Back to Journals » Patient Preference and Adherence » Volume 16
Patients’ Satisfaction with Ophthalmology Clinic Services in a Public Teaching Hospital
Authors Sakti DH ![]() , Firdaus AT, Utami TP, Jati KDP
, Firdaus AT, Utami TP, Jati KDP ![]() , Mahayana IT
, Mahayana IT ![]() , Wardhana FS, Handayani N
, Wardhana FS, Handayani N
Received 2 November 2021
Accepted for publication 4 March 2022
Published 19 March 2022 Volume 2022:16 Pages 723—735
DOI https://doi.org/10.2147/PPA.S347394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Dhimas Hari Sakti,1,2 Aufar Tirta Firdaus,1 Tiara Putri Utami,1 Krisna Dwi Purnomo Jati,1,2 Indra Tri Mahayana,1,2 Firman Setya Wardhana,1,2 Novika Handayani3
1Department of Ophthalmology, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 2Department of Ophthalmology, Dr. Sardjito General Hospital, Yogyakarta, Indonesia; 3Center for Health Policy and Management, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Correspondence: Dhimas Hari Sakti, Department of Ophthalmology, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Jl. Farmako Sekip Utara, Yogyakarta, 55281, Indonesia, Tel +62 274 560300, Email [email protected]
Purpose: To evaluate patients’ satisfaction with ophthalmology health services in a teaching clinic of a tertiary public hospital.
Patients and Methods: This was a cross-sectional study in ophthalmology clinic of Dr. Sardjito teaching hospital, Yogyakarta, Indonesia conducted in 2019. Patients were surveyed using the Patient Satisfaction Questionnaire-18 (PSQ-18). PSQ-18 subscale score was analyzed based on patients’ characteristics. The main outcome was the odds of reaching top satisfaction score (TSS) of 4– 5 from a Likert scale 1 to 5.
Results: Our study recorded 269 participants who consisted of 138 males (51.3%) and 131 females (48.7%) with median age of 52 (18– 87) years old. Variables with higher odds of reaching TSS on “patient overall satisfaction” was public health insurance (OR: 7.959 [95% CI: 1.989– 31.852], p=0.003) while examination time (OR: 0.955 [95% CI: 0.923– 0.988], p=0.008) had lower odds. Examination waiting time (OR: 0.992 [95% CI: 0.985– 0.999], p=0.027) and examination time (OR: 0.941 [95% CI: 0.908– 0.976], p=0.001) had lower odds of reaching TSS in “general satisfaction”. Family monthly income (OR: 1.829 [95% CI: 1.038– 3.223], p=0.037) had higher odds of reaching TSS in “technical quality” while examination time (OR: 0.961 [95% CI: 0.931– 0.993], p=0.017) and education (OR: 0.549 [95% CI: 0.322– 0.934], p=0.027) had lower odds. Comorbidities (OR: 0.533 [95% CI: 0.301– 0.944], p=0.031) had lower odds of reaching TSS in “financial aspects”. Retina subspecialty clinic (OR: 3.436 [95% CI: 1.154– 10.232], p=0.027) had higher odds of reaching TSS in “time spent with doctor”. Registrar as attending physician (OR: 0.427 [95% CI: 0.205– 0.89], p=0.0230) and examination time (OR: 0.957 [95% CI: 0.924– 0.991], p=0.013) had lower odds of reaching TSS in “accessibility-convenience”.
Conclusion: Examination time and examination waiting time should be shortened, specialist doctors should always see the patients whenever possible, and registrars’ technical and communication skill should be improved. Alternative funding for patients without health insurance also should be provided to increase satisfaction.
Keywords: Patient Satisfaction Questionnaire-18, PSQ-18, health service quality, examination time, health survey
Introduction
There are approximately 3 million people (1.5% of population) living with blindness in Indonesia making it one of the biggest causes of social and economic burden within the society.1 Accordingly, the quality of ophthalmology health service should be one of the main concerns in a health service institution. Patient’s satisfaction is essential for improving the quality of healthcare and vice versa.2 Patient’s satisfaction is expected to lead to better compliance to treatment and therefore a better patient outcome.3
The Indonesian health care system is developing to resemble health system similar in European countries with the tax based public funding. However in 2017, public health care funding was only 37.8% while private funding, mainly out of pocket payment, contributed 62.2%.4 Patients in Indonesia are also able to go to a specialist doctor in a private clinic or hospital directly without referral from a general practitioner. As a result, middle-upper income patients tend to go directly to the specialist. Scheduled doctor appointments are unusual resulting in longer time spent in any health service.
Patients’ satisfaction has been studied in Indonesia on various settings but rarely in ophthalmology health service.5–10 Previous studies in ophthalmology settings have been conducted around the globe with different instruments.3,11–14 Ideally, a standardized tool that can be used across multi-disciplines is used to enable comparison among them. The Patient Satisfaction Questionnaire Short Form (PSQ-18) is a general and relatively short satisfaction questionnaire that can be used for this purpose and has been used in ophthalmology clinics previously.3,15,16
Given the different health care system of Indonesia compared to other countries, the aim of this study was to determine the patients’ satisfaction toward health services quality in ophthalmology clinic in Indonesia using PSQ-18.
Materials and Methods
Design and Subjects
This was a cross-sectional study in the ophthalmology clinic of Dr. Sardjito teaching hospital, Yogyakarta, Indonesia conducted in July-September 2019. The Patient Satisfaction Questionnaire Short Form (PSQ-18) was translated into the Indonesian language by a certified English translator and approved by a consultant ophthalmologist (head of ophthalmology health service). Using Isaac and Michael table, the minimum number of samples needed to reach 5% error rate was 297.17 This study followed the tenets of the Declaration of Helsinki and was approved by Medical and Health Research Ethical Committee of the Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia. Simple randomization of the patients was done using www.randomizer.org limited to 8 patients per day to avoid selection bias and achieve a ratio of participants similar with the usual patient distribution in our ophthalmology clinic based on subspecialty. Written informed consent for study participation and data publication was obtained from all study participants. Underage (<18 years old) participants consent form and questionnaire were completed by their guardians.
The study population was all established patients in the ophthalmology clinic. This population was chosen since the interviews could be conveniently done before their scheduled eye examination on the same day. Previous experience in our clinic showed that patients were reluctant to join a survey if it was done after their examination. The questionnaires’ data were obtained by one trained data collector (medical doctor) after the patients had their blood pressure (BP) checked by a nurse. The completion of the forms was assisted by the interviewer, especially for the visually impaired participants. The participants then were given the forms to record BP waiting time, examination waiting time, examination time, and positive-negative feedback.
Data Analysis
The PSQ-18 questionnaires consists of 18 questions with a Likert scale for answers ranging from 1–5. Scores from the 18 questions were divided into 7 subscales of PSQ-18 namely
General Satisfaction (2 questions), Technical Quality (4 questions), Interpersonal Manner (2 questions), Communication (2 questions), Financial Aspect (2 questions), Time Spent With Doctor (2 questions), and Accessibility-Convenience (4 questions)
and coded according to the development study by Marshall and Hays.18 The scores from these 7 subscales were averaged into a new subscale called “Patient’s overall satisfaction” to enable analysis consisting all the subscale. Score of 4–5 in was classified as reaching top satisfaction score (TSS) and described as a satisfied patient. Then the odds of reaching TSS on “patient’s overall satisfaction” and satisfied score on each PSQ-18 subscales were analyzed using binary logistic regression analysis based on patients’ demographic and health service characteristics (age, sex, ethnicities, education, occupation, marital status, family monthly income, health insurance, visual acuity (VA), comorbidities, subspecialty clinics, attending physicians, BP measurement waiting time, examination waiting time, examination time, and total time spent in clinic). BP measurement waiting time, examination waiting time, examination time, and total time spent in clinic were further analyzed using Independent-samples median test according to the subspecialty clinic. Internal reliability was tested using Cronbach’s alpha. The English (Supplemental Table 1) and Indonesian (Supplemental Table 4) version of the questionnaires are available in the supplemental data with its coding (Supplemental Table 2) and scoring (Supplemental Table 3) instruction.
Results
A total of 301 patients were asked to join the study with 1 patient who refused. Then it was decided to exclude non-adult participants from the PSQ-18 analysis to avoid bias since the form was completed by the guardians. As the result, a total of 269 participants were analysed consisting of 138 males (51.3%) and 131 females (48.7%) with median age of 52 years (18–87) (Table 1).
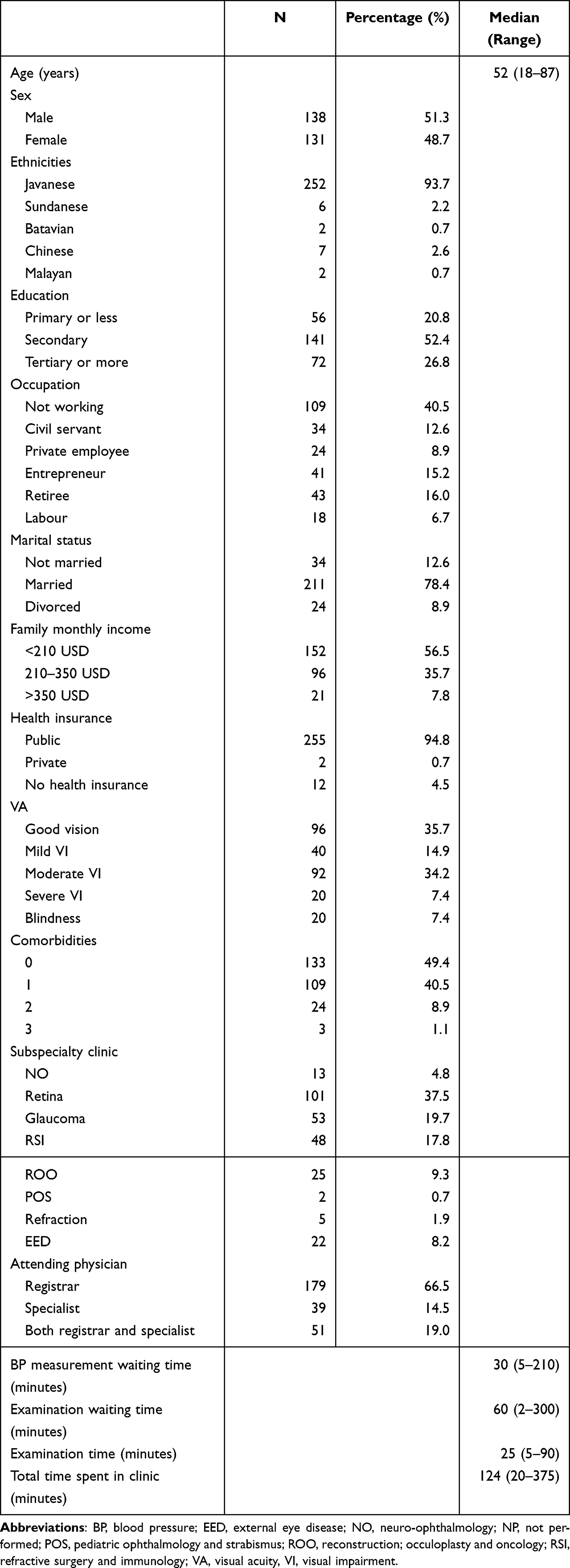 |
Table 1 Patient’s Demographic and Health Service Characteristic |
PSQ-18 Internal Reliability
The Cronbach’s alpha was 0.689. If deleted, “communication” subscale can improve the Cronbach’s alpha to 0.721 (Table 2).
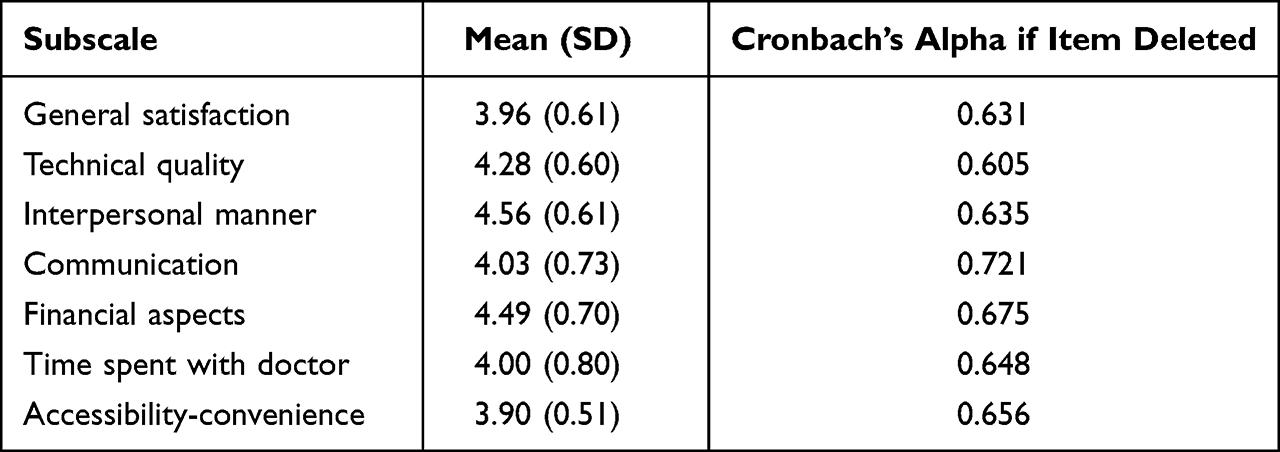 |
Table 2 Average of PSQ-18 Subscales Score and Internal Reliablity |
PSQ-18 Scores
“Interpersonal manner” subscale had the highest average score with 4.56 (0.61) while “accessibility-convenience” had the lowest with 3.90 (0.51) (Table 2). Univariate analysis on “patient’s overall satisfaction” found that age (OR: 1.027 [95% CI: 1.009–1.045], p=0.003) and public health insurance (OR: 5.727 [95% CI: 1.67–19.644], p=0.006) had higher odds of reaching TSS while not married marital status (OR: 0.296 [95% CI: 0.09–0.976], p=0.046), examination time (OR: 0.954 [95% CI: 0.988–1], p=0.002), and total time spent in clinic (OR: 0.994 [0.90–0.999], p=0.018) had lower odds of reaching TSS.
Multivariate analysis on “patient’s overall satisfaction” found that public health insurance (OR: 7.959 [95% CI: 1.989–31.852], p=0.003) had higher odds of reaching TSS while examination time (OR: 0.955 [95% CI: 0.923–0.988], p=0.008) had lower odds. Multivariate analysis was also done for each PSQ-18 subscales. Examination waiting time (OR: 0.992 [95% CI: 0.985–0.999], p=0.027) and examination time (OR: 0.941 [95% CI: 0.908–0.976], p=0.001) had lower odds of reaching TSS in “general satisfaction” subscale. Family monthly income (OR: 1.829 [95% CI: 1.038–3.223], p=0.037) had higher odds of reaching TSS in “technical quality” subscale while examination time (OR: 0.961 [95% CI: 0.931–0.993], p=0.017) and education (OR: 0.549 [95% CI: 0.322–0.934], p=0.027) had lower odds. Comorbidities (OR: 0.533 [95% CI: 0.301–0.944], p=0.031) had lower odds of reaching TSS in “financial aspects” subscale. Retina subspecialty clinic (OR: 3.436 [95% CI: 1.154–10.232], p=0.027) had higher odds of reaching satisfied score in “time spent with doctor” subscale. Registrar as attending physician (OR: 0.427 [95% CI: 0.205–0.89], p=0.0230) and examination time (OR: 0.957 [95% CI: 0.924–0.991], p=0.013) had lower odds of reaching satisfied score in “accessibility-convenience” subscale (Table 3 and Figure 1).
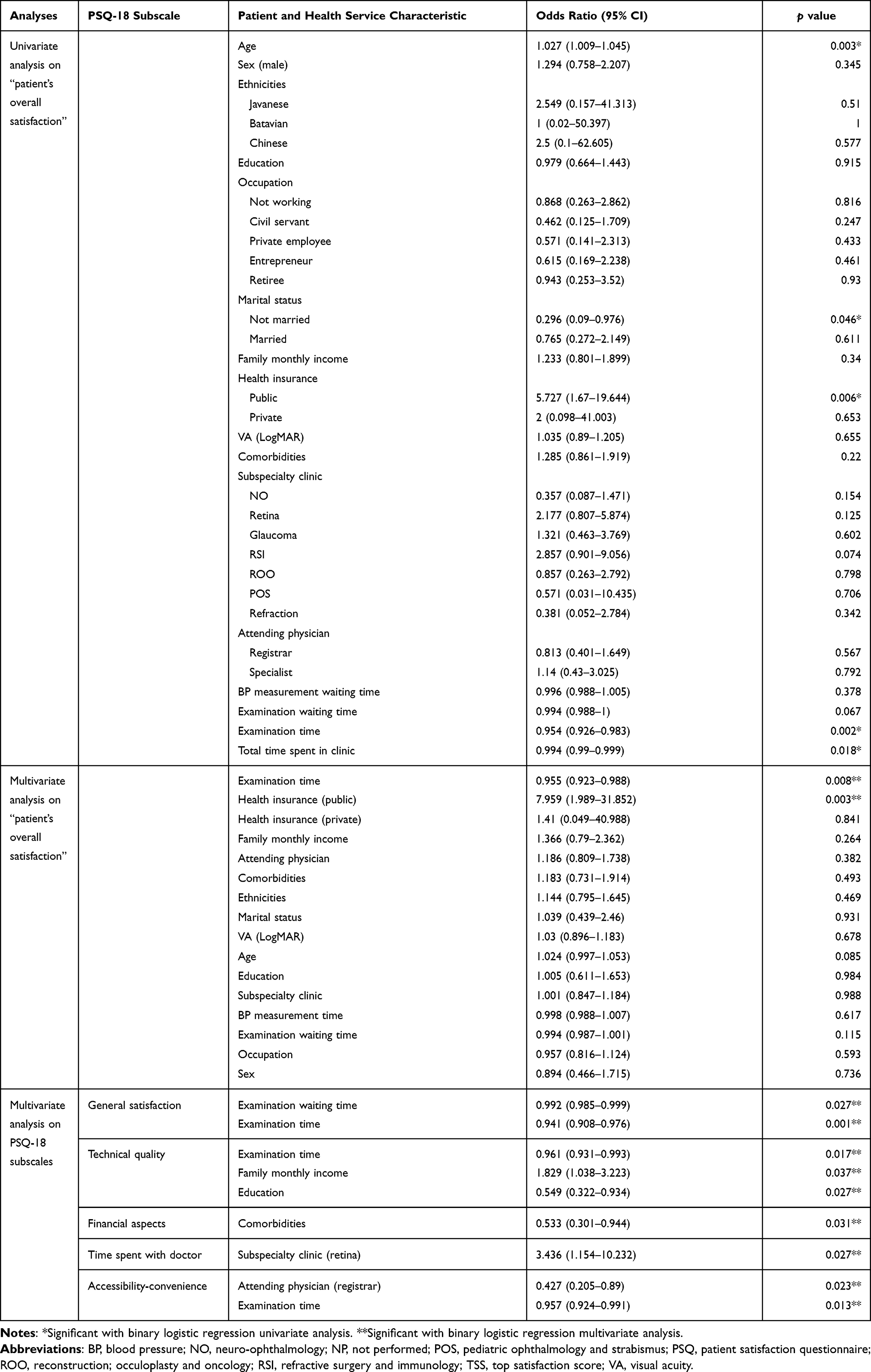 |
Table 3 Univariate and Multivariate Analyses of Patient’s Demographic and Health Service Characteristic on Reaching TSS |
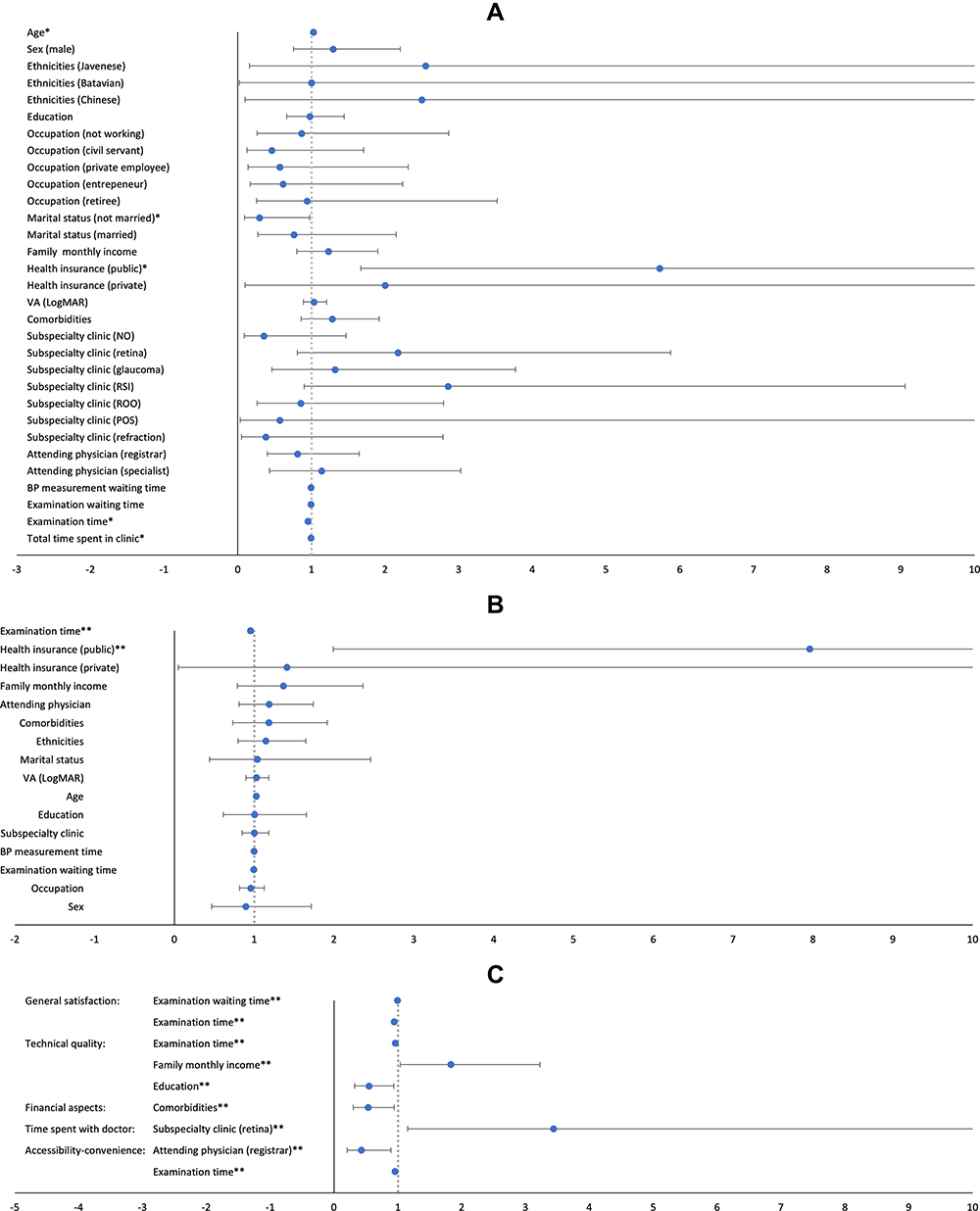 |
Figure 1 Forest plot of univariate and multivariate analyses of patient and health service characteristic on reaching TSS. (A) Univariate analysis on “patient’s overall satisfaction”. Reference group for marital status and health insurance were “divorced” and “no health insurance” respectively. (B) Multivariate analysis on “patient’s overall satisfaction”. Reference group for health insurance was “no health insurance”. (C) Multivariate analysis on each subscale of PSQ-18. Reference groups for subspecialty clinic and attending physician were “EED” and “both registrar and specialist” respectively. There was no significant multivariate analysis found on “interpersonal manner” and “communication” subscales. |
Examination and Waiting Time per Subspecialty
There was no significant difference in BP measurement waiting time and examination waiting time between subspecialty clinic. Significant differences were found in examination time and total time with p values of 0.012 and 0.042 respectively. Pairwise analyses found significant difference in examination time between Retina vs NO with p value of 0.005 (Table 4).
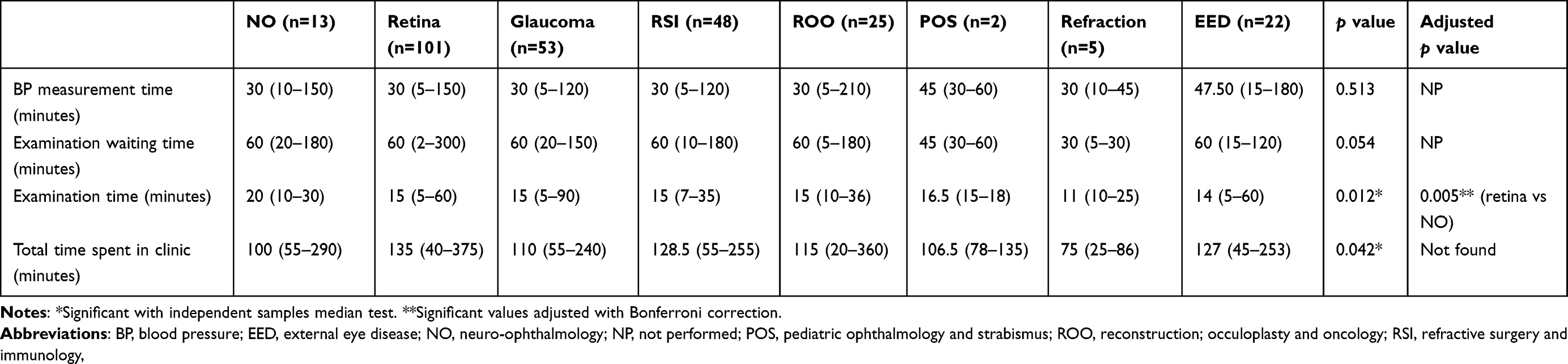 |
Table 4 Median and Range of BP Measurement Time, Examination Waiting Time, Examination Time, and Total Time Spent in Clinic Based on Subspecialty Clinic |
Open Feedback
Positive and negative feedback forms were completed by 89 patients (33.1%) and 124 patients (46.1%), respectively. One hundred and six (106) positive feedbacks were obtained, revealing “Overall service” (63.2%) and “Staff’s hospitality” (20.8%) as the most often mentioned (Table 5). One hundred and fifty eight (158) negative feedbacks were acquired, displaying “Waiting time” (53.2%) and “Staff’s communication” (13.3%) as the most mentioned (Table 5). “Staff” was defined as all people working in the clinic including the doctor, nurse, and the administrator.
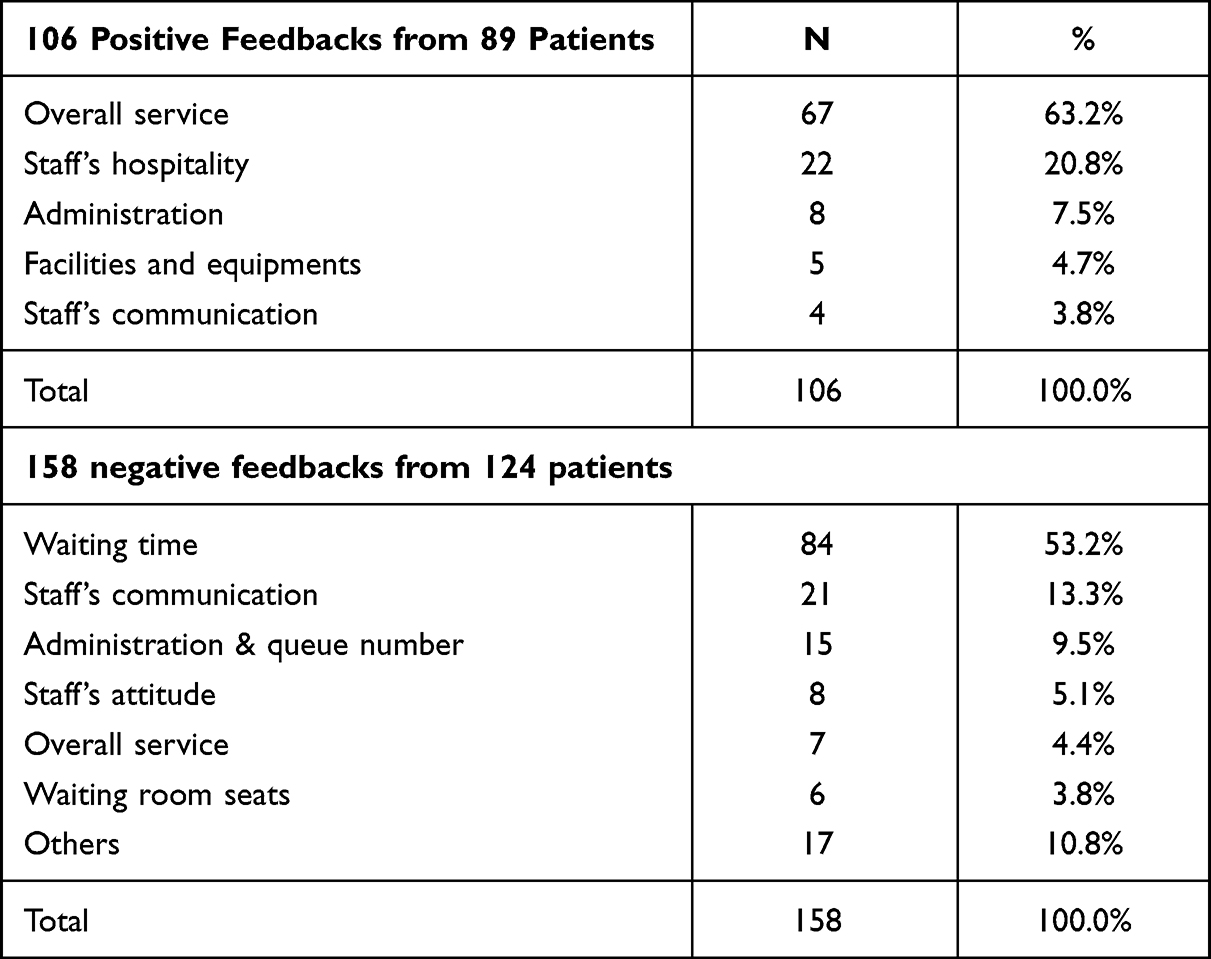 |
Table 5 Positive and Negative Feedbacks |
Discussion
Measuring patients’ satisfaction helps a medical service improve its business.19 PSQ-18 is a robust patients’ satisfaction instrument to be applied in multiple discipline and was developed using Cronbach’s alpha to assess the internal reliability.15,18 The overall Cronbach’s alpha coefficient of 0.689 found in our study can be classified as adequate.20 The English version of PSQ-18 gave a high coefficient in previous study,21 while the translated ones had high coefficient for the Spanish translation22 or low coefficient for the one in Hindi.23 A possible cause of our low result was its translation into the Indonesian language. The Delphi method and agreement measurement can be viable options to address this problem in the future study.16
In this study, the overall highest satisfaction score is the “interpersonal manner” subscale while the lowest satisfaction score is the “accessibility-convenience” subscale. “Interpersonal manner” subscale also had the highest score in previous study in ophthalmology or other settings.16,24–26 Another ophthalmology study also had “accessibility-convenience” subscale as the lowest.16 “Financial aspects” subscale was the lowest in a previous study of combined public-private hospital.24 Physician manner can be expressed by non-medical chat and patient’s opportunity to give feedback, which are related to higher satisfaction.27,28 It was underlined from studying the National Health Services (NHS) of England that compassion, expressed in a physician manner, is an inherent aspect of health care.29 On the other hand, low score on “accessibility-convenience” subscale found in our study might be attributed to the relatively long waiting time during visits in our teaching clinic.
Our participants preferred shorter examination time. It was reflected from “patient’s overall satisfaction”, “general satisfaction”, “technical quality”, and “accessibility-convenience” subscale. On the contrary, previous studies showed that longer time spent with physician correlated with higher patients’ satisfaction.11,27,28,30,31 Further exploration needs to be done to answer this preference of shorter examination time. It might be due to the fact that the patients spent a relatively long waiting time before the examination. Therefore, they want a quick examination since afterwards they also might need to go to other departments on the same day.
Compared to no health insurance, patients with public health insurance had higher odds of reaching satisfaction in “patient’s overall satisfaction”. Concordantly, a study in Ghana found a similar result.32 Study by Bohm found that American patients with employer based insurance had a higher satisfaction than patients with Canadian national insurance.33 On the other hand, insurance type did not affect satisfaction in previous studies in ophthalmology and other settings.8,12,34 Alternative funding should be offered to address the unsatisfied patients with no insurance in our study.
Shorter examination waiting time was also preferred, reflected in the “general satisfaction” subscale. We also recorded more negative feedbacks than the positive one, mainly for the “waiting time” since at the time this study commenced, there was no time appointment system for the patients’ queue. Patients with scheduled appointment had a higher satisfaction compared to patients in walk-in clinic.35 Waiting time was found as the main influence for patient satisfaction in the ophthalmology clinic.13 On the other hand, perception towards waiting time and not the actual waiting time was found to have more influence on patient satisfaction.36 Patients might accept the actual time as long as they are kept informed. Lean Six Sigma techniques derived from Toyota production system can be used to improve patients’ flow time.37
Family monthly income had higher odds of reaching satisfied patient in “technical quality”. Similarly, Detollenaere et al found that low income patients had lower satisfaction for their general practitioner38 while no association found between income and satisfaction in previous study by Hall et al.39 On the other hand, Ganasegaran et al found that higher income had lower satisfaction.21 The income appears to gave different satisfaction results in different settings.
Increased education level had lower odds of reaching satisfied patient in “technical quality”. Previous studies in ophthalmology and other settings found similar findings3,9,21,39 while other study found that education did not affect satisfaction.38 We hypothesized that higher educated patients possibly read or study about their condition first before meeting the doctor. Consequently, they ask more questions and demanding more explanation.
Comorbidities was associated with lower odds of satisfied patients in the “financial aspects” subscale. More comorbidities led to low satisfaction score. Ezat et al found that comorbidities affected “interpersonal manner”, “time spent with doctor”, and “technical quality” subscales.40 This findings is understandable since patients with more comorbidities probably need to spend more money for their overall condition and have more difficulty to work to earn money.
Retina subspecialty clinic had higher odds of satisfied patients in “time spent with doctor” subscale. Previous study found marital status, stage of disease, duration of the disease, comorbidities, and financial affected this subscale.40 Vitreoretinal surgery department also increased the odds of satisfaction in the univariate analysis of Han et al but not in their multivariate analysis.12 Interestingly, retina subspecialty clinic did not have the longest examination time in our study (Table 4). However, this was the only subspecialty clinic at the time of study that have a specialist doctor available every working day with full-time working hours and might be the reason for our specific finding suggesting the importance of specialist attendance.
Furthermore, registrar as attending physician had lower odds of satisfied patient in the “accessibility-convenience” subscale. On the contrary, using PSQ-18 adaptation Jagadeesan et al found that patients were generally satisfied with the service provided by registrar.41 In emergency medicine setting, patients were more satisfied with the registrar compared with the supervising doctor.42 Our finding suggested that a specialist doctor should always see the patients whenever possible to improve patients’ satisfaction as also reflected by our finding in the retina subspecialty clinic. Technical and communication skill of the registrar should also be improved to address this issue.
In the univariate analysis of this study, older age was associated with more satisfaction. On the contrary, previous studies in ophthalmology settings found that older age was related to less satisfaction.3,14
Examination waiting time, examination time, family monthly income, education, comorbidities, subspecialty clinic, and attending physician influenced patient’s satisfaction in our study. These significant associations were partly in concordance to the results of the previous meta-analysis study which found that satisfaction was significantly associated various characteristics such as age, education, marital status, and social status while no relationship was found with ethnicity, sex, income, and family size.39 Sixma et al also found that patient’s demographic factors contributed to 90–95% of variance in satisfaction scores.43 Patient’s satisfaction studies results were varied as the consequence of no single globally accepted instrument to measure satisfaction.44 Patients with negatively framed survey had a significant lower satisfaction compared to patients with positively framed survey creating a potential bias.45 However, PSQ-18 was designed with equal number of negative and positive framed survey questions.18
Patient centered health service is the ultimate goal as 70% of patients would not go back after dissatisfaction and 75% would tell at least 9 relatives not to go.46–48 Although important, technical quality improvement alone does not directly translate into better patient-perceived quality care.49 Healthcare providers should evaluate themselves through the patients’ eyes and improvement should be implemented as “work smarter rather than harder”.50,51 This improvement also needs to be supported by the leaders of the healthcare through their policies.52 Technology use, patient flow redesigning, and offering distractions could improve the actual wait time and the satisfaction itself.53 In addition, big data from social media could be the answer to assess healthcare quality because it can capture the candid experiences of the patients.54,55
There were some limitations of this study. Surveys were given in established patients before they had new health services in the day of surveying. Therefore, recall bias might affect the results of the survey. However, there was an evidence that satisfaction survey done after 2 weeks and 3 months had a higher satisfaction compared to immediately after visit.56
Conclusions
Examination time and examination waiting time should be shortened, specialist doctors should always see the patients whenever possible, and registrars' technical and communication skill should be improved. Alternative funding for patient without health insurance also should be provided to increase satisfaction.
Acknowledgments
Authors thank all ophthalmology clinic team for their support during the study. Authors also want to thank Mr. S. Darmadi, Dr. M.B. Sasongko, and Dr. G. van Empel for their advice of statistical methods.
Funding
This study was funded by Sardjito General Hospital Research Grant HK. 02.03/ XI.2/19030/ 2018.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Indonesian Ophthalmologists Association. Vision 2020 in Indonesia. 2017; Available from: https://perdami.or.id/2017/07/16/vision-2020-di-indonesia/.
2. Naidu A. Factors affecting patient satisfaction and healthcare quality. Int J Health Care Qual Assur. 2009;22(4):366–381. doi:10.1108/09526860910964834
3. Peterson KM, Huisingh CE, Girkin C, Owsley C, Rhodes LA. Patient satisfaction with care in an urban tertiary referral academic glaucoma clinic in the US. Patient Prefer Adherence. 2018;12:775–781. doi:10.2147/PPA.S162439
4. Mahendradhata Y, Trisnantoro L, Listyadewi S, et al. The Republic of Indonesia Health System Review. India: World Health Organization; 2017.
5. Husain Akbar F, Tegar Jaya M. Relationship between service quality on public health center and patient satisfaction. Glob J Health Sci. 2017;9(7):96. doi:10.5539/gjhs.v9n7p96
6. Juhana D, Manik E, Febrinella C, Sidharta I. Empirical study on patient satisfaction and patient loyalty on public hospital in Bandung, Indonesia. Int J Appl Bus Econ Res. 2015;13(6):4305–4326.
7. Lestaringingsih T, Hadiyati E, Astuti R. Study of service quality and patient satisfaction to trust and loyalty in public hospital, Indonesia. Int J Bus Market Manag. 2018;3(2):1–12.
8. Dewi A, Ramadhan NK. The difference of satisfaction level in BPJS health insurance patient and non insurance patient toward health service. Int J Public Health Sci. 2016;5(1):36–40.
9. Kurniawan HD, Tamtomo D, Murti B. Contextual effect of community health center on patient satisfaction of health care service in Ngawi, East Java. J Health Policy Manag. 2019;4(1):23–30. doi:10.26911/thejhpm.2019.04.01.03
10. Widayati MY, Tamtomo D, Adriani RB. Factors affecting quality of health service and patient satisfaction in community health centers in north Lampung, Sumatera. Int J Health Policy Manag. 2017;02(02):165–175. doi:10.26911/thejhpm.2017.02.02.08
11. Long C, Tsay EL, Jacobo SA, Popat R, Singh K, Chang RT. Factors associated with patient press Ganey satisfaction scores for ophthalmology patients. Ophthalmology. 2016;123(2):242–247. doi:10.1016/j.ophtha.2015.09.044
12. Han MM, Hsueh J, Chen AX, et al. Ophthalmology provider ratings and patient, disease, and appointment factors. J Patient Exp. 2021;8:23743735211033750. doi:10.1177/23743735211033750
13. McMullen M, Netland PA. Wait time as a driver of overall patient satisfaction in an ophthalmology clinic. Clin Ophthalmol. 2013;7:1655–1660. doi:10.2147/OPTH.S49382
14. Obuchowska I, Lugowska D, Mariak Z, Konopinska J. Subjective opinions of patients about step-by-step cataract surgery preparation. Clin Ophthalmol. 2021;15:713–721. doi:10.2147/OPTH.S298876
15. Thayaparan AJ, Mahdi E. The Patient Satisfaction Questionnaire short form (PSQ-18) as an adaptable, reliable, and validated tool for use in various settings. Med Educ Online. 2013;18:21747. doi:10.3402/meo.v18i0.21747
16. Ziaei H, Katibeh M, Eskandari A, Mirzadeh M, Rabbanikhah Z, Javadi MA. Determinants of patient satisfaction with ophthalmic services. BMC Res Notes. 2011;4(7). doi:10.1186/1756-0500-4-7
17. Isaac S, Michael W. Handbook in Research and Evaluation. California: EDITS; 1995.
18. Marshall GN, Hays RD. The Patient Satisfaction Questionnaire Short Form (PSQ-18). Santa Monica, CA: RAND Corporation; 1994.
19. Riskind P, Fossey L, Brill K. Why measure patient satisfaction? J Med Pract Manage. 2011;26(4):217–220.
20. Taber KS. The use of Cronbach’s Alpha when developing and reporting research instruments in science education. Res Sci Educ. 2017;48(6):1273–1296. doi:10.1007/s11165-016-9602-2
21. Ganasegeran K, Perianayagam W, Manaf RA, Jadoo SA, Al-Dubai SA. Patient satisfaction in Malaysia’s busiest outpatient medical care. ScientificWorldJournal. 2015;2015:714754. doi:10.1155/2015/714754
22. Iglesias-Puzas A, de Miguel-abildua E, Conde-Taboada A, Iglesias-Bayo L, Lopez-Bran E. [Cross-cultural adaptation and Spanish validation of Patient Satisfaction Questionnaire in dermatology (PSQ-18)]. J Healthc Qual Res. 2021;36(5):269–274. Spanish. doi:10.1016/j.jhqr.2021.04.004
23. Shrivastava M, Shah N, Dixit A, Pandey M. Hindi translation and cross-cultural reliability and validity of Patient Satisfaction Questionnaire short form (PSQ-18). World J Psychosoc Oncol. 2017;4:1–7.
24. Ghazanfar A, Idress IN, Zia Z, Munir N, Maryam S. Comparison of patient’s satisfaction levels in public and private tertiary care centres. J Pak Med Assoc. 2017;67(8):1305–1308.
25. Chino F, Peppercorn J, Taylor DH, et al. Self-reported financial burden and satisfaction with care among patients with cancer. Oncologist. 2014;19:414–420. doi:10.1634/theoncologist.2013-0374
26. Chander V, Bhardwaj AK, Raina SK, Bansal P, Agnihotri RK. Scoring the medical outcomes among HIV/AIDS patients attending antiretroviral therapy center at Zonal Hospital, Hamirpur, using Patient Satisfaction Questionnaire (PSQ-18). Indian J Sex Transm Dis AIDS. 2011;32(1):19–22. doi:10.4103/0253-7184.81249
27. Gross D, Zyzanski S, Borawski E, Cebul R, Stange K. Patient satisfaction with time spent with their physician. J Fam Pract. 1998;47(2):133–137.
28. Zyzanski S, Stange K, Langa D, Flocke S. Trade-offs in high-volume primary care practice. J Fam Pract. 1998;46(5):397–402.
29. Fotaki M. Why and how is compassion necessary to provide good quality healthcare? Int J Health Policy Manag. 2015;4(4):199–201. doi:10.15171/ijhpm.2015.66
30. Anderson RT, Camacho FT, Balkrishnan R. Willing to wait?: the influence of patient wait time on satisfaction with primary care. BMC Health Serv Res. 2007;7:31. doi:10.1186/1472-6963-7-31
31. Lin C-T, Albertson GA, Schilling LM, et al. Is patients perception of time spent with the physician a determinant of ambulatory patient satisfaction? Arch Intern Med. 2001;161:1437–1442. doi:10.1001/archinte.161.11.1437
32. Fenny AP, Enemark U, Asante FA, Hansen KS. Patient satisfaction with primary health care - A comparison between the insured and non-insured under the National Health Insurance Policy in Ghana. Glob J Health Sci. 2014;6(4):9–21. doi:10.5539/gjhs.v6n4p9
33. Bohm J. Relating patient satisfaction to insurance coverage: a comparison of market based and government sponsored health care. Acad Bus Res J. 2013;1:1–11.
34. Devadasan N, Criel B, Damme WV, Lefevre P, Manoharan S, Stuyft P. Community health insurance schemes & patient satisfaction - evidence from India. Indian J Med Res. 2011;133:40–49.
35. Eilers GM. Improving patient satisfaction with waiting time. J Am Coll Health. 2004;53(1):41–43. doi:10.3200/JACH.53.1.41-48
36. Thompson DA, Yarnold PR, Williams DR, Adams SL. Effect of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the emergency department. Ann Emerg Med. 1996;28(6):657–665. doi:10.1016/S0196-0644(96)70090-2
37. Ciulla TA, Tatikonda MV, ElMaraghi YA, et al. Lean Six SIgma techniques to improve ophthalmology clinic efficiency. Retina. 2018;38:1688–1698. doi:10.1097/IAE.0000000000001761
38. Detollenaere J, Hanssens L, Schafer W, Willems S. Can you recommend me a good GP? Describing social differences in patient satisfaction within 31 countries. Int J Qual Health Care. 2018;30(1):9–15. doi:10.1093/intqhc/mzx157
39. Hall JA, Dornan MC. Patient sociodemographic characteristics as predictors of satisfaction with medical care: a meta-analysis. Soc Sci Med. 1990;30(7):811–818. doi:10.1016/0277-9536(90)90205-7
40. Ezat WPS, Fuad I, Hayati Y, Zafar A, Kiyah GAW. Observational study on patient’s satisfactions and Quality of Life (QoL) among cancer patients receiving treatment with palliative care intent in a tertiary hospital in Malaysia. Asian Pac J Cancer Prev. 2014;15(2):695–701. doi:10.7314/APJCP.2014.15.2.695
41. Jagadeesan R, Kalyan DN, Lee P, Stinnett S, Challa P. Use of a standardized patient satisfaction questionnaire to assess the quality of care provided by ophthalmology residents. Ophthalmology. 2008;115(4):738–743 e733. doi:10.1016/j.ophtha.2007.05.033
42. Lang SC, Weygandt PL, Darling T, et al. Measuring the correlation between emergency medicine resident and attending physician patient satisfaction scores using press Ganey. AEM Educ Train. 2017;1(3):179–184. doi:10.1002/aet2.10039
43. Sixma HJ, Spreeuwenberg PMM, Pasch MAAVD. Patient satisfaction with the general practitioner: a two-level analysis. Med Care. 1998;2:212–229. doi:10.1097/00005650-199802000-00010
44. Batbaatar E, Dorjdagva J, Luvsannyam A, Savino MM, Amenta P. Determinants of patient satisfaction: a systematic review. Perspect Public Health. 2017;137(2):89–101. doi:10.1177/1757913916634136
45. Dunsch F, Evans DK, Macis M, Wang Q. Bias in patient satisfaction surveys: a threat to measuring healthcare quality. BMJ Glob Health. 2018;3(2):e000694. doi:10.1136/bmjgh-2017-000694
46. Saha S, Beach MC, Cooper LA. Patient centeredness, cultural competence and healthcare quality. J Natl Med Assoc. 2008;100(11):1275–1285. doi:10.1016/S0027-9684(15)31505-4
47. Lee PM, Lee PM, Khong P, Ghista DN. Impact of deficient healthcare service quality. TQM Mag. 2006;18(6):563–571. doi:10.1108/09544780610707075
48. Burton MJ, Ramke J, Marques AP, et al. The lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5
49. Alhassan RK, Duku SO, Janssens W, et al. Comparison of perceived and technical healthcare quality in primary health facilities: implications for a sustainable national health insurance scheme in Ghana. PLoS One. 2015;10(10):e0140109. doi:10.1371/journal.pone.0140109
50. Schembri S. Experiencing health care service quality: through patients’ eyes. Aust Health Rev. 2015;39(1):109–116. doi:10.1071/AH14079
51. Hayes CW, Batalden PB, Goldmann D. A ‘work smarter, not harder’ approach to improving healthcare quality. BMJ Qual Saf. 2015;24(2):100–102. doi:10.1136/bmjqs-2014-003673
52. Batalden PB, Davidoff F. What is “quality improvement” and how can it transform healthcare? Qual Saf Health Care. 2007;16(1):2–3. doi:10.1136/qshc.2006.022046
53. Bradshaw A, Raphaelson S. Improving patient satisfaction with wait times. Nurs. 2021;51(4):67–69.
54. Greaves F, Ramirez-Cano D, Millett C, Darzi A, Donaldson L. Harnessing the cloud of patient experience: using social media to detect poor quality healthcare. BMJ Qual Saf. 2013;22:251–255. doi:10.1136/bmjqs-2012-001527
55. Rozenblum R, Bates DW. Patient-centred healthcare, social media and the internet: the perfect storm? BMJ Qual Saf. 2013;22(3):183–186. doi:10.1136/bmjqs-2012-001744
56. Jackson JL, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52:609–620. doi:10.1016/S0277-9536(00)00164-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.