Back to Journals » Patient Preference and Adherence » Volume 16
Patient-Reported Quality of Life Before and After Total Knee Arthroplasty: A Multicenter Observational Study
Authors Chang J, Fu M, Cao P, Ding C, Wang D ![]()
Received 19 January 2022
Accepted for publication 14 March 2022
Published 22 March 2022 Volume 2022:16 Pages 737—748
DOI https://doi.org/10.2147/PPA.S357632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Jinghui Chang,1,* Manru Fu,1,2,* Peihua Cao,3 Changhai Ding,3,4,* Dong Wang1,*
1School of Health Management, Southern Medical University, Guangzhou, 510515, People’s Republic of China; 2The Third Affiliated Hospital, Southern Medical University, Guangzhou, 510282, People’s Republic of China; 3Clinical Research Center, Zhujiang Hospital, Southern Medical University, Guangzhou, 510282, People’s Republic of China; 4Menzies Institute for Medical Research, University of Tasmania, Hobart, Tasmania, Australia
*These authors contributed equally to this work
Correspondence: Dong Wang, School of Health Management, Southern Medical University of China, Guangzhou, 510515, People’s Republic of China, Tel +86 18620089545, Email [email protected]
Purpose: To compare patients’ self-reported health-related quality of life (HRQoL) before and after total knee arthroplasty (TKA) and determine factors contributing to any heterogeneity in HRQoL.
Patients and Methods: This prospective multicenter observational study included 404 patients with knee osteoarthritis who underwent TKA between April 1, 2019 and December 30, 2019 and whose HRQoL was assessed preoperatively and 7 days and 1, 3, and 6 months postoperatively. Sociodemographic characteristics were assessed using a General Information Questionnaire, disability using the Knee Injury and Osteoarthritis Outcome Score (KOOS-PS), resting pain using the visual analogue scale (Pain-VAS), and HRQoL using the European Quality of Life Five Dimension Five Level (EQ-5D-5L) scale. The growth mixture model was used to identify group heterogeneity in the developmental trajectories of KOOS-PS, Pain-VAS, and EQ5D5L. Logistic regression was used to explore the factors influencing the developmental trajectories of factors affecting the developmental trajectory of HRQoL.
Results: The mean EQ-5D-5L score improved from 0.69 preoperatively to 0.90 at 6 months postoperatively. Longitudinal heterogeneity in HRQoL was observed in patients during recovery: 1) patients with a small and slow improvement in HRQoL and 2) patients who showed marked and rapid improvement in HRQoL. The main characteristics of the latter group were decreasing VAS pain scores, a monthly family income > 2000 CNY (100 CNY equals approximately 14.9 USD), exercising for < 30 min daily, and better knee function at baseline. Baseline knee function and change in knee function were significantly associated with the percentage change in HRQoL.
Conclusion: HRQoL improved considerably after TKA. However, there was heterogeneity in the changes in HRQoL depending on patients’ socioeconomic status, exercise, and baseline knee function. Dynamic tracking of the HRQoL of TKA patients and timely provision of rehabilitation guidance will promote continuous improvement of the HRQoL of TKA patients.
Keywords: knee osteoarthritis, knee replacement, knee function
Introduction
Osteoarthritis is a common chronic musculoskeletal disease that affects nearly 400 million people worldwide and imposes a heavy socioeconomic burden on individuals and health care systems in many countries.1–3 Knee osteoarthritis (KOA) is present in 86.8% of osteoarthritis cases and is the main cause of knee pain.2,4 It is characterized by the destruction of the articular cartilage of the knee and osteophyte formation. Patients with KOA often have reduced self-care ability and even disability due to joint pain, stiffness, and limited activity, which have an increasingly severe impact on their quality of life and leads to a wide range of social problems over time.3
The prevalence of KOA in the Chinese population over the age of 40 years is reported to be 17.0%, affecting 12.3% of men and 22.2% of women, and both these figures are higher than the world average values.5 Furthermore, the proportion of younger patients with KOA is increasing, and it is projected that the proportion of the population over the age of 45 years with a diagnosis of KOA will increase from 13.8% to 15.7% by 2032.6,7 This degenerative disease adversely affects the health-related quality of life (HRQoL) of middle-aged and older patients and represents a substantial burden of disease in China.
Total knee arthroplasty (TKA) is the most effective treatment for end-stage KOA8–11 and has been performed for over 40 years.12,13 Previous studies have shown that 80–85% of patients with KOA have good outcomes after TKA.14–16 However, several studies have reported that not all patients are satisfied with the outcome after surgery, with 15–20% of patients reporting persistent pain, poor joint function, and postoperative infection, among other complications, warranting a need for revision surgery.17
Previous studies of TKA have focused primarily on the clinical effectiveness of the surgery and its risk factors,18,19 costs versus benefits of surgery,20 or the safety and efficacy of postoperative rehabilitation.21 Although some studies have investigated HRQoL of patients after TKA,22,23 the factors affecting changes in HRQoL are not clear. The Growth Mixture Model (GMM) has the advantage of being able to identify different growth trajectories of unobservable subgroups in longitudinal data analysis (eg, Figures S1 and S2) and thus provides insights into the development of individuals using longitudinal data; this makes this model very suitable for the analysis of the follow-up evaluation of the HRQoL of patients with KOA. The specific process for fitting GMM is described in the Trajectory Analysis section of the Supplementary Materials.
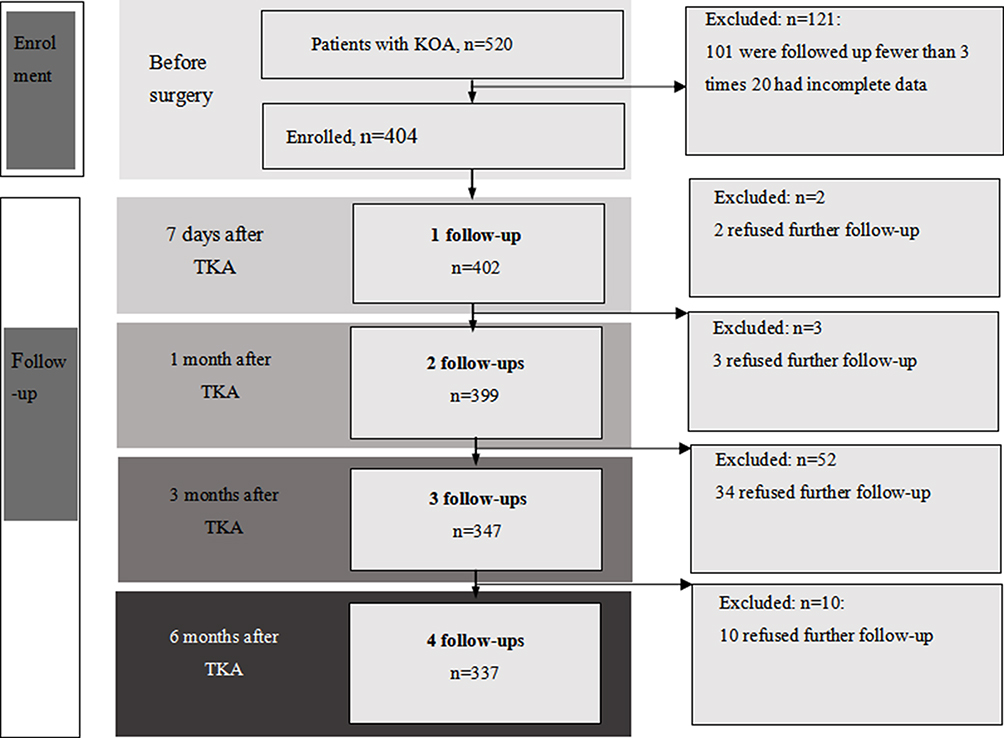 |
Figure 1 Flow chart showing the study screening and enrolment process. Abbreviations: KOA, knee osteoarthritis; TKA, total knee arthroplasty. |
Therefore, we conducted this multicenter observational study in Guangzhou, the largest city in Southern China, to assess the self-reported HRQoL trajectories of patients with KOA before and after TKA and to identify the factors contributing to any differences observed in these trajectories.
Materials and Methods
Study Design and Participants
This prospective observational study enrolled patients who underwent TKA at one of four tertiary hospitals in four districts in Guangzhou, China, between April 1, 2019 and December 30, 2019. The following inclusion criteria were used: 1) diagnosis of KOA based on the 2018 clinical guidelines for the diagnosis of osteoarthritis in China,24 2) first TKA procedure, 3) willingness and ability to complete questionnaires, and 4) completion of at least three of five follow-up questionnaires. Patients with a psychiatric disorder, those with serious comorbidities (eg malignant tumors, post-stroke state, end-stage renal disease, severe Parkinson’s disease), and those who were not independently self-caring were excluded. Questionnaires were distributed to patients by the investigators and medical students at the five assessment points. In total, 404 of 520 patients with KOA screened at baseline met the study inclusion criteria and attended at least three follow-up visits. The screening process and follow-up of patients throughout the study are shown in Figure 1. This study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement for the reporting of observational studies.
Ethics
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Southern Medical University (approval number 2018-IORG-10-1) and performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all study participants.
General Information Questionnaire
Sociodemographic characteristics were obtained from a questionnaire adapted from the General Information Questionnaire developed by the International Consortium for Health Outcomes Measurement for KOA. Information collected included that on sex, age, marital status, education level, weight, height, monthly family income, basic health insurance, smoking status, alcohol consumption, frequency of physical activity, history of KOA, and history of knee surgery. Body mass index (BMI, in kg/m2) was calculated for each patient. Using the BMI cut-off values reported for the Chinese population, patients were classified as follows: underweight (<18.5), normal weight (18.5–23.9), overweight (24.0–27.9), and obese (≥28).25
Knee Injury and Osteoarthritis Outcome Score
The Knee Injury and Osteoarthritis Outcome Score (KOOS-PS) is a short version of the original KOOS. It is a self-administered instrument that measures the outcomes of impairment, disability, and handicap after knee injury and comprises seven dimensions, each of which is scored from 0 to 4 for the degree of difficulty (0, none; 1, slight; 2, moderate; 3, very; and 4, extreme). The original total score ranges from 0 to 28, with a higher score indicating better joint function.26 The KOOS-PS standard score is obtained by converting the score formula specified by the scale and ranges from 0 to 100.13
Visual Analogue Pain Scale
Patients’ subjective perception of resting pain was estimated using the visual analogue scale (VAS) score, which is widely used and determined by measuring the distance on a 10-cm line between the “no pain” anchor and mark made by the patient. Patients use a vertical line to mark their current level of knee pain. Scores range from 0 to 10, and a higher score indicates greater pain intensity.
European Quality of Life Five Dimension Five Level Scale
The European Quality of Life Five Dimension Five Level (EQ-5D-5L) scale is a standardized instrument developed by the EuroQol group to measure health status and is widely used internationally.27 It comprises five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which is rated on a 5-point scale (none, not difficult; slight, a little difficult; moderate, some difficulty; severe, very difficult; or extreme, impossible). The scores obtained were converted into a total score using the Chinese scoring system and ranged from −0.391 to 1.000, with higher scores representing a better health status.28
Reliability
Internal consistency was measured using the Cronbach’s alpha coefficient. An alpha value between 0.70 and 0.95 was considered to indicate acceptable reliability. Cronbach’s coefficients for the five measurements of the KOOS-PS scale and five measurements of the EQ-5D-5L scale are listed in Table 1.
 |
Table 1 Reliability of KOOS-PS and EQ-5D-5L Scores at Five Time Points from Before Surgery to 6 Months After Surgery |
Statistical Analysis
Continuous variables are summarized as mean and standard deviation, and categorical variables are shown as frequency (percentage). Categorical variables were compared using Pearson’s test, and continuous variables were compared using Student’s t-test or the Wilcoxon test. Statistical significance was set at a p-value < 0.05. Spearman correlation coefficient was used to describe the correlation between the KOOS-PS and EQ-5D-5L scores at each time point. The GMMs were fitted in a two-step approach to identify potential heterogeneity of KOOS-PS, VAS, and EQ-5D-5L, where factor loadings of the slope terms as well as variances and covariances of continuous latent variables were free estimates across groups. First, two unconditional GMMs were fitted to KOOS-PS and VAS, respectively. Next, a conditional GMM was fitted to the EQ-5D-5L score, where KOOS-PS_I (the intercept term of KOOS-PS), KOOS-PS_S (the slope term of KOOS-PS), and VAS_C (the categorical latent variable of VAS) from the first step were entered as covariables. The categorical latent variables of the EQ-5D-5L were used as the grouping variables. Univariable and multivariable logistic regression models were used to explore the factors associated with the EQ-5D-5L score. The multivariable logistic regression model was established by including variables with a p-value < 0.1. Monthly family income, exercise, KOOS-PS_I, KOOS-PS_S, and VAS_C were independent variables, and EQ-5D-5L_C was the dependent variable. VAS_C and EQ-5D-5L_C represented categorical latent variables. R 3.6.2 was used for data cleaning, statistical description, and regression analysis, and Mplus 8.3 software was used for the GMM analysis.
Results
Patient Characteristics
The patient characteristics are presented in Table 2. Of the 404 study participants, 313 (77.48%) were women, 395 (97.77%) were over the age of 40 years, 396 (98.2%) were married, and 221 (55.22%) had not been educated beyond the elementary School level. Monthly family income was < 2000 CNY for 198 (49.75%), 2000–4000 CNY for 106 (26.63%), and > 4000 CNY for 94 (23.62%) patients. A total of 141 patients (34.90%) did not exercise daily, 106 (26.24%) exercised for < 30 min daily, and 157 (38.86%) exercised for > 30 min daily. A total of 289 (71.53%) patients were overweight or obese.
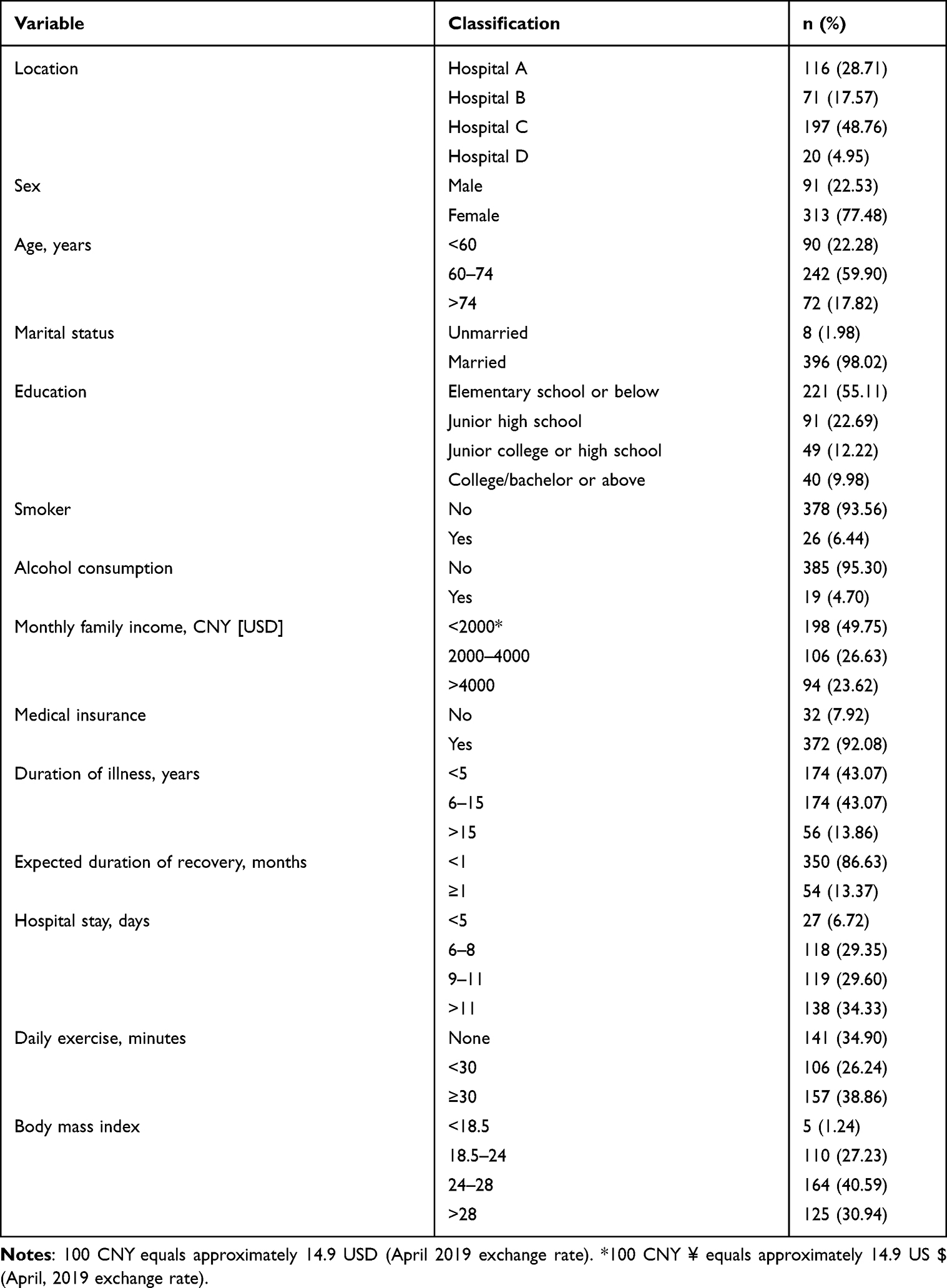 |
Table 2 Patients’ Demographic and Clinical Characteristics (n=404) |
Changes in EQ-5D-5L and KOOS-PS Across Five Time Periods
Table 3 shows the changes in HRQoL and knee function over time, as assessed using the EQ-5D-5L and KOOS-PS scores. In comparison with preoperative values, HRQoL and knee function scores were lower on postoperative day 7 but improved significantly by 6 months after surgery. There was a significant correlation between the KOOS-PS score and the EQ-5D-5L score before surgery; at 7 days; and at 1, 3, and 6 months after surgery, with Spearman correlation coefficients of 0.568, 0.654, 0.579, 0.525, and 0.538 (p<0.001), respectively.
 |
Table 3 EQ-5D-5L and KOOS-PS Mean Scores at Five Time Points from Before Surgery to 6 Months After Surgery |
Selection of the Best GMM
KOOS-PS, VAS, and EQ-5D-5L scores did not show linear or quadratic growth trajectories over time (Figures S3–S5); therefore, GMMs were fitted in a two-step approach to identify potential heterogeneity of KOOS-PS, VAS, and EQ-5D-5L, where factor loadings of the slope terms as well as variances and covariances of continuous latent variables were free estimates across groups. First, two unconditional GMMs were fitted to KOOS-PS and VAS, respectively. The model fitting results (Tables S1 and S2) showed that the best classifications for KOOS-PS and VAS pain scores were 1 class (latent growth curve modeling) and 2 class, respectively. Next, a conditional GMM was fitted to the EQ-5D-5L score, where KOOS-PS_I (the intercept term of KOOS-PS), KOOS-PS_S (the slope term of KOOS-PS), and VAS_C (the categorical latent variable of VAS) from the first step were entered as covariables.29–31 According to Table S3, the 2-class GMM was deemed to be the best fitting model for representing the HRQoL trajectories over five time periods. The individual growth trajectories of these two classes are shown in Figures S6 and S7. The average trajectory of the 2-class GMM-C is shown in Figure 2. Patients in whom the average HRQoL trajectory (EQ-5D-5L) improved markedly and rapidly after TKA were classified as the “rising” group, and those in whom the increase in the HRQoL trajectory was slower and less marked were classified as the “stable” group.
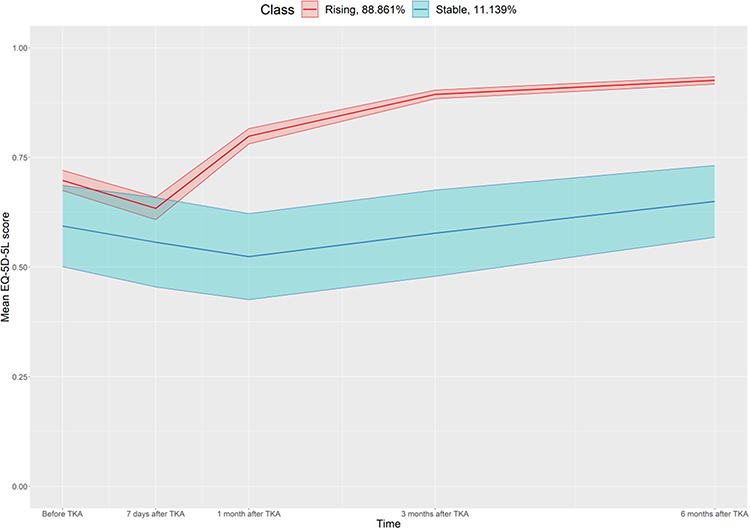 |
Figure 2 Average health-related quality of life trajectory based on the EQ-5D-5L score in a 2-class growth mixture model. Abbreviations: EQ-5D-5L, European Quality of Life Five Dimension Five Level; TKA, total knee arthroplasty. |
Parameter Estimates of HRQoL in the 2-Class GMM
Table S4 presents the parameter estimates for the selected 2-class GMM of the EQ-5D-5L scores. In the stable group (n = 45), the baseline EQ-5D-5L scores (EQ-5D-5L_I) were positively associated with the baseline KOOS-PS scores (KOOS-PS_I) (β = 0.021, p < 0.001). The results of the heterogeneity analysis in the stable group also showed that there were differences in the baseline HRQoL scores among individuals (residual mean-0.446, p = 0.044 and residual variance, −0.023, p = 0.014), although there were no significant differences in the change in HRQoL among individuals (p = 0.569 and p = 0.742). The intercept was not correlated with the slope (p = 0.972). In the rising group (n = 359), the baseline EQ-5D-5L (EQ-5D-5L_I) score (β= 0.030, p < 0.001) was positively associated with the baseline KOOS-PS score (KOOS-PS_I). However, KOOS-PS_I was negatively associated with the rate of change in EQ-5D-5L (EQ-5D-5L_S; β=−0.015, p < 0.0001). The residual differences in the initial HRQoL scores among individuals were significant (p < 0.001), as was the rate of change (p < 0.001).
Latent HRQoL Variables as Risk Factors
In univariable analysis, the KOOS-PS knee function score, monthly family income, amount of daily exercise, and VAS_C were associated with being in the rising EQ-5D-5L group (p<0.1) (Table 4). In the multivariable logistic regression model (Table 5), compared with that of patients with a monthly family income < 2000 CNY, the odds of being in the rising group was higher for patients with a monthly family income of 2000–4000 CNY (odds ratio [OR] 6.19, 95% confidence interval [CI] 2.16–21.57) and > 4000 CNY (OR 19.73, 95% CI 3.77–366.69). The odds of being in the rising group were higher for patients who exercised for < 30 min daily than for those who did not (OR 2.95, 95% CI 1.06–9.02). However, when daily exercise was performed for > 30 min, the odds were not significant (OR 1.62, 95% CI 0.66–4.02), considering patients who did not exercise as reference. For patients with a decreasing VAS pain score, the odds of being in the rising group were higher than for those with a stable VAS pain score (OR 6.09, 95% CI 2.72–14.07). Compared with that with the preoperative KOOS-PS score, we also found that the odds of being in the rising group increased with higher KOOS-PS scores (Table 5).
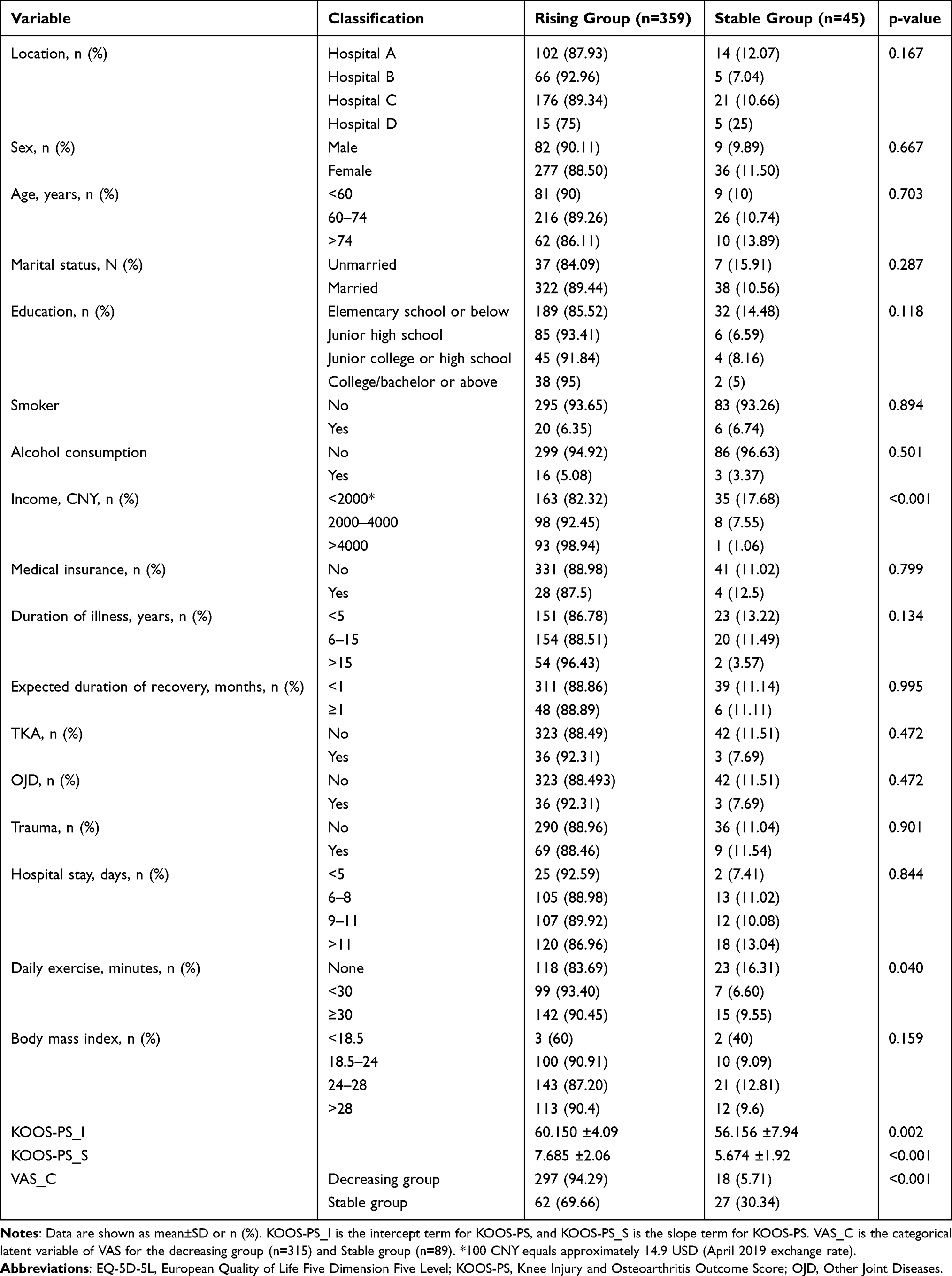 |
Table 4 Comparison of Sociodemographic Characteristics Between the Stable and Rising Groups |
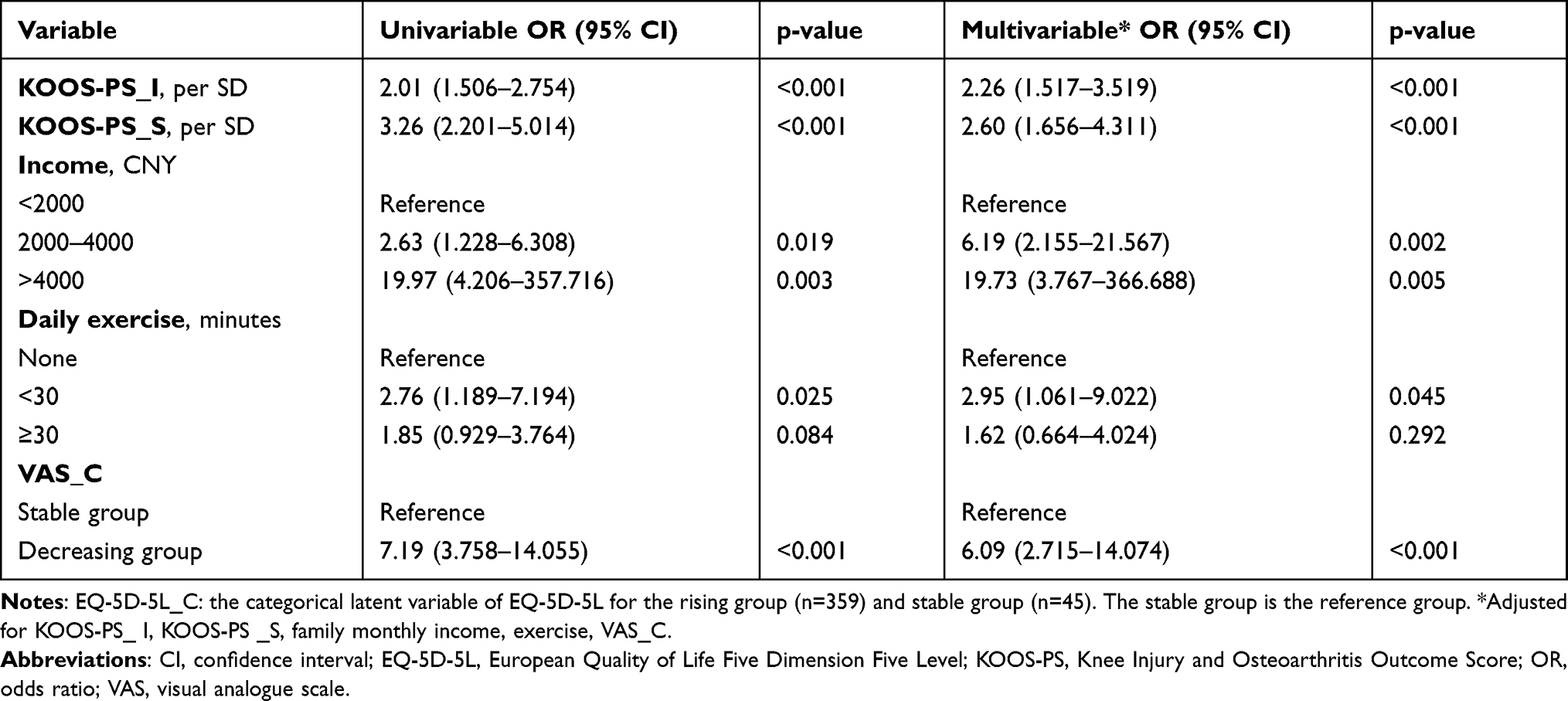 |
Table 5 Logistic Regression with EQ-5D-5L_C as the Dependent Variable |
Discussion
This study aimed to identify any population heterogeneity in factors influencing changes in the HRQoL of patients with KOA that can be used to develop individualized treatment strategies.
We found that patients showed improvement in knee function and HRQoL after TKA, which is consistent with the findings of Zhang et al 32 and Neuprez et al.33 The trajectory for EQ-5D-5L indicated that patients experienced a cycle of change in knee function and HRQoL after TKA. HRQoL would be expected to deteriorate for a short period immediately after TKA owing to postoperative bed rest, limited knee function, and wound pain. Osteotomy, unicompartmental knee arthroplasty, TKA, and arthroscopic surgery can all improve functional scores of patients with KOA; however, follow-up studies indicate that TKA is better than other interventions in terms of relieving knee pain and improving knee function in the long term.34 HRQoL is not only an indicator of physical fitness but also a reflection of the psychological and socioeconomic status. Therefore, mental well-being may be almost as important as physical discomfort and activity restriction in determining self-reported outcomes and HRQoL after TKA.35,36 High preoperative expectations are associated with clinical improvement, including pain reduction.37 Maintaining a stable emotional state and a positive attitude toward short-term discomfort are important for patients undergoing TKA. Additionally, patients should follow medical advice strictly and adhere to examinations, treatment, and rehabilitation exercises. Doctors and rehabilitation therapists should strengthen preoperative communication and psychological counseling for these patients. Appropriate guidance and care are essential to gain the full trust of patients with KOA and to boost their confidence, which is essential for the success of the treatment.38
In this study, the results of 2-class GMM indicate that higher the baseline knee function score, the more rapid the improvement in knee function and HRQoL after surgery. This finding suggests that patients with better knee function at baseline would derive maximum benefit from surgery, which is consistent with the findings of Fortin et al.39 Age-related neuromotor changes lead to skeletal muscle weakness and reduced power. Muscle strength and power have been reported to decrease by at least 24% in TKA recipients compared with controls.40 However, more demanding rehabilitation protocols may help overcome these deficits. Postoperative rehabilitation following TKA would make a substantial contribution to patient outcomes, including a shorter hospital stay and fewer complications. Early rehabilitation, telerehabilitation, outpatient therapy, and high intensity and high velocity exercise may be beneficial to reduce pain intensity and joint stiffness.39 Therefore, joint rehabilitation training and functional exercises should be initiated under medical supervision as soon as possible for these patients. An improved focus on patient rehabilitation after discharge, including home-based exercise and dietary guidance, may also be needed to maximize the benefits of surgery.41
In this study, patients with a monthly family income < 2000 CNY had less improvement in postoperative knee function and HRQoL than their more affluent counterparts, and this difference was observed over a long period of time. Most patients were over the age of 50 years, and those with a monthly family income < 2000 CNY were mostly agricultural or migrant workers. These individuals generally have less health knowledge, a lower socioeconomic status, and relatively poor self-Management skills.42 For financial reasons, they are less likely to protect their knees when performing daily activities and are more likely to opt for less expensive drugs, medical consumables, and therapies. Furthermore, they often return to work prematurely without adequate rest and rehabilitation after surgery.
Patients in this study who exercised for < 30 min daily had better outcomes than those who did not exercise. An appropriate amount of regular exercise both protects and improves knee function in patients with KOA and accelerates postoperative recovery. Pain was also identified to affect the outcome of TKA, which is consistent with previous reports.43,44 Pain severely affects both mobility and mental well-being of patients with KOA. Therefore, adequate perioperative pain management is important for these patients. A study found that some patients with KOA and mild pain did not ask for pain relief soon enough and missed the opportunity for intervention in the early stage of inflammation,42 which led to worsening of the disease. Pain should be controlled effectively in the early stages of KOA, with consideration of interventions such as physical therapy to avoid progression of acute pain to uncontrollable chronic pain. As soon as KOA is diagnosed, doctors and patients’ families should make decisions together and cooperate to standardize pain management45 and encourage patients to exercise as appropriate to help preserve their joint function.
This study had some potential limitations. First, data for 67 patients could not be collected at all five time points; these missing results may have resulted in a reporting bias. Longer term (1–2 years) follow-up should be performed in the future. Second, the size of the stable group in the 2-class GMM was small, meaning that the effects of certain patient factors, such as age, sex, and BMI, might not be well reflected. Future analysis should consider the impact of patient expectation and satisfaction subscores on HRQoL.46 Third, the effects of TKA were not analyzed according to the implantation method used. Therefore, future studies should investigate the impact of the implantation method and rehabilitation protocol used on postoperative HRQoL in patients who undergo TKA.
Conclusion
Our results demonstrated that TKA can significantly improve HRQoL and knee function in patients with KOA. TKA should be recommended for patients with end-stage KOA and for those who do not respond to pharmacological therapy. For orthopedic clinicians, patients with poor preoperative joint functional status and who do not perform any exercise are a key concern. Doctors should encourage them to undergo joint rehabilitation training as early as possible, pay attention to joint function exercises, and communicate with doctors about the status of joint function rehabilitation in a timely manner. Health care professionals should also pay more attention to patients’ out-of-hospital rehabilitation status and strengthen their health guidance after discharge, including joint function rehabilitation guidance and dietary guidance, so that patients can maximize their HRQoL.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request and are strictly for research purposes.
Ethics Approval
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Southern Medical University (approval number 2018-IORG-10-1) and performed in accordance with the Declaration of Helsinki.
Consent
Written informed consent was obtained from all study participants.
Acknowledgments
We would like to thank our study participants for taking the time and effort to participate in this research.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. DW and CD contributed equally to this work and should be considered co-corresponding authors.
Funding
This study was funded by a Grant from the MOE (Ministry of Education in China) Project of Humanities and Social Science (18YJAZH086), a Grant from Philosophy and Social Sciences of Guangdong College for the project “Public Health Policy Research and Evaluation” Key Laboratory (2015WSYS0010), a Grant from the Public Health Service System Construction Research Foundation of Guangzhou (2021–2023), and a Grant from the National Subject Incubation Program Projects of the School of Health Management, Southern Medical University (2019RFT002). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–1749. doi:10.1016/S0140-6736(19)30417-9
2. Prieto-Alhambra D, Judge A, Javaid MK, Cooper C, Diez-Perez A, Arden NK. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis. 2014;73(9):1659–1664. doi:10.1136/annrheumdis-2013-203355
3. Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol. 2014;10(7):437–441. doi:10.1038/nrrheum.2014.44
4. Roberts NL, Mountjoy-Venning WC, Anjomshoa M, Banoub JA, Yasin YJ. GBD 2017 disease and injury incidence and prevalence collaborators. global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi:10.1016/S0140-6736(18)32279-7
5. Xiao-jia T, Ru-geng Z, Meng Z, et al. [Prevalence of knee osteoarthritis in the middle-aged and elderly in China: a meta-analysis]. Zhongguo Zuzhi Gongcheng Yanjiu. 2018;22:650. Chinese.
6. Cross M, Smith E, Hoy D, et al. The global burden of hip and knee osteoarthritis: estimates from the Global Burden Of Disease 2010 Study. Ann Rheum Dis. 2014;73:1323–1330. doi:10.1136/annrheumdis-2013-2047636
7. Turkiewicz A, Petersson IF, Björk J, et al. Current and future impact of osteoarthritis on health care: a population-based study with projections to year 2032. Osteoarthritis Cartilage. 2014;22:1826–1832. doi:10.1016/j.joca.2014.07.015
8. Price AJ, Alvand A, Troelsen A, et al. Knee replacement. Lancet. 2018;392:1672–1682. doi:10.1016/S0140-6736(18)32344-4
9. National Joint Registry. 14th annual report 2017. national joint registry for England, Wales, Northern Ireland and the Isle of Man: surgical data to 31 december; 2016. Available from: https://www.hqip.org.uk/resource/national-joint-registry-14th-annual-report-2017/#.YIX7BOgzbIU.
10. Culliford D, Maskell J, Judge A, Cooper C, Prieto-Alhambra D, Arden NK. COASt Study Group. Future projections of total hip and knee arthroplasty in the UK: results from the UK Clinical Practice Research Datalink. Osteoarthritis Cartilage. 2015;23:594–600. doi:10.1016/j.joca.2014.12.022
11. Inacio M, Paxton EW, Graves SE, Namba RS, Nemes S. Projected increase in total knee arthroplasty in the United States An alternative projection model. Osteoarthritis Cartilage. 2017;25:1797–1803. doi:10.1016/j.joca.2017.07.022
12. Murray DW, MacLennan GS, Breeman S, et al. A randomised controlled trial of the clinical effectiveness and cost-effectiveness of different knee prostheses: the Knee Arthroplasty Trial (KAT). Health Technol Assess. 2014;18:1–235. doi:10.3310/hta18190
13. Pabinger C, Lothaller H, Geissler A. Utilization rates of knee-arthroplasty in OECD countries. Osteoarthritis Cartilage. 2015;23:1664–1673. doi:10.1016/j.joca.2015.05.008
14. MacLean C. Value-based purchasing for osteoarthritis and total knee arthroplasty: what role for patient-reported outcomes? J Am Acad Orthop Surg. 2017;25(Suppl 1):S55–S59. doi:10.5435/JAAOS-D-16-00638
15. Dakin H, Gray A, Fitzpatrick R, MacLennan G, Murray D. KAT Trial Group. Rationing of total knee replacement: a cost-effectiveness analysis on a large trial data set. BMJ Open. 2012;2:e000332. doi:10.1136/bmjopen-2011-000332
16. Williams DP, Blakey CM, Hadfield SG, Murray DW, Price AJ, Field RE. Long-term trends in the Oxford knee score following total knee replacement. Bone Joint J. 2013;95:45–51. doi:10.1302/0301-620X.95B1.28573
17. Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open. 2012;2:e000435. doi:10.1136/bmjopen-2011-000435
18. Thambiah MD, Nathan S, Seow BZ, Liang S, Lingaraj K. Patient satisfaction after total knee arthroplasty: an Asian perspective. Singapore Med J. 2015;56:259–263. doi:10.11622/smedj.2015074
19. Kayani B, Konan S, Tahmassebi J, Oussedik S, Moriarty PD, Haddad FS. A prospective double-blinded randomised control trial comparing robotic arm-assisted functionally aligned total knee arthroplasty versus robotic arm-assisted mechanically aligned total knee arthroplasty. Trials. 2020;21:194. doi:10.1186/s13063-020-4123-8
20. Vestergaard V, Becic PA, Borbjerg HK, Morville SH, Troelsen A. Knee fracture increases TKA risk after initial fracture treatment and throughout life. Clin Orthop Relat Res. 2020;478(9):2036–2044. doi:10.1097/CORR.0000000000001099
21. Liptak MG, Theodoulou A, Kaambwa B, et al. The safety, efficacy and cost-effectiveness of the Maxm Skate, a lower limb rehabilitation device for use following total knee arthroplasty: study protocol for a randomised controlled trial. Trials. 2019;20(1):36. doi:10.1186/s13063-018-3102-9
22. Bade MJ, Struessel T, Dayton M, et al. Early high-intensity versus low-intensity rehabilitation after total knee arthroplasty: a randomized controlled trial. Arthritis Care Res. 2017;69(9):1360–1368. doi:10.1002/acr.23139
23. Shah A, Afzal F, Ans M, et al. Quality of life before and after total knee arthroplasty in clinical settings across Lahore, Pakistan. Pak J Pharm Sci. 2019;32(2 Suppl):769–772.
24. Chinese Orthopaedic Association. [Clinical guidelines for osteoarthritis 2018 edition]. China J Ortho. 2018;38. 705–715. Chinese. doi:10.3760/cma.j.issn.0253-2352.2018.12.001
25. National Health and Family Planning Commission of the People’s Republic of China. WS/T428-2013 health industry standard of the People’s Republic of China-Adult weight determination. Beijing: China Standard Press; 2013.
26. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee injury and Osteoarthritis Outcome Score (KOOS)–development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28:88–96. doi:10.2519/jospt.1998.28.2.88
27. Xing YB, Ma AX. [Study on reliability and validity of Chinese version of EQ-5D-5L]. Shanghai Med Pharmaceut J. 2013;34:40–43. Chinese.
28. Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K. Estimating an EQ-5D-5L value set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
29. Muthén BO. Latent variable analysis: growth mixture modeling and related techniques for longitudinal data. In: Handbook of Quantitative Methodology for the Social Sciences. SAGE Publications Inc; 2004: 345–368.
30. Li L, Hser YI. On inclusion of covariates for class enumeration of growth mixture models. Multivariate Behav Res. 2011;46:266–302. doi:10.1080/00273171.2011.556549
31. Stegmann G, Grimm KJ. A new perspective on the effects of covariates in mixture models. Struct Equ Model. 2018;25:167–178. doi:10.1080/10705511.2017.1318070
32. Zhang GD. Clinical effect of joint replacement in elderly patients with knee degenerative osteoarthritis. Chin Pharm J Eco. 2015;10:102–103.
33. Neuprez A, Neuprez AH, Kaux JF, et al. Total joint replacement improves pain, functional quality of life, and health utilities in patients with late-stage knee and hip osteoarthritis for up to 5 years. Clin Rheumatol. 2020;39:861–871. doi:10.1007/s10067-019-04811-y
34. Shan L, Shan B, Suzuki A, Nouh F, Saxena A. Intermediate and long-term quality of life after total knee replacement: a systematic review and meta-analysis. J Bone Joint Surg Am. 2015;97(2):156–168. doi:10.2106/JBJS.M.00372
35. Canovas F, Dagneaux L. Quality of life after total knee arthroplasty. Orthop Traumatol Surg Res. 2018;104(1 Suppl):S41–S46. doi:10.1016/j.otsr.2017.04.017
36. Hossain FS, Konan S, Patel S, Rodriguez-Merchan EC, Haddad FS. The assessment of outcome after total knee arthroplasty: are we there yet? Bone Joint J. 2015;97(1):3–9. doi:10.1302/0301-620X.97B1.34434
37. Hafkamp FJ, de Vries J, Gosens T, den Oudsten BL. High pre-operative expectations precede both unfulfilled expectations and clinical improvement after total hip and total knee replacement. J Arthroplasty. 2020;35(7):1806–1812. doi:10.1016/j.arth.2020.02.061
38. Casazza GA, Lum ZC, Giordani M, Meehan JP. Total knee arthroplasty: fitness, heart disease risk, and quality of life. J Knee Surg. 2020;33:884–891. doi:10.1055/s-0039-1688768
39. Fortin PR, Penrod JR, Clarke AE, et al. Timing of total joint replacement affects clinical outcomes among patients with osteoarthritis of the hip or knee. Arthritis Rheum. 2002;46(12):3327–3330. doi:10.1002/art.10631
40. Dávila CIM, Recai TM, Abraham MM, et al. Rehabilitation protocols following total knee arthroplasty: a review of study designs and outcome measures. Ann Translat Med. 2019;7(Suppl 7):S255. doi:10.21037/atm.2019.08.15
41. Zhou L, Xu RH, Xu Y, Chang J, Wang D. Inpatients’ perception of patient-centered care in Guangdong Province, China: a cross-sectional study. J Health Care Organ Prov Financ. 2021;58:1–11. doi:10.1177/00469580211059482
42. Choojaturo S, Sindhu S, Utriyaprasit K, Viwatwongkasem C. Factors associated with access to health services and quality of life in knee osteoarthritis patients: a multilevel cross-sectional study. BMC Health Serv Res. 2019;19(1):688. doi:10.1186/s12913-019-4441-2
43. Zhu CX, Guo YM, Chen W, Ji HM, Li CH. [Related factors about the quality of life in the elderly with knee osteoarthritis]. Chin J Rehabil Theory Pract. 2011;17:1052–1055. Chinese.
44. Ackerman IN, Buchbinder R, Osborne RH. Factors limiting participation in arthritis self-management programmes: an exploration of barriers and patient preferences within a randomized controlled trial. Rheumatology. 2013;52(3):472–479. doi:10.1093/rheumatology/kes295
45. Xu RH, Zhou L, Wong EL, Wang D. The association between patients’ ehealth literacy and satisfaction with shared decision-making and well-being: multicenter cross-sectional study. J Med Internet Res. 2021;23(9):e26721. doi:10.2196/26721
46. Özden F, Tuğay N, Umut Tuğay B, et al. Psychometrical properties of the Turkish translation of the New Knee Society Scoring System Science Direct. Acta Orthopaedica et Traumatologica Turcica. 2019;53(3):184–188. doi:10.1016/j.aott.2019.03.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.