Back to Journals » Clinical Ophthalmology » Volume 19
Patient Reported Visual Outcomes, Dry Eye Symptoms, and Satisfaction Following Topography-Guided LASIK
Authors Brunson PB, Mann II PM, Hall B ![]()
Received 22 May 2025
Accepted for publication 2 September 2025
Published 12 September 2025 Volume 2025:19 Pages 3363—3369
DOI https://doi.org/10.2147/OPTH.S542097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Phillip B Brunson,1 Paul M Mann II,1 Brad Hall2
1Mann Eye Institute, Houston, TX, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Phillip B Brunson, Mann Eye Institute, 5115 Fannin St Suite 1000, Houston, TX, USA, Tel +1 713 580 2500, Email [email protected]
Purpose: To assess the subjective satisfaction, visual disturbances, and dry eye symptoms following Phorcides planned Contoura topography-guided LASIK.
Methods: This was a single site, single arm, prospective study of patient reported outcomes after bilateral Phorcides planned Contoura topography-guided LASIK. Preoperative and postoperative data were collected for responses on the Patient-Reported Outcomes with LASIK Symptoms and Satisfaction (PROWL-SS) questionnaire (a lower score represented a worse outcome), Ocular Surface Disease Index (OSDI) questionnaire (a higher score represented a worse outcome), refraction, and visual acuity. Linear mixed effect models were used to compare preoperative and postoperative scores on the PROWL-SS for satisfaction, and the frequency, bothersomeness, and visual impact of glare, halo, starbursts, and double images.
Results: A total of 50 subjects completed the study. Mean age was 29.3 ± 5.0 years (range 20 to 39 years). The mean 3-month postoperative satisfaction score was 53.2 higher than the mean preoperative score (p < 0.0001). Mean 3-month postoperative scores were 7.4, 13.7, 18.0, and 29.2 higher postoperatively compared to preoperatively for double image, glare, halo, and starburst, respectively. All differences were significant (p < 0.0001) with the exception of double image. Mean score on the OSDI questionnaire was 27.0 ± 22.4 preoperatively, compared to 7.5 ± 6.7 at 3 months postoperatively (p < 0.0001). Postoperatively, 97% of eyes (90/100) had MRSE within ± 0.5 D and postoperative residual astigmatism was ≤ 0.5 D in 96% of eyes (96/100). Postoperative UDVA was 20/20 or better in 98% (98/100) of eyes, 20/16 or better in 81% (81/100) of eyes, and 20/12.5 or better in 31% (31/100) of eyes.
Conclusion: The results of this study suggest improved patient reported satisfaction, reduced dry eye symptoms, and overall decrease in visual disturbances at 3 months following Phorcides planned Contoura LASIK.
Plain Language Summary: Laser in situ keratomileusis (LASIK) is a common and effective procedure to correct myopia, hyperopia, and astigmatism. Despite good refractive and visual outcomes, patients often experience the temporary complication of dry eye. Subjective questionnaires are useful to assess patient reported outcomes, including symptoms of dry eye, satisfaction, and visual disturbances before and after LASIK. However, to date there are minimal data the subjective outcomes of patients that had laser refractive surgery with the Contoura Phorcides treatment plan. The purpose of this study is to assess the subjective satisfaction, visual disturbances, and dry eye symptoms following laser refractive surgery with the Contoura Phorcides treatment plan. The results of this study suggest improved patient reported satisfaction, reduced dry eye symptoms, and overall decrease in visual disturbances following Phorcides planned Contoura LASIK.
Keywords: topography-guided LASIK, Phorcides, Contoura
Introduction
Laser in situ keratomileusis (LASIK) is a common and effective procedure to correct myopia, hyperopia, and astigmatism. Despite good refractive and visual outcomes, patients often experience the temporary complication of dry eye.1 Postoperatively, it is estimated that 50% of patients at 1 week experience dry eye symptoms, 40% at 1 month, and between 20% and 40% at 6 months.2,3 The decrease in the incidence of symptoms has led some authors to use the term Surgical Temporary Ocular Discomfort Syndrome (STODS),4 to describe the ocular surface perturbations induced by surgery. Post-LASIK dry eye is considered to be caused by a multitude of factors including corneal nerve damage during flap creation, damage to goblet cells, inflammation, and changes in corneal shape.5
One method to subjectively evaluate dry eye symptoms following LASIK is to use the Ocular Surface Disease Index (OSDI) questionnaire.6 This questionnaire asks respondents to rate their dry eye symptoms using a series of 12 questions. Responses on these 12 questions are totaled and scaled to give a final score from 0 to 100, with a lower score representative of normal and higher scores indicative of severe dry eye disease.
The Patient-Reported Outcomes with LASIK Symptoms and Satisfaction (PROWL-SS) is a subjective assessment preoperatively and postoperatively for LASIK patients.7,8 Respondents are asked to rate their satisfaction with their vision (1 question) and the frequency, bothersomeness, and visual impact of glare (8 questions), halo (8 questions), starburst (8 questions), and double image (8 questions) for a total of 33 questions. Satisfaction and each visual disturbance are evaluated using a scaled score from 0 to 100, with a higher score indicative of greater satisfaction and less frequency, bothersomeness, and visual impact of visual disturbances.
Topography-guided LASIK using the Contoura Vision procedure® (Alcon Vision, LLC) has been reported to achieve good visual outcomes for patients.9 The Phorcides Analytic Engine (Phorcides LLC), which is a proprietary surgical planning software, when combined with Contoura, may further improve results. The Phorcides Analytic Engine aids in surgical planning by utilizing geometric imaging software and optics to determine the optimal sphere and cylinder treatment.10 To date, there is minimal data on the subjective outcomes of patients that had laser refractive surgery with the Contoura Phorcides treatment plan.10–12 The purpose of this study is to assess the subjective satisfaction, visual disturbances, and dry eye symptoms following Phorcides planned Contoura topography-guided LASIK.
Methods
This was a single site, single arm, prospective study. As this study was conducted in private practice, an independent institutional review board (Salus IRB) reviewed and approved the study (approval PB-23-01). All patients provided written informed consent. This study was also registered on clinicaltrials.gov (NCT05848817), and was conducted in accordance with Good Clinical Practice (GCP), International Harmonization (ICH) guidelines, and the tenets of the Declaration of Helsinki.
Subjects were included who were candidates for uncomplicated bilateral LASIK, had treated spherical equivalent refractive errors from 0.00 to −9.00 D with maximum-treated cylinder up to 3.00 D and sphere ≤ −8.00 D treatments, had residual stromal bed thickness 250 µm or greater, and had a preoperative corrected distance visual acuity (CDVA) of 20/20 or better in each eye. Contact lens wearers were also included if they discontinued their lens wear (minimum 3 days for soft lenses and 1 month for rigid gas permeable lenses), had stable refraction, and stable keratometry readings. Subjects were excluded who had history of previous ocular surgery, topographic evidence of keratoconus or ectasia, autoimmune disease, were pregnant or nursing, had systemic disease likely to affect wound healing, such as diabetes and severe atopy, or had any ocular disease (including un-controlled dry eye) which in the investigator’s opinion would affect the outcome of refractive surgery.
One experienced surgeon performed all LASIK surgeries (PM). All flaps were created with the WaveLight FS200 (Alcon Vision, LLC) femtosecond laser, to a flap depth of 110 µm. The Wavelight EX500 laser was used for stromal ablations. A 6.5 mm optical zone was used. The treatment plan was created by integrating information from corneal topography into the Phorcides software. All patients instilled prednisolone phosphate 1% and moxifloxacin 0.5% eye drops four times daily for 5 days postoperatively.
Data were collected preoperatively and at 3 months postoperatively for refractive error, visual acuity, responses PROWL-SS questionnaire, and responses on the OSDI questionnaire. The PROWL-SS questionnaire was used to assess satisfaction with vision and the frequency, bothersomeness, and visual impact of glare, halo, starbursts, and double images. The PROWL-SS questionnaire and information about scoring are available from the American Academy of Ophthalmology Academy (https://www.aao.org/education/prowl-ss). The OSDI questionnaire was used to assess dry eye symptoms and their visual impact. The OSDI questionnaire consists of 12 questions, scored 0 to 4. The total score was determined by dividing the sum of scores by the number of questions answered, then multiplying the result by 25 to get a final score from 0 to 100. A higher score is indicative of more severe symptoms.
The primary endpoint was the percentage of subjects satisfied (defined as Completely Satisfied or Very Satisfied) with vision after Phorcides Planned Contoura LASIK compared to preoperative, based on subjective responses on the PROWL-SS questionnaire. The secondary endpoint was the percentage of eyes with postoperative MRSE ± 0.50 D. Exploratory endpoints were preoperative and postoperative subjective responses about dysphotopsias (PROWL-SS), and preoperative and postoperative OSDI scores.
All statistical analyses were performed using the software R (version 4.4.0; The R Foundation for Statistical Computing, Vienna, Austria. Linear mixed effect models, which accounted for bias from multiple measures from the same subjects, were used to compare preoperative and postoperative scores on the PROWL-SS for satisfaction, and the frequency, bothersomeness, and visual impact of glare, halo, starbursts, and double images. A p-value less than or equal to 0.05 was considered significant. The mEYEstro software (version 1.0; Total Cornea Lasik Inc, Montreal, Canada) was used to create standard plots.13 We estimated that the study would require a sample size of 46 subjects to achieve a power of 90% and a level of significance of 5%, for detecting a mean of difference of 25 points in satisfaction (using the PROWL questionnaire) between pairs, and assuming the standard deviation of the differences to be 50 points.7 To account for dropout, 52 subjects were targeted.
Results
A total of 50 subjects completed the study. Demographic and preoperative data are summarized in Table 1. There were no adverse events reported during the study.
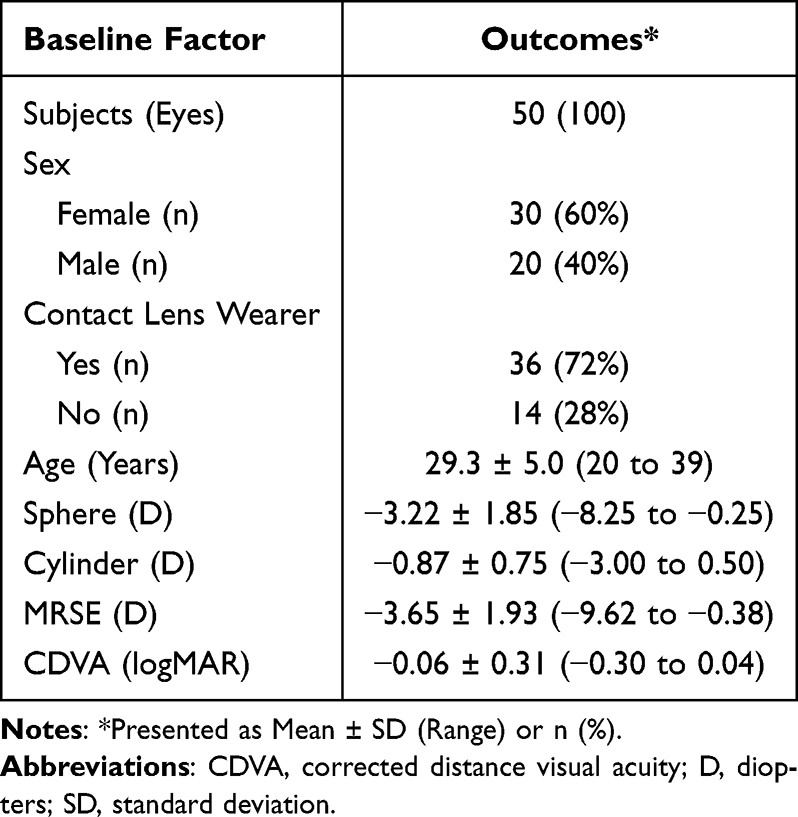 |
Table 1 Preoperative and Demographic Data |
Mean satisfaction scores on the PROWL-SS preoperatively and at 3 months postoperatively are summarized in Table 2. Higher scores are indicative of higher satisfaction and lower frequency, bothersomeness, and impact on vision for double image, glare, halo, and startburst. Mean postoperative satisfaction score was 53.2 higher than the mean preoperative score, which was significant (p <0.0001). In addition, 100% (50/50) of subjects were satisfied (Completely Satisfied or Very Satisfied) with their vision at 3 months postoperative compared to 14% (7/50) preoperatively. Mean visual disturbance scores on the PROWL-SS were improved postoperatively, compared to preoperatively. Mean differences were 7.4, 13.7, 18.0, and 29.2 for double image, glare, halo, and starburst, respectively. All differences were significant (p <0.0001) with the exception of double image. Additionally, 96% (45/47), 65% (32/49), 56% (27/48), 35% (17/49) of subjects reported Never or Rarely seeing double images, glare, halo, or starburst when wearing their best vision correction preoperatively. In contrast, 98% (49/50), 92% (46/50), 74% (37/50), 70% (35/50) of subjects reported Never or Rarely seeing double images, glare, halo, or starburst when wearing no vision correction at 3 months postoperatively. Mean score on the OSDI questionnaire was 27.0 ± 22.4 preoperatively, compared to 7.5 ± 6.7 at 3 months postoperatively (p <0.0001).
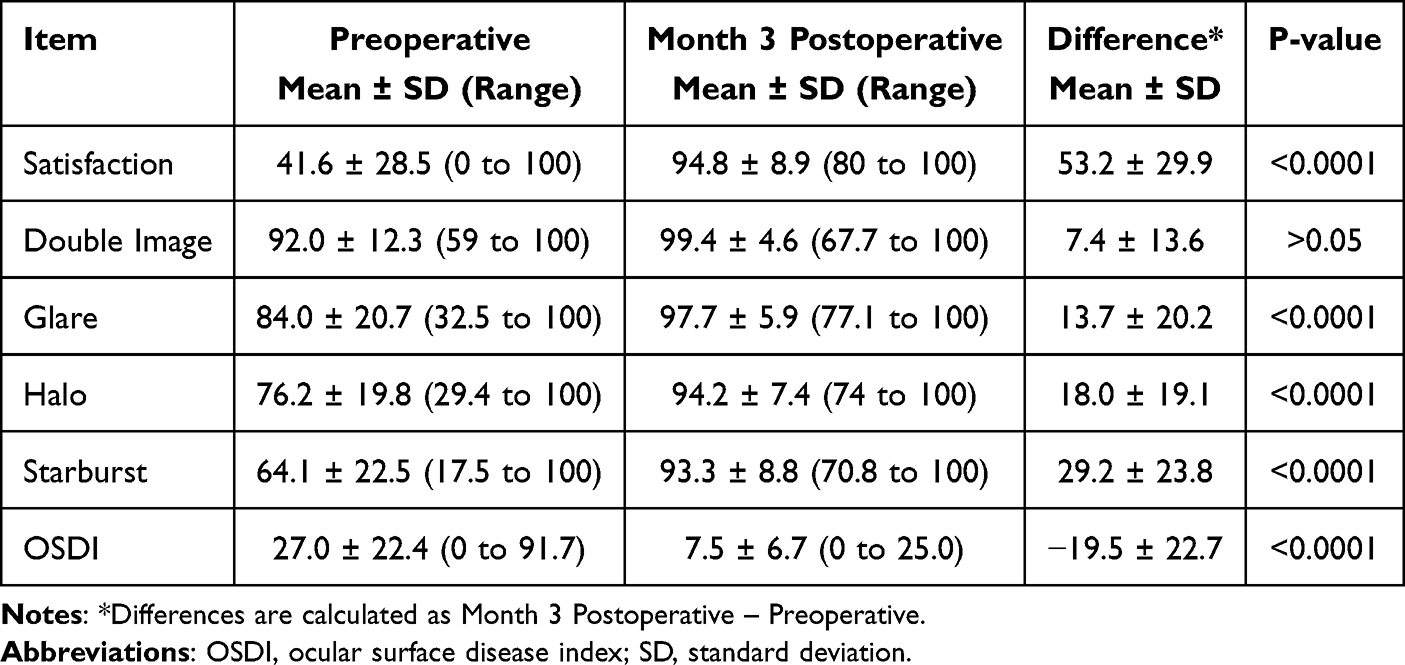 |
Table 2 Mean Scaled Scores on the PROWL-SS and OSDI Questionnaire |
Refractive and visual outcomes are summarized in Figure 1. Postoperatively, 97% of eyes (90/100) had MRSE within ± 0.5 D. Likewise, postoperative residual astigmatism was ≤ 0.5 D in 96% of eyes (96/100). Postoperative UDVA was 20/20 or better in 98% (98/100) of eyes, 20/16 or better in 81% (81/100) of eyes, and 20/12.5 or better in 31% (31/100) of eyes. In addition, 66% (66/100) eyes gained 1 or more lines of CDVA at 3 months postoperatively compared to preoperative CDVA.
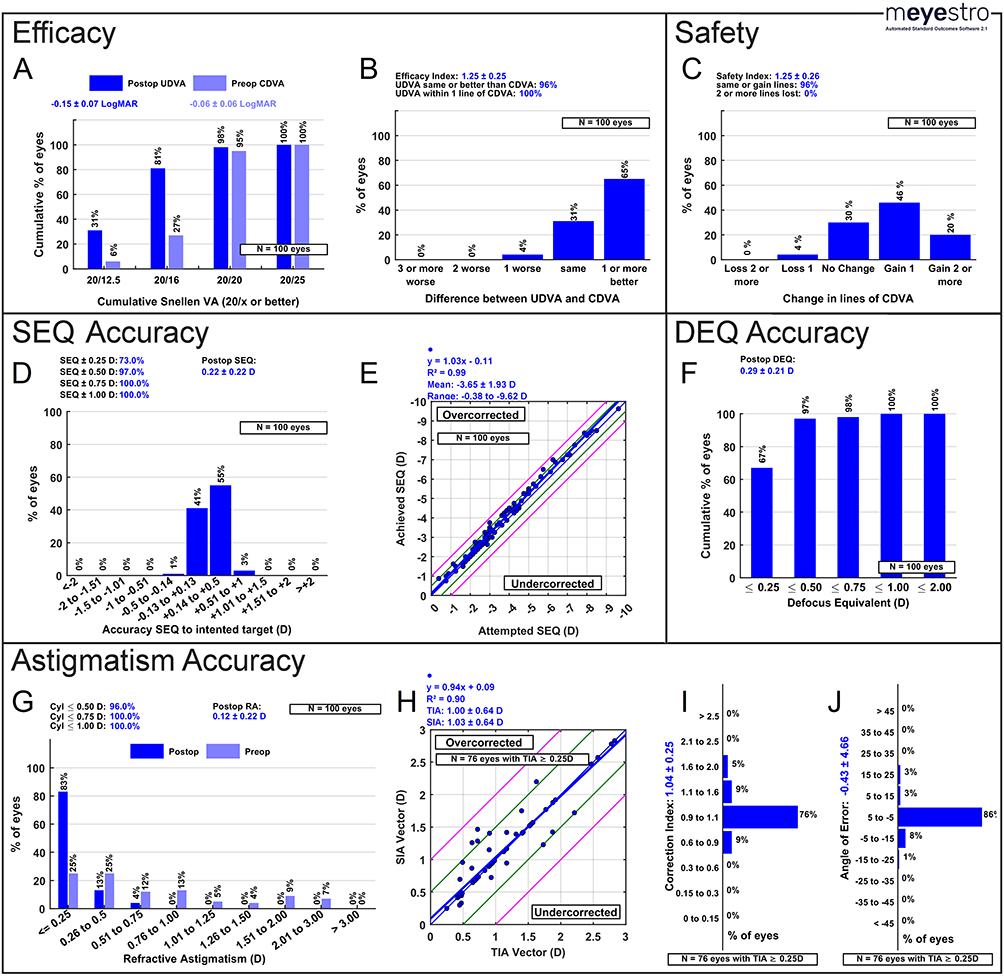 |
Figure 1 Standard plots for laser vision correction. (A) Cumulative Snellen visual acuity; (B) Difference between UDVA and CDVA; (C) Change in lines of CDVA; (D) SEQ accuracy; (E) Attempted versus achieved SEQ; (F) DEQ accuracy; (G) Distribution of astigmatism; (H) TIA versus SIA; (I) Correction index; (J) Angle of error. Abbreviations: CDVA, corrected distance visual acuity; D diopters; DEQ, defocus equivalent; SEQ, spherical equivalent; SIA, surgically induced astigmatism; TIA, target-induced astigmatism; UDVA, uncorrected distance visual acuity. |
Discussion
Dry eye symptoms following LASIK are commonly described as a side effect of the treatment.1 However, our study observed a net improvement on the OSDI questionnaire, suggesting less dry eye symptoms at 3 months post-topography-guided LASIK compared to preoperatively. Prior to surgery, the mean OSDI score was 27.0, compared to 7.5 postoperatively, which is considered within the normal OSDI range. One possible explanation is that our study included 72% contact lens wearers, which are notorious for experiencing dry eye symptoms.14 Rush et al15 also reported that subjective dry eye symptoms (Dry Eye Symptom Index score) were improved at 6 months postoperatively following topography-guided LASIK compared to preoperative. However, the authors suggested that the likely explanation was the inclusion of only eyes with healthy ocular surfaces. Ma and Manche16 also observed a decrease in mean OSDI score up to 12 months post wavefront-guided LASIK compared to mean preoperative OSDI score, but did not offer an explanation. The results of our study and others suggest a potential benefit of fewer dry eye symptoms following LASIK compared to preoperatively, and that STODS is temporary.
Another common side effect of LASIK are visual disturbances. These include halo, glare, and starbursts and can lead to decreased patient satisfaction.17 In our study, we observed that mean satisfaction, double image, halo, glare, and starburst scores on the PROWL-SS questionnaire were improved 3 months postoperatively compared to preoperatively, though the differences for double image were not significant. This indicated higher satisfaction and lower frequency, less bothersome, or less impact from visual disturbances 3 months post-LASIK compared to preoperative. Rush et al18 performed Phorcides Planned Contoura topography-guided LASIK and reported similar results to ours using a modified PROWL questionnaire. The authors observed significant improvements 26 weeks after LASIK for patient-reported halo, glare, and starbursts. Ma and Mache19 performed wavefront-guided LASIK and also reported similar results to our study, using the PROWL questionnaire up to 12 months postoperatively. In contrast, Moin et al20 reported that patient symptoms of glare on the Quality of Vision questionnaire were increased 3 months after Phorcides Planned Contoura topography-guided LASIK compared to preoperatively, while symptoms of halos, rings, and starburst remained constant. Differences in our study may be explained by differences in patient populations.
The 3-month postoperative monocular visual acuities were excellent with 81% and 31% of eyes having UDVA 20/16 or better and 20/12.5 or better, respectively. This result at 20/16 or better is higher than reported for the FDA clinical trial of topography-guided LASIK (69%),9 however it is similar at 20/12.5 or better (32%). Other studies have reported UDVA ranges of (57% to 91%) for 20/16 or better and (51%) for 20/12.5 or better with topography-guided LASIK.10,20–22 The results of our study and others suggest excellent visual acuities following topography-guided LASIK.
The primary limitation of this study is the 3-month follow-up period. This is relatively short compared to the 12-month follow-up in the FDA clinical trial of Contoura,9 however, this time frame is typical for topography-guided LASIK studies. Nonetheless, we are unable to draw any long-term conclusions for patient-reported symptoms of dry eye, satisfaction, and frequency, bothersomeness, and impact on vision of visual disturbances. In addition, the results of this study are from a single surgeon, which may not be applicable to all surgeons. The lack of comparison to other LASIK platforms is another limitation. Finally, we acknowledge that including contact lens wearers in the study may be a confounding factor, as it is difficult to discern if the questionnaire results are due to the LASIK procedure or the cessation of contact lens wear. However, the inclusion of contact lens wearers better represents what clinicians will experience in the real world.
In conclusion, the results of this study suggest improved patient reported satisfaction, reduced dry eye symptoms, and overall decrease in visual disturbances at 3 months following Phorcides planned Contoura LASIK.
Acknowledgment
Melissa Wright from Mann Eye Institute and Laser Centers assisted with data collection and data checking. This paper will be presented at the 2025 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference paper.
Funding
This study was supported with an investigator-initiated study grant (76882857) from Alcon Vision, LLC, Fort Worth, TX, USA.
Disclosure
Dr Paul Mann is a consultant for Alcon. The authors report no other conflicts of interest for this work.
References
1. Toda I. Dry eye after LASIK. Invest Ophthalmol Vis Sci. 2018;59:DES109–DES115. doi:10.1167/iovs.17-23538
2. De Paiva CS, Chen Z, Koch DD, et al. The incidence and risk factors for developing dry eye after myopic LASIK. Am J Ophthalmol. 2006;141:438–445. doi:10.1016/j.ajo.2005.10.006
3. Shoja MR, Besharati MR. Dry eye after LASIK for myopia: incidence and risk factors. Eur J Ophthalmol. 2007;17:1–6. doi:10.1177/112067210701700101
4. Hirabayashi MT, Barnett BP. Solving STODS—surgical temporary ocular discomfort syndrome. Diagnostics. 2023;13.
5. Shtein RM. Post-LASIK dry eye. Expert Rev Ophthalmol. 2011;6:575–582. doi:10.1586/eop.11.56
6. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118:615–621. doi:10.1001/archopht.118.5.615
7. Eydelman M, Hilmantel G, Tarver ME, et al. Symptoms and satisfaction of patients in the patient-reported outcomes with laser in situ keratomileusis (PROWL) studies. JAMA Ophthalmol. 2017;135:13–22. doi:10.1001/jamaophthalmol.2016.4587
8. Hays RD, Tarver ME, Spritzer KL, et al. Assessment of the Psychometric Properties of a Questionnaire Assessing Patient-Reported Outcomes With Laser In Situ Keratomileusis (PROWL). JAMA Ophthalmol. 2017;135:3–12. doi:10.1001/jamaophthalmol.2016.4597
9. Stulting RD, Fant BS, Group TCS, et al. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42:11–18. doi:10.1016/j.jcrs.2015.08.016
10. Lobanoff M, Stonecipher K, Tooma T, Wexler S, Potvin R. Clinical outcomes after topography-guided LASIK: comparing results based on a new topography analysis algorithm to those based on the manifest refraction. J Cataract Refract Surg. 2020;46:814–819. doi:10.1097/j.jcrs.0000000000000176
11. Brunson PB, Mann II PM, Mann PM, Potvin R. Clinical outcomes after topography-guided refractive surgery in eyes with myopia and astigmatism – comparing results with new planning software to those obtained using the manifest refraction. Clin Ophthalmol. 2020;14:3975–3982. doi:10.2147/OPTH.S280959
12. Stulting RD, Durrie DS, Potvin RJ, et al. Topography-guided refractive astigmatism outcomes: predictions comparing three different programming methods. Clin Ophthalmol. 2020;14:1091–1100. doi:10.2147/OPTH.S244079
13. Gauvin M, Wallerstein A. mEYEstro software: an automatic tool for standardized refractive surgery outcomes reporting. BMC Ophthalmol. 2023;23:171. doi:10.1186/s12886-023-02904-6
14. Kojima T. Contact lens-associated dry eye disease: recent advances worldwide and in Japan. Invest Ophthalmol Vis Sci. 2018;59:DES102–DES108. doi:10.1167/iovs.17-23685
15. Rush S, Pickett CJ, Rush RB. Patient-reported dry eye outcomes after myopic femtosecond-LASIK: a 6-month prospective analysis. Clin Ophthalmol. 2023;17:2141–2147. doi:10.2147/OPTH.S421369
16. Ma KK, Manche EE. Corneal sensitivity and patient-reported dry eye symptoms in a prospective randomized contralateral-eye trial comparing laser in situ keratomileusis and small incision lenticule extraction. Am J Ophthalmol. 2022;241:248–253. doi:10.1016/j.ajo.2022.05.010
17. Bailey MD, Mitchell GL, Dhaliwal DK, Boxer Wachler BS, Zadnik K. Patient satisfaction and visual symptoms after laser in situ keratomileusis. Ophthalmology. 2003;110:1371–1378. doi:10.1016/S0161-6420(03)00455-X
18. Rush SW, Pickett CJ, Wilson BJ, Rush RB. Topography-guided LASIK: a prospective study evaluating patient-reported outcomes. Clin Ophthalmol. 2023;17:2815–2824. doi:10.2147/OPTH.S429991
19. Ma KK, Manche EE. Patient-reported quality of vision in a prospective randomized contralateral-eye trial comparing LASIK and SMILE. J Cataract Refract Surg. 2022.
20. Moin KA, Manion GN, Pandiri S, Hoopes PC, Moshirfar M. Three-month comprehensive outcomes of topography-guided LASIK versus Keratorefractive Lenticule Extraction (KLEx): a prospective contralateral study. Ophthalmol Ther. 2024;13:2265–2284. doi:10.1007/s40123-024-00987-y
21. Zhang J, Shao J, Cao X, Zhang Y, Zheng L. Fitting-shape-based strategy for topography-guided LASIK: a prospective study. J Refract Surg. 2024;40:e336–e343. doi:10.3928/1081597X-20240415-01
22. Rowen S, Tooma T, Trieu N, Hall B. Retrospective study comparing topography-guided and wavefront-optimized lasik procedures in a single center. Clin Ophthalmol. 2024;18:1615–1622. doi:10.2147/OPTH.S455262
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Topography-Guided LASIK: A Prospective Study Evaluating Patient-Reported Outcomes
Rush SW, Pickett CJ, Wilson BJ, Rush RB
Clinical Ophthalmology 2023, 17:2815-2824
Published Date: 25 September 2023