Back to Journals » Clinical Ophthalmology » Volume 19
Patients’ Perspectives on Social Barriers to Care and the Acceptability and Impact of a Community Health Worker Program in Outpatient Ophthalmology
Authors Rustam Z ![]() , Amezcua Moreno J, Tran D, Ferguson K, Woods R, Cai CX
, Amezcua Moreno J, Tran D, Ferguson K, Woods R, Cai CX
Received 20 May 2025
Accepted for publication 30 July 2025
Published 8 August 2025 Volume 2025:19 Pages 2647—2657
DOI https://doi.org/10.2147/OPTH.S541632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zainab Rustam,1 Jose Amezcua Moreno,1 Diep Tran,1 Kenya Ferguson,2 Randi Woods,2 Cindy X Cai1,3
1Wilmer Eye Institute, Johns Hopkins School of Medicine, Baltimore, MD, USA; 2Sisters Together and Reaching, Inc, Baltimore, MD, USA; 3Department of Biomedical Informatics and Data Science, Johns Hopkins School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Cindy X Cai, Wilmer Eye Institute, 1800 Orleans Street, Room 711, Baltimore, MD, 21287, USA, Tel +1 410 502-2789, Email [email protected]
Introduction: Community Health Workers (CHWs) are trusted members of the community who can work as an integral liaison between community members and health care to address adverse social determinants of health (SDoH). The purpose of this semi-qualitative study was 1) solicit patient-reported social needs and what they consider barriers to their ophthalmic care, 2) determine the acceptability of discussing SDoH in eye care, and 3) determine the acceptability of leveraging a CHW to address social needs.
Methods: A total of 50 adults with type 2 diabetes at the Wilmer Eye Institute participated in semi-structured interviews. The interview included questions on barriers to care, acceptance of SDoH discussion in eye clinics, ideas to address SDoH and acceptability of CHWs. The transcripts were analyzed using traditional text analysis based on classic grounded theory to identify themes.
Results: Patients reported transportation (66%), scheduling conflicts (50%), forgetting appointments (50%) and other illnesses (40%) as barriers to attending eye appointments. Motivators included knowing the importance of maintaining regular eye appointments (22%), desire to maintain eyesight (22%) and health (10%). 88% felt positive about addressing SDoH in the eye clinic but were apprehensive about the front desk (14%) asking the questions citing lack of privacy. Some preferred doctors (20%) or specialized staff (14%) to ask the questions. 82% felt no topics should be off limits, understanding that questions aimed to help them. Ideas to address SDoH in eyecare included improving communication (44%), increasing resource access (36%) and introducing social workers (32%). 16% were aware of existing social services for eyecare. After explaining the role of CHWs, (90%) were enthusiastic about incorporating CHW in eyecare.
Conclusion: These findings support the assessment of SDoH in ophthalmology clinics and the integration of CHWs to address social needs from the patients’ perspectives.
Keywords: diabetic retinopathy, social determinants of health, barriers to care, social needs
Introduction
Diabetic retinopathy, or the ophthalmic manifestation of diabetes, continues to be a major cause of vision loss.1 Regular and repeat ophthalmic examinations are critical for identifying vision threatening complications and initiating therapy to prevent vision loss. Lack of ophthalmic screening, lapses in diabetic retinopathy care, and the underutilization of eye care services remain potential modifiable risk factors in reducing vision loss from diabetic retinopathy.2–5
There is an increasing awareness that social determinants of health (SDoH) impact health outcomes.6 SDoH are the conditions in which people are born, live, work, and play that affect a wide range of health and health outcomes.7,8 In the context of diabetic retinopathy care, adverse SDoH (eg, not having a primary care physician, having housing difficulties) are associated with the underutilization of eye care services, increased lapses in care, and poor vision outcomes.9–12 However, there remains a gap between identifying the social risk factors that negatively impact diabetic retinopathy outcomes and patient acceptable interventions to address those social needs. Critically, social risk factors are the adverse social conditions or individual-level SDoH associated with poor health while social needs reflect what patients have identified and prioritized for social intervention.13,14
Evaluation of SDoH is not currently a routine part of the eyecare visit nor is there widely deployed evidence-based interventions to address social needs. The patient acceptability of evaluating and assessing social risk factors at the point of ophthalmic care is unknown.15 Some authors suggest that patients dealing with adverse SDoH may be reluctant to share those barriers with specialists and doctors they do not have a relationship with.15,16 Although there are no widely deployed interventions, there is evidence that community health workers (CHWs) can be effective strategies to address social needs and improve the health of communities.17 CHWs are trusted members of the community in which they serve and have extensive knowledge about community resources, and can work as an integral liaison between community members and health care.18 CHWs are under-utilized strategies in the eye care community in the US and have been primarily leveraged in low-resource countries such as India, Nepal and Sierra Leone.19–21 The acceptability of patients to working with CHWs deployed in the ophthalmic clinic is currently unknown. The purpose of this prospective semi-qualitative study at a single academic medical center located in an urban environment was to: 1) solicit patient reported social needs and what they consider barriers to their ophthalmic care, 2) determine the acceptability of discussing SDoH in the context of eye care, and 3) the acceptability of leveraging a CHW to address social needs.
Methods
Participants and Procedure
Adult patients over 18 years of age with type 2 diabetes mellitus (T2D) seen in the Patient Access Center for the Eye (PACE) from 1/1/2024 to 7/1/2024 at the Wilmer Eye Institute at Johns Hopkins Hospital were screened for eligibility. Patients were excluded if they did not speak English or were unable to provide informed consent. Patients were given a $20 gift card for their participation. Participants underwent a semi-structured interview conducted by a single research coordinator (JAM) consisting of questions about the topics of: barriers/motivators to eye care, acceptability of being asked social determinants of health questions, and acceptability of potentially working with a community health worker (Supplemental Figure 1). A series of open-ended questions followed by specific prompts were created based on the World Health Organization SDoH framework, Healthy People 2030 and prior literature demonstrating the link between lower eye care use and poor housing conditions, lack of primary care provider, financial insecurity, and transportation difficulties.8,22 Other questions emerged from the dialogue between the interviewer and interviewee(s). Data collection was performed until thematic saturation occurred. Interviews ranged from 5 to 48 minutes (average 18 minutes). The study was approved by the Johns Hopkins Institutional Review Board (IRB00399279) and followed the Declaration of Helsinki.
Data Analysis
The interview was audio recorded and transcribed using Microsoft Word (Version 2108). Qualitative data analysis was conducted by two members (J.A.M. and Z.R.) using traditional text analysis based on classic grounded theory.23 This method involves isolating themes from the transcripts, highlighting texts that relate to the theme and sorting them into categories. To maintain consistency, members met regularly to clarify, discuss and merge codes. Frequently applied codes were extracted to identify the main themes from each interview and data was stored in Excel.
Additional patient sociodemographic information was extracted from the electronic health record (EHR) including age, sex, self-reported race/ethnicity, and insurance. Ocular characteristics including severity of diabetic retinopathy were extracted from the EHR from all prior office visits using codes as previously described.11 The census block group of the patients’ residential addresses were also extracted from the Johns Hopkins Precision Medicine Analytics Platform and matched to the 2021 Area Deprivation Index.24
Results
A total of 50 participants were included in the study. (Table 1) Most participants were female (66%), ≥50 years (70%) with mean age of 57 years, Black (72%), and non-Hispanic (94%) (Table 1).
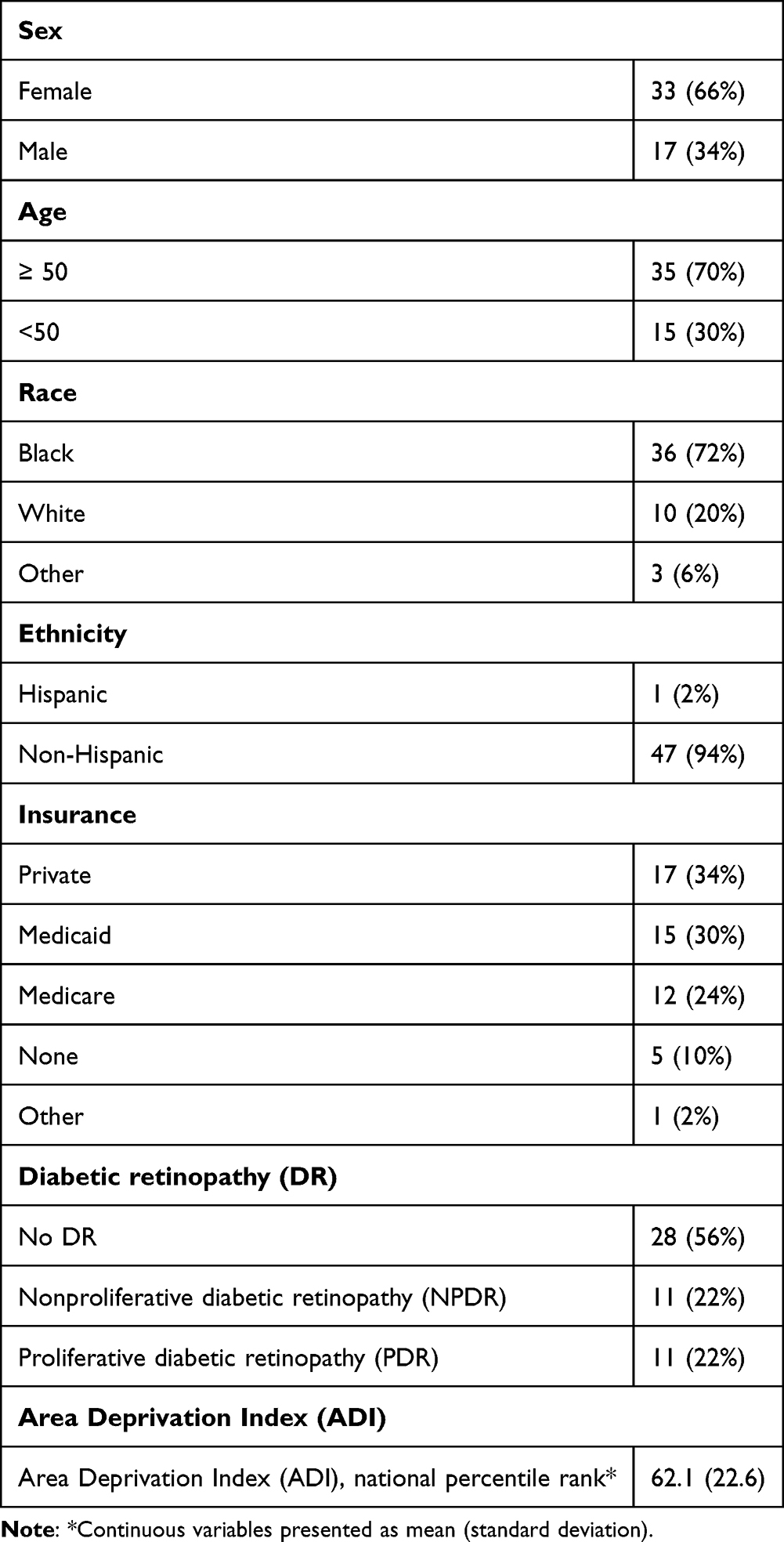 |
Table 1 Baseline Demographic Characteristics of Patients with Diabetes Included in the Study |
The themes that emerged from each of the 3 interviewed topics are summarized below.
Topic 1: Barriers to/Motivators of Eye Care
Participants were asked about barriers to eye care. (Table 2) The most commonly reported barrier (N = 33, 66%) was transportation. For example, participants cited how challenging it was to find parking, miss the bus, or arrange a ride to the eye care appointment, expressed in these quotes:
…I think the parking should be better for the patients. It’s difficult to park. You’re in the parking lot for an hour trying to find. [parking].
…it’s so intimidating finding out where you’ve got to be to this place. It’s not clear…where you’re supposed to park and…if you are coming from a more rural area and…tend to have a bigger vehicle, you get stuck in the parking garage.
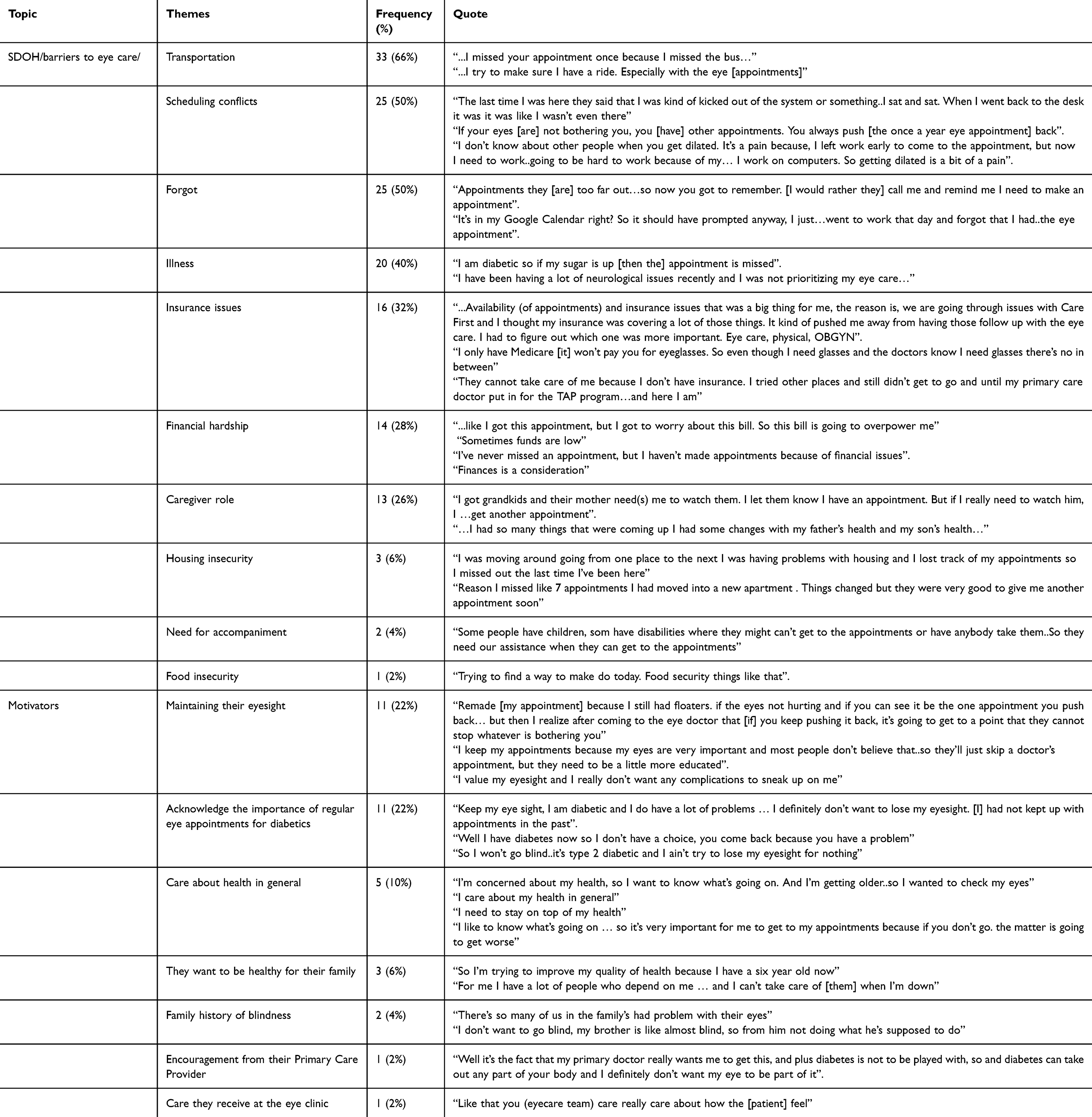 |
Table 2 Participants Self-Reported Barriers to Care and Motivators to Attend Appointments |
Other top challenges included scheduling conflicts (N = 25, 50%); for example, when patients had to miss work for the appointment or when the provider canceled an appointment at the last minute, as explained by a participant: “My follow up had been scheduled and I came up and was ready for it…And when I got here they told me that the doctor had decided to reschedule it”. Sometimes, patients forget about their eye appointments because it was often scheduled far in advance (N = 25, 50%). Many patients with diabetes also managed other medical issues and illnesses (N = 20, 40%) that resulted in missed appointments. Insurance issues (N = 16, 32%) or financial hardship (N = 14, 28%) were other commonly cited barriers. Having caregiver responsibilities (N = 13, 26%) as stated by a participant, “I was dealing with my husband who had alcoholism. I was a caretaker for my mother, so I couldn’t take care of myself” resulting in patients not being able to step away for appointments, was another barrier. Lastly, having housing insecurity (N = 3, 6%), need for accompaniment (N = 2, 4%), and food insecurity (N = 1, 2%) were also cited as barriers to eye care. The following quotes demonstrate some of the barriers:
Right now I’m going through housing problem. I’m going to like Section 8, trying to waiting for the house to come through. I’ll deal with that [then] I’ll see my medical problems.
Like I’m not seeing very well right now. If you don’t have a caregiver of sorts to accompany you, that could possibly be an issue
Participants also shared what motivates them to keep their regular eye appointments. (Table 2) Many participants cited the importance of regular eye appointments for patients with diabetes (N = 11, 22%) and expressed a desire to maintain their eyesight (N =11, 22%) and health (N = 5, 10%). Some credited their primary care provider for providing counseling and encouragement (N = 1, 2%) or the excellent care they received at the eye clinic (N =1, 2%) as reasons they return. Others wanted to stay healthy for their family (N =3, 6%) and feared going blind (N = 2, 4%). These themes were captured by the following quotes:
[It is] very important that I get the injections for my eye to keep the swelling and the bleeding down, so I came in on my own accord and made this last appointment for today
I know the importance of it being a diabetic you have to keep an eye out for retinopathy and stuff like that
…I want to live better, for my husband, for my children … and to myself too
Topic 2: Acceptance of Discussing SDoH in a Clinical Setting
The majority of patients felt positively about discussing SDoH at their eye appointment (N = 44, 88%). (Supplemental Table 1) Some felt strongly SDoH topics should be brought up by the doctor (N = 10, 20%), or other staff on the team such as the technician (N = 12, 24%). Some felt that it should not be the front desk staff (N = 7, 14%) due to lack of privacy, but most did not have a preference (N = 26, 52%). In terms of the timing of these questions, many participants preferred for it to take place after the appointment (N = 25, 50%). Some preferred being asked before (N = 15, 30%) or during (N = 10, 20%) the appointment, so the provider can tailor patient care and make decisions based on patients’ social conditions. Most preferred to answer these questions one-on-one verbally (N = 28, 56%). The majority of patients (N = 41, 82%) felt no topics should be off limits because they know the questions are being asked to help them and they trust the healthcare team. However, some felt that questions about abuse (N = 1, 2%), relationships (N = 2, 4%) and sexual activities (N = 1, 2%) should not be asked since they are unrelated to eye care (N = 1, 2%).
Topic 3: Ideas to Address SDoH and Acceptability of Community Health Workers
Participants were asked to give their opinions on how they think barriers to eye care should be addressed. (Supplemental Table 2) Most (N = 22, 44%) felt improving communication between the eye care team and patients would be helpful. Other ideas included maintaining excellent care (N = 20, 40%), increasing access to resources (N = 18, 36%), introducing social workers (N = 16, 32%), providing free transportation (N = 14, 28%), and assisting patients with technology (N = 6, 12%).
Participants were asked to share their current knowledge of social programs to address barriers to care. (Supplemental Table 2) Most of them had no information (N = 18, 36%), some had limited to moderate (N = 26, 52%), and very few (N = 5, 10%) had extensive knowledge. Programs that patients identified addressed transportation needs, housing and food insecurities. Only 8 patients (16%) were aware of free services provided by Wilmer Eye Institute, which includes the Free Diabetes Screening clinic.25
The role of CHWs was explained to the participants. We described how CHWs could help with scheduling clinic appointments, connections to community resources and providing social support. Participants were enthusiastic about the idea of incorporating a CHW in an ophthalmology clinic (N = 45, 90%). (Table 3) Opinions on potential tasks of the CHW such as home visits, taking patients and involvement in acquiring resources were mixed. Some participants (N = 24, 48%) were in favor of home visits but 15 (30%) felt they were too intrusive or were in favor of it in certain situations. Their opinion on CHW taking patients to resources also varied. Some were in favor (N = 11, 22%), but a few felt that independence should be encouraged, and patients should approach resources themselves (N = 10, 20%).
 |
Table 3 Participants Opinion on the Acceptability of CHW in a Clinical Setting |
Discussion
This prospective semi-qualitative study of patients with T2D seeking eye care at an academic facility in Baltimore City identified several social needs patients felt were barriers to seeking eye care, for example, transportation difficulties, scheduling conflicts, forgetfulness, and dealing with other illnesses. Overall, the majority of patients saw the value of and were receptive to being asked about social risk factors at their eye appointment. Most patients did not know about existing community resources. Lastly, the vast majority of patients were enthusiastic about the idea of working with a CHW to get them connected to social resources.
Differences in patient identified social needs and published social risk factors highlight the need for direct patient engagement in efforts to address adverse SDoH.26 For example, while financial insecurity is strongly associated with lapses in care and lower eye care utilization, only a small proportion of patients recognize it as a barrier to accessing their eye care.12,27 A barrier commonly reported by patients but not typically asked for in national surveys, is scheduling conflicts initiated by the provider.28 For example, 50% of patients reported scheduling conflicts, but on further discussion, many of these were last minute cancellations initiated by the provider’s office.
Assessment of SDoH are now a routine component of primary care visits but have not yet become commonplace in specialty clinics. Studies indicate patients are open to discussing SDoH but their willingness depends on their rapport with the provider, clarity on how the social factors impact care, and availability of resources to address the barriers.29 Many reported they would like their doctor or clinic to ask these questions and had concerns with housing (22%), transportation (27%) and food (22%).30,31 In our cohort, 88% responded positively to the idea of SDoH discussion during clinic visits. Some patients preferred that either the doctor or specialized staff such as social workers ask such questions but others did not have a preference. One study reported a favorable SDoH screening experience when conducted by physician assistants but not with nurse practitioners; highlighting the importance of personnel selection when approaching sensitive discussions with patients.32 However, an important stakeholder perspective not evaluated in our study was the provider perspective. A study assessing provider perspective on SDoH collection found that the majority of providers believe social needs play a role in health quality and outcomes. Specialists believed that PCPs should be responsible for collecting and addressing these needs through a dedicated team and health system.33,34 A study at Mayo Clinic discovered higher completion rate of SDoH screening during primary care visits compared to specialty care visits, this may suggest a difference in priorities, training, awareness and time constraints between these healthcare settings.35 Future interventions should incorporate the perspectives of the clinical team in addition to the patients.
Pilot programs introducing CHWs to a population have received positive feedback from participants, demonstrating high acceptability and satisfaction with CHW initiatives. These programs have improved participants’ medical knowledge enabling them to better understand their health conditions and treatment options.36 Additionally, CHWs played a role in improving access to social resources, fostering skill development and promoting self-efficacy.37 Their cultural familiarity and close ties to the community allows them to offer emotional support and build stronger connections with patients.38,39
Patients have reported a great appreciation for the trusted relationship they have developed with their CHW, the range of teaching material tailored to diverse populations, and noted positive behavioral changes as a result of these interventions.40,41 With disease-specific training, CHWs are equipped to measure blood pressure, assess vision, and navigate test results.42 Participants in CHW based interventions have experienced improvement in health outcomes such as decrease in blood pressure and HbA1c levels, indicating adherence to treatment regimens and recommended behavioral interventions.38,43 These experiences and interventions advocate for expansion of CHW programs across different specialties to enhance patient support, health care accessibility and wellbeing.18
The role of community health workers has not been extensively explored in ophthalmology. In the United States, the Manhattan Vision Screening program utilized community health workers to improve eye disease detection and specialist referral in vulnerable populations. The program resulted in high adherence to appointments and early pathology detection in 84.8% of the participants.44 Similarly, the Philadelphia Glaucoma Detection and Treatment Project was another initiative which implemented community based intervention to improve glaucoma management.45 Internationally, CHWs have been primarily used to increase referral to eye care providers for urgent conditions=.19,20,46,47 These programs focus on integration of CHWs to provide eye care services in community centers to enhance eye disease detection, management, and referrals.19,20,46,47 However, these programs did not address social barriers to care such as transportation, housing and financial insecurity which can impact access to ophthalmic care.
There are several limitations to this study. Since this was a semi-qualitative study at a single academic institution, we do not know the generalizability of our findings to other institutions. Participants were adults with diabetes who consented to this interview might not be representative of the perspectives of all patients being seen at our clinics. Future interventions will need to continually assess patient acceptance and have to continue to actively engage the communities they are seeking to help.48
Conclusion
This study explores the barriers to care that patients face in ophthalmology clinics, their awareness of community health care workers and acceptability of CHWs in ophthalmic care. Our findings support SDoH questioning during patient assessment and integration of CHW in ophthalmology clinics to, for example, enhance patient education, accessibility and appointment adherence.
Ethics Approval
This research project was approved by Johns Hopkins Institutional Review Board (IRB00399279). All participants provided written informed consent to participate and gave approval for quotations from their transcripts to be published. Data collected have been stored safely in an IRB approved secure folder.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
CXC: K23 award from the NIH/NEI (award number K23EY033440), unrestricted grant from Research to Prevent Blindness (Wilmer Eye Institute), Dr. Cai is the Jonathan and Marcia Javitt Rising Professor of Ophthalmology.
Disclosure
CXC: grants from Regeneron Pharmaceuticals Inc, equipment from Optomed USA Inc, personal fees from Boehringer Ingelheim and 4D Molecular Therapeutics, Inc. (outside of the submitted work). The authors report no other conflicts of interest in this work.
References
1. Curran K, Peto T, Jonas JB; Vision Loss Expert Group of the Global Burden of Disease Study, GBD 2019 Blindness and Vision Impairment Collaborators. Global estimates on the number of people blind or visually impaired by diabetic retinopathy: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2047–2057. doi:10.1038/s41433-024-03101-5
2. Lee PP, Feldman ZW, Ostermann J, Brown DS, Sloan FA. Longitudinal rates of annual eye examinations of persons with diabetes and chronic eye diseases. Ophthalmology. 2003;110(10):1952–1959. doi:10.1016/S0161-6420(03)00817-0
3. Schoenfeld ER, Greene JM, Wu SY, Leske MC. Patterns of adherence to diabetes vision care guidelines: baseline findings from the diabetic retinopathy awareness program. Ophthalmology. 2001;108(3):563–571. doi:10.1016/S0161-6420(00)00600-X
4. Chou CF, Barker LE, Crews JE, et al. Disparities in eye care utilization among the United States adults with visual impairment: findings from the behavioral risk factor surveillance system 2006-2009. Am J Ophthalmol. 2012;154(6 Suppl):S45–S52.e1. doi:10.1016/j.ajo.2011.09.025
5. Cai CX, Tran D, Tang T, et al. Health disparities in lapses in diabetic retinopathy care. Ophthalmol Sci. 2023;3(3):100295. doi:10.1016/j.xops.2023.100295
6. Krause TM, Schaefer C, Highfield L. The association of social determinants of health with health outcomes. Am J Manag Care. 2021;27(3):e89–e96.
7. Social determinants of health. Available from: https://odphp.health.gov/healthypeople/priority-areas/social-determinants-health.
8. A conceptual framework for action on the social determinants of health. 2010. Available from: https://www.who.int/publications/i/item/9789241500852.
9. Schein Y, Wang Z, Tran D, Crews DC, Zeger SL, Cai CX. Racial and ethnic disparities in receipt of retinal imaging among patients with diabetes. JAMA Ophthalmol. 2024;142(11):1091. doi:10.1001/jamaophthalmol.2024.4120
10. Xie WY, Rustam Z, Tran D, et al. Association of neighborhood socioeconomic disadvantage with proliferative diabetic retinopathy. Ophthalmol Retina. 2025;9(2):98–104. doi:10.1016/j.oret.2024.10.012
11. Tang T, Tran D, Han D, Zeger SL, Crews DC, Cai CX. Place, race, and lapses in diabetic retinopathy care. JAMA Ophthalmol. 2024;142(6):581. doi:10.1001/jamaophthalmol.2024.0974
12. Taccheri C, Jordan J, Tran D, et al. The impact of social determinants of health on eye care utilization in a national sample of people with diabetes. Ophthalmology. 2023;130(10):1037–1045. doi:10.1016/j.ophtha.2023.06.007
13. Alderwick H, Gottlieb LM. Meanings and misunderstandings: a social determinants of health lexicon for health care systems. Milbank Q. 2019;97(2):407–419. doi:10.1111/1468-0009.12390
14. Green K, Zook M. When talking about social determinants, precision matters. Forefront Group. 2019. doi:10.1377/forefront.20191025.776011
15. American Academy of Ophthalmology. Ophthalmology’s challenge: tackling social determinants of health. 2022. Available from: https://www.aao.org/eyenet/article/tackling-social-determinants-of-health.
16. DesRoches CM, Wachenheim D, Garcia A, et al. Clinician and patient perspectives on the exchange of sensitive social determinants of health information. JAMA Network Open. 2024;7(10):e2444376. doi:10.1001/jamanetworkopen.2024.44376
17. Knowles M, Crowley AP, Vasan A, Kangovi S. Community health worker integration with and effectiveness in health care and public health in the United States. Annu Rev Public Health. 2023;44(1):363–381. doi:10.1146/annurev-publhealth-071521-031648
18. Chang W, Oo M, Rojas A, Damian AJ. Patients’ perspectives on the feasibility, acceptability, and impact of a community health worker program: a qualitative study. Health Equity. 2021;5(1):160–168. doi:10.1089/heq.2020.0159
19. Srinivasan M, Ravilla T, Vijayakumar V, et al. Community health workers for prevention of corneal ulcers in South India: a cluster-randomized trial. Am J Ophthalmol. 2022;237:259–266. doi:10.1016/j.ajo.2021.12.010
20. O’Brien KS, Byanju R, Kandel RP, et al. Village-integrated eye workers for prevention of corneal ulcers in Nepal (VIEW study): a cluster-randomised controlled trial. Lancet Glob Health. 2022;10(4):e501–e509. doi:10.1016/S2214-109X(21)00596-9
21. Pente V, Bechange S, Jolley E, et al. Task-shifting eye care to ophthalmic community health officers (OCHO) in Sierra Leone: a qualitative study. J Glob Health. 2021;11(07001):07001. doi:10.7189/jogh.11.07001
22. Social determinants of health. Available from: https://odphp.health.gov/healthypeople/priority-areas/social-determinants-health.
23. Birks M, Mills J. Grounded Theory: A Practical Guide.
24. Kind AJH, Buckingham WR. Making neighborhood-disadvantage metrics accessible - the neighborhood atlas. N Engl J Med. 2018;378(26):2456–2458. doi:10.1056/NEJMp1802313
25. Nguyen PL, Amezcua Moreno J, Tran D, et al. Baseline characteristics and clinical outcomes of patients seen through the free diabetes screening (FDS) program. Clin Ophthalmol. 2024;18:3227–3236. doi:10.2147/OPTH.S483004
26. Nwanyanwu KH, Grossetta Nardini HK, Shaughness G, Nunez-Smith M, Newman-Casey PA. Systematic review of community-engaged research in ophthalmology. Expert Rev Ophthalmol. 2017;12(3):233–241. doi:10.1080/17469899.2017.1311787
27. Cai CX, Han D, Tran D, Moreno JA, Zeger SL, Crews DC. Social risk groups in patients with diabetes with differing eye care utilization and vision outcomes. Transl Vis Sci Technol. 2024;13(3):13. doi:10.1167/tvst.13.3.13
28. Chou CF, Sherrod CE, Zhang X, et al. Barriers to eye care among people aged 40 years and older with diagnosed diabetes, 2006-2010. Diabetes Care. 2014;37(1):180–188. doi:10.2337/dc13-1507
29. Kiles TM, Cernasev A, Leibold C, Hohmeier K. Patient perspectives of discussing social determinants of health with community pharmacists. J Am Pharm Assoc. 2022;62(3):826–833. doi:10.1016/j.japh.2022.01.007
30. Udezi V, Dixon J, Bonilla L. Clinician and patient perceptions of social determinants of health screening. Soc Determinants Vulnerable Populations. 2023. doi:10.1370/afm.22.s1.5667
31. Leary JC, Rijhwani L, Bettez NM, et al. Parent perspectives on screening for social needs during pediatric hospitalizations. Hosp Pediatr. 2022;12(8):681–690. doi:10.1542/hpeds.2021-006411
32. Rudisill AC, Eicken MGA, Gupta D, et al. Patient and care team perspectives on social determinants of health screening in primary care: a qualitative study. JAMA Network Open. 2023;6(11):e2345444. doi:10.1001/jamanetworkopen.2023.45444
33. Palacio A, Seo D, Medina H, Singh V, Suarez M, Tamariz L. Provider perspectives on the collection of social determinants of health. Popul Health Manag. 2018;21(6):501–508. doi:10.1089/pop.2017.0166
34. Schickedanz A, Hamity C, Rogers A, Sharp AL, Jackson A. Clinician experiences and attitudes regarding screening for social determinants of health in a large integrated health system. Med Care. 2019;57 Suppl 6 Suppl 2(Suppl 2):S197–S201. doi:10.1097/MLR.0000000000001051
35. Savitz ST, Nyman MA, Kaduk A, Loftus C, Phelan S, Barry BA. Association of patient and system-level factors with social determinants of health screening. Med Care. 2022;60(9):700–708. doi:10.1097/MLR.0000000000001754
36. Shepherd-Banigan M, Hohl SD, Vaughan C, Ibarra G, Carosso E, Thompson B. “the promotora explained everything”: participant experiences during a household-level diabetes education program. Diabetes Educ. 2014;40(4):507–515. doi:10.1177/0145721714531338
37. Bouchonville MF, Hager BW, Kirk JB, Qualls CR, Arora S. Endo echo improves primary care provider and community health worker self-efficacy in complex diabetes management in medically underserved communities. Endocr Pract. 2018;24(1):40–46. doi:10.4158/EP-2017-0079
38. Jafar TH, Gandhi M, de Silva HA, et al. A community-based intervention for managing hypertension in rural South Asia. N Engl J Med. 2020;382(8):717–726. doi:10.1056/NEJMoa1911965
39. Gampa V, Smith C, Muskett O, et al. Cultural elements underlying the community health representative - client relationship on Navajo Nation. BMC Health Serv Res. 2017;17(1):19. doi:10.1186/s12913-016-1956-7
40. Szajna A, Tekkalaki B, Nandagaon V, et al. Feasibility and acceptability of a community health worker administered behavioral activation intervention for postpartum depression: a single arm pilot study from India. Front Psychiatry. 2024;15:1284674. doi:10.3389/fpsyt.2024.1284674
41. Grant V, Litchfield I. Acceptability of community health worker and peer supported interventions for ethnic minorities with type 2 diabetes: a qualitative systematic review. Front Clin Diabetes Healthc. 2024;5:1306199. doi:10.3389/fcdhc.2024.1306199
42. Pérez-Escamilla R, Damio G, Chhabra J, et al. Impact of a community health workers-led structured program on blood glucose control among latinos with type 2 diabetes: the DIALBEST trial. Diabetes Care. 2015;38(2):197–205. doi:10.2337/dc14-0327
43. Hansotte E, Andrea SB, Weathers TD, Stone C, Jessup A, Staten LK. Impact of community health workers on diabetes management in an urban United States Community with high diabetes burden through the COVID pandemic. Prev Med Rep. 2024;39(102645):102645. doi:10.1016/j.pmedr.2024.102645
44. Hark LA, Tan CS, Kresch YS, et al. Manhattan vision screening and follow-up study in vulnerable populations: 1-month feasibility results. Curr Eye Res. 2021;46(10):1597–1604. doi:10.1080/02713683.2021.1905000
45. Hark L, Waisbourd M, Myers JS, et al. Improving access to eye care among persons at high-risk of glaucoma in Philadelphia--design and methodology: the Philadelphia glaucoma detection and treatment project. Ophthalmic Epidemiol. 2016;23(2):122–130. doi:10.3109/09286586.2015.1099683
46. Burn H, Puri L, Roshan A, Singh SK, Burton MJ. Primary eye care in Eastern Nepal. Ophthalmic Epidemiol. 2020;27(3):165–176. doi:10.1080/09286586.2019.1702217
47. Yasmin S, Schmidt E. Primary eye care: opportunities for health system strengthening and improved access to services. Int Health. 2022;14(Suppl 1):i37–i40. doi:10.1093/inthealth/ihab062
48. Wallerstein N, Duran B. Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. Am J Public Health. 2010;100 Suppl 1(S1):S40–S46. doi:10.2105/AJPH.2009.184036
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025