number of motorcycles in India eventually leading to increased number of two-wheeler RTA.24
Most of the patients with tooth fractures reported to the dental hospital after substantial delay. The more severe injuries like complicated tooth fracture and avulsion are more likely to be reported to the dentist within 24hrs than the less severe injuries like enamel–dentin fractures. Lack of affordability and accessibility to quality dental care can be one of the reasons for the delay/reluctance of the patients to seek treatment. Also, this institution is located in a semi-rural area catering to people with lower-income group. This urban–rural divide is also very prominent in a developing country like India. The comparatively faster reporting of complicated tooth fracture in our study might be attributed to possible pain and esthetics experienced by patients over uncomplicated tooth fracture injuries, reiterating the insufficient knowledge status of the patients over long-term effects of dental injuries. Research conducted in several other countries also demonstrated that the information regarding management of TDI is insufficient among the lay people.25,26 Several studies show that the knowledge of emergency treatment of dental trauma is inadequate even among health care professionals.27–30 Awareness of first aid and importance of reaching the dental office without delay must be reinforced.
The need for these studies stems from the fact that the data collected about the traumatic injuries will help in identifying the risk groups, which in turn will assist the public health authorities to implement strong preventive programs in the state. Furthermore, awareness about TDI and its immediate management should be integrated into the public health system. Efforts should also be directed towards raising the community’s awareness about the various preventive measures.
This study has few potential limitations: 1) The data were collected from one hospital which limits the generalizability of the study results and 2) combination injuries of luxation and fractures were not recorded and this increases the risk of overlooking the minor concomitant injuries.
Conclusion
Uncomplicated crown fracture was the most commonly observed type of TDI, and RTAs were the primary cause of TDI in this population. The more severe injuries like complicated tooth fracture and avulsion are more likely to be reported to the dentist within 24hrs than the less severe injuries like enamel–dentin fractures.
Abbreviations
RTA, road traffic accidents; TDI, traumatic dental injury; NHANES, National Health and Nutrition Examination Survey.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained for study participation. The research was conducted in accordance with the World Medical Association Declaration of Helsinki and approved by the Institutional Ethics Committee of the Chettinad Academy of Research and Education, Tamil Nadu, India.
Consent for Publication
Not Applicable.
Acknowledgments
The authors thank all the patients who agreed to participate in this study.
Author Contributions
AR and SIRK designed the study and have taken an active role in data collection, analysis and drafting and revising the manuscript. JKB and MA took an active role supervising the study and drafting the manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study did not receive any financial support.
Disclosure
The authors declare that there are no competing interests.
References
1. Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis – one billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34(2):71–86. doi:10.1111/edt.12389
2. Andersson L. Epidemiology of traumatic dental injuries. J Endod. 2013;39(3 Suppl):S2–5. doi:10.1016/j.joen.2012.11.021
3. Petersson EE, Andersson L, Sorensen S. Traumatic oral vs non-oral injuries. Swed Dent J. 1997;21(1–2):55–68.
4. Kaste LM, Gift HC, Bhat M, Swango PA. Prevalence of incisor trauma in persons 6–50 years of age: United States, 1988–1991. J Dent Res. 1996;75:. doi:10.1177/002203459607502S09
5. Ankola AV, Hebbal M, Sharma R, Nayak SS. Traumatic dental injuries in primary school children of South India – a report from district-wide oral health survey. Dent Traumatol. 2013;29(2):134–138. doi:10.1111/j.1600-9657.2012.01139.x
6. Basha S, Mohammad RN, Swamy HS. Incidence of dental trauma among obese adolescents – a 3-year-prospective study. Dent Traumatol. 2015;31(2):125–129. doi:10.1111/edt.12137
7. Mathur MR, Watt RG, Millett CJ, Parmar P, Tsakos G. Determinants of socioeconomic inequalities in traumatic dental injuries among urban Indian adolescents. PLoS One. 2015;10(10):e0140860. doi:10.1371/journal.pone.0140860
8. Brunner F, Krastl G, Filippi A. Dental trauma in adults in Switzerland. Dent Traumatol. 2009;25(2):181–184. doi:10.1111/j.1600-9657.2008.00752.x
9. Ivancic Jokic N, Bakarcic D, Fugosic V, Majstorovic M, Skrinjaric I. Dental trauma in children and young adults visiting a university dental clinic. Dent Traumatol. 2009;25(1):84–87. doi:10.1111/j.1600-9657.2008.00711.x
10. Locker D. Self-reported dental and oral injuries in a population of adults aged 18–50 years. Dent Traumatol. 2007;23(5):291–296. doi:10.1111/j.1600-9657.2006.00457.x
11. Hecova H, Tzigkounakis V, Merglova V, Netolicky J. A retrospective study of 889 injured permanent teeth. Dent Traumatol. 2010;26(6):466–475. doi:10.1111/j.1600-9657.2010.00924.x
12. Ruikar M. National statistics of road traffic accidents in India. J Orthopedics Traumatol Rehab. 2013;6(1):1. doi:10.4103/0975-7341.118718
13. National Crime Records Bureau. Ministry of Home Affairs. Government of India. Accidental deaths and suicides in India; 2010.
14. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
15. Andreasen JO, Bakland LK, Flores MT, Andreasen FM, Andersson L. Classification of dental injuries. In: Andreasen JO, Bakland LK, Flores MT, Andreasen FM, Andersson L, editors. Traumatic Dental Injuries – A Manual.
16. Atabek D, Alacam A, Aydintug I, Konakoglu G. A retrospective study of traumatic dental injuries. Dent Traumatol. 2014;30(2):154–161. doi:10.1111/edt.12057
17. Bratteberg M, Thelen DS, Klock KS, Bardsen A. Traumatic dental injuries – prevalence and severity among 16-year-old pupils in western Norway. Dent Traumatol. 2018;34(3):144–150. doi:10.1111/edt.12399
18. Lauridsen E, Hermann NV, Gerds TA, Kreiborg S, Andreasen JO. Pattern of traumatic dental injuries in the permanent dentition among children, adolescents, and adults. Dent Traumatol. 2012;28(5):358–363. doi:10.1111/j.1600-9657.2012.01133.x
19. Yamamoto K, Matsusue Y, Horita S, et al. Trends and characteristics of maxillofacial fractures sustained during sports activities in Japan. Dent Traumatol. 2018;34(3):151–157. doi:10.1111/edt.12395
20. Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000;45(1):2–9. doi:10.1111/j.1834-7819.2000.tb00234.x
21. Lexomboon D, Carlson C, Andersson R, von Bultzingslowen I, Mensah T. Incidence and causes of dental trauma in children living in the county of Varmland, Sweden. Dent Traumatol. 2016;32(1):58–64. doi:10.1111/edt.12218
22. Andreasen JO. Etiology and pathogenesis of traumatic dental injuries. A clinical study of 1298 cases. Scand J Dent Res. 1970;78(4):329–342. doi:10.1111/j.1600-0722.1970.tb02080.x
23. Ravikumar R. Patterns of head injuries in road traffic accidents involving two wheelers: an autopsy study. J Indian Acad Forensic Med. 2013;35(4):971–973.
24. Pathak SM, Jindal AK, Verma AK, Mahen A. An epidemiological study of road traffic accident cases admitted in a tertiary care hospital. Med J Armed Forces India. 2014;70(1):32–35. doi:10.1016/j.mjafi.2013.04.012
25. Glendor U. Has the education of professional caregivers and lay people in dental trauma care failed? Dent Traumatol. 2009;25(1):12–18. doi:10.1111/j.1600-9657.2008.00707.x
26. McIntyre JD, Lee JY, Trope M, Vann WF
27. De carvalho cardoso L, Poi WR, Panzarini SR, et al. Knowledge of firefighters with special paramedic training of the emergency management of avulsed teeth. Dent Traumatol. 2009;25(1):58–63. doi:10.1111/j.1600-9657.2008.00684.x
28. Zhao Y, Gong Y. Knowledge of emergency management of avulsed teeth: a survey of dentists in Beijing, China. Dent Traumatol. 2010;26(3):281–284. doi:10.1111/j.1600-9657.2010.00877.x
29. Al-Haj Ali SN, Algarawi SA, Alrubaian AM, Alasqah AI. Knowledge of general dental practitioners and specialists about emergency management of traumatic dental injuries in Qassim, Saudi Arabia. Int J Pediatr. 2020;2020.
30. Ali SNA-H. Awareness of emergency management of dental trauma among mothers in Al-Qassim, Saudi Arabia. Int J Stomatol Occlusion Med. 2016;8(S1):25–29. doi:10.1007/s12548-015-0140-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.