")
Back to Journals » Patient Preference and Adherence » Volume 16
Patient Preference for Biologic Treatments of Psoriasis in the Chinese Setting
Authors Lang Y , Wu B, Sun Z, Ye E, Dou G, Guan X
Received 28 January 2022
Accepted for publication 9 April 2022
Published 21 April 2022 Volume 2022:16 Pages 1071—1084
DOI https://doi.org/10.2147/PPA.S357795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Yitian Lang,1 Bin Wu,2 Zhilin Sun,3 Erjia Ye,4 Guanshen Dou,4 Xin Guan3
1Department of Pharmacy, Huangpu Branch, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200011, People’s Republic of China; 2Medical Decision and Economic Group, Department of Pharmacy, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 201100, People’s Republic of China; 3Department of Dermatology, Peking University Third Hospital, Peking University, Haidian District, Beijing, People’s Republic of China; 4Lilly China Drug Development and Medical Affairs Center, Eli Lilly and Company, Shanghai, People’s Republic of China
Correspondence: Xin Guan, Department of Dermatology, Peking University Third Hospital, Peking University, No. 49, Huayuan North Road, Haidian District, Beijing, People’s Republic of China, Email [email protected]
Objective: Assessments of patients’ preferences can support in clinical decision-making regarding biologic therapies for psoriasis. Our objective was to investigate patient preference for biologic treatments in patients with psoriasis in China.
Methods: From October 2020 to January 2021, psoriasis patients were recruited for a survey that included demographic and disease-related questions, as well as a discrete choice experiment to measure their preferences for biologic therapy. A discrete-choice experiment was used in which respondents selected psoriasis treatments based on benefits (ie, early onset of efficacy, long-term efficacy, sustained efficacy) and treatment costs. We analyzed choice data using conditional logit model.
Results: This study included 236 patients with moderate-to-severe psoriasis. The relative importance of the cost of biologic treatments, probability of keeping PASI100 at 5 years, probability of achieving PASI100 at 3 months and time to achieve PASI50 after initiation the biologic treatment were 0.593, 0.137, 0.185 and 0.085. Over 50% of patients regarded the cost of biologic treatments as the most important attribute. High-income and low-income subgroups had higher preference weight in probability of achieving PASI100 at 3-month and monthly cost.
Conclusion: The cost of biologic treatments was found as the most important attribute for Chinese patients with psoriasis. Among efficacy attributes, the probability of achieving PASI100 at 3 months showed most sensitive. These results may be helpful to understand patient preference for biologic treatments used for psoriasis in China.
Keywords: biologics, discrete choice experiment, Chinese setting, patient preference, psoriasis
Introduction
Psoriasis is an inflammatory skin disease triggered by the immune system. Only a few studies have been conducted on the incidence and prevalence of psoriasis worldwide. According to a systematic review, the prevalence in adults ranged from 0.91% (the United States) to 8.5% (Norway). In adults, it varied from 78.9/100,000 person-years (the United States) to 230/100,000 person-years (Italy).1 The disease burden of psoriasis should not be underestimated. The global report on psoriasis by WHO (World Health Organization) showed that global average DALY (disability-adjusted life year) for psoriasis was estimated at 1,050,660 in 2010, which is twice as much as for acute hepatitis C.2 The continued development of effective therapies for patients with psoriasis is urgently needed. It has long been recognized that patient preferences support the principle of patient-centeredness in clinical decisions.3 During past decades, a growing number of patient preferences are now being measured using elicitation methods that quantify them in the clinical setting, such as standard gamble, time trade-off, person trade-off and discrete choice experiment (DCE).4 Several methods have more recently also been used for psoriasis treatment.5–7 In recent years, the study of quantifying psoriasis patients’ treatment preferences is expanding to include regulatory marketing authorization decisions of new biologic treatments.8–10 To adjust decision-making for patient opinion on the meaning and significance of treatment attributes, such as the balance between estimated effects and adverse reactions, quantitative assessments of patient preferences may be helpful in regulatory marketing approvals.11,12 Adherence to a treatment program could be improved by better tailoring it to patient preferences.12
Patients with psoriasis are often treated with multiple disease-modifying anti-psoriasis drugs. Each of these drugs has its own characteristic and method of action, as well as a different frequency of administration and chance for adverse events and monitoring requirements. Patients with mild disease (PASI ≤10) and mild or moderate quality-of-life impairment (DLQI ≤10) may only need topical therapy.13 Patients with severe or moderate psoriasis (PASI >10) or significant quality-of-life restrictions (DLQI >10) has several options for treatment. These include phototherapies, conventional systemic immunosuppressive medications, or modern small molecules or biologic agents. Individual risk factors, associated diseases, national guidelines, and approval criteria (which might consider economic aspects) can impact the choice of treatment.13 Clinicians should therefore inform patients of the extent of and probability of experiencing side effects associated with these treatments. Although treatment costs can be an important determinant of preference, they are less relevant in countries with universal health-care systems, as is the case for most of developing regions. Despite the fact that treatment costs can be a determinant of preference, in regions with universal health-care systems, as is the case for the majority of developing regions, treatment costs are less relevant in determining preference.
As professionals, clinicians should get to know our patients’ perspectives and preferences when discussing potential treatments. This will allow patients to participate in decisions about their treatment, aligning with their preferences.12 Quantitative assessments of patient preferences have the potential to support both clinicians and regulators when they consider patient perspectives. In considering patient perspectives, both clinicians and regulators can benefit from quantitative assessments. Presently, numerous studies have investigated preference associated with psoriasis. A systematic review summarized 23 studies identified 4 areas of preferences related to psoriasis, which covered preferences for treatment options (eg, state preferences with regard to two different ointments or a cream vs an ointment), preferences for attributes of treatment (eg, frequency of drug administration, treatment benefits or avoidance of potential adverse effects), preferences for different health states (eg, health state utility), preferences for different health state domains (eg, interquartile range).4 For treatment attributes, efficacy (eg, duration of benefit, coverage, lesion severity, etc.) and safety (eg, risk of infection, unspecified adverse events, etc.) were selected in most studies.14 Additionally, the global report on psoriasis pointed out that onset speed (get better skin quickly) and complete removal of skin lesions (recover from all skin lesions) are the top two importance of patient needs related to treatment of psoriasis, which accounted for more than 90%.2 However, few studies have evaluated the onset speed, complete removal of skin lesions, and cost-related indicators. Lack of evidence concerning the extent to which patients feel that biologic treatments would be cost-effective and acceptable in a middle-income country, especially in the context of China. The present study examines the preferences of psoriasis patients in China with moderate-to-severe psoriasis regarding biologic therapies and the heterogeneity within these perceptions. It is based on these preferences that one can estimate the relative importance of different treatment characteristics, as well as calculate patients’ willingness to pay (WTP) for biologic treatments in China with primarily out-of-pocket payment markets.
Materials and Methods
Recruitment
A study invitation was sent to the members of the Chinese online psoriasis community via email, social media and mobile application. During the study, each participant was informed about the research procedure and provided their informed consent before completing the survey. The survey was distributed online by a consulting and marketing research company (Adelphi FocusRx). For inclusion, there were the following criteria: established moderate-to-severe diagnosis psoriasis (BSA ≥3%, PASI ≥3, DLQI ≥6, based on the guideline for psoriasis in China), over 18 years of age, the experience of receiving biologic treatments, and the ability to properly understand and answer the raised questions. The sample size for the DCE was calculated using the Johnson and Orme methodology that the sample size required for the main effects depends on the number of choice tasks (t), the number of alternatives (a), and the number of analysis cells (c) according to the following equation: N > 500c/(t × a).15 Data were collected from October 2020 to January 2021.
Methodology of Discrete Choice Experiment
A DCE method was used to determine treatment preferences for patients with moderate-to-severe psoriasis, which is a cross-sectional survey method used for quantitative assessment of patient preferences for health-care policies, services, and interventions.16,17 Based on the random utility theory (RUT), DCE quantifies the relative importance of one treatment characteristic versus another. In RUT-based approach, the utility (U) of alternative j for individual i in the choice set k was specified as: Uijk=Xijkβ+εijk, where Uijk is the utility function of individual i from choosing alternative j in choice set k. Xijkβ represents a linear specification of the DCE attributes. It is assumed that the utility of a product can be determined by the value of the characteristics of that product (ie, attributes) and their levels. In a DCE, respondents are given a choice of hypothetical scenarios with different attributes and levels. Respondents are asked to choose their preferred option for each question and select the option that yields the maximum utility. By modeling the choices respondents make between alternative treatments described by different choice questions, the utility of each treatment can be estimated. Also, DCEs can be used to measure and explain the heterogeneity among the preferences of patients. When out-of-pocket costs are taken into account in a DCE, the results can be used to calculate the value of or WTP for improvements in medication attributes.18,19
Attributes and Levels
To determine attributes and levels to include in the DCE, we followed a stepwise process. The first step was to review previous literature on patient preferences for treatment in psoriasis and to identify 13 potential treatment characteristics.8,10,20 The second step was to consult 5 dermatologists to make sure the attributes and levels described reflected current clinical practice in China.21 Thirdly, a nominal group technique was used for two focus groups with patients with moderate-to-severe psoriasis (n = 11) and these patients were asked to identify new attributes and rank all potential attributes from the most to the least important. The focus groups were audio recorded and conducted using an interview guide, which lasted approximately 60 minutes. Furthermore, five dermatologists, the research team, and eleven patient research partners reviewed and discussed the results from the focus groups during several validation meetings. These meetings revealed four attributes: the average time for achieving 50% reduction after initiation of treatment, proportion of achieving 100% reduction after 3-months treatment, proportion of maintaining 100% reduction after 5-years treatment and monthly average cost on medication. Each attribute was revealed to have four levels based on current clinical knowledge of existing therapies. All attributes and levels included in the DCE are displayed in Table 1.
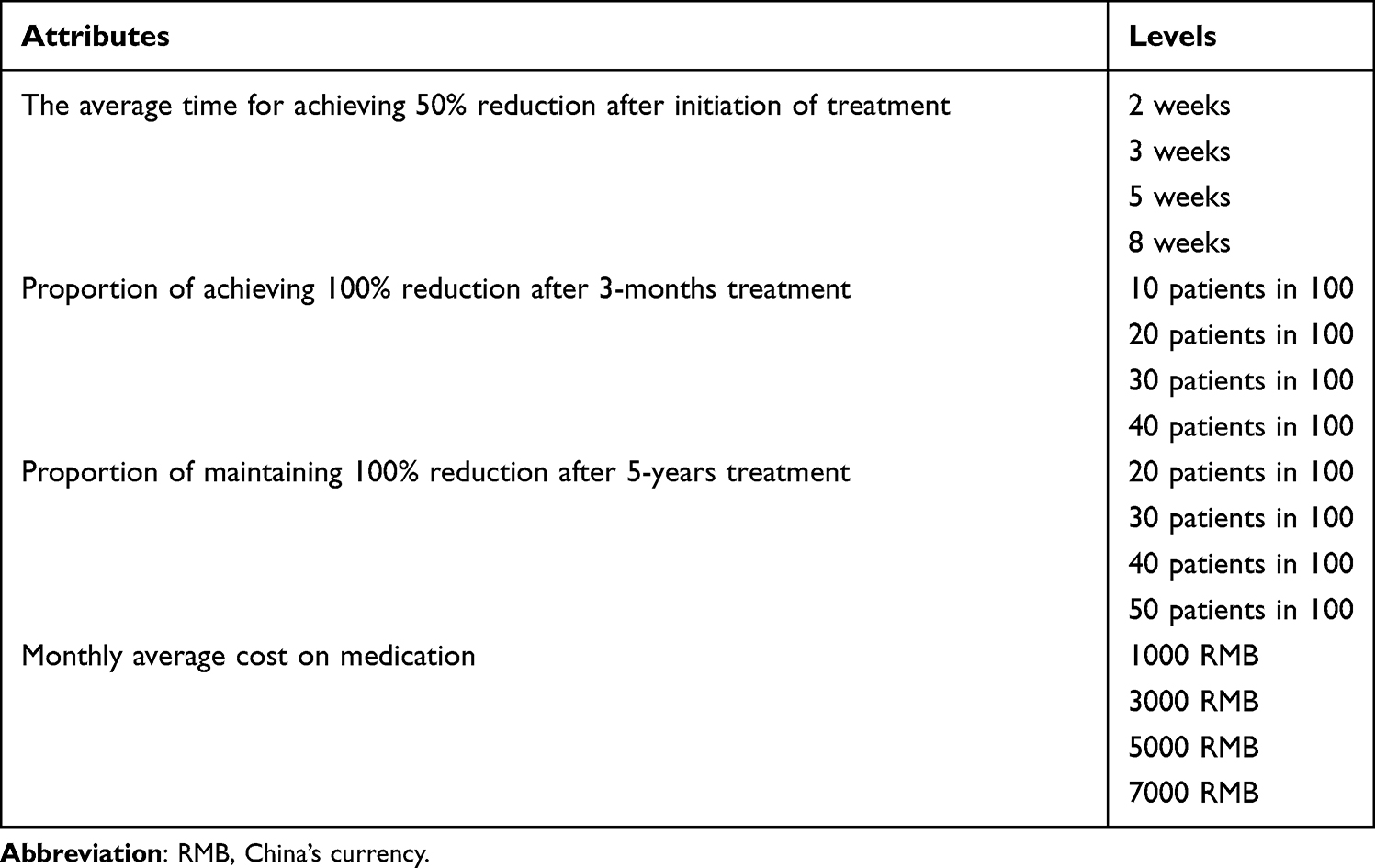 |
Table 1 Attributes and Levels in Discrete Choice Experiment |
Experimental Design and Survey
Based on the recommendations of experimental designs for discrete-choice experiments released by the ISPOR task force,22 the current study adopted a fractional factorial design to lighten respondent burden by reducing the number of choice sets. We used R Package “choiceDes” for a D-efficient experimental design. Designing using the D-efficient method results in orthogonality, level balance, minimum balance, and overlap, all favorable features. Then, 13 choice-set questions were generated from the design. Each choice set included two hypothetical treatment options: alternative of medication A and alternative of medication B. Figure 1 presents an example of a choice question (the questionnaire can be found in the following website: http://qs.focusrxonline.com/limesurvey/index.php/441618?lang=zh-Hans). The participants accessed an online survey website and answered the questionnaire. Prior to entering the DCE, the survey began with information about psoriasis, demographics, and disease-related questions. Thus, the study was designed to make it possible to complete the survey in approximately 30 minutes.
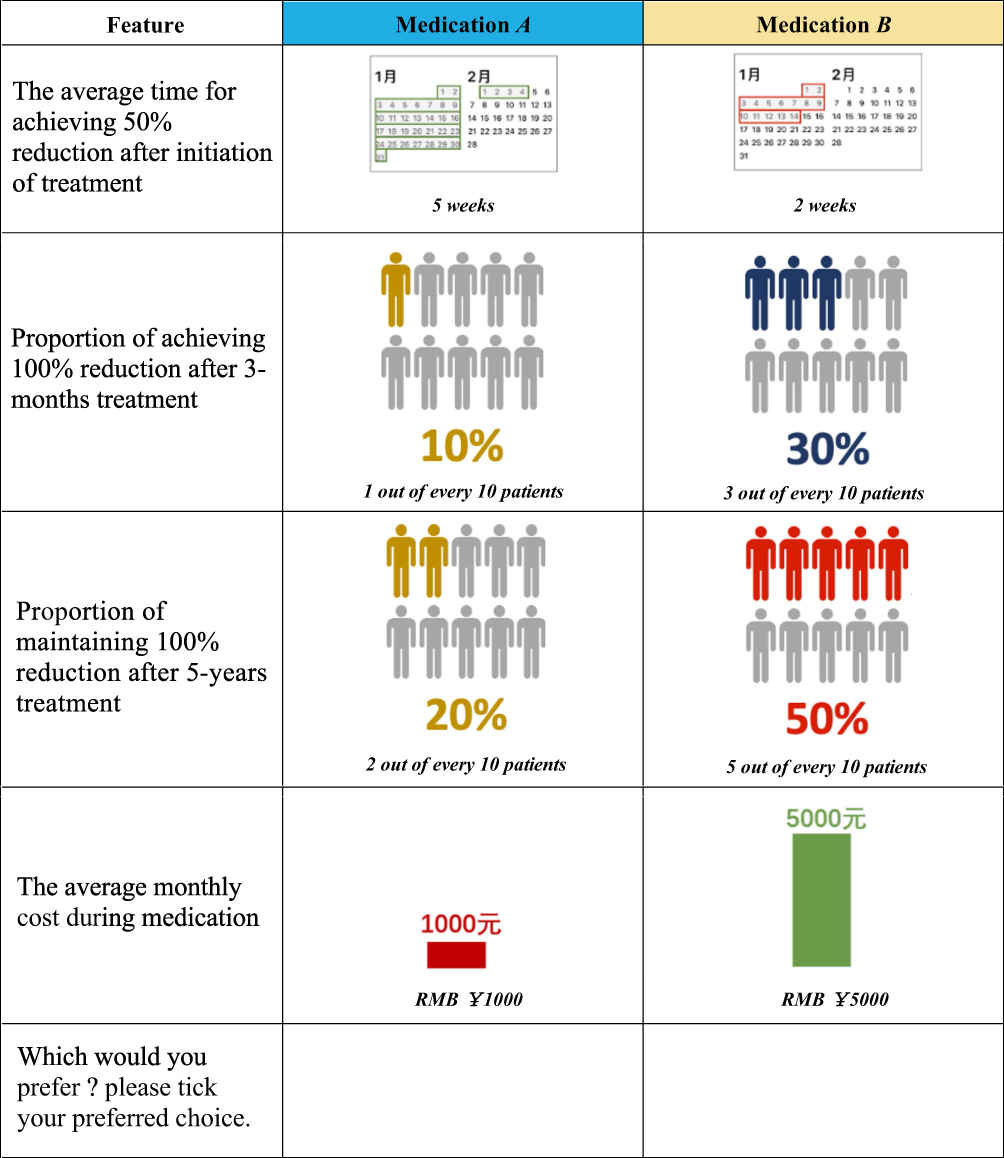 |
Figure 1 Example of presented discrete choice experiment question. |
Statistical Analysis
Before statistical analysis, we checked the quality of the collected questionnaires. If respondents chose either Medicine A or Medicine B for all choices, it indicated that they were inattentive to the choice questions. Therefore, the questionnaire results of the respondents will not be included. The rest of the questionnaire results are retained for statistical analysis. Then, statistical analysis was conducted based on the recommendations of statistical methods for the analysis of discrete choice experiments released by the ISPOR task force.23 Demographic data were analyzed using descriptive statistics. Using conditional logit models, we estimated preference weights for respondents’ choices among pairs of treatment alternatives, where the different treatment and cost aspects were entered as separate categorical variables (effects-coded). When coding effects, zero indicates the mean of all attribute levels rather than the omitted level as in dummy coding. With this procedure, each attribute level has a parameter estimate, where the parameter on the omitted level of each attribute is the negative sum of the parameters on the other levels of that attribute. The resulting log-odds estimates can be interpreted as preference weights. The relative importance (%) was calculated by dividing the distance between the highest and lowest preference weights for each attribute divided by the sum of all preference weight differences. Patient preference was assessed based on preference weights and relative importance.
The preference weights were used to estimate WTP for improvements in treatment efficacy. WTP is the mean maximum monetary equivalent that an individual is willing to pay for a given improvement in treatment efficacy. WTP represents the variation in out-of-pocket costs that yield a decrease in estimated utility that exactly balances the increase in utility yielded by an improved treatment efficacy. For example, WTP for an improvement in the average time for achieving 50% reduction after initiation of treatment from 5-weeks (WEEK5) to 4-weeks (WEEK4) is calculated as the level of cost (X) that satisfies following equation: −βCOST(X) = βWEEK4 −βWEEK5. β represents the coefficients for each attribute level. X may fall between two cost levels since the cost levels are categorical. Interpolating linearly was used between the preferences for the surrounding cost levels to determine the value of X.24
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The survey was approved by the medical ethics committee of the Renji Hospital, Shanghai, China (no. KY2020-110).
Results
Respondents
Totally, 613 individuals responded to the invitation, of which 456 consented and completed the survey. There were 437 patients who completed the questionnaire, among whom 201 had no variation in their responses and were excluded from the analysis.
The characteristics of the remaining 236 patients are summarized in Table 2. Most of the patients were male (approximately 62.3%), were 26–35 years old (approximately 46.2%), and had at least some college education (47%). Median monthly household income was between RMB ¥ 4000 and RMB ¥ 5999. The main psoriasis characteristics of these respondents were light red and partly scaly (approximately 40.3%). Most of these respondents whose psoriasis surface area was equal to the size of 3–5 hands (approximately 22.5%) and mainly distributed in the legs or hips (approximately 59.3%) and scalp (approximately 56.4%).
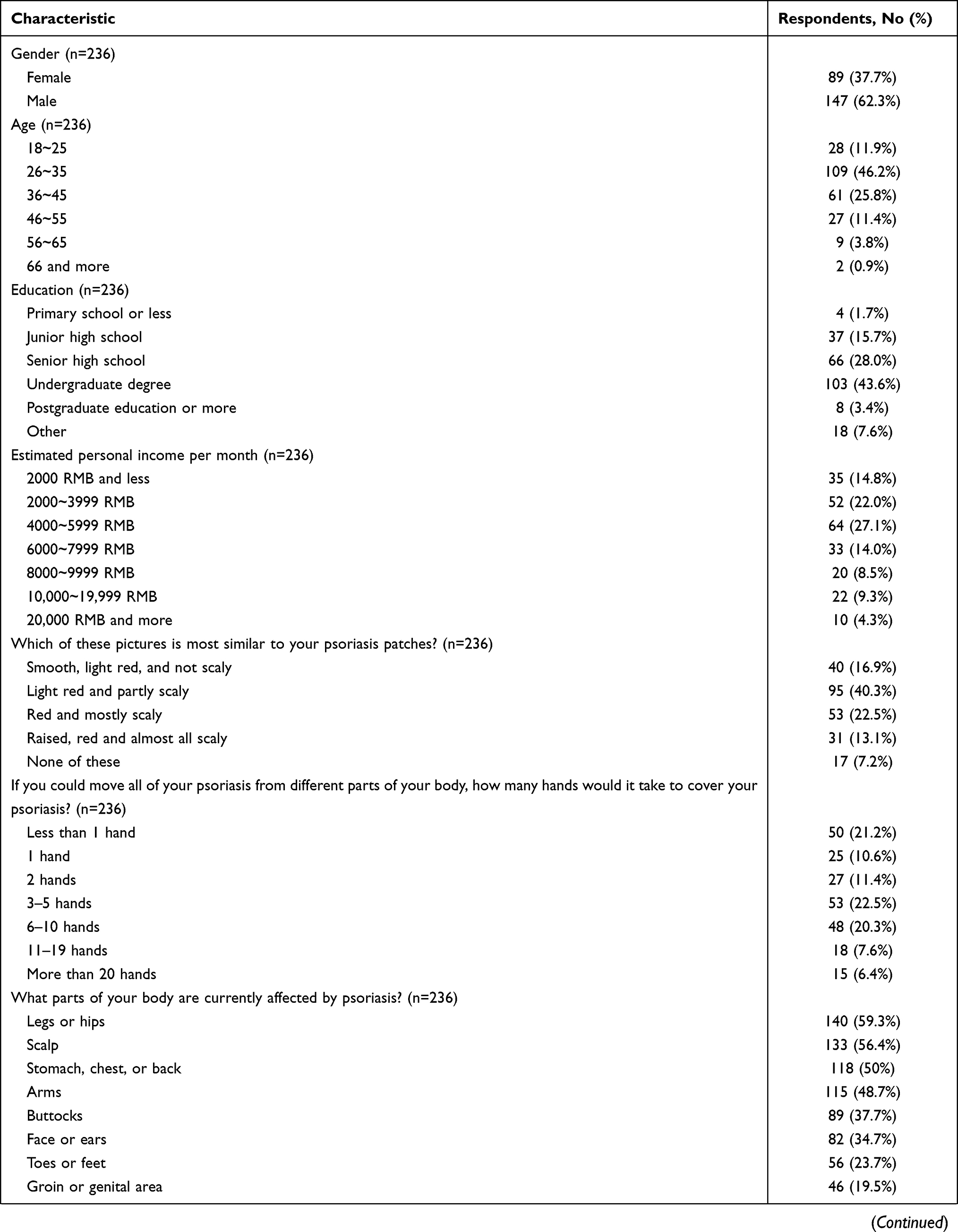 |  |  |
Table 2 Respondent Characteristics |
Weight of Factor Levels in the Entire Cohort
Among the participants, preference weights derived from the attribute levels indicated that the participants preferred lower costs of biologic treatments and a higher likelihood of retaining PASI 100 after three-month treatment. Preference weights derived from the attribute levels showed that the participants favored the lower cost of biologic treatments and higher probability of keeping PASI 100 at 3 months (Figure 2 and Supplementary Table 1). The distance score of the reduction of monthly costs from RMB ¥ 7000 to ¥ 1000 is 0.711, whereas improvements from 20% to 50% in the probability of keeping PASI 100 at 5-years is 0.164, improvements from 10% to 40% in the probability of achieving PASI100 at 3 months is 0.221, and improvements from 8 weeks to 2 weeks in the time to achieve PASI50 after initiation the biologic treatment is 0.101, respectively.
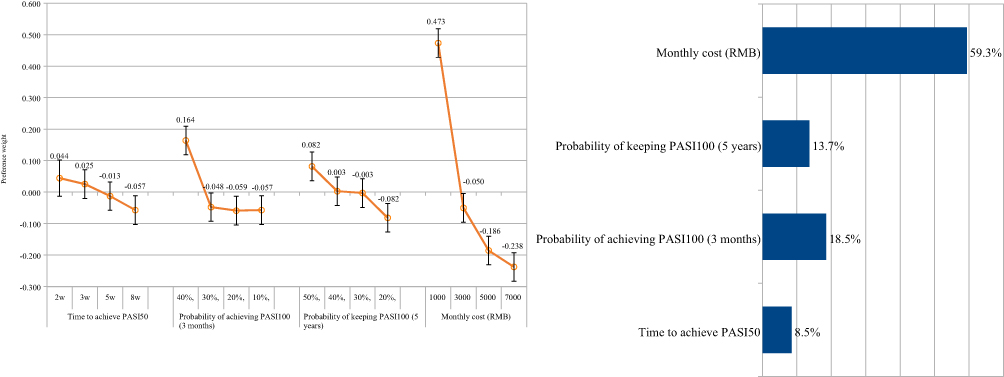 |
Figure 2 Preference weights for attribute levels and Relative importance of attributes (overall results, n = 236). Preference weights are showed on the vertical scale, describing how much each level was selected within one attribute. Non-overlapping error bars indicate statistically significant differences across levels within attributes; Relative importance is relatively described values calculated by the distance between the highest and the lowest attribute levels. |
Across all participants, the attribute regarded as the most important was monthly cost (relative importance [RI]: 59.4%), probability of achieving PASI100 at 3 months (RI: 18.5%), probability of keeping PASI100 at 5-years (RI: 13.6%) and time to achieve PASI50 after initiation the biologic treatment (RI: 8.5%).
Subgroup Analyses in Income Subgroup
According to the monthly income, entire cohort is divided into low-income subgroup and high-income subgroup based on the monthly income of less than 8000 and more than 8000.
Preference weights derived from the attribute levels showed that the high-income subgroup preferred the lower cost of biologic treatments and the time to achieve PASI50 after initiation of the biologic treatment (Figure 3). The distance score of the reduction of monthly costs from RMB ¥ 7000 to ¥ 1000 is 0.370, whereas improvements from 20% to 50% in the probability of keeping PASI 100 at 5-years is 0.110, improvements from 10% to 40% in the probability of achieving PASI100 at 3 months is 0.327, and improvements from 8 weeks to 2 weeks in the time to achieve PASI50 after initiation the biologic treatment is 0.223, respectively. Across all participants, the attribute regarded as most important was monthly cost (RI: 35.9%), probability of achieving PASI100 at 3-month (RI: 31.7%), probability of keeping PASI100 at 5-years (RI: 21.7%) and time to achieve PASI50 after initiation the biologic treatment (RI: 10.7%).
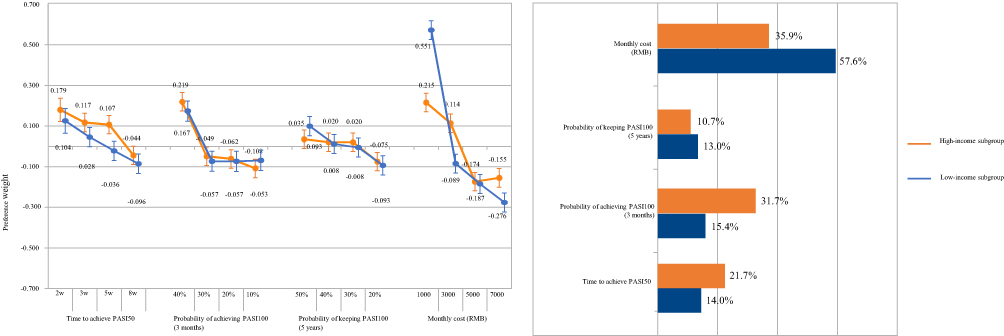 |
Figure 3 Preference weights for attribute levels and Relative importance of attributes. Orange represents the high-income subgroup (monthly income more than RMB ¥ 8000, n = 52); Blue represents the low-income subgroup (monthly income less than RMB ¥ 8000, n = 184). Preference weights are showed on the vertical scale, describing how much each level was selected within one attribute. Non-overlapping error bars indicate statistically significant differences across levels within attributes; Relative importance is relatively described values calculated by the distance between the highest and the lowest attribute levels. |
Preference weights derived from the attribute levels showed that the low-income subgroup favored the lower cost of biologic treatments, probability of keeping PASI100 at 5-years and the probability of achieving PASI100 at 3 months (Figure 3). The distance score of the reduction of monthly costs from RMB ¥ 7000 to 1000 is 0.83, whereas improvements from 20% to 50% in the probability of keeping PASI 100 at 5-years is 0.19, improvements from 10% to 40% in the probability of achieving PASI100 at 3 months is 0.22, and improvements from 8 weeks to 2 weeks in the time to achieve PASI50 after initiation the biologic treatment is 0.20, respectively. Among this subgroup participants, the attribute regarded as most important was monthly cost (relative importance [RI]: 57.6%), probability of achieving PASI100 at 3 months (RI: 15.4%), time to achieve PASI50 after initiation the biologic treatment (RI: 14%) and probability of keeping PASI100 at 5-years (RI: 13.0%).
Subgroup Analyses in Disease Condition Subgroup
According to the matching degree between the psoriasis and the picture features, the patients were divided into five subgroups: Mild, Moderate, Severe, Very Severe, Clear disease.
Preference weights derived from the attribute levels showed that the Mild disease subgroup preferred the lower cost of biologic treatments (RI: 34.9%), the probability of keeping PASI100 at 5-years (RI: 34.5%), the probability of achieving PASI100 at 3 months (RI: 24.6%) and the time to achieve PASI50 after initiation the biologic treatment (RI: 6.0%); Across the Moderate disease subgroup, the attribute regarded as the most important was the monthly cost (RI: 36.0%), and the time to achieve PASI50 after initiation the biologic treatment (RI: 25.8%), probability of achieving PASI100 at 3 months (RI: 20.2%), probability of keeping PASI100 at 5-years (RI: 17.9%), respectively; Preference weights showed that the Severe disease subgroup favored the lower cost of biologic treatments (RI: 39.6%), the probability of achieving PASI100 at 3 months (RI: 32.3%), the probability of keeping PASI100 at 5-years (RI: 19.2%) and the time to achieve PASI50 after initiation the biologic treatment (RI: 8.8%); And in very severe disease subgroup, the attribute regarded as the most important was the monthly cost (RI: 49.6%), probability of keeping PASI100 at 5-years (RI: 22.3%), probability of achieving PASI100 at 3 months (RI: 18.0%), and the time to achieve PASI50 after initiation the biologic treatment (RI: 10.1%); Across the Clear disease subgroup, the attribute regarded as the most important was the monthly cost (RI: 62.7%), and the time to achieve PASI50 after initiation the biologic treatment (RI: 25.9%), probability of achieving PASI100 at 3 months (RI: 10.4%), probability of keeping PASI100 at 5-years (RI: 1.0%), respectively. The distance scores of each attribute are summarized in Figure 4.
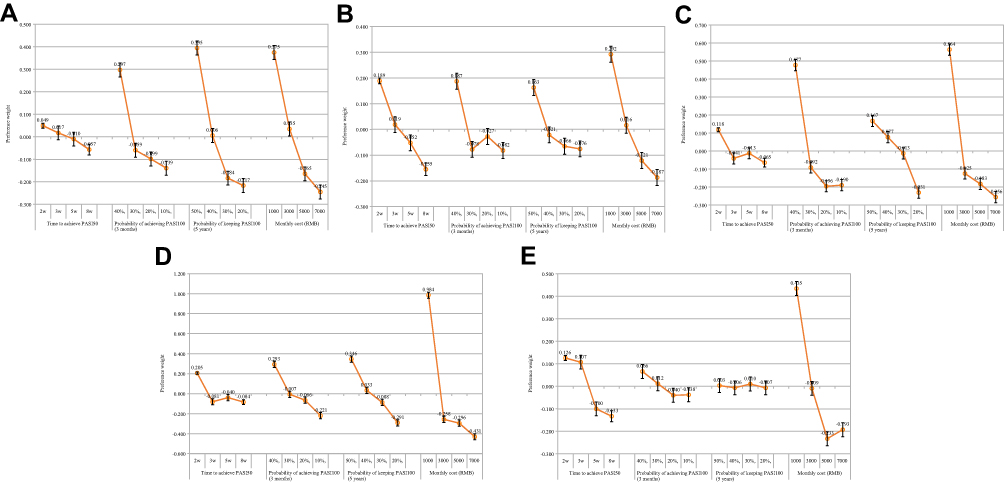 |
Figure 4 Preference weights for attribute levels (results in disease condition subgroup n =191). (A) Mild disease subgroup (n = 40); (B) moderate disease subgroup (n = 95); (C) severe disease subgroup (n = 53); (D) very severe disease subgroup (n = 31); (E) clear disease subgroup (n = 17). Preference weights are showed on the vertical scale, describing how much each level was selected within one attribute. Non-overlapping error bars indicate statistically significant differences across levels within attributes. |
Subgroup Analyses in Disease Location Subgroup
According to the disease location distributed in body, the entire cohort was divided into the following subgroups: Legs or hips, Toes and feet, Buttocks, Groin or genital area, Stomach, chest, or back, Arms, Fingers or hands, Nails, Neck, Face or ears, Scalp. Across the foot and toe subgroup, the attribute regarded as the most important was probability of keeping PASI100 at 5-years (RI: 37.3%), the monthly cost (RI: 34.1%), probability of achieving PASI100 at 3 months (RI: 22.8%), and the time to achieve PASI50 after initiation the biologic treatment (RI: 5.8%), respectively. And in leg and hip subgroup, the attribute regarded as the most important was the monthly cost (RI: 66.8%), probability of keeping PASI100 at 5-years (RI: 15.2%), probability of achieving PASI100 at 3 months (RI: 12.7%), and the time to achieve PASI50 after initiation of the biologic treatment (RI: 5.3%), respectively. Additionally, preference weights and relative importance of attributes in other disease location subgroups are displayed in Supplementary Figure 1-22.
Willingness to Pay
As expected, all patients were willing to pay more for improvement in probability of keeping PASI100 at 5-years (from RMB ¥666 to ¥1379), probability of achieving PASI100 at 3-month (from RMB ¥-15 to ¥1867) and time to achieve PASI50 after initiation of the biologic treatment (from RMB ¥376 to ¥858). The WTP estimates for improving treatment efficacy in other subgroups (monthly income subgroup, disease condition subgroup, disease location subgroup) are summarized in Table 3.
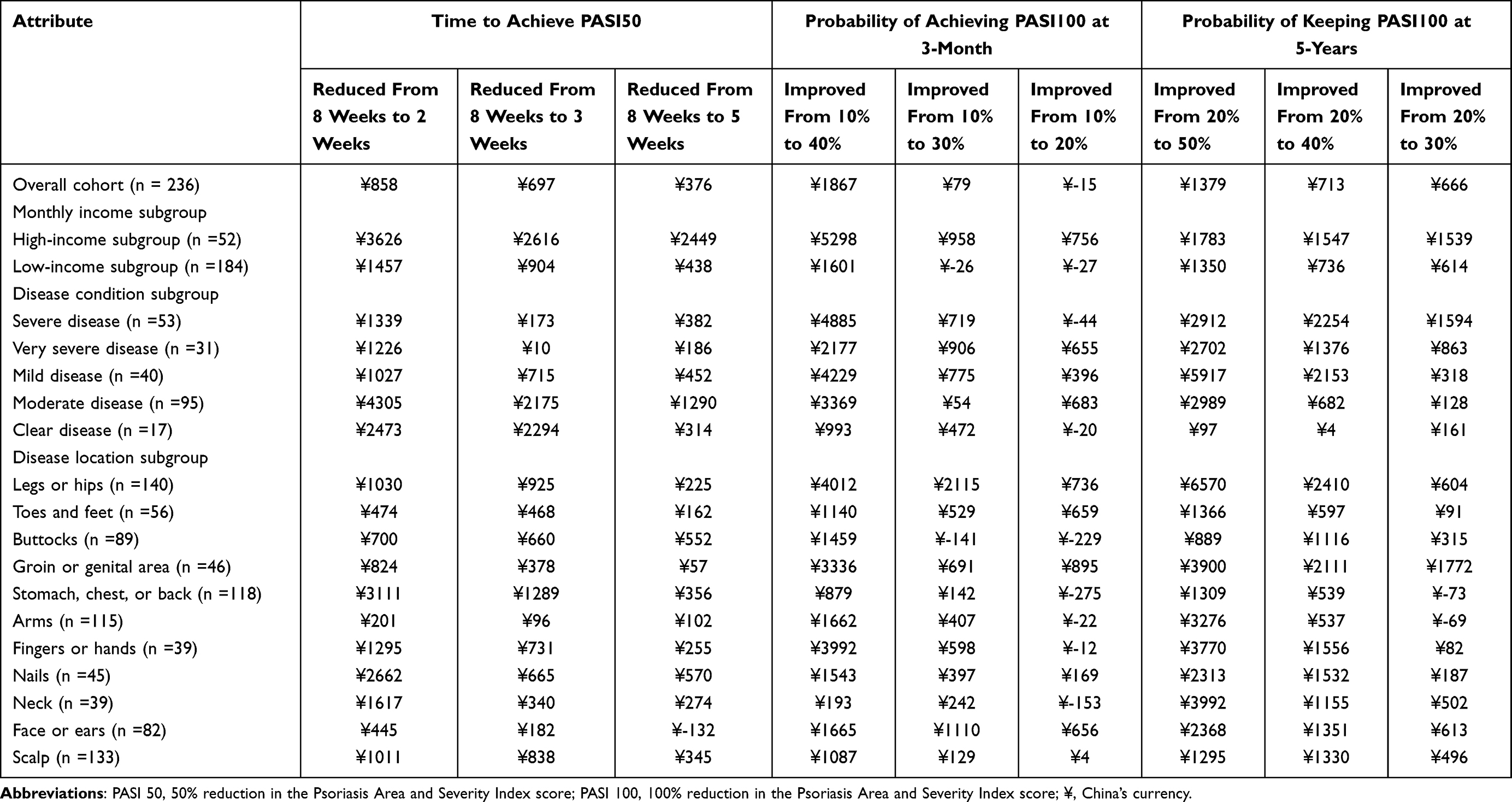 |
Table 3 Willingness to Pay for Improvements in Treatment Efficacy in Overall Cohort and Subgroup |
Discussion
Our study was designed to quantify and explore psoriasis patients’ preference among different biological agents from a Chinese perspective and estimated the WTP for different attributes. Among patients with psoriasis, non-adherence rates are high partly due to a disagreement between recommended treatments and individual preferences.25 Compliance can be greatly improved by following patients’ preference. To our knowledge, there are no relevant studies conducted in China, which to a large extent provide references for future research on psoriasis from the perspective of geographical location. All four attributes (the average time for achieving 50% reduction after initiation of treatment, proportion of achieving 100% reduction after 3-months treatment, proportion of maintaining 100% reduction after 5-years treatment and monthly average cost on medication) were consistent with a prior expectation in terms of the direction and magnitude of the estimated coefficients. Among them, the average time for achieving 50% reduction after initiation of treatment and proportion of achieving 100% reduction after 3-months treatment represented quick response, proportion of maintaining 100% reduction after 5-years treatment was related to the long-term, sustained efficacy.
Overall cohort and most subgroups, regardless of their individual characteristics, attached the highest importance to monthly cost. The probability of achieving PASI100 after 3-months treatment was the second preferred attribute by patients in the entire cohort. Additionally, in the monthly income subgroup, most of patients prioritized quick response (achieving PASI100 at 3-month) compared with long-term, sustained efficacy (achieving PASI100 at 5-year). Moreover, results showed high-income subgroup favored more about onset speed of efficacy than low-income subgroup. In contrast, low-income subgroup only attached the greatest interest to the monthly cost. A systematic review about psoriasis showed that many preference studies conducted previously focused on the efficacy and safety, especially from the perspective of physicians.26 However, from the patients’ point of view, several studies included the attribute of cost. For instance, a German study included the treatment expenditure per month in the process attributes and calculated the relative importance score (RIS) of participants stratified based on disease duration, number of previous therapies, etc.27 Another study conducted in German showed compared with other attributes, the attribute of cost is not given as much attention.28 Italian studies on biologics for psoriasis included the cost attribute and illustrated that treatment costs and expected therapeutic response concurrently can provide valuable insights which complement and improve the traditional risk-benefit profile and drive treatment decisions.29,30 Probably this depends on different health systems and medicine reimbursement policies in Europe. However, in the process of choosing treatment strategies, medical expenditure has gradually become an important factor for patients in the context of China. It may be due to the income gap between patients in developing and developed countries. With the progress of health insurance negotiations in China during recent two years, the price of biological agents has dropped significantly, to a certain extent, which met the needs of some patients who tend to use biological agents. But the price of biologic agents was still high compared with other types of therapy and became a factor affecting the patient’s choice when considering the cost. This finding indicated the expenditure should be raised extensive attention, especially in China. And one strategy, called “reduced doses”, can be used well for clinical setting to control the expenditure, which seek for the minimal doses necessary to reach a good response while achieving a potential reduction of adverse effects. Many studies on optimal dosing strategy using biologic agents for psoriasis involved advantages in terms of drug-exposure risk and cost saving.31–33 Regarding efficacy attribute, several DCE researches adopted PASI90 response for testing patients’ preferences on efficacy. For instance, Schaarschmidt’s finding indicated both patients and physicians considered PASI90 response is more important (RIS 21.4 and 20.8, respectively) than other attributes.34 But we chose PASI50 and PASI100 in our study, which were common endpoint of clinical trials. First, 50% and 100% reduction are easier to understand for participants than PASI 75 or PASI 90 response. Second, 50% reduction can roughly test participants the response to the concern about quick efficacy. Third, to determine whether or not the PASI50 response is still important for patients. Likewise, we found that quick response may be concerned as the secondary factor. It could indicate that psoriasis as facial skin disease has influences on patients’ appearance and impression, which are related to physiological and psychosocial function of patients.35 A higher incidence of anxiety and depression, along with lower quality of life, may be attributed to psoriasis. So, quick response may help patients with psoriasis get rid of the troubles caused by the disease.36 As for onset speed of efficacy, several studies on psoriasis-related treatment found that patients preferred differently. For instance, a research about patients with psoriasis preferred durability over onset speed of efficacy in psoriasis treatment in Japan.37 It is noteworthy that the most preferred element was “sustained efficacy after drug withdrawal” even though those drugs are not currently available in the clinical setting. In addition, for WTP, we can find from the results that patients are willing to spend higher costs for better efficacy. Especially in the high-income subgroup, the values of WTP for efficacy improving are higher than that in the low-income subgroup, which is consistent with our prior expectation. Clearly, the efficacy of biologic agents is still an unmet need for patients.
Several limitations exist in this study. Discrete choice experiment is a theoretical method, which that can be cognitively challenging. It means that actual patients might choose actual medications differently and participants are required to choose one of the two scenarios regardless of whether they like either. A direct conclusion based on individual preferences cannot be made from average preferences. Obviously, the treatment decisions made for each patient are based on their individual preferences. In order to better advise patients about their treatment options, physicians should be aware of what the majority of patients are concerned about and what their preferences are influenced by sociodemographic and disease-related characteristics. To optimize treatment satisfaction, adherence, and outcomes, physicians should incorporate their knowledge of each patient’s preferences, needs, and concerns into their therapeutic decisions. Some results of subgroup analyses are not consistent with our expectations due to the limited number of participants in the study. Subgroups with different demographic characteristics may differ significantly in their preferences, but a large sample size study is still required to verify this in the future. It is possible that some deviations will occur since the study was only conducted online. Several elderly patients may not be familiar with using digital devices, which limits the distribution of socio-demographic characteristics of participants in this survey. Additionally, the research questionnaire did not include a safety attribute. The safety profile is an important attribute among biologic agents, non-biologic systemic agents and topical compounds in the management of psoriasis.38,39 For example, the risk of infections caused by biologics is also a key safety profile.40 And during the COVID-19 pandemic, clinical management of patients with psoriasis is challenging due to their impaired immune status, especially for those using biologics inhibiting key pathogenic cytokines such as TNF-a and IL-17.41 In our study, the preferences were evaluated in patients with psoriasis using the biologic agents, and the risk of adverse events was similar among biologic agents. Some studies indicated that, despite individual risk tolerances, responders were willing to accept risks above likely clinical exposures to improve psoriasis symptoms or compatible with their personal and professional lifestyle.28,42 Considering that some biologic agents have just been listed in China, the efficacy and cost of biologic agents were primarily considered in order to estimate the economic burden, so this attribute was not included in our research questionnaire.
Conclusions
In conclusion, people are concerned about treatment cost when making decisions regarding the biological treatment regardless of incomes. In the efficacy attribute, the probability of achieving PASI100 at 3-month was the most sensitive factor. Clinicians might change their perceptions of what aspects of treatment plans need to be discussed with patients and their families during consultations based on our findings. It is necessary to conduct future studies using larger and more representative samples to enforce our current findings and to facilitate the measurement of potential preference heterogeneity among individuals.
Ethics Statement
Ethical approval was obtained from the Renji Hospital (no. KY2020-110).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; All authors took part in drafting the article or revising it critically for important intellectual content and agreed to submit to the current journal; All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Funding
This study was funded by Lilly Suzhou Pharmaceutical Co. Ltd.
Disclosure
Erjia Ye and Guanshen Dou are employees of Eli Lilly and Company. The other authors have no conflicts of interest.
References
1. Parisi R, Symmons DPM, Griffiths CEM, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Investigative Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339
2. World Health Organization (WHO). Global report on psoriasis. Published online October 26; 2016. Available from: https://www.who.int/publications/i/item/global-report-on-psoriasis.
3. Charles C, Gafni A. The vexing problem of defining the meaning, role and measurement of values in treatment decision-making. J Comp Eff Res. 2014;3(2):197–209. doi:10.2217/cer.13.91
4. Umar N, Yamamoto S, Loerbroks A, Terris D. Elicitation and use of patients’ preferences in the treatment of psoriasis: a systematic review. Acta Derm Venerol. 2012;92(4):341–346. doi:10.2340/00015555-1304
5. Ontario Health (Quality). Home narrowband ultraviolet B phototherapy for photoresponsive skin conditions: a health technology assessment. Ont Health Technol Assess Ser. 2020;20(12):1–134.
6. Thaçi D, de la Cueva P, Pink AE, et al. General practice recommendations for the topical treatment of psoriasis: a modified-Delphi approach. BJGP Open. 2020;4(5):34. doi:10.3399/bjgpopen20X101108
7. Sacristán JA, Dilla T, Díaz-Cerezo S, Gabás-Rivera C, Aceituno S, Lizán L. Patient-physician discrepancy in the perception of immune-mediated inflammatory diseases: rheumatoid arthritis, psoriatic arthritis and psoriasis. A qualitative systematic review of the literature. PLoS One. 2020;15(6):e0234705. doi:10.1371/journal.pone.0234705
8. Feldman SR, Regnier SA, Chirilov A, Hey F, Gilloteau I, Cella D. Patient-reported outcomes are important elements of psoriasis treatment decision making: a discrete choice experiment survey of dermatologists in the United States. J Am Acad Dermatol. 2019;80(6):1650–1657. doi:10.1016/j.jaad.2019.01.039
9. Zhang M, Carter C, Olson WH, et al. Patient preference for dosing frequency based on prior biologic experience. J Drugs Dermatol. 2017;16(3):220–226.
10. Tada Y, Ishii K, Kimura J, Hanada K, Kawaguchi I. Patient preference for biologic treatments of psoriasis in Japan. J Dermatol. 2019;46(6):466–477. doi:10.1111/1346-8138.14870
11. Mühlbacher AC, Juhnke C, Beyer AR, Garner S. Patient-focused benefit-risk analysis to inform regulatory decisions: the European Union perspective. Value Health. 2016;19(6):734–740. doi:10.1016/j.jval.2016.04.006
12. Ho M, Saha A, McCleary KK, et al. A framework for incorporating patient preferences regarding benefits and risks into regulatory assessment of medical technologies. Value Health. 2016;19(6):746–750. doi:10.1016/j.jval.2016.02.019
13. Ghoreschi K, Balato A, Enerbäck C, Sabat R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet. 2021;397(10275):754–766. doi:10.1016/S0140-6736(21
14. Gonzalez JM. Evaluating risk tolerance from a systematic review of preferences: the case of patients with psoriasis. Patient. 2018;11(3):285–300. doi:10.1007/s40271-017-0295-z
15. de Bekker-grob EW, Donkers B, Jonker MF, Stolk EA. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient. 2015;8(5):373–384. doi:10.1007/s40271-015-0118-z
16. Goossens LMA, Jonker MF, Rutten-van Mölken MPMH, et al. The fold-in, fold-out design for DCE choice tasks: application to burden of disease. Med Decis Making. 2019;39(4):450–460. doi:10.1177/0272989X19849461
17. Vass C, Rigby D, Payne K. The role of qualitative research methods in discrete choice experiments. Med Decis Making. 2017;37(3):298–313. doi:10.1177/0272989X16683934
18. Johnson FR, Banzhaf MR, Desvousges WH. Willingness to pay for improved respiratory and cardiovascular health: a multiple-format, stated-preference approach. Health Econ. 2000;9(4):295–317. doi:10.1002/1099-1050(200006)9:4<295::
19. Johnson FR, Mohamed AF, Zdemir SÖ, Marshall DA, Phillips KA. How does cost matter in health-care discrete-choice experiments? Health Econ. 2011;20(3):323–330. doi:10.1002/hec.1591
20. Fairchild AO, Reed SD, Johnson FR, Anglin G, Wolka AM, Noel RA. What is clearance worth? Patients’ stated risk tolerance for psoriasis treatments. J Dermatolog Treat. 2017;28(8):709–715. doi:10.1080/09546634.2017.1329499
21. Goh SSL, Lai PSM, Liew SM, Tan KM, Chung WW, Chua SS. Development of a PATIENT-Medication Adherence Instrument (P-MAI) and a HEALTHCARE PROFESSIONAL-Medication Adherence Instrument (H-MAI) using the nominal group technique. PLoS One. 2020;15(11):e0242051. doi:10.1371/journal.pone.0242051
22. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
23. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical Methods for the Analysis of Discrete Choice Experiments: a Report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
24. Hauber AB, Han S, Yang JC, et al. Effect of pill burden on dosing preferences, willingness to pay, and likely adherence among patients with type 2 diabetes. Patient Prefer Adherence. 2013;7:937–949. doi:10.2147/PPA.S43465
25. Schmieder A, Schaarschmidt ML, Umar N, et al. Comorbidities significantly impact patients’ preferences for psoriasis treatments. J Am Acad Dermatol. 2012;67(3):363–372. doi:10.1016/j.jaad.2011.08.023
26. Sain N, Willems D, Charokopou M, Hiligsmann M. The importance of understanding patient and physician preferences for psoriasis treatment characteristics: a systematic review of discrete-choice experiments. Curr Med Res Opin. 2020;36(8):1257–1275.
27. Schaarschmidt ML, Umar N, Schmieder A, et al. Patient preferences for psoriasis treatments: impact of treatment experience: treatment experience impacts patient preferences. J Eur Acad Dermatol Venereol. 2013;27(2):187–198. doi:10.1111/j.1468-3083.2011.04440.x
28. Schaarschmidt ML. Patient preferences for psoriasis treatments: process characteristics can outweigh outcome attributes. Arch Dermatol. 2011;147(11):1285. doi:10.1001/archdermatol.2011.309
29. Zagni E, Bianchi L, Fabbrocini G, et al. A real-world economic analysis of biologic therapies for moderate-to-severe plaque psoriasis in Italy: results of the CANOVA observational longitudinal study. BMC Health Serv Res. 2021;21(1):924. doi:10.1186/s12913-021-06866-7
30. Torbica A, Fattore G, Ayala F. Eliciting preferences to inform patient-centred policies: the case of psoriasis. PharmacoEconomics. 2014;32(2):209–223. doi:10.1007/s40273-013-0126-6
31. Llamas-Velasco M, Daudén E. Reduced doses of biological therapies in psoriasis may increase efficiency without decreasing drug survival. Dermatol Ther. 2020;33(6):e14134. doi:10.1111/dth.14134
32. Hansel K, Bianchi L, Lanza F, Bini V, Stingeni L. Adalimumab dose tapering in psoriasis: predictive factors for maintenance of complete clearance. Acta Derm Venereol. 2017;97(3):346–350. doi:10.2340/00015555-2571
33. Piaserico S, Gisondi P, De Simone C, et al. Down-titration of adalimumab and etanercept in psoriatic patients: a multicentre observational study. Acta Derm Venereol. 2016;96(2):251–252. doi:10.2340/00015555-2209
34. Schaarschmidt M, Herr R, Gutknecht M, et al. Patients’ and physicians’ preferences for systemic psoriasis treatments: a nationwide comparative discrete choice experiment (PsoCompare). Acta Derm Venerol. 2018;98(2):200–205. doi:10.2340/00015555-2834
35. Kelly A, Ryan C. Genital psoriasis: impact on quality of life and treatment options. Am J Clin Dermatol. 2019;20(5):639–646.
36. Martínez-Ortega JM, Nogueras P, Muñoz-Negro JE, Gutiérrez-Rojas L, González-Domenech P, Gurpegui M. Quality of life, anxiety and depressive symptoms in patients with psoriasis: a case-control study. J Psychosom Res. 2019;124:109780.
37. Tada Y, Ishii K, Kimura J, Hanada K, Kawaguchi I. Patient preference for biologic treatments of psoriasis in Japan. J Dermatol. 2019;46(6):466–477.
38. Marques E, Paluch Z, Boháč P, Slanař O, Běláček J, Hercogová J. The safety profile of biologic agents in comparison with non-biologic systemic agents, and topical compounds in the management of psoriasis-A 30-month prospective, observational cohort study. Int J Clin Pract. 2021;75(12):e14915. doi:10.1111/ijcp.14915
39. Campanati A, Ganzetti G, Giuliodori K, Molinelli E, Offidani A. Biologic therapy in psoriasis: safety profile. CDS. 2016;11(1):4–11. doi:10.2174/1574886310666151014115532
40. De Simone C, Fargnoli MC, Amerio P, et al. Risk of infections in psoriasis: assessment and challenges in daily management. Expert Rev Clin Immunol. 2021;17(11):1211–1220. doi:10.1080/1744666X.2021.1997592
41. Talamonti M, Galluzzo M, Chiricozzi A, et al. Management of biological therapies for chronic plaque psoriasis during COVID-19 emergency in Italy. J Eur Acad Dermatol Venereol. 2020;34(12):e770–e772. doi:10.1111/jdv.16841
42. Kauf TL, Yang JC, Kimball AB, et al. Psoriasis patients’ willingness to accept side-effect risks for improved treatment efficacy. J Dermatological Treatment. 2015;26(6):507–513. doi:10.3109/09546634.2015.1034071
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.