Back to Journals » Patient Preference and Adherence » Volume 20
Patients’ Perspectives on the Role of General Practice-Based Pharmacists: A Focus Group Study
Authors Hazen A ![]() , Kempen T, Leendertse A, Bouvy M
, Kempen T, Leendertse A, Bouvy M ![]() , van Dijk L
, van Dijk L ![]() , Zwart D
, Zwart D
Received 4 September 2025
Accepted for publication 20 January 2026
Published 19 February 2026 Volume 2026:20 565194
DOI https://doi.org/10.2147/PPA.S565194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ramón Morillo-Verdugo
Ankie Hazen,1 Thomas Kempen,2,3 Anne Leendertse,4 Marcel Bouvy,2 Liset van Dijk,5 Dorien Zwart1
1Julius Center for Health Sciences and Primary Care, Department of General Practice & Nursing Science, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands; 2Division of Pharmacoepidemiology & Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Utrecht, the Netherlands; 3Department of Pharmacy, Uppsala University, Uppsala, Sweden; 4Patient Advocate, Egmond aan Zee, the Netherlands; 5Nivel, Netherlands Institute for Health Services Research, Utrecht, the Netherlands
Correspondence: Ankie Hazen, Email [email protected]
Background: An aging population, increasingly complex health conditions, and high workloads in primary care highlight the need for more efficient healthcare organisation. Integrating pharmacists into general practice can improve pharmacotherapeutic care and reduce hospital admissions. In the Netherlands, this collaborative model is being explored for broader implementation. Limited research has examined how patients perceive the role of pharmacists within general practice settings.
Aim: What are the perspectives of patients using chronic medications on the role of general practice-based pharmacists?.
Methods: A qualitative descriptive study using focus group interviews was conducted with patients from five health centers in the Netherlands. Between May and September 2024 five focus groups were held: two with patients who had experience with pharmacist services in general practice, three with inexperienced patients. The inclusion criterion was the use of at least one medication on a chronic basis; no exclusion criteria were applied. An independent patient representative moderated the session, using a semi-structured topic guide. Discussions were audio-recorded, transcribed, and analysed using inductive thematic analysis in NVivo 12.
Results: A total of 31 patients participated, with five to eight in each group. Patients recognised and trusted general practice-based pharmacists for their expertise in complex pharmacotherapy, clear role distinction from GPs and community pharmacists, and strong communication skills. Key enablers of trust included secure data handling, adequate funding, and accessibility. Pharmacists were valued for delivering personalised, proactive care, contributing to multidisciplinary networks, and reducing GP workload. It was also suggested that a pharmacist working across both community pharmacy and general practice may offer added value, though this hybrid role could potentially lead to fragmented care.
Conclusion: Overall, patients perceived the role of the general practice-based pharmacist as a valuable addition to primary care, particularly in the management of complex medication regimens. Trust in the pharmacist’s new role and clear delineation of responsibilities between health care professionals are crucial for success.
Keywords: primary health care, pharmacists, general practitioners, patient perspectives, medication
Introduction
Worldwide, there is an aging population. Older people have an increased risk of multimorbidity, which is often accompanied with polypharmacy, making care for this group increasingly complex.1 People with multimorbidity and polypharmacy are at higher risk of harm due to drug-therapy problems with adverse events and hospital admissions.2
The Medication without Harm’ initiative, launched in 2017 by the World Health Organisation, recommends clinical medication reviews by pharmacists as an important strategy to improve the quality of prescribing and to prevent drug-therapy problems.3 Another key point of the initiative is that the knowledge of physicians, nurses, pharmacists, and other healthcare professionals needs to be integrated to ensure effective polypharmacy management.
One way to achieve this is through a collaborative care model with general practice-based pharmacists as integral members of the primary care medical team. These pharmacists are a relatively recent addition to primary care teams in the Netherlands and in many other countries. General practice-based pharmacists typically support medication reviews, deprescribing initiatives, chronic disease management, and the resolution of medication-related problems in close collaboration with general practitioners (GPs).This model has demonstrated both effectiveness and cost-efficiency4,5 and is increasingly being adopted internationally.6,7 Integrated teamwork between GPs and pharmacists reduces medication-related hospital admissions and improves the quality of life for patients with chronic illnesses by minimising adverse effects, falls, and inappropriate prescribing.8,9 Additionally, it facilitates knowledge exchange, enhances interprofessional collaboration and job satisfaction, and contributes to cost savings.4,10
A recent qualitative meta-synthesis on patient perspectives by Hassan et al shows that patients generally value the contribution of general practice-based pharmacists, particularly for medication-related support, while also highlighting persistent challenges regarding role awareness and accessibility.11 However, the qualitative evidence is limited and geographically concentrated, mostly from the UK, with little insight into emerging roles of general practice-based pharmacists in other healthcare systems. Existing studies focus mainly on patients who have consulted a general practice-based pharmacist, leaving non-users, hesitant patients, and vulnerable populations—like older adults with multimorbidity and polypharmacy—largely unexplored. Patients’ perspectives on how general practice-based pharmacists impact continuity of care and the GP–patient relationship are also underexamined.
In many countries, the role of general practice-based pharmacists is still relatively new and not yet widely implemented. To inform further development and scaling of this role, it is essential to explore the patient perspective. What do patients with polypharmacy need from their pharmacist, how do they experience the shift from the traditional dispensing role to the pharmacist’s role as practitioner and how do they perceive the role of general practice-based pharmacists?
Understanding the patient perspective is crucial to ensure success and legitimacy of any role development. Patients are the ultimate beneficiaries of health service innovations and should therefore have a voice in shaping care models. Prior research has shown that patients with little to no experience with general practice-based pharmacists are often uncertain about the nature and scope of the pharmacist’s role. In contrast, patients with experience tend to value the care received.12–14 Gaining insight into patient’s preferences and concerns is essential to ensure that care models are patient-centered and responsive to public expectations. This knowledge can help to tailor communication, improve service design, and ultimately support more widespread and accepted integration of pharmacists in primary care.
In the Netherlands, a novel model of collaborative care is being introduced, in which a pharmacist is active in both community pharmacy and general practice. This so-called hybrid model has the potential to strengthen the connections between both settings, improve communication, enhance the visibility and accessibility of pharmacists for patients, and improve the quality of pharmaceutical care overall.
Despite a growing body of international literature, there remains a lack of in-depth research on how patients using chronic medications perceive the clinical services of general practice-based pharmacists, particularly in healthcare systems where this role is still emerging, and where pharmacists operate in hybrid practice models, such as in the Netherlands. To address this gap, the present qualitative study aims to explore the perspectives of both experienced and inexperienced patients on the evolving role of general practice-based pharmacists.
Method
Design and Setting
A qualitative descriptive study using focus group interviews was undertaken in five primary health care centers in the Netherlands. Structured focus groups were used to capture multiple perspectives and in-depth insights that might not come up in individual interviews. This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.15
In the Dutch primary care context, the concept of general practice-based pharmacists is not yet common. Fewer than 20 practices nationwide currently employ such pharmacists. However, the number has doubled in the past two years, with most of the newly appointed pharmacists working in hybrid roles, combining responsibilities in general practice with continued employment in community pharmacy.
Focus Groups
A total of five focus groups were conducted, one at each of five different health centers in a private on-site meeting room or staff lounge that were not accessible to others during the sessions. Two focus groups consisted of patients who had received care from a pharmacist with ten years of experience working within general practice (“experienced patients”), and three focus groups consisted of patients who were unfamiliar with this role (“inexperienced patients”). The focus groups were deliberately organised separately to ensure that experienced patients did not influence inexperienced patients, and vice versa. We aimed at including six to twelve patients in each focus group.16 A requirement was that patients used at least one medication on a chronic basis. Chronic medication use was defined as the regular use of a prescribed medication for at least three consecutive months for the treatment or prevention of a chronic disease. The professionals who invited the patients to take part, checked this before inviting them.
Patient Recruitment
Five practices were selected through purposive sampling within the professional network of the research group. Practices differed in size, population and location (2 village and 3 urban settings), and were all located in the central region of the Netherlands (Utrecht, de Bilt and Ermelo). Participant identification and recruitment were carried out within each practice. For focus groups 1 and 2, the general practice–based pharmacist identified potential participants; for focus groups 3–5, the practice nurse, GP, or community pharmacist did so based on their recent interactions with the service and their suitability for the study (ie the use of at least one chronic medication). The health care professionals purposefully selected patients they considered able and willing to discuss the study topics. Because the research team relied on these clinicians to identify suitable participants, the selection was influenced by the clinician’s familiarity with their patient population. Rather than aiming for statistical representativeness, the study aimed to obtain a diverse and information-rich sample, asking clinicians to invite patients with varying educational backgrounds and both positive and critical perspectives.
Individuals were approached either during or immediately after a scheduled consultation with the pharmacist, practice nurse, or GP, or were contacted directly by Email or telephone using practice-held records. Staff introduced the study, assessed interest, and obtained permission to share the patient’s contact details with the research team. The participating healthcare professionals at each centre continued approaching eligible patients until the maximum number of nine patients per focus group was reached. The total number of patients approached was not systematically recorded, nor were the reasons for non-participation. Once a patient agreed to be contacted, a member of the research team (AH) or a research student emailed the participant a study information sheet and a consent form. Participants were given time to review the study information, ask questions, and consider their participation.
All patients received the same information and were aware that they were contributing to the evaluation of the pharmacists’ professional role. After the participants were welcomed and had settled into the room, they were asked to complete a short questionnaire, taking no longer than 5 minutes to complete. The questionnaire collected a standard set of demographics (age, gender, education, employment, residence) and relevant health-related characteristics (number of GP and pharmacist consultations in the past 12 months), with items selected based on study objectives, team discussion, and prior literature.- (Appendix 1). All patients received a 30-euro gift card afterwards.
Topic List Development
A topic list (Appendix 2) was developed based on literature review12,14 and interviews with patients from a previous Dutch study about the perspectives of patients on prescribing authority for pharmacists in primary care.7 These interviews also included general practice-based pharmacists and addressed, in part, the collaboration between GPs and pharmacists. The list was discussed with an expert group including a patient representative and was revised accordingly. The following topics were covered in every group discussion: 1) healthcare needs of patients using chronic medications, 2) patients’ expectations of the general practice-based role for pharmacists, 3) perceived advantages and disadvantages of the collaborative model,4) exploration of the hybrid model where the pharmacist operates both in general practice and community pharmacy and 5) important preconditions for carrying out this role in general practice. The first focus group was used to test whether the topic guide was appropriate for the target audience. No significant changes were made after the first focus group.
Data Collection
The focus groups were carried out between May and September 2024 and were moderated by a male, patient representative and expert by experience (MW, see acknowledgements), with experience in facilitating group discussions. This patient representative, who was not part of the research team and had no established relationship with the participants of the focus groups, was deliberately selected to facilitate the focus group discussions. This decision was made to ensure that the questions were posed by someone who could relate well to the participants while maintaining a degree of objectivity, as the main researchers might have been more inclined to ask leading questions. The moderator had no specific personal or professional interest in the topic of the study and acted solely in his role as a patient representative and experienced group facilitator. The moderator was briefed in advance on the theme, aim and objectives of the study by the lead researcher (AH) and the patient representative in the research team (AL). A research student and senior researcher or local pharmacist who helped in the organisation of the meeting, were present to welcome the patients and briefly introduced the topic to the inexperienced patients. The research student was also responsible for time management, to observe and make any additional notes on non-verbal cues.
The focus group interviews were recorded using an audio recorder and transcribed verbatim by an AI-generated transcription service (Happy Scribe) and manually checked for inaccuracies and pseudonymised by one of the research students.
Data Analysis
We used a two-phase approach for data collection and content analysis. In the first phase, we conducted three focus groups (one with participants who had experience with a general practice-based pharmacist and two without such experience). Data from these initial focus groups were analysed immediately after collection. This allowed us to identify preliminary themes, assess the richness and diversity of the data, and evaluate whether additional perspectives were needed. Based on the first three focus groups, we proceeded with two additional focus groups in the second phase (one with participants who had experience with a general practice-based pharmacist and one without such experience). The purpose of these groups was to further explore emerging themes and to assess whether data saturation had been reached.
Transcripts were analysed using inductive thematic analysis. Transcripts were read repeatedly to ensure familiarisation with the data and were independently coded line-by-line by a research student and researcher (AH) using NVivo 12 software. The researchers (TK, AH) and students agreed upon a coding scheme through discussion. Codes were subsequently organised into subthemes and the subthemes synthesised into themes through further collaborative interpretative analysis with the multidisciplinary research team, including a patient representative. Codes and (sub)themes were compared between the experienced and inexperienced patients by manually contrasting them during research team meetings to identify similarities and differences in perspectives. Coding was an iterative process with continued reference to the source data. Although a visual coding tree is not provided, all coding decisions and theme development were documented in NVivo. No formal member checking was performed, because the study aimed to generate inductively derived themes across the full dataset rather than to validate individual accounts.17 However, participants received an interim summary of the study results in November 2024 and were invited to provide comments or suggestions. A patient representative (AL) with an academic background was an integral member of the research team and played an active role in the interpretation of the data.
Reflexivity
The research team consisted of senior researchers who were either (clinical) pharmacist (TK, MB, AH) or a GP (DZ), a patient representative (AL) and a sociologist, who was an honorary professor of Pharmacy Health Services, with a special focus on medication adherence, pharmaceutical patient care and communication (LvD). Two research students, (one enrolled in pharmacy and involved in Phase 1, and one enrolled in medicine and involved in Phase 2) participated in this study as part of their master’s thesis under supervision of two senior researchers (AH, TK). This multidisciplinary composition allowed us to critically reflect on our professional assumptions and disciplinary lenses during data collection and analysis. The involvement of a patient representative and a sociologist helped challenge profession-centric viewpoints, while analytic decisions were critically reviewed during team meetings and supervisory sessions.
Data Handling
After transcribing, the recordings were permanently deleted from the recorder. All data was anonymised and stored on a secured network drive, and only the lead researchers (AH and DZ) had access. Patient data was anonymised and not traceable to participating patients. Data will be stored for the statutory period of ten years after study closure.
Ethical Considerations and Safeguards
This study was approved by the Internal Review Board of the Julius Center for Health Services and primary care, University Medical Center Utrecht (24U-1416). Written informed consent was obtained from all patients prior to the focus groups. Informed consent included publication of anonymised responses and direct quotes.
Via a patient information leaflet, and prior to the start of the focus groups, participants were informed of recording, their right to withdraw at any time and ensuring confidentiality of personal and medical information. Focus group discussions were conducted in a safe and supportive environment, with facilitators attentive to participants’ comfort and understanding. The study was conducted in accordance with the “Code of Conduct for Health Research” and complies with the EU GDPR (General Data Protection Regulation) and the WGBO (Medical Treatment Contracts Act) and complies with the Declaration of Helsinki.
Results
Thirty-one patients participated in the five focus groups (Table 1) and all five planned focus groups were conducted as scheduled. Each focus group included five to eight patients. The mean age of the patients was 75 years, 52% were female, all had the Dutch nationality and educational backgrounds varied. The majority of patients (65%) reported polypharmacy (≥5 medications in use), with differences in number of consultations with either GP, general practice-based pharmacist or community pharmacist in the last 12 months. Each focus group interview lasted between 55 and 95 minutes.
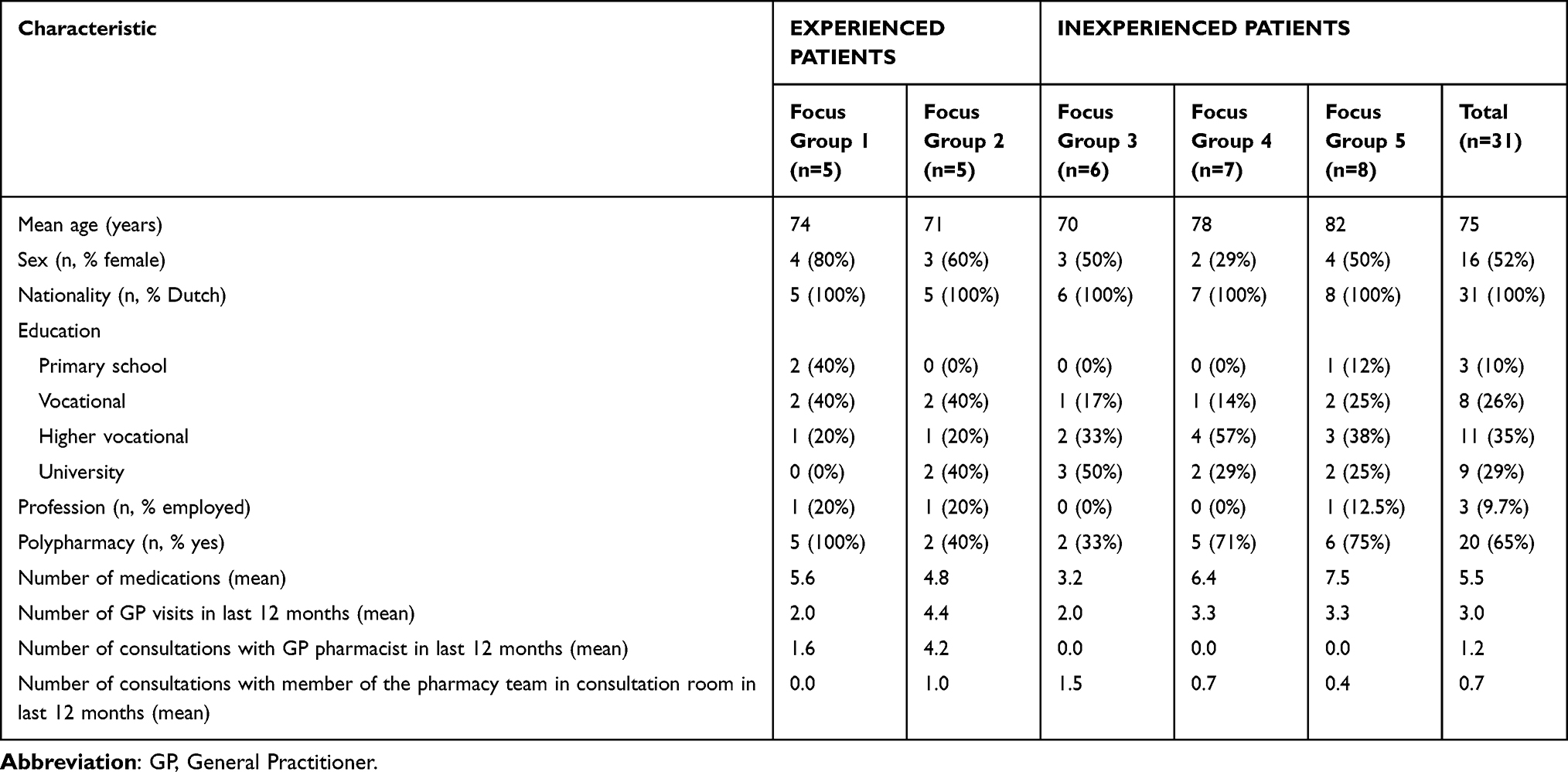 |
Table 1 Patient Characteristics |
Two main themes with various subthemes were derived from the data (Table 2). Where relevant, different perspectives between experienced and inexperienced patients are highlighted. Participant quotations were presented to illustrate the themes and findings, and each quotation is referenced using anonymised participant codes (P1, P2, etc).
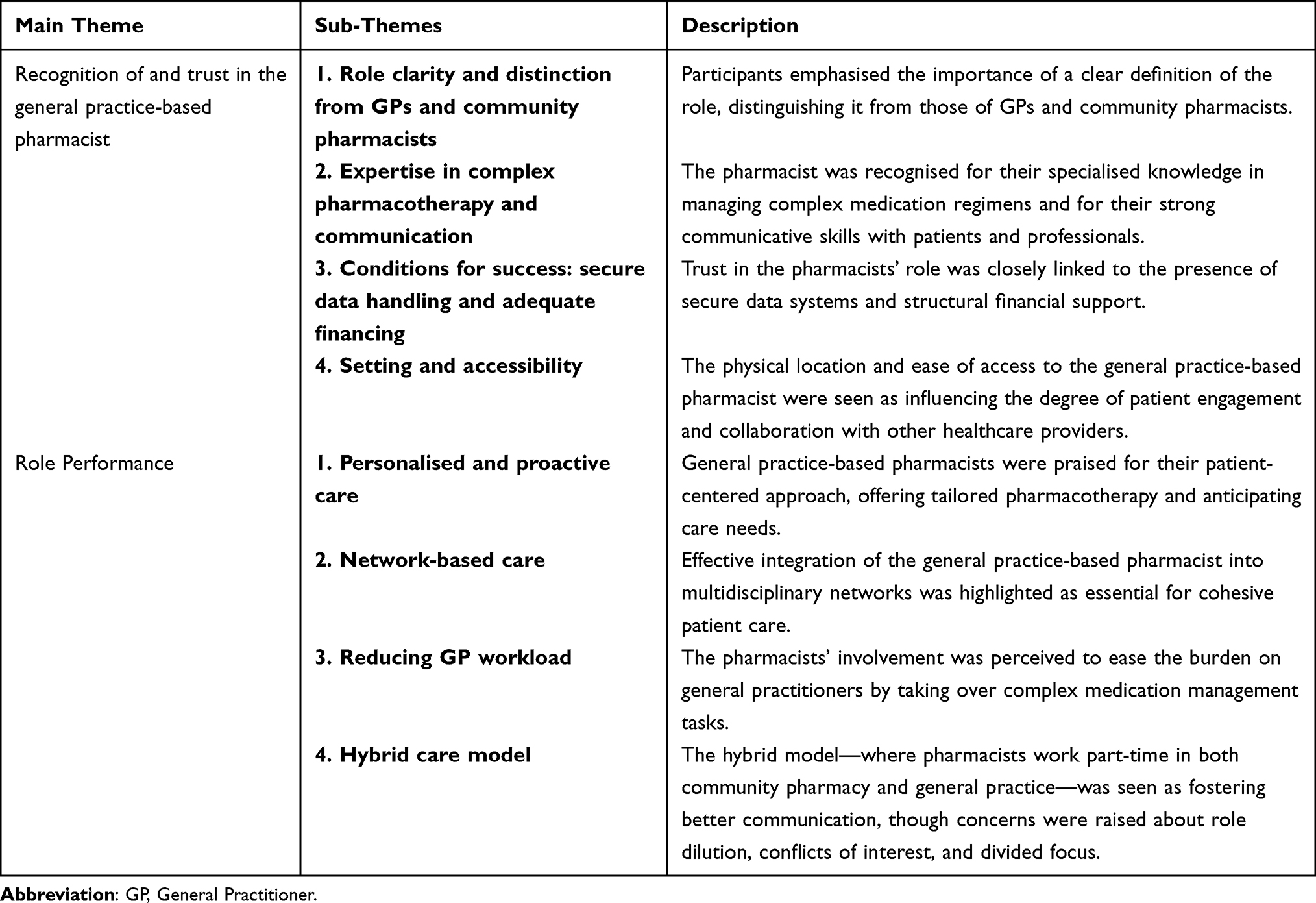 |
Table 2 Overview of Themes and Subthemes |
Recognition of and Trust in the General Practice-Based Pharmacist
The first overarching theme was the development of trust in and recognition of the general practice-based pharmacist. Patients’ willingness to engage with the general practice-based pharmacist, and their perception of its value, was shaped by the patient’s understanding of the role, the pharmacist’s expertise and communication skills, and the way the role was embedded within the GP practice. Four subthemes highlighted the interdependent factors shaping recognition and trust.
Role Clarity and Distinction with GP and Community Pharmacy
Patients’ first reactions to the general practice-based pharmacist’s role revealed a lack of awareness and confusion about its purpose, particularly in relation to the roles of GPs and community pharmacists. Many had grown accustomed to the GP as prescriber and the community pharmacist as dispenser. Moreover, most patients preferred consulting the GP rather than the community pharmacist for medication-related questions. Both experienced and inexperienced patients indicated that introducing a third professional can lead to initial hesitation.
“I always thought, the GP makes the decision about my medication and the pharmacist is the dispenser. […] But if I knew that this role existed then I would have asked for a consultation with the pharmacist”. [P7, focus group 4 – inexperienced patients]
Some inexperienced patients questioned the added value, worrying about the need to repeat their story and expressing doubts about building a new professional relationship, alongside the GP and community pharmacist. Familiarity and long-term relationships with their GP fostered more trust among some inexperienced patients, making them reluctant to engage with a pharmacist instead.
“So, I think the condition is that you understand what the role involves. That’s what I was missing in the beginning. I thought, do I have to explain everything to someone else again? Why?” [P1, focus group 2 – experienced patients]
“Because I, well, maybe it’s a bit old-fashioned, but you tend to trust the GP more, since they know you for a long time. And the GP has my complete medical history” [P5, focus group 5 – inexperienced patients]
Inexperienced patients expected a leading role from the GP in terms of deciding on whether the patient needs a medication evaluation by the general practice-based pharmacist. A referral by the GP often served as a legitimising mechanism, increasing patients’ willingness to consult the general practice-based pharmacist. Experienced patients increasingly consulted the general practice-based pharmacist, reducing the need to visit their GP, indicating a shift in trust.
“Normally, you go to the GP and they prescribe something. Then you go downstairs [to the community pharmacy] and get your medication. […] But at that point, you still don’t know what the effects will be. When I go to the general practice-based pharmacist, they really look into it, like: is this the right medication or could we maybe try something else that might work better or fit in better with the rest?” [P2, focus group 2 – experienced patients]
Most patients perceived community pharmacists as primarily focused on dispensing and safety checks. General practice-based pharmacists, on the other hand, were seen as having a supporting and caring role for the patient and their pharmacotherapy, offering comprehensive pharmacotherapy support, and providing structural follow-up. Some patients acknowledged that the general practice-based pharmacist could function as a bridge between the GP and community pharmacy and expressed strong support for expanding this role in close collaboration with GPs.
“ I would really like it if this could be implemented in the future.” [P4, focus group 1, experienced patients]
“I can only say that this is a very positive development, a general practice-based pharmacist who can support and collaborate with the GP.” [P4, focus group 3, inexperienced patients]
Expertise in Complex Pharmacotherapy and Communication
Most experienced patients using long-term medications appreciated the pharmacist’s potential to optimise their treatment. Inexperienced patients were more divided—some found their GP sufficient, while others acknowledged the general practice-based pharmacist’s potential value for complex medication regimens. Some experienced and inexperienced patients emphasised that not every patient requires this level of attention. The patients’ evaluation of the added value of the general practice-based pharmacist was clearest in complex or vulnerable patients, offering reassurance during uncertain treatment phases.
“I personally don’t need it, but my disabled son who has been very poorly and needed a lot of medication before, I would have appreciated more contact with the pharmacist. […] Because we were insecure. [P5, focus group 5 – inexperienced patients] “
“There must also be a necessity to involve such a person [general practice-based pharmacist]. It shouldn’t be taken for granted [that every person who used medication will be seen by the general practice-based pharmacist]. There isn’t enough time to do that anyway. It should provide added value in specific cases.” [P1, focus group 3 – inexperienced patients]
Some participants expressed frustration that such expertise had not been available sooner in their care trajectory.
“My husband, who I believe had ten or more medications, never had any contact with a pharmacist about it. Never. In hindsight, I think there were probably many medications that weren’t working well together, and perhaps he would have lived longer if there had been better oversight.” [P3, focus group 5 – inexperienced patients]
For some experienced patients, the general practice-based pharmacist filled a gap in knowledge and support that their GP could not provide, particularly in complicated cases. A patient with treatment resistant hypertension mentioned:
“I went to the GP, but she said “I really don’t know what to do anymore”. I am going to send you to our general practice-based pharmacist, and that is how I got here. And it is fantastic, it really is.” [P4, focus group 1 – experienced patients]
Good communication was repeatedly mentioned as a prerequisite for trust. General practice-based pharmacists who listened actively, provided clear explanations, and showed compassion helped reduce patients’ uncertainty and increased their confidence in the role. Given the patient-facing nature of the role, both experienced and inexperienced patients assumed that general practice-based pharmacists possess strong communication skills, or would at least have received additional training.
“Yes, different communication skills are needed in the consultation room.” [P6, focus group 4 – inexperienced patients]
Several experienced and inexperienced patients viewed the general practice-based pharmacist as an important professional in primary care, not just as a complement to the GP, but as someone with authority and autonomy in pharmacotherapeutic care.
“It is needed that the pharmacist, if I may put it bluntly, does not become merely a distributor of medicines, but actually applies their expertise to authorise treatments, guide patients, advise GPs and specialists, and provide proper support to patients.” [P4, focus group 3 – inexperienced patients]
Conditions; Secure Data Handling and Adequate Financing
Patients’ trust in the general practice-based pharmacist was closely tied to issues of data access and financial structure. Experienced patients generally accepted that pharmacists accessed their medical records, assuming secure data handling. They appreciated that the general practice-based pharmacist and GP have the same information and adjust it if necessary. On the other hand, some inexperienced patients felt uncomfortable with the idea that the pharmacist had access to their full medical journal and expressed reluctance to share highly personal information with pharmacists:
“For example, nightmares or other personal things, I feel comfortable discussing them with the GP, but I don’t think the pharmacist needs to know about that.” [P9, focus group 5 – inexperienced patients]
The majority of inexperienced patients emphasised a distinction between general health information and more intimate or psychological issues, suggesting that pharmacists’ access should be limited or patient-controlled.
“I wouldn’t want the community pharmacist to have full access to my medical record. […] I want some sort of control about where my information is” [P8, focus group 5 – inexperienced patients]
Trust in the pharmacists’ role was also influenced by how the service was financed. Some experienced patients indicated a willingness to contribute financially to consultations, reflecting a perceived added value. The majority of patients opposed any fees, as they had not chosen to consult the pharmacist. Furthermore, several patients argued that since the general practice-based pharmacist takes over part of the GP’s responsibilities, it would be logical for the service to be included under the same insurance coverage. As such, consensus—across both experienced and inexperienced patients—was that consultations with general practice-based pharmacists should be covered by basic health insurance. This was seen as critical to ensuring equal access and reinforcing the legitimacy of the role.
“I think it should be in the basic package. It should be available to everyone, even for people who can’t afford supplemental insurance. I think that’s very important.” [P6, focus group 4 – inexperienced patients]
Setting and Accessibility
The physical and organisational embedding of the pharmacist within the general practice was a key facilitator of trust and recognition. The majority of patients emphasised the difference between the quick, transactional nature of the pharmacy counter and the more personal setting of the GP practice. The latter offered more attention, privacy, and time — factors that made patients feel seen, heard and supported— particularly when dealing with complex medication issues.
“I think the community pharmacist is far too busy. I think a general practice-based pharmacist would have more time, because he is doing a face to face consultation.” [P1, focus group 5 – inexperienced patients]
In contrast to brief exchanges at the pharmacy counter, the majority of experienced and inexperienced patients valued the opportunity for seated conversations in a calm setting—something they associated more with the GP environment.
“When you receive a medication for the first time at the pharmacy, the pharmacy technician provides some education, in addition to the side effects or the leaflet, and they also charge a fee for that. So I say, let the general practice-based pharmacist provide that explanation as well. I think the GP setting is calmer, because you’re not standing at a counter, but rather sitting and having a conversation.” [P7, focus group 5 – inexperienced patients]
Some acknowledged that consultations could—and ideally should—be conducted in both settings, depending on what is most accessible or appropriate for the situation. However, many had not previously experienced a medication consultation in the community pharmacy and felt that the interaction there was often limited to pharmacy technicians, with many patients not knowing their pharmacist.
“Yes, I would say do it [medication consultations] everywhere [both in pharmacy and general practice] because it is really needed. You never talk to the community pharmacist, always the technician.” [P 9, focus group 5 – inexperienced patients]
Additionally, patients noted that having the pharmacist physically present in the general practice allowed for shorter lines of communication with the GP, facilitating better coordination of care.
“Maybe they [GP + general practice-based pharmacist] can also provide joint consultations to evaluate my medication”. [P5, focus group 4 – inexperienced patients]
Role Performance of the General Practice-Based Pharmacist
The second overarching team referred to the role performance of the general practice-based pharmacist. Patients described the general practice-based pharmacist as fulfilling a multifaceted role within primary care. The patients’ input revealed four aspects that together define how the role is experienced and valued: personalised and proactive engagement, network-based care, relieving GP workload, and the emerging hybrid model.
Personalised and Pro-Active Care
A key element of the general practice-based pharmacist’s role, according to patients, is the combination of a personalised and proactive approach to pharmacotherapeutic care. Most experienced patients valued time and focus given to tailoring medication regimens to their specific health situation. General practice-based pharmacists were seen not just as advisors, but as active partners in optimising pharmacotherapy. Among experienced patients there was appreciation for how the pharmacist initiated, tapered or discontinued medication, while ensuring regular follow-up to monitor effects.
“You have symptoms and they might be caused by the fact that you’ve been taking that medication for so long. Then the general practice-based pharmacist says: shall we try changing it once and see how it goes?” [P7, focus group 1 – experienced patients]
The personalised approach and one-on-one consultations created a sense of being genuinely cared for, rather than being managed in a standardised way. Some patients emphasised the value of the general practice-based pharmacist’s proactive attitude to invite patients based on proactive risk screening, for example patients using potentially harmful medication. Some experienced patients reported that these pharmacists took the initiative to reach out, schedule consultations, and conduct medication reviews.
“They introduced themself by saying: I am indeed affiliated with the general practice, and I would like to schedule an appointment with you to review all your medications and check if everything fits well together, if something can be discontinued, and if there are any other questions.” [P2, focus group 1 – experienced patients]
This proactive engagement extended beyond the initial consultation. The majority of experienced patients appreciated that the general practice-based pharmacist followed up regularly, to check on their well-being, inquire about side effects and the effect of treatment changes, and carries out further checks, like blood pressure monitoring. Most inexperienced patients also believed that the general practice-based pharmacist should proactively invite patients for consultations and provide monitoring and follow-up.
“And there’s another difference, I think. At the pharmacy downstairs, I get answers to my questions. But the general practice-based pharmacist does it the other way around too. They also call me to ask: How are you doing? How are the side effects? Are you coming in again for your blood pressure” [P5, focus group 2 – experienced patients]
“Yes, they [the general practice-based pharmacist] do the follow-up, I think that’s fantastic” [P2, Focus group 1 – experienced patients]
Another aspect that was mentioned by a group of inexperienced patients was the proactive involvement of general practice-based pharmacists in managing repeat prescriptions to intercept overprescribing. These patients expressed hope that the general practice-based pharmacists can help reduce unnecessary medications, and offer more tailored support, for example where repeat prescriptions are issued without thorough review—something they felt was rarely addressed in GP-led care.
“There is no GP in the Netherlands who monitors that, so those repeats just keep being continued, over and over. That’s exactly why it’s great to have a general practice-based pharmacist, who can keep an eye on that and slow down the constant repeat prescriptions” [P5, focus group 3 – inexperienced patients] Network-based care
Network-based Care
Both experienced and inexperienced patients recognised that general practice-based pharmacists play a role in coordinating care by collaborating with GPs, nurse practitioners, specialists, and other healthcare professionals. Collaboration and the need for seamless referrals from specialists and hospital consultants was seen as crucial, especially for patients managing multiple medications. Experienced patients appreciated that while general practice-based pharmacists may not always make independent decisions, they proactively consult specialists when needed. Co-location within the general practice facilitates communication and continuity of care:
“I think […] the lines of communication are much shorter. They are team members, and they probably consult much more than the community pharmacist and GP do.” [P6, focus group 2 – experienced patients]
A few inexperienced patients expressed a wish for better integration of pharmacists into specialist-led care trajectories as well. There was awareness that hospital specialists may not consider referring to the general practice-based pharmacist, which patients felt could be a missed opportunity.
“The GP can refer to the general practice-based pharmacist next door, but can a specialist do that as well? Is he equipped to do that, will he think of referring to the pharmacist? That should be considered, how you can make that possible in the future” [P9, focus group 5 – inexperienced patients]
In complex cases, patients valued that the general practice-based pharmacist took responsibility for gathering input from multiple professionals and synthesising this into a coherent treatment plan. Some patients noted that certain cases require input from multiple disciplines, and appreciated that the general practice-based pharmacist ensured seamless communication between professionals and relayed consolidated information to the patient, which contributed significantly to their sense of being supported and understood.
“If necessary, they [the general practice-based pharmacist] will call the cardiologist. […] She [the GPP] can’t decide that on her own, but she can after consultation. And that makes a difference, because it means I don’t have to go to the hospital” [P7, focus group 1 – experienced patients]
“And what they did, which really helped, was that they said: well, I’m still concerned about it. I’ll consult with the GP and the gynecologist. And then I said: could you please also involve the menopause consultant? And they did. […] They provided a very clear update and the outcome was something I was really satisfied with, so I felt incredibly taken seriously. They played an important role in bringing all the information together and I was very happy with that. [P1, focus group 2 – experienced patients]
Relieving the GP’s Workload
Both experienced and inexperienced patients mentioned that the general practice-based pharmacist takes on certain responsibilities traditionally handled by the GP, such as medication reviews, follow-up, and detailed medication counseling. Experienced patients highly appreciated this, believing it significantly reduces the GP’s workload.
“I would recommend it to every practice. It’s a relief for the GP and an added benefit for the patients. And we also assume it eases the workload for the pharmacy because they don’t have to handle everything. So, it’s like hitting three birds with one stone.” [P2, focus group 1 – experienced patients]
Additionally, a group of inexperienced patients indicated that, in cases of medication-related problems, the general practice-based pharmacist and specialist can confer and formulate a well-considered recommendation, with the GP largely uninvolved except for being informed of the outcome. This shift in tasks and responsibilities was compared to the growing role of advanced nurse practitioners, with patients recognising similar efficiencies and role differentiation.
However, some inexperienced patients pointed out the potential for overlap, questioning whether the conversations with a general practice-based pharmacist added enough beyond what the GP already provides.
“I think: what a huge overlap with the conversation I just had with the GP. Because they also ask: how are you doing? [.] How are the side effects and is the medication use going well? […] But since the pharmacist is probably better at it, it makes sense for that task to lie with the pharmacist” [P9, focus group 5 – inexperienced patients]
Hybrid Model
Patients across the five focus groups expressed a range of perspectives on the hybrid model, in which pharmacists divide their time between community pharmacy and general practice. Many patients appreciated the potential for improved continuity of care, better communication between sectors, and more comprehensive pharmaceutical expertise. They felt that a pharmacist operating in both settings would be better positioned to anticipate issues such as medication shortages or brand substitution and to offer timely, personalised advice. The model was also seen as fostering shorter lines of communication between healthcare professionals and increasing the pharmacist’s awareness of both clinical and logistical aspects of pharmacotherapy.
“Maybe it’s even better because it keeps that connection to the pharmacy itself.” [P2, focus group 1 – experienced patients]
At the same time, several patients in both the experienced and inexperienced focus groups voiced concerns about the feasibility and clarity of the role. Some patients worried that splitting roles might lead to time constraints, a dilution of expertise, or limited availability in either setting. This split focus could result in not being able to fully dedicate to one role and develop the necessary skills for both community pharmacy and general practice-based work.
“If you’re working half in the pharmacy and half in the general practice, you end up with a more generalist role. You know a bit about everything, but you can’t go in-depth in either area.” [P1, focus group 2 – experienced patients]
There were also reflections on a potential conflict of interest when a pharmacist is involved in both advising and dispensing. Patients clearly distinguished between the transactional nature of community pharmacy work and the more supportive, patient-centred role of the general practice-based pharmacist. Working in both settings could blur professional boundaries or create a tension between care and commerce, questioning whether a pharmacist could remain fully independent in their clinical role:
“In the morning, you try to sell as many medications as possible, and in the afternoon, you try to reduce them. That hybrid thing, it’s tricky.” [P5, focus group 2 – experienced patients]
“The strength of a GP is that they have no commercial interest. If the pharmacist is tied to both, that could be a problem.” [P8, focus group 5 – inexperienced patients]
Thus, the hybrid role was seen as potentially valuable, but only if the pharmacist remained sufficiently embedded, independent, and able to maintain up-to-date expertise across both domains.
Discussion
Key Findings
This study identified two overarching themes when discussing with patients about the evolving role of the general practice-based pharmacist: trust in and recognition of the general practice-based pharmacist’s role, and their role performance in practice. Most patients appreciated the added value of having a pharmacist embedded within the general practice, particularly for patients with complex medication needs. Both experienced and inexperienced patients valued the personal approach, in-depth consultations, network-based and pro-active care, and strengthened collaboration with GPs. Both groups acknowledged the potential for general practice-based pharmacists to support GPs through medication reviews, coordinate with other healthcare professionals, and provide follow-up in complex pharmacotherapy. Key differences between the experienced and unexperienced patients centered on awareness, confidence, and perceived added value: experienced patients reported greater understanding, trust, and willingness to shift medication-related care to general practice-based pharmacists, whereas inexperienced patients initially expressed uncertainty, reliance on the GP, and hesitation about privacy or role overlap. Once informed about the pharmacist’s role, many inexperienced participants recognised potential benefits. The hybrid model was perceived as promising, though somewhat fragmented and patients generally supported broader implementation of the general practice-based role, provided it remains accessible through basic health insurance.
Comparison with Existing Literature
A key theme that emerged from the current study is the importance of interprofessional collaboration between GP and general practice-based pharmacist. This collaboration is closely tied to the development of trust in and recognition of the pharmacist’s role, as well as the perceived value of their contributions to patient care. Corbaz‑Kurth’s framework on trust in interprofessional collaboration conceptualises trust as an intangible resource that emerges through relationships, individuals, organisation and education.18 In line with this framework, patients in our study recognised the pharmacist’s expertise and appreciated their contributions when they observed effective communication and integration within the general practice setting, reflecting relational determinants of trust. Individual determinants, such as ability, confidence, integrity, and responsibility, are key factors in building interprofessional trust. When general practice-based pharmacists demonstrate these qualities in practice, they not only strengthen trust among professional colleagues but also reinforce patients’ confidence in the pharmacist’s expertise. Organisational factors, such as visible role integration, secure data systems and structural financial support, helped patients see the general practice-based pharmacist as a credible member of the care team, while educational initiatives can further support understanding of interprofessional roles.
The importance of interprofessional collaboration also aligns with the findings of Reeves et al (2016), who argue that collaboration between healthcare professionals improves patient care by enhancing communication, reducing errors, and providing more accessible services.19 In our study, the ability of the general practice-based pharmacist to actively communicate with the GP and integrate their input into GP-based care contributed to how patients recognised and appreciated the pharmacist’s role. Patient awareness and appreciation are critical enablers of role effectiveness: when patients view the pharmacist as a credible and integral source of GP-based care, they are more likely to engage proactively, follow up on medication-related advice, and seek support for complex therapeutic issues.20 A lack of recognition may lead to underutilisation of the pharmacist’s expertise, diminished trust, and confusion about their function within the healthcare team. Our findings show that inexperienced patients were often uncertain about the general practice-based pharmacist’s expertise and responsibilities, which is understandable given that trust and appreciation build through direct experience. This highlights the importance of engagement, effective communication, and repeated positive encounters about medication-related matters to ensure that the new pharmacists’ role is optimally utilised.21
Focussing on the second main theme, role performance, our study highlights that patients perceive the general practice-based pharmacist as a clinician who takes an active, responsible role in managing their medication, a role that extends beyond the dispensing duties typically associated with community pharmacists. This aligns with Kellar ‘s scoping review, which found that while pharmacists often embody multiple professional identities, including dispenser, patient counsellor, and physician supporter, the clinician identity is one that many pharmacists aspire to adopt but do not uniformly enact in practice.22 Hazen’s work on professional identity formation suggests that pharmacists transitioning into general practice can experience a transformative shift toward this clinician identity, which – consistent with our findings - may enhance both their role performance and patient recognition.23
This clinical role, as perceived by patients in our study, also aligns with research suggesting that general practice-based pharmacists can act as critical partners in managing complex health issues.24 Patients especially appreciate the longer consultations and attention offered by the general practice-based pharmacist, as these provide an opportunity for more in-depth discussions about their personal health and medication. Patients reported that they felt more seen, heard, and understood, and more confident in the management of their conditions. Mann et al (2022) similarly found that patients value longer interactions with pharmacists, feeling that this more personalised care allows for better management of their conditions, medication adherence and greater satisfaction.14
In comparison with the meta-synthesis by Hassan et al (2025) about patients’ views on the role of general practice-based pharmacists, our study underscores similar themes regarding patients’ perceptions of general practice-based pharmacists.11 Both studies highlight the importance of patients’ awareness of the role and their clinical responsibilities, which is often limited. However, our findings extend this by emphasising the trust patients place in general practice-based pharmacists, especially in patients with complex pharmacotherapy questions. While Hassan et al also note challenges related to accessibility and medication review processes, our study suggests that the hybrid model - where pharmacists work in both community pharmacy and general practice - has potential to overcome some of these barriers. This model is increasingly being implemented in the Netherlands and offers potential, as it may foster closer collaboration and improved continuity of care. On the other hand, views on the hybrid model were mixed and several patients expressed concerns about divided attention, limited specialisation, and potential conflicts of interest. These concerns highlight the importance of clear role definition and robust support structures to avoid fragmentation and to ensure that pharmacists can work effectively across both settings.
Our study also reveals some skepticism, particularly among inexperienced patients who already have strong relationships with their GPs. These patients sometimes question the necessity of involving a pharmacist in their care, echoing the findings of Hurley et al (2018), who found that many patients consider their GP as the primary healthcare provider and may not immediately recognise the added value of the pharmacist.25 This – again - underscores the importance of well-defined roles and clinical responsibilities and of promoting trust in pharmacist’ expertise by demonstrating complementary -rather than overlapping - competencies with GPs, and ensuring that patients experience concrete benefits from pharmacist-led interventions Patients’ experiences with general practice-based pharmacists align closely with the views of other key stakeholders, such as GPs and pharmacists. Like patients in our study, GPs generally value general practice-based pharmacists as partners in medication management, patient safety, and practice efficiency, particularly through roles such as structured medication reviews that support rather than replace the GP. At the same time, PGs reported concerns on role boundaries, workload, funding, and training mirroring patients’ uncertainties about role clarity and fragmentation of care.26–29 Across stakeholder groups, clear role delineation, strong collaboration, adequate funding, and sufficient clinical training were identified as key facilitators for successful integration.30 Overall, these perspectives reinforce the relevance of our patient findings and highlight the importance of addressing organisational and relational conditions when implementing general practice-based pharmacist roles.
Additionally, concerns related to privacy and the management of personal medical information were raised by several inexperienced patients mirroring the issues highlighted by Rasiah et al (2022).31 These concerns should be understood not only as individual perceptions, but as a sociotechnical issue arising from the interaction between digital technologies, human behavior, organisational structures, and regulatory frameworks. In healthcare, and particularly in pharmaceutical care, shared access to patient records between GPs and pharmacists is essential for safe medication management in older patients with complex therapies, yet it also introduces vulnerabilities such as risks of unauthorized access, data breaches, and unequal control over personal health information. Patients expressed discomfort with the idea of pharmacists having access to their complete medical records, stressing the need for transparency regarding who can access data, for what purpose and under which safeguards. In other words, the benefits of integrated digital records are balanced against risks related to privacy, data security, and accountability. Importantly, this concern appeared to diminish among experienced patients, who tended to express greater trust in the pharmacist’s professionalism and saw access to medical records as beneficial for integrated care. For these patients, access to shared records was increasingly viewed as a prerequisite for effective interprofessional collaboration rather than a threat to privacy. Similar findings, albeit about prescribing pharmacists, were reported by Jebara et al (2018), who showed that patients’ initial concerns about liability decreased once they experienced the practice in real-life settings.32
Strengths and Limitations
One of the strengths of this study is its focus on an emerging model of care, providing timely data on patient perspectives in the early stages of implementation in the Netherlands. The use of focus groups allowed for rich, qualitative data collection, giving participants the opportunity to express their views in a group dynamic, facilitating in-depth understanding of patient perspectives. The study included a wide age range of participants amongst both experienced and inexperienced patients, providing a unique perspective on the new role of the general practice-based pharmacist from varying levels of familiarity.
This study has several limitations. First, only five focus groups were conducted, which may limit the diversity of perspectives captured, particularly across different practice settings or cultural backgrounds. On the other hand, the range of three to five focus groups is well documented in literature33–35 and it was considered unlikely that additional groups would provide new information. Second, the five focus groups varied in size, although a minimum number of 5 participants was ensured, which may have influenced group dynamics and the depth of discussions. Third, participant selection was influenced by clinicians’ judgment. As the research team relied on the clinicians to identify and approach suitable participants, the selection process was inevitably shaped by the clinicians’ familiarity with their patient population, which may have introduced selection bias. Fourth, although rigorous qualitative methods were applied, data analysis is inherently interpretative and may be influenced by researchers’ perspectives. Measures such as independent coding and multidisciplinary consensus discussions were employed to enhance trustworthiness, but subjective interpretation cannot be fully eliminated. Finally, while the inclusion of centres varying in size, patient population, and location enhanced the diversity of perspectives, the transferability of findings may still be limited. Patients’ and professionals’ views on general practice-based pharmacists may differ in other regions, healthcare systems, or cultural contexts.
Practical Implications and Future Research
The findings underscore several implications for practice, policy, and future research.
- Role clarification and GP endorsement: Clear and consistent communication about the general practice-based pharmacist’s responsibilities, competencies, and access to medical records – actively endorsed by GPs - is essential to build patient trust and engagement, particularly among patients unfamiliar with the role.
- Support for hybrid models: The implementation of hybrid pharmacist roles within both general practice and community pharmacy requires structured organisational support to ensure continuity of care and prevent divided attention, especially during early implementation phases where GP involvement helps legitimise pharmacists’ consultations.
- Patient engagement strategies: Repeated positive interactions, personalised consultations, and proactive engagement in clinical medication review and shared decision-making can strengthen therapeutic relationships and enhanced patient confidence and engagement.36
- Privacy and transparency: Robust protocols governing access to electronic medical records, combined with clear explanations for patients are critical to addressing privacy concerns and reinforcing trust in the general practice-based pharmacist’s role.
- Policy and future research: Reimbursement of general practice-based pharmacists’ services through basic insurance schemes is crucial to promote equitable access and legitimise the role. Future research should explore how different organisational models influence the uptake of the interprofessional care model with a general practice-based pharmacist. Research should also focus on high-risk or underserved patient groups, as well as individuals who decline or never access pharmacist services, to better understand barriers to uptake, misconceptions, and trust-related concerns regarding skill mix with GPs.
Conclusion
This study provides important insights into patients’ perspectives on the evolving role of the general practice-based pharmacist, highlighting trust and role performance as central themes shaping patient experiences. Across both experienced and inexperienced patients, embedding a pharmacist within general practice was widely perceived as adding value, particularly for individuals with complex medication needs, through a personalised, proactive approach, in-depth consultations, and strengthened collaboration with GPs. While initial awareness and confidence varied, experience with the role was associated with greater trust, clearer role recognition, and a willingness to shift certain medication-related care from the GP to the pharmacist. In this context, the general practice-based pharmacist is perceived as a clinician who takes accountability for complex medication-related issues in primary medical care and contributes to coordinated, network-based care. The hybrid model holds promise but must be carefully structured to preserve professional depth, trust and continuity.
Successful implementation of general practice-based pharmacists requires clear role definition, GP endorsement, and structured organisational support. Robust protocols for data access and transparent communication are essential to maintain patient trust, while personalised engagement strategies can strengthen patient confidence. Policy measures, including reimbursement through standard insurance schemes, are needed to legitimise the role, and future research should examine how organisational models and patient characteristics influence uptake, particularly among high-risk or underserved populations.
Acknowledgments
The authors would like to thank Menno Wagenaar, patient representative, for his valuable contribution as moderator of the focus groups. We are also grateful to the five participating health care centers for their collaboration and support in conducting this study.
Funding
A research grant was obtained from the Netherlands Organisation for Health Research and Development (Grant Agreement Number 10140292110007). The study sponsor had no role in the design of the study, nor in the data collection, analyses, interpretation of the data and in the writing of the report or in the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aggarwal P, Woolford SJ, Patel HP. Multi-morbidity and polypharmacy in older people: challenges and opportunities for clinical practice. Geriatrics. 2020;5(4):85. doi:10.3390/geriatrics5040085
2. Davies LE, Spiers G, Kingston A, Todd A, Adamson J, Hanratty B. Adverse outcomes of polypharmacy in older people: systematic review of reviews. J Am Med Dir Assoc. 2020;21(2):181–17. doi:10.1016/j.jamda.2019.10.022
3. Organization GWH. Medication without harm - global patient safety challenge on medication safety. 2017.
4. O’Mahony C, Dalton K, O’Hagan L, et al. Economic cost-benefit analysis of person-centred medicines reviews by general practice pharmacists. Int J Clin Pharm. 2024;46(4):957–965. doi:10.1007/s11096-024-01732-y
5. Sloeserwij VM. The Non-Dispensing Pharmacist in Primary Care: An Interprofessional Model to Improve Pharmaceutical Care and Patient Safety. Utrecht University; 2020.
6. Karampatakis GD, Patel N, Stretch G, Ryan K. Integration and impact of pharmacists in general practice internationally: a rapid review. J Health Serv Res Policy. 2024;29(1):56–67. doi:10.1177/13558196231179831
7. Kempen TGH, Benaissa Y, Molema H, et al. Pharmacists’ current and potential prescribing roles in primary care in the Netherlands: a case study. J. Interprof. Care. 2024;38(5):787–798. doi:10.1080/13561820.2024.2374017
8. Hazen A, Sloeserwij V, Pouls B, et al. Clinical pharmacists in Dutch general practice: an integrated care model to provide optimal pharmaceutical care. Int J Clin Pharm. 2021;43(5):1155–1162. doi:10.1007/s11096-021-01304-4
9. Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. J Multidiscip Healthc. 2021;14:1701–1710. doi:10.2147/JMDH.S309938
10. Hayhoe B, Cespedes JA, Foley K, Majeed A, Ruzangi J, Greenfield G. Impact of integrating pharmacists into primary care teams on health systems indicators: a systematic review. Br J Gen Pract. 2019;69(687):e665–e74. doi:10.3399/bjgp19X705461
11. Hassan AHF, Barry HE, Hughes CM. Perspectives of patients on the role of general practice pharmacists: a systematic review and meta-synthesis of qualitative studies. BMC Prim Care. 2025;26(1):90. doi:10.1186/s12875-025-02787-0
12. Karampatakis GD, Patel N, Stretch G, Ryan K. Patients’ experiences of pharmacists in general practice: an exploratory qualitative study. BMC Family Practice. 2021;22(1):48. doi:10.1186/s12875-021-01393-0
13. Als JG, Thomsen JL, Sørensen SS, Johnsen SP, Merrild CH. ‘You would rather not fill your body with pills’-patient perspectives on polypharmacy and medication reviews by pharmacists in general practice. Scand J Prim Health Care. 2025;43(2):411–421. doi:10.1080/02813432.2025.2451660
14. Mann C, Anderson C, Boyd M, Karsan Y, Emerson T. Perspectives of pharmacists in general practice from qualitative focus groups with patients during a pilot study. BJGP Open. 2022;6(2):
15. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
16. Cleary M, Horsfall J, Hayter M. Data collection and sampling in qualitative research: does size matter? J Adv Nurs. 2014;70(3):473–475. doi:10.1111/jan.12163
17. Varpio L, Ajjawi R, Monrouxe LV, BC O, Rees CE. Shedding the cobra effect: problematising thematic emergence, triangulation, saturation and member checking. Med Educ. 2017;51(1):40–50. doi:10.1111/medu.13124
18. Corbaz-Kurth S, Weissbrodt R, Juvet TM, et al. How does trust emerge in interprofessional collaboration? A qualitative study of the significance, importance, and dynamics of trust in healthcare teams and networks. J Interprof Care;2025. 1–10. doi:10.1080/13561820.2025.2495013
19. Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6(6):CD000072. doi:10.1002/14651858.CD000072.pub3
20. Mann C, Anderson C, Boyd M. The role of clinical pharmacists in general practice in England: impact, perspectives, barriers and facilitators. Res Social Adm Pharm. 2022;18(8):3432–3437. doi:10.1016/j.sapharm.2021.10.006
21. Te Paske R, van Dijk L, Yilmaz S, et al. Factors associated with patient trust in the pharmacy team: findings from a mixed method study involving patients with asthma & COPD. Patient Prefer Adherence. 2023;17:3391–3401. doi:10.2147/PPA.S429969
22. Kellar J, Singh L, Bradley-Ridout G, et al. How pharmacists perceive their professional identity: a scoping review and discursive analysis. Int J Pharm Pract. 2021;29(4):299–307. doi:10.1093/ijpp/riab020
23. Hazen ACM, de Groot E, de Bont AA, et al. Learning through boundary crossing: professional identity formation of pharmacists transitioning to general practice in the Netherlands. Acad Med. 2018;93(10):1531–1538. doi:10.1097/ACM.0000000000002180
24. Rushworth GF, Forsyth P, Radley A, et al. A pharmacist clinician model as part of a collaborative clinical workforce: a philosophical critique. Res Social Adm Pharm. 2024;20(9):918–925. doi:10.1016/j.sapharm.2024.06.006
25. Hurley E, Gleeson LL, Byrne S, Walsh E, Foley T, Dalton K. General practitioners’ views of pharmacist services in general practice: a qualitative evidence synthesis. Family Practice. 2021;39(4):735–746. doi:10.1093/fampra/cmab114
26. Care KSNP. Clinical pharmacists in primary Care: evidence of impact. Available from: https://yhtraininghubs.co.uk/wp-content/uploads/2024/01/Clinical-Pharmacists-Evidence-of-impact.pdf.2024.
27. Hasan Ibrahim AS, Barry HE, Hughes CM. General practitioners’ experiences with, views of, and attitudes towards, general practice-based pharmacists: a cross-sectional survey. BMC Prim Care. 2022;23(1):6. doi:10.1186/s12875-021-01607-5
28. Hurley E, Foley T, Walsh E, Byrne S, Dalton K. GPs’ perceptions of pharmacists working in general practices: a mixed methods survey study. Eur J Gen Pract. 2023;29(1):2273841. doi:10.1080/13814788.2023.2273841
29. Hurley E, Walsh E, Foley T, Heinrich CH, Byrne S, Dalton K. General practitioners’ perceptions of pharmacists working in general practice: a qualitative interview study. Fam Pract. 2023;40(2):377–386. doi:10.1093/fampra/cmac115
30. Freeman C, Cottrell WN, Kyle G, Williams I, Nissen L. Integrating a pharmacist into the general practice environment: opinions of pharmacist’s, general practitioner’s, health care consumer’s, and practice manager’s. BMC Health Serv Res. 2012;12(1):229. doi:10.1186/1472-6963-12-229
31. Rasiah S, Jaafar S, Yusof S, Ponnudurai G, Chung KPY, Amirthalingam SD. A study of the nature and level of trust between patients and healthcare providers, its dimensions and determinants: a scoping review protocol. BMJ Open. 2020;10(1):e028061. doi:10.1136/bmjopen-2018-028061
32. Jebara T, Cunningham S, MacLure K, Awaisu A, Pallivalapila A, Stewart D. Stakeholders’ views and experiences of pharmacist prescribing: a systematic review. Br J Clin Pharmacol. 2018;84(9):1883–1905. doi:10.1111/bcp.13624
33. Twohig PL, Putnam W. Group interviews in primary care research: advancing the state of the art or ritualized research? Family Practice. 2002;19(3):278–284. doi:10.1093/fampra/19.3.278
34. Barbour RS. Making sense of focus groups. Med Educ. 2005;39(7):742–750. doi:10.1111/j.1365-2929.2005.02200.x
35. Hennink MM, Kaiser BN, Weber MB. What influences saturation? estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
36. Te Paske R. Building Bridges for Trust: Strengthening Patient-Centred Communication in Pharmacy for Optimal Inhaler Use in Asthma and COPD Patients. University of Groningen; 2025.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.