Back to Journals » Clinical Ophthalmology » Volume 11
Patient selection for corneal collagen cross-linking: an updated review
Authors Galvis V, Tello A ![]() , Ortiz AI
, Ortiz AI ![]() , Escaf LC
, Escaf LC ![]()
Received 4 January 2017
Accepted for publication 7 March 2017
Published 7 April 2017 Volume 2017:11 Pages 657—668
DOI https://doi.org/10.2147/OPTH.S101386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Virgilio Galvis,1–3 Alejandro Tello,1–3 Alvaro I Ortiz,3 Luis C Escaf2
1Centro Oftalmológico Virgilio Galvis, Floridablanca, 2Department of Ophthalmology, Faculty of Health Sciences, Universidad Autónoma de Bucaramanga, Bucaramanga, 3Department of Ophthalmology, Fundación Oftalmológica de Santander (FOSCAL), Floridablanca, Santander, Colombia
Abstract: Corneal cross-linking (CXL) is an option that in the last decade has demonstrated its efficacy and safety in halting the progression of keratoconus (KCN) and other corneal ectasias. Its indication has been extended beyond the classic definition that required evidence of KCN progression, especially in the presence of some risk factors for a possible progression (particularly the younger age). However, the results can be still somewhat variable today. There are several protocols, each with its own advantages and disadvantages. Some predictors of CXL outcome have been identified. We will review the current knowledge on patient selection for CXL, its indications, and options in special cases (such as thin corneas).
Keywords: keratoconus, cornea, cross-linking, corneal collagen cross-linking, keratoectasia
Introduction
Among corneal ectasias, primary forms include keratoconus (KCN) and pellucid marginal degeneration (PMD), while secondary ones occur as a late complication of Laser-Assisted In-Situ Keratomileusis (LASIK) or other refractive surgery procedures.1–6
Before the introduction of corneal cross-linking (CXL), there was no effective way in stopping corneal ectasias progression, which led to an important number of keratoplasties.7 Since its introduction in the late 1990s, CXL has been established as a mainstream treatment for ectasias with signs of progression with many studies showing good short-term results and some reporting good long-term results between 7 and 10 years after the procedure.8–14 However, Sykakis et al15 in a recent Cochrane Review, which included three randomized clinical trials, concluded that the evidence for the use of CXL in the management of KCN is limited due to the lack of properly designed and conducted studies. The three studies comprised 119 eyes undergoing CXL according to the Dresden protocol and 100 keratoconic eyes as controls, but all the three clinical trials were found to be at high risk for detection bias (only in one of the studies an attempt to mask outcome assessment was done), performance bias (absence of masking), and attrition bias (incomplete follow-up). In addition, it was not possible to pool data because of differences in measuring and reporting outcomes.16–18
CXL has also shown mixed results in the treatment of nonectatic disorders such as corneal infections, chemical burns, and bullous keratopathy.19,20–23 Those indications will not be included in this review.
Principles of corneal collagen cross-linking
The main objective of CXL is to achieve strengthening of corneal tissue as a means to stop further progression of corneal ectasia. In order to induce cross-links within and between collagen fibers of corneal stroma, long-wave ultraviolet A (UVA) radiation (370 nm) is used combined with a chromophore (riboflavin, vitamin B2). Riboflavin acts as photosensitizer that when exposed to UVA is excited, producing oxygen free radicals that initiate the creation of those new covalent bonds bridging the amino groups of collagen fibrils and possibly other corneal macromolecules such as proteoglycans and nucleic acids.24 This photopolymerization process results in the increased rigidity of corneal tissue.19,25,26
During late 1990s and early 2000s, several authors explored the use of riboflavin and UVA light in order to increase corneal stiffness in animal eyes, but a group of researchers from Dresden (Germany) were the ones who achieved the greatest breakthroughs at that moment.27,28 Wollensak et al,29 members of that group, in 2003 published the first in vivo study on 22 patients with progressive KCN, in which they documented a halted progression in all the cases and reduction of the maximal keratometry readings in around 70% of these cases.
Currently, CXL is an established procedure in managing progressive corneal ectatic disorders virtually all around the world; however, there is undoubtedly still much room for progress in improving the technique and the results of the procedure, in terms of reducing its invasiveness and increasing its safety profile and its stabilization effects.9,11,12,19
Current protocols
“Dresden protocol”: Epi-off CXL
It was named “Dresden protocol” because it was originally developed at the Technical University of Dresden (Dresden, Germany) by Wollensak et al.29 It is still considered to be the standard CXL treatment protocol. “Dresden protocol” includes removal of central 8–9 mm of epithelium, application of 0.1% riboflavin solution every 5 minutes for 30 minutes, followed by exposure to UVA (370 nm, 3 mW/cm2) for 30 minutes with the application of riboflavin solution every 5 minutes during exposure.29–31 Medium-term results (mean follow-up time between 6 and 26 months) have been shown to be good using this technique, in terms of safety and efficacy, as also shown in a recent meta-analysis.8,31–34 However, long-term results are less defined. The group of Dresden published 10-year results in 2015 and concluded that CXL achieved long-term stabilization of the condition in 34 eyes.12 Nevertheless, there are some concerns with regard to the quality of the data in that group of cases.35 Poli et al36 reported their results with 6 years of follow-up. CXL was effective in stabilizing KCN and other ectatic disorders, but had a long-term failure rate, in terms of progression, in 11% of the eyes. O’Brart et al11 also published their long-term (7 years) results in 2015 and concluded that improvements in both topographic and wavefront parameters found 1 year after the procedure continued to improve up to 5 years after the CXL and were maintained at 7 years. Not one of the 36 treated eyes progressed over the 7-year follow-up period.
Some groups have reported results using modifications, as partial deepithelization, suggesting also stabilization at short and medium term.37–39 However, it remains to be determined whether this approach would have any real advantage over the traditional “Dresden protocol.”
Other modification of the “Dresden protocol” included mechanical compression of the tissue by suturing a semiscleral rigid contact lens with a flat curvature (back surface radius of 11.0 mm) to the cornea after applying the riboflavin. Then, riboflavin was injected every 5 minutes under the contact lens during UVA irradiation, using a blunt cannula. Since the UV filter in the contact lens absorbed 11% of the UVA light, the irradiation time was increased to 34 minutes. The contact lens was left in place for 1 hour after the procedure. However, in spite of improving the corneal flattening effect, the results of this technique at 6 months were inferior compared to the standard “Dresden protocol.” A possible explanation could be the differences in the precorneal riboflavin film with the contact lens in place.40
Epi-on CXL technique
Initial studies showed limited diffusion of riboflavin (a large hydrophilic molecule with a molecular weight of 376.37 g/mol) through corneal epithelial tight junctions, thus reducing CXL effectiveness presented if this layer was not removed.30 Nevertheless, epithelial debridement is considered to be the major source of complications secondary to CXL like keratitis, persistent epithelial defect, and most frequently reported severe postoperative pain.41–43 Various techniques have been explored to solve this issue by adding chemical enhancers causing epithelial disruption of corneal epithelium, like the surfactant benzalkonium chloride (BAC) or ethylenediaminetetraacetic acid (EDTA). Wollensak and Iomdina44 performed the first experimental study using iso-osmolar riboflavin (20% dextran) +0.005% BAC, and it increased the biomechanical changes after cross-linking in comparison to a control group, also without removing the epithelium but using no BAC. However, as discussed later, the CXL without epithelial removal using BAC-containing proparacaine eye drops led to a biomechanical stiffening effect of only one-fifth of that induced by cross-linking according to the Dresden epi-off standard protocol.
Some providers of medical supplies offer different options of riboflavin for CXL. The company Avedro offers a particular formulation (ParaCel™, MedioCROSS TE, Avedro, Waltham, MA, USA [0.25% riboflavin, 1.2% hydroxypropyl methylcellulose, and 0.01% BAC]) for transepithelial epithelium-on technique. However, it is not clear if these transepithelial techniques, even with those special formulations of riboflavin, allow sufficient riboflavin absorption into the stroma to efficiently cause CXL. As mentioned, experimental studies with animal eyes by Wollensak and Iomdina44 suggested that disruption of the epithelial tight junctions with BAC prior to CXL increased corneal stiffness only by around one-fifth of what regular epi-off CXL can achieve. A study in porcine eyes treated with an epi-off technique versus a transepithelial protocol (using 0.02% BAC and 0.44% NaCl as enhancers of the penetration) showed that the latter was around 70% less effective.45 Some groups have reported good results, but efficacy of transepithelial techniques is still a matter of debate, with few studies showing increase in keratometric values and retreatment necessity in a significant percentage of cases.46–50
Accelerated cross-linking
With the standard “Dresden protocol” using 3 mW/cm2 of energy in a 9 mm treatment zone for 30 minutes, a total energy of 5.4 J/cm2 is delivered.30 Therefore, it can be inferred that by using higher intensity light the necessary, exposure time can be reduced to achieve the same total energy.
In an ex vivo study using porcine eyes, Wernli et al51 examined their response to different levels of irradiances between 3 and 90 mW/cm2 and found that irradiances above 50 mW/cm2, with illumination times of less than 2 minutes, failed to increase corneal stiffness.30
Experimental studies have shown that the use of UVA irradiance alone has a high cytotoxic activity, especially in endothelial cells. Cytotoxic level of UVA irradiance has been described as approximately 0.35 mW/cm2, which would be twice as much as it reaches in the use of the standard protocol (0.18 mW/cm2). The use of riboflavin aims to reduce the toxic effect of the use of UVA alone while still increasing corneal stiffness.52 CXL effect on corneal endothelium has been a matter of debate, especially in the setting of accelerated cross-linking because of the higher levels of irradiance. Corneal thickness of a minimum of 400 microns has been described as the cut-off point to avoid endothelial damage, even though there have been case reports of endothelial changes in corneas thicker than 400 μm before surgery.30
A study by Kanellopoulos with a mean follow-up of 46 months, in 21 patients treated with accelerated CXL (7 mW/cm2 for 15 minutes) in one eye and with Dresden standard protocol CXL (3 mW/cm2 for 30 minutes) in the fellow eye showed similar results in both eyes with no progression of KCN and equivalent improvement in visual acuity and keratometry. There was no evidence of endothelial damage.53
Shetty et al54 compared four protocols of CXL in eyes with steep preoperative keratometry between 48.6 diopters (D) and 50.5 D. They found that over a follow-up period of 1 year, standard “Dresden protocol” CXL (3 mW/cm2 for 30 minutes) showed greater flattening effect than accelerated CXL protocols of 9 mW/cm2, 18 mW/cm2, and 30 mW/cm2. Though the latter two groups did not show progression at 12 months, there was no significant corneal flattening in eyes in these two groups. No significant endothelial cell loss was detected.
Another comparative study between standard Dresden protocol CXL and accelerated CXL (18 mW/cm2, 365 nm UVA light, 5 minutes) also showed that the effect of the latter being lower on flattening of the cornea.52
A recent review concluded that with the short follow-up time of almost all the studies (usually 1 year or less), accelerated CXL seems to be a safe and effective method to stop the progression of ectasia, but the effect on flattening the cornea is most probably less than the standard “Dresden protocol.”55
Experimentally, studies have also found that the effect of accelerated CXL is less than the standard 30 minutes protocol. In porcine eyes, increased corneal enzymatic resistance was lower with accelerated CXL (9 mW/cm2 for 10 minutes and 18 mW/cm2 for 5 minutes).56 Also, in porcine corneas exposed to riboflavin 0.1% and different protocols of UVA irradiation (3 mW/cm2 for 30 minutes, 9 mW/cm2 for 10 minutes, and 18 mW/cm2 for 5 minutes), a decreased stiffening effect was found with increasing UVA intensity. In fact, using an irradiance of 18 mW/cm2 for 5 minutes the stiffness of the corneas was not augmented compared to untreated controls. The authors suggested that using high irradiance with short irradiation time settings causes higher oxygen consumption, and due to limited intrastromal oxygen diffusion capacity, the treatment efficiency is reduced.57
For a few years now, it has been known that oxygen presence at an adequate concentration in the stroma is necessary for CXL to occur when applying UVA light in the presence of riboflavin.58 According to a theoretical model of photochemical kinetics of corneal cross-linking, the UVA illumination produced a rapid reduction of stromal available dissolved oxygen in a riboflavin-soaked cornea, secondary to the process of generation of reactive oxygen species (including singlet oxygen). However, turning the UV light off allowed recovery of the oxygen to its original level, from the environment, within 3–4 minutes.59
Therefore, an alternative used to increase the availability of oxygen in the corneal stroma is pulsing the UV light during cross-linking treatment, to permit the reoxygenation during pauses in exposure. Mazzotta et al60 found that a modified protocol of pulsed accelerated cross-linking (pl-ACXL) with 8 minutes of exposure time (1 second on and 1 second off) and 30 mW/cm2, with a total energy dose of 7.2 J/cm2 (ie, higher than in the “Dresden protocol”) had some better results than continuous light accelerated corneal collagen cross-linking (cl-ACXL) with the same instrument (UVA power setting at 30 mW/cm2 for 4 minutes of continuous UVA light exposure, and energy dose of 7.2 J/cm2). With regard to “Topographic-derived apical curvature value”, no statistically significant differences were recorded after cl-ACXL, while a statistically significant decrease by a mean value −1.39 D at 1-year follow-up was found in pl-ACXL. With respect to topographic simulated K average value, a not statistically significant decrease by a mean value of −0.13 D was observed with cl-ACXL, while a statistically significant reduction by a mean value of −1.20 D was observed after pl-ACXL. It is striking that both groups exhibited a loss of corneal endothelial cells density: cl-ACXL: 3.9% and pl-ACXL: 6.6%. The demarcation line after cl-ACXL was uneven and at mean depth of 160 μm and after pl-ACXL, it showed a mean depth of 200 μm. The results on demarcation line depth were similar to those by Peyman et al61 also using a total fluence of 7.2 J/cm2 and a group of eyes with pulsed irradiation and the other with continuous light exposure. However, recently, Kymionis et al,62 using another modified high-intensity CXL protocol for 7 minutes with 18 mW/cm2 of UVA continuous irradiation with a total energy dose of 7.5 J/cm2, found a deeper demarcation line, with no differences with the standard “Dresden protocol” (313.4 microns versus 341.8 microns, respectively).
Another interesting approach is the oxygen enrichment of the environment to which the cornea is exposed during the procedure. Unfortunately, the ex vivo experimental results, recently published by Diakonis et al,63 showed that in human corneas there was no significant effect of supplemental oxygen when accelerated cross-linking was performed (3 minutes exposure to UVA light at 30 mW/cm2 after application of riboflavin). Further studies are required.
Iontophoresis
This alternative has the purpose of enhancing riboflavin penetration through corneal epithelium, using a noninvasive system by means of a low-intensity electric field created by applying on the cornea two electrodes that are connected to a generator which delivers a small electric current. Iontophoresis transepithelial CXL avoids debridement of corneal epithelium and has been shown to provide better riboflavin saturation than epi-on approach. Clinical studies have shown good results in halting of KCN progression and improvement in topographic and visual parameters. However, the effect has shown to be inferior when compared to standard epi-off technique using the “Dresden protocol.”64,65
Patient selection
Indications
The most common indication for CXL is KCN. However, CXL is not primarily a refractive procedure but has the purpose of stopping the progression of corneal ectasia. Therefore, when the ectatic disorder is already stable, the procedure is not indicated. As the age increases, corneal collagen fibrils become thicker, and naturally occurring cross-linking increases stiffness of the tissue (determined by a parameter called the Young’s modulus).29,66,67 These natural changes might explain that when KCN presents earlier in life, the patient has a higher risk of requiring keratoplasty and the classical finding that the condition usually progresses until the third to fourth decade of life, when it typically halts.2,68–74 The Collaborative Longitudinal Evaluation of Keratoconus Study (CLEK study) found among 300 subjects, between 48 and 59 years of age, that there was a slow progression of KCN (0.24 D difference in steep K readings over a period of 3 years), which was statistically significant but clinically nonsignificant.75 In fact, it has been suggested that KCN might regress in patients older than 60 years, because the number of patients in that age group seen by cornea specialists is very low.76
CXL has also been used in other ectatic diseases like PMD and in degenerative corneal diseases like Terrien Marginal Degeneration. However, a much smaller body of evidence supports the indication of CXL in these conditions.19,22,77,78
Therefore, one crucial requisite in order to determine the indication of CXL in KCN is to have definitive criteria for progression, but unfortunately there is no real global consensus. Parameters to consider are change in refraction (including sphere and astigmatism), uncorrected distance visual acuity (UCDVA), corrected distance visual acuity (CDVA), and measurements reflecting corneal shape (as determined by keratometry, Placido disk reflection topography, or tomography using scanning slit with or without applying the Scheimpflug principle).18,29,31,79–81 Clinical measurements, both refractive using manifest refraction and structural using diverse devices, are challenging and have lower repeatability in KCN due to the presence of irregular astigmatism and altered reflection of the corneal mires of the devices on the irregular corneal surface.82–86 In addition, progression of KCN has been shown to be highly variable.72 In the CLEK study, which gathered a very large sample of 1,988 eyes with KCN in adults, flat keratometry increased in average 1.60 D over a period of 8 years, but 24.1% of those eyes showed an increase greater than or equal to 3.00 D.87,88
The Global Delphi Panel of Keratoconus and Ectatic Disease published in 2015 recognized that there was no clear definition of ectasia progression, and so the experts suggested that it should be defined by a reliable change for the worse in two or three of the following parameters: radius of the anterior corneal curvature; radius of the posterior corneal curvature and central corneal thickness; or increase in the rate of change of pachymetry from the periphery to the thinnest point. The experts considered that although KCN progression frequently leads to a worsening in CDVA, a change in both UCDVA and CDVA was not required for documenting progression. In addition, they agreed that specific quantitative data were lacking to determine progression and that such data would most probably be specific to a given device. Also, that the interval between corneal examinations should be shorter among younger patients and that the same measuring equipment, when possible, should be used. However, they did not recommend a specific length of time between two consecutive examinations in order to define progression.89 Moreover, the panel not only stated concerning the indication for CXL that it was essential in the management of KCN with documented clinical progression but also affirmed that it was useful for the treatment of KCN with a significant risk of progression even if the progression had not been documented, as it has been proposed by Chatzis and Hafezi.73 This statement, which reflects the current reality, leaves the door open for the procedure to be performed when the clinician’s judgment indicates it, even if the case does not meet the criteria for progression of the KCN. As we will discuss in the next section, the individualized evaluation of each patient will allow the clinician to make the best decision, taking into account other risk factors, such as age.89
In Table 1, we summarize diverse progression criteria that have been used in CXL studies by several authors.
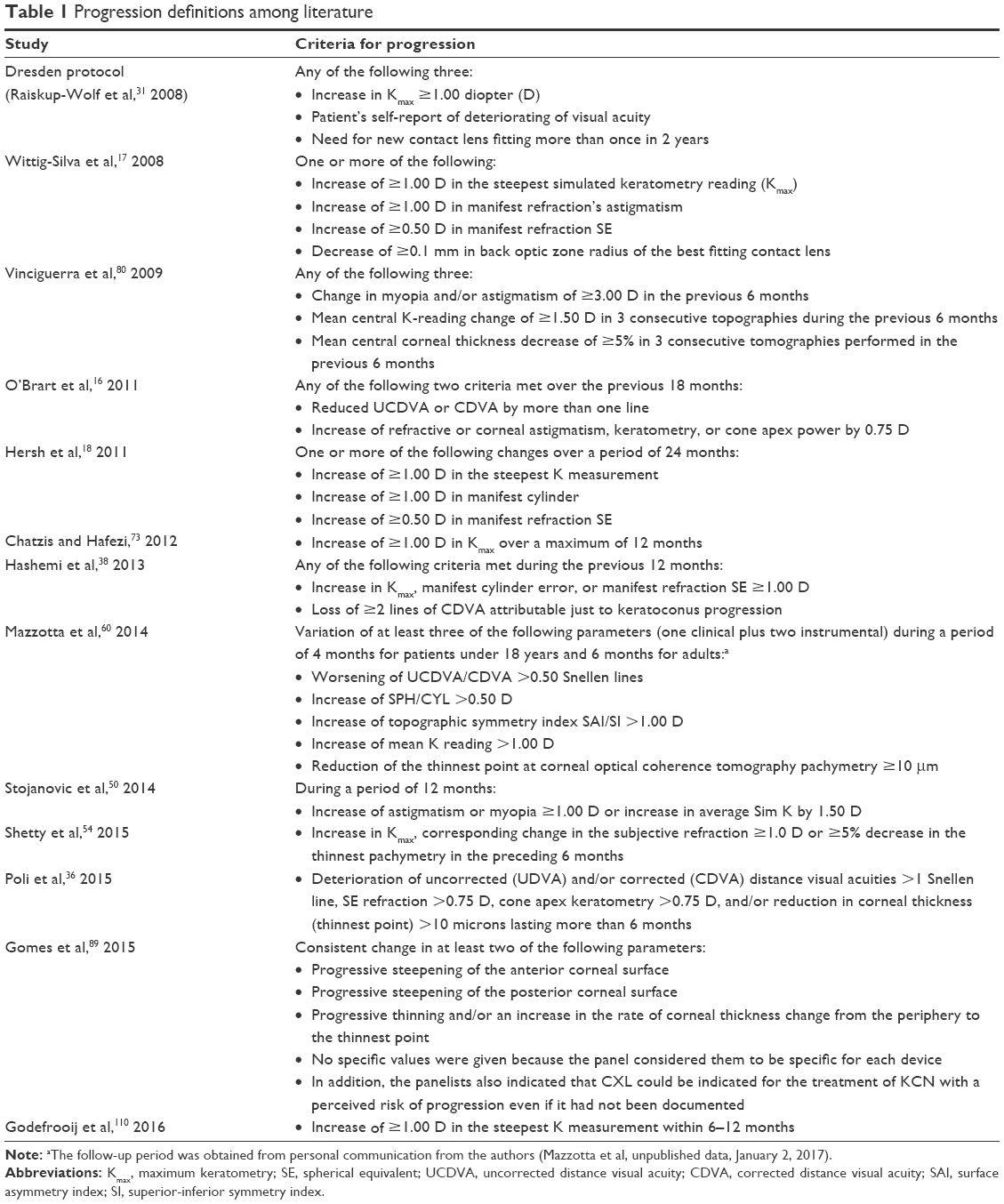 | Table 1 Progression definitions among literature |
Age
KCN may appear very early in life. The youngest patients with KCN were 4 years of age: a girl with persistent eye rubbing and another one with Down syndrome (who in fact, underwent CXL).90–92 Furthermore, modern ophthalmologists are more aware of KCN, and with the available diagnostic tools, it can be detected in very young children (as young as 4 years old, as mentioned), so the cornea specialist faces the dilemma of treating a child without evidence of progression or waiting until progression occurs. Now, as mentioned before, according to a panel of experts and other several authors, if there are risk factors that make progression very likely, CXL is indicated without an age limit. Those groups at risk include children and adolescents, and patients with advanced KCN. Some have suggested that unilateral KCN and CDVA 20/40 or worst are also indications of CXL.73,89
However, with regard to CXL in children, there is a scarcity of randomized control trials, so the majority of the information is extrapolated from the also limited data from clinical trials and case series with adults. So, it is not possible to affirm that there is a gold standard protocol to follow for making decisions in children. However, according to the results from the Siena CXL Pediatrics trial, it is the standard epi-off (“Dresden protocol”) option that should be used when the available evidence is too weak to support the practice of other alternatives (like epi-on CXL). Topographic and functional improvement was obtained in 80% of children included in the study, while only 4.6% of the cases showed progression after CXL.87,93 Nevertheless, according to some reports, CXL in children might not be as successful as in adults, and therefore the former need close postoperative follow-up, as the risk of progression is real and further CXL may be warranted.87,94–96 In a recent report on long-term results, Godefrooij et al96 found that among 54 eyes of 36 children, who underwent CXL with the “Dresden protocol” and had a follow-up time up to 5 years (18 eyes followed for 4 years and 9 eyes for 5 years), the maximum keratometry showed a significant improvement of 2.06 D on average, but in 12 eyes (22%) of nine children (25%), a progression in the keratometry values of 1.0 D or higher presented at the last follow-up visit.94
Recently, Frucht-Pery and Wajnsztajn97 indicated that most of their patients undergoing CXL in the last 2 years have been diagnosed only several months earlier, because they do not wait for progression to happen if the patient is in a high-risk group, especially children and adolescents. However, they also stated that a case-by-case assessment is required to weigh the risks against the benefits of the surgery. We, as other clinicians and researchers, fully agree with their concepts and apply them in our clinical practice.94
In the case of children with mild disease, with good vision (CDVA of 20/20 or better), and few or undefined topographic signs, most probably will benefit from closer observation with frequent examination (every 1–3 months). Now, if the child presents with a topographically evident KCN, in a relatively advanced stage, CXL most probably will be of benefit to the patient without waiting for the evidence of progression.87,91
When there is a fellow apparently healthy eye, it is important to remember that there is no such thing as a true “unilateral” KCN.86 CXL is indicated in the eye with the progressive disease, and, unless another significant risk factor is present (very young age, persistent eye-rubbing, etc.), the less compromised eye with good vision can be maintained in close observation.
The longest reported follow-up time of CXL in children has been 3 years, and the effect of the procedure seemed to diminish after 2 years.89,98 Therefore, the possibility of requiring an additional CXL should be considered when progression is found after the first procedure.99 Some parameters have been suggested by Hamada et al90 to determine the indication of a new CXL treatment: increase in the flattest K (K1), steepest K (K2), or Kmax >1 D, a change in the difference map between two consecutive topographies by 1 D, a deterioration of CDVA or any consistent change in the refractive astigmatism.87
Corneal thickness
Before first trials in humans, animal models (specifically in rabbits) were used to establish that the currently used parameters usually affect the anterior 250–350 microns corneal stroma; therefore, a minimum of 400 microns stromal thickness was set as a safety margin in order to protect corneal endothelial cells.29
However, taking into account that KCN causes stromal thinning, in advanced cases the corneas frequently have less than 400 microns of thickness. Performing standard cross-linking on those cases implies the risk of endothelial cell loss, as shown by Kymionis et al100 who treated 14 eyes (pachymetry after epithelial removal between 340 and 399 microns) and found a loss of endothelial cells of 10.7%.101
Several alternatives have been proposed in those cases.95 In 2009, Hafezi et al102 described a modified protocol for corneas thinner than 400 microns, swelling the stroma using hypoosmolar riboflavin solution. The standard iso-osmolar riboflavin 0.1% solution used in the “Dresden protocol” is prepared by diluting vitamin B2-riboflavin-5-phosphate 0.5% (Streuli Pharma, Uznach, Switzerland) with dextran T500 20% to reach an osmolarity of 402.7 mOsmol/L, while hypoosmolar riboflavin 0.1% solution is prepared by diluting vitamin B2–riboflavin–5-phosphate 0.5% with sodium chloride 0.9% solution, having 310 mOsmol/L, which causes corneal swelling. They used the treatment in corneas as thin as 323 microns after epithelial debridement and reached more than 400 microns after swelling in 20 cases.103 However, a case that presented rapid progression after the procedure was reported. Pachymetry after epithelial debridement was 268 microns, which reached 406 microns after swelling with hypoosmolar riboflavin solution and showed 2.3 D of progression 6 months after CXL.55,104,105 Recently, accelerated (9 mW/cm2 for 10 minutes) CXL with hypoosmolar riboflavin solution was shown to be effective in 49 eyes with thin corneas at short term (6 months of follow-up).98 One advantage on the safety when using accelerated cross-linking in thin corneas is that the effect is most probably more superficial so that the corneal endothelium would be more protected. However, efficacy could be diminished.99
In corneas between 350 and 400 microns of thickness after epithelial abrasion, Jacob et al106 used iso-osmolar solution of riboflavin 0.1% in dextran and an ultraviolet barrier-free hilafilcon soft contact lens (90 microns in thickness) soaked in iso-osmolar riboflavin 0.1% placed on the cornea to reach more than 400 microns of thickness of the complex contact lens-cornea. Then UVA irradiation was applied. In 14 eyes followed for around 6 months, no progression occurred and 28.5% showed a decrease in Kmax in 1.00 D or more.107 Currently, in very thin corneas, which do not reach 400 microns even after the use of hypoosmolar riboflavin, we are performing a study with a different approach: protection of the 4 mm central cornea. This is thought to allow the CXL procedure to act at least in the periphery of the cornea, so that the receptor tissue is best prepared when a penetrating or lamellar anterior keratoplasty is performed in those advanced KCNs.
CXL predictors of outcomes
Although some short-term and long-term studies have reported a rate of success of 100% in stopping the progression of KCN using CXL, failure rates between 7.6% and 11% have been found for other groups.11,41,36,108–110
In relation to corneal flattening, steeper pretreatment Kmax (≥54 D), a more centrally located cone apex, and central pachymetry ≥450 microns have all been reported as predictive factors.109–112
Godefrooij et al110 identified possible predictors for results of the effect of CXL in a prospective cohort, and recently in a different prospective cohort they performed a validation study.108 They found by using univariate analysis that a predictor of higher improvement in Kmax was male sex, while atopia was a predictor of a slight (but significant) decrease in improvement in visual acuity.108 Using a multivariable linear regression analysis, baseline visual acuity and cone eccentricity were the only two independent factors for predicting change in postoperative CDVA and Kmax, respectively. Patients with lower pretreatment visual acuity were more likely to have improved visual acuity after CXL, and patients with more central cones had more possibility of greater corneal flattening.108 The latter finding was is in concordance with those reported by Greenstein and Hersh.109 Godefrooij et al110 suggested, as Greenstein and Hersh,109 that this might be related to the angle of exposure to UVA light: it is more perpendicular in central cones while peripheral ones receive light rays with an oblique incidence.108 Therefore, they proposed that focusing the UVA light on the cone apex, instead of the geometrical center of the cornea, could improve results in eccentric cones.108 In their validation set, Godefrooij et al110 found similar results to their original prospective cohort.108 Baseline preoperative CDVA was found to be the sole independent factor predicting an improvement in CDVA 1 year after the procedure, with patients with lower pretreatment visual acuity showing higher possibilities to benefit from CXL (with regard to visual acuity) and eyes with more central cones obtaining more benefit from the procedure in terms of corneal flattening.110 In addition, unlike the findings in their first cohort, in the validation study they found that younger patients had significantly better results with respect to visual acuity.108,110 Soeters et al113 had also identified age as a prognostic factor.110
In another recent study, Godefrooij et al96 also identified using a multivariable logistic regression analysis that cone eccentricity was the only independent factor significantly related to the progression of KCN in children who underwent CXL (mean age 14.8 years of age).
Greenstein and Hersh109 studied 104 eyes of patients older than 13 years of age who had an axial corneal topography (Pentacam, Oculus Optikgeräte GmbH, Wetzlar, Germany) consistent with KCN or postrefractive surgery corneal ectasia and who underwent CXL. They found that in the multivariate regression analysis, the CDVA and maximum K value from the topography were the only significant predictors of the 1-year postoperative CDVA. However, although the multivariate analysis identified an association between the preoperative maximum K value and the postoperative CDVA, OR analyses failed to reach statistical significance. Their multivariate analysis also found that preoperative maximum K was the only significant predictor of the 1-year postoperative maximum K. In eyes with a maximum preoperative K value from the topography of 55.0 D or steeper, they calculated a probability 5.4 times higher to have a flattening of 2.0 D or more 1 year after CXL than eyes with a maximum K value of less than 55.0 D. While 45.4% of 44 eyes with a maximum K value of 55.0 D or more showed a flattening by 2.0 D or more, 13.3% of 60 eyes had a preoperative maximum K of less than 55.0 D.109
With regard to topographic progression (1.0 D or more of topographic corneal steepening as determined using the maximum K) 1 year after the procedure, they found no difference between eyes with a maximum preoperative K value of 55.0 D or more, and eyes with a maximum K value less than 55.0 D. 10.0% of 44 eyes form the former group and 8.3% of 60 eyes in the latter group showed that level of postoperative progression.109 On the other hand, Koller et al41 had previously found that comparing a number of eyes undergoing CXL that showed progression 1 year after the surgery (8 eyes – 7.6% of a group of 105) with those without progression, maximum preoperative K over 58.0 D and female sex were identified as risk factors, with an OR of 5.32 for K and 3.11 for sex.
CXL contraindications
Pachymetry thinner than 400 microns
Traditionally, corneal thickness below 400 microns was considered a contraindication to CXL. However, as mentioned earlier, some alternatives exist in order to perform CXL in those corneas safely.95–101 Therefore, a pachymetry thinner than 400 microns is now not an absolute contraindication but a relative one.
Prior herpetic ocular infection
In a case series of infectious keratitis published by Price et al,114 one patient having an apparently microbial keratitis, but with negative bacterial and fungal cultures, and who later turned out to have herpes simplex, developed severe dendritic lesions after receiving CXL.
Several other case reports of herpetic keratitis after CXL have been published in KCN, it being striking that patients denied a past history of the disease. Kymionis et al115 reported the case of a young adult woman who 5 days after CXL presented with geographic epithelial herpetic keratitis and iritis. The etiology was confirmed by polymerase chain reaction of tear samples. Yuksel et al116 also published the case of a 31-year-old woman who 4 days after CXL presented with a dendritic ulcer. The diagnosis was confirmed with polymerase chain reaction analysis of the corneal swab for herpes simplex.
More recently, Al-Qarni and AlHarbi117 reported two cases of young adults who also had no past history of herpetic keratitis and presented dendritic ulcers in the early postoperative period.
Thus, past history of herpetic keratitis is a contraindication for CXL, but, as seen, herpetic keratitis may develop in a patient without past history of herpetic disease.
Other contraindications
Concurrent ocular infection, severe corneal scarring, or opacification, neurotrophic keratopathy, past history of poor epithelial wound healing, severe dry eye, autoimmune disorders, and pregnancy are currently considered contraindication for CXL in corneal ectatic diseases.
Conclusion
Experimental and clinical findings have demonstrated CXL effectiveness in the last 10 years, and the number of patients undergoing the procedure has increased significantly. Since the beginning of its use in the clinic by the group of researchers from Germany, almost 20 years ago, cross-linking had traditionally been indicated in cases of documented progression of corneal ectasia in a period of 6–12 months. However, since KCN is a disease that appears in the first 2 decades of life and usually has a more aggressive progression in young patients, it is the responsibility of ophthalmologists to treat these children and adolescents early, which is why the criterion of waiting for progression to be documented should be analyzed on a case-by-case basis. There are viable alternatives to offer treatment even in eyes with thin corneas (less than 400 microns after the deepithelization). Certain small changes in the technique (such as centering the treatment at the apex of the cone) may increase its effectiveness. Until there is a proven superior alternative treatment, CXL using UVA light and riboflavin will remain the backbone of KCN treatment in modern ophthalmology.
Disclosure
The authors report no conflicts of interest in this work.
References
Ziaei M, Barsam A, Shamie N, et al. Reshaping procedures for the surgical management of corneal ectasia. J Cataract Refract Surg. 2015;41(4):842–872. | ||
Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. | ||
Romero-Jiménez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review. Cont Lens Anterior Eye. 2010;33(4):157–166; quiz 205. | ||
Galvis V, Sherwin T, Tello A, Merayo J, Barrera R, Acera A. Keratoconus: an inflammatory disorder? Eye (Lond). 2015;29(7):843–859. | ||
Santhiago MR, Giacomin NT, Smadja D, Bechara SJ. Ectasia risk factors in refractive surgery. Clin Ophthalmol. 2016;10:713–720. | ||
Wolle MA, Randleman JB, Woodward MA. Complications of refractive surgery: ectasia after refractive surgery. Int Ophthalmol Clin. 2016;56(2):127–139. | ||
Galvis V, Tello A, Gomez AJ, Rangel CM, Prada4 AM, Camacho PA. Corneal transplantation at an ophthalmological referral center in Colombia: indications and techniques (2004–2011). Open Ophthalmol J. 2013;7:30–33. | ||
Raiskup F, Spoerl E. Corneal crosslinking with riboflavin and ultraviolet A. Part II. Clinical indications and results. Ocul Surf. 2013;11(2):93–108. | ||
Randleman JB, Khandelwal SS, Hafezi F. Corneal cross-linking. Surv Ophthalmol. 2015;60(6):509–523. | ||
Farjadnia M, Naderan M. Corneal cross-linking treatment of keratoconus. Oman J Ophthalmol. 2015;8(2):86–91. | ||
O’Brart DP, Patel P, Lascaratos G, et al. Corneal cross-linking to halt the progression of keratoconus and corneal ectasia: seven-year follow-up. Am J Ophthalmol. 2015;160(6):1154–1163. | ||
Raiskup F, Theuring A, Pillunat LE, Spoerl E. Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: ten-year results. J Cataract Refract Surg. 2015;41(1):41–46. | ||
Shalchi Z, Wang X, Nanavaty MA. Safety and efficacy of epithelium removal and transepithelial corneal collagen crosslinking for keratoconus. Eye (Lond). 2015;29(1):15–29. | ||
O’Brart DP. Corneal collagen crosslinking for corneal ectasias: a review. Eur J Ophthalmol. In press 2016. | ||
Sykakis E, Karim R, Evans JR, et al. Corneal collagen cross-linking for treating keratoconus. Cochrane Database Syst Rev. 2015;(3):CD010621. | ||
O’Brart DP, Chan E, Samaras K, Patel P, Shah SP. A randomised, prospective study to investigate the efficacy of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linkage to halt the progression of keratoconus. Br J Ophthalmol. 2011;95(11):1519–1524. | ||
Wittig-Silva C, Whiting M, Lamoureux E, Lindsay RG, Sullivan LJ, Snibson GR. A randomized controlled trial of corneal collagen cross-linking in progressive keratoconus: preliminary results. J Refract Surg. 2008;24(7):S720–S725. | ||
Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(1):149–160. | ||
Sorkin N, Varssano D. Corneal collagen crosslinking: a systematic review. Ophthalmologica. 2014;232(1):10–27. | ||
Tabibian D, Mazzotta C, Hafezi F. PACK-CXL: corneal cross-linking in infectious keratitis. Eye Vis (Lond). 2016;3:11. | ||
Tabibian D, Richoz O, Hafezi F. PACK-CXL: Corneal cross-linking for treatment of infectious keratitis. J Ophthalmic Vis Res. 2015;10(1):77–80. | ||
Balparda K, Maldonado MJ. Corneal collagen cross-linking. A review of its clinical applications. Arch Soc Esp Oftalmol. Epub 2016 Nov 30. | ||
Khan MS, Basit I, Ishaq M, Shakoor T, Yaqub A, Intisar R. Corneal collagen cross linking (CXL) in treatment of pseudophakic bullous keratopathy. Pak J Med Sci. 2016;32(4):965–968. | ||
Pacifici RE, Davies KJ. Protein degradation as an index of oxidative stress. Meth Enzymol. 1990;186:485–502. | ||
Raiskup F, Spoerl E. Corneal crosslinking with riboflavin and ultraviolet A. I. Principles. Ocul Surf. 2013;11(2):65–74. | ||
da Paz AC, Bersanetti PA, Salomão MQ, Ambrósio R Jr, Schor P. Theoretical basis, laboratory evidence, and clinical research of chemical surgery of the cornea: cross-linking. J Ophthalmol. 2014;2014:890823. | ||
Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66(1):97–103. | ||
Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg. 2003;29(9):1780–1785. | ||
Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. | ||
Spoerl E, Mrochen M, Sliney D, Trokel S, Seiler T. Safety of UVA-riboflavin cross-linking of the cornea. Cornea. 2007;26(4):385–389. | ||
Raiskup-Wolf F, Hoyer A, Spoerl E, Pillunat LE. Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg. 2008;34(5):796–801. | ||
Craig JA, Mahon J, Yellowlees A, et al. Epithelium-off photochemical corneal collagen cross-linkage using riboflavin and ultraviolet a for keratoconus and keratectasia: a systematic review and meta-analysis. Ocul Surf. 2014;12(3):202–214. | ||
Kymionis GD, Diakonis VF, Kalyvianaki M, et al. One-year follow-up of corneal confocal microscopy after corneal cross-linking in patients with post laser in situ keratosmileusis ectasia and keratoconus. Am J Ophthalmol. 2009;147(5):774–778, 778.e1. | ||
Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010;149(4):585–593. | ||
Galvis V, Tello A, Ortiz AI. Corneal collagen crosslinking with riboflavin and ultraviolet for keratoconus: long-term follow-up. J Cataract Refract Surg. 2015;41(6):1336–1337. | ||
Poli M, Lefevre A, Auxenfans C, Burillon C. Corneal collagen cross-linking for the treatment of progressive corneal ectasia: 6-year prospective outcome in a French population. Am J Ophthalmol. 2015;160(4):654.e1–662.e1. | ||
Razmjoo H, Rahimi B, Kharraji M, Koosha N, Peyman A. Corneal haze and visual outcome after collagen crosslinking for keratoconus: a comparison between total epithelium off and partial epithelial removal methods. Adv Biomed Res. 2014;3:221. | ||
Hashemi H, Seyedian MA, Miraftab M, Fotouhi A, Asgari S. Corneal collagen cross-linking with riboflavin and ultraviolet a irradiation for keratoconus: long-term results. Ophthalmology. 2013;120(8):1515–1520. | ||
Galvis V, Tello A, Carreño NI, et al. Corneal cross-linking (with a partial deepithelization) in keratoconus with five years of follow-up. Ophthalmol Eye Dis. 2016;8:17–21. | ||
Rehnman JB, Lindén C, Hallberg P, Behndig A. Treatment effect and corneal light scattering with 2 corneal cross-linking protocols: a randomized clinical trial. JAMA Ophthalmol. 2015;133(11):1254–1260. | ||
Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. | ||
Pollhammer M, Cursiefen C. Bacterial keratitis early after corneal crosslinking with riboflavin and ultraviolet-A. J Cataract Refract Surg. 2009;35(3):588–589. | ||
Dhawan S, Rao K, Natrajan S. Complications of corneal collagen cross-linking. J Ophthalmol. 2011;2011:869015. | ||
Wollensak G, Iomdina E. Biomechanical and histological changes after corneal crosslinking with and without epithelial debridement. J Cataract Refract Surg. 2009;35(3):540–546. | ||
Scarcelli G, Kling S, Quijano E, Pineda R, Marcos S, Yun SH. Brillouin microscopy of collagen crosslinking: noncontact depth-dependent analysis of corneal elastic modulus. Invest Ophthalmol Vis Sci. 2013;54(2):1418–1425. | ||
Boxer Wachler BS, Pinelli R, Ertan A, Chan CC. Safety and efficacy of transepithelial crosslinking (C3-R/CXL). J Cataract Refract Surg. 2010;36(1):186–188; author reply 188–189. | ||
Koppen C, Wouters K, Mathysen D, Rozema J, Tassignon MJ. Refractive and topographic results of benzalkonium chloride-assisted transepithelial crosslinking. J Cataract Refract Surg. 2012;38(6): 1000–1005. | ||
Caporossi A, Mazzotta C, Paradiso AL, Baiocchi S, Marigliani D, Caporossi T. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2013;39(8):1157–1163. | ||
Raiskup F, Veliká V, Veselá M, Spörl E. [Cross-Linking in Keratoconus: “Epi-off” or “Epi-on?”]. Klin Monbl Augenheilkd. 2015;232(12):1392–1396. | ||
Stojanovic A, Zhou W, Utheim TP. Corneal collagen cross-linking with and without epithelial removal: a contralateral study with 0.5% hypotonic riboflavin solution. Biomed Res Int. 2014;2014:619398. | ||
Wernli J, Schumacher S, Spoerl E, Mrochen M. The efficacy of corneal cross-linking shows a sudden decrease with very high intensity UV light and short treatment time. Invest Ophthalmol Vis Sci. 2013;54(2):1176–1180. | ||
Chow VW, Chan TC, Yu M, Wong VW, Jhanji V. One-year outcomes of conventional and accelerated collagen crosslinking in progressive keratoconus. Sci Rep. 2015;5:14425. | ||
Kanellopoulos AJ. Long term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconus. Clin Ophthalmol. 2012;6:97–101. | ||
Shetty R, Pahuja NK, Nuijts RM, et al. Current protocols of corneal collagen cross-linking: visual, refractive, and tomographic outcomes. Am J Ophthalmol. 2015;160(2):243–249. | ||
Medeiros CS, Giacomin NT, Bueno RL, Ghanem RC, Moraes HV, Santhiago MR. Accelerated corneal collagen crosslinking: technique, efficacy, safety, and applications. J Cataract Refract Surg. 2016;42(12): 1826–1835. | ||
Aldahlawi NH, Hayes S, O’Brart DP, Meek KM. Standard versus accelerated riboflavin-ultraviolet corneal collagen crosslinking: resistance against enzymatic digestion. J Cataract Refract Surg. 2015;41(9):1989–1996. | ||
Hammer A, Richoz O, Arba Mosquera S, Tabibian D, Hoogewoud F, Hafezi F. Corneal biomechanical properties at different corneal cross-linking (CXL) irradiances. Invest Ophthalmol Vis Sci. 2014;55(5):2881–2884. | ||
Richoz O, Hammer A, Tabibian D, Gatzioufas Z, Hafezi F. The biomechanical effect of corneal collagen cross-linking (CXL) with riboflavin and UV-A is oxygen dependent. Transl Vis Sci Technol. 2013;2(7):6. | ||
Kamaev P, Friedman MD, Sherr E, Muller D. Photochemical kinetics of corneal cross-linking with riboflavin. Invest Ophthalmol Vis Sci. 2012;53(4):2360–2367. | ||
Mazzotta C, Traversi C, Paradiso AL, Latronico ME, Rechichi M. Pulsed light accelerated crosslinking versus continuous light accelerated crosslinking: one-year results. J Ophthalmol. 2014;2014:604731. | ||
Peyman A, Nouralishahi A, Hafezi F, Kling S, Peyman M. Stromal demarcation line in pulsed versus continuous light accelerated corneal cross-linking for keratoconus. J Refract Surg. 2016;32(3):206–208. | ||
Kymionis GD, Tsoulnaras KI, Liakopoulos DA, Skatharoudi CA, Grentzelos MA, Tsakalis NG. Corneal stromal demarcation line depth following standard and a modified high intensity corneal cross-linking protocol. J Refract Surg. 2016;32(4):218–222. | ||
Diakonis VF, Likht NY, Yesilirmak N, et al. Corneal elasticity after oxygen enriched high intensity corneal cross linking assessed using atomic force microscopy. Exp Eye Res. 2016;153:51–55. | ||
Bikbova G, Bikbov M. Standard corneal collagen crosslinking versus transepithelial iontophoresis-assisted corneal crosslinking, 24 months follow-up: randomized control trial. Acta Ophthalmol. 2016;94(7):e600–e606. | ||
Magli A, Chiariello Vecchio E, Carelli R, Piozzi E, Landro F Di, Troisi S. Pediatric keratoconus and iontophoretic corneal crosslinking: refractive and topographic evidence in patients underwent general and topical anesthesia, 18 months of follow-up. Int Ophthalmol. 2016;36(4):585–590. | ||
Malik NS, Moss SJ, Ahmed N, Furth AJ, Wall RS, Meek KM. Ageing of the human corneal stroma: structural and biochemical changes. Biochim Biophys Acta. 1992;1138(3):222–228. | ||
Knox Cartwright NE, Tyrer JR, Marshall J. Age-related differences in the elasticity of the human cornea. Invest Ophthalmol Vis Sci. 2011;52(7):4324–4329. | ||
Tuft SJ, Moodaley LC, Gregory WM, Davison CR, Buckley RJ. Prognostic factors for the progression of keratoconus. Ophthalmology. 1994;101(3):439–447. | ||
Ertan A, Muftuoglu O. Keratoconus clinical findings according to different age and gender groups. Cornea. 2008;27(10):1109–1113. | ||
Sherwin T, Brookes NH. Morphological changes in keratoconus: pathology or pathogenesis. Clin Experiment Ophthalmol. 2004;32(2):211–217. | ||
Choi JA, Kim MS. Progression of keratoconus by longitudinal assessment with corneal topography. Invest Ophthalmol Vis Sci. 2012;53(2):927–935. | ||
Brown SE, Simmasalam R, Antonova N, Gadaria N, Asbell PA. Progression in keratoconus and the effect of corneal cross-linking on progression. Eye Contact Lens. 2014;40(6):331–338. | ||
Chatzis N, Hafezi F. Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents. J Refract Surg. 2012;28(11):753–758. | ||
Olivares Jiménez JL, Guerrero Jurado JC, Bermudez Rodriguez FJ, Serrano Laborda D. Keratoconus: age of onset and natural history. Optom Vis Sci. 1997;74(3):147–151. | ||
Fink BA, Sinnott LT, Wagner H, Friedman C, Zadnik K. The influence of gender and hormone status on the severity and progression of keratoconus. Cornea. 2010;29(1):65–72. | ||
Krachmer JH. Potential research projects. Cornea. 2007;26(3):243–245. | ||
Bayraktar S, Cebeci Z, Oray M, Alparslan N. Corneal collagen cross-linking in pellucid marginal degeneration: 2 patients, 4 eyes. Case Rep Ophthalmol Med. 2015;2015:840687. | ||
Hafezi F, Gatzioufas Z, Seiler T, Seiler T. Corneal collagen cross-linking for Terrien marginal degeneration. J Refract Surg. 2014;30(7):498–500. | ||
Poli M, Cornut PL, Balmitgere T, Aptel F, Janin H, Burillon C. Prospective study of corneal collagen cross-linking efficacy and tolerance in the treatment of keratoconus and corneal ectasia: 3-year results. Cornea. 2013;32(5):583–590. | ||
Vinciguerra P, Albè E, Trazza S, et al. Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking. Ophthalmology. 2009;116(3):369–378. | ||
Wittig-Silva C, Chan E, Islam FM, Wu T, Whiting M, Snibson GR. A randomized, controlled trial of corneal collagen cross-linking in progressive keratoconus: three-year results. Ophthalmology. 2014;121(4):812–821. | ||
Edrington TB, Szczotka LB, Begley CG, et al. Repeatability and agreement of two corneal-curvature assessments in keratoconus: keratometry and the first definite apical clearance lens (FDACL). CLEK Study Group. Collaborative Longitudinal Evaluation of Keratoconus. Cornea. 1998;17(3):267–277. | ||
McMahon TT, Anderson RJ, Joslin CE, Rosas GA. Precision of three topography instruments in keratoconus subjects. Optom Vis Sci. 2001;78(8):599–604. | ||
McMahon T, Anderson R, Roberts C, et al. Repeatability of corneal topography measurement in keratoconus with the TMS-1. Optom Vis Sci. 2005;82(5):405–415. | ||
Szalai E, Berta A, Hassan Z, Módis L Jr. Reliability and repeatability of swept-source Fourier-domain optical coherence tomography and Scheimpflug imaging in keratoconus. J Cataract Refract Surg. 2012;38(3):485–494. | ||
Davis LJ, Schechtman KB, Begley CG, Shin JA, Zadnik K. Repeatability of refraction and corrected visual acuity in keratoconus. The CLEK Study Group. Collaborative Longitudinal Evaluation of Keratoconus. Optom Vision Sci. 1998;75(12):887–896. | ||
Davis LJ, Schechtman KB, Wilson BS, et al. Longitudinal changes in visual acuity in keratoconus. Invest Ophthalmol Vis Sci. 2006;47(2):489–500. | ||
Wagner H, Barr JT, Zadnik K. Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study: methods and findings to date. Cont Lens Anterior Eye. 2007;30(4):223–232. | ||
Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. | ||
Hamada S, Barua A, Caporossi A, et al. Corneal cross-linking in children. In: Sinjab MM, Cummings A, editors. Corneal Collagen Crosslinking. Cham, Switzerland: Springer; 2017:229–268. | ||
Gunes A, Tok L, Tok Ö, Seyrek L. The youngest patient with bilateral keratoconus secondary to chronic persistent eye rubbing. Semin Ophthalmol. 2015;30(5–6):454–456. | ||
Sabti S, Tappeiner C, Frueh B. Corneal cross-linking in a 4-year-old child with keratoconus and down syndrome. Cornea. 2015;34(9):1157–1160. | ||
Caporossi A, Mazzotta C, Baiocchi S, Caporossi T, Denaro R, Balestrazzi A. Riboflavin-UVA-induced corneal collagen cross-linking in pediatric patients. Cornea. 2012;31(3):227–231. | ||
Wisse RP, Godefrooij DA, Soeters N. Reply. Cornea. 2016;35(11):e36. | ||
Viswanathan D, Kumar NL, Males JJ. Outcome of corneal collagen crosslinking for progressive keratoconus in paediatric patients. Biomed Res Int. 2014;2014:140461. | ||
Godefrooij DA, Soeters N, Imhof SM, Wisse RP. Corneal cross-linking for pediatric keratoconus: long-term results. Cornea. 2016;35(7):954–958. | ||
Frucht-Pery J, Wajnsztajn D. Clinical application and decisión making. In: Sinjab MM, Cummings A, editors. Corneal Collagen Crosslinking. Cham, Switzerland: Springer; 2017:167–188. | ||
Zotta P, Moschou K, Diakonis V, et al. Corneal collagen cross-linking for progressive keratoconus in pediatric patients: a feasibility study. J Refract Surg. 2012;28(11):793–799. | ||
Antoun J, Slim E, Hachem R, et al. Rate of corneal collagen crosslinking redo in private practice: risk factors and safety. J Ophthalmol. 2015;2015:690961. | ||
Kymionis G, Portaliou D, Diakonis V, Kounis G, Panagopoulou S, Grentzelos M. Corneal collagen cross-linking with riboflavin and ultraviolet-A irradiation in patients with thin corneas. Am J Ophthalmol. 2012;153(1):24–28. | ||
Chen X, Stojanovic A, Eidet J, Utheim TP. Corneal collagen cross-linking (CXL) in thin corneas. Eye Vis. 2015;2:15. | ||
Hafezi F, Mrochen M, Iseli H, Seiler T. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009;35(4):621–624. | ||
Wollensak G, Aurich H, Wirbelauer C, Sel S. Significance of the riboflavin film in corneal collagen crosslinking. J Cataract Refract Surg. 2010;36(1):114–120. | ||
Hafezi F. Limitation of collagen cross-linking with hypoosmolar riboflavin solution: failure in an extremely thin cornea. Cornea. 2011;30(8):917–919. | ||
Koç M, Uzel M, Koban Y, Tekin K, Taşlpnar A, Ylmazbaş P. Accelerated corneal cross-linking with a hypoosmolar riboflavin solution in keratoconic thin corneas: short-term results. Cornea. 2016;35(3):350–354. | ||
Jacob S, Kumar D, Agarwal A, Basu S, Sinha P, Agarwal A. Contact lens-assisted collagen cross-linking (CACXL): a new technique for cross-linking thin corneas. J Refract Surg. 2014;30(6):366–372. | ||
Mazzotta C, Jacob S, Agarwal A, Kumar D. In vivo confocal microscopy after contact lens-assisted corneal collagen cross-linking for thin keratoconic corneas. J Refract Surg. 2016;32(5):326–331. | ||
Wisse RP, Godefrooij DA, Soeters N, Imhof SM, Van der Lelij A. A multivariate analysis and statistical model for predicting visual acuity and keratometry one year after cross-linking for keratoconus. Am J Ophthalmol. 2014;157(3):519–525.e1–e2. | ||
Greenstein SA, Hersh PS. Characteristics influencing outcomes of corneal collagen crosslinking for keratoconus and ectasia: implications for patient selection. J Cataract Refract Surg. 2013;39(8):1133–1140. | ||
Godefrooij DA, Boom K, Soeters N, Imhof SM, Wisse RP. Predictors for treatment outcomes after corneal crosslinking for keratoconus: a validation study. Int Ophthalmol. Epub 2016 May 24. | ||
Toprak I, Yaylali V, Yildirim C. Factors affecting outcomes of corneal collagen crosslinking treatment. Eye (Lond). 2014;28(1):41–46. | ||
Sloot F, Soeters N, van der Valk R, Tahzib NG. Effective corneal collagen crosslinking in advanced cases of progressive keratoconus. J Cataract Refract Surg. 2013;39(8):1141–1145. | ||
Soeters N, Van der Lelij A, van der Valk R, Tahzib NG. Corneal crosslinking for progressive keratoconus in four children. J Pediatr Ophthalmol Strabismus. 2011;48 Online:e26–e29. | ||
Price M, Tenkman L, Schrier A, Fairchild K, Trokel S, Price F. Photoactivated riboflavin treatment of infectious keratitis using collagen cross-linking technology. J Refract Surg. 2012;28(10):706–713. | ||
Kymionis G, Portaliou D, Bouzoukis D, et al. Herpetic keratitis with iritis after corneal crosslinking with riboflavin and ultraviolet A for keratoconus. J Cataract Refract Surg. 2007;33(11):1982–1984. | ||
Yuksel N, Bilgihan K, Hondur A. Herpetic keratitis after corneal collagen cross-linking with riboflavin and ultraviolet-A for progressive keratoconus. Int Ophthalmol. 2011;31(6):513–515. | ||
Al-Qarni A, AlHarbi M. Herpetic keratitis after corneal collagen cross-linking with riboflavin and ultraviolet-a for keratoconus. Middle East Afr J Ophthalmol. 2015;22(3):389–392. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.