")
Back to Journals » Patient Preference and Adherence » Volume 15
Patients’ Perception of Factors Influencing Noncompliance with Medication among Cardiac Patients in Fiji: A Qualitative Study
Authors Kumar A, Mohammadnezhad M , May W
Received 31 May 2021
Accepted for publication 30 July 2021
Published 24 August 2021 Volume 2021:15 Pages 1843—1852
DOI https://doi.org/10.2147/PPA.S322731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Avnit Kumar,1 Masoud Mohammadnezhad,2 William May3
1Department of Primary Care and Nutrition, Fiji National University, Suva, Fiji Islands; 2Department of Public Health and Health Services Management, Fiji National University, Suva, Fiji Islands; 3Department of Internal Medicine, Fiji National University, Suva, Fiji Islands
Correspondence: Masoud Mohammadnezhad
Department of Public Health and Health Services Management, Fiji National University, Suva, Fiji Islands
Email [email protected]
Background: Noncompliance with prescribed medication leads to disease progression, which often leads to premature deaths. It often leads to worsening symptoms of cardiac conditions and hospitalization. Due to the lack of previous research, this study aimed to explore the factors contributing to noncompliance with medication in cardiac patients in Fiji.
Methods: This qualitative study was conducted among 25 cardiac patients with congestive heart failure and coronary heart disease who attended special outpatient department (SOPD) clinics at Sigatoka Subdivisional Hospital in Fiji. Purposive sampling was used to select the study sample, and in-depth face-to-face interviews were conducted using a semistructured, open-ended questionnaire. Data were analyzed using thematic analysis, whereby the data collected were grouped in subthemes and then common themes related to the topic.
Results: A total of 25 patients were interviewed, with a majority (n=14) being men and 15 Fijian of Indian descent. A greater number (n=17) of participants were above the age of 60 years, 19 had had primary education, while 12 were unemployed. Eight themes were identified as factors affecting noncompliance with medication: scarcity of knowledge, patients’ negative attitudes, poor family support, financial constraints, forgetfulness, irregular clinic attendance, heavy alcohol use, and alternative treatment vs pharmaceutical medication.
Conclusion: Noncompliance with medication in cardiac patients contributes to worsening cardiac disease and premature deaths. For factors related to noncompliance, awareness can be raised in SOPD clinics for patients to realize the effects of noncompliance and provide ways to improve compliance. Providing professional counseling services for all SOPD patients would greatly help in increasing compliance with medication in Fiji.
Keywords: determinants, noncompliance with medication, cardiac patients, qualitative study, Fiji
Introduction
Medication compliance plays a significant part in patient management on an outpatient basis, and should be included in the package of care given to patients before discharge and on a continuing basis thereafter.1 Noncompliance with prescribed medication leads to disease progression, which often leads to premature deaths. It often leads to worsening symptoms of cardiac conditions and hospitalization.2 Drug noncompliance is a major issue in the management of patients with noncommunicable diseases.3 Compliance with therapy is a primary determinant of treatment success. Noncompliance is a serious problem that not only affects the patient but also the health-care system.4 Medication noncompliance results in approximately 125,000 preventable deaths a year globally.5 Medication compliance in medical management of cardiovascular disease is vital. Patients with acute coronary syndrome who do not adhere to their medication have threefold the likelihood of death of patients who adhere to their prescriptions.6 Poor compliance with heart failure (HF) drugs is associated with an increased number of cardiovascular-related emergency-department visits and inpatient hospital days.7 HF and poor medication adherence are often associated with high morbidity and mortality and poor quality of life. An 80% compliance rate is needed for optimal therapeutic efficacy. However, with chronic medication, compliance is around 50%.8 This is mainly due to poor access to medication, poor health-care services, and lack of knowledge of medication and diagnosis.9
Premature deaths due to cardiovascular diseases are a major issue in Fiji. Fiji experienced almost twice as many cardiovascular-related deaths as those resulting from diabetes in 2017, which is in line with global trends.10 A significant proportion of patients that are seen at outpatient clinics in Sigatoka Subdivisional Hospital (SSH) are observed to have poor compliance with medication. This is one of the main factors behind relapse of symptoms and repeated admissions.11
A literature review on this topic found a few studies done in Fiji and Pacific Island countries.12 Most of the research was based on medical professionals’ views, and patient factors in noncompliance were not captured. It is important to carry out this study to determine the patient factors that affect medication noncompliance in the local setting. This study aimed to explore factors affecting medication noncompliance in cardiac patients in Fiji. Knowledge gaps need to be addressed to facilitate better compliance with medication and prevent morbidity and premature mortality.
Methods
Design and Setting
This qualitative study was conducted among cardiac patients who attended the special outpatient department (SOPD) clinic at SSH from January 1, 2019 to December 31, 2019. SSH has 56 admission beds and receives primary referrals from seven health centers, while it refers cases to its tertiary hospital — Lautoka Hospital. The medical clinic was targeted for the purpose of this study to identify patients with cardiovascular disease, mainly coronary heart disease and congestive failure in this particular group for the study sample.
Sample and Sampling
All congestive HF and coronary heart–disease patients (diagnosis confirm by checking SOPD folders and register) were included in the study. Patients with rheumatic heart disease, mental/psychiatric conditions, and those not interested in taking part were excluded. Purposive sampling was done from the group of medical patients who attended SOPD at SSH during the study period, and all patients selected were noncompliant. Noncompliance was assessed by history-taking, abnormal vitals, and deterioration in cardiac condition. Patients were first identified verbally, and then diagnosis and noncompliance was confirmed by reviewing folders and the SOPD register. From this sample, 25 patients who met the study criteria were interviewed after giving their consent.
Data-Collection Tools
A semistructured, open-ended questionnaire was used as a guide to conduct in-depth face-to-face interviews, as in-depth interviews help individuals talk about their everyday experiences.13
The questionnaire for this study was developed after reviewing the literature and was based on the research questions. It was divided into two parts: part 1 gathered relevant demographic information, i.e., age, sex, ethnicity, education, employment status, marital status, and monthly income, and part 2 contained nine open-ended questions to explore participants’ views and perceptions and thus to identify factors associated with noncompliance with medication and clinic attendance. Patient solutions for those factors were gleaned by leading questions during the interview process.
Procedure
The SOPD nurse at SSH was approached and informed about the study. Her help was requested in locating participants, but she was not involved in data collection. A brief introduction of the study — its aim, what was expected of the participants, and the potential benefits that the study would bring about — was provided verbally in three languages (English, Hindi, and i-Taukei) by a bilingual translator to the patients while they were waiting for medical consultation by the medical officer at the SOPD clinic. This verbal introduction was done at medical clinics consisting of cardiac patients and other medical patients every Tuesday for the 3 months of data collection. Together with this verbal introduction, information sheets were provided to all interested patients (who fulfilled inclusion and exclusion criteria) in their preferred language. Those who agreed to participate were given consent forms in their preferred language.
Interviews were conducted individually and all recorded device and kept safely. Interviews took place in a consulting room in the SOPD clinic at SSH, and lasted approximately 30–45 minutes. Following collection of demographic information, an open-ended question on the topic was posed that set the stage for the interview. Questions tended to graduate from general to more particular in focus, dependent largely on interviewees’ responses. Due to the semistructured nature of interviews, the interviewer had the freedom to probe or prompt discussion of interesting issues that arose. There was a bilingual translator — an i-Taukei staff nurse sworn to confidentiality — who translated into i-Taukei for participants who did not understand English.
Data Management and Analysis
All interviews were audio-recorded, saved on a computer, and transcribed into a word-processing document by the researchers. Noticeable pauses and nonverbal behavior, such as laughter, were included in transcripts, as were interruptions and audible words. Data were analyzed manually using thematic analysis. Six phases of thematic analysis were used as a guide. The six steps of thematic analysis were becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, defining themes and writing up.14
Study Rigor
To ensure credibility, all study participants were actively involved in the interview process. They were asked to clarify if more information were needed during the interviews. To make sure the interview process was correct, it was continuously discussed with supervisors. To ensure reliability, all interviews were transcribed independently and codes, subthemes, and themes checked by the supervisors. Transferability was ensured using purposive sampling, discussing study methodology, and reaching data saturation. Study conformity was ensured by recording the interviews and taking notes.
Ethics
Ethics approval was received from the College Health Research Ethics Committee and Fiji National Health Research and Ethics Review Committee. An “in-principle” letter was obtained from the subdivisional medical officer, and permission was sought to go through the SOPD register from the head sister at SSH. All the patients provided informed consent prior to commencement of the study. We confirm that consent was obtained from study participants to have anonymized responses published. They were also informed that their participation would be voluntary and information gathered in the interviews and discussions would be confidential. The study was conducted in accordance with the Declaration of Helsinki.
Results
Demographic Characteristics
Table 1 gives the characteristics of all participants. A majority of participants (n=14) were men, and 15 Fijian of Indian descent. Seventeen were aged >60 years, 19 had had primary education, and 12 were unemployed. The average monthly income for most participants (n=20) was <FJ$400.
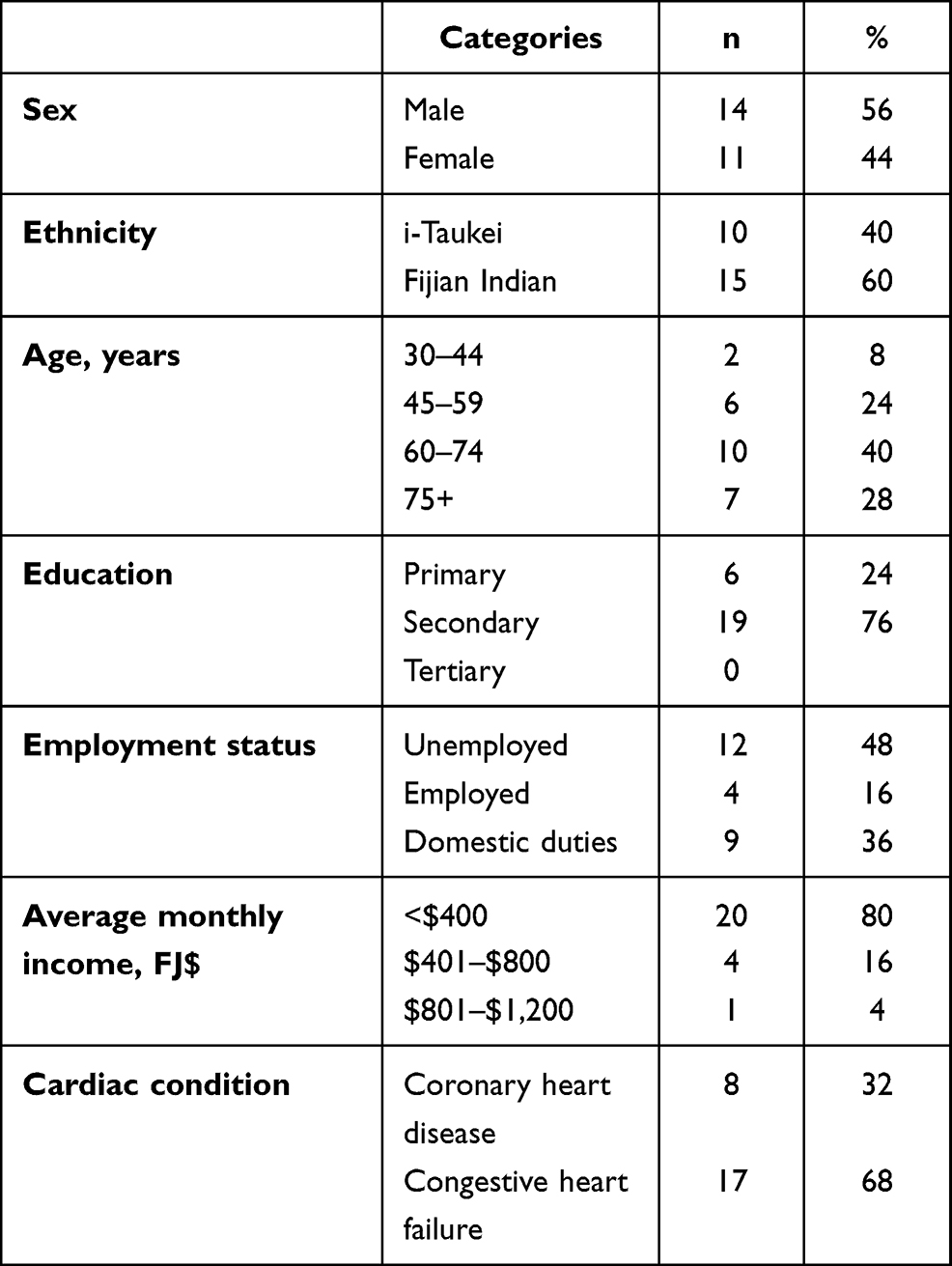 |
Table 1 Sociodemographic characteristics of participants (n=25) |
Themes Related to Noncompliance
Eight themes emerged from data analysis: scarcity of knowledge, negative attitudes, poor family support, financial constraints, forgetfulness, irregular clinic attendance, heavy alcohol use, and alternative treatment vs pharmaceutical medication. Table 2 summarizes the themes and codes.
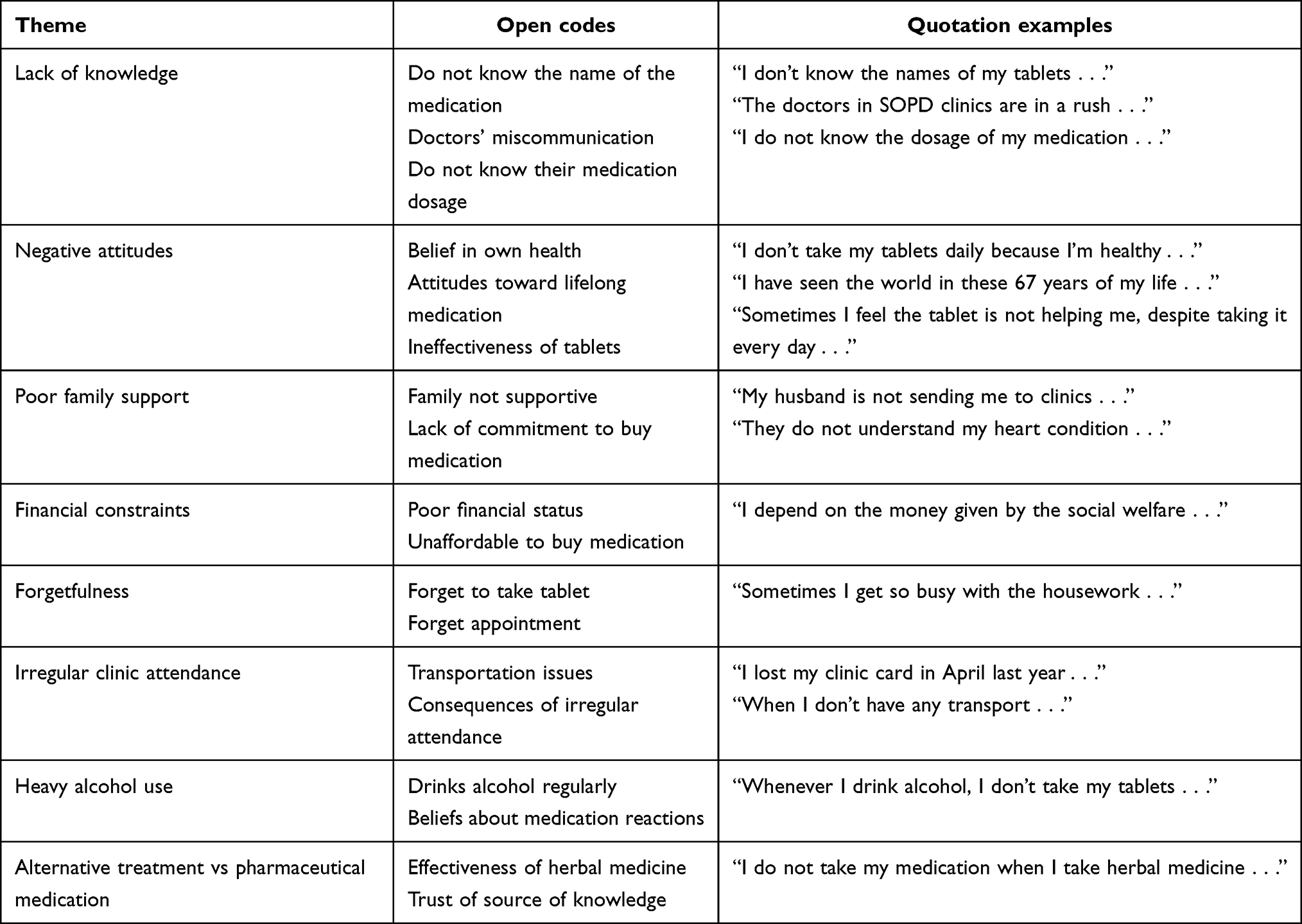 |
Table 2 Themes and codes |
Theme 1: Scarcity of Knowledge
Poor compliance is often associated with inadequate knowledge of prescribed medication. There were many patients who did not know the name of the medication they were taking, and hence missed out on taking some tablets. A participant of the study stated that he did not know the name of his medication. He showed the tablets:
I don’t know the names of my tablets, but I can show them to you, as I have brought them with me. (P6, 34-year-old male i-Taukei)
Few patients considered doctors’ miscommunication as the cause of lack of enough knowledge of the medication they were prescribed. One said that the doctors in SOPD clinics were usually in a rush, as they did not have enough time to explain the name and purpose of the medication:
The doctors in SOPD clinics are in a rush: they just write the precription and give it to you. They never give the name of the medication or what it is for. (P20, 65-year-old male Fijian of Indian descent)
Knowledge of prescribed medication also includes dosage. Patients who had better knowledge of their dosage were more compliant than those who had little or no knowledge.
A few participants stated that they did not know their dosage, as they were not very well educated:
I do not know the dosage of my medication . . . I just went to school till class 2 and I do not know English, so I do not know what’s written on the label. (P6, 34-year-old male i-Taukei)
Theme 2: Negative Attitudes
The desire to be healthy depends on a patient’s attitude toward their medication compliance. A few participants stated that they did not take their tablets, because they were healthy and they were able to do their daily activities effectively. They also mentioned that they would not die early if they did not take the medication every day:
I don’t take my tablets daily because I’m healthy and I’m able to do my household duties. (P3, 80-year-old female Fijian of Indian descent)
Another patient stated:
I won’t die early, so I do not take my tablets daily. (P2, 46-year-old male i-Taukei)
Another participant revealed that he was not compliant with his medication, as he had seen the world and eventually had to die one day:
I do not take my tablets everyday, as eventually I have to die one day, and I have seen the world in these 67 years of my life. (P10, 67-year-old male Fijian of Indian descent)
Patient attitudes are a significant predictor of health-related behavior, including medication adherence. Patients’ beliefs about treatment have a significant effect on prescription-medication use. This study showed that a majority of the study group lacked belief in the medication that had been prescribed to them, and some had negative behavior regarding their medication. A few mentioned that their tablets were not helping to improve their symptoms. One mentioned that she occasionally skipped doses because she did not feel the drug was helping her, despite taking it daily:
Sometimes, I feel the tablet is not helping me, despite taking it every day . . . and because of this feeling I skip my tablets sometimes. (P14, 75-year-old female i-Taukei)
Theme 3: Poor Family Support
Support from family members is another factor in medication compliance. A few participants mentioned that lack of family support was the cause of their noncompliance. One stated that her husband did not give her any money to get to the SOPD clinic and sent her to hospital only when she was sick:
My husband is not sending me to the clinic and doesn’t give me money to travel there . . . he tells me to go to hospital only when I’m sick and not for the clinic. (P5, 51-year-old female i-Taukei)
Another patient revealed that her family was not supportive of her health and did not buy her medication if it out of stock at the hospital pharmacy:
My family is not very supportive . . . they do not understand my heart condition. They do not buy me the tablets if I can’t get it from the hospital pharmacy. (P11, 45-year-old female i-Taukei)
Theme 4: Financial Constraints
There is a strong link between socioeconomic status and medication compliance. Many patients were noncompliance due to poor financial status. One mentioned that he could not work due to his heart problem, and thus depended on social welfare to feed his family. When he could not get his medication from the hospital pharmacy, he could not afford to buy it himself.
Due to my heart problem I cannot work . . . I depend on the money given by social welfare . . . so when I don’t get the supply from the hospital pharmacy, I can’t afford to buy from a pharmacy in town, as I have to feed my family from the money I get from social welfare. (P2, 46-year-old male i-Taukei)
Theme 5: Forgetfulness
One of the most common reasons given by participants for being noncompliant with cardiac medication was being forgetful. One stated that she often forgets to take her medication because of her household chores:
Sometimes I get so busy with the house work, I forget to take my tablets. (P4, 71-year-old female Fijian of Indian descent)
Another participant revealed that at times she misses her dose as she forgets it:
Sometime I miss my tablets . . . because I forget to take them. (P11, 45-year-old female i-Taukei)
Theme 6: Irregular Clinic Attendance
Clinic attendance is often related to medication non compliance. Those patients who miss clinic appointments usually run short of medication, and thus do not take the medication. A participant mentioned that he was not attending the clinic as he had lost his clinic card and being fearful of nurses’ anger:
I lost my clinic card in April last year. Since then, I’ve not attended SOPD clinics . . . I didn’t want to come, because the nurse in SOPD gets angry and tells us off for losing our card. (P13, 64-year-old male i-Taukei)
Another participant stated that due to transportation issues, he had missed clinic appointments as he could not travel on the bus because of his medical condition:
Sometimes I miss my appointments . . . when I don’t have any transport. This is because of my condition — I cannot travel on the bus. (P22, 75-year-old male Fijian of Indian descent)
Theme 7: Heavy Alcohol Use
Alcohol misuse has a number of potential psychological, legal, and health complications, including medication nonadherence. A few patients agreed that alcohol use had affected their usual schedule of cardiac medication intake. One mentioned that he did not consume his tablet when he drank alcohol, because he thought it might react with his tablets:
Whenever I drink alcohol, I don’t take my tablets. I’m afraid the tablets might react with alcohol. (P21, 56-year-old male Fijian of Indian descent)
Another participant revealed that when he drank alcohol, he did not take his tablets, as he knew taking tablets with alcohol would not be of any benefit:
The doctor told me not to drink alcohol, but sometimes I have a few drinks with my friends to relax a bit . . . when I drink alcohol, I don’t take my tablets . . . I know the tablets will not work if I take them with alcohol. (P20, 65-year-old male Fijian of Indian descent)
Theme 8: Alternative Treatment vs Pharmaceutical Medication
Herbal medicine is considered by many to offer a substitute for treatment of various diseases, particularly such lifestyle illnesses as noncommunicable diseases, that require lifelong pharmaceutical medication and thus raise safety concerns. One participant stated that they did not take their medication when they took herbal medicine, as herbal medicine worked for them.
I do not take my medication when I take herbal medicine . . . yup, herbal medicine works for me. (P11, 45-year-old female i-Taukei)
On the other hand, a patient stated that he had stopped taking his medication for his heart condition when he saw something on Facebook regarding how to avoid bypass surgery, so he had being taking herbal medication since then.
You know, doctor? I saw this thing on Facebook last week — you should also advise your patients to use it too . . . it showed things I can use to avoid heart-bypass surgery . . . I have been doing it, and stopped taking my medicine for my heart problem. (P20, 65-year-old male Fijian of Indian descent)
Discussion
Factors identified as patient-related were scarcity of knowledge, negative attitudes, lackof/poor family support, low socioeconomic status, forgetfulness, clinic nonattendance, heavy alcohol use, and herbal medicine/alternative treatment vs pharmaceutical medication.
Knowledge of prescribed medication is vital for adherence. It was revealed from this study that many patients lacked knowledge of their cardiac medication. Some of them did not know the names or dosage of their medication, while some were able to identify the dosage (number of tablets) by looking at the color and size of the tablets. The results of this study are in line with a cross-sectional study conducted at the Mazandaran Heart Center in Iran to evaluate predictors of medication adherence among patients with HF. A total of 300 patients who were hospitalized with HF were included. Education had a significant effect on medication compliance (p=0.012); however age, sex, employment status, place of residence, income, and number of hospitalizations were insignificant.15
A randomized controlled trial to determine the effect of health literacy on medication adherence in pharmacy-based intervention for HF patients also supported the findings of recent studies. Electronic prescription container monitors on cardiovascular drugs were used over 9 months to assess medication compliance. They showed that 69.4% of patients with adequate literacy had greater adherence to medication than the 54.2% with inadequate literacy from the usual-care group, which was similar to this study. Medication adherence in the intervention group was not significantly different between the groups of patients with adequate and inadequate health literacy. The association between health literacy and adherence was supported by multivariate analysis.16 These findings were similar to a recent study in which patients with inadequate knowledge about medication and cardiovascular diseases had poor compliance with medication.
This study also found that a few participants lacked motivation to be healthy, while others described a strong motivation to be as healthy as they could, to stay out of hospital, and to preserve a good quality of life. The same has been found in another study that showed the primary motivator for medication compliance among patients was the desire to be healthy. The process of making connections boosted medication compliance. Patients with good knowledge of their illness and symptoms stated that prescribed medication helped them relieve those symptoms. Relationships of the patient with the health-care provider and family members also boosted medication adherence.17
Noncompliance with prescribed medication is thought to result in frequent hospitalization and even premature deaths. CHF-related hospital admissions are often preventable. Some participants believed that the medication they were on did not have any benefits for their cardiac conditions, similar to the findings of a 5-year randomized study in Sweden. That was done to understand adherence to medication of congestive HF patients. Overall, 94% of 302 HF patients at baseline stated that they felt better when they took the study medication, which was either carvedilol or metoprolol. It was demonstrated that patient experience of medication impact on functional ability, symptoms, and well-being may be related to belief in medication.18
Patients with cardiac diseases, such as HF, need motivation in their daily lives. Poor social support often leads to poor medication compliance. This is often behavior-related, which is observed in patients with cardiac diseases, and poor compliance results from patient-related factors and other factors external to them. Some participants mentioned that they lacked social support from family members in management of their cardiac condition. Some reasons stated were an uncooperative partner, son staying with his own family separately, children busy with their work schedules, and not being accompanied to the SOPD clinic. A prospective study was done on 134 patients with HF to determine factors contributing to medication compliance. The results showed that ethnicity and perceived social support predicted dose count and financial status, perceived social support predicted dose day, and financial status predicted dose time.19
The finding of lack of family support being a factor in noncompliance is supported by another study in Philadelphia evaluating the effects of social support among patients with HF and whether aspects of social support were associated with self-care, including medication adherence, dietary adherence, and HF-symptom monitoring. The sample comprised 74 HF patients from cardiology clinics of a Veterans Affairs Medical Center and a university-affiliated hospital. Relationships between social support and patient self-care were tested. Family members, especially spouses, were often involved in the medical care of older adult patients with chronic HF, and provided a range of levels of support to patients. Self-care was generally poor in many HF patients. Social support was generally associated with better self-reported medication, dietary adherence, and other aspects of self-care, such as daily weigh-ins.20
Socioeconomic status played an important role in medication adherence of patients with cardiac conditions. Many participants were unemployed. Some were relying on social welfare assistance for their daily living, and could not afford to buy their medication if it were not available at the public hospital pharmacy. Other unemployed participants had financial support from their family members, who were buying their medication. These findings were similar to a study done in Nigeria that revealed lack of finances and side effects of medication accounted for 23.8% and 16.2% of noncompliance, respectively.21
Another prospective study was done in central Kentucky to determine factors contributing to medication compliance in patients with HF. Medication adherence was measured objectively using the medication event–monitoring system for 3 months. This system was used to assess three indicators of adherence: dose count, ie, percentage of prescribed doses taken; dose days, ie,percentage of days the correct number of doses were taken; and dose-time, ie, percentage of doses that were taken on schedule. Barriers to medication adherence, ethnicity, and perceived social support predicted dose count (p<0.001). New York Heart Association functional class, barriers to medication adherence, financial status, and perceived social support predicted dose days (p<0.001), and barriers to medication adherence and financial status predicted dose time (p=0.005),19 similar to a recent study.
A majority of the participants in this study mentioned that one of the factors contributing to their noncompliance was forgetfulness. Many patients forgot to take their medication, ie, either they missed one dose during the day or they missed the whole day’s doses. Forgetfulness was noted in all age-groupp. To develop interventions to enhance compliance with cardiovascular medication, more insight is needed into the complex character of medication nonadherence. A cross-sectional study by showed that experiencing difficulties with medication use due to forgetting, insufficient knowledge on what to do when a dose is forgotten, and an ambivalent attitude toward medicines (beliefs of high necessity and high concerns) were some of the factors involved in noncompliance with cardiovascular medication that were identified from this study.22
A pilot interventional study in the US showed poor medication compliance before the intervention, but significant improvement from preintervention to postintervention. It was concluded that a pictorial medication sheet improved medication adherence in complex medication regimens. This intervention could be used by patients of a recent study to increase compliance with medication.23
Our study showed that most participants were not attending regular follow-up. Reasons for missing appointments were lost clinic cards, finances (transportation), poor family support, and forgetting appointment dates. A cohort study conducted by van Der Wal et al revealed that 72% of HF patients were compliant with their management. The authors found that >90% of their study population were compliant with medication and appointments, in contrast to compliance with diet control (83%) and exercise (39%).9 The results of that study were different from this cohort study in that many participants were noncompliant with appointments and hence nonadherent to prescribed medication.
Care of HF patients involves a number of health-care providers, and thus can lead to discontinuity and fragmentation of care, which reduces trust and hence poorer medication adherence. Uijen et al explored HF patients’ experiences with continuity of care and the relationship to medication adherence. Overal, 53% of the patients mentioned that they had not seen any care provider in general practice in the last year regarding their HF, 25% had contacted a care provider in general practice, and 46% had contacted two or more care providers. Respectively, 38% and 51% of patients experienced the highest levels of team and cross-boundary continuity. Patients who had higher scores on personal continuity had significantly better medication adherence, which was also present in the current study.24
Some of the patients would drink a few glasses of alcohol to relax. This made them not take their medication, thinking it might react with the alcohol. A few of them knew that they would not get any benefits from the medication if it were taken with alcohol. Alcohol misuse is a modifiable risk factor for noncommunicable disease, and it has been associated with medication nonadherence. A randomized controlled trial done by Bryson showed that adherence to medication was generally lower in alcohol-misuse groups than nondrinkers. Alcohol misuse was associated with increased risk of medication nonadherence, which was also found in this current study.25
A common practice in Fiji is the use of herbal medication to treat chronic illnesses. Some participants mentioned that they were using herbal medication to treat their cardiac condition instead of the prescribed medication. The main reasons behind using herbal medication over prescribed medication are availability of medication at public hospital pharmacy and unaffordability of medication from a private pharmacy. There is a frequent and rapidly growing use of herbal medicine for cardiovascular disease. Sadik et al showed that herbal medication use was significantly associated with low medication adherence,26 which was also found in a recent study.
Interventions to improve adherence include reminders, reinforcement, and feedback on patient progress, education, reinforcement of cognitive cues through question–answer sessions, improvements in transportation to the clinic, waiting time; improvements in system variables, such as careful evaluation of the frequency of scheduled follow-up, and improvements in access to providers.27
Limitations
The results of this study cannot be generalized to all hospitals in Fiji, as it only focused on participants in Sigatoka. This study focused only on patients and their perceptions. It would have been preferable to include other groups, such as doctors, nurses, and pharmacists, but this was not done due to time limitations.
Conclusion
Medication adherence is a multidimensional behavior influenced by several factors. Therefore, care providers need first to identify these factors and then consider them in training and treatment planning for patients, in order to increase their medication compliance. Not all participants had all the factors on noncompliance. The enthusiasm from patients and caregivers was tempered by potential burdens, and this should be considered when designing interventions to promote adherence. The effectiveness of a treatment depends on both the efficacy of a medication and patient adherence to the therapeutic regimen. Patients, health-care providers, and health-care systems all have a role to play in improving medication adherence. A single method cannot improve adherence on its own, so a combination of various adherence techniques should be implemented to improve patient adherence to prescribed treatment. Providing professional counseling services to all SOPD patients would help greatly in increasing compliance with medication.
Acknowledgments
We would like to thank Dr Rufina Latu for her support and guidance. We express our sincere thanks to the patients who participated in this study and also to Sigatoka Hospital managers for allowing us to conduct this study at their hospital.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
2. World Life Expectancy.Coronary heart disease death rate by country (male). n.d. [updated March 11, 2019]. Available from: https://www.worldlifeexpectancy.com/cause-of-death/coronary-heart-disease/by-country/male.
3. Yuvaraj K, Gokul S, Sivaranjini K, et al. Prevalence of medication adherence and its associated factors among patients with noncommunicable disease in rural Puducherry, South India – a facility-based cross-sectional study. J Family Med Prim Care. 2021;8(2):701. doi:10.4103/jfmpc.jfmpc_350_18
4. Jimmy B, Jose J. Patient Medication Adherence: Measures in Daily Practice. Oman Med J. 2011;26(3):155–159. doi:10.5001/omj.2011.38
5. Ruppar TM, Cooper PS, Mehr DR, Delgado JM, Dunbar‐Jacob JM. Medication adherence interventions improve heart failure mortality and readmission rates: systematic review and meta‐analysis of controlled trials. J Am Heart Assoc. 2016;5(6). doi:10.1161/jaha.115.002606
6. NCD Alliance.Bridging the Gap on NCDs: From global promises to local. [updated April 8, 2019]. Available from: https://ncdalliance.org/resources/bridging-the-gap-on-ncds-from-global-promises-to-local-progress-policy-brief.
7. Wu J, Lennie TA, Chung ML, et al. Medication adherence mediates the relationship between marital status and cardiac event-free survival in patients with heart failure. Heart Lung. 2012;41(2):107–114. doi:10.1016/j.hrtlng.2011.09.009
8. Martin U. 2018. Non adherence-the elephant in the room.
9. van Der Wal MH, Jaarsma T, Moser DK, Veeger NJ, Gilst WH, Veldhuisen DJ. Compliance in heart failure patients: the importance of knowledge and beliefs. Eur Heart J. 2005;27(4):434–440. doi:10.1093/eurheartj/ehi603
10. Health.gov.fj. 2018. Ministry of Health, World Health Organization statement on ncd rates in fiji – ministry of health & medical services. Available from: http://www.health.gov.fj/ministry-of-health-world-health-organization-statement-on-ncd-rates-in-fiji/.
11. Rehman ZU, Siddiqui AK, Karim M, Majeed H, Hashim M. Medication non-adherence among patients with heart failure. Cureus. 2019. doi:10.7759/cureus.5346
12. Nakajima R, Nakamura K, Turagabeci A, Takano T. Barriers to medication adherence among patients with non-communicable diseases: Fijian health professional’s perceptions. J Int Health. 2014;29(4):313–320.
13. DeJonckheere M, Vaughn L. Semistructured interviewing in primary care research: a balance of relationship and rigour. Fam Med Community Health. 2019;7(2):e000057. doi:10.1136/fmch-2018-000057
14. Caulfield J. How to do thematic analysis | a step-by-step guide & examples; 2019 [updated January 20, 2020] Available from: https://www.scribbr.com/methodology/thematic-analysis//.
15. Shafipour V, Amininasab S, Lolaty H, Moosazadeh M. Medication adherence and its predictors among patients with heart failure. Nurs Midwifery Stud. 2018;7(2):81. doi:10.4103/nms.nms_9_17
16. Noureldin M, Plake KS, Morrow DG, Tu W, Wu J, Murray MD. Effect of health literacy on drug adherence in patients with heart failure. Pharmacotherapy. 2012;32(9):819–826. doi:10.1002/j.1875-9114.2012.01109.x
17. Wu J, Reilly CM, Holland J, Higgins M, Clark PC, Dunbar SB. Relationship of health literacy of heart failure patients and their family members on heart failure knowledge and self-care. J Fam Nurs. 2017;23(1):116–137. doi:10.1177/1074840716684808
18. Ekman I, Andersson G, Boman K, et al. Adherence and perception of medication in patients with chronic heart failure during a five-year randomised trial. Patient Educ Couns. 2006;61(3):348–353. doi:10.1016/j.pec.2005.04.005
19. Wu J, Moser D, Chung M, Lennie T. Predictors of medication adherence using a multidimensional adherence model in patients with heart failure. J Card Fail. 2008;14(7):603–614. doi:10.1016/j.cardfail.2008.02.011
20. Sayers SL, Riegel B, Pawlowski S, Coyne JC, Samaha FF. Social Support and self-care of patients with heart failure. Ann Behav Med. 2008;35(1):70–79. doi:10.1007/s12160-007-9003-x
21. Amira CO, Okubadejo NU. Factors influencing non-compliance with anti-hypertensive drug therapy in Nigerians. Niger Postgrad Med J. 2007;14(4):325–9.
22. Laan DM, Elders PJ, Boons CC, Nijpels G, Hugtenburg JG. Factors associated with nonadherence to cardiovascular medications. J Cardiovasc Nurs. 2019;34(4):344–352. doi:10.1097/jcn.0000000000000582
23. Hawkins LA, Firek CJ. Testing a novel pictorial medication sheet to improve adherence in veterans with heart failure and cognitive impairment. Heart Lung. 2014;43(6):486–493. doi:10.1016/j.hrtlng.2014.05.003
24. Uijen A, Bosch M, Van den bosch W, Bor H, Wensing M, Schers H. Heart failure patients’ experiences with continuity of care and its relation to medication adherence: a cross-sectional study. BMC Fam Pract. 2012;13(1):1–7. doi:10.1186/1471-2296-13-86
25. Bryson CL, Anu AH, Sun H, Williams EC, Kivlahan DR, Bradley KA. Alcohol screening scores and medication nonadherence. Ann Intern Med. 2008;149(11)795–804. doi:10.7326/0003-4819-149-11-200812020-00004
26. Sadik A, Yousif M, Mcelnay JC. Pharmaceutical care of patients with heart failure. Br J Clin Pharmacol. 2005;60(2):183–193. doi:10.1111/j.1365-2125.2005.02387.x
27. Koçer A, Ince N, Koçer E, Taşçı A. Factors influencing treatment compliance among Turkish people at risk for stroke. J Prim Prev. 2006;27(1):81–89. doi:10.1007/s10935-005-0020-x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.