Back to Journals » Nature and Science of Sleep » Volume 18

Patient-Reported Outcomes for LEMborexant Treatment in Chinese Patients with Insomnia (PROEM): A Multicenter, Prospective, Real-World Observational Study
Authors Zheng S, Li X, Jian W ![]() , Tang Y, Lin Y, Jia F, Zhang B
, Tang Y, Lin Y, Jia F, Zhang B ![]()
Received 19 January 2026
Accepted for publication 4 May 2026
Published 27 May 2026 Volume 2026:18 596731
DOI https://doi.org/10.2147/NSS.S596731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Shuqiong Zheng,1– 3,* Xueli Li,4,* Weiying Jian,5 Yamei Tang,6 Yongqiang Lin,7 Fujun Jia,4 Bin Zhang1– 3
1Department of Psychiatry, Sleep Medicine Center, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Institute of Brain Disease, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 3Key Laboratory of Mental Health of the Ministry of Education, Southern Medical University, Guangzhou, People’s Republic of China; 4Guangdong Mental Health Center, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 5Guangzhou United Family Hospital, Guangzhou, People’s Republic of China; 6Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 7Clifford Hospital, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Zhang, Department of Psychiatry, Sleep Medicine Center, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China, Email [email protected] Fujun Jia, Guangdong Mental Health Center, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: Studies of Lemborexant (LEM) treatment for patients with insomnia in China in real-world setting have been limited. This study assessed efficacy and safety of LEM in treating Chinese patients with insomnia.
Patients and Methods: In this 12-week, multicenter, prospective, observational study, 205 adult patients diagnosed with insomnia with an Insomnia Severity Index (ISI) score of ≥ 10 were enrolled and treated with LEM in China. The primary endpoint was remission rate (the proportion of patients with an ISI< 8) after 4 weeks of LEM treatment. Treatment-emergent adverse events (TEAEs) were recorded.
Results: The full analysis set included 200 patients with a mean baseline ISI of 17.44± 4.45. Remission rate and responder (≥ 6-point reduction in ISI) rate after 4 weeks of LEM treatment was 30.5% (61/200) and 55.0% (110/200), respectively. ISI scores decreased significantly from baseline after 1 weeks of treatment and kept decreasing. LEM treatment also improved symptoms of depression and anxiety. Compared with patients with mild insomnia, patients with severe baseline insomnia were less likely to be insomnia remitters and more likely to be LEM responders and to have greater ISI decrease after 4 weeks of treatment. Additionally, patients who switched to LEM from other hypnotics were less likely to be LEM responders than patient receiving initial LEM monotherapy. 21.0% (43/205) of the patients reported at least one mild or moderate TEAE, and none reported serious TEAEs. Ten (4.9%) patients withdrew from the study due to TEAEs. The most common TEAEs were somnolence, dizziness and nightmare.
Conclusion: Lemborexant was effective and safe in treating Chinese adult patients with insomnia.
Clinicaltrials.gov Registration Number: NCT06225947 (Date of registration: January 17, 2024).
Keywords: lemborexant, insomnia, Chinese, the insomnia severity index, the patient health questionnaire-9, the general anxiety disorder-7
Introduction
Chronic insomnia, a common sleep disorder, has a prevalence of 15.0% in China.1–3 Although cognitive behavioral therapy (CBT) is a first-line treatment for insomnia, pharmacotherapy is commonly used in many patients.4 The most commonly prescribed insomnia medications are benzodiazepines (BZDs) and non-BZDs (also called Z drugs).2,4 However, as both BZDs and Z drugs are positive allosteric modulators of gamma-aminobutyric acid type A (GABA-A) subunit alpha 1 receptor, they induce sleep by inhibiting central nervous system (CNS) activity broadly.4 As a result, they could cause side effects such as next-day residual effects, dependence, increased risk of car accidents and/or fall, cognitive impairment and withdrawal symptoms.4 Therefore, BZDs and Z drugs should only be used for short-term (no more than 4 weeks) treatment of insomnia and their long-term use is not recommended.3,5
Lemborexant (LEM) is a dual orexin receptor antagonist (DORA) approved to treat insomnia in the United States, Canada, Australia, Japan and several other countries.2 As a DORA, LEM binds rapidly and reversibly to orexin receptor type 1 (OX1R) and type 2 (OX2R) and targets the orexin signal pathway involved in regulating sleep/wake signals.2,3 Unlike BZDs and Z drugs that broadly inhibit CNS activities and alter sleep stages, LEM reduces wakefulness and facilitates sleep consistent with normal sleep pattern by suppressing orexin mediated wake drive.1–4 Two pivotal Phase III, randomized controlled trials (RCTs) investigated efficacy and safety of LEM in treating adult patients with insomnia and found that both LEM 5mg and 10mg per night (qn) were effective in improving sleep onset and maintenance (including in the second half of the night) and were safe and tolerable.4,6 LEM had little next-day residual effects and little impact on daily functioning such as cognition and driving, and did not lead to rebound insomnia or withdrawal symptoms.3,7
In May 2025, LEM was approved for the treatment of adults with insomnia in China, and Mi et al, in a Phase III RCT, demonstrated that LEM 10mg qn was effective and safe in treating Chinese patients with chronic insomnia8 However, the real-world effectiveness and safety of LEM 5mg and 10mg qn in Chinese patients remain to be fully investigated Real-world patients are more clinically complex, with diverse treatment patterns, compared to the patients in clinical trials Most patients enrolled in clinical trials of LEM treatment were patients with primary insomnia who were generally physically and mentally healthy, as phase III regulatory trials of hypnotics in recent years generally have very strict inclusion / exclusion criteria and only a small percentage of real-world patients were eligible.9 The most common reasons for exclusion from these trials were comorbidities, daytime napping and sleep.9 Both the pivotal SUNRISE 1 and 2 studies excluded patients who had a history of medical or psychiatric condition(s) deemed to be unsuitable for the trials.4,6 In addition, patients who had recently received insomnia treatment in the SUNRISE 1 and 2 studies had to have a sufficient wash-out of the previously taken hypnotics.4,6 In real-world practice, many patients with insomnia have various comorbidities such as psychiatric disorder(s) and have been receiving insomnia treatment. As a result, efficacy and safety of LEM add-on therapy and switch to LEM, both of which were common in daily practice in China, remain to be elucidated. In addition, patients seeking insomnia treatment in real-life practice vary widely in insomnia severity, age and use of benzodiazepine receptor (BZDR) agonist(s) (BZRAs). Therefore, investigating efficacy of LEM across different treatment patterns, age groups, insomnia severities and concomitant use of BZRAs, along with its effects on mood disorders such as depression and anxiety, in a real-world setting is important for clinical practice. The findings could guide treatment decisions. Consistent efficacy observed across different subgroups could provide additional evidence that LEM is broadly applicable to the overall population, reflecting the extent to which the efficacy observed in the overall population applies to a target subgroup of patients. On the other hand, if inconsistent efficacy is observed among different subgroups of patients, proper interpretation of the inconsistency could also inform clinical practice and provide insights for further analyses and research. Furthermore, exploring efficacy differences across various patient populations is also an essential component of benefit–risk assessment. To date, only one case report and one retrospective study from a single center have explored the efficacy and safety of LEM in treating Chinese insomnia patients in real-world settings.10,11 Studies that performed comprehensive subgroup efficacy analyses of LEM have also been lacking. The current multicenter, prospective, real-world observational study assessed efficacy and safety of LEM treatment for patients with insomnia in routine clinical practice in China, with pre-specified subgroup efficacy analyses across different treatment patterns, age groups, insomnia severities as well as concomitant use of BZRAs. Such a comprehensive study could provide useful information to clinicians in China who wish to consider LEM as a treatment option for their patients with insomnia. This study was conducted under the Hong Kong and Macao Medicine and Equipment Connect policy that allows designated hospitals in the Greater Bay Area (GBA) to utilize drugs and medical devices that are already approved in Hong Kong or Macao but have not yet received formal approval from the National Medical Products Administration (NMPA) in mainland China. Under this policy, LEM was approved for the treatment of insomnia in designated hospitals in the GBA by the Guangdong Provincial Food and Drug Administration on January 16, 2023.
Materials and Methods
Patients and Study Design
This multicenter, prospective, real-world observational study was carried out at the following five hospitals in China: 1) Guangdong Provincial People’s Hospital, 2) Nanfang Hospital, 3) Guangzhou United Family Hospital, 4) Sun Yat-sen Memorial Hospital, and 5) Clifford Hospital. This study was conducted in designated hospitals in the GBA, leveraging the Hong Kong and Macao Medicine and Equipment Connect policy that allows early access to drugs not yet fully approved by NMPA. The study was conducted in accordance with the principle of the Declaration of Helsinki. All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the Institutional Review Board of Guangdong Provincial People’s Hospital (approval number: KY2023-1072-02). The privacy rights of human subjects have been observed, and written informed consent to be part of the study was obtained from all participating patients. The study was registered prospectively at clinicaltrials.gov (NCT06225947) on January 17, 2024. The reporting of this study adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
This is a 12-week study consisting of a core 4-week treatment period followed by an exploratory 8-week treatment period, with follow-up visits after 1, 2, 4 and 12 weeks of LEM treatment.
The inclusion criteria were as follows: 1) Adult patients diagnosed with insomnia according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and patients with acute or subacute insomnia (symptoms lasting <3 months) were also eligible, 2) had a baseline Insomnia Severity Index (ISI) score of ≥10, and 3) were in need of pharmacotherapy for insomnia as determined by their physicians.
Exclusion criteria: 1) Severe depression and/or anxiety disorder (the Patient Health Questionnaire-9 [PHQ-9] ≥20 and/or the General Anxiety Disorder-7 [GAD-7] ≥15), 2) any suicidal ideation or a history of suicide, 3) history of serious medical conditions, psychiatric disorders, taking medication(s) that might cause insomnia or excitement, and uncontrolled poor sleep habits that may interfere with the study assessment or participant safety, as judged by the physicians, 4) narcolepsy, or 5) females who were breastfeeding or pregnant.
The patient enrolment started on February 22, 2024 and was completed on February 28, 2025. The last patient out was on May 28, 2025.
Treatment
All of the enrolled patients took LEM (DAYVIGO, Eisai, Tokyo, Japan) orally at bedtime qn. The physicians determined the dose of LEM for their patients according to the Food and Drug Administration approved package insert of LEM and their routine clinical practice.12 Generally, the initial daily LEM dose was 5mg and could be up-titrated to 10mg after seven days if the efficacy was unsatisfactory, as reported by the patients. The maximum permissible dose was 10mg/day. LEM monotherapy was prescribed for hypnotics-naïve patients. In the case of patients who had been taking other hypnotics before their enrollment, switch to LEM was the top choice. For those patients who could not tolerate the switch, LEM add-on (adding LEM to the existing treatment regimen) was used. The switch to LEM could be direct, in which patients discontinued prior hypnotics on the same night they began LEM treatment, or managed with a gradual taper of the concomitant hypnotics. In patients who started LEM as an add-on therapy, the dose of concomitant hypnotics could be reduced later during the 12-week treatment if the patient tolerated the reduction. Though not mandatory, all patients were educated at the beginning and during the study about the importance of maintaining a regular daily routine.
Dose increase of hypnotics other than LEM or taking sedating medications or non-pharmacological treatment in addition to those taken since the beginning of the study was not allowed during the first four weeks of the study. Hypnotics other than LEM and sedating medications included BZRAs (BZDs and Z drugs), melatonin agonists such as ramelteon, sedative antidepressants such as trazodone, antipsychotics such as quetiapine and H1-antihistamine drugs such as diphenhydramine. Non-pharmacological treatment consisted of CBT for insomnia.
Finally, patients who wished to withdraw from the study before completing 4 weeks of LEM treatment were required to provide a reason, whereas after 4 weeks of treatment, they could stop at any time without providing a reason.
Data Collection
During the baseline visit, the following information was collected: age, gender, weight, height, duration of insomnia, use of hypnotics and/or psychotropic medications, presence or absence of depression and/or anxiety. Patients were asked to complete the ISI, PHQ-9 and GAD-7 and their baseline ISI, PHQ-9 and GAD-7 scores were determined.
During each follow-up visit, patients completed the ISI, PHQ-9 and GAD-7 and their ISI, PHQ-9 and GAD-7 scores were determined. In addition, treatment-emergent adverse events (TEAEs) were recorded.
Efficacy Outcome Measures
The primary endpoint was remission rate (the proportion of patients with an ISI<8 [no clinically significant insomnia]) after 4 weeks of LEM treatment. The ISI is a validated, self-report questionnaire that assesses insomnia severity and it consists of seven items: 1) Difficulties in sleep onset; 2) difficulties in sleep maintenance; 3) early morning awakening; 4) dissatisfaction with sleep; 5) interference with daytime functioning; 6) noticeability of sleep difficulties by others; and 7) distress caused by difficulty in sleep.2,11 Each item is scored by a patient on a scale of 0 (no problem) to 4 (very severe problem) and the ISI total score is the sum of the seven scores. An ISI total score of 0–7, 8–14, 15–21 and 22–28 indicates no clinically significant insomnia, subthreshold (mild) insomnia, moderate insomnia and severe insomnia, respectively.2,13 In addition, responders were those patients who had a ≥6-point reduction in their ISI total scores from baseline. The ≥6-point reduction was set as the criterion for LEM responders because it has been reported that a 6-point reduction in ISI represented clinically meaningful improvement in insomnia.14
Secondary endpoint included: 1) Remission rate after 1 and 2 weeks of LEM treatment; 2) responder rate after 1, 2 and 4 weeks of treatment, 3) changes in the ISI, PHQ-9 and GAD-7 scores from baseline after 1, 2 and 4 weeks of treatment, and 4) changes in the ISI nighttime sub-score (sum of the scores of items 1–3) and daytime impact sub-score (sum of the scores of items 4–7) from baseline after 1, 2 and 4 weeks of treatment.
Exploratory endpoints were remission rate, responder rate, and the ISI, PHQ-9 and GAD-7 changes from baseline after 12 weeks of LEM treatment.
In addition, subgroup analyses of remission rates, responder rates and ISI changes from baseline based on treatment pattern, baseline insomnia severity, age and concomitant use of BZRAs were performed.
Furthermore, factors associated with insomnia remitters, LEM responders and ISI changes from baseline after 4 weeks of LEM treatment were identified.
Safety
Safety assessments were conducted at every follow-up visit throughout the study and at the end of study. These assessments consisted of monitoring and recording all adverse events (AEs). TEAEs and treatment-related TEAEs were recorded using the Medical Dictionary for Regulatory Activities (MedDRA) version 26.0, and their severities were graded according to the Common Terminology Criteria for Adverse Events (CTCAE).15
Sample Size
According to the post hoc analysis of the SUNRISE 2 study, the percentage of subjects with an ISI total score below 8 for LEM 5 mg was 21.8% at month 1, compared to 11.3% for placebo.13 As every patient enrolled in our study had a baseline ISI score of ≥10, lower than the ≥15 points required for the patients enrolled in the SUNRISE 2 study, a higher placebo remission rate than that reported in the SUNRISE 2 study was expected. Assuming a target remission rate of 14% after 4 weeks of treatment (2.7% higher than that in the SUNRISE 2 study), and setting the expected remission rate after 4 weeks of LEM treatment at 22%, which was 8% higher than the target remission rate, at least 166 patients were needed to have a statistical power of 80% for a one-sided test at a significance level of 0.025.16 Assuming a dropout rate of 20%, it was planned that 200 patients would be enrolled.
To test the robustness of the sample size, a sensitivity analysis was conducted. Assuming a placebo remission rate between 14%-18%, a sample size of 200 provided a >80% power to detect a treatment difference of ≥8% between LEM and placebo. Specifically, a single-group design was used to test whether the proportion was greater than x=0.11–0.18 (H0: P ≤ x versus H1: P >x). The comparison was made using a one-sided, one-sample exact test, with a Type I error rate (α) of 0.025. To detect a difference (P1 - P0) of 0.08 with a sample size of 200, the power was 0.9067–0.8058.
Statistical Analysis
Patient demographics and baseline clinical characteristics were analyzed in the full analysis set (FAS) (all patients who received ≥1 dose of LEM and had at least one post-dosing efficacy assessment). Efficacy analyses were performed in the FAS and the per-protocol set (PPS) (all patients who completed the study without major protocol deviations, in this case, all patients who complete the core 4-week treatment without increasing dose of hypnotics other than LEM or taking sedating medications in addition to those taken since the beginning of the study). Safety analyses were performed in the safety set (SS) (all patients who received ≥1 dose of LEM and had at least one post-dosing safety assessment). Missing data for remission rate and responder rate after 4 weeks of treatment in the FAS population were imputed using last observation carried forward (LOCF), and other missing data were not imputed. For those patients who stopped taking LEM before the end of the study, efficacy data recorded after their treatment discontinuation were not imputed. In addition, sensitivity analyses of the remission rates and responder rates were conducted wherein missing data were imputed using multiple imputation.
Descriptive analysis was used. Quantitative variables with normal distribution and with non-normal distribution were expressed as mean±standard deviations (SD) and median (interquartile range [IQR] or range), respectively. Qualitative variables were expressed as n (%). Between-group comparisons of continuous variables were performed using group t test or Wilcoxon rank sum test. Comparisons among ≥3 groups of continuous variables were performed using analysis of variance (ANOVA) or Kruskal–Wallis rank sum test. Paired t test or Wilcoxon signed-rank test was used for intragroup comparisons of continuous variables, chi-square test or Fisher’s exact test was used for intragroup comparisons of categorical variables, and Wilcoxon rank sum test or Cochran–Mantel–Haenszel test was used for intragroup comparisons of ranked variables.
Multivariate logistic regression analyses were conducted to identify factors associated with insomnia remitters and LEM responders after 4 weeks of LEM treatment. Multivariate linear regression analysis was conducted to identify factors associated with changes in ISI total scores from baseline after 4 weeks of treatment. All of the regression analyses included gender, age, body mass index (BMI), duration of insomnia, treatment pattern, severities of insomnia, depression and anxiety, and concomitant use of BZRA(s) as independent variables.
Kaplan-Meier curves were plotted to analyze the occurrence of somnolence, nightmare and headache.
If and only if the lower limit of the 95% CI for the primary endpoint (remission rate after 4 weeks of LEM treatment) is above the target value of 14%, achieving statistical significance, can the study be considered to have met its primary endpoint goal. The P values from statistical analyses of other endpoints were regarded as descriptive analyses only.
SAS 9.4 (SAS Institute, Cary, NC, United States) was used for the statistical analyses in the study. Statistical significance was achieved with a P value of 0.05.
Results
Demographic and Baseline Characteristics of Patients
Study flow chart was depicted in Figure 1. A total of 205 patients were enrolled. The FAS included 200 patients and the SS included 205 patients. One hundred and sixty patients completed the core 4-week LEM treatment and did the subsequent follow-up visit. The PPS included 135 patients. Thirty-six patients completed the subsequent exploratory 8-week treatment and did the subsequent follow-up visit (Figure 1).
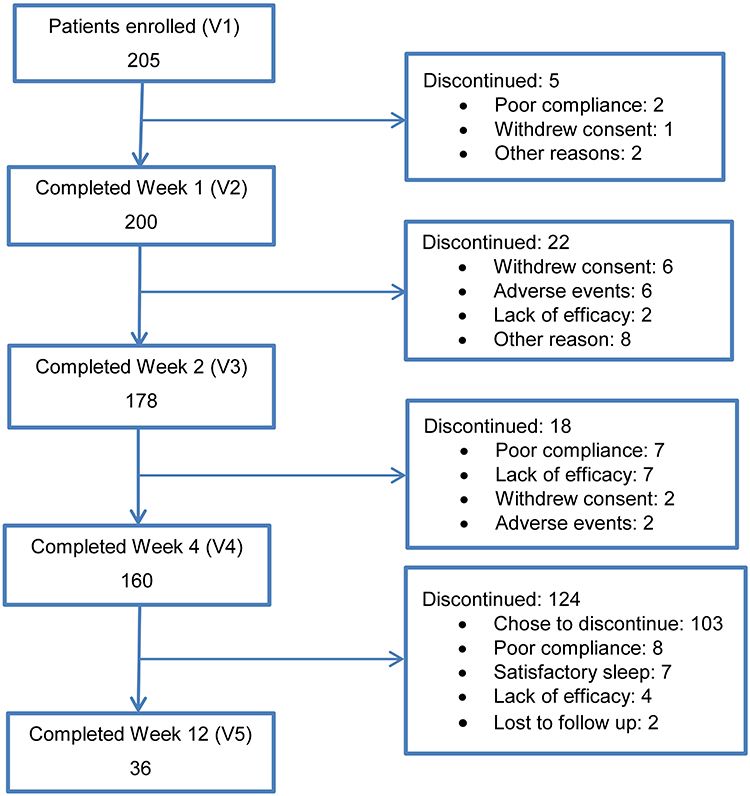 |
Figure 1 Study flow chart. Abbreviation: V, Visit. |
Patient demographics and baseline characteristics were reported in Table 1. The FAS had a mean age of 46.08±14.56 years and 124 (62.0%) of them were female. They had a mean duration of insomnia of 7.55±8.66 years and a mean baseline ISI score of 17.44±4.45. Among them 180 (90.91%) patient had chronic insomnia and 18 (9.09%) patients had acute or subacute insomnia. The most common symptoms of insomnia were difficulties in sleep initiation, sleep maintenance and falling back asleep after waking up (97.0%, 84.5% and 59.0% respectively), and being easily awakened (62.0%). Seventy-five (37.5%) patients used concomitant BZDs and 44 (22.0%) patients used concomitant Z drugs. Forty-two (21.0%), 33 (16.5%) and 125 (62.5%) patients received LEM monotherapy, switched to LEM and received LEM add-on therapy, respectively (Table 1). One hundred and ninety-four (97.0%) patients started with LEM 5mg qn, One hundred and fifty-three (76.5%) and 15 (7.5%) patients had a final LEM daily dose of 5mg and 10mg, respectively. Sixty-eight (34.0%) patients have comorbid depression and 109 (54.5%) patients had comorbid anxiety (Table 1).
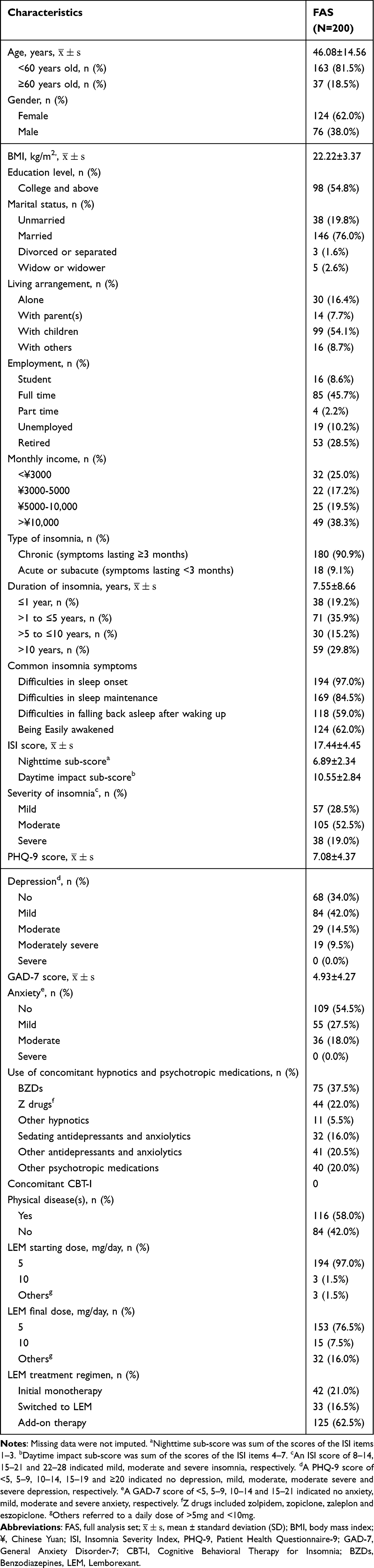 |
Table 1 Demographics and Baseline Clinical Characteristics |
Ninety-six (48.0%) patients took concomitant BZRA(s) with a median baseline daily diazepam equivalence dose of 8.00mg (IQR 5.00mg, 20.00mg). After 4 weeks of LEM treatment, their daily diazepam equivalence dose was significantly reduced (median 8.00mg [IQR 4.00mg,16.00mg], P=0.009), and 52 (55.3%) of the patients took concomitant BZRAs at a reduced dose.
Among the 33 patients who switched to LEM, 23 (69.7%) patients switched to LEM directly, discontinuing their prior hypnotics on the same night they started taking LEM, and 10 (30.3%) patients initiated LEM treatment while gradually tapering off their concomitant hypnotics. After 4 weeks of LEM treatment, 30 (90.9%) of the 33 patients discontinued their previous hypnotics and took LEM only (Supplementary Table S1).
Remission Rates, Responder Rates and Changes in the ISI Scores from Baseline
In the FAS, remission rate after 4 weeks of LEM treatment was 30.5% (61/200) (95% CI: 24.2%, 37.39%). Responder rate after 4 weeks of treatment was 55.0% (110/200) (95% CI: 47.82%, 62.02%). Additionally, remission rates after 1 and 2 weeks of treatment were 16.0% (32/200) and 26.4% (47/178), respectively, and the respective responder rates after 1 and 2 weeks of treatment were 36.0% (72/200) and 56.2% (100/178). The PPS showed a similar trend to the FAS in remission rates and responder rates across the treatment period (Table 2). Sensitivity analyses using multiple imputation for missing data produced similar results (Supplementary Table S2).
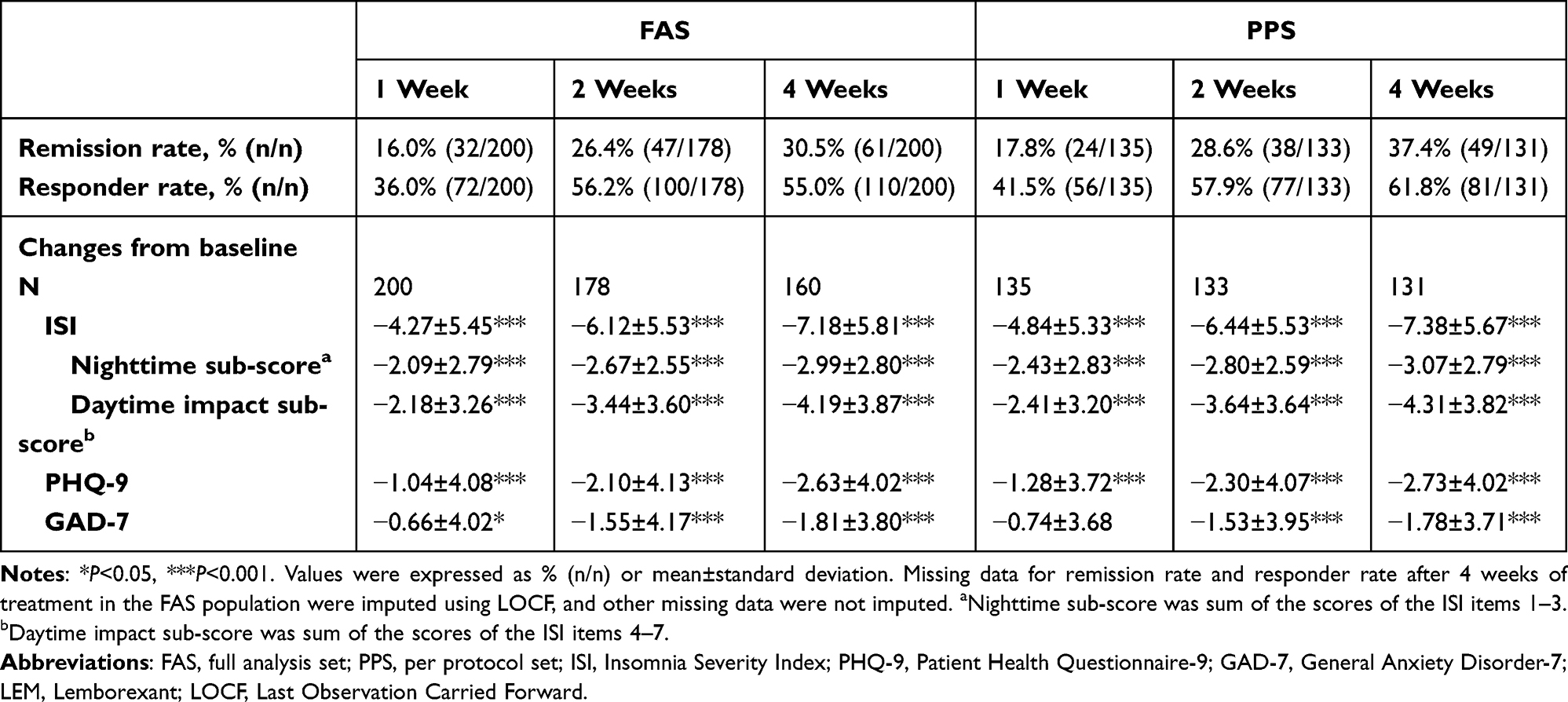 |
Table 2 Remission Rates, Responder Rates and Changes in the ISI, PHQ-9 and GAD-7 Scores from Baseline After LEM Treatment |
In both the FAS and the PPS, the ISI scores decreased significantly from baseline after 1 week of LEM treatment (FAS: −4.27±5.45, P<0.001) and kept decreasing (FAS: −6.12±5.53 and −7.18±5.81 after 2 and 4 weeks of treatment, respectively, both P<0.001) (Table 2). In addition, significant decreases in both the ISI nighttime sub-score and daytime impact sub-score were observed after 1 weeks of treatment, and both sub-scores continued to decrease during the next 3 weeks of treatment (Table 2).
Subgroup Analyses of Remission Rates, Responder Rates and Changes in the ISI Scores
Treatment regimen-based subgroup analyses of the FAS revealed significant differences in remission rates and responder rates after 4 weeks of LEM treatment among patients who received initial LEM monotherapy, who switched to LEM and who had LEM add-on therapy (P=0.021 and 0.040, respectively). Patients on initial monotherapy had the highest remission rate and responder rate (54.1% [20/37] and 78.4% [29/37], respectively) (Figure 2A and B). In addition, patients on initial monotherapy had an insignificant trend of greater ISI decrease than patients who switched to LEM and those who received LEM add-on therapy after 4 weeks of treatment (−9.03±4.87, −6.86±4.79 and −6.56±6.30, P=0.085), The PPS results were consistent with the FAS results (Supplementary Figure S1A and B).
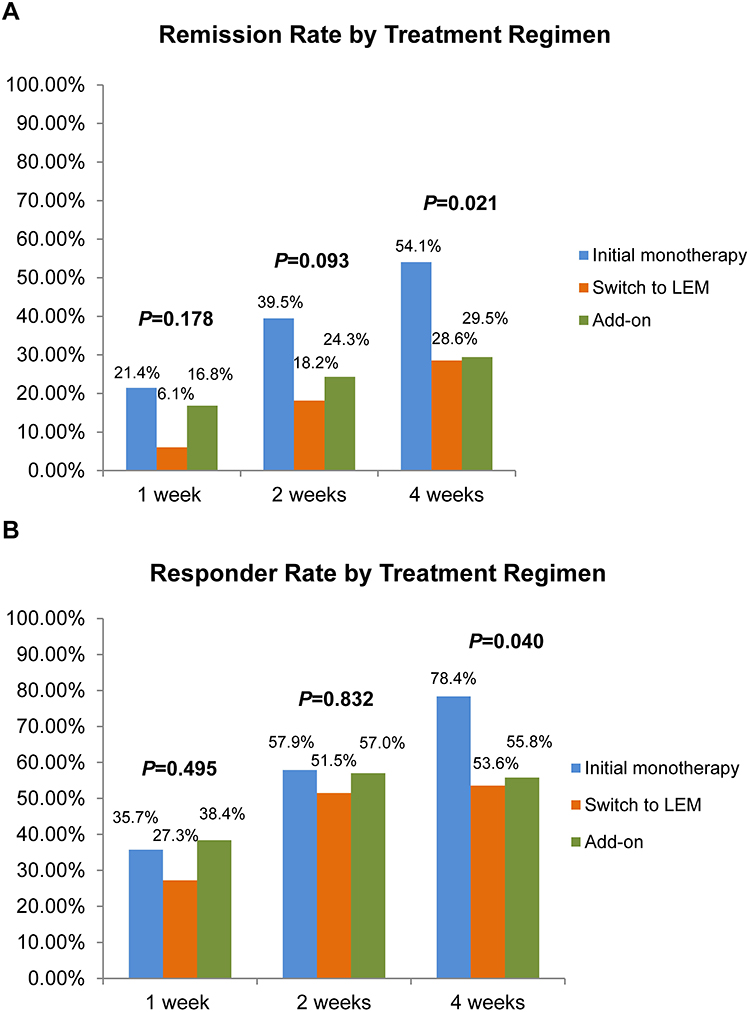 |
Figure 2 Treatment regimen-based subgroup analyses in the FAS population. (A) Remission rates and (B) Responder rates after 1, 2 and 4 weeks of LEM treatment in patients receiving initial LEM monotherapy, those who switched to LEM and those receiving LEM add-on. Abbreviations: FAS, full analysis set; LEM, Lemborexant. |
Subgroup analyses of the FAS based on baseline insomnia severity revealed significant difference in remission rates among patients with mild, moderate and severe baseline insomnia after 2 weeks of treatment (P=0.005), with remission rate being the highest in patients with mild baseline insomnia (38.8% [19/49]). Similar insignificant differences were observed among the three groups of patients after 1 and 4 weeks of treatment (P=0.066 and 0.075, respectively) (Figure 3A). Results from the PPS were consistent with the FAS results (Supplementary Figure S2A).
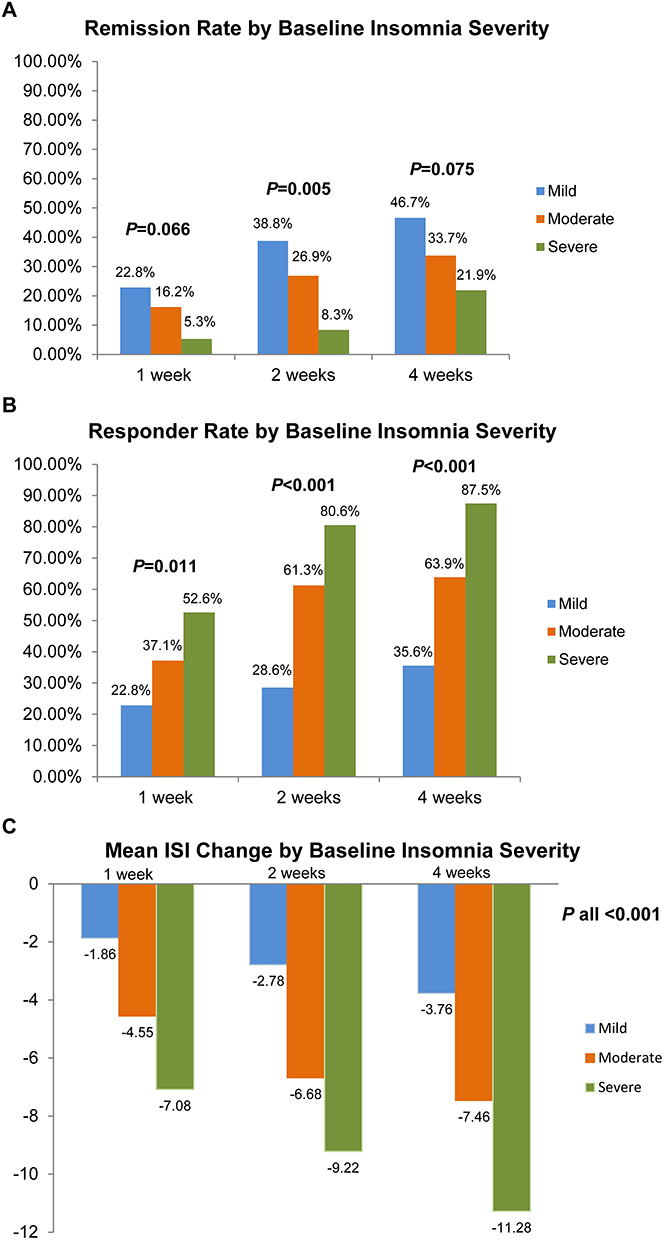 |
Figure 3 Baseline insomnia severity-based subgroup analyses in the FAS population. (A) Remission rates, (B) Responder rates and (C) ISI changes from baseline after 1, 2 and 4 weeks of LEM treatment in patients with mild, moderate and severe baseline insomnia. An ISI score of 8–14, 15–21 and 22–28 indicated mild, moderate and severe insomnia, respectively. Abbreviations: FAS, full analysis set; ISI, Insomnia Severity Index; LEM, Lemborexant. |
Responder rates after 1, 2 and 4 weeks of treatment were also significantly different among patients with mild, moderate and severe baseline insomnia (P=0.011, <0.001 and <0.001, respectively), and so were ISI decreases from baseline (all P<0.001). Responder rates and ISI decreases were the highest in patients with severe baseline insomnia and the lowest in patients with mild baseline insomnia (87.5% [28/32] vs 35.6% [16/45], and −11.28±5.46 vs −3.76±5.04 after 4 weeks of treatment, respectively) (Figure 3B and C, Supplementary Table S3). The PPS produce the same results as the FAS (Supplementary Figure S2B and C and Table S3).
Patients <60 years old and those ≥60 years old in the FAS and the PPS had comparable remission rates, responder rates and ISI changes from baseline after 1, 2 and 4 weeks of LEM treatment (P all >0.05), Additionally, in both the FAS and the PPS, patients receiving concomitant BZRA(s) and those not taking concomitant BZRA(s) had comparable remission rates, responder rates and ISI changes after 1, 2 and 4 weeks of treatment (P all >0.05).
Factors Associated with Insomnia Remitters, LEM Responders and Change in the ISI Score After 4 Weeks of Treatment
Multivariate logistic regression analyses revealed that compared with patients with mild insomnia, patients with severe baseline insomnia were less likely to be insomnia remitters (odd ratio [OR] 0.211, 95% CI: 0.06–0.76, P=0.018) and were more likely to be LEM responders (OR 31.192, 95% CI: 6.59. 147.74, P<0.001) after 4 weeks of treatment. Patients with moderately severe baseline insomnia were also more likely than those with mild insomnia to be LEM responders (OR 4.464, 1.81, 11.02, P=0.001). In addition, compared with patients who received LEM initial monotherapy, patients who received LEM add-on were less likely to be insomnia remitters (OR 0.331, 95% CI: 0.12, 0.94, P=0.038) and LEM responders (OR 0.175, 95% CI: 0.05, 0.61, P=0,007). Finally, patients who switched to LEM was less likely to be LEM responders than patients who received initial LEM monotherapy (OR 0.131, 95% CI: 0.03–0.50, P=0.003) (Table 3).
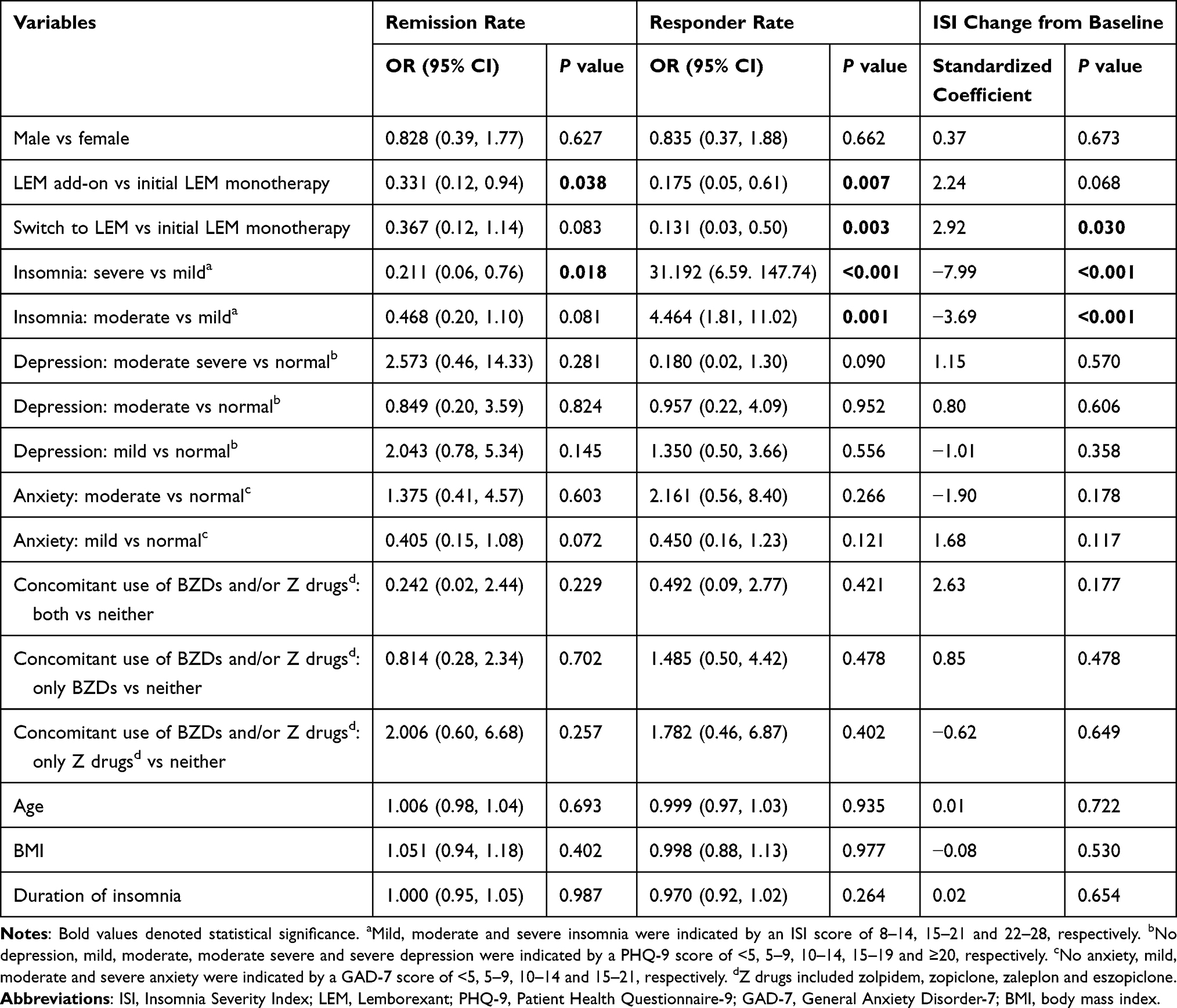 |
Table 3 Regression Analyses of Factors Associated with Remitters, LEM Responders and ISI Change from Baseline After 4 Weeks of LEM Treatment |
Multivariate linear regression analysis revealed that moderate or severe baseline insomnia was significantly associated with greater decrease in ISI score from baseline compared with mild insomnia (Standardized coefficient −3.69 and −7.99, respectively, both P<0.001). In addition, switch to LEM was significantly associated with less decrease in ISI score from baseline compared with initial LEM primary monotherapy (Standardized coefficient 2.92, P=0.030) (Table 3).
Changes in the PHQ-9 and GAD-7 Scores After LEM Treatment
The patients had a mean baseline PHQ-9 and GAD-7 scores of 7.08±4.37 and 4.93±4.27, respectively. In both the FAS and the PPS, there was significant decrease in the PHQ-9 score after 1 week of treatment (FAS: −1.04±4.08, P<0.001) and the decrease continued (FAS: −2.63±4.02 after 4 weeks, P<0.001) (Table 2).
LEM treatment led to significant decrease in the GAD-7 score in the FAS after 1 week of treatment (−0.66±4.02, P=0.016) and the decrease continued (−1.81±3.80 after 4 weeks of treatment, P<0.001). While in the PPS, although the decrease was not significant after 1 week of treatment, it became significant after 2 weeks of treatment and was maintained over the next 2 weeks (Table 2).
Efficacy After 12 Weeks of Treatment
Thirty-six patients in the FAS completed the 12-week treatment as well as the end-of study follow-up visit. Twenty-nine (80.6%) of the patients stopped taking concomitant hypnotics and received LEM only, and the remaining seven patients took still took concomitant hypnotics in combination with LEM. The remission rate and responder rate after 12 weeks of treatment were 27.8% (10/36) and 69.4% (25/36), respectively, and their mean ISI scores decreased significantly from baseline (−7.72±6.31, P<0.001). In addition, after 12 weeks of treatment, significant decreases were observed in their PHQ-9 and GAD-7 scores as well (−3.36±5.44, P<0.001; −2.81±5.23, P=0.002, respectively). The PPS results were consistent with the FAS results.
Safety
The SS included 205 patients. Forty-three (21.0%) patients reported at least one TEAE and 37 (18.1%) of them had treatment-related TEAEs. Forty-one (20.0%) patients had CTCAE grade 1 TEAEs and 5 (2.4%) patients had grade 2 TEAEs. None of the patients had any grade ≥3 TEAEs (Table 4). Ten (4.9%) patients withdrew from the study due to TEAEs and the most common TEAEs leading to withdrawal were somnolence (5 [2.4%]), dizziness (4 [2.0%] and nightmare (2 [1.0%]). Overall, the most common TEAEs were somnolence (14 [6.8%]), dizziness (11 [5.4%]), nightmare (8 [3.9%]), fatigue (6 [2.9%]) and headache (5 [2.4%]) (Table 4).
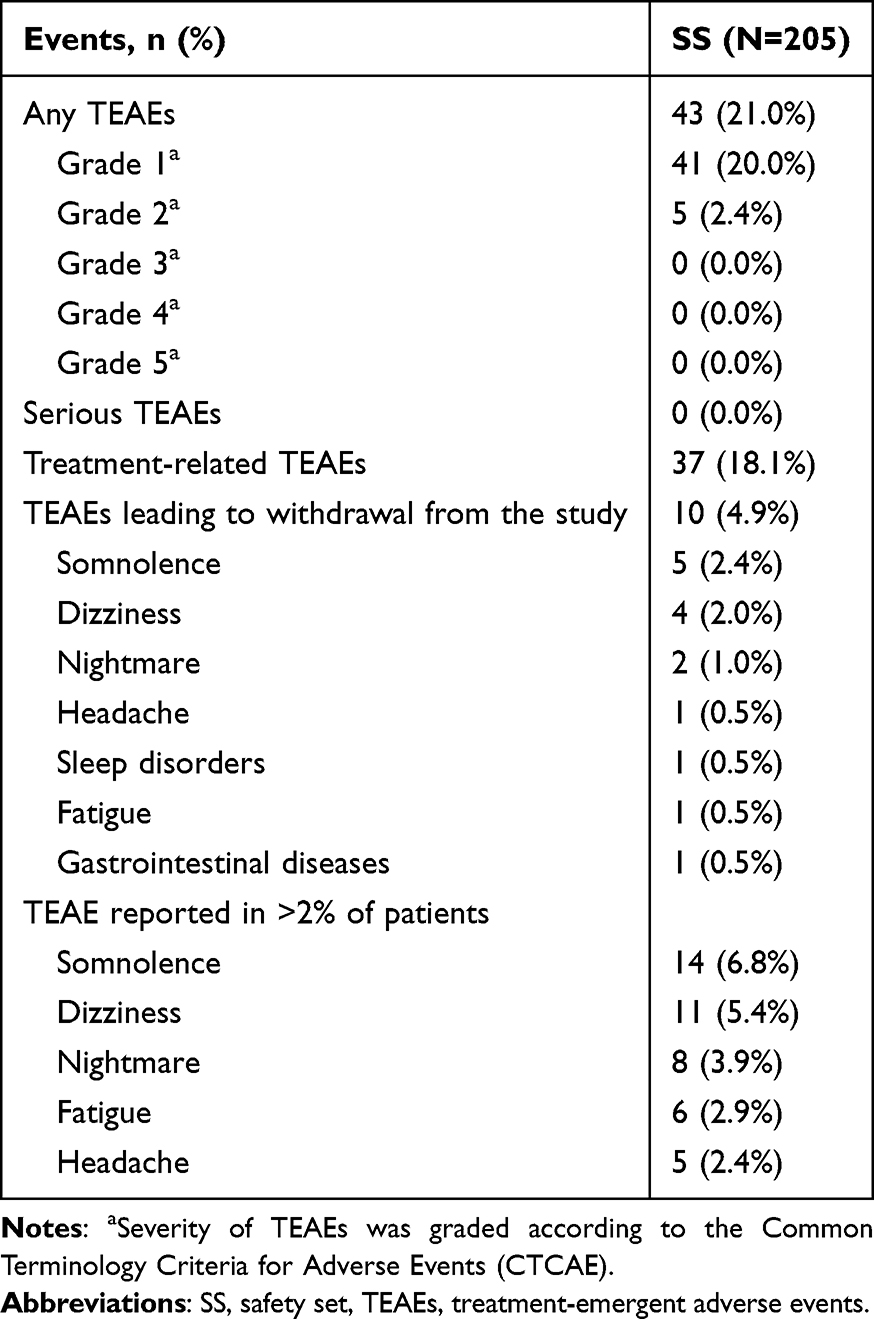 |
Table 4 Treatment-Emergent Adverse Events (SS) |
Most incidents of somnolence, nightmare and headache started during the first 20 days of the treatment and lasted 10.64±7.32 days, 12.00±14.94 days and 13.67±7.51 days, respectively (Figure 4).
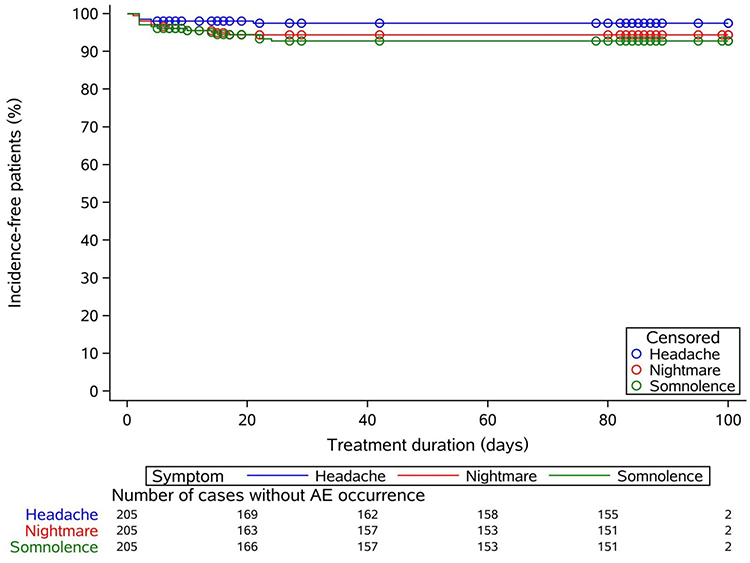 |
Figure 4 Kaplan-Meier curves for the occurrence of somnolence, nightmare and headache. |
Discussion
In this first prospective study of LEM treatment in Chinese patients with insomnia in real-world setting, LEM was effective and safe in treating insomnia. The patient population in this observational study included a higher percentage of patients with psychiatric comorbidities than the SUNRISE 1 and 2 studies.4,6 The remission rate and responder rate after 4 weeks of LEM treatment was 30.5% and 55.0%, respectively. Additionally, LEM treatment led to significantly decreased ISI, PHQ-9 and GAD-7 scores. We also found that compared with patients with mild baseline insomnia, patients with severe baseline insomnia were less likely to be insomnia remitters but more likely to be LEM responders and to have greater ISI decreases. Furthermore, compared with patients who received initial LEM monotherapy, patients who switched to LEM were less likely to be LEM responders and to have greater ISI decrease. Additionally, patients who received LEM add-on were less likely to be insomnia remitters and LEM responders than patients who received initial LEM monotherapy. Finally, LEM treatment was well-tolerated in our study and all of the TEAEs were mild or moderate. The most common TEAEs were somnolence, dizziness and nightmare.
Our findings on the remission rates, responder rates and significantly decreased ISI scores were consistent with previous studies.13,17 Roth et al, a post-hoc analyses of the global, double-blinded Phase 3 RCT SUNRISE 2, found that the remission rates for LEM 5mg qn and LEM 10mg qn after 1 month of treatment were 21.8% and 22.2%, respectively, and were 25.9% and 29.2% after 3 months of treatment, respectively.1,6,13 In addition, it reported that the responder rates for LEM 5mg and 10mg qn were 44.0% and 44.4% after 1 months of treatment, respectively, and were 53.5% and 52.1% after 3 months of treatment, respectively.1,6,13 Finally, it also reported significant decreases in ISI score from baseline after 1 months of treatment (−7.1±5.9 and −7.2±6.4 for LEM 5mg and 10mg qn, respectively) and after 3 months of treatment (−8.6±6.3 and −8.9±6.4 for LEM 5mg and 10mg qn, respectively).13 Ozone et al, an open-label, multicenter trial, reported that remission rates for patients who transitioned to LEM increased from 13.3% at baseline to 28.7% after 2 weeks of treatment, to 45.1% after 6 weeks of treatment and to 49.3% after 14 weeks of treatment.17 Their observations were similar to our findings that the remission rates increased from week 1 to week 2 and from week 2 to week 4. Remission rates in our study were very similar to the increase of remission rates from baseline in Ozone et al, and ISI decreases in our study were similar to those reported by Roth et al13,17 The higher responder rates in our study compared with Roth et al were probably due to the stricter criterion for LEM responders (≥7-point reduction in ISI) adopted by Roth et al than ours (≥6-point reduction). In addition, consistent with Jian et al that observed significantly decreased scores of all of the seven items of ISI after 4 weeks of LEM treatment in Chinese patients,11 our study found that both the ISI nighttime sub-scores and daytime impact sub-score decreased significantly after 1 week of LEM treatment and continued to decrease. Overall, like previous studies, our study demonstrated that LEM were effective in treating adult Chinese patients with insomnia, and its effectiveness applied to both the nighttime symptoms and daytime impact of insomnia.
Unlike RCTs, our observational study did not include a placebo group. However, placebo effect was included in the sample size calculation in our study. In addition, a post-hoc analysis of the SUNRISE 2 study, one of the two pivotal studies that established the effectiveness and safety of LEM in treating insomnia and led to its FDA approval, found that placebo remission rate after 1 month of treatment was 11.3%, compared with the 21.8% and 22.2% remission rates associated with LEM 5 mg and 10 mg per night, respectively.13 Adopting this placebo remission rate, the 30.5% remission rate in our study suggested that the net remission rate was approximately 19.2%, Therefore, the effectiveness of LEM was indicated. Furthermore, in a RCT of sequential therapy for insomnia, patients treated with 6 weeks of zolpidem, a commonly prescribed Z drug, had a remission rate (ISI<8) of 30.3%,18 very similar to the remission rate associated with LEM in our study.
The exploratory endpoint, remission rate after 12 weeks of LEM treatment was 27.8%, numerically lower than the remission rate after 4 weeks of treatment (30.5%). The SUNRISE 2 study have demonstrated sustained efficacy of LEM over 12 months.1,6 In addition, a post hoc analysis of the SUNRISE 2 study reported higher remission rate after 3 months than after 1 months of LEM treatment (25.9% vs 21.8% for LEM 5mg qn, and 29.2% vs 22.2% for LEM 10mg qn), and even higher remission rate after 12 months of treatment (36.1% for LEM 5mg qn and 34.6% for LEM 10mg qn).13 In our study, only 36 patients completed 12 weeks of LEM treatment and 103 patients chose to discontinue the study. Therefore, the observed decline in the remission rate here was most likely due to its small sample.
Our study further found that among patients with mild, moderate and severe baseline insomnia, patients with severe insomnia had the highest responder rate and the greatest ISI decrease, while patients with mild insomnia had the lowest responder rate and the smallest ISI decrease. On the other hand, patients with mild insomnia tended to have a lower remission rate than those with moderate insomnia, who tended to have a lower remission rate than those with severe insomnia. This finding was corroborated by our multivariate regression analyses, as it revealed that compared with patients with mild baseline insomnia, patients with severe baseline insomnia were less likely to be insomnia remitters but more likely to be LEM responders and to have greater ISI decreases. The FLUID study is a single-arm trial that assessed LEM treatment in adult patients with insomnia using sleep electroencephalogram (EEG) monitor.7 Its relationship analysis between baseline and post-LEM treatment improvement revealed that poor sleep at baseline was associated with greater improvement in latency to persistent sleep, wake after sleep onset, total sleep time and sleep efficiency, and it concluded that patients with mild insomnia benefited modestly from LEM treatment while patients with severe insomnia benefited significantly from LEM.7 It further suggested that LEM could effectively remediate insomnia in severe cases without leading to unnecessarily prolonged sleep in mild cases, making it effective as well as well-tolerated.7 Our observations seemed to support their results. A seeming contradiction in our findings was the lowest remission rate and the highest responder rate associated with severe baseline insomnia as well as the highest remission rate and the lowest responder rate associated with mild insomnia. However, this observation makes sense as compared with patients with severe insomnia (baseline ISI 24.18±2.15), considerably less ISI decrease was needed for patients with mild insomnia (baseline ISI 12.30±1.13) to achieve remission (ISI<8). In addition, patients with higher ISI baseline scores (severe insomnia) had more room for ISI reduction upon treatment and thus were more likely to have a greater treatment response than patients with lower ISI baseline scores.19 Therefore it was much easier for patients with mild insomnia to achieve remission although they had smaller ISI decrease and lower responder rates.
As patients with mild insomnia in our study achieved the highest remission rates with the smallest absolute ISI changes, some may wonder whether these patients could have experienced spontaneous fluctuation comparable to the ISI changes associated with LEM and recovered without pharmacological treatment and whether pharmacotherapy was justified. Indeed, some patients with mild insomnia in real life may recover without pharmacological intervention. For those individuals, the decision to prescribe sleep medication should be made on a case-by-case basis. However, in our study, most patients had chronic insomnia and many had been taking sleep medication(s) long term. In addition, all of the patients in our study expressed a preference for long-term pharmacotherapy. Because LEM had a good safety profile and did not lead to rebound insomnia or withdrawal symptoms,3,7 they wished to try it as a treatment for insomnia.
In our study, patients receiving initial LEM monotherapy had significantly higher responder rate, remission rate as well as an insignificant trend of greater ISI decrease than those who switched to LEM and who received LEM add-on therapy. Our multivariate regression analyses had similar findings. Compared with patients who received initial LEM monotherapy, patients who switched to LEM were less likely to be LEM responders and to have greater ISI decrease. In addition, patients who received LEM add-on were less likely to be insomnia remitters and LEM responders than patients who received initial LEM monotherapy. Our observation was in line with Tanaka-Mizuno et al, a nationwide claims database study of switch to and add-on LEM in Japan.19 It found that hypnotics-naïve patients had higher success rate than patients who switched to LEM and those who received LEM add-on, wherein success was defined as when a patient was prescribed LEM monotherapy or when no hypnotics was prescribed during days 180–210 after LEM was initially prescribed (day 0).20 As patients who received initial LEM monotherapy were hypnotics-naïve, with no prior hypnotic exposure and thus no tolerance to any sleep medications, they would have responded better to any sleep medication(s) than patients who had prior exposure, particularly those who switched to LEM, many of whom had to contend with withdrawal reactions. As expected, findings from our study as well as from Tanaka-Mizuno et al suggested that LEM performed best in hypnotics-naïve patients. Finally, we acknowledge that a limitation of our treatment regimen-based efficacy analyses was that the multivariate regression models did not account for duration of prior insomnia pharmacotherapy, the specific sleep medications involved, or the history and degree of prior treatment failure.
Age did not affect LEM efficacy in our study, and LEM were equally effective in patients <60 years old and those ≥60 years old, making it potentially suitable for adult patients of all ages. This was consistent with Mishima et al that observed that age was not a factor affecting overall improvement in patients receiving LEM treatment5 In addition, the presence or absence of concomitant BZDs and/or Z drugs did not significantly affect efficacy of LEM in our study, again making LEM potentially suitable for a wide range of patients, including those patients who, because of serious withdrawal symptoms, receive LEM as an add-on therapy for a period of time before gradually transitioning to LEM monotherapy.
Among the 33 patients who switched to LEM, 30 patients discontinued their previous hypnotics and took LEM only 4 weeks of LEM treatment, and only three patients took concomitant hypnotics with LEM. Many long term users of BZRAs experience withdrawal reactions when they attempt to discontinue the treatment, which makes it difficult for them to stop.4,20 Our study suggested that LEM could help suppress withdrawal symptoms, thereby making it easier for patients to discontinue prior hypnotic treatment. Consistent with our findings, numerous real-world studies conducted in Japan demonstrated high success rate of switching to LEM from BZRAs.17,20,21 Furthermore, the Japanese expert consensus recommend LEM and suvorexant as first options for discontinuing or reduced BZRAs by switching to other hypnotics, a position shared by Canadian experts.22,23 Therefore, switching to LEM represents a new viable approach for patients who have difficulty discontinuing BZRAs. Moreover, also consistent with prior real-world studies,17,20,21,24 more than half of the patients who took concomitant BZRA(s) in our study had BZRA(s) dose reduction. Thus, in patients who still have insomnia while taking BZRAs and who could not tolerate switching to LEM, LEM add-on followed by dose reduction of BZRAs later could be tried as a strategy for later complete transition to LEM monotherapy.
Patients with insomnia in real life often have symptoms of depression and/or anxiety, and insomnia is a common comorbidity of both depression and anxiety,25 In order to provide some guidance for neurologists treating patients with insomnia accompanied by symptoms of depression and/or anxiety, we investigated changes in their PHQ-9 and GAD-7 scores after LEM treatment, because the PHQ-9 is a questionnaire designed to assess severity of depression and the GAD-7 is a tool for anxiety assessment.26 In our study, LEM treatment significantly decreased the patients’ PHQ-9 and GAD-7 scores, suggesting that LEM treatment could improve symptoms of depression and anxiety of our patients and this was consistent with previous studies.10,11 Insomnia increases the risk of psychiatric conditions such as depression and anxiety, and at the same time, depression and anxiety are contributing factors for insomnia.27,28 It is possible that LEM improved these patients’ symptoms of depression and anxiety by improving their sleep. However, it is also possible that the observed changes in PHQ-9 and GAD-7 were the result of spontaneous fluctuation or regression to the mean as the mean baseline PHQ-9 and GAD-7 scores in our study were relatively low (7.08 and 4.93, respectively), and their changes following 4 weeks of LEM treatment were small in magnitude (approximately 2–3 points) though statistically significant. As our study does not have a control group, a causal relationship between these changes and LEM treatment could not be established.
LEM treatment was well-tolerated in our study and all of the TEAEs were mild or moderate. As previously reported,1,4,6,7,17 the most common TEAEs were somnolence, dizziness, nightmare, fatigue and headache. All of the TEAEs in our study have been reported before and no new safety concern has been raised.1,4,6,7,13,17 The incidence of TEAEs (21.0%) and TEAEs leading to withdrawal from the study (4.9%) were close to Dash et al, a prespecified analysis of Asian patients in the SUNRISE 2 study, in which the incidence of TEAEs and TEAEs leading to withdrawal were 27.9% and 3.3% in patients receiving LEM 5mg qn during the first 6 months of treatment.2 Our observation that most incidents of somnolence, nightmare and headache started during the first 20 days of the treatment and lasted less than two weeks also suggested these TEAEs became tolerable over time.
This study has several limitations. First, as it is a 12-week study consisting of a core 4-week treatment followed by an exploratory 8-week treatment, efficacy and safety of LEM treatment beyond 4 weeks could not be determine from our study. Second, after completing the core 4-week treatment, 103 (50.2%) patients chose to discontinue the treatment and their data during weeks 5–12 were not collected, and the number of patients who completed the 12-week treatment and the subsequent follow-up visit was modest (36 patients). The Chinese guideline recommends that patients with insomnia be treated with hypnotics for no more than four weeks, after which monthly evaluations should be conducted to determine whether further treatment is needed.29 Therefore, patients who completed four weeks of LEM treatment in our study could choose not to enter the subsequent 8-week exploratory phase. As this study was conducted under the Hong Kong and Macao Medicine and Equipment Connect policy before LEM was approved by NMPA, LEM was unavailable in most of the local hospitals and its expense (about $100 per month) was not covered by insurance. As a result, many patients opted to discontinue the treatment after 4 weeks as expected. Because of the sharply decreased sample size, there was potential selection bias during Weeks 5–12 of the study and findings from this period should be viewed with this potential bias in mind. Third, as this study does not include a placebo group, the possibility of placebo effects could not be excluded considering only subjective outcome measures were adopted in our study. This real-world observational study aimed to assess the efficacy and safety of LEM in a broader patient population than the populations studied in RCTs such as the SUNRISE 1 and 2 studies,4,6 While a placebo group is routinely included in phase 3 RCTs for drug approval and registration, it is rarely included in real-world observational studies out of ethical considerations. Despite the absence of a placebo group, placebo effect was quantified based on the SUNRISE 2 study13 and included in the sample size calculation in our study. Fourth, as patients with severe anxiety and/or depression were excluded from our study, the effect of LEM on improving symptoms of anxiety and depression observed in our study should be interpreted with this limitation in mind. The study has the following strength: First, this is a large-scale, multicenter, prospective, observational study that obtained treatment data from a heterogeneous Chinese patient population. Second, both the FAS and PPS were analyzed and they produced consistent results, ensuring the reliability of our results. Third, this study was conducted in designated hospitals in the GBA area, taking advantage of the Hong Kong and Macao Medicine and Equipment Connect policy that allows early access to drugs not yet fully approved by NMPA, and thus was able to collect prospective, real-world data on Chinese patients early in the drug’s lifecycle.
Conclusions
LEM was effective and safe in treating Chinese adult patients with insomnia in real-life clinical practice. It was effective regardless the insomnia treatment regimen, although it appeared that LEM as initial monotherapy was the most effective. In addition, patients with severe insomnia had the greatest improvement, while patients with mild severe had modest improvement. Age did not affect LEM efficacy. Therefore, LEM treatment could provide relief to a wide range of patients with insomnia. As LEM was recently approved as a treatment of insomnia in China, our study could provide timely guidance for clinicians in China who wish to consider LEM as a treatment option for their patients.
Abbreviations
CBT, cognitive behavioral therapy; BZDs, benzodiazepines; GABA-A, gamma-aminobutyric acid type A; CNS, central nervous system; LEM, lemborexant; DORA, dual orexin receptor antagonist; OX1R, orexin receptor type 1, OX2R, orexin receptor type 2; RCTs, randomized controlled trials; qn, per night; GBA, the Greater Bay Area; NMPA, the National Medical Products Administration; ISI, the Insomnia Severity Index; PHQ-9, the Patient Health Questionnaire-9; GAD-7, the General Anxiety Disorder-7, TEAEs, treatment-emergent adverse events; BZRA, benzodiazepine receptor agonist; AEs, adverse events; MedDRA, the Medical Dictionary for Regulatory Activities; CTCAE, the Common Terminology Criteria for Adverse Events; CI, confidence interval; FAS, the full analysis set; PPS, the per-protocol set; SS, the safety set; LOCF, last observation carried forward; SD, standard deviations; IQR, interquartile range; ANOVA, analysis of variance; BMI, body mass index; OR, odd ratio; EEG, electroencephalogram; ORAs, orexin receptor antagonists.
Data Sharing Statement
The datasets generated during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principle of the Declaration of Helsinki. All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the Institutional Review Board of Guangdong Provincial People’s Hospital (approval number: KY2023-1072-02). The privacy rights of human subjects have been observed, and written informed consent to be part of the study was obtained from all participating patients. The study was registered at clinicaltrials.gov (NCT06225947).
Acknowledgments
We acknowledge the contribution of all participants. Ashermed served as the contract research organization (CRO) responsible for monitoring study data.
Author Contributions
Shuqiong Zheng: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. Xueli Li: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. Weiying Jian: Investigation, Methodology, Writing-review and editing. Yamei Tang: Investigation, Methodology, Writing-review and editing. Yongqiang Lin: Investigation, Methodology, Writing-review and editing. Fujun Jia: Conceptualization, Methodology, Investigation, Supervision, Writing-reviewing and editing. Bin Zhang: Conceptualization, Methodology, Investigation, Supervision, Writing-reviewing and editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Eisai China lnc. (Shanghai, China). The funder had no role in the study design, collection, analysis and interpretation of data, writing of the report and decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
The abstract of this paper was presented at the SLEEP 2025 as a poster presentation with interim findings. The poster’s abstract was published in Sleep. 2025;48(Supplement 1):A239–A240. https://doi.org/10.1093/sleep/zsaf090.0549.
In addition, the abstract of the paper was also presented at the 18th Annual Meeting of the World Sleep Congress; September 5-10, 2025; Singapore as a poster presentation with interim findings. The poster’s abstract has not been published yet.
References
1. Yardley J, Kärppä M, Inoue Y, et al. Long-term effectiveness and safety of lemborexant in adults with insomnia disorder: results from a phase 3 randomized clinical trial. Sleep Med. 2021;80:333–20. doi:10.1016/j.sleep.2021.01.048
2. Dash A, Pinner K, Inoue Y, et al. Efficacy and safety of lemborexant over 12 months in Asian adults with insomnia disorder. Sleep Med. 2022;4:100044. doi:10.1016/j.sleepx.2022.100044
3. Kim W-J, Kim H-S. Emerging and upcoming therapies in insomnia. Transl Clin Pharmacol. 2024;32(1):1–17. doi:10.12793/tcp.2024.32.e5
4. Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder: a phase 3 randomized clinical trial. JAMA Network Open. 2019;2(12):e1918254. doi:10.1001/jamanetworkopen.2019.18254
5. Mishima K, Fujimoto K, Endo A, Ishii M. Safety and efficacy of lemborexant in insomnia patients: results of a postmarketing observational study of Dayvigo® Tablets. Drugs R D. 2024;24(2):211–226. doi:10.1007/s40268-024-00462-w
6. Kärppä M, Yardley J, Pinner K, et al. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: results from the phase 3 randomized clinical trial SUNRISE 2. Sleep. 2020;43(9):zsaa123. doi:10.1093/sleep/zsaa123
7. Miyata S, Iwamoto K, Okada I, et al. Assessing the real-world, long-term impact of Lemborexant on sleep quality in a home-based clinical study. Nat Sci Sleep. 2024;16:291–303. doi:10.2147/NSS.S448871
8. Mi W-F, Wen D, Xu L, et al. A phase 3, multicenter, double-blind, randomized, placebo-controlled clinical trial of lemborexant in adults with insomnia disorder. Sleep Med. 2026;139:108722. doi:10.1016/j.sleep.2025.108722
9. Golebiowski R, Mansukhani MP, Kolla BP. Are clinical trials for insomnia recruiting real-world patients? J Clin Sleep Med. 2023;19(8):1553–1555. doi:10.5664/jcsm.10640
10. Jian W, Feng M, Li J. Lemborexant for the treatment of insomnia in patients from China: four case studies. Cureus. 2024;16(7):e64655. doi:10.7759/cureus.64655
11. Jian W, Feng M, Zhao Y, Li J. Efficacy and safety of Lemborexant in treating adult patients with insomnia in China: a single-center, retrospective observational study. Front Neurol. 2025;16:1495965. doi:10.3389/fneur.2025.1495965
12. Food and Drug Administration (FDA). DAYVIGO ® prescribing information; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212028s002lbl.pdf.
13. Roth T, Rosenberg R, Morin CM, et al. Impact of lemborexant treatment on insomnia severity: analyses from a 12-month study of adults with insomnia disorder. Sleep Med. 2022;90:249–257. doi:10.1016/j.sleep.2022.01.024
14. Yang M, Morin CM, Schaefer K, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25(10):2487–2494. doi:10.1185/03007990903167415
15. National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 2017. Available from: https://dctd.cancer.gov/research/ctep-trials/for-sites/adverse-events/ctcae-v5-8x11.pdf.
16. Egbuchulem KI. The basics of sample size estimation: an editor’s view. Ann Ib Postgrad Med. 2023;21(1):5–10.
17. Ozone M, Hirota S, Ariyoshi Y, et al. Efficacy and safety of transitioning to Lemborexant from Z-drug, Suvorexant, and Ramelteon in Japanese insomnia patients: an open-label, multicenter study. Adv Ther. 2024;41(4):1728–1745. doi:10.1007/s12325-024-02811-2
18. Morin CM, Edinger JD, Beaulieu-Bonneau S, et al. Effectiveness of sequential psychological and medication therapies for insomnia disorder: a randomized clinical trial. JAMA Psychiatry. 2020;77(11):1107–1115. doi:10.1001/jamapsychiatry.2020.1767
19. O’Hora KP, Morehouse AB, Freidman L, et al. Comparative effectiveness and predictors of cognitive behavioral therapy for insomnia and its components in older adults: main outcomes of a randomized dismantling trial. J Clin Sleep Med. 2025;21(10):1679–1695. doi:10.5664/jcsm.11756
20. Tanaka-Mizuno S, Fujimoto K, Mishima K, et al. Evaluation of prescribing patterns of switching to and add-on lemborexant in patients treated with hypnotic medication: a nationwide claims database study in Japan. Expert Opin Pharmacother. 2024;25(12):1707–1716. doi:10.1080/14656566.2024.2392018
21. Suzuki H, Hibino H. Characteristics of patients who were able to switch from benzodiazepine hypnotics to lemborexant. SAGE Open Med. 2021;9:20503121211037903. doi:10.1177/20503121211037903
22. Takaesu Y, Sakurai H, Aoki Y, et al. Treatment strategy for insomnia disorder: japanese expert consensus. Front Psychiatry. 2023;14:1168100. doi:10.3389/fpsyt.2023.1168100
23. Chow W, Khullar A, Lalla DF, et al. Practical recommendations for hypnotic switching in insomnia management: a canadian expert clinical framework. Can Prim Care Today. 2025;3(s01):2–12.
24. Tachibana M, Kanahara N, Oda Y, Hasegawa T, Kimura A, Iyo M. A retrospective clinical practice study comparing the usefulness of dual-orexin receptor antagonists and a melatonin receptor agonist in patients switching from long-term benzodiazepine receptor agonists. J Clin Sleep Med. 2024;20(4):603–613. doi:10.5664/jcsm.10946
25. Carpi M, Palagini L, Fernandes M, et al. Clinical usefulness of dual orexin receptor antagonism beyond insomnia: neurological and psychiatric comorbidities. Neuropharmacology. 2024;245:109815. doi:10.1016/j.neuropharm.2023.109815
26. Chen S, Xu Z, Li Y, et al. Clinical efficacy of the Chinese herbal medicine Shumian capsule for insomnia: a randomized, double-blind, placebo-controlled trial. Neuropsychiatr Dis Treat. 2022;18:669–679. doi:10.2147/NDT.S349427
27. Mason EC, Harvey AG. Insomnia before and after treatment for anxiety and depression. J Affect Disord. 2014;168:415–421. doi:10.1016/j.jad.2014.07.020
28. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
29. Chinese Sleep Research Society. Guidelines for the diagnosis and treatment of insomnia disorder (2025 edition). Zhonghua Yi Xue Za Zhi, 2025; 105(34):2960–2981. doi:10.3760/cma.j.cn112137-20250421-00981
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.