Back to Journals » Patient Preference and Adherence » Volume 17
Patients’ Perception of Patient-Centered Care and Associated Factors Among Patients Admitted in Private and Public Hospitals: A Comparative Cross-Sectional Study
Authors Ewunetu M ![]() , Temesgen W, Zewdu D
, Temesgen W, Zewdu D ![]() , Andargie A, Kebede M, Lidetu T
, Andargie A, Kebede M, Lidetu T ![]()
Received 21 December 2022
Accepted for publication 5 April 2023
Published 17 April 2023 Volume 2023:17 Pages 1035—1047
DOI https://doi.org/10.2147/PPA.S402262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mengistu Ewunetu,1 Worku Temesgen,2 Dagmawit Zewdu,2 Astewle Andargie,1 Mulu Kebede,1 Tadios Lidetu2
1Department of Adult Health Nursing, College of Medicine and Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Adult Health Nursing, College of Medicine and Health Science, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Mengistu Ewunetu, Debre Tabor University, P.O.Box Address: 272, Debre Tabor, Ethiopia, Tel +251945575289, Email [email protected]
Introduction: The provision of patient-centered care is challenging around the globe, including in Ethiopia. There is a scarcity of information on this issue. Therefore, this study aimed to assess patients’ perceptions of patient-centered care and associated factors among patients admitted to public and private hospitals in Bahir Dar city.
Methods: A facility-based comparative cross-sectional study was conducted from May 8–June 15, 2022. Using a multistage sampling approach, the study participants were selected. An interviewer was used to collect the data. Bi-variable and multivariable logistic regressions were used to analyze the data. Statistical significance was declared using a p value< 0.05.
Results: Overall, 53.7% of patients reported poor patient-centered care. And it was higher among public hospitals (66.3%) than private hospitals (40.3%). Length of stay (AOR = 4.2; 95% CI [1.1, 15.3] and AOR = 4.3; 95% CI [1.4, 13]), intimacy with providers (AOR = 2.4; 95% CI [1.2, 4.6] and AOR = 3.9; 95% CI [1.1– 9.6]), privacy during care (AOR = 4.2; 95% CI [1.93, 8.9]and AOR=3.3;95% CI: [1.5– 7]), easy access to service (AOR=2.76;95% CI [1.33, 5.74] and AOR=3.8;95% CI [1.15, 12.7]) were associated with patient-centered care in public and private hospitals respectively. Awareness of the disease (AOR = 2.3; 95% CI [1.12, 4.8]), information on plans of care (AOR = 4.6; 95% CI [1.9, 10]), and being involved in decisions (AOR = 2.7; 95% CI [1.28, 5.9]) were associated factors in private hospitals. The following factors were associated with the practice of patient-centered care only in public hospitals: residence (AOR = 2.9; 95% CI [1.4, 5.5]), medication information (AOR = 2.88; 95% CI [1.34, 6.2]), and external appearance of hospital (AOR = 2.27; 95% CI [1.04, 4.97]).
Conclusion: This study showed that the practice of patient-centered care in public hospitals was poor compared to that in private hospitals. Hence, hospitals should train their staff regarding a culture of patient-centered care in order to deliver high-quality and safer care.
Keywords: patient-centered care, public hospitals, private hospitals
A Letter to the Editor has been published for this article.
Introduction
Patient-centered care was introduced by the American Institute of Medicine (IOM) to improve the quality of health care services in the 21st century.1 The American Institute of Medicine defines patient-centered care (PCC) as care that is organized around the patient and where providers partner with patients and families to identify and satisfy the patient’s full range of needs and preferences.1 Patient-centered care aims to put patients at the center of their healthcare and treat them as individuals and as a partner and to let them be responsible for developing more integrated services that have the potential to generate significant benefits, including improving access to care, better health knowledge, increased compliance with the agreed care plan and treatment, increased survival/healing process, increased satisfaction with care, decreased patient distress, reduced length of stay in hospitals, reduced overall costs, and increased physical wellbeing.2–9 And also, PCC is directly and indirectly associated with quality and patient safety because it suppresses the negative impact of the staffing shortage and duty length on the quality of care and patient safety and complements the positive impact of a healthy work environment on the outcomes of care.10–12
Lack of patient-centered health care also contributes to poor quality of health care by causing missed appointments and decreased treatment adherence.13 Examining patients’ perception of services given to patients is the main concern of the health organization.14 This is an important way for patients, health professionals, and health care organizations to provide quality care by encouraging patients to take a more active role in maintaining and promoting their care.15 The Picker Institute and Harvard University proposed eight dimensions to measure PCC; these are patients’ preferences, information and education, access to care, physical comfort, emotional support,16,17 involving family and friends, continuity and transition, and the coordination of care.18
Patient-centered care has been central to health professionals’ developing a holistic care approach, including a biopsychosocial approach to the patients they are serving.19 But around the globe, the health system is failing to meet the needs of patients, despite the rising sophistication of equipment and the mobilization of massive resources. In Africa, especially in the sub-Saharan region, there is poor implementation related to providers, organizational features of the health system, and the wide socio-economic environment in which health care providers work.20
A study conducted in low- and middle-income countries showed that 8.6 million deaths occurred each year related to poor-quality health care.21 A cross-sectional study conducted in Saudi Arabia shows that around 73% of patients perceived patient-centered care as good.22
A survey from South Africa suggests that the percentage of patients who rated their experiences as poor patient-centered health care practice was 16.8% for public and 3.2% for private health institutions, respectively.23 A study done in Addis Ababa showed that 51% perceived poor patient-centered health care practice among patients admitted to hospitals.24 Even though patients differ in terms of social, biologic, or cultural characteristics as well as in their preferences and the need for a more patient-centered approach in clinical practice and evaluation, this is widely recommended.25 Previous studies from different literature show that residency, intimacy with care providers, awareness of disease, information on medication, easy access to services, involvement in decision making, privacy during care, appearance of the hospitals, and information on plans of care were factors that affected patients’ perception of patient-centered health care.22,24,26,27 In Ethiopia’s health system, it has been a priority area of health selectors’ transformation plan (HSTP) and the focus of quality improvement (QI), but it is mostly being implemented from a provider-centered approach. It also had limited understanding of patients’ perspectives, and less is known regarding the PCC of patients admitted to private and public hospitals.24 Currently, there is no such published study on patient-centered care and associated factors in this area at governmental and private hospitals. Therefore, this study aimed to assess patients’ perception of patient-centered care and associated factors among admitted patients in Bahir Dar city public and private hospitals. Thus, measuring patient-centered care from patients’ perspectives is critical to identify and prioritize areas of health care where improvements are needed during delivery of care, identifying patients’ desires, and gaining important feedback for health professionals to make meaningful improvements during care, as well as an important service indicator to measure the performance of a healthcare facility.28–30 This can increase information about services given in the organization and ensure trust between health care providers and patients as well as health institutions.
Methods and Materials
Study Setting and Study Period
The study was conducted in Bahir Dar, the capital city of the Amhara regional state in northern Ethiopia; it is far (565km) from Addis Ababa, the capital city of Ethiopia. According to data obtained from the Amhara regional health bureau, there are 7 hospitals in Bahir Dar city. Among these, there are 3 public hospitals (Tibebe Ghion specialized hospitals, Felege Hiwot compressive specialized hospitals, and Addis Alem primary hospitals) with 581, 629, and 250 average monthly adult patient admissions respectively, and four private hospitals (Gamby, Afilas, Adinas, and Dream Care) are found in the city with monthly average adult patient admissions of 170, 95, 115, and 64 respectively. The study was conducted from May 8 to June 15, 2022.
Study Design
A facility-based comparative cross-sectional study was conducted.
Source Population
All adult patients who were admitted in Bahir Dar city governmental and private hospitals.
Study Population
All adult patients admitted to Bahir Dar city selected governmental and private hospitals who were available during data collection.
Inclusion and Exclusion Criteria
At the time of data collection, all adult patients who were admitted to surgical, medical, and gynecological wards and those who were waiting in hospitals for 24 hours or more were included in the study. In contrast, all severely ill patients who were unable to give information at the time of data collection and outpatient clients were excluded from interviews.
Operational Definition and Terms
Patient-centered care is the involvement of patients in clinical care with health care providers and measured with the eight dimensions of patient-centered care. Respondents who scored above or equal to the mean of the scored data, were classified as receiving “good patient-centered health care practice”, and if they scored below the mean, they were classified as receiving “poor patient-centered health care practice”.24
Easy access to service: the presence of timely health service available in the institution without difficulty. Patients had “good” perception if they scored above or equal to the mean and “poor” perception, if they scored below the mean.18,24
Communication on plan of care: the perception of the patient regarding clear information on treatment plan during hospital stay. Patients had “good” perception, if they scored above or equal to the mean and “poor” perception, if they scored below the mean.18,24
Privacy during care: perception of the respondent whether there was privacy during care. Patients had “good” perception, if they scored above or equal to the mean and “poor” perception, if they scored below the mean.18,24
Intimacy with providers: respondents’ perception regarding whether they knew their health care providers or care givers. It was measured with “yes” or “no”.24
Decision involvement regarding treatment: perception of patients regarding their involvement with healthcare provider in the choice of treatments or procedure, it was measured with “yes” or “no”.18,24
Information on medication: patients’ perception regarding the medication, how/when he/she were informed by health care providers, it was measured with “yes” or “no”.24
Sample Size Determination and Sampling Methods
Sample Size Determination
Using independent variables, EPI INFO version 7.2.0.1 was used to calculate the sample size. Thus, variables were information sharing regarding medication, intimacy with providers, and easy access to service. Using the assumption of CI = 95%, power =80%, the ratio of unexposed to exposed was 1:1, the percent outcome in the exposed group (P1 = 72.1%), and the percent outcome in the unexposed group (P2 = 27.8%).24 Accordingly, the sample size calculated by using the independent variable patients’ intimacy with care providers was found to be the highest, and 10% of non-respondents were considered. The calculated sample size was 400. Considering the design effect of 1.5, n=1.5*400, n=600. Therefore, using a 1:1 ratio, the final estimated sample size was 600 (300 from public and 300 from private) participants.
Sampling Methods
A multi-stage sampling technique was used. There are seven hospitals in Bahir Dar city; among those, two (TGSH and FHCSH) public hospitals and three (Gamby, Afilas, and Adinas) private hospitals were selected using a simple random sampling technique using a lottery method. The sample size was allocated equally to both private and public hospitals. Then a sample size was allocated for each hospital proportionally based on inpatient flow from the previous month’s average number of patients. From this, 156 for FHSCH, 144 for TGSH, 107 for Gamby, 95 for Afilas, and 98 for Adinas hospital were proportionally allocated. Then proportional allocation was done for selected wards (surgical, medical, and gynecology) based on the previous month’s average admitted numbers of patients. The first patient was randomly selected after calculating the interval for both public and private hospitals, and then every 4th patient for public hospitals and every 2nd patient for private hospitals were selected from each ward until a sample size was achieved for each hospital (Figure 1). Patients who were not present at the time of data collection were skipped, and the next number was included.
 |
Figure 1 Sampling procedure for patients’ perception of patient-centered care among patients admitted in Bahir Dar city public and private hospitals, 2022. |
Data Collection Tools and Procedure
An interviewer-administered structured questionnaire was used to collect data from participants during the study period. The data collection was done by three nurses (diploma) and one BSc nurse in a supervisory role. It has four parts, socio-demographics, eight dimensions of patient-centered health care, organizational and care provider-related factors.
The Institute of Picker and Harvard University developed eight dimensions for patient-centered care that are used to assess providers and health organizations on PCC. The dimension included respect for patients’ needs and preferences; physical comfort; coordination and integration of care; transition and continuity of care; emotional support; accessibility of care; information and education for patients; and family and friends’ involvement; and the tool had a five-point Likert scale with a total of 34 items.31 The 34 items were computed and dichotomized as “good” and “poor”. The questionnaire was adapted from studies done in Addis Ababa and was established in the Netherlands with the reliability of the tool checked by researchers and Cronbach’s α was 0.89.24,27,32 It has a provider-related questionnaire, which has six items and answered with yes or no for each question. The organizational related variables had nine items answered on a five-point Likert scale, and each variable was computed and dichotomized. The data were reported as “good” and “poor” patient-centered care.
Data Quality Assurance and Control
The Structure questionnaire was translated into the local language (Amharic) and then back to English for consistency. To ensure the quality of data, three nurses (diploma) for data collection and one BSc nurse as supervisor were recruited and training was given for two days on how to collect data, objective, exclusion, and inclusion criteria. The questionnaires were also pretested on 5% (30) of patients from Addis Alem primary hospital before data collection to assess the questionnaire’s reliability, consistency, and appropriateness, with subsequent correction and modification. Throughout the data collection period, the investigators and supervisor also did continuous follow-up and supervision. The collected data were reviewed and checked for completeness every day and before data entry.
Data Analysis and Presentation
The data were checked for completeness and consistency, and then cleaned, coded, and entered into Epidata 4.6 and exported to SPSS version 25 for analysis. Multi-collinearity was checked using variance inflation factor (VIF) and the VIF of each variable was <5. The Hosmer and Lemeshow goodness-of-fit test was performed (P > 0.05).
Descriptive statistical analysis such as frequency distribution and proportion was done for dependent and independent variables. To control the possible effect of confounders, all explanatory variables with a p-value of 0.25 from the binary logistic regression model were fitted into the multivariable logistic regression model, and finally the variables that had been independently associated with the dependent variable were identified on the basis of 95% CI and p-value less than 0.05.
Result
Socio-Demographic Characteristics of Respondents
A total of 600 admitted patients were included in this study, with a response rate of 100% for both public and private hospitals. The mean ±SD age of the study participants in public and private hospitals was 46.6±37.5 and 42.29 ±25.84 years, respectively. Of the total study participants, 154 (51.3%) were male in public hospitals and 167 (55.7%) in private hospitals. Of the total respondents, 156 (52%) patients admitted to public hospitals and 141 (49.6%) patients admitted to private hospitals were from rural areas. From the admitted patients, 173 (57.7%) stayed in public hospitals for 6–10 days, and 243 (81%) stayed in private hospitals for 1–5 days (Table 1).
 |
Table 1 Socio-Demographic Characteristics of the Respondents in Public and Private Hospitals |
Provider Related Factors
Of the study participants, 170 (56.7%) and 144 (48%) did not know their health care providers from public and private hospitals during care, respectively. In addition, more than half of the 196 (65.3%) patients were not involved in decision making during their care in public hospitals, and 121 (40.3%) patients were not involved in decision making in private hospitals. Number of study participants who did not respond to “awareness of their disease or diagnosis” was 234 (78%) in public hospitals and 136 (45.3%) in private hospitals (Table 2).
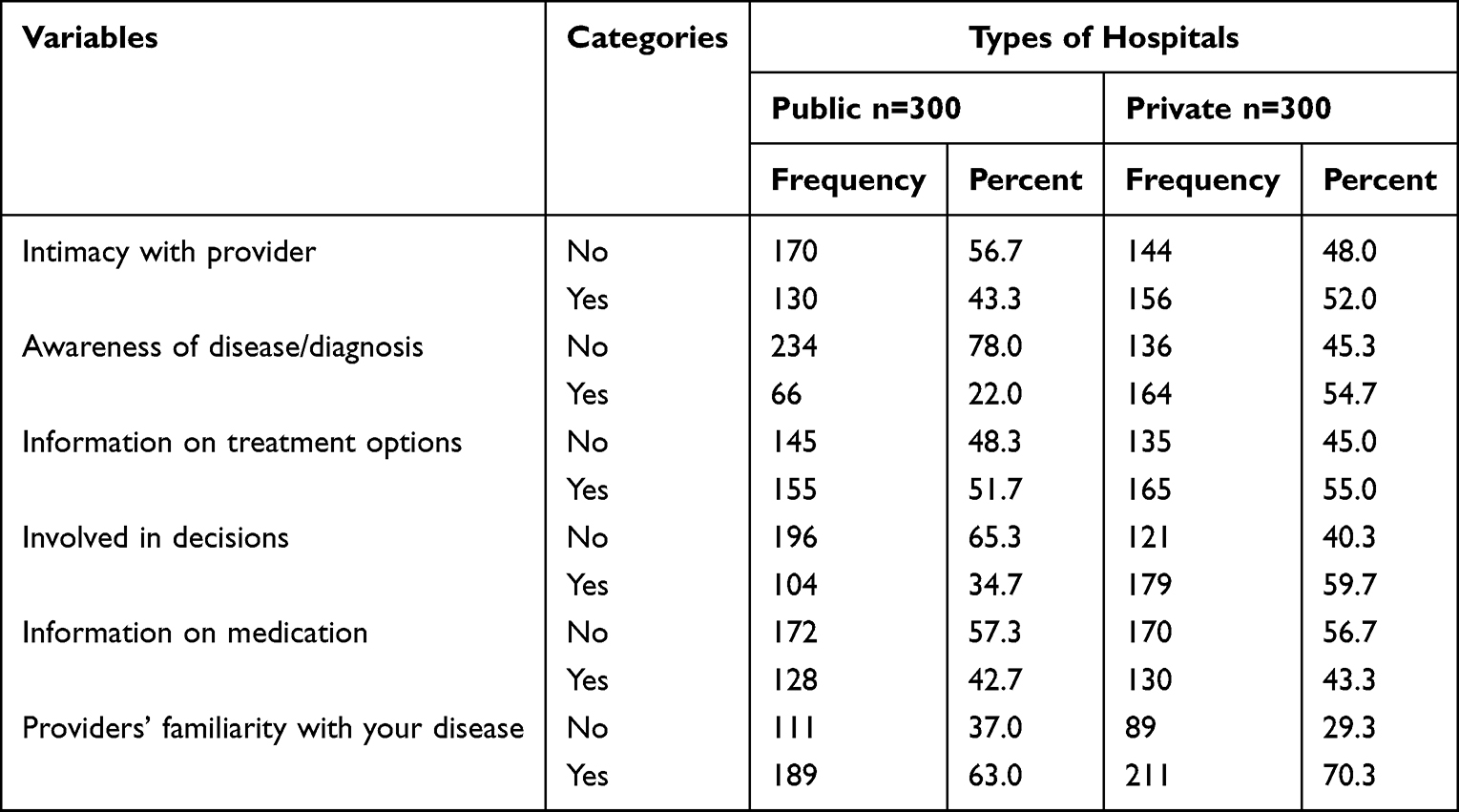 |
Table 2 Perceived Health Providers’ Related Factors That Might Affect Patient-Centered Care in Public and Private Hospitals of Bahir Dar City, 2022 |
Institutional Related Factors
Among study participants, 118 (39.5%) in public hospitals and 192 (64%) in private hospitals had a good perception of “easy access to services”. More than half, 156 (52%), of the study participants were from private hospitals, and 107 (35.7%) of public hospital users perceived the hospital to have provided “privacy during care”. Of the total, 181 (60.3%), of the private hospital study participants perceived that the hospital had a “good external appearance”. On the contrary, 104 (34.7%) participants from public hospitals perceived a “good external appearance” of hospitals (Table 3).
 |
Table 3 Perceived Institutional Related Factors That Might Affect the Patient-Centered Care at Public and Private Hospitals of Bahir Dar City, 2022 |
Overall Prevalence of Patient-Centered Care
The overall mean patient-centered health care practice was 112 (SD ± 30) with a range of 43 up to 170. The current finding showed that perceived poor patient-centered health care practices in public and private hospitals were 66.3% (95% CI; 62–72%) and 40% (95% CI; 35–46%), respectively. The overall finding showed that more than half, 322 (53.7%), of patients experienced poor patient-centered health care practice in Bahir Dar city hospitals (Table 4).
 |
Table 4 Eight Dimension Measuring of Patient-Centered Care at Public and Private Hospitals of Bahir Dar City, 2022 |
Factors Related To Patient-Centered Care at Public Hospitals
In a bi-variable analysis, fifteen variables were associated with patient-centered health care practice in public hospitals. In multivariable analysis, seven of them were found to be significantly associated. When compared to patients with rural residence, the odds of an urban resident perceiving poor patient-centered health care practices were 2.9 times more likely (AOR = 2.9; 95% CI: (1.4, 5.5). The odds of patients who stayed at hospitals for 6–10 and 11–14 days perceiving poor patient-centered health care practice were 3.3 and 4.2 times higher as compared to the odds of patients who stayed at hospitals for less than five days (AOR=3.3; 95% CI (1.6,7) and (AOR=4.2 (1.1, 15.3) respectively. Patients who knew their health care provider were 2.4 times more likely to perceive poor patient-centered health care practice as compared to patients who did not know their health care provider (AOR = 2.4; 95% CI: (1.2, 4.6). Patients who did not receive information on medication making during care were 2.88 times more likely to perceive poor patient-centered health care as compared to their counterparts (AOR = 2.88; 95% CI: (1.34, 6.2). Patients who did not agree on easy access to service were 2.76 times more likely to perceive poor patient-centered health care practice as compared to those who did agree (AOR = 2.76; 95% CI: (1.33, 5.74). Patients who perceived the external appearance of the hospitals as not good looking were 2.27 times more likely to perceive poor patient-centered health care practice as compared to patients who perceived the external appearance of the hospitals as good-looking (AOR = 2.27; 95% CI: 1.04, 4.97). Patients who perceived poor privacy during hospital care were 4.2 times more likely than patients who perceived good privacy during hospital care to perceive poor patient-centered health care practice (AOR = 4.2; 95% CI: 1.93, 8.99) (Table 5).
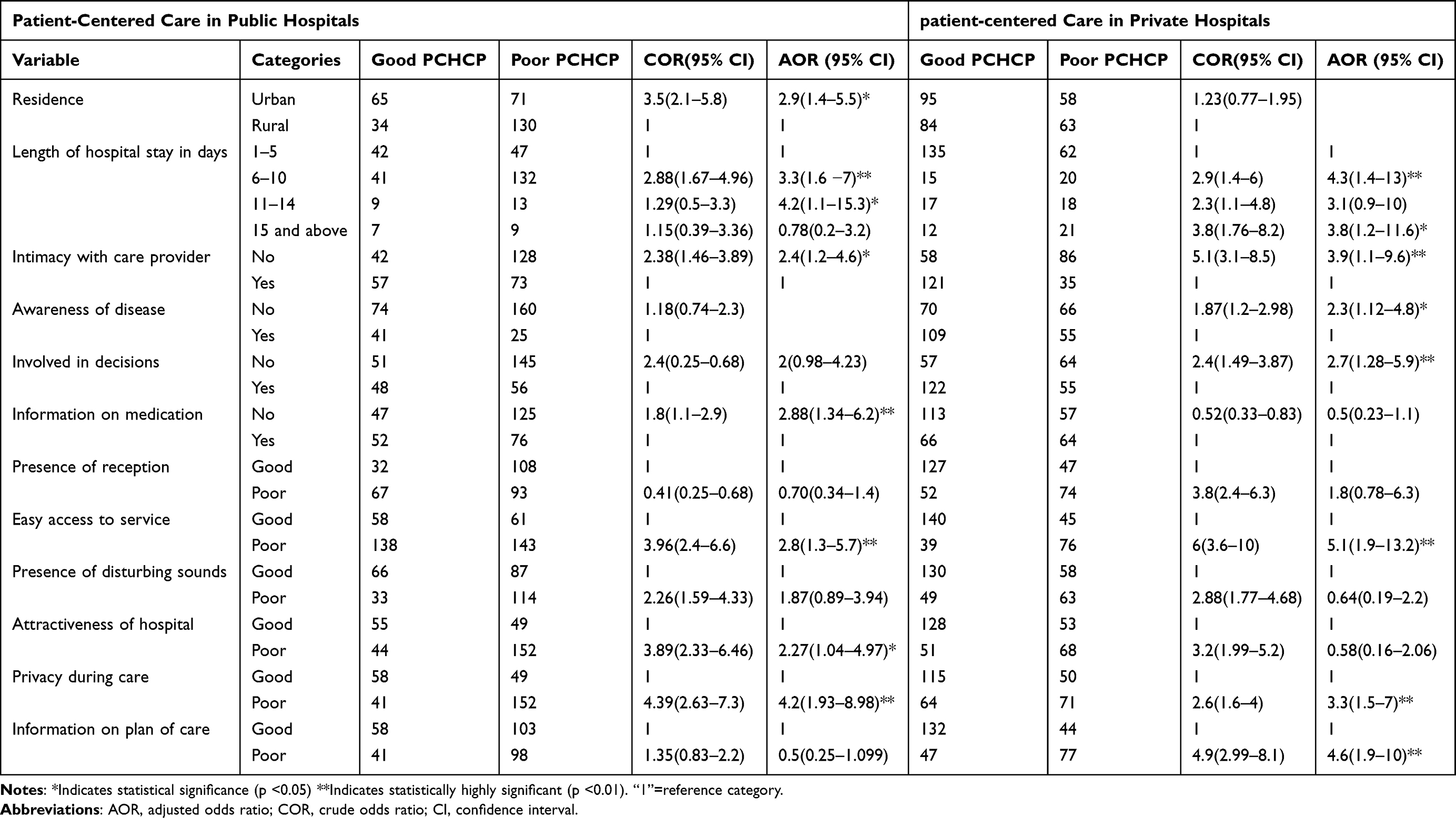 |
Table 5 Bi-Variable and Multivariable Logistic Regression Analysis of Patient-Centered Care in Private and Public Hospitals |
Factors Related to Patient-Centered Care at Private Hospitals
Both bivariable and multivariable logistic regression analyses were implemented to determine factors that were associated with patient-centered care in private hospitals. Respondents who had stayed in the hospital for 6–10 days or more were 4.3 and 3.8 times more likely to perceive poor patient-centered care, respectively (AOR = 4.3; 95% CI: 1.4, 13) and (AOR = 3.8; 95% CI: 1.2, 11.6). When compared to their counterparts, patients who did not know their health care provider were 3.9 times (AOR = 3.9; 95% CI: 1.1–9.6) more likely to have poor patient-centered care. The odds of poor patient-centered were 2.3 times more likely among patients who did not receive information on disease than their counterparts (AOR = 2.3; 95% CI: 1.12, 4.8). And also, respondents who had not received information on the plan of care were 4.6 times more likely to perceive poor patient-centered care (AOR = 4.6; 95% CI: 1.9, 10). Patients who did not have any involvement in decisions during care were 2.7 times more likely to perceive poor patient-centered care than their counterparts (AOR = 2.7; 95% CI: 1.28, 5.9). On the other hand, as compared to patients who perceived good privacy, those who perceived the opposite were 3.3 times more likely to perceive the care as poor (AOR: 3.3; 95% CI: 1.5–7). Furthermore, patients who did not agree on easy access to service were 5.1 times more likely to perceive poor patient-centered care (AOR=5.1;95% CI:1.9, 13.2) (Table 5).
Discussion
This study aimed to measure perceived patient-centered care in private and public hospitals in Bahir Dar, Ethiopia. In addition, the study tried to compare perceived patient-centered care and its associated factors among patients admitted to private and public hospitals. The current finding showed that rate of poor patient-centered care among patients admitted to governmental and private hospitals was 66.3% and 40% respectively. This finding was much higher than that of a study conducted in South Africa, which found 16.8% of public hospital patients and 3.2% of private hospital patients perceived poor patient-centered care.23 This discrepancy might be due to different socioeconomic status, infrastructure, and measuring tools.33 The current finding showed a higher magnitude of poor patient-centered care was in public hospitals as compared to private hospitals, which was similar to the study done in Addis Ababa.24 This might be due to the ease of access to services, including the reception of patients, equipped with modern equipment and provision of quality care to attract more customers to private hospitals.34,35
The overall (both public and private hospitals) finding showed that more than half, 53.7%, of patients perceived poor patient-centered care. This finding was similar to the study conducted in Addis Ababa (51%).24 However this finding was higher as compared to the study conducted in Saudi Arabia (27%)22 and Norway (15%).9 This inconsistency might be due to difference in sociodemographics and measuring tools, as the previous study used 17 scale questionnaires.36 This finding showed that low level of patient-centered care indicates poor quality of care given to patients by health facility.
We found patients staying for longer in hospital were more likely to have a poor perception of patient-centered care as compared to patients staying in hospital for less than five days among patients admitted in both private and public hospitals. This was similar to the study done in South Wollo.27 This might be due to the fact that patients who stay longer in hospital have higher demands, physical disturbance, sleep deprivation, and might have hospital-acquired infections as they spend more time in hospitals.
On the other hand, the odds of having a poor perception of patient-centered care were higher in patients with a poor perception of access to service as compared to those with a good perception of access to service in private and public hospitals. The study showed poor patient experience regarding easy access to service risks patients who might have returned for future health care needs.37
Privacy during care was significantly associated with a poor perception of patient-centered care. Study participants who had poor perceptions of privacy during care were more likely to perceive poor patient-centered care among public and private hospitals. The findings of this study were similar to those in Addis Ababa.24 This might be due to over-disclosures of private patient information unpleasantly affecting patients’ trust which can lead to ending their relationship with healthcare providers.38
Patient involvement in decisions during treatment was significantly associated with patient-centered care only in private hospitals. This finding showed that study participants who were not involved in decisions during treatment were more likely to have poor perception of patient-centered care as compared to those who were involved in decisions. This finding is similar to the study done in Switzerland.39 A study showed that involvement of patients in decisions during care increases knowledge about the condition, of the harm and benefit, increases responsibility sharing, increases the quality of care, and better patient outcome.35,40
Information on plans of care was significantly associated with perceiving poor patient-centered care only in private hospitals. This was similar to studies done in Tanzania41 and Addis Ababa.24 The association might be due to patients’ limited understanding of their plan of care which may adversely affect their ability to provide informed consent for hospital treatment and success in treating their disease.42
Patients who did not know their care provider were more likely to perceive poor patient-centered care as compared to patients who had good intimacy with care provider in public and private hospitals. This was similar to a study done in Ethiopia, Addis Ababa.24 Patients who have good intimacy with care providers may have improved relationships and be encouraged to disclose their issues without frustration.43
Also, being an urban resident, attractiveness of hospitals and information on medication were significantly associated with poor patient-centered care only in public hospitals. The odds of perceived poor patient-centered care among urban residents were higher as compared to rural residents. This was similar to the study done in South Wollo.27 This might be due to patients from rural areas being satisfied with simple bits of help, and it might be related to the awareness and access to health information and educational status of urban residents.
From this study, information on medication was significantly associated with perceived patient-centered care. Study participants who did not receive information on medication were more likely to perceive poor patient-centered care as compared to those who did get information on medication. This was similar to the study done in Addis Ababa.24 The association of perceived patient-centered health care and information on medication might be due to the fact that patients who receive clear advice on medication are more likely to adhere to their treatment and decrease intentional non-adherence to treatment.44
Attractiveness of hospitals was significantly associated with perceived patient-centered care. Study participants who perceived the attractiveness of the hospitals as “not good” were more likely to perceive poor patient-centered care as compared to patients who perceived the hospitals as good looking among patients admitted to public hospitals. This might be due to the external appearance of hospitals, which may affect the health and comfort of patients, staff, and visitors and can exacerbate patient suffering.45
Another factor that was significantly associated with perceived patient-centered care among patients admitted only to private hospitals was awareness of their disease. This finding also showed that patients who were not aware of their disease were more likely to perceive the healthcare encountered as poor. The study is in agreement with a study done in Addis Ababa.46 A finding showed patients who do not fully understand their disease are more likely to have decreased self-care and noncompliance with treatment. This result indicates the need for health professional accountability and responsibility to provide optimal information.47
Limitation and Strength of the Study
A strength of the study is that primary data were used and it was a multi-center cross-sectional study.
Social desirability bias might be a limitation due to patients’ self-rating patient-centered care, and because participants rated their previous interaction with healthcare providers which could lead to some bias due to fear of getting service the next time. To reduce this bias, interviewers were selected out of selected representative hospitals and participants were interviewed in a private room.
Conclusion
This study showed that more than half of the patients perceived poor patient-centered care. Moreover, the magnitude of poor patient-centered care was higher among public hospitals as compared to private hospitals. Length of stay, intimacy with care provider, privacy during care, easy access to service were commonly associated with patient-centered care in both private and public hospitals. Awareness of disease, involvement in decisions, and information on planes of care were significantly associated with perceived poor patient-centered care among patients admitted in private hospitals, whereas residence, information on medication and external appearance were associated with poor patient-centered care in public hospitals.
This study provides input for policymakers and helps the health care system provide high quality care. This will help fulfill the targets of reducing patient hazards and improving outcomes. Therefore, the government shall better support the care given in these institutions and instill the culture of patient-centered care because the majority of patients utilize public hospitals.
Recommendations
For Health Professionals
The health care professional shall see the gaps that lead to the possible reasons for poor patient-centered health care practice among hospitals’ inpatient service regarding giving quality care such as creating good intimacy with patients, involving patients in decisions during treatment by providing optimal information, promoting awareness of the disease, and giving information on medication. Reduce patients’ length of stay in hospital by providing appropriate healthcare services.
Regional Health Bureau and Federal Ministry of Health
The Federal Ministry of Health and the Regional health bureau should give greater emphasis and provide appropriate strategies to provide patient-centered health care practice that increases patients’ levels of perception by assisting hospitals or filling gaps, as well as providing scheduled capacity-building training for health care providers.
For Researchers
Future researchers should evaluate provider’s perspective of patient-centered health care. And also, as the study was assessing patients’ perception, future researchers should conduct qualitative studies to have in-depth knowledge of poor patient-centered health care practice.
Abbreviations
AOR, adjusted odds ratio; ADH, Adinas hospitals; AFH, Afilas hospitals; CAHP, Californian Association of Health Plan; COR, crude odds ratio; FHCSH, Felege Hiwot Comprehensive Specialized Hospital; GH, Gamby hospitals; G w, Gynecology ward; HSTP, Health Sectors Transformation Plan; IOM, Institute of Medicine; LMIC, low and middle income country; M, Medical ward; NADH, no. of inpatient admission in Adinas hospitals; NAFH, no. of inpatient in Afilas hospitals; NGH, no of inpatient admission in Gamby general hospitals; NFHH, no of inpatients admission in Felege Hiwot hospitals; NTG, no of inpatient admission; PCHCP, patient-centered health care practice; QI, Quality Improvement; S, Surgical ward; TGSH, Tibebe ghion specialized hospital.
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for the research was obtained from Bahir Dar University, college of medicine and health sciences, institutional review board and ethics committee with protocol number 413/2022. The patients were informed about the confidentiality of the information they provided, and written consent was obtained from each participant. The participants were not required to write their names on the questionnaires. The respondents were informed that they had the right to refuse or terminate the interview at any point. This study was conducted following the ethical standards of the Declaration of Helsinki.
Acknowledgment
We would like to acknowledge Bahir Dar University for the opportunity and financial support. We also acknowledge the private and public hospitals’ administrators, ward coordinators for their help during the data collection for this thesis. Finally, special gratitude goes to the study participants who shared their ideas. The abstract of this paper was presented at the https://ir.bdu.edu.et/handle/123456789/15069 as a thesis.
Author Contributions
Mengistu Ewunetu, Worku Temsgen (associate professors, PHD), Dagmawit Zewdu, Astewle Andargie, Mulu Kebede, and Tadios Lidetu played their role in contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding for this work.
Disclosure
The authors declare that they have no competing interests.
References
1. Plsek P. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington: DC National Academies Pr; 2001.
2. Paparella G. Person-Centred Care in Europe: A Cross-Country Comparison of Health System Performance, Strategies and Structures. Picker Institute; 2016.
3. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. 2019;19(1):1–9. doi:10.1186/s12913-018-3818-y
4. Barry MJ, Edgman-Levitan S, Sepucha K. Shared decision-making: staying focused on the ultimate goal. NEJM Catalyst. 2018;4:5.
5. Kane P, Murtagh F, Ryan K, et al. The gap between policy and practice: a systematic review of patient-centred care interventions in chronic heart failure. Heart Fail Rev. 2015;20(6):673–687. doi:10.1007/s10741-015-9508-5
6. Sahlen K-G, Boman K, Brännström M. A cost-effectiveness study of person-centered integrated heart failure and palliative home care: based on a randomized controlled trial. Palliat Med. 2016;30(3):296–302. doi:10.1177/0269216315618544
7. World Health Organization. People-Centred and Integrated Health Services: An Overview of the Evidence: Interim Report. World Health Organization; 2015.
8. Hyde E, Hardy M. Patient centred care in diagnostic radiography (Part 1): perceptions of service users and service deliverers. Radiography. 2021;27(1):8–13. doi:10.1016/j.radi.2020.04.015
9. Endacott RBF, Cooper SJ, Forbes H, et al. Leadership and teamwork in medical emergencies: performance of nursing students and registered nurses in simulated patient scenarios. J Clin Nurs. 2015;24(1–2):90–100.
10. Jarrar M, Al-Bsheish M, Aldhmadi BK, et al. Effect of practice environment on nurse reported quality and patient safety: the mediation role of person-centeredness. In: Healthcare. Multidisciplinary Digital Publishing Institute; 2021.
11. Jarrar M, Minai MS, Al‐Bsheish M, Meri A, Jaber M. Hospital nurse shift length, patient‐centered care, and the perceived quality and patient safety. Int J Health Plann Manage. 2019;34(1):e387–e96. doi:10.1002/hpm.2656
12. Jarrar M, Rahman HA, Minai MS, AbuMadini MS, Larbi M. The function of patient‐centered care in mitigating the effect of nursing shortage on the outcomes of care. Int J Health Plann Manage. 2018;33(2):e464–e73. doi:10.1002/hpm.2491
13. National Academies of Sciences E, Medicine. Crossing the Global Quality Chasm: Improving Health Care Worldwide. National Academies of Sciences E, Medicine; 2018.
14. Bokhour BG, Fix GM, Mueller NM, et al. How can healthcare organizations implement patient-centered care? Examining a large-scale cultural transformation. BMC Health Serv Res. 2018;18(1):1–11. doi:10.1186/s12913-018-2949-5
15. Grob R. The heart of patient-centered care. J Health Polit Policy Law. 2013;38(2):457–465. doi:10.1215/03616878-1966406
16. Vancampfort D, Koyanagi A, Hallgren M, Probst M, Stubbs B. The relationship between chronic physical conditions, multimorbidity and anxiety in the general population: a global perspective across 42 countries. Gen Hosp Psychiatry. 2017;45:1–6. doi:10.1016/j.genhosppsych.2016.11.002
17. Read JR, Sharpe L, Modini M, Dear BF. Multimorbidity and depression: a systematic review and meta-analysis. J Affect Disord. 2017;221:36–46. doi:10.1016/j.jad.2017.06.009
18. Cramm JM, Nieboer AP. Validation of an instrument to assess the delivery of patient-centred care to people with intellectual disabilities as perceived by professionals. BMC Health Serv Res. 2017;17(1):1–11. doi:10.1186/s12913-017-2424-8
19. Ortiz MR. Patient-centered care: nursing knowledge and policy. Nurs Sci Q. 2018;31(3):291–295. doi:10.1177/0894318418774906
20. De Man J, Mayega RW, Sarkar N, et al. Patient-centered care and people-centered health systems in sub-Saharan Africa: why so little of something so badly needed? 2016.
21. Kruk ME, Gage AD, Joseph NT, Danaei G, García-Saisó S, Salomon JA. Mortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countries. Lancet. 2018;392(10160):2203–2212. doi:10.1016/S0140-6736(18)31668-4
22. Al-Sahli B, Eldali A, Aljuaid M, Al-Surimi K. Person-centered care in a tertiary hospital through patient’s eyes: a cross-sectional study. Patient Prefer Adherence. 2021;15:761. doi:10.2147/PPA.S286237
23. Maseko LHB, Harris B. People-entireness in health system reform. Public perceptions of private and public hospitals in South Africa. S Afr J Occup Ther. 2018;48:22–27. doi:10.17159/2310-3833/2017/vol48n1a5
24. Birhanu F, Yitbarek K, Animut Addis DA, Shifera N, Shifera N. Patient-centered care and associated factors at public and private hospitals of Addis Ababa: patients’ perspective. Patient Relat Outcome Meas. 2021;12:107. doi:10.2147/PROM.S301771
25. Lusk JM, Fater K. A concept analysis of patient‐centered care. In: Nursing Forum. Wiley Online Library; 2013.
26. Chiwire P, Beaudart C, Evers SM, Mahomed H, Hiligsmann M. Enhancing public participation in public health offerings: patient preferences for facilities in the western cape province using a discrete choice experiment. Int J Environ Res Public Health. 2022;19(1):590. doi:10.3390/ijerph19010590
27. Biks GA, Worku N, Endalew B, Dellie E, Dellie E. Patient-centered care and associated factors among Adult Admitted patients in south wollo public hospitals, Northeast Ethiopia. Patient Prefer Adherence. 2022;16:333. doi:10.2147/PPA.S346000
28. Farhadfar AH, Nasiripour AA, Haji Nabi K, Comprehensive A. Review of patient-centered care in the hospitals. J Healthc Manag. 2019;9(4):91–98.
29. Tzelepis F, Sanson-Fisher RW, Zucca AC, Fradgley EA. Measuring the quality of patient-centered care: why patient-reported measures are critical to reliable assessment. Patient Prefer Adherence. 2015;9:831. doi:10.2147/PPA.S81975
30. Chen C-B, Kao P-L. The effects of the hospital marketing promotion on consumers’ choice of hospitals consumers. J Human Resour Adult Learn. 2012;8(1):156.
31. McCormack B. Person‐centredness in gerontological nursing: an overview of the literature. J Clin Nurs. 2004;13:31–38. doi:10.1111/j.1365-2702.2004.00924.x
32. Cramm JM, Nieboer AP. Validation of an instrument for the assessment of patient-centred care among patients with multimorbidity in the primary care setting: the 36-item patient-centred primary care instrument. BMC Fam Pract. 2018;19(1):1–10. doi:10.1186/s12875-018-0832-4
33. Valentine NB, de Silva A, Kawabata K, Darby C, Murray CJ, Evans DB. Health system responsiveness: concepts, domains and operationalization. In: Health Systems Performance Assessment: Debates, Methods and Empiricism. Geneva: World Health Organization; 2003:96.
34. Kamra V, Sethi SK, Sharma J. An empirical study on service quality comparison between private and public hospitals in Delhi-NCR. Int J Mark Bus Commun. 2019;8:4.
35. Fatima T, Malik SA, Shabbir A. Hospital healthcare service quality, patient satisfaction and loyalty: an investigation in context of private healthcare systems. Int J Qual Reliab Manag. 2018;35:1195–1214. doi:10.1108/IJQRM-02-2017-0031
36. Slater P, McCance T, McCormack B. The development and testing of the Person-centred Practice Inventory–Staff (PCPI-S). Int J Qual Health Care. 2017;29(4):541–547. doi:10.1093/intqhc/mzx066
37. Sharma AE, Grumbach K. Engaging patients in primary care practice transformation: theory, evidence and practice. Fam Pract. 2017;34(3):262–267. doi:10.1093/fampra/cmw128
38. Hartigan L, Cussen L, Meaney S, O’Donoghue K. Patients’ perception of privacy and confidentiality in the emergency department of a busy obstetric unit. BMC Health Serv Res. 2018;18(1):1–6. doi:10.1186/s12913-018-3782-6
39. Bachnick S, Ausserhofer D, Baernholdt M, Simon M, Group MRS. Patient-centered care, nurse work environment and implicit rationing of nursing care in Swiss acute care hospitals: a cross-sectional multi-center study. Int J Nurs Stud. 2018;81:98–106. doi:10.1016/j.ijnurstu.2017.11.007
40. Palumbo R, Annarumma C, Manna R, Musella M, Adinolfi P. Improving quality by involving patient. The Role of Health Literacy in Influencing Patients’ Behaviors International. J Healthc Manag. 2021;14(1):144–152.
41. Rosen HE, Lynam PF, Carr C, et al. Direct observation of respectful maternity care in five countries: a cross-sectional study of health facilities in East and Southern Africa. BMC Pregnancy Childbirth. 2015;15(1):1–11. doi:10.1186/s12884-015-0728-4
42. Lotfi M, Zamanzadeh V, Valizadeh L, Khajehgoodari M. Assessment of nurse–patient communication and patient satisfaction from nursing care. Nurs Open. 2019;6(3):1189–1196. doi:10.1002/nop2.316
43. Lee N-J, Ahn S, Lee M. Mixed-method investigation of health consumers’ perception and experience of participation in patient safety activities. BMJ Open. 2020;10(3):e035831. doi:10.1136/bmjopen-2019-035831
44. Lee JL, Dy SM, Gurses AP, et al. Towards a more patient-centered approach to medication safety. J Patient Exp. 2018;5(2):83–87. doi:10.1177/2374373517727532
45. Eijkelenboom A, Bluyssen PM. Comfort and health of patients and staff, related to the physical environment of different departments in hospitals: a literature review. Intell Build Int. 2022;14(1):95–113. doi:10.1080/17508975.2019.1613218
46. Teklu AM, Abraha M, Legesse T, et al. Awareness of diagnosis, treatment plan and prognosis among patients attending public hospitals and health centers in Addis Ababa, Ethiopia. PLoS One. 2022;17(6):e0270397. doi:10.1371/journal.pone.0270397
47. Kwame A, Petrucka PM. Communication in nurse-patient interaction in healthcare settings in sub-Saharan Africa: a scoping review. Int J Africa Nurs Sci. 2020;12:100198. doi:10.1016/j.ijans.2020.100198
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficiency of Medical Equipment Utilization and Its Associated Factors at Public Referral Hospitals in East Wollega Zone, Oromia Regional State, Ethiopia
Tesfaye Geta E, Terefa DR, Desisa AE
Medical Devices: Evidence and Research 2023, 16:37-46
Published Date: 22 February 2023
Drug Therapy Problems and Associated Factors Among Hypertensive Patients in North Wollo Public Hospitals, Northeast Ethiopia: Institutional-Based Cross-Sectional Study
Baye T, Girmaw F, Ashagrie G, Kassaw AT
Integrated Blood Pressure Control 2023, 16:47-57
Published Date: 20 July 2023