Back to Journals » Patient Preference and Adherence » Volume 17
Patient Preferences for Anesthesiologist Attire During Preoperative Visits in China: A Cross-Sectional Survey
Authors Xu X, Lu Z, Liu Z ![]() , Han Y, Zhang Y
, Han Y, Zhang Y ![]() , Shen L
, Shen L ![]()
Received 10 August 2023
Accepted for publication 23 September 2023
Published 2 October 2023 Volume 2023:17 Pages 2421—2431
DOI https://doi.org/10.2147/PPA.S430942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xiaohan Xu,1,* Zhilong Lu,1,* Zijia Liu,1 Yue Han,1 Yuelun Zhang,2 Le Shen1
1Department of Anesthesiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Medical Research Center, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zijia Liu; Le Shen, Department of Anesthesiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, 100730, People’s Republic of China, Tel +86 10 6915 2020, Fax +86 10 6915 5580, Email [email protected]; [email protected]
Background: It is important for anesthesiologists to leave good impressions and build rapport with patients during preoperative visits. However, patient preferences for anesthesiologist attire have not been well studied in China.
Purpose: To characterize patient perceptions of anesthesiologist attire during preoperative visits.
Patients and Methods: In this cross-sectional survey, we included adult patients who underwent elective operations in various surgical departments. We presented photographs of both male and female models wearing six combinations of attire (formal in a white coat buttoned, formal in a white coat unbuttoned, casual in a white coat buttoned, casual in a white coat unbuttoned, scrubs in a white coat buttoned, and scrubs in a coat of the same green color buttoned) in a randomized sequence. Participants were asked to rate each attire combination in five domains, including professionalism, experience, attitude, approachability, and caring.
Results: Of the 541 surveys distributed, 516 (95.4%) were completed and included in the analysis. The majority of respondents were female [389 (75.4%)] and aged 31– 45 years [234 (45.3%)]. The combination of scrubs in a buttoned coat of the same color had the highest composite rating score [median (interquartile range): 50 (45, 50), adjusted P< 0.001 compared with the other five combinations]. There was no significant difference in preference for standardized disposable or personalized cloth operating caps. Respondents’ age was independently associated with the perceived importance of anesthesiologist attire (46– 60 years vs 18– 35 years: odds ratio 2.17, 95% confidence interval 1.12– 4.18, P=0.021).
Conclusion: Patients prefer anesthesiologists wearing scrubs in coats of the same color. Standardizing anesthesiologist attire based on these findings may improve patient satisfaction.
Keywords: dressing, scrubs, color, patient satisfaction, preoperative anesthesia visit
Introduction
The majority of patients prefer physicians to dress professionally, and over 93% of patients believe that physician attire has a significant impact on patient satisfaction.1 Patient satisfaction is associated with various health outcomes, including medication adherence, 30-day readmission, and mortality.
Traditionally, the white coat has been a symbol of cleanliness, professionalism, and academic achievement in medicine.2 Physicians who wear white coats and formal attire are often viewed as more competent and better able to build rapport with their patients.3 However, the white coat can also reinforce hierarchical delineation and create a sense of distance between physicians and patients.4 With the development of enhanced recovery after surgery, perioperative management has become more team-based and patient-centered. In this process, hierarchy is downplayed, and friendliness is emphasized. Patient perception of physician attire may also vary by country. An international survey showed that the most preferred inner wear was scrubs in Italy and Switzerland and formal attire in Japan and the United States.5
Preoperative visits are an important component of perioperative management, during which anesthesiologists come to surgical wards to evaluate patients and obtain informed consent within a limited time. For ease of transition between operating rooms and surgical wards, anesthesiologists typically wear scrubs rather than formal or casual attire during preoperative visits. However, to control the risk of nosocomial infections, our hospital does not allow staff to wear scrubs alone outside of the operating room area and instead offers daily laundered coats of the same color as scrubs as outwear. Despite this policy, some anesthesiologists still prefer to wear white coats over scrubs. In recent years, personalized cloth operating caps have become increasingly popular as an alternative to disposable operating caps, increasing the diversity of anesthesiologists’ attire. This variety of attire can make it difficult for patients to identify anesthesiologists during preoperative visits, sometimes causing confusion with other healthcare providers.
Two previous studies did not show a significant effect of anesthesiologist attire on patient satisfaction during preoperative visits in the United Kingdom.6,7 However, both studies were conducted approximately 30 years ago, and the sample sizes were small. Therefore, we conducted this cross-sectional survey to characterize public preferences and perceptions of anesthesiologists’ attire during preoperative visits and provide evidence to inform policies on dressing standards.
Materials and Methods
Study Design and Participants
Our study team conducted a web-based survey in Chinese through an online survey platform (https://www.wjx.cn). The study protocol was reviewed and approved by the Ethics Committee and Institutional Review Board of Peking Union Medical College Hospital (PUMCH, ethical approval number: SK-1950). Written informed consent was obtained from all individual participants included in the study. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional studies.
We included patients aged 18 years or older who were scheduled for elective surgery in August 2022 in the Departments of General Survey, Gynecology, Orthopedics, Thoracic Surgery, Urology, and Ears-Nose-Throat at PUMCH, a tertiary general teaching hospital in Beijing, China. We attempted to reach all the patients who met the inclusion criteria and thus did not use any sampling techniques. Respondents were informed that they volunteered to participate, and no personally identifiable information would be collected.
Questionnaire Design and Data Collection
The questionnaire was jointly developed by the Dean of Anesthesiology Department, a male and a female attending anesthesiologist, and an attending surgeon at PUMCH. The questionnaire contained four sections (Supplemental File 1). The first section collected demographic factors, including age, sex, education, geographical region, surgery department, and previous experience with preoperative visits.
In the second section, the respondents were shown six photographs of deidentified models wearing various combinations of unbranded healthcare attire, including formal inner wear in a white coat, casual inner wear in a white coat, scrubs in a white coat outwear, and scrubs in a coat of the same green color (Figure 1). The infection management office of PUMCH has adopted stringent dress codes. It was not allowed to wear green coats over personal clothes except scrubs or to wear unbuttoned white or green coats with the scrubs exposed outside the operating room area. However, some doctors might wear white coats unbuttoned with nonscrub clothing inside. Therefore, we added two combinations: formal inner wear and white coat unbuttoned outwear and casual inner wear and white coat unbuttoned outwear. We believed that doctors who unbutton coats would not like to wear masks; thus, the models of both unbuttoned combinations did not wear masks.
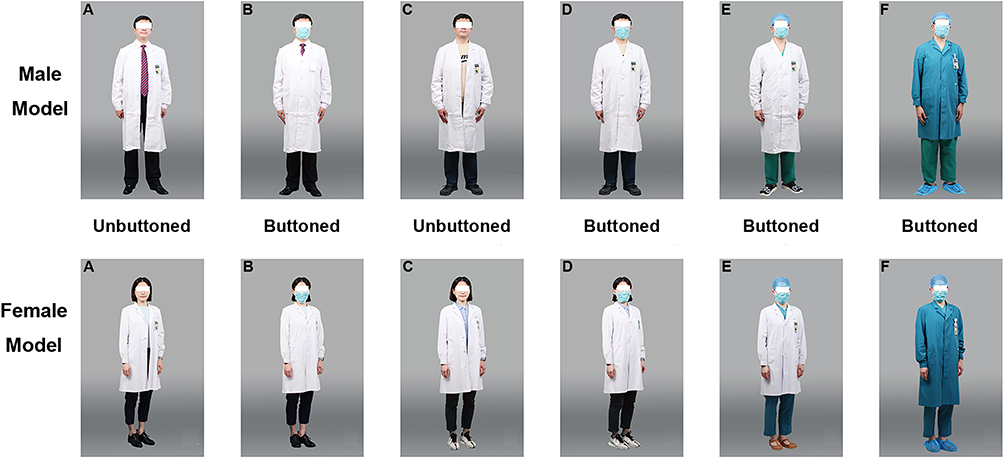 |
Figure 1 Photograph of models presented in the questionnaire: male and female anesthesiologists in various attire combinations. ((A) formal in a white coat unbuttoned, (B) formal in a white coat buttoned, (C) casual in a white coat unbuttoned, (D) casual in a white coat buttoned, (E) scrubs in a white coat buttoned, (F) scrubs in a green coat buttoned). |
To minimize potential bias of gender conformity, each combination of medical attire was presented by the same male and female models. Both models were volunteer members of the research team, and both provided written consent to allow the publication of their photographs. Photographs were taken by the same professional photographer at the same time, ensuring that visual cues (eg, facial expressions, pose, lighting and background) that might influence preference were kept consistent. The six photographs were shown in a randomized sequence automatically generated by the online survey platform to control for anchoring effects. Respondents were asked to rank each of the six randomized attire on a 10-point Likert scale, with 1 indicating the lowest rating and 10 indicating the highest rating in the domains of professionalism, clinical experience, work attitude, approachability, and caring for patients. These five domains were selected according to previous studies on public perception of physician attire.8–10 Respondents were also asked to select their most and least preferred attire and whether anesthesiologists should fasten all the buttons of the white or green coat.
In the third section, respondents were presented with photographs of the same male and female models wearing disposable operating caps and personalized cloth operating caps (Figure 2). Similar to the second section, they were asked to rank each cap on a 10-point Likert scale in the domains of professionalism, clinical experience, and approachability and select their preferred caps.
 |
Figure 2 Photograph of models presented in the questionnaire: male and female anesthesiologists wearing different operation caps. ((A) disposable operating cap, (B) personalized cloth operating cap). |
The final section investigated the perceived importance of anesthesiologist attire. Respondents were asked to rate their level of agreement with the statement that anesthesiologist attire was important to build trust during preoperative visits on a 5-point Likert scale (1 indicated “strongly agree”, 2 “agree”, 3’ neither agree nor disagree’, 4 “disagree” and 5 “strongly disagree”). Since the percentages of respondents who chose 3, 4, and 5 were very low, these three categories were combined, and data were trichotomized into neutral or disagree (3, 4 and 5), agree (2), and strongly agree (1) in the analysis.
The survey was piloted with 20 respondents to ensure that photographs, questions, ratings and the randomly generated sequence functioned as intended. The questionnaire was revised based on the feedback from the pilot survey.
Anesthesiologists routinely visited their patients in wards one day before the day of surgery at PUMCH. To minimize the effects of this visit on patient perception, our research staff visited targeted patients prior to this, explained the purpose and significance of this study to them, obtained their written informed consent, and sent the electronic questionnaires to their smartphones. Respondents could request assistance from the research staff if they had any questions. To ensure data integrity, the questionnaire could not be submitted until all questions were answered, and only one submission per IP address was permitted.
Outcome Measures
The primary outcome was the overall preference of the six attires during preoperative visits, measured by the composite rating scores of all five domains (professionalism, experience, attitude, approachability, and caring). Secondary outcomes included the preference of the operation caps and the factors associated with the perceived importance of anesthesiologist attire.
Statistical Analysis
Statistical analysis was conducted using R (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria, 2022). The distribution of the continuous variables was examined using the Shapiro‒Wilk test. Normally distributed continuous variables, nonnormally distributed continuous variables, and categorial variables are described as the mean ± standard deviation (SD), median [interquartile range (IQR)], and number (percentage), respectively.
The pairwise comparisons of the primary outcome were analyzed using paired Wilcoxon signed rank tests, and Bonferroni correction was used to adjust the significance level at a two-sided α of 0.05 due to multiple comparisons. In the analyses of the secondary outcomes, the preference of the operation caps was analyzed using the Chi-squared test, and the factors associated with the perceived importance of anesthesiologist attire were analyzed using the multivariable ordinal regression model, in which age, gender, education, surgery department, and previous experience of preoperative visit were selected as explanatory variables. No multiple comparison adjustment was conducted in the analyses of secondary outcomes; hence, these findings were regarded as exploratory results.
We used the results of the pilot survey to calculate the sample size. The closest composite rating scores of anesthesiologist attire between combinations were 45.5 ± 9.8 in the scrubs in a white coat combination and 47.5 ± 9.6 in the scrubs in a green coat combination. A sample of 449 respondents would provide 90% power to detect the above difference with a Bonferroni-adjusted 2-sided α of 0.05. Given an assumed completion rate of 85%, the survey would be distributed to at least 528 patients.
Results
Demographics
The survey was distributed to 541 patients who met our inclusion criteria, and 25 (4.6%) patients refused to participate. In total, 516 patients participated in the study and completed the questionnaire, resulting in a completion rate of 95.4%. All complete surveys were included in the final analysis. The majority of respondents were aged 31–45 years [234 (45.3%)] and female [389 (75.4%)], with over half holding a bachelor’s degree or above [377 [73.1%)]. Table 1 provides further details of the respondents’ characteristics.
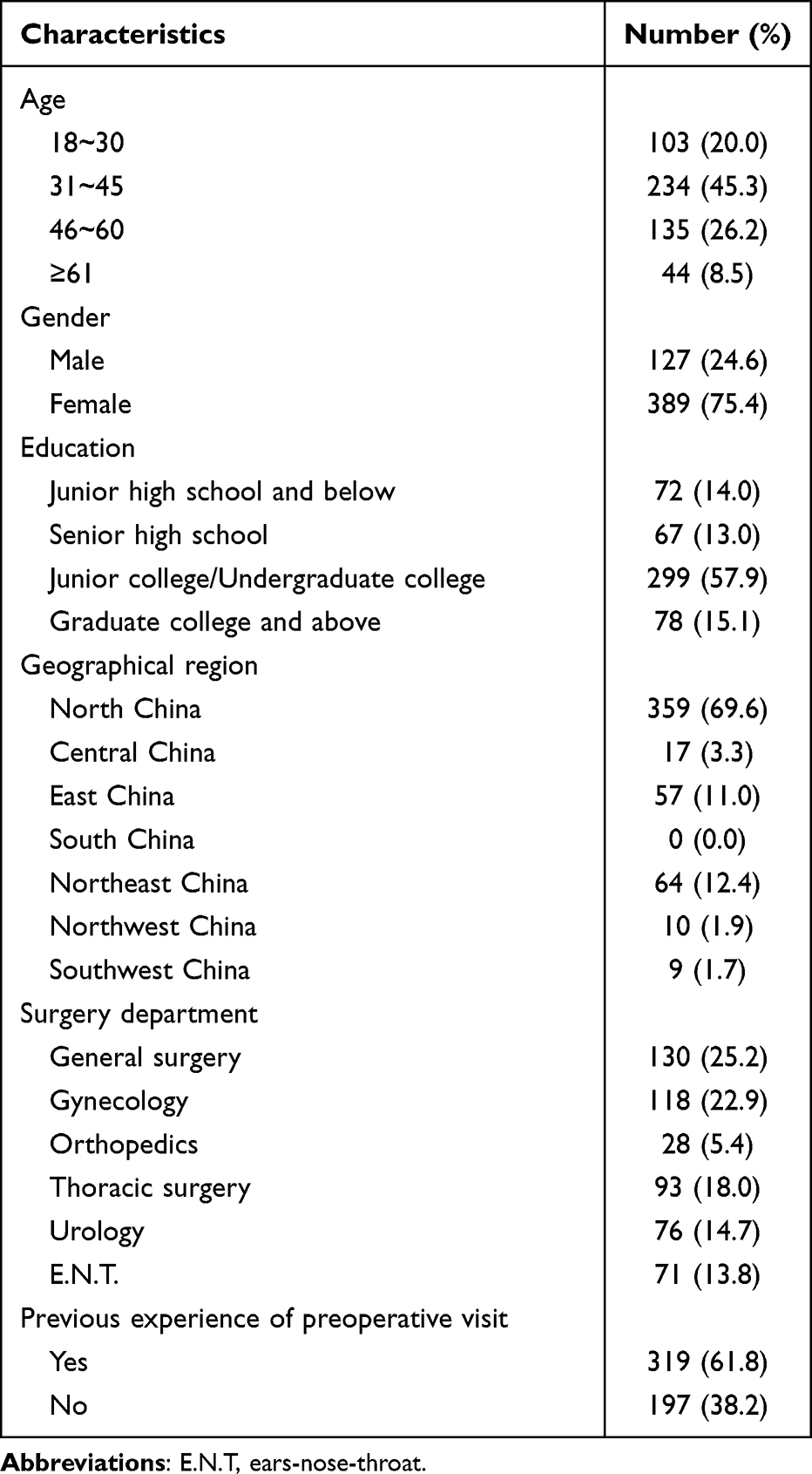 |
Table 1 Respondent Characteristics (N=516) |
Ratings of Anesthesiologist Attire
Figure 3A-E show the box plots of the ratings for the five attire domains. The combination of scrubs in a green coat and scrubs in a white coat buttoned had the two highest median ratings across all five domains. The median (IQR) of the composite rating score was as follows: formal in a white coat unbuttoned 43 (33, 50), formal in a white coat buttoned 45 (38, 50), casual in a white coat unbuttoned 40 (29, 50), casual in a white coat buttoned 45 (35, 50), scrubs in a white coat buttoned 48 (40, 50), and scrubs in a green coat 50 (45, 50) (Figure 3F). The composite ratings were significantly higher for the combination of scrubs in a green coat (adjusted P <0.001 compared to the other five combinations), with scrubs in a white coat buttoned ranked second (adjusted P <0.001 compared to the other five combinations) (Figure 3F).
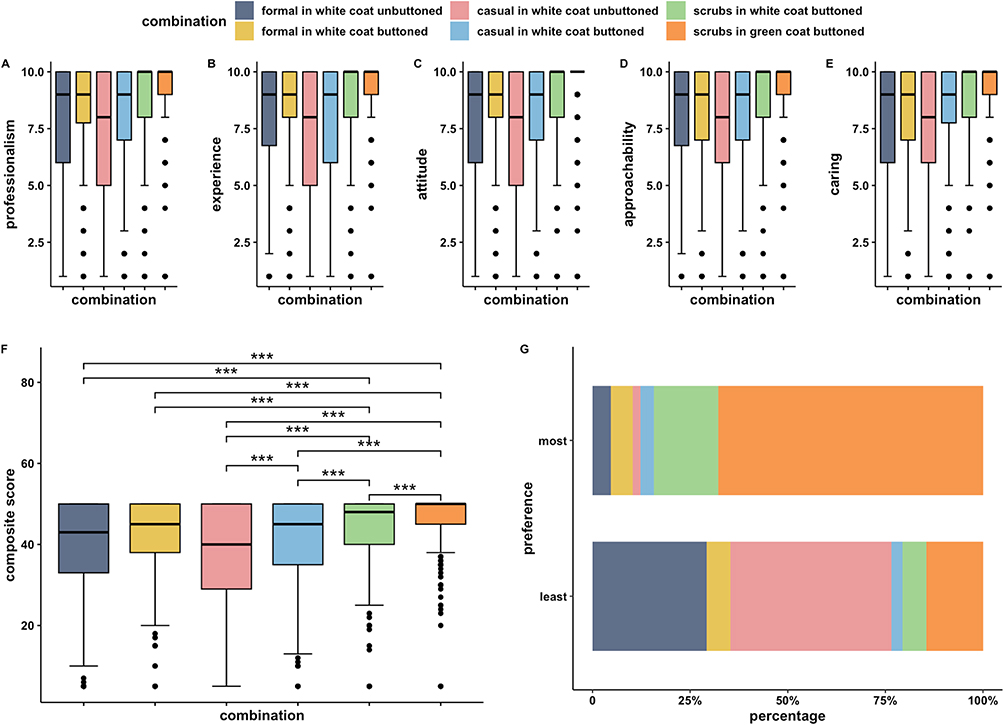 |
Figure 3 Boxplots of the rating scores of attire combinations in the five domains ((A) professionalism, (B) clinical experience, (C) work attitude, (D) approachability, (E) caring for patient) and the composite rating scores (F). (G) Bar plot of the highest and lowest preference. ***Bonferroni-adjusted P <0.001 in the paired Wilcoxon signed rank tests of pairwise comparisons. |
When asked about their preferred attire during preoperative visits, most respondents [350 (67.8%)] chose scrubs inner wear and green coat outwear, consistent with the result of the composite rating score. In comparison, the attire patients least preferred was a combination of casual in white coat unbuttoned [213 (41.3%)] (Figure 3G). The majority of patients (382, 74.0%) reported that anesthesiologists should fasten all buttons, regardless of whether they wore a white coat or green coat during preoperative visits.
Ratings of Anesthesiologist Operating Cap
A greater percentage of respondents believed that disposal operating caps had advantages in demonstrating professionalism (41.3% vs 18.8%) and clinical experience (39.1% vs 19.8%) but not communicating skills (31.6% vs 38.0%) compared to personalized cloth caps (Figure 4). More respondents (217, 42.1%) preferred disposable caps than personalized caps (168, 32.6%), while 131 (25.4%) reported no difference in preference (Figure 4). The chi-squared test did not show any significant differences in the preference of the operation caps (P>0.999).
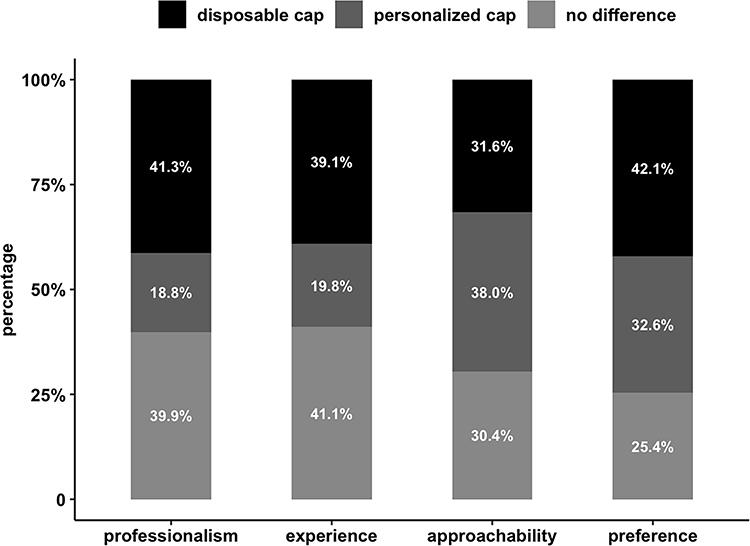 |
Figure 4 Bar plots of the preference of operating caps in the domains of professionalism, clinical experience, and approachability and overall preference. |
Perceived Importance of Anesthesiologist Attire
The majority of respondents [405 (78.4%)] strongly agreed that the anesthesiologist’s attire was important to build trust during the preoperative visit, 77 (14.9%) agreed, 31 (6.0%) neither agreed nor disagreed, 1 (0.2%) disagreed, and 2 (0.4%) strongly disagreed. Table 2 provides the associations between respondents’ characteristics and their perceived importance of the anesthesiologist’s attire. In the multivariable ordinal regression model, the respondents aged 46–60 years perceived greater importance of the anesthesiologist attire compared to those aged 18–30 years [odds ratio (OR) 2.17, 95% confidence interval (CI) 1.12–4.18, P=0.021] (Table 2). However, respondents aged 31–45 years and >60 years showed no significant differences. Notably, the type III P value of age was 0.122 in this model; hence, the overall association between age and perceived importance should be interpreted with caution. We found no significant association between the perceived importance of the anesthesiologist attire and gender, education, surgery department, or previous experience of preoperative visits (Table 2).
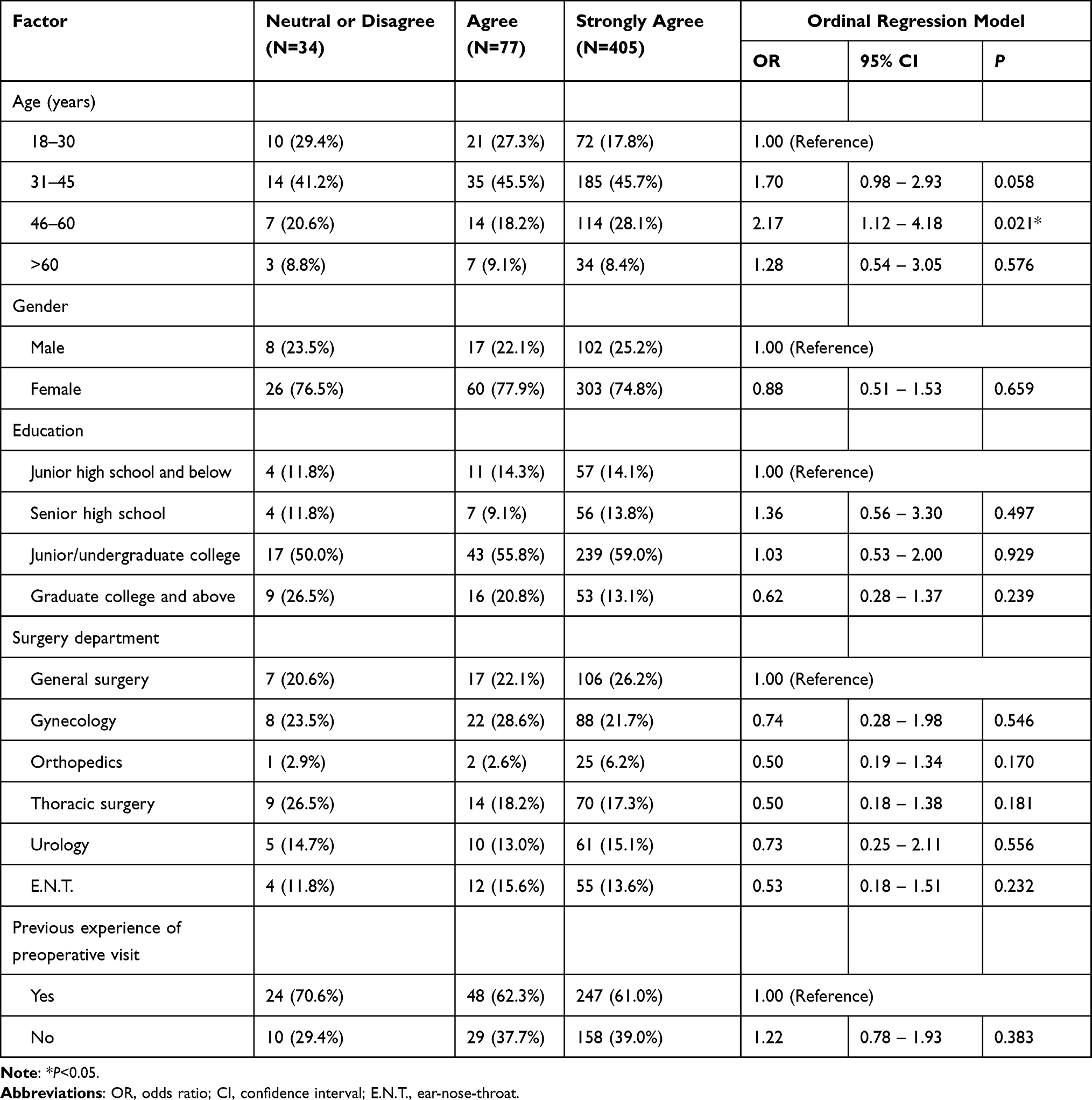 |
Table 2 Factors Associated with the Perceived Importance of Anesthesiologists’ Attire During Preoperative Visits (N=516) |
Discussion
To our knowledge, this is the first study to characterize patient preferences for anesthesiologist attire during preoperative visits. Our findings suggest that the combination of scrubs in a coat of the same color was the most preferred attire, with advantages in conveying a sense of professionalism, clinical experience, work attitude, approachability, and caring for patients.
Scrubs were the most preferred inner wear for anesthesiologists among our respondents. Similarly, scrubs were preferred over formal attire for surgeons according to two nationwide surveys in the United States and an international survey, whereas there was a strong disinclination toward wearing scrubs for family physicians.5,8,9 This was possibly because patients could have known from public media that scrubs are the standard dress in operating rooms and thus might expect anesthesiologists and surgeons to wear scrubs.11 Scrubs were also the most preferred inner wear in outpatient clinics in Switzerland and China but not Japan, indicating that the perception of attire varied across different sociocultural contexts.10,12,13
Interestingly, our respondents preferred coats of the same green color as scrubs for anesthesiologists, which differed from previous studies that showed that white coats were the most preferred outwears for physicians of other specialties.5,8,14,15 One possible explanation could be that the majority of our anesthesiologists and surgeons wore green coats over scrubs in surgical wards, making our patients accustomed to this combination. The same green color of scrubs and outwear could also create a sense of harmony and relaxation. Additionally, concerns about the transmission of nosocomial pathogens have raised questions about the hygiene of white coats, particularly during the COVID-19 pandemic.16–18 Green coats were laundered more frequently than white coats in our hospital and were thus perceived as more hygienic. Sometimes physicians would like to leave outwears unbuttoned for the ease of putting on and off.8 However, we found that patients disliked unbuttoned coats, particularly when physicians wear causal inner wears, possibly because unbuttoned clothes were regarded as being informal in Chinese culture. As stated before, scrubs alone were not allowed to wear outside the operating room area in our hospital and thus were not included as a response option in this survey. However, it is worth noting that situations are different in the other countries. For example, long-sleeve clothing is not recommended by the Department of Health of the United Kingdom due to the risk of contamination of cuffs.19 After the implementation of this policy, the number of physicians wearing white coats considerably decreased, and scrubs without outwears became the most common attire, but this did not undermine the doctor‒patient relationship.20 In fact, patients even preferred scrubs alone over scrubs in white coats for surgeons.5,9
Our study also assessed patients’ perception of operating caps and did not observe significant inclinations. Our hospitals provided disposable operating caps, whereas many anesthesiologists preferred personalized cloth caps, as they were deemed more comfortable, recognizable, and capable of containing long hair. A previous study showed that cloth skull caps were more effective than disposable bouffants and comparable to disposable skull caps in preventing airborne contamination.21 Our results and these findings suggested that wearing personalized cloth caps might not affect either patient satisfaction or the risk of contamination.
More than 90% of our respondents strongly agreed or agreed on the importance of anesthesiologist attire in building trust, which was consistent with previous studies focused on physicians in other specialties.22 Unlike the other specialties, anesthesiologists do not have many opportunities to communicate with their patients. Thus, it is more important for them to dress appropriately and leave good impressions within the limited time of preoperative visit.23 Our data implied that respondents’ age was independently associated with the perceived importance of anesthesiologists’ attire. We only found significant differences between respondents aged 18–30 years and 46–60 years. However, previous studies demonstrated that patients older than 65 years might have different opinions on physicians’ attire.5,8–10 The small sample size of our respondents older than 65 years could explain why we failed to detect differences in this population.
Our study had the following limitations. First, our survey was designed based on the healthcare system and sociocultural norms in China; hence, the results might be different in other clinical contexts. Second, the majority of our responders were females, possibly because 22.9% of our responders were from the Department of Gynecology and we did not use sampling techniques. Furthermore, we did not include cardiovascular, plastic, outpatient, or emergency surgeries, which might limit our generalizability. Third, the validity and reliability of our questionnaire had not been confirmed before. The structured questions and the use of Likert scales might also limit our ability to capture subtle variations in preference or reasons behind them. Fourth, models of the two unbuttoned combinations did not wear masks, while the other models did. This might lead to confounding effects since wearing a mask can affect patient preference. Finally, our cross-sectional study design did not allow us to make causal inferences, so the association between patients’ age and perceived importance of attires should be further determined in the future.
Conclusion
Our findings suggested that anesthesiologists wearing scrubs in coats of the same color leave the best impression on surgical patients during preoperative visits. There was no significant difference in preference for standardized disposable or personalized cloth operating caps. Respondents’ age was independently associated with the perceived importance of anesthesiologist attire. These findings may provide evidence for making policies on the dress codes of anesthesiologists during preoperative visits, which may improve patient satisfaction.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the Ethics Committee and Institutional Review Board of Peking Union Medical College Hospital (ethical approval number: SK-1950). Written informed consent was obtained from all individual participants included in the study.
Consent for Publication
Written informed consent was obtained from the male and female models involved in this study.
Acknowledgments
The authors would like to thank Doctor Shuang Ma and Doctor Lu Che from the Department of Anesthesiology of Peking Union Medical College Hospital for their great support of the study and agreement of appearances as models in the questionnaire. We would also like to thank the following contributors who helped with data collection: Doctor Li Xiang, Zhang Yu of the Department of Anesthesiology of Peking Union Medical College Hospital, and Dr. Ning Fenghua of the Department of Anesthesiology of Cangzhou Hospital of Integrated Traditional Chinese and Western Medicine of Hebei Province.
Funding
This work was supported by National High Level Hospital Clinical Research Funding [2022-PUMCH-B-007]. This funding did not involve any of the stages from study design to submission of the paper for publication.
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Chung H, Lee H, Chang DS, et al. Doctor’s attire influences perceived empathy in the patient-doctor relationship. Patient Educ Couns. 2012;89(3):387–391. doi:10.1016/j.pec.2012.02.017
2. Hochberg MS. The Doctor’s White Coat--an Historical Perspective. The Virtual Mentor. 2007;9(4):310–314. doi:10.1001/virtualmentor.2007.9.4.mhst1-0704
3. Petrilli CM, Mack M, Petrilli JJ, Hickner A, Saint S, Chopra V. Understanding the role of physician attire on patient perceptions: a systematic review of the literature--targeting attire to improve likelihood of rapport (TAILOR) investigators. BMJ open. 2015;5(1):e006578. doi:10.1136/bmjopen-2014-006578
4. Banu A, Anand M, Nagi N. White coats as a vehicle for bacterial dissemination. J Clin Diagn Res. 2012;6(8):1381–1384. doi:10.7860/JCDR/2012/4286.2364
5. Houchens N, Saint S, Petrilli C, et al. International patient preferences for physician attire: results from cross-sectional studies in four countries across three continents. BMJ Open. 2022;12(10):e061092. doi:10.1136/bmjopen-2022-061092
6. Hennessy N, Harrison DA, Aitkenhead AR. The effect of the anaesthetist’s attire on patient attitudes. The influence of dress on patient perception of the anaesthetist’s prestige. Anaesthesia. 1993;48(3):219–222. doi:10.1111/j.1365-2044.1993.tb06905.x
7. Sanders LD, Gildersleve CD, Rees LT, White M. The impact of the appearance of the anaesthetist on the patient’s perception of the pre-operative visit. Anaesthesia. 1991;46(12):1056–1058. doi:10.1111/j.1365-2044.1991.tb09923.x
8. Xun H, Chen J, Sun AH, Jenny HE, Liang F, Steinberg JP. Public Perceptions of Physician Attire and Professionalism in the US. JAMA Netw Open. 2021;4(7):e2117779. doi:10.1001/jamanetworkopen.2021.17779
9. Petrilli CM, Saint S, Jennings JJ, et al. Understanding patient preference for physician attire: a cross-sectional observational study of 10 academic medical centres in the USA. BMJ Open. 2018;8(5):e021239. doi:10.1136/bmjopen-2017-021239
10. Zollinger M, Houchens N, Chopra V, et al. Understanding patient preference for physician attire in ambulatory clinics: a cross-sectional observational study. BMJ Open. 2019;9(5):e026009. doi:10.1136/bmjopen-2018-026009
11. Chung JE. Medical Dramas and Viewer Perception of Health: testing Cultivation Effects. Hum Commun Res. 2014;40(3):333–349. doi:10.1111/hcre.12026
12. Zou Y, Wang Y, Song Y, et al. Patients’ Preference for Physician Attire in the Internal Medicine Outpatient Department. Biomed Res Int. 2023;2023:2992888. doi:10.1155/2023/2992888
13. Yamada Y, Takahashi O, Ohde S, Deshpande GA, Fukui T. Patients’ preferences for doctors’ attire in Japan. Intern Med. 2010;49(15):1521–1526. doi:10.2169/internalmedicine.49.3572
14. Jennings JD, Pinninti A, Kakalecik J, Ramsey FV, Haydel C. Orthopaedic Physician Attire Influences Patient Perceptions in an Urban Inpatient Setting. Clin Orthop Relat Res. 2019;477(9):2048–2058. doi:10.1097/CORR.0000000000000822
15. Jennings JD, Ciaravino SG, Ramsey FV, Haydel C. Physicians’ Attire Influences Patients’ Perceptions in the Urban Outpatient Orthopaedic Surgery Setting. Clin Orthop Relat Res. 2016;474(9):1908–1918. doi:10.1007/s11999-016-4855-7
16. Goyal S, Khot SC, Ramachandran V, Shah KP, Musher DM. Bacterial contamination of medical providers’ white coats and surgical scrubs: a systematic review. Am J Infect Control. 2019;47(8):994–1001. doi:10.1016/j.ajic.2019.01.012
17. Nordrum OL, Aylward P, Callaghan M. Hospital doctors’ attire during COVID-19 and beyond: time for a permanent change. Ir J Med Sci. 2022;191(6):2445–2447. doi:10.1007/s11845-022-02922-1
18. Kuehn BM. Time to hang up the white coat? Epidemiologists suggest ways to prevent clothing from spreading infection. JAMA. 2014;311(8):786–787. doi:10.1001/jama.2014.794
19. Department of Health. Uniforms and workwear: guidance for NHS employers. Available from: https://www.england.nhs.uk/wp-content/uploads/2020/04/Uniforms-and-Workwear-Guidance-2-April-2020.pdf.
20. Shelton CL, Raistrick C, Warburton K, Siddiqui KH. Can changes in clinical attire reduce likelihood of cross-infection without jeopardising the doctor-patient relationship? J Hosp Infect. 2010;74(1):22–29. doi:10.1016/j.jhin.2009.07.031
21. Markel TA, Gormley T, Greeley D, et al. Hats Off: a Study of Different Operating Room Headgear Assessed by Environmental Quality Indicators. J Am Coll Surg. 2017;225(5):573–581. doi:10.1016/j.jamcollsurg.2017.08.014
22. Roehrens HJ, Ehlers JP, Zupanic M. Clothes Make the Man-What Impact Does the Dress of Interprofessional Teams Have on Patients? Healthcare. 2022;10(10):2109. doi:10.3390/healthcare10102109
23. Salgaonkar SV, Kulkarni AD, Chapane SP. Assessment of communication skill during process of preoperative visit and informed consent by anesthesiology residents. J Anaesthesiol Clin Pharmacol. 2021;37(4):548–553. doi:10.4103/joacp.JOACP_414_19
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.