")
Back to Journals » Patient Preference and Adherence » Volume 17
Patients’ and Healthcare Professionals’ Perspectives on Preoperative Informed Consent Procedure Obstacles and Potential Solutions, 2021: A Qualitative Study
Authors Negash T , Teshome D , Fenta E , Belete K , Fentie Y , Mequanint A, Tesfaw A , Ayele TT, Fentie F, Daniel T, Oumer KE
Received 7 June 2023
Accepted for publication 9 September 2023
Published 19 September 2023 Volume 2023:17 Pages 2343—2351
DOI https://doi.org/10.2147/PPA.S421256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Tadese Negash,1 Diriba Teshome,1 Efrem Fenta,1 Kumlachew Belete,1 Yewlsew Fentie,1 Aderajew Mequanint,2 Aragaw Tesfaw,3 Tamiru Tilahun Ayele,4 Fissiha Fentie,5 Tenbite Daniel,5 Keder Essa Oumer1
1Department of Anesthesia, School of Medicine, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Surgery, School of Medicine, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 3School of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 4Department of Anesthesia, College of Health Sciences, Wolkite University, Wolkite, Ethiopia; 5Department of Anesthesia, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Tadese Negash, Email [email protected]
Background: Informed consent discussions are individualized not only with regard to the patients’ surgical condition and goals but also with their varying information needs, health literacy, and anxiety. Information is lacking regarding the views of patients and concerned healthcare professionals on the informed consent process.
Objective: This study is aimed to explore patients’ and healthcare professionals’ perceived barriers during informed consent process and identify suggested solutions for improvement.
Methods: Patients who underwent elective surgery, anesthetists, and surgeons were the subjects of a qualitative study employing focused group discussions and in-depth interviews. The study participants were chosen through the use of purposeful sampling.
Results: The main barriers identified by the patients include: inadequate explanation about the intended procedure, family’s influence in the decision-making, fear of surgery, fear of light/power interruption, inadequate time for discussion, and not letting the family members attend the discussion. On the other hand, healthcare professionals also identified various barriers, which includes: inability of patients to understand the information, limited time to discuss with patients in detail, poorly designed informed consent form, poor awareness of patients, fear of patient refusal for surgery if the risks and associated health problems are explained, lack of adequate investigation to confidently explain about the disease condition, use of medical jargons, poor documentation habit of professionals and lack of legal system regarding ethical dilemmas.
Conclusions and Recommendation: Patients and healthcare professionals have identified avoidable barriers that need the attention of concerned health professionals, educators, and the healthcare delivery system.
Keywords: anesthesia, barriers, informed consent, preoperative, surgery
Introduction
Informed consent is a process by which the treating healthcare professional discloses appropriate information to a competent patient so that the patient may make a voluntary choice to accept or refuse treatment.1 It is a fundamental principle in health care that guarantees the care received represents the patient’s goals, preferences, and values by allowing them to participate in the decision-making process.2–5 In informed consent, healthcare professionals have an obligation to disclose facts to the patient’s level of understanding in order for them to make a right decision.5–7 In other words, it refers to the entire complex process of gathering information, making decisions, and consenting, rather than a single instant of agreement.1,7,8
It is better to think of informed consent as a process rather than an event. Throughout the patient’s care, there is an ongoing communication between the patient and healthcare providers. It all starts with a preoperative evaluation and continues with surgery and postoperative care.5,9–11 No patient can be coerced, directly or indirectly, to accept therapy that he/she may refuse, even if it is painless, useful, without danger, or even life threatening.5,12,13 Informed consent, in addition to the law, is a cornerstone of medical ethics and surgical practice because it allows patients’ autonomy and dignity to be respected.5,9 In short, it is an essential ethical and legal requirement in medical practice.
The three fundamental criteria required for informed consent to be valid are that the patient must be competent, adequately informed and not coerced. They must have the capacity to be able to understand and assess the information given, communicate their choices, and understand the consequences of their decision. The physician must provide adequate information, with a minimum being the diagnosis, the procedure with its risks, benefits, and the alternatives, along with their benefits and risks including doing nothing. The decision must be voluntary.1,14 The fourth criteria is that the informed consent procedure should be conducted in an appropriate environment and time in order to maximize patient’s comfort for informed decision.
The appropriate environment for obtaining informed consent for surgery is a private and confidential space where the patient can freely communicate with the healthcare provider without any interruptions. This ensures that the patient can ask questions, express concerns, and receive detailed explanations about the surgical procedure. Regarding the timing of obtaining informed consent, it should be done well in advance of the scheduled surgery. Sufficient time should be given to the patient to review the provided information, discuss it with their family or trusted individuals, seek a second opinion if desired, and make an informed decision without feeling rushed or pressured.15
In most countries, a competent individual aged 18 or older can give legally binding informed consent to the proposed procedure. Patients who are less than 18 years without capacity cannot consent themselves. In this case, surrogates or care givers or family members could give consent on behalf of incapacitated individuals.5,7,9
Inappropriate informed consent (IC) can lead to a legal claim to the HCPs where the patient can prevail even if the basis for negligence is weak. Thus, a better understanding of the informed consent process benefits both patients and healthcare professionals (HCPs) in patient-centered practice. As a result, it is critical that the consents obtained are legally genuine and cover all aspects of an Informed Consent Process (ICP).5,12
Since the medico-legal requirement concerns the HCPs’ interest more than the information component, it is feared that HCPs may secure documentation of ICP without genuinely ensuring that the patient has received and understood the relevant information. Currently, Compassionated, Respectful and Caring (CRC) healthcare practice is being advocated by the Ministry of Health.5,16,17 As part of CRC, the success of the informed consent process in meeting the patients’ needs and rights, as well as the patients’ own perceptions of how the process should be, is a critical component of surgical patient care.
On the other hand, informed consent and how it should be obtained gained more attention as a result of rising medico-legal litigation and a desire to offer patients greater autonomy over their treatment. A patient requires accurate information in order to make an informed decision about his or her own treatment.5,15
However, paternalistic medical approaches, varying patient health literacy, a minimal emphasis on medical ethics education, high patient flow, time constraints, a lack of documented information sheets, and language and cultural differences are some of the common barriers to obtaining satisfactory preoperative informed consent.5,6,18 Furthermore, most preoperative informed consent are obtained by junior staff or staff who are not members of the surgical team through oral disclosure of information and are unlikely to have the necessary experience in dealing with the many potential ramifications that may arise during the informed consent process.12,19 On the other hand, HCPs may think that telling patients about possible complications would discourage them from going ahead with surgery.5,6 Therefore, keeping these factors in mind, it is essential to formally explore the views of patients’ and HCPs on the practice of informed consent process. From our observation, there are patients who refused the proposed procedure or type of anesthesia possibly because of inappropriate information disclosure. This can lead to the complication and/or death of patient related to the disease, which could have been treated if they have agreed and consented for the proposed surgery.
The process of informed consent requires expertise in counseling patients to the level of their understanding, allocating adequate time, building trust and recommendation by the responsible health professionals.6,20 Because of fear of litigation, some health professionals hesitate in providing a recommendation to their patients to help with surgical decision-making leading to increased difficulty by patients during the decision-making process. Despite the above constraints in the practice of obtaining informed consent, information is not available on patients’ and HCPs views and perceived barriers in the informed consent process in our setting. The aim of this study is therefore, to assess perceived barriers and suggested solutions in the informed consent process from patients’ and HCPs perspectives.
Methods
Study Design
A qualitative study using in-depth interview, focused group discussion, and thematic analysis was employed on elective surgical patients and concerned healthcare professionals.
Source Population
All surgical patients and HCPs (Surgeons, Anesthetists, and Gynecologists/Obstetricians) working in Debre Tabor Comprehensive Specialized Hospital.
Study Population
Surgical patients who underwent elective surgery, Surgeons, Anesthetists, and Gynecologists/Obstetricians.
Study Variables
Patients and HCPs perceived barriers and suggested solutions in preoperative informed consent process were considered as dependent variables. Socio-demographic factors such as: sex, age, residency, religion, educational level, marital status, income, and clinical factors including: diagnosis, ASA physical status, type of surgery, repetition of surgery and type of anesthesia were considered as independent variables.
Sample Size
We estimated to conduct 15 in-depth interviews and four Focussed Group Discussions. However, using the theory of saturation of information from patients’ and HCPs perspectives, twelve patients were participated on the in-depth interview and two FGDs; one with surgeons (composed of general surgeons, orthopedic surgeons and gynecologists/obstetricians), and one with anesthesia professionals.
Sampling Technique
Purposive sampling technique was used to select study participants, surgeons, Gynecologists/obstetricians, and anesthetists based on their years of service and educational qualifications.
Eligibility Criteria
Inclusion Criteria
Postoperative surgical patients and HCPs with more than 2 years work experience (surgeons, Gynecologists/obstetricians, and anesthetists).
Exclusion Criteria
Patients with critical illness, age less than 18 years old, minor surgeries, patients’ known mental illness and geriatric patients (age >65 years) were excluded from the study. HCPs who have less than 2-year experience and/or who were not providing clinical service during the study period were excluded from the study.
Data Collection Technique
In-depth interviews and FGDs were used with interview guide to collect data. Interview themes/questions were focused on the perceived barriers and possible solutions on the informed consent process. Data were collected by experienced data collectors in qualitative research. Data from patients were collected within the first week of postoperative period before discharge.
Data Quality Assurance
A variety of quality control measures were employed to ensure the trustworthiness of the study findings. Interview guide was developed by the research team following a thorough literature review and initial key informant interviews. Training was given for the data collectors, and the tool was pretested. Then we reviewed our data collection instruments for the main research data collection. Daily briefings were held, and locations for safe, quiet, and wind-free data collection were chosen. All interviews were recorded on tape, and in the case that the audio recorder failed to capture everything said during the interviews, suitable written notes were also collected. The interview process was carried out until the data became idea-saturated. Through repeated listening to the audio recorded data, thorough understanding and internalization of the recorded data were accomplished throughout data transcription. Daily briefing, selection of safe, silent, and wind-free data collection place were conducted.
Data Analysis
Upon completion of each interview, a complete transcript with clean verbatim was produced in Amharic then translated to English. The interviewer read and reviewed carefully the transcribed data to ensure that they are clear and compared the transcriptions with the original audio recordings for accuracy and consistency. Then line-by-line coding was made with the assistance of Open Code version 4.02 software. Thematic analysis was made by coding or dividing the text into meaningful elements, and the results were narrated using sample quotes.
Results
Twelve patients from general surgery, orthopedics, and gynecology/obstetrics departments participated in the in-depth interview (Table 1), and two FGDs were conducted on HCPs in this study.
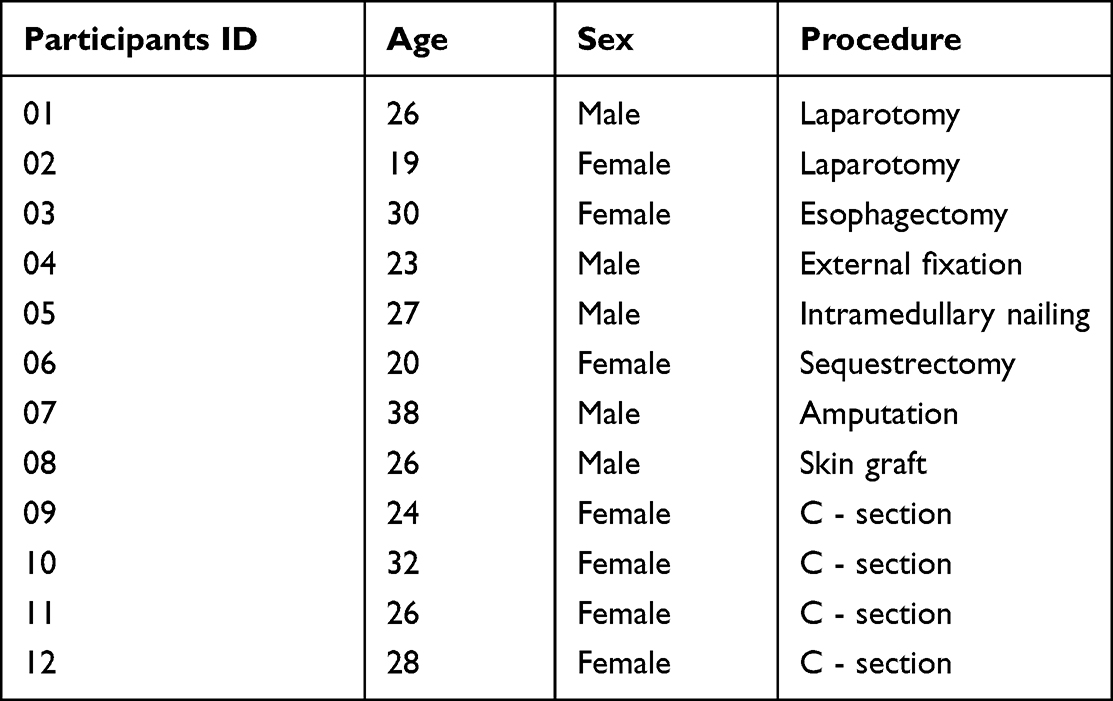 |
Table 1 Socio-Demographic and Clinical Characteristics of the Study Participants |
Barriers During Preoperative Informed Consent Process from Patients’ Perspective
Almost all the study participants identified that inadequate explanation about the intended procedure as a main barrier during the ICP.
They (HCPs) didn’t give me any information about the planned surgery but they said that just you have to sign to confirm your agreement for anesthesia and surgery. I agreed and consented because it was not more than the bullet injury I am suffering. This was the only problem of the doctors. I understand that they are very busy ….. (A 27-year-old male patient who had intramedullary nailing)
The other participant explained lack of adequate information for consent as
They asked me to sign on the consent form. I signed with fingerprint after discussing with myself. No one told me why and how my finger should be cut….. (A 38 year-old male patient who underwent amputation)
The other frequently raised barrier by participants was the interference of family members on the decision of the patient. Some family members intend to decide on behalf of the patient. The following barriers were also identified by the participants: anxiety, fear of light/power interruption during surgery, inadequate time for discussion, and not letting the family members during ICP.
Suggested Solutions by Patients
Most of the participants suggested HCPs to provide adequate information both for the patient and the family members, understanding patient’s condition (eg, anxiety and pain) and providing adequate time to discuss with family members and decide.
… so, information has to be given for the patient as well as for the family. Patient should sign voluntarily and the family should be available (a 26-year-old male patient who underwent external fixation of left leg)
Barriers During Informed Consent Process from HCPs Perspectives
We conducted one FGD with general surgeons, orthopedic surgeons, and gynecologists/obstetricians (2 participants from each). The discussion took 48 minutes. We omitted the sociodemographic data of the participants to insure confidentiality.
Various challenges and solutions were discussed in detail with the study participants. The main barriers identified by the participants frequently include: inability of patients to understand the information, limited time to explain the risks and benefits of planned procedure, poor written informed consent form, poor awareness of patients/community about surgery, fear of patient refusal for surgery if risks explained and associated health problems, lack of adequate investigations to confidently explain about the disease, poor documentation habit of HCPs, lack of legal system that help HCPs during difficult situations like in ethical dilemmas, lack of attention by HCPs for the informed consent process and related consequences, fear of patients to request the proposed procedure if they changed their mind after refusal for the procedure and informed consent being obtained by not the operating/senior surgeon.
Fear of patient refusal for surgery if we explained the risks of operation. Lack of time during emergency conditions. The consent form is very short and it does not give adequate information. You can tell them orally but they can deny later in case any complication happens. (gyn/obs specialist)
The proposed solutions by the participants include: creating awareness for patients, HCPs, and for the community using different media, providing adequate time for the patients to discuss and decide, establishing a legal system that supports HCPs when they encounter ethical dilemmas, being a role model for students, the operating/senior surgeon should be available during informed consent process, HCPs need to be patient friendly and explain risks and benefits carefully considering the level of health literacy and documenting the information delivered.
Regrading patients; we need to give them health education, the media also should give coverage to create awareness (TV & radio), and health extensions also need to work on this issue to improve health literacy. The legal issue needs great emphasis especially for incapacitated patients. In our setup we let go the patient if the proxy of the incapacitated patient is refused to consent. But ideally the medical board or legal support can decide to proceed for the surgery. But no one is doing this method in our set up. Regarding medical ethics education there is improvement in medical education. There are different courses on ethical issues. But theory could not improve the performance of future graduates. So, we need to be exemplary during our practice. (One of the general surgeons)
Similarly, we conducted another FGD with anesthesia professionals, which took 50 minutes duration. The main barriers raised by anesthetists include: use of medical jargons, fear of patient refusal, cultural and family influences on patients’ decision, inability of HCPs to check whether the patient has understood the given explanation, lack of standardized informed consent form, poor awareness of patients about anesthesia, inability of HCPs to explain risks and benefits of proposed anesthesia plan, urgency of procedure/shortage of time, inability to understand patients’ condition (lack of empathy), fatigue of HCPs, and incapacitated patients to give consent.
Some professionals use informed consent as a frustration tool for the intention not to do the operation. This is lack of empathy … (participant III)
Even though I know the risks of having the operation I ignore letting the patient know the risks due to fear of patient understanding. I do have one experience regarding informed consent; one of my patients refused to take spinal anesthesia, then I told him some of the minor side effects of general anesthesia and obtained informed consent for GA. Then, I gave him GA as per his request. Unfortunately, he developed severe complications during the operation. It was very difficult if he died or had severe consequence (participant III)
The anesthetists also suggested the following solutions: creating awareness to patient, anesthesia professionals, and community about informed consent process
Patients may perceive that signing informed consent is agreeing for death (providing adequate explanation to the patients’ level of understanding). It is also important to improve the attitude of professionals regarding informed consent.
Doing audit on the practice of informed consent to identify gaps, developing standardized informed consent form, providing training for anesthetists to bridge knowledge gap and improve documentation of conversations.
… as a result, better to understand patients’ disease condition and explain the information to their level of understanding …. (Participant II)
… so, based on this experience I learnt that we should not only explain the risks and benefits, but also, we have to document our conversations to avoid ethical and legal problems related to anesthesia. (Participant III)
Discussion
In this study, most of patients identified the following barriers during preoperative informed consent process. These include: inadequate explanation about the intended procedure, family’s influence in the decision-making process, fear of surgery, fear of light/power interruption, inadequate time for discussion, and not letting the family members attend the discussion. Most of the participants suggested HCPs to provide adequate information regarding the procedure both for the patient and the family members, understanding patient’s condition (eg, anxiety and pain) and give adequate time to discuss with family members and let the patient decide by themselves.
Similar qualitative study conducted on Sri Lankan patients to identify the different perceptions of surgical patients on the informed surgical consent revealed that giving consent for surgery was a collaborative effort between the patient, family members, and the physician, rather than a decision made only by the patient. Some patients avoided asking doctors questions because they were “busy”, “short-tempered”, or “stressed out.” Some people believe that nurses are more approachable than doctors. Patients stated that having a bystander there during the consent process would help them relax. Clinicians need to focus more on the postoperative lifestyle adjustments and pre-procedure counseling. Some proposed brochures or booklets can be handed to the patients at preanesthesia clinic to educate patients about their operation.21
Another study conducted in Auckland (New Zealand) to assess surgical patients’ perceptions of the adequacy of informed consent found that the senior doctor performing the procedure should provide more specific information (including the nature of the planned operation, alternatives, and complications) before the patient is admitted to hospital. This study has highlighted the need of validating that the patient believes they understand and are entirely satisfied with the information provided, as well as the capability to ask questions without feeling rushed. The study has also revealed where changes in this key part of patient care could be achieved by giving voice to our patients’ thoughts on the adequacy of the informed consent process.22–24
On the otherhand, Čebron et al found that paternalistic approach to medicine and patient education was the most common obstacle to getting informed consent. Lack of ethical education among surgeons in low- and middle-income countries, cultural perceptions about healthcare, and language issues between surgeons and patients were other common obstacles.6
In the current study, HCPs (surgeons and anesthetists) identified various challenges and solutions. The main barriers identified by HCPs include: inability of patients to understand information, limited time, poor written informed consent form, poor awareness of patients/community about surgery, fear of patient refusal for surgery if risks explained and associated health problem, lack of adequate investigation to confidently explain about the disease, use of medical jargons, poor documentation habit of HCPs, lack of legal system that help HCPs during difficult situations like in ethical dilemmas, lack of attention by HCPs for the informed consent process and related consequences, fear of patients to request the proposed procedure if they changed their mind after refusal for the procedure and informed consent being obtained by junior staff members. Some of the stated barriers are supported by a qualitative research done in the UK, which found shortage of time, inexperienced staff, and patients’ reluctance to be involved as a barrier to ICP.19
HCPs suggested that creating awareness for patients, HCPs, and for the community using different media, providing adequate time for the patients to discuss and decide, establishing a legal system that supports HCPs when they encounter ethical dilemmas, being a role model for students, the operating/senior surgeon needs to be available during informed consent process, HCPs need to be patient friendly and explain risks and benefits carefully considering the level of patients’ health literacy and documenting the information delivered.
This study implies that addressing the perspectives of both patients and healthcare professionals during informed consent for surgery and anesthesia fosters collaborative decision-making, promotes patient autonomy, improves satisfaction, and ensures efficient and effective healthcare delivery.
Conclusion
Patients and HCPs have identified avoidable barriers that need the attention of HCPs, health profession educators, and the healthcare delivery system in general. The health care providers need to implement the standard requirements of informed consent process to strengthen patient safety practice and keep the ethical norm of the informed consent process.
We recommend health care decision makers, patients and clinicians, health professions educators, and policymakers to give more emphasis on improving health outcomes, patient satisfaction, and better adherence to treatment recommendations, fewer malpractice claims, and reduced healthcare expenditure associated with informed consent process.
Abbreviations
ASA, American Society of Anesthesiologist; CRC, compassionate respectful care; FGD, focused group discussion; GA, General anesthesia; IC, informed consent; ICP, informed consent process; HCP, Health Care Professional.
Patients or Public Contribution
In this study patients who underwent elective surgery at the study hospital were participated voluntarily by providing information on their lived experience, challenges and possible solutions regarding the informed consent process. Similarly, purposely selected healthcare professionals working at the study site participated on the focused group discussion to share their experiences and insights.
Data Sharing Statement
The data sets of the current study are available from the corresponding author on reasonable request.
Ethical Clearance
The study was conducted in accordance with the World Medical Association Declaration of Helsinki – Ethical Principles for Medical Research involving human subjects, article number 23–26 which is amended in October 2013.25 Before beginning the study, we got an ethical approval letter from Debre Tabor University, College of Health Science Ethical Review Committee with reference number of CHS3399/2013, as well as permission letter was obtained from the hospital administrator after providing detailed information about the study’s objectives.
Data collectors obtained written informed consent from each patient and health professional All participants were informed that they have the right to withdraw from the study if they are uncomfortable. Participants’ norms, values, and morals were respected by data collectors during the data collection procedure.
Acknowledgment
We would like to acknowledge Debre Tabor University for providing financial support to conduct this study. Our thanks also go to Debre Tabor Comprehensive Specialized Hospital staffs, our data collectors, and study participants for their co-operation during data collection.
The descriptive (quantitative part) of this paper was published in Sage journal (Clinical Ethics): https://doi.org/10.1177/1477750921994281.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support to conduct this study was obtained from Debre Tabor University. However, the university has no role and/or influence on the study design, data collection, analysis and write-up of the study findings.
Disclosure
The authors report no competing of interests in this study.
References
1. Cocanour CS. Informed consent—It’s more than a signature on a piece of paper. Am J Surg. 2017;214(6):993–997. doi:10.1016/j.amjsurg.2017.09.015
2. Wheeler R. Consent in surgery. Ann R Coll Surg Engl. 2006;88(3):261–264. doi:10.1308/003588406X106315
3. Clark S, Mangram A, Ernest D, Lebron R, Peralta L. The informed consent: a study of the efficacy of informed consents and the associated role of language barriers. J Surg Educ. 2011;68(2):143–147. doi:10.1016/j.jsurg.2010.09.009
4. Sivanadarajah N, El-Daly I, Mamarelis G, Sohail M, Bates P. Informed consent and the readability of the written consent form. Ann R Coll Surg Engl. 2017;99(8):645–649. doi:10.1308/rcsann.2017.0188
5. Ayele TT, Negash TT, Mekuanint A, et al. Patients’ satisfaction and associated factors towards preoperative informed consent process: a cross-sectional study. Ann Med Surg. 2022;79:104104. doi:10.1016/j.amsu.2022.104104
6. Čebron U, Honeyman C, Berhane M, Patel V, Martin D, McGurk M. Barriers to obtaining informed consent on shortterm surgical missions. Plast Reconstr Surg Glob Open. 2020;8(5):e2823.
7. Taylor HA. Barriers to informed consent. In: Seminars in Oncology Nursing. Elsevier; 1999.
8. Adhikari P, Pradhananga RB. Patients’ expectations on informed consent before ENT surgery. Int Arch Otolaryngol. 2007;11:1–5.
9. Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006;141(1):86–92. doi:10.1001/archsurg.141.1.86
10. Kay R, Siriwardena A. The process of informed consent for urgent abdominal surgery. J Med Ethics. 2001;27(3):157–161. doi:10.1136/jme.27.3.157
11. Dixon-Woods M, Williams SJ, Jackson CJ, Akkad A, Kenyon S, Habiba M. Why do women consent to surgery, even when they do not want to? An interactionist and Bourdieusian analysis. Soc Sci Med. 2006;62(11):2742–2753. doi:10.1016/j.socscimed.2005.11.006
12. Goswami D, Agarwal SS, Vaishnav SB, Kumar L, Chavali KH. Audit of informed consent document for major surgical procedures at a tertiary care hospital. J Med Soc. 2019;33(2):91.
13. Jawaid M, Farhan M, Masood Z, Husnain S. Preoperative informed consent: is it truly informed? Iran J Public Health. 2012;41(9):25.
14. Negash W, Assefa N, Baraki N, Wilfong T. Practice and factors associated with informed consenting process for major surgical procedures among health-care workers, south eastern Ethiopia. Int J Gen Med. 2021;14:7807–7817. doi:10.2147/IJGM.S338243
15. Anderson OA, Wearne IMJ. Informed consent for elective surgery—what is best practice? J R Soc Med. 2007;100(2):97–100. doi:10.1177/014107680710000226
16. Abate M, Debie A, Tsehay CT, Amare T, Spradley FT. Compassionate and respectful care among outpatient clients at public health facilities in Northwest Ethiopia: a mixed-methods study. PLoS One. 2021;16(6):e0252444. doi:10.1371/journal.pone.0252444
17. Edmealem A, Tsegaye D, Andualem A, Ademe S, Gedamu S. Implementation of compassionate and respectful health care service at Northeast Ethiopia: patients’ perspective. Int J Care Caring. 2020;13(2):991–1003.
18. Jahan F, Roshan R, Nanji K, Sajwani U, Warsani S, Jaffer S. Factors affecting the process of obtaining informed consent to surgery among patients and relatives in a developing country: results from Pakistan. East Mediterr Health J. 2014;20(9):569–577. doi:10.26719/2014.20.9.569
19. Wood F, Martin SM, Carson‐Stevens A, Elwyn G, Precious E, Kinnersley P. Doctors’ perspectives of informed consent for non‐emergency surgical procedures: a qualitative interview study. Health Expect. 2016;19(3):751–761. doi:10.1111/hex.12258
20. Hanson M, Pitt D. Informed consent for surgery: risk discussion and documentation. Can J Surg. 2017;60(1):69. doi:10.1503/cjs.004816
21. Samaranayake UMJE, Mathangasinghe Y, Banagala ASK. Are predominantly western standards and expectations of informed consent in surgery applicable to all? A qualitative study in a tertiary care hospital in Sri Lanka. BMJ open. 2019;9(1):e025299. doi:10.1136/bmjopen-2018-025299
22. McKeague M, Windsor J. Patients’ perception of the adequacy of informed consent: a pilot study of elective general surgical patients in Auckland. N Z Med J. 2003;116(1170):U355.
23. Abitew DB, Worku A, Mulugeta A, Bazzano AN. Rural children remain more at risk of acute malnutrition following exit from community based management of acute malnutrition program in South Gondar Zone, Amhara Region, Ethiopia: a comparative cross-sectional study. PeerJ. 2020;8:e8419. doi:10.7717/peerj.8419
24. Caljouw M, Van Beuzekom M, Boer F. Patient’s satisfaction with perioperative care: development, validation, and application of a questionnaire. Br J Anaesth. 2008;100(5):637–644. doi:10.1093/bja/aen034
25. Association WM. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.