Back to Journals » Patient Preference and Adherence » Volume 17
Patient Preferences for Cardiac Rehabilitation – A Systematic Review
Authors Liu Y ![]() , Su M
, Su M ![]() , Lei Y
, Lei Y ![]() , Tian J
, Tian J ![]() , Xue L, Zhang L
, Xue L, Zhang L ![]()
Received 7 October 2022
Accepted for publication 30 November 2022
Published 6 January 2023 Volume 2023:17 Pages 75—88
DOI https://doi.org/10.2147/PPA.S392417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract of "Patient preferences for cardiac rehabilitation" [ID 392417].
Views: 106
Yunyue Liu,1,* Mengyu Su,1,* Yang Lei,1 Jinping Tian,1,2 Leng Xue,1 Lin Zhang1
1School of Nursing, Nanjing Medical University, Nanjing, Jiangsu Province, People’s Republic of China; 2Department of Cardiology, the First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Lei, School of Nursing, Nanjing Medical University, No. 101, Longmian Avenue, Jiangning District, Nanjing, Jiangsu Province, People’s Republic of China, Tel +86 19955062997, Fax +86 258 6869 555, Email [email protected] Jinping Tian, The First Affiliated Hospital with Nanjing Medical University, No. 300, Guangzhou Road, Gulou District, Nanjing, Jiangsu Province, People’s Republic of China, Tel +86 13851550156, Fax +86 519 6809 1881, Email [email protected]
Background: Although a large number of studies have demonstrated the effectiveness of cardiac rehabilitation(CR), patient preferences for CR remain unclear. Knowing patient preferences may contribute to increasing patient participation and adherence, thus improving patient prognosis.
Methods: A systematic search was carried out using electronic databases and manual reference checks from inception until 15th June 2022. Quantitative studies, qualitative studies and mixed methods studies assessing patient preferences for CR were included. Two researchers independently conducted study selectionand data extraction. CR preferences were divided into three categories: CR settings, CR components, and CR contents. A narrative synthesis was applied to integrate the results of the included studies. The Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of included studies.
Results: Ultimately, 17 publications were included in this study. Regarding CR settings, most patients preferred the hospital to home, some considered both, and a few were willing to accept the local CR club as an alternative setting to the hospital. For CR components, regardless of age and gender, patients considered exercise training and nutrition counseling to be the most important and smoking cessation to be the least important. In exercise intervention of CR contents, progress discussion and encouragement were rated as most critical, and non-conflicting with other activities was rated as least critical. In psychological intervention of CR contents, most patients were willing to accept psychological intervention, and a few patients wanted to heal the trauma with the passage of time.
Conclusion: This systematic review provides important insights into patient preferences for CR, clarifying patient preferences for CR settings, components, and contents, along with possible influencing factors. Patient preferences may change due to the COVID-19 epidemic, and there is still a need to focus on patient preferences for CR and conduct more relevant primary research to validate the findings of this paper in the future.
Keywords: cardiac rehabilitation, patient preference, systematic review, COVID-19
Introduction
Cardiovascular disease (CVD) has become the leading cause of mortality and fundamental cause of disability worldwide, not only causing chest pain and shortness of breath, reducing health-related quality of life, but also imposing a substantial financial burden on healthcare systems.1–3 Cardiac rehabilitation (CR), aimed at reducing cardiovascular risk, mortality and readmission rates, improving prognosis and reducing the economic burden, is therefore essential.4 Previously, patients often underwent CR in hospital, however, due to the COVID-19 pandemic, many hospitals have suspended their CR programs in order to curb the spread of the virus.5 Remote CR, benefiting from rapid advances in information and communication technology, can provide adequate guidance and expert advice to CVD population during the COVID-19 outbreak.6 Equipped with remote CR technology, home CR may act as a suitable alternative to hospital CR.7 Compared to hospital CR, home CR overcomes barriers such as long distances to CR facilities, financial costs, and conflicting work schedules.8 In addition, technology-assisted home CR can extend healthcare support to more patients, and patients from rural areas have more access to CR.9
Despite many proven benefits, CR currently suffers from low participation and adherence due to a mismatch between patients and CR programs that does not take into account patient preferences.10,11 In addition, a wide range of CR settings, components, and contents are available for patients. For example, exercise-based CR includes hospital-based CR and home-based CR, with different contents such as various exercise frequency, intensity, time, and form, thus resulting in different risks and benefits.12 However, in practice, CR programs are often dominated by the health care providers, patient preferences are not well understood and need further exploration.13,14 Health care professionals are recommended to take greater account of patient preferences and make greater efforts to involve them in the decision-making process, when they develop individualized CR programs for their patients.15
Inherent in patient preference is the relative desirability of different attributes to patients and the trade-off between pros and cons when faced with multiple choices.16 The inclusion of patient preferences in medical research has become a recognized approach to promoting patient-centered care, and its use has increased significantly.17 Patient preferences can be described in several ways, including quantitative (eg, discrete choice experiments, best-worst scaling, adaptive conjoint analysis) and qualitative research methods (eg, focus groups, semi-structured interviews, in-depth interviews).18 Combining these research methods allows us to gain a more comprehensive understanding of patient preferences for CR. Healthcare professionals who consider patient preferences when designing CR programs can be beneficial in improving patient participation and adherence to CR, thereby improving CR effects and patient prognosis.
Previous studies have provided limited insight into patient preferences, and systematic reviews that integrated patient preferences for CR are currently lacking. Therefore, we conducted a systematic review to systematically summarize the evidence related to patient preferences for CR and its related factors, theoretically bridging the limitations of previous studies.
Methods
The findings of this systematic review are presented in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.19 This systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO [CRD42020184232]).
Search Strategy
The Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Web of Science, Embase, CINAHL, China National Knowledge Infrastructure(CNKI), and WANFANG databases were systematically searched from their inception until 15th June 2022. Search terms incorporated MeSH terms and keywords related to “cardiac rehabilitation” in combination with “patient preference” “patient choice” “stated preference”. A detailed search strategy is displayed in Supplementary Table 1. Open Grey was used to search the grey literature. We also manually searched the reference lists of all eligible articles and relevant reviews for additional studies that were not identified by the search strategy.
Eligibility Criteria
Studies were included if they (1) targeted at patients with CVD requiring CR or healthy people with assumed CR needs; (2) assessed patient preferences for CR; (3) published in English or Chinese. Studies were excluded if they (1) only assessed economic evaluation or willingness to pay for CR, patient satisfaction with CR or adherence to CR; (2) were duplicate studies or contained no original data, such as reviews, editorial, opinion articles, letters, preclinical studies, and conference papers.
Study Selection
All the retrieved records were imported into EndNote (version 20.0) to remove duplicates. Two researchers (LYY and SMY) independently screened study titles and abstracts for eligibility. Full-text articles of potentially relevant abstracts were independently retrieved and assessed for inclusion by two researchers (LYY and SMY). Authors of the respective articles were contacted through email with additional information requests if the information was incomplete. Any disparities in study selection would be resolved by discussion and consulting a third reviewer (XL) to reach a consensus.
Data Extraction and Analysis
Two researchers (LYY and SMY) independently extracted data from each article that met the inclusion criteria, including study characteristics (author, year, country), study objectives, study population (patient source, sample size, age, gender), methods of assessing preferences, study design and patient preferences. To categorize these heterogeneous studies, we referred to the assessment categories for CR recommended by the European Association for Preventive Cardiology which take CR components and CR contents as two separate categories.20 CR components refer to the core components of CR. CR contents refer to what the patients prefer to do for a particular component, and in the case of exercise component, its contents include timing, form, and duration of exercise. We also included CR settings as one of the categories. This has been especially important during social distancing restrictions associated with COVID-19. Patient preferences for CR were eventually grouped into three main categories: CR settings, CR components, and CR contents. Disagreements were resolved through adjudication with a third researcher (XL).
Due to the heterogeneity and mostly observational design of the eligible studies, we did not statistically integrate results in a meta-analysis but conducted an in-depth narrative synthesis to clarify patient preferences for CR.
Quality Assessment
Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of multiple included studies.21 MMAT can evaluate the methodological quality of 5 types of studies: qualitative studies, randomized controlled trials, non-randomized studies, quantitative descriptive studies, and mixed methods studies. The 2018 version has five separate evaluation entries for each type of study, except for mixed studies, which have 15 evaluation entries. A total score is up to 5 points, with 1 point for meeting the standard and 0 points for not. Two investigators (LYY and SMY) conducted the quality evaluation independently, and any disagreements were resolved in consultation with a third investigator (ZL).
Results
Studies Selection
In total, 4384 publications were identified, and 4014 publications remained after removing duplicates. Fifty-three articles were retrieved for further full-text screening, and 17 of these articles met the eligibility criteria. In addition, a manual search of reference lists of eligible publications did not reveal additional publications for inclusion. Ultimately, a total of 17 publications were included in the final review.16,18,22–36 Figure 1 depicts the PRISMA flow chart of literature screening and selection.
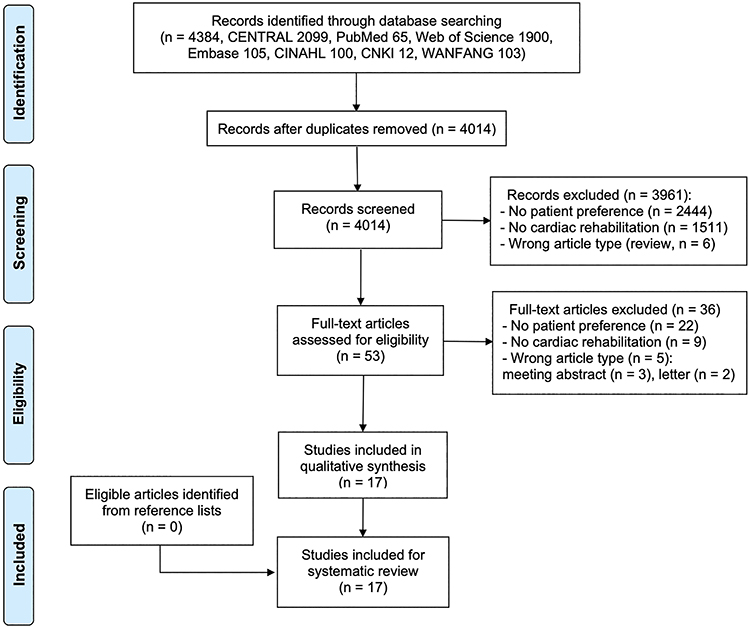 |
Figure 1 The PRISMA flow chart of literature screening and selection process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. Creative Commons. |
Study Characteristics
Seventeen included studies were all published from 1996 to 2021. The sample size ranged from 16 to 512. Most of the studies were published in the UK (n = 5). Seven different assessment methods were used: rating, discrete choice experiment, questionnaire, count analysis, semi-structured interview, in-depth interview, and focus group. The study characteristics are shown in Table 1. Patient preferences for CR were classified into three categories based on the criteria, but due to insufficient original literature, the focus was mainly on exercise and psychological intervention of CR contents. The categories of CR preferences were as follows: (1) CR settings; (2) CR components; and (3) CR contents, including exercise intervention and psychological intervention. Patient preferences for CR are shown in Table 2.
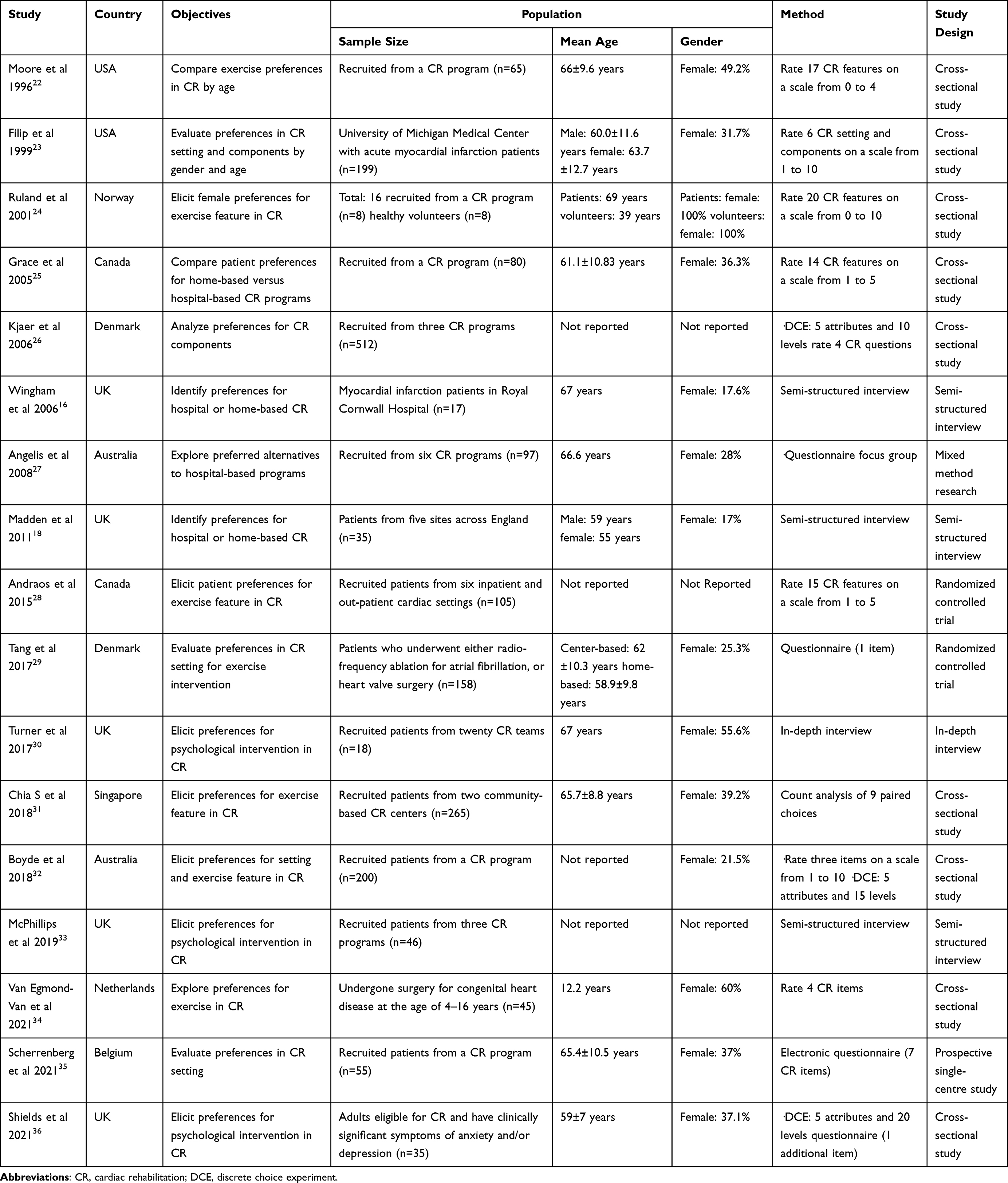 |
Table 1 Study Characteristics for Included Studies |
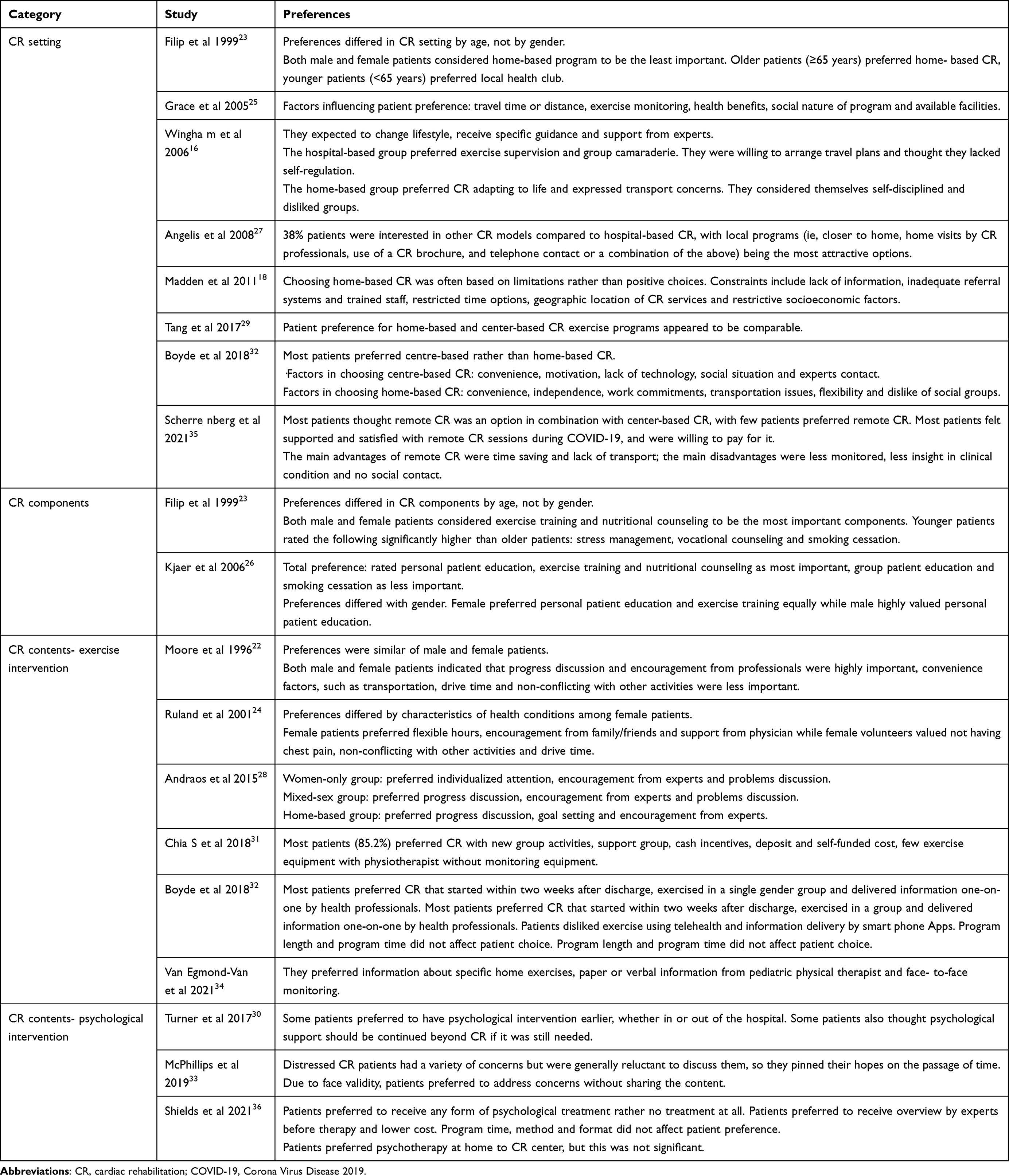 |
Table 2 Patient Preferences for CR in Included Studies |
Quality Assessment
According to the quality evaluation criteria of MMAT, all included studies scored three or higher, with high quality. Quantitative descriptive studies were biased in sampling strategy and statistical analysis methods, randomized controlled trials were biased in randomization, blinding, and participant compliance, qualitative studies were biased in qualitative approaches, and mixed methods studies were biased in inconsistencies. The quality assessment results are shown in Table 3.
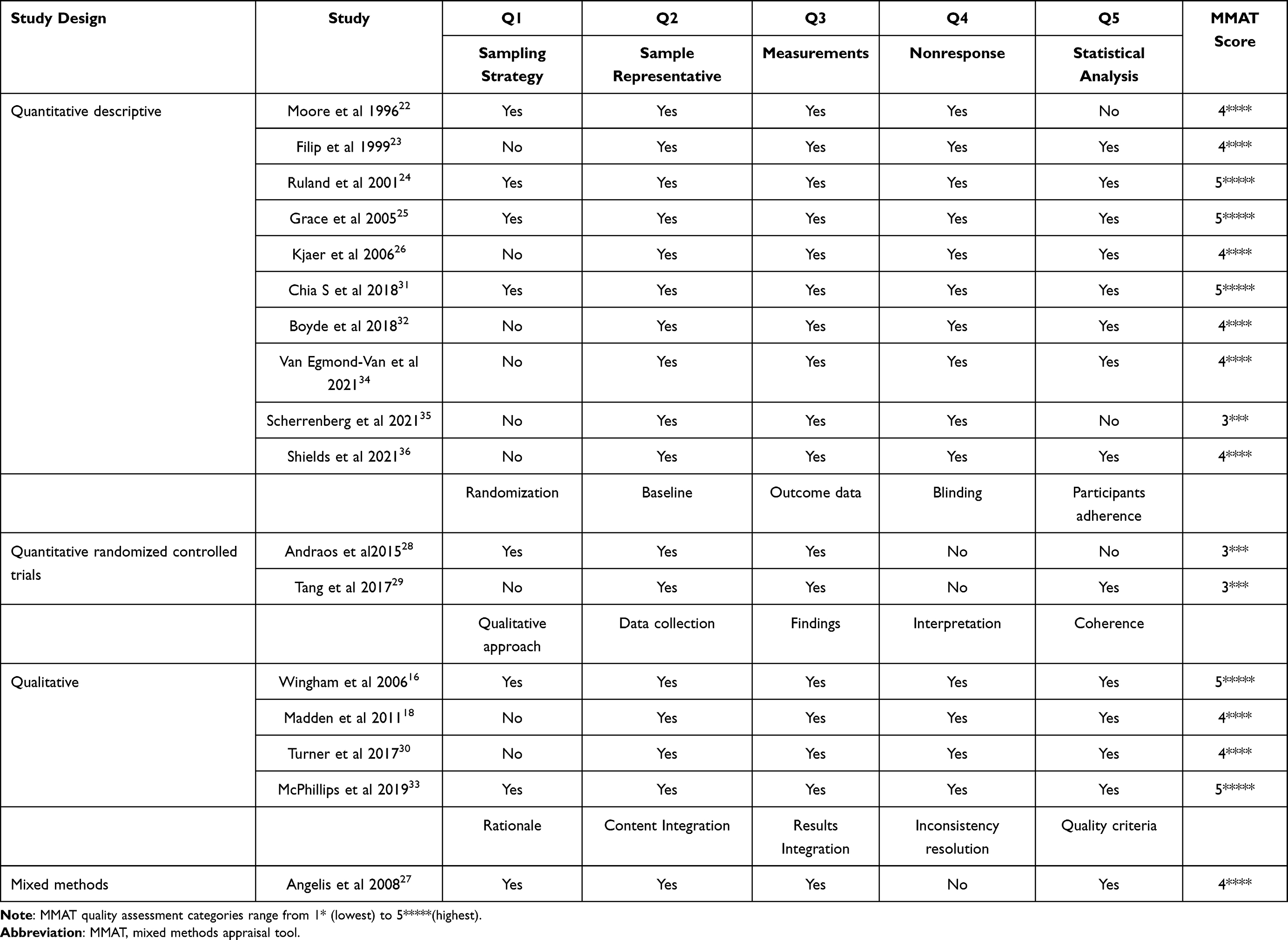 |
Table 3 Quality Assessment Results of Included Studies |
Patient Preference for CR Settings
Eight studies described patient preferences for CR settings, including hospital, home, and local CR clubs. Patient preferences for CR settings varied, with most patients preferring hospital CR over home CR,32,35 some patients considering both,29 and a few patients willing to accept local CR clubs as an alternative to hospital CR.27 People with different demographic characteristics had different preferences for CR settings. Older patients (≥65 years) preferred home CR, and younger patients preferred local CR clubs.23 Factors influencing patient preferences for CR settings were travel time, distance, facilities, and trained staff.18,25 Patients who chose hospital CR were more concerned with peer discussion and exercise supervision, while those who chose home CR were more concerned with independent exercise and flexible scheduling.16,32
Patient Preference for CR Components
Two studies described patient preferences for CR components. Regardless of age and gender, patients considered exercise training and nutrition counseling to be the most important CR components, and smoking cessation to be the least important.23,26 Specifically, patient preferences for CR components were slightly different among patients with different characteristics. Younger patients emphasized stress management, vocational counseling, and smoking cessation more than older patients.23 Female patients valued personal education and exercise training equally, while male patients highly preferred personal education.26
Patient Preference for CR Contents
Six studies described patient preferences for exercise intervention in CR contents. Regardless of gender, patients rated discussing progress and encouragement from experts as highly important, while non-conflicting with other activities as less important.22,28 Female patients focused more on individualized attention compared to male patients.28 Preferences differed by characteristics of health conditions that female patients preferred flexible hours, encouragement from family/friends and physician support while female health volunteers attached importance to no chest pain, non-conflicting with other activities and driving time.24 About the timing of exercise intervention, most patients preferred to start within two weeks after discharge.32 In addition, patients preferred to exercise in a group and receive information from health professionals.31,32,34 They disliked exercise using telehealth and information obtained by smartphone Apps.32 Length and time of exercise intervention did not affect patient choice.32
Three studies described patient preferences for psychological intervention in CR contents. Compared with no psychological therapy, most patients preferred to receive any form of psychological intervention.36 However, some distressed patients were reluctant to discuss their psychological problems, hoping that time would heal the psychological wounds.33 Some patients preferred to have psychological intervention earlier, either in hospital or discharge, even beyond CR, if it was still needed.30 As for the location of psychological intervention, patients preferred to receive psychological treatment at home compared to hospital.36 Due to the protection of personal privacy, some patients preferred to address psychological worries but without describing the distress.33 Specifically, patients preferred to receive a briefing before psychological treatment, and costs were lower. Furthermore, time, method, and format of psychological intervention did not affect patient choice.36
Discussion
This systematic review included 17 papers summarizing patient preferences for CR and categorized by CR settings, components, and contents. This review summarizes patient preference for CR and the related influencing factors.
Previous studies have shown no significant differences between home-based and hospital-based CR in terms of functional capacity, psychological symptoms, quality of life, and all-cause hospitalization.7,9 In addition, a recent systematic review has shown that home CR can be a safe alternative to CR.37 Despite this, most patients prefer hospital-based compared with home-based CR.32,35 Exploring the reasons, patients choose hospital-based CR primarily due to the constraints of time, location, facility, and inadequate healthcare system, rather than the active selection.18,25 Compared with younger patients, older patients preferred home-based CR.23 Home-based CR, which integrates interventions into everyday life, was more effective for older patients, who are hindered by inaccessible locations, limited transportation, and comorbid conditions to attend hospital-based CR.38 Although patients currently prefer hospital-based CR, patient preferences may shift in the future. The recent COVID-19 epidemic has added a severe obstacle to CR programs, and many hospitals may not offer CR to minimize the risk of infection.39 With increasing emphasis on social distancing and caregiving strategies for out-of-hospital patients, it seems a crucial time to revisit the value of home-based CR.40 Less restricted by the epidemic, home-based CR, which is transport-free, less costly, and flexible, allows for uninterrupted care for patients.41 Future research could explore whether patient preferences for CR have shifted following the COVID-19 epidemic, and if so, what the reasons are and whether a new CR program needs to be constructed.
As a crucial component of secondary prevention in CVD, CR is a multidisciplinary program that includes exercise training, nutrition counseling, psychological management, patient education, and risk factor modification.42,43 Regardless of age and gender, patients identified exercise training and nutrition counseling as the most critical, and smoking cessation as the least important.23,26 Studies have shown that exercise plays an irreplaceable role in decreasing cardiovascular risk factors and reducing hospital admissions.44 There is consensus that proper nutrition can reduce CVD and protect the heart.45 The importance of smoking cessation varies, with smokers considering it important while non-smokers consider it unimportant.46 Whether patient preferences differ between males and females, older and younger patients, due to different statistical methods, have not been consistently concluded and need to be explored in more studies. In addition, patient preferences can be taken into account, and patients can be involved in decision-making when developing CR programs in the future. If shared decision-making can benefit patients more, then such CR programs are worth generalization.
Exercise-based CR is recognized internationally as a class 1 clinical practice recommendation for patients with CVD.47 Our study found that patients rated progress discussion and encouragement as most important, and non-conflicting with other activities as least important.22,28 When specialists discuss their conditions and encourage patients, patients are more likely to adhere to the CR program and achieve the desired results.48 Most patients who participate in CR place CR program as their priority, and when CR conflicts with other activities, they tend to prefer CR.49 Female patients tend to have a greater fear of exercise and a greater lack of social support, thus desiring more individualized attention.50 Social stereotypes of men and their higher resilience make them more reluctant to express pain, so they prefer CR with a lower incidence of pain during exercise.51 Study of adults revealed that patients intensely disliked exercise intervention using telehealth.32 Due to the fact that telehealth solves transportation and time constraints and has lower economic costs, an increasing number of patients show an interest in exercise intervention using telehealth.52–54 In addition, patient preference indicated that there is more need for information on exercise intervention than currently available.34 This is consistent with the study of Carolina et al, who believed that specific guideline recommendations are underutilized, the applicability of exercise interventions is inadequate, and still needs to be promoted.55 Future research could be devoted to implementing specific guideline recommendations for exercise-based CR and improving the applicability of exercise intervention.
More than a third of patients with CVD suffer from anxiety or depression, leading to increased adverse cardiovascular events, poorer quality of life, and higher healthcare costs, making effective psychological interventions essential.56 There is evidence that the longer the waiting time before CR, the more severe the anxiety and depressive symptoms may be. In addition, some patients experience anxiety and depressive symptoms after CR, therefore, timely and longer interventions are indispensable.57,58 Notably, patients prefer to receive psychological interventions at home.36 On the one hand, this study was conducted during an epidemic so that patients felt safer at home. On the other hand, patients thought they could better share their feelings with their families at home, making psychological interventions more effective.59 Future attempts could be made to explore the impact of different settings of delivering psychological intervention on patient prognosis.
Some limitations of this systematic review should be noted. First, due to the lack of original literature, only exercise and psychological intervention are summarized in CR contents. Original research on other contents of CR could be conducted in the future to refine patient preferences for CR. Second, due to the heterogeneity of included studies, we could not rank all attributes of patient preference. Third, despite the increasing emphasis on patient decision-making and patient preference, only 3 of the 11 quantitative studies collaborated with patients on attribute selection for the CR program.60 Excluding patients from attribute selection may result in selection bias and, therefore may lead to biased results for patient preference.17 Fourth, only English and Chinese studies were included. The lack of data in some regions and the variability of healthcare systems between the areas limit the generalizability of the results.61,62
Conclusion
This systematic review summarizes patient preferences for CR and its related factors in the hope of increasing CR effects and improving patient prognosis. Despite the rapid development of telehealth, most patients still prefer hospital-based rather than home-based CR. Regarding CR components, exercise training and nutrition counseling are the priorities, while smoking cessation is the least valued. In exercise intervention, progress discussion and encouragement were rated as most important, and non-conflicting with other activities was rated as least critical. As for psychological intervention, most patients were willing to accept psychological intervention, and a few patients wanted to heal the trauma with the passage of time. However, with the emergence of the COVID-19 epidemic and the development of telehealth, patient preferences may change in the future, and more studies still need to be included to validate the findings of this review.
Acknowledgments
This work was granted by Natural Science Foundation of Jiangsu Province of China (No. BK20190658) and Natural Science Foundation of the Higher Education Institutions of Jiangsu Province, China (No.19KJB320017).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American heart association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
2. Jalali-Farahani S, Amiri P, Fakhredin H, et al. Health-related quality of life in men and women who experienced cardiovascular diseases: Tehran lipid and glucose study. Health Qual Life Outcomes. 2021;19(1):225. doi:10.1186/s12955-021-01861-2
3. Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action. J Am Coll Cardiol. 2020;76(25):2980–2981. doi:10.1016/j.jacc.2020.11.021
4. Yuan G, Shi J, Jia Q, et al. Cardiac Rehabilitation: a Bibliometric Review From 2001 to 2020. Front Cardiovasc Med. 2021;8:672913. doi:10.3389/fcvm.2021.672913
5. Antoniou V, Davos CH, Kapreli E, et al. Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-Analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
6. Antoniou V, Xanthopoulos A, Giamouzis G, et al. Efficacy, efficiency and safety of a cardiac telerehabilitation programme using wearable sensors in patients with coronary heart disease: the TELEWEAR-CR study protocol. BMJ Open. 2022;12(6):e059945. doi:10.1136/bmjopen-2021-059945
7. Imran HM, Baig M, Erqou S, et al. Home-based cardiac rehabilitation alone and hybrid with center-based cardiac rehabilitation in heart failure: a systematic review and meta-analysis. J Am Heart Assoc. 2019;8(16):e012779. doi:10.1161/JAHA.119.012779
8. Winnige P, Filakova K, Hnatiak J, et al. Validity and reliability of the Cardiac Rehabilitation Barriers Scale in the Czech Republic (CRBS-CZE): determination of key barriers in East-Central Europe. Int J Environ Res Public Health. 2021;18(24):13113. doi:10.3390/ijerph182413113
9. Nso N, Nassar M, Mbome Y, et al. Comparative assessment of the long-term efficacy of home-based versus center-based cardiac rehabilitation. Cureus. 2022;14(3):e23485. doi:10.7759/cureus.23485
10. Lolley R, Forman DE. Cardiac rehabilitation and survival for ischemic heart disease. Curr Cardiol Rep. 2021;23(12):184. doi:10.1007/s11886-021-01616-x
11. Lee M, Wood T, Chan S, et al. Cardiac rehabilitation program: an exploration of patient experiences and perspectives on program dropout. Worldviews Evid Based Nurs. 2022;19(1):56–63. doi:10.1111/wvn.12554
12. Patti A, Merlo L, Ambrosetti M, et al. Exercise-based cardiac rehabilitation programs in heart failure patients. Heart Fail Clin. 2021;17(2):263–271. doi:10.1016/j.hfc.2021.01.007
13. Ghisi GLM, Grace SL. Validation of the Physician Attitudes toward Cardiac Rehabilitation and Referral (PACRR) scale. Heart Lung Circ. 2019;28(8):
14. Chindhy S, Taub PR, Lavie CJ, et al. Current challenges in cardiac rehabilitation: strategies to overcome social factors and attendance barriers. Expert Rev Cardiovasc Ther. 2020;18(11):777–789. doi:10.1080/14779072.2020.1816464
15. Dalal HM, Doherty P, McDonagh ST, et al. Virtual and in-person cardiac rehabilitation. BMJ. 2021;373:n1270. doi:10.1136/bmj.n1270
16. Jackson Y, Janssen E, Fischer R, et al. The evolving role of patient preference studies in health-care decision-making, from clinical drug development to clinical care management. Expert Rev Pharmacoecon Outcomes Res. 2019;19(4):383–396. doi:10.1080/14737167.2019.1612242
17. Van Overbeeke E, Vanbinst I, Jimenez-Moreno AC, Huys I. Patient centricity in patient preference studies: the patient perspective. Front Med. 2020;7:93. doi:10.3389/fmed.2020.00093
18. Brett Hauber A, Fairchild AO, Reed Johnson F. Quantifying benefit-risk preferences for medical interventions: an overview of a growing empirical literature. Appl Health Econ Health Policy. 2013;11(4):319–329. doi:10.1007/s40258-013-0028-y
19. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
20. Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol;2020. 2047487320913379. doi:10.1177/2047487320913379
21. Hong QN, Pluye P, Fàbregues S, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clin Epidemiol. 2019;111:49–59. doi:10.1016/j.jclinepi.2019.03.008
22. Moore SM, Kramer FM. Women’s and men’s preferences for cardiac rehabilitation program features. J Cardiopulm Rehabil. 1996;16(3):163–168. doi:10.1097/00008483-199605000-00003
23. Filip J, Mcgillen C, Mosca L. Patient preferences for cardiac rehabilitation and desired program elements. J Cardiopulm Rehabil. 1999;19(6):339–343. doi:10.1097/00008483-199911000-00002
24. Ruland CM, Moore SM. Eliciting exercise preferences in cardiac rehabilitation: initial evaluation of a new strategy. Patient Educ Couns. 2001;44(3):283–291. doi:10.1016/S0738-3991(00)00189-0
25. Grace SL, McDonald J, Fishman D, Caruso V. Patient preferences for home-based versus hospital-based cardiac rehabilitation. J Cardiopulm Rehabil. 2005;25(1):24–29. doi:10.1097/00008483-200501000-00006
26. Kjaer T, Gyrd-Hansen D, Willaing I. Investigating patients’ preferences for cardiac rehabilitation in Denmark. Int J Technol Assess Health Care. 2006;22(2):211–218. doi:10.1017/S0266462306051038
27. De Angelis C, Bunker S, Schoo A. Exploring the barriers and enablers to attendance at rural cardiac rehabilitation programs. Austr J Rural Health. 2008;16(3):137–142. doi:10.1111/j.1440-1584.2008.00963.x
28. Andraos C, Arthur HM, Oh P, Chessex C, Brister S, Grace SL. Women’s preferences for cardiac rehabilitation program model: a randomized controlled trial. Eur J Prev Cardiol. 2015;22(12):
29. Tang LH, Kikkenborg Berg S, Christensen J, et al. Patients’ preference for exercise setting and its influence on the health benefits gained from exercise-based cardiac rehabilitation. Int J Cardiol. 2017;232(1):
30. Turner KM, Winder R, Campbell JL, et al. Patients’ and nurses’ views on providing psychological support within cardiac rehabilitation programmes: a qualitative study. BMJ Open. 2017;7(9):e017510. doi:10.1136/bmjopen-2017-017510
31. Chia S, Wong XY, Toon ML, et al. Patient preferences for types of community-based cardiac rehabilitation programme. Heart Asia. 2018;10(1):e010976. doi:10.1136/heartasia-2017-010976
32. Boyde M, Rankin J, Whitty JA, et al. Patient preferences for the delivery of cardiac rehabilitation. Patient Educ Couns. 2018;101(12):2162–2169. doi:10.1016/j.pec.2018.07.010
33. McPhillips R, Salmon P, Wells A, Fisher P. Cardiac rehabilitation patient’s accounts of their emotional distress and psychological needs: a qualitative study. J Am Heart Assoc. 2019;8(11):e011117. doi:10.1161/JAHA.118.011117
34. Van Egmond-van Dam JC, Vliet Vlieland TPM, Kuipers IM, Blom NA, Ten Harkel ADJ. Improvement of physical activity levels in children and adolescents after surgery for congenital heart disease: preferences and use of physical therapy. Disabil Rehabil. 2021;1–8. doi:10.1080/09638288.2021.1924298
35. Scherrenberg M, Falter M, Dendale P. Patient experiences and willingness-to-pay for cardiac telerehabilitation during the first surge of the COVID-19 pandemic: single-centre experience. Acta Cardiol. 2021;76(2):151–157. doi:10.1080/00015385.2020.1846920
36. Shields GE, Wright S, Wells A, Doherty P, Capobianco L, Davies LM. Delivery preferences for psychological intervention in cardiac rehabilitation: a pilot discrete choice experiment. Open Heart. 2021;8(2):e001747. doi:10.1136/openhrt-2021-001747
37. Stefanakis M, Batalik L, Antoniou V, et al. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–126. doi:10.1016/j.hrtlng.2022.04.016
38. Snoek JA, Prescott EI, van der Velde AE, et al. Effectiveness of home-based mobile guided cardiac rehabilitation as alternative strategy for non participation in clinic-based cardiac rehabilitation among elderly patients in Europe: a randomized clinical trial. JAMA Cardiol. 2021;6(4):463–468. doi:10.1001/jamacardio.2020.5218
39. Besnier F, Gayda M, Nigam A, Juneau M, Bherer L. Cardiac rehabilitation during quarantine in COVID-19 pandemic: challenges for center-based programs. Arch Phys Med Rehabil. 2020;101(10):1835–1838. doi:10.1016/j.apmr.2020.06.004
40. Kawada T. Clinical benefits in patients with home-based cardiac rehabilitation in the era of COVID-19 pandemic. Heart Lung. 2022;52:197. doi:10.1016/j.hrtlng.2021.12.004
41. Drwal KR, Forman DE, Wakefield BJ, El Accaoui RN. Cardiac rehabilitation during COVID-19 pandemic: highlighting the value of home-based programs. Telemed J E Health. 2020;26(11):1322–1324. doi:10.1089/tmj.2020.0213
42. Grace SL, Kotseva K, Whooley MA. Cardiac rehabilitation: under-utilized globally. Curr Cardiol Rep. 2021;23(9):118. doi:10.1007/s11886-021-01543-x
43. Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022;19(3):180–194. doi:10.1038/s41569-021-00611-7
44. Nichols S, McGregor G, Breckon J, Ingle L. Current insights into exercise-based cardiac rehabilitation in patients with coronary heart disease and chronic heart failure. Int J Sports Med. 2021;42(1):19–26. doi:10.1055/a-1198-5573
45. Lara-Breitinger K, Lynch M, Kopecky S. Nutrition intervention in cardiac rehabilitation: a review of the literature and strategies for the future. J Cardiopulm Rehabil Prev. 2021;41(6):383–388. doi:10.1097/HCR.0000000000000660
46. Grace SL, Prior PL, Mamataz T, Hartley T, Oh P, Suskin N. Cardiac rehabilitation component attendance and impact of intervening clinical events, as well as disease severity and risk factor burden. J Cardiopulm Rehabil Prev. 2021;41(1):40–45. doi:10.1097/HCR.0000000000000571
47. Taylor JL, Bonikowske AR, Olson TP. Optimizing outcomes in cardiac rehabilitation: the importance of exercise intensity. Front Cardiovasc Med. 2021;8:734278. doi:10.3389/fcvm.2021.734278
48. Rangel-Cubillos DM, Vega-Silva AV, Corzo-Vargas YF, et al. Examining facilitators and barriers to cardiac rehabilitation adherence in a low-resource setting in latin america from multiple perspectives. Int J Environ Res Public Health. 2022;19(4):1911. doi:10.3390/ijerph19041911
49. Sanaie N, Darvishpoor-Kakhki A, Ahmadi F. Patient commitment to cardiac rehabilitation: a qualitative study. Iran J Nurs Midwifery Res. 2021;26(6):479–486. doi:10.4103/ijnmr.IJNMR_200_20
50. Khadanga S, Gaalema DE, Savage P, Ades PA. Underutilization of cardiac rehabilitation in women: barriers and solutions. J Cardiopulm Rehabil Prev. 2021;41(4):207–213. doi:10.1097/HCR.0000000000000629
51. Keogh E, Boerner KE. Exploring the relationship between male norm beliefs, pain-related beliefs and behaviours: an online questionnaire study. Eur J Pain. 2020;24(2):423–434. doi:10.1002/ejp.1499
52. Ramachandran HJ, Jiang Y, Tam WWS, et al. Effectiveness of home-based cardiac telerehabilitation as an alternative to Phase 2 cardiac rehabilitation of coronary heart disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29(7):1017–1043. doi:10.1093/eurjpc/zwab106
53. Su JJ, Yu DS. Effects of a nurse-led eHealth cardiac rehabilitation programme on health outcomes of patients with coronary heart disease: a randomised controlled trial. Int J Nurs Stud. 2021;122:104040. doi:10.1016/j.ijnurstu.2021.104040
54. Marcin T, Bengel C, Goldberg T, Peterhans J, Eser P, Wilhelm M. Patient interest in mHealth as part of cardiac rehabilitation in Switzerland. Swiss Med Wkly. 2021;151:w20510. doi:10.4414/smw.2021.20510
55. Santiago de Araújo Pio C, Chaves GS, Davies P, Taylor RS, Grace SL. Interventions to promote patient utilisation of cardiac rehabilitation. Cochrane Database Syst Rev. 2019;2(2):CD007131. doi:10.1002/14651858.CD007131.pub4
56. Wells A, Reeves D, Capobianco L, et al. Improving the effectiveness of psychological interventions for depression and anxiety in cardiac rehabilitation: pathway-a single-blind, parallel, randomized, controlled trial of group metacognitive therapy. Circulation. 2021;144(1):23–33. doi:10.1161/CIRCULATIONAHA.120.052428
57. Hinde S, Harrison A, Bojke L, et al. Quantifying the impact of delayed delivery of cardiac rehabilitation on patients’ health. Eur J Prev Cardiol. 2020;27(16):1775–1781. doi:10.1177/2047487320912625
58. Sumner J, Böhnke JR, Doherty P. Does service timing matter for psychological outcomes in cardiac rehabilitation? Insights from the National Audit of Cardiac Rehabilitation. Eur J Prev Cardiol. 2018;25(1):19–28. doi:10.1177/2047487317740951
59. Li X, Chen L, Lei B, Xie C. Home-based psychological nursing interventions for improvement of sleep quality and psychological health in patients with hypopharyngeal carcinoma undergoing surgical resections: a randomized trial. Ann Palliat Med. 2021;10(12):12347–12357. doi:10.21037/apm-21-3029
60. Marron JM. Adolescent shared decision-making: where we have been and where we are going. J Adolesc Health. 2021;69(1):6–7. doi:10.1016/j.jadohealth.2021.04.009
61. Daw P, Withers TM, van Zanten JJCSV, et al. A systematic review of provider-and system-level factors influencing the delivery of cardiac rehabilitation for heart failure. BMC Health Serv Res. 2021;21(1):1267. doi:10.1186/s12913-021-07174-w
62. Ebinger JE, Lan R, Driver MP, et al. Disparities in geographic access to cardiac rehabilitation in Los Angeles County. J Am Heart Assoc. 2022;11(18):e026472. doi:10.1161/JAHA.121.026472
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.