Back to Journals » Patient Preference and Adherence » Volume 17
Patient Satisfaction and Perspectives on Self-Management Education Programs: A Qualitative Study
Authors Ricci L ![]() , Buzzi M, Kivits J, Rat AC
, Buzzi M, Kivits J, Rat AC ![]()
Received 14 April 2023
Accepted for publication 28 June 2023
Published 1 September 2023 Volume 2023:17 Pages 2175—2186
DOI https://doi.org/10.2147/PPA.S414126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Laetitia Ricci,1,2 Marie Buzzi,1,2 Joelle Kivits,2 Anne-Christine Rat2,3
1CIC, Epidémiologie Clinique, CHRU-Nancy, INSERM, Université de Lorraine, Nancy, F-54000, France; 2APEMAC, équipe MICS, Université de Lorraine, Nancy, F-54000, France; 3UMR-S 1075-Mobilités: Vieillissement, Pathologie, Santé COMETE, Caen Normandie University, Caen, France
Correspondence: Laetitia Ricci, CIC-EC, CHRU de NANCY - Hôpitaux de Brabois Allée du Morvan Vandœuvre-lès-Nancy Cedex, Nancy, 54511, France, Tel +336 64 74 68 16, Email [email protected]
Purpose: According to the Centre for Disease Control and Prevention, “Self-management education (SME) refers to programs that help people who have ongoing health conditions learn how to live life to the fullest”. Most studies to date have focused on SME outcomes, such as the acquisition of predefined knowledge or skills or quality of life. However, no study has yet investigated patients’ satisfaction with SMEs. The aim of the present study was therefore to explore participants’ subjective appreciation of SME programs using qualitative methods and formulate propositions based on patients’ preferences to improve ultimately clinical outcomes.
Patients and Methods: Twenty-five participants from five French SME programs to conduct focus groups were recruited. An inductive approach using grounded theory as an overall methodology orientation for the thematic analysis process has been followed. The study was reported in compliance with the consolidated criteria for reporting qualitative research criteria (COREQ).
Results: Patients expressed great satisfaction concerning the effective delivery of SME sessions. They appreciated the considerations for their concerns and needs, the adaptation of sessions’ content to their interests and questions, and learning to take care of themselves. Moreover, patients had a positive opinion on the quality of their relationship with health care providers. However, the major point of improvement of SMEs was the opportunity to repeat the program if needed, as this opportunity was not offered. This consideration was particularly salient when patients did not consider themselves autonomous for disease management at the end of the program, ie, when they had low levels of perceived self-efficacy.
Conclusion: While patients expressed great satisfaction regarding SME programs, our results suggest that some changes might be needed to make the endpoint of SME interventions coincide with the patient’s perception of self-efficacy in disease self-management and ultimately improve clinical outcomes.
Keywords: satisfaction, self-management educations, qualitative methods, patients view, self-efficacy
Introduction
According to the Centers for Disease Control and Prevention (CDC), “Self-management education (SME) refers to programs that help people who have ongoing health conditions learn how to live life to the fullest. For many people, this means to live with less stress, more energy, and a greater ability to do the things they want to do. SME programs are clinically proven to reduce symptoms and improve quality of life. SME programs help you learn strategies and develop the skills and confidence to cope with symptoms, manage fatigue, handle stress, reduce depression, communicate with doctors, manage medications, eat healthy, and be active”.1 SME can be an effective tool to cope with change in self-identity and to plan, pace and prioritize.2 Interventions can be based on health education, promotion of medical adherence, illness-related problems in everyday life, promotion of physical activities, psychological support and social counselling.3
Several studies have shown that SME interventions are beneficial for patients.4–7 These studies focused on SME outcomes, such as the acquisition of predefined knowledge or skills or quality of life.
In addition to such outcomes, we need to investigate patients’ satisfaction with the SME intervention, which depends both on clinical results and on the subjective appreciation of the intervention.8,9 Qualitative methods are particularly relevant to get a detailed understanding of patients’ subjective appreciation of SMEs. In a previous study, patients with chronic obstructive pulmonary disease or chronic heart failure who participated in a self-management program described several characteristics of the SME that are important and could have a positive impact on them:10 1) being listened to with interest and without interruption by both group leaders and fellow patients, 2) repeating issues from the previous session, 3) sharing experiences of symptom management between patients, and 4) the input of the program must be quickly transformed into actions in daily life. Another study explored how patients with chronic inflammatory polyarthritis described coping with their disease after following a patient education program and compared these experiences to those of patients in a control group who did not receive any education. Results showed that patients who attended the educational program expressed a better confidence to cope with their symptoms. They also better knew how to initiate changes in health behaviours. Moreover, they were more confident about taking their medications as prescribed because they had gotten a deeper understanding of beneficial effects and more knowledge about possible side effects.11
A few studies with qualitative exploration addressed effective elements of SME programs from the patients’ perspective. They illustrated the perceived key components: eg the need for a supportive environment with other patients11,12 or with health care providers, 13 shared responsibility for healthcare, guided discovery and non-didactic communication and practice.14
To the best of our knowledge, no study has already explored patients’ satisfaction with the characteristics of different SME programs. However, such data are crucial to help formulate self-management propositions based on patients’ preferences and optimize clinical outcomes.15
The present study is part of the Classification of Patient Therapeutic Education Programs Components (CONCErTO) project with the objective of identifying the institutional, organizational, pedagogical, psychosocial, medical and individual preference elements affecting the outcome, participation and sustainability of SME programs (ClinicalTrials.gov Identifier: NCT02717182).
Materials and Methods
Design
A qualitative study reported in compliance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) criteria.16
Study Population and Sampling
SME Program Selection
Sample heterogeneity is essential to capture comprehensive and diverse data in depth.17 To construct a maximum variation sampling, we identified three key elements of variation in programs: diseases of interest, hospital or nonhospital programs and urban or rural programs.
For the entire CONCErTO project, we chose 12 programs among the Lorraine regional health agency‐authorized programs (Est of France with a population of over 2 million inhabitants). Diseases addressed by the different SME programs were digestive cancers (n = 2), cardiovascular diseases (n = 1), kidney failure (n = 2), asthma (n = 1), chronic pain (n = 1), multiple sclerosis (n = 1), hepatitis (n = 1), diabetes obesity (n = 2) and multiple pathology (n = 1).
The list from the regional health agency included the name and contact information of the program SME coordinator (public data). Agreement to participate was obtained from the SME coordinators after informing them of the objectives and process of the CONCErTO project. No coordinator refused to participate in the study.
Participants and Recruitment
Among the 12 programs included in the Lorraine region for the CONCErTO project, we selected five programs to conduct patient focus groups. Our aim was to meet the maximal variation criteria of our sample strategy. No program refused to organize patient recruitment (see the paragraph participants below).
Description of the five selected programs:
- Disease of interest: Asthma (n = 1), cardiovascular diseases (n = 1), diabetes/obesity (n = 2), multiple pathology (n = 1)
- Institutional context: Nonhospital programs (n = 3), hospital programs (n = 2)
- Geographical location: Rural programs (n = 3), urban programs (n = 2)
Coordinators from each of the five selected programs sent a call for volunteers in the form of a letter that the project team wrote. The letter explained the project, specified the date and time of the proposed focus group, and presented the 35-euro gift certificate offered to volunteers. At the patients’ level, our sample was a convenience sample. Groups were set up by pathology, without selecting patients based on other criteria, particularly socio-demographic criteria.18 We pursued recruitment via mail reminders until we received at least five patients’ favorable responses for participation.
Data Collection
We conducted focus groups with patients who followed a complete SME program. Focus group exchanges are frequently used to gain an in-depth understanding of a phenomena of interest.19
Focus groups are relevant for bringing together participants with a shared experience on which they can exchange.20 Focus groups emphasize on interactions between participants instead of exchanges between the researcher and the participants.21
Face-to-face focus groups were conducted where programs took place by an experienced female health PhD psychologist (XX) and a female experienced PhD sociologist (XX) from November 2019 to November 2022. No one else was present besides the participants and the researcher during the focus groups. With one exception in one of the programs Diabetes/Obesity, the presence of an administrative officer was needed. The researchers did not have any relationship with participants before the start of the study. The duration of the focus groups was approximately an hour and a half.
Each participant agreed to participate after a short presentation of the CONCErTO project (see the ethics paragraph).
Focus groups were integrally audio-recorded and transcribed.
Qualitative studies can reach saturation from four to six focus groups.22,23 With narrowly defined objectives, as is the case in our study, saturation can be achieved with a relatively small sample size.24
A clinician/epidemiologist (XX), a sociologist (XX) and a psychologist (XX) designed an interview guide during three meetings. The questions asked were designed to explore in-depth the three main drivers of satisfaction with SME intervention. Box 1 presents some illustrative in-depth questions.
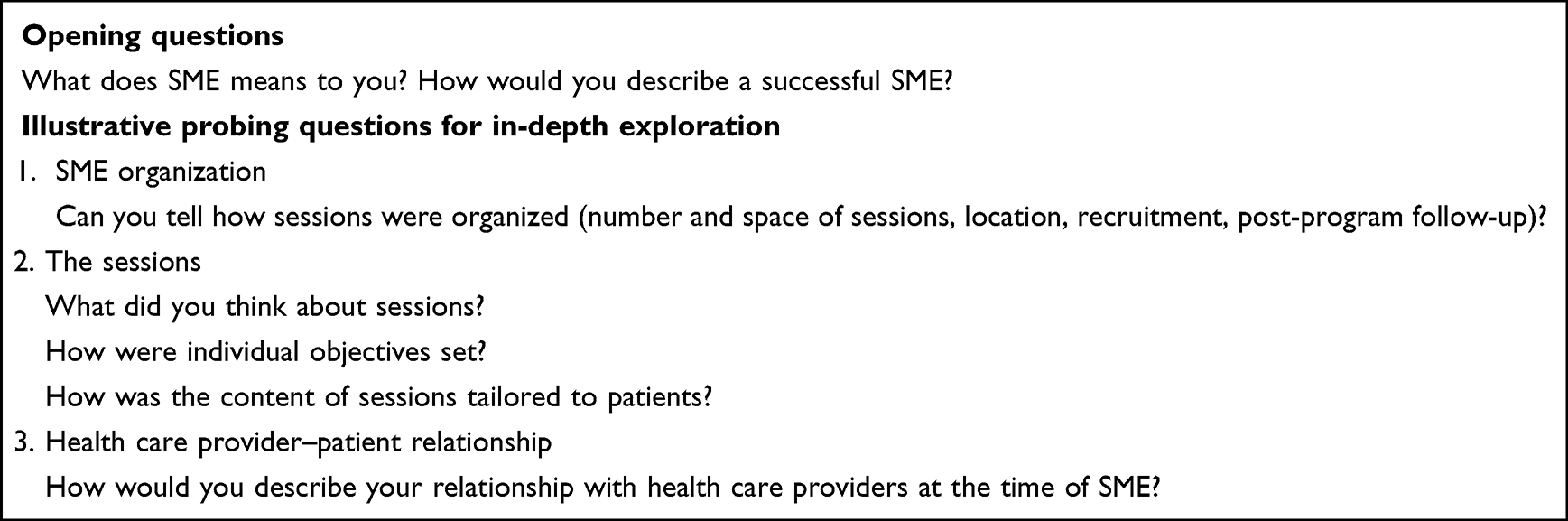 |
Box 1 Interview Guide for Questions on Main Satisfaction Factors About SME |
Data Analysis
We followed a general inductive approach to identify themes from the participant discourse to properly capture their perception about satisfactory factors in SMEs using grounded theory as an overall methodology orientation for the thematic analysis process.25 In this approach, the researchers read the raw data to generate categories of analysis (without a priory expectation) and thus allow the theory to emerge.26 A health psychologist (XX) read the transcriptions and proposed a draft of a coding grid that was refined during a meeting with the clinician/epidemiologist (XX).
Data analysis was performed using NVivo v11.
Study Rigor
In 2022, we worked with a physician (XX) in a research-training year to develop the coding grid. The physician and the health psychologist encoded all the material together. Disagreement between the two coders was resolved by discussion, and the final kappa value was 0.83.
Results
Participants
Twenty-five patients participated in five focus groups. Table 1 shows a large diversity of patients’ profiles since we included men and women, from 55 to 78 years old, from lowest to highest level of education and with marital and single life. For variation in SME program characteristics, see “Description of the five selected programs”.
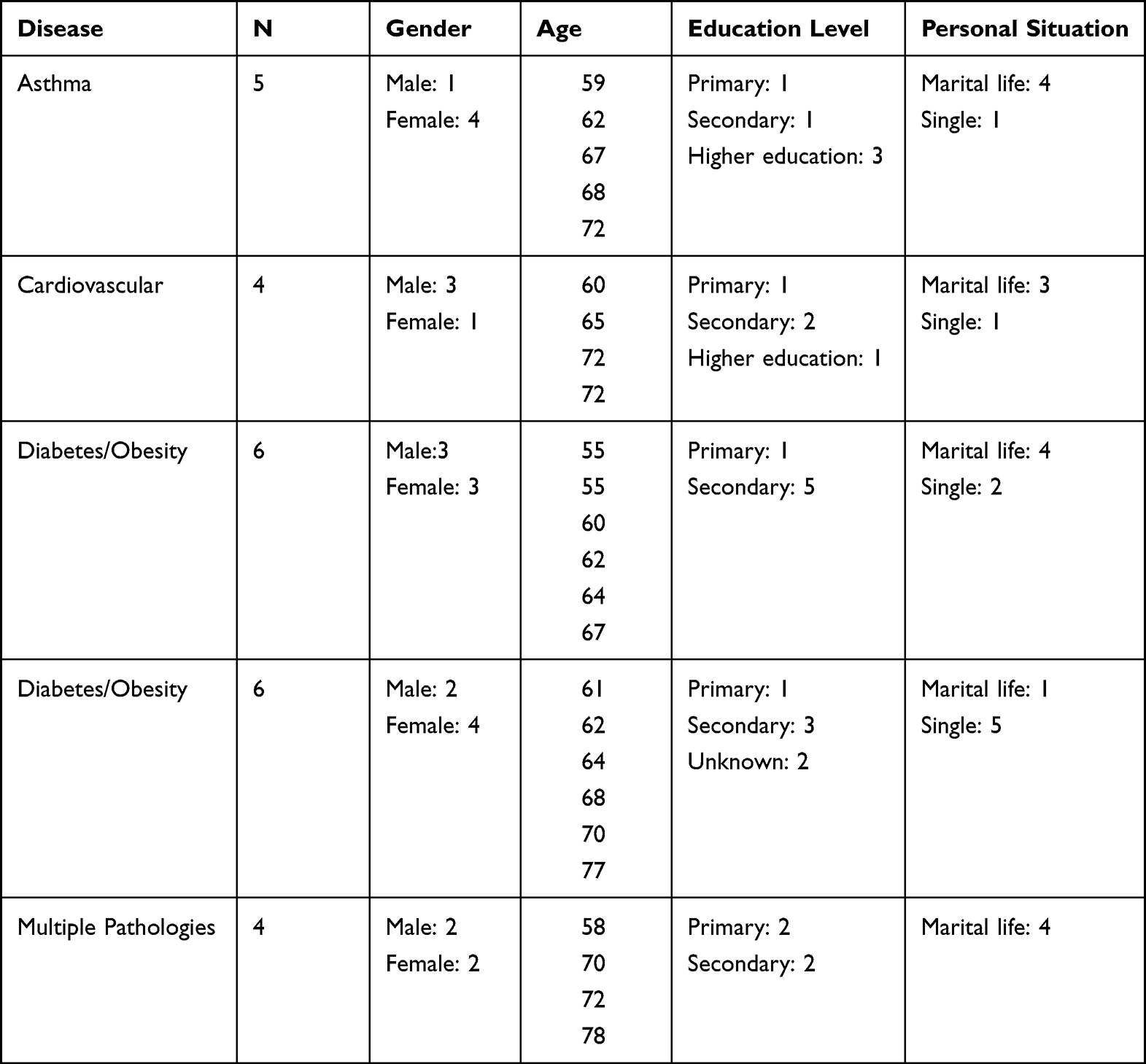 |
Table 1 Description of the Focus Group Participants per SME Program |
Table 2 shows the subthemes declination for the three themes of factors affecting satisfaction in SMEs.
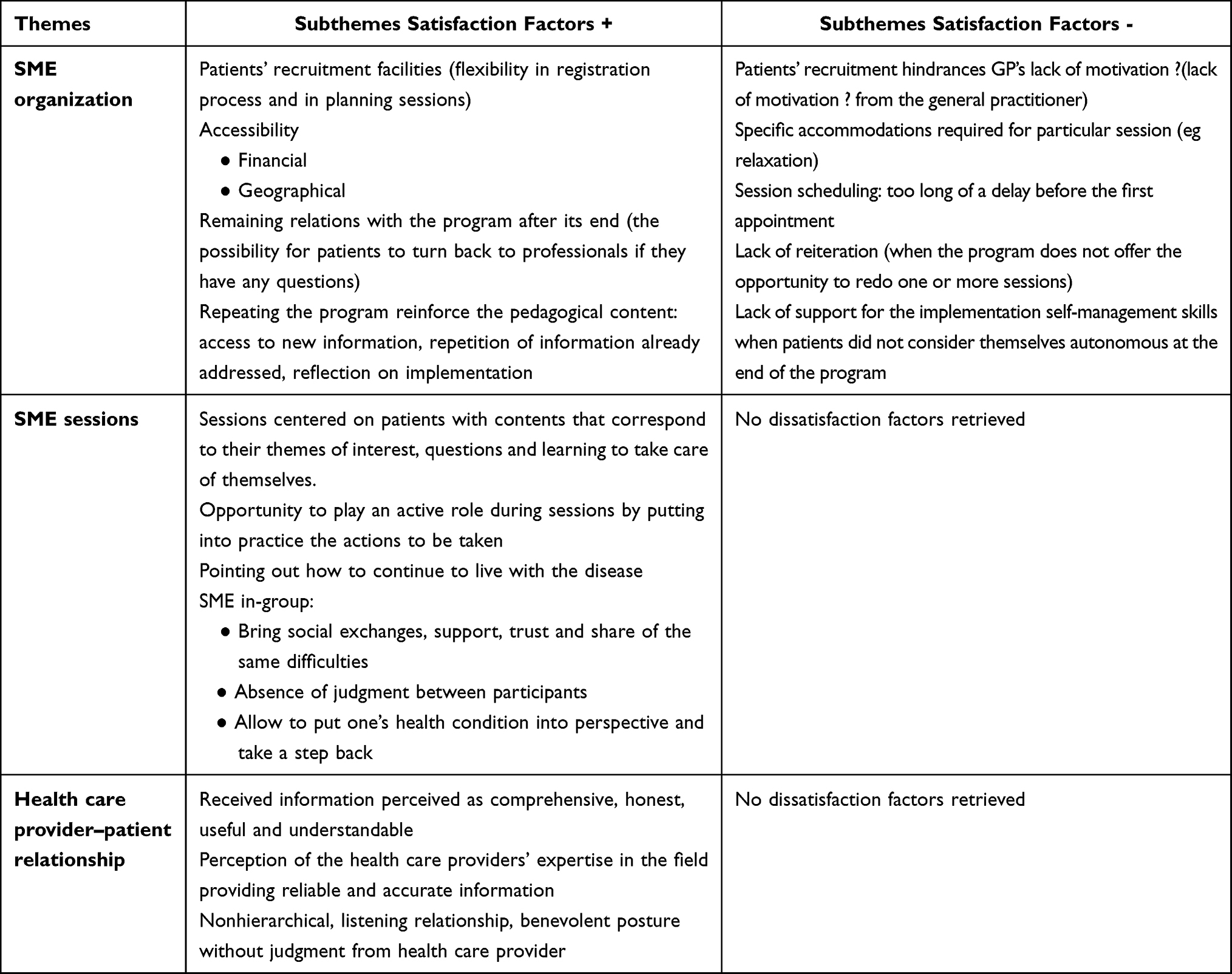 |
Table 2 Synthesis of Themes and Subthemes Retrieved from Qualitative Analysis Related to Factors Affecting Satisfaction in SMEs |
Globally, the analysis of focus group data with patients revealed great satisfaction with SMEs, particularly concerning effective delivery sessions and relationships with health care providers. However, some areas for improvement remain at the organizational level of SMEs.
Theme 1: Satisfaction Factors About SME Organization
Patient Recruitment
There are two main ways for patients to be recruited in SME: after a hospitalization for hospital programs and via the general practitioner for nonhospital programs.
For patients in nonhospital programs, lack of knowledge, omission or will from general practitioners hinder the recruitment process.
I wonder if the doctors are convinced by what exists there. Because I go to see my doctor and I tell him “is there a medical prescription for sport?” (...) and then I look above him, there was a small poster and I show him and he says “ah but yes, that’s [The program]. (Participant 17, Female, 77 years old)
An easy registration process and flexibility of the sessions are satisfactory elements.
Once we filled out our registration form, it was easy. Everything falls into place. We register for the sessions where we want, or where we can. (Participant 12, Female, 55 years old)
Accessibility
Financial
Patients appreciated the free-of-charge program, as it may have not been affordable otherwise.
The good thing is that it’s free. This is important for low income people. (Participant 14, Male, 55 years old)
Even if you are not in the lowest income bracket, there is relaxation. You have to sign up for relaxation; there is gym, you have to sign up for the cardio gym; there is walking, you have to join a walking club; there is psychology, you have to pay for the psychologist, which is not reimbursed by social security (...). The diet, you have to pay for the diet. You add all that up at the end, it adds up to a certain price. Personally, I would not have been able to do all that if it hadn’t been free. (Participant 12, Female, 55 years old)
There is also the fact that it’s free, that is a positive for us, because each of us has different means, so this chance to have access to that for free. Wow! (Participant 21, Male, 61 years old)
Geographical
A rural program proposed sessions spread over a vast territory. Sessions next to patients’ homes facilitate their participation. Nevertheless, this modality has an unexpected effect since sessions are no longer chosen on the basis of their content but also on the basis of the distance from home.
People go according to where the sessions are located, which also plays a role. (Participant 12, Female, 55 years old)
Physical Environment
Patients pointed out that some particular sessions required specific premises accommodations.
If we wanted to do relaxation, [the room] was too small. (Participant 13, Male, 60 years d)
The sound insulation (…) you make a session of relaxation, but you hear all that occurs next door. (Participant 11, Female, 62 years old)
Session Scheduling
Too long of a delay before the first appointment far in the future may discourage patients.
I find that the appointments are long term, too long term, that is to say that when we have an appointment for a session, it takes often 3 months (...) I find that for our personal organization, I don’t like to have long term things like that. (Participant 17, Female, 77 years old)
Availability of the Team After Program Ending
The program does not always end formally, and patients can turn back to professionals when questions arise.
Anyway, when I need something I ask them. (Participant 2, Female, 59 years old)
It’s true that I don’t come back because I don’t need it, but if I had to ask for advice, they would listen to me. (Participant 3, Female, 62 years old)
Repeating the Program
It is interesting to note that when programs do not systematically provide for reiterations, participants regret it and call for it. However, when programs provide for this opportunity, participants emphasize its value. For them, the perceived interest lies in the reinforcement of the pedagogical contents: access to new information, repetition of information already addressed reflection on implementation.
It’s been almost two times that I’ve done 4 sessions (...) Well, because I’m interested, we always learn [something], already in terms of nutrition. (Participant 9, Male, 60 years old)
This is also good because, once we did a session on fats and then we schedule another one in 6 months, well there are things that we forgot so it’s good to come back to it [the program]. (Participant 11, Female, 62 years old)
And then put us back in the bath, by saying well you know, you knew that but you don’t apply maybe do it [a session] again. (Participant 22, Female, 77 years old)
Regret of a Lack of Reiteration
Patients often regretted when the program does not offer the opportunity to redo one or more sessions of the program.
No but I don’t say follow up, follow through but do it [a session] from time to time. (Participant 24, Male, 72 years old)
A refresher course. (Participant 25, Male, 70 years old)
Yes, doing it from time to time (...) yes because you forget quickly. (Participant 24, Male, 72 years old)
Once, twice, three times and when she told us, well, here it is [the end], I thought it was a long-term thing. (Participant 2, Female, 59 years old)
Lack of Support for the Implementation of Their Self-Management Skills at the End of the Program
Patients sometimes did not consider themselves autonomous for disease management at the end of the program and would have liked to be supported in pursuing the actions they had initiated in real life (outside of the program).
There is not enough continuity; for example, for sports, Mrs. X indicates us an association, which makes sports, but it is true that we return in the world. I followed that, we return in the world a little bit normal and there we are not, we feel uh… (Participant 21, Male, 61 years old)
Yeah, we’re not seasoned enough to get out of it [the program] yet actually. (Participant 18, Female, 70 years old)
We are like in a kind of cocoon, we are with people who have medical problems and when we go to a club, in a thing like that, well for example, we will find ourselves with little girls with tights and everything, uh… (Participant 17, Female, 77 years old)
Absolutely, we’ll get it, we’ll get it. (Participant 18, Female, 70 years old)
Theme 2: Satisfaction Factors About the SME Sessions
Sessions as Patient-Centered
Patients appreciated the patient-focused sessions with content relevant to their interests, questions and learning to take care of themselves.
They [health care providers] answer your questions truly well and they reassure you, they explain well, they truly take the person into account. (Participant 4, Female, 68 years old)
What is also good is that in the group sessions, we propose a theme. If we have encountered a difficulty, if we have a question, it can be the idea of a session. (Participant 10, Female, 64 years old)
As you are in the menus, it’s the same, for example, there is a recipe that I saw in a cookbook, any cookbook, and I like it, but I said to myself, yeah, but I put this, my diet, it’s not good, there is too much fat and so on. I can bring my recipe [to a session], and we adapt it. (Participant 11, Female, 62 years old)
I would say that it [SME] refocuses us on ourselves, all these sessions, these health care providers refocus us on ourselves, we have spent a lifetime working, not taking care of ourselves and here, we focus on ourselves (...) to put words and find ourselves refocused on ourselves, we come back, we talk about us as a person, we are able to manage ourselves much better. (Participant 21, Male, 61 years old)
Be an Active Actor During Sessions
Patients expressed the need to put into practice what was being said, and to learn how to change things and be an actor.
When we cook with the diet, we don’t just cook, we have sessions, she [the diet] gives us a classic menu, and it’s up to us to break it down to adjust it to people who are diabetic or overweight. We reduce, we change the flour by if the fruits by that, we work a little bit anyway. (Participant 15, Male, 67 years old)
Having Plans, Continuing to Live with the Disease
Patients appreciated the program’ focus on how to manage their disease in order to live their life to the full.
That it was a chronic disease but that it was not the reason why we could not continue to live normally. Doing sports, going on holydays, swimming, skiing, that’s it. So I learned a lot of things. (Participant 2, Female, 59 years old)
SME In-Group
Activity in-group is satisfactory and brings social exchanges, support, trust and sharing of the same difficulties.
It is a sharing; we receive something from a person. (Participant 9, Male, 60 years old)
Yeah, you meet people who have the same pathologies as us, so that helps too. More or less because we are not all the same thing. (Participant 15, Male, 67 years old)
And then, there are people who don’t know how to cook at all and one of us will go to him or her and help him or her and that’s how we do it (...) Ah yes, even if we don’t know each other, everyone is nice to each other, we are like a little family. (Participant 15, Male, 67 years old)
It’s like in a cocoon, we know we all have problems so we’re with each other, it’s the togetherness that gives us confidence and that’s important and it’s truly carried by the health care providers. (Participant 21, Male, 61 years old)
The group also provides a space for patients to share tips.
It’s good because we share with others, we are not alone in the same situation, we can give each other tips, advice. (Participant 10, Female, 64 years old)
It is the exchange, the advice that one will give the advice that the other will give. (Participant 22, Female, 77 years old)
The basis of a satisfactory group session is the absence of judgment between participants.
You don’t feel judged. That’s what’s important. (Participant 15, Male, 67 years old)
Group sessions help to put one’s health condition into perspective and take a step back.
It’s also true that when you’re with people who have different problems, you say to yourself: you’re nothing compared to the others, we’re positive, when you complain there are others who are worse than you. (Participant 20, Male, 62 years old)
No patient highlighted any negative aspect concerning group sessions.
Theme 3: Satisfaction Factors About Health Care Provider–Patient Relationship
Received Information
Patients perceive received information as comprehensive, honest, useful, and understandable. Health care providers help patients raise awareness of the disease (its consequences and how to manage it).
We come with questions and we have answers. (Participant 21, Male, 61 years old)
Honest answers, because when you go to your doctor, you don’t have time. (Participant 17, Female, 77 years old)
However, I wasn’t aware of it, but for the past month I’ve been aware that asthma can kill you. (Participant 3, Female, 62 years old)
Even if you don’t understand something, you can always go see Mrs X, she has open arms. (Participant 24, Male, 72 years old)
Perception of Health Care Providers’ Expertise in the Field
For patients, health care providers provided reliable and accurate information.
It’s done by professionals, they know what they’re talking about, they have the experience of all the people who came before, for me it’s all positive. I don’t see any improvements (...) and what’s good with the nurse is that I can ask questions that I don’t ask in a doctor’s office. On tests, they can read a test result as well as a doctor. (Participant 17, Female, 77 years old)
Nonhierarchical, Listening Relationship, Benevolent Posture without Judgment from Health Care Providers
Patients felt recognized as part of a balanced and mutually respectful relationship with healthcare providers.
Everyone is simple, there is no, I don’t know how to say it, no fuss. (Participant 15, Male, 67 years old)
It’s true that it’s important, we’re all on the same level and no one is crushing you. (Participant 11, Female, 62 years old)
Oh yes, it’s true that they have a smile, they [health care providers] are simple so we feel at ease right away. (Participant 13, Male, 60 years old)
Yes, they [health care providers] are at our level, they listen to us (...) There is no real barrier between them and the patient, they are open, they are natural. (Participant 4, Female, 68 years old)
They [health care providers] know, we respect them. If someone gets out of line, they are able to put them back without aggression, without putting them down in front of everyone. (Participant 15, Male, 67 years old)
The health care providers don’t judge us. (Participant 11, Female, 62 years old)
They [health care providers] are very attentive. I see, even the gym sessions, cardio if you cannot do. I have a bad back, we are not judged, we are not forced. (Participant 15, Male, 67 years old)
They [health care providers] don’t tell me “you must”, they accept our limits. (Participant 10, Female, 64 years old)
Discussion
Patients expressed overall great satisfaction, particularly concerning effective delivery of the sessions and their content.
In addition, our results highlighted that patients significantly preferred a centered approach through a perceived tailored SME intervention27 with considerations of their concerns and needs and contents that corresponded to their themes of interest, their questions and learning to take care of themselves. A previous systematic review showed that personalized care improves patients’ capability to self-manage their chronic condition when compared to usual care.28 Qualitative studies conducted during development of SME programs or to assess their feasibility have also highlighted the need to develop patients centered SME programs.29–31 Patient-centeredness is increasingly perceived as crucial in health policies.32 A scoping review showed that although authors often claimed their intervention to be patient-centered, no specific tools are generally used to implement patient-centered interventions, highlighting that health care providers encounter difficulties in adopting this approach.33
Moreover, patients positively estimated the quality of their relationship with health care providers in the context of SMEs. Participants appreciated that health care providers communicated in an attentive and nondidactic style. They cared about participants, provided understanding and commitment, created the conditions of a secure and supportive environment and facilitated the condition and the belief that the disease would be manageable.34,35
The major point of improvement of SMEs was the opportunity to repeat the program if needed when this opportunity was not offered. This consideration was particularly salient when patients did not consider themselves autonomous for disease management at the end of the course, ie, with a lack of perception of self-efficacy. For Chan (2021), self-efficacy is a key determinant of chronic disease self-management, and “Patients with high self-efficacy in coping with their chronic diseases reflect a perceived ability to manage challenges related to their diseases and a sense of control over their lives”.36 Our analysis of the main factors affecting satisfaction with SME interventions in a transversal way (ie, with several programs included) allowed us to conduct a reflection on the SME considered a health service. We are able to state that to optimize clinical outcomes, the endpoint of SME interventions should coincide with the patient’s perception of self-efficacy in disease self-management. In our results, the maintenance of the link with the SME program could take two major forms: an informal form with the opportunity to call health care providers from the SME program when questions arise and a formal form with the opportunity to participate in a new round of the program.
Limitations
A major criticism addressed to inductive thematic analysis is that interpretation of the researcher depends on their own perception and perspective however, prior knowledge and expectations is inevitable.25 The analysis done by coders can limit this drawback. In our study, we calculated the amount of agreement between two coders having two different background (a physician and a health psychologist) to provide sound interpretation of data.37
Besides, we based our sampling strategy at the patients’ level on a convenience sample of volunteers that “may not provide participants who can supply the best information (Gill, 2020)”.18 However, with a voluntary sample, we recruited 25 patients from 55 to 78 years old in five SME programs. Since the prevalence of chronic disease increases with age, our sample is necessarily composed of an older population. However, we did not succeed in integrating “young” participants with high family and professional constraints, which would have allowed us to capture their perceptions of programs’ capabilities to take into account responsibilities generally assumed by younger patients. Data collection in the context of inductive thematic analyses occurs until saturation point25 We estimated sample size based on literature.22,23 However, we did not assess and report thematic saturation using a calculation approach such as the one proposed by Guest et al.38
Patients appreciated group sessions, which brought social exchanges, support, trust and sharing of the same difficulties. It is, however, difficult to draw any conclusion based on our results since patients who participated in our focus groups were volunteers to take part in an exchanges in-group and thus were compliant with this modality of organization. Let us remember that SME interventions in France mostly proposed as in-group sessions.
In focus groups, attention must be paid to the internal heterogeneity (in terms of genders, for example) of the groups that may condition an inequality in the participation of participants.20 In our study, the researchers were both experienced in qualitative data collection and aware of issues concerning focus groups management.
Conclusion
While patients expressed great satisfaction regarding SME programs, our results suggest that to optimize outcomes of SME, programs should integrate the need to inquire patient’s perception. Particularly self-efficacy in disease self-management in order to adapt delivered support in case of lack of perceived autonomy.
Ethics Approval and Informed Consent
The protocol was approved by the Comité de Protection des Personnes (CPP (Sud Est 1)) (no. ID‐RCB: 2017‐A00247‐46, CPP no.: 2017‐12). Prior to begin focus groups, oral and written consent was obtained, including publication of anonymized quotes. Participants were invited to ask any questions they might have wanted before starting the exchanges.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the French Ministry of Health (Programme de Recherche sur la Performance du système de Soins (PREPS). The funding agency played no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; the decision to submit for publication or preparation, review or approval of the manuscript for publication.
Disclosure
Professor Anne-Christine Rat reports personal fees and/or non-financial support from Pfizer, Lilly, Sanofi, BMS, AbbVie, Galapagos, Novartis, Sandoz, Biogen, and Chugai, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. What is self-management education? | Self-management education: learn more. Feel better. CDC; 2018. Available from: https://www.cdc.gov/learnmorefeelbetter/sme/index.htm.
2. Kralik D, Koch T, Price K, Howard N. Chronic illness self-management: taking action to create order. J Clin Nurs. 2004;13(2):259–267. doi:10.1046/j.1365-2702.2003.00826.x
3. Meng K, Musekamp G, Schuler M, et al. The impact of a self-management patient education program for patients with chronic heart failure undergoing inpatient cardiac rehabilitation. Patient Educ Couns. 2016;99(7):1190–1197. doi:10.1016/j.pec.2016.02.010
4. Tran SHN, Weaver RG, Manns BJ, et al. Factors affecting the reception of self-management health education: a cross-sectional survey assessing perspectives of lower-income seniors with cardiovascular conditions. Patient Prefer Adherence. 2022;16:971–981. doi:10.2147/PPA.S351459
5. Conn VS, Hafdahl AR, Brown SA, Brown LM. Meta-analysis of patient education interventions to increase physical activity among chronically ill adults. Patient Educ Couns. 2008;70(2):157–172. doi:10.1016/j.pec.2007.10.004
6. Stenberg U, Haaland-Øverby M, Fredriksen K, Westermann KF, Kvisvik T. A scoping review of the literature on benefits and challenges of participating in patient education programs aimed at promoting self-management for people living with chronic illness. Patient Educ Couns. 2016;99(11):1759–1771. doi:10.1016/j.pec.2016.07.027
7. Lagger G, Pataky Z, Golay A. Efficacy of therapeutic patient education in chronic diseases and obesity. Patient Educ Couns. 2010;79(3):283–286. doi:10.1016/j.pec.2010.03.015
8. Sitzia J, Wood N. Patient satisfaction: a review of issues and concepts. Soc Sci Med. 1997;45(12):1829–1843. doi:10.1016/S0277-9536(97)00128-7
9. Haute Autorité de Santé. Qualité des soins perçue par le patient - Indicateurs PROMs et PREMs: panorama d’expériences étrangères et principaux enseignements [Patients' perception of quality of care - PROMs ans PREMs indicators: overview of foreign experiences and key lessons]. Available from: https://www.has-sante.fr/jcms/p_3277049/fr/qualite-des-soins-percue-par-le-patient-indicateurs-proms-et-prems-panorama-d-experiences-etrangeres-et-principaux-enseignements.
10. Luhr K, Holmefur M, Theander K, Eldh AC. Patient participation during and after a self-management programme in primary healthcare - The experience of patients with chronic obstructive pulmonary disease or chronic heart failure. Patient Educ Couns. 2018;101(6):1137–1142. doi:10.1016/j.pec.2017.12.020
11. Grønning K, Midttun L, Steinsbekk A. Patients’ confidence in coping with arthritis after nurse-led education; a qualitative study. BMC Nurs. 2016;15(1):28. doi:10.1186/s12912-016-0150-x
12. Bourgault P, Lacasse A, Marchand S, et al. Multicomponent interdisciplinary group intervention for self-management of fibromyalgia: a mixed-methods randomized controlled trial. PLoS One. 2015;10(5):e0126324. doi:10.1371/journal.pone.0126324
13. Dures E, Kitchen K, Almeida C, et al. “They didn’t tell us, they made us work it out ourselves”: patient perspectives of a cognitive-behavioral program for rheumatoid arthritis fatigue. Arthritis Care Res. 2012;64(2151–4658):494–501. doi:10.1002/acr.21562
14. Dager TN, Kjeken I, Fjerstad E, Hauge MI. “It is about taking grips and not let myself be ravaged by my body”: a qualitative study of outcomes from in-patient multidisciplinary rehabilitation for patients with chronic rheumatic diseases. Disabil Rehabil. 2012;34(11):910–916. doi:10.3109/09638288.2011.626485
15. Jia L, Hu Y. Self-management about adjuvant therapy in breast cancer survivors: a qualitative study. Patient Prefer Adherence. 2022;16:2663–2681. doi:10.2147/PPA.S379435
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
18. Gill SL. Qualitative sampling methods. J Hum Lact. 2020;36(4):579–581. doi:10.1177/0890334420949218
19. Nyumba TO, Wilson K, Derrick CJ, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Methods Ecol Evol. 2018;9(1):20–32. doi:10.1111/2041-210X.12860
20. Busetto L, Wick W, Gumbinger C. How to use and assess qualitative research methods. Neurol Res Pract. 2020;2(1):14. doi:10.1186/s42466-020-00059-z
21. Baillie L. Exchanging focus groups for individual interviews when collecting qualitative data. Nurse Res. 2019;27(2):15–20. doi:10.7748/nr.2019.e1633
22. Hennink MM, Kaiser BN, Weber MB. What influences saturation? Estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
23. Guest G, Namey E, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes. Field Methods. 2017;29(1):3–22. doi:10.1177/1525822X16639015
24. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
25. Chapman AL, Hadfield M, Chapman CJ. Qualitative research in healthcare: an introduction to grounded theory using thematic analysis. J R Coll Physicians Edinb. 2015;45(3):201–205. doi:10.4997/JRCPE.2015.305
26. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
27. Ricci L, Villegente J, Loyal D, Ayav C, Kivits J, Rat AC. Tailored patient therapeutic educational interventions: a patient-centred communication model. Health Expect. 2022;25(1):276–289. doi:10.1111/hex.13377
28. Coulter A, Entwistle VA, Eccles A, Ryan S, Shepperd S, Perera R. Personalised care planning for adults with chronic or long‐term health conditions. Cochrane Database Syst Rev. 2015. doi:10.1002/14651858.CD010523.pub2
29. Wendebourg MJ, Feddersen LK, Lau S, et al. Development and feasibility of an evidence-based patient education program for managing fatigue in multiple sclerosis: the “Fatigue Management in MS” Program (FatiMa). Int J MS Care. 2016;18(3):129–137. doi:10.7224/1537-2073.2014-105
30. Ammerlaan JW, van Os-Medendorp H, de Boer-Nijhof N, et al. Preferences and needs of patients with a rheumatic disease regarding the structure and content of online self-management support. Patient Educ Couns. 2017;100(3):501–508. doi:10.1016/j.pec.2016.10.009
31. Hilow HJ, Whibley D, Kratz AL, Ghanbari H. A focus group study to inform design of a symptom management intervention for adults with atrial fibrillation. Cardiovasc Digit Health J. 2021;2(5):246–255. doi:10.1016/j.cvdhj.2021.09.001
32. Zill JM, Scholl I, Härter M, Dirmaier J. Which dimensions of patient-centeredness matter? - Results of a web-based expert delphi survey. PLoS One. 2015;10(11):e0141978. doi:10.1371/journal.pone.0141978
33. Lafontaine S, Bourgault P, Girard A, Ellefsen E. Dimensions, application, and outcomes of person-centered self-management interventions for those living with type 2 diabetes: a scoping review. Patient Educ Couns. 2020;103(10):1961–1982. doi:10.1016/j.pec.2020.06.020
34. Dures E, Hewlett S, Ambler N, Jenkins R, Clarke J, Gooberman-Hill R. A qualitative study of patients’ perspectives on collaboration to support self-management in routine rheumatology consultations. BMC Musculoskelet Disord. 2016;17:17. doi:10.1186/s12891-016-0984-0
35. Zangi HA, Ndosi M, Adams J, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015;74(6):954–962. doi:10.1136/annrheumdis-2014-206807
36. Chan SWC. Chronic disease management, self-efficacy and quality of life. J Nurs Res. 2021;29(1):e129. doi:10.1097/JNR.0000000000000422
37. MacPhail C, Khoza N, Abler L, Ranganathan M. Process guidelines for establishing intercoder reliability in qualitative studies. Qual Res. 2016;16(2):198–212. doi:10.1177/1468794115577012
38. Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. 2020;15(5). doi:10.1371/journal.pone.0232076
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.